
INTRODUCTION
Acute myeloid leukemia (AML) is a serious disease of the hematopoietic system characterized by de-differentiation and uncontrolled proliferation of immature hematopoietic precursor cells in the bone marrow [1]. It is usually based on many parameters including age, white blood cell count, cytogenetic abnormalities, and specific mutations [2]. AML results from the accumulation of genetic and epigenetic alterations during the multistep process of tumorigenesis, including activation of oncogenes and/or inactivation of tumor suppressor genes.
The Wilms’ tumor gene 1 (WT1), located at chromosome 11p13, was firstly cloned in 1990 as a suppressor in Wilms’ tumor [3]. WT1 regulates transcription, RNA metabolism, translation and both oncogenic and tumor suppressor functions [4]. Since the expression of WT1 in many solid cancers is upregulated, it is considered as a potential oncogene [5]. Although the pathogenesis of WT1 in leukemia has not been completely revealed, the phenomenon that low expression of WT1 and high expression of WT1 are accompanied with clinical remission and relapse respectively shows that WT1 may be a potential prognostic factor in acute leukemia [6].
Although a number of studies suggested that WT1 rs16754 polymorphism might be related to decreased relapse free survival (RFS) and overall survival (OS). The results remain controversial [7-18]. In this study, meta-analysis of the association between WT1 rs16754 polymorphism and OS and RFS of AML was conducted. Twelve studies involving 3903 patients with AML are pooled in the meta-analysis.
RESULTS
Characteristics of the studies
The flow chart in Figure 1 summarizes this literature review process. Twelve publications with 3903 AML patients had met the inclusion criteria and were included in this meta-analysis. Seven studies were conducted in Caucasians, 3 were conducted in Asians, and the remaining 2 studies were conducted in mixed ethnic groups. Two studies included child and the remaining studies included adults. Characteristics of the included studies are shown in Table 1.
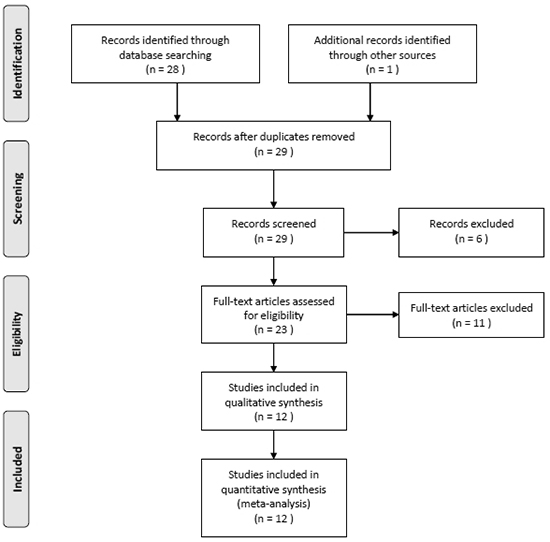
Figure 1: Study flow diagram of included studies.
Table 1: Characteristics of the included studies
No. |
First author |
Year |
Study design |
Race |
Age |
Female (%) |
Subtype |
Sample size |
Adjusted for OS |
Adjusted for RFS |
|---|---|---|---|---|---|---|---|---|---|---|
1 |
Damm |
2010 |
Cohort |
Caucasian |
45 |
48 |
CN-AML |
249 |
NPM1/FLT3 mutation status, age, Platelet, CEBPA mutation status, WBC |
NPM1/FLT3 mutation status, Platelet, CEBPA mutation status, WBC |
2 |
Hollink |
2010 |
Cohort |
Caucasian |
9 |
40 |
Mix |
272 |
NA |
NA |
3 |
Wagner |
2010 |
Cohort |
Caucasian |
49 |
83 |
CN-AML |
275 |
Age, IDH1 SNP rs11554137, NPM1/FLT3 mutation status, Platelets |
NPM1 mutation status, CEBPA mutation status |
4 |
Becker |
2011 |
Cohort |
Mix |
62 |
50 |
CN-AML |
433 |
NA |
NA |
5 |
Ho |
2011 |
Cohort |
Mix |
10 |
45 |
NA |
790 |
Risk group, WBC, race |
Risk group, WBC, race |
6 |
Renneville |
2011 |
Cohort |
Caucasian |
51 |
46 |
Mix |
511 |
NA |
NA |
7 |
Damm |
2012 |
Cohort |
Caucasian |
47 |
48 |
CN-AML |
269 |
ID1, age, BAALC expression, Platelets, FLT3-ITD, CEBPA mutation |
ID1, Platelets, NPM1 mutation, CEBPA mutation |
8 |
Choi |
2012 |
Cohort |
Asian |
42 |
63 |
CN-AML |
73 |
NA |
NA |
9 |
Luna |
2012 |
Cohort |
Caucasian |
62 |
43 |
de novo AML |
175 |
NPM1, FLT3-ITD, and CEBPA, expression levels of WT1, age, WBC count, platelet count, hemoglobin level, percentage of blood blasts, cytogenetic risk group, and FAB classification |
NPM1, FLT3-ITD, and CEBPA, expression levels of WT1, age, WBC count, platelet count, hemoglobin level, percentage of blood blasts, cytogenetic risk group, and FAB classification |
10 |
Luo |
2014 |
Cohort |
Asian |
45 |
58 |
de novo non-M3 AML |
182 |
Age, percentage of blood blasts, WT1 expression, WBC, FLT3 |
Age, percentage of blood blasts, WT1 expression, WBC, FLT3 |
11 |
Niavarani |
2015 |
Cohort |
Caucasian |
45 |
55 |
CN-AML |
469 |
Age, sex, WBC, secondary disease, performance status, FLT3-ITD, and NPM1 mutations |
Age, sex, WBC, secondary disease, performance status, FLT3-ITD, and NPM1 mutations |
12 |
Zhang |
2015 |
Cohort |
Asian |
40 |
46 |
Mix |
205 |
Risk stratification, allogeneic hematopoietic stem cell transplantation |
Risk stratification, allogeneic hematopoietic stem cell transplantation |
Association between WT1 rs16754 polymorphism and OS of AML
When all eligible studies were pooled into one dataset for the meta-analysis, we found WT1 rs16754 polymorphism was significantly associated with OS in AML (OR = 0.62; 95% CI 0.52 – 0.75; p < 0.00001; Figure 2). In the subgroup analysis of race, both Asians and Caucasians showed better OS in AML (OR = 0.61; 95% CI 0.43 – 0.85; p = 0.004; and OR = 0.60; 95% CI 0.44 – 0.81; p = 0.001). In addition, both de novo AML and CN-AML showed better OS in AML (OR = 0.40; 95% CI 0.24 – 0.67; p = 0.0004; and OR = 0.60; 95% CI 0.43 – 0.84; p = 0.001). In a further stratified analysis by age, both children and adults showed better OS in AML (OR = 0.67; 95% CI 0.51 – 0.88; p = 0.004; and OR = 0.60; 95% CI 0.47 – 0.75; p < 0.0001). The results were showed in Table 2.
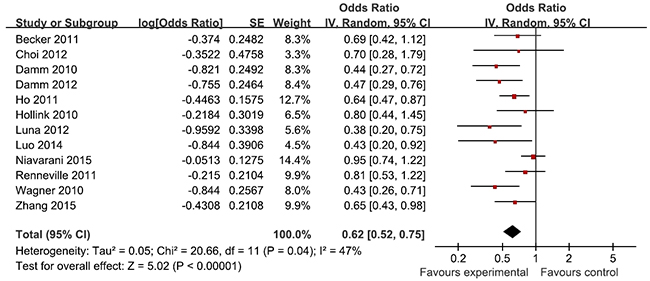
Figure 2: Meta-analysis of the association between WT1 rs16754 polymorphism and OS of AML.
Table 2: Results of the meta-analysis
OR (95% CI) |
P Value |
I2 (%) |
p Value |
|
|---|---|---|---|---|
OS |
0.62 (0.52-0.75) |
<0.00001 |
47 |
0.04 |
Subtype |
||||
de novo AML |
0.40 (0.24-0.67) |
0.0004 |
0 |
0.82 |
CN-AML |
0.60 (0.43-0.84) |
0.003 |
67 |
0.009 |
Race |
||||
Asian |
0.61 (0.43-0.85) |
0.004 |
0 |
0.61 |
Caucasian |
0.60 (0.44-0.81) |
0.001 |
69 |
0.004 |
Age |
||||
<18 years |
0.67 (0.51-0.88) |
0.004 |
0 |
0.50 |
>18 years |
0.60 (0.47-0.75) |
<0.0001 |
55 |
0.02 |
RFS |
0.69 (0.57-0.83) |
<0.001 |
46 |
0.04 |
Subtype |
||||
de novo AML |
0.42 (0.26-0.68) |
0.0004 |
0 |
0.49 |
CN-AML |
0.74 (0.62-0.88) |
0.007 |
36 |
0.12 |
Race |
||||
Asian |
0.61 (0.42-0.88) |
0.008 |
0 |
0.65 |
Caucasian |
0.64 (0.49-0.85) |
0.002 |
63 |
0.001 |
Age |
||||
<18 years |
0.74 (0.55-1.00) |
0.05 |
0 |
0.50 |
>18 years |
0.68 (0.54-0.85) |
0.0006 |
55 |
0.02 |
Association between WT1 rs16754 polymorphism and RFS of AML
As for RFS of AML, WT1 rs16754 polymorphism was found to be significantly associated with RFS (OR = 0.69; 95% CI 0.57 – 0.83; p < 0.001; Figure 3). In the subgroup analysis of race, both Asians and Caucasians with this polymorphism exhibited better RFS in AML (OR = 0.61; 95% CI 0.42 – 0.88; p = 0.008; and OR = 0.64; 95% CI 0.49 – 0.85; p = 0.002). In terms of AML subtype, both de novo AML and CN-AML displayed better RFS in AML (OR = 0.42; 95% CI 0.26 – 0.68; p = 0.0004; and OR = 0.74; 95% CI 0.62 – 0.88; p = 0.007). In the stratified analysis by age, a significantly better RFS was found among children (OR = 0.74; 95% CI 0.55 – 1.00; p = 0.05), and was also found among adults (OR = OR = 0.68; 95% CI 0.54 – 0.85; p = 0.0006). The results were listed in Table 2.
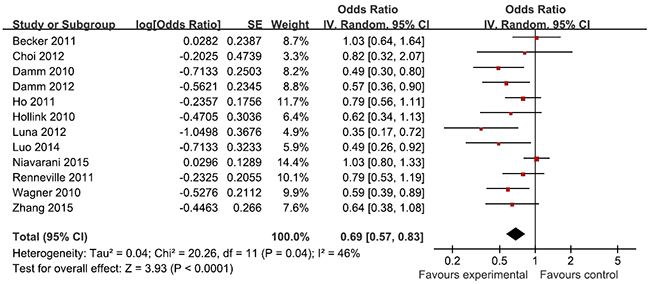
Figure 3: Meta-analysis of the association between WT1 rs16754 polymorphism and RFS of AML.
Sensitivity analyses and publication bias
The results of sensitivity analyses showed that the estimates before and after the deletion of each study were similar (Figures 4 and 5). The shapes of the funnel plot seemed symmetrical (Figures 6 and 7), suggesting that there was no obvious publication bias.
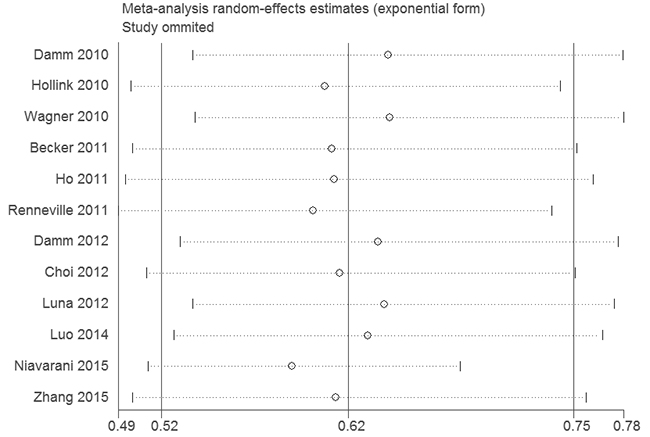
Figure 4: Sensitivity analysis of the association between WT1 rs16754 polymorphism and OS of AML.
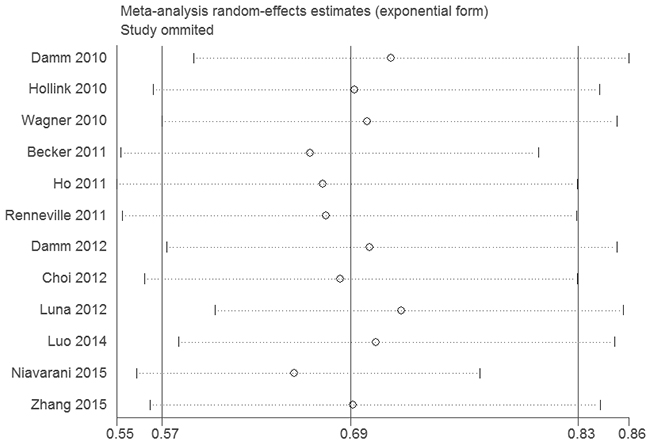
Figure 5: Sensitivity analysis of the association between WT1 rs16754 polymorphism and RFS of AML.
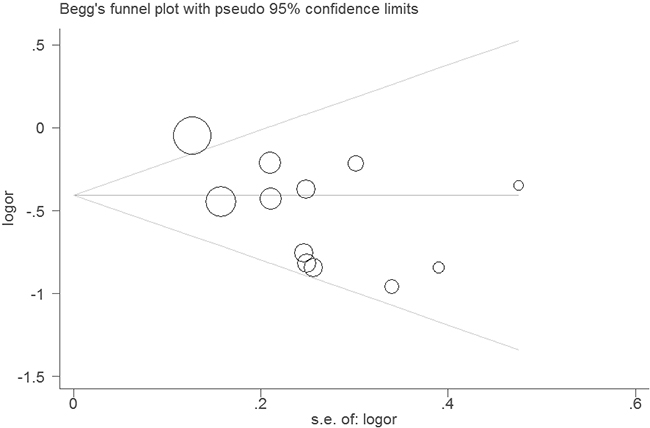
Figure 6: Funnel plot of the association between WT1 rs16754 polymorphism and OS of AML.
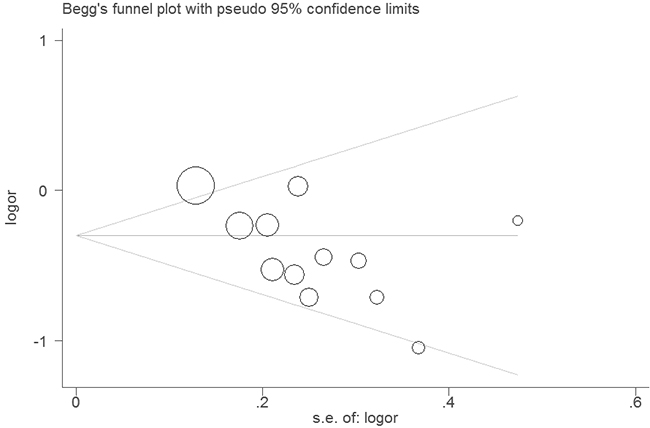
Figure 7: Funnel plot of the association between WT1 rs16754 polymorphism and RFS of AML.
DISCUSSION
Many studies have investigated the relation of WT1 rs16754 polymorphism with prognosis of AML, but the conclusions are still controversial. In view of this issue, we comprehensively analyzed the association between WT1 rs16754 polymorphism and OS or RFS of AML via the method of meta-analysis, and found that WT1 rs16754 polymorphism affected the survival of AML. Thus, WT1 rs16754 polymorphism might be a prognostic factor of AML.
WT1 expression is detectable in CD34+ progenitor cells, but is down-regulated during the process of hematopoietic differentiation, and undetectable in mature leukocytes [19]. WT1 overexpression could be observed in the majority of AML patients at diagnosis, which disappeared when complete remission (CR) was achieved by chemotherapy. Hence, WT1 expression has been regarded as a potential biomarker for the detection of minimal residual dis-ease (MRD) in clinic [20]. Ujj et al. also suggested that disappearance of WT1-positivity during chemotherapy had a favorable effect on survival [21]. Casalegno-Garduño et al. indicated that WT1 is a suitable marker for the detection of minimal residual disease after SCT or chemotherapy [22]. Recently, analysis of WT1 expression in circulating RNA in plasma in AML patients could be a simple, convenient and noninvasive method to predict latent information about relapse [23]. WT1 rs16754 polymorphism consists in a change ofthe nucleotide adenine (A) into guanine (G). Zhang et al. found that the WT1 GG patients showed significantly higher WT1 mRNA expression than the WT1 GA/AA patients [18]. Thus, it might be the reason for why WT1 rs16754 polymorphism could influence the survival of AML.
We performed sensitivity analysis by excluding studies to verify the stability of results. However, this present study also has some limitations. First, the sample size was relatively small in subgroup analyses. Second, significant heterogeneity was detected in included studies and the accuracy of results would be affected in spite of utilizing the random-effects model to calculate pooled ORs. Third, we didn’t explore gene-gene and gene-environment interactions because of the insufficient data. Finally, this study is a meta-analysis of case-control study and cohort study. Confounding cannot be avoided and should be considered.
In conclusion, WT1 rs16754 polymorphism is associated with better survival of AML. It could be used as a cost-effective prognostic biomarker for AML.
MATERIALS AND METHODS
Publication search
Published reports were searched in PubMed, EMBASE, and Google Scholar, with the following key words: “acute myeloid leukemia” and “Wilms’ tumor gene 1”. The MeSH terms, such as “leukemia, myeloid, acute” and “genes, wilms tumor”, were used. Publication language was not restricted in this search. Reference lists of articles retained for review were examined manually to further identify potentially relevant reports.
Study selection
Two reviewers independently screened the abstracts of papers identified by the literature search, retrieved potentially relevant studies and determined study eligibility. Studies were included if: (1) study design was prospective or retrospective cohort study; (2) the exposure of interest was WT1 rs16754 polymorphism; (3) the studied reported relative risks (RRs), hazard ratios (HRs), or odds ratios (ORs) with corresponding 95% confidence intervals (CIs); and (4) the outcome was RFS or OS. If the same cohort was used in more than one publication, we included the publication that reported the results in greater detail or, if similar, the one with the largest number of cases. Data published only in abstract form were excluded. Case reports, review articles and commentary articles were also excluded.
Data extraction
The following data including: the first author, year, study design, ethnicity of the study population, age, sex, subtype, number of patients included in analysis, adjusted factors, and OR with its 95% CI for OS and RFS were extracted from each eligible study by two investigators.
Statistical analysis
The strength of association between WT1 rs16754 polymorphism and RFS and OS of AML was evaluated by calculating the OR and 95% CI. To assess the significance of OR, we conducted the Z test and we regarded it as significant difference when P value less than 0.05 was detected. Moreover, X2 based Q and I2 test were performed to evaluate the between-study heterogeneity and P<0.1 was defined as statistical significance. The random-effects was used to calculated the OR if significant heterogeneity existed. Otherwise, the fixed-effects model was applied. Furthermore, we also conducted subgroup analyses stratified by ethnicity (Caucasian and Asian), age (child and adult), and subtype of AML. Publication bias was assessed by asymmetry of funnel plots. In sensitivity analysis, we sequentially excluded each study on the software to evaluate the stability of the results. We conducted all the analyses by using software Review Manager 5.1 (Nordic Cochrane Center, Copenhagen, Denmark) and STATA 11.0 software (Stata Corporation, College Station, TX, USA).
ACKNOWLEDGMENTS
This work was supported by National Natural Science Foundation of China (81300421), Science and Technology Planning Project of Guangdong Province (2012B031800032, 2013B021800284), Doctoral Fund of Ministry of Education of China (20130171120054), and Guangdong Natural Science Foundation (S2013040014343).
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
1. Zhang H, Alberich-Jorda M, Amabile G, Yang H, Staber PB, Di Ruscio A, Welner RS, Ebralidze A, Zhang J, Levantini E, Lefebvre V, Valk PJ, Delwel R, et al. Sox4 is a key oncogenic target in C/EBPα mutant acute myeloid leukemia. Cancer Cell. 2013;24:575-588.
2. Patel JP, Gönen M, Figueroa ME, Fernandez H, Sun Z, Racevskis J, Van Vlierberghe P, Dolgalev I, Thomas S, Aminova O, Huberman K, Cheng J, Viale A, et al. N Engl J Med. 2012;366:1079-1089.
3. Katherine M. Call, Tom Glaser, Caryn Y. Ito, Alan J. Buckler, Jerry Pelletier, Daniel A. Haber, Elise A. Rose, Astrid Kral, Herman Yeger, William H. Lewis, Carol Jones, David E. Housm Isolation and characterization of a zinc finger polypeptide gene at the human chromosome 11 Wilms’ tumor locus. Cell. 1990;60:509-520.
4. Kang HJ, Park JH, Chen W, Kang SI, Moroz K, Ladanyi M, Lee SB. EWS-WT1 oncoprotein activates neuronal reprogramming factor ASCL1 and promotes neural differentiation. Cancer Res. 2014;74:4526-4535.
5. Koido S, Homma S, Okamoto M, Takakura K, Mori M, Yoshizaki S, Tsukinaga S, Odahara S, Koyama S, Imazu H, Uchiyama K, Kajihara M, Arakawa H, et al. Treatment with chemotherapy and dendritic cells pulsed with multiple Wilms’ tumor 1 (WT1)-specific MHC class I/II-restricted epitopes for pancreatic cancer. Clin Cancer Res. 2014;20:4228-4239.
6. Zhang R, Yang JY, Sun HQ, Jia H, Liao J, Shi YJ, Li G. Comparison of minimal residual disease (MRD) monitoring by WT1 quantification between childhood acute myeloid leukemia and acute lymphoblastic leukemia. Eur Rev Med Pharmacol Sci. 2015;19:2679-2688.
7. Damm F, Heuser M, Morgan M, Yun H, Grosshennig A, Göhring G, Schlegelberger B, Döhner K, Ottmann O, Lübbert M, Heit W, Kanz L, Schlimok G, et al. Single nucleotide polymorphism in the mutational hotspot of WT1 predicts a favorable outcome in patients with cytogenetically normal acute myeloid leukemia. J Clin Oncol. 2010;28:578-585.
8. Hollink IH, van den Heuvel-Eibrink MM, Zimmermann M, Balgobind BV, Arentsen-Peters ST, Alders M, Willasch A, Kaspers GJ, Trka J, Baruchel A, Creutzig U, Pieters R, Reinhardt D, et al. No prognostic impact of the WT1 gene single nucleotide polymorphism rs16754 in pediatric acute myeloid leukemia. J Clin Oncol. 2010;28:e523-526.
9. Wagner K, Damm F, Göhring G, Görlich K, Heuser M, Schäfer I, Ottmann O, Lübbert M, Heit W, Kanz L, Schlimok G, Raghavachar AA, Fiedler W, et al. Impact of IDH1 R132 mutations and an IDH1 single nucleotide polymorphism in cytogenetically normal acute myeloid leukemia: SNP rs11554137 is an adverse prognostic factor. J Clin Oncol. 2010;28:2356-2364.
10. Becker H, Maharry K, Radmacher MD, Mrózek K, Metzeler KH, Whitman SP, Schwind S, Kohlschmidt J, Wu YZ, Powell BL, Carter TH, Kolitz JE, Wetzler M, et al. Clinical outcome and gene- and microRNA-expression profiling according to the Wilms tumor 1 (WT1) single nucleotide polymorphism rs16754 in adult de novo cytogenetically normal acute myeloid leukemia: a Cancer and Leukemia Group B study. Haematologica. 2011;96:1488-1495.
11. Ho PA, Kuhn J, Gerbing RB, Pollard JA, Zeng R, Miller KL, Heerema NA, Raimondi SC, Hirsch BA, Franklin JL, Lange B, Gamis AS, Alonzo TA, et al. WT1 synonymous single nucleotide polymorphism rs16754 correlates with higher mRNA expression and predicts significantly improved outcome in favorable-risk pediatric acute myeloid leukemia: a report from the children’s oncology group. J Clin Oncol. 2011;29:704-711.
12. Renneville A, Boissel N, Helevaut N, Nibourel O, Terré C, Pautas C, Gardin C, Thomas X, Turlure P, Reman O, Berthon C, Dombret H, Castaigne S, et al. Wilms’ tumor 1 single-nucleotide polymorphism rs16754 does not predict clinical outcome in adult acute myeloid leukemia. Leukemia. 2011;25:1918-1921.
13. Damm F, Wagner K, Görlich K, Morgan M, Thol F, Yun H, Delwel R, Valk PJ, Löwenberg B, Heuser M, Ganser A, Krauter J. ID1 expression associates with other molecular markers and is not an independent prognostic factor in cytogenetically normal acute myeloid leukaemia. Br J Haematol. 2012;158:208-215.
14. Choi Y, Lee JH, Hur EH, Kang MJ, Kim SD, Lee JH, Kim DY, Lim SN, Bae KS, Lim HS, Seol M, Kang YA, Lee KH. Single nucleotide polymorphism of Wilms’ tumor 1 gene rs16754 in Korean patients with cytogenetically normal acute myeloid leukemia. Ann Hematol. 2012;91:671-677.
15. Luna I, Such E, Cervera J, Barragán E, Jiménez-Velasco A, Dolz S, Ibáñez M, Gómez-Seguí I, López-Pavía M, Llop M, Fuster Ó, Oltra S, Moscardó F, et al. Analysis of SNP rs16754 of WT1 gene in a series of de novo acute myeloid leukemia patients. Ann Hematol. 2012;91:1845-1853.
16. Luo S, Yu K, Yan QX, Shen ZJ, Wu JB, Chen HM, Gao SM. Analysis of WT1 mutations, expression levels and single nucleotide polymorphism rs16754 in de novo non-M3 acute myeloid leukemia. Leuk Lymphoma. 2014;55:349-357.
17. Niavarani A, Horswell S, Sadri R, Bonnet D. The Wilms Tumor-1 (WT1) rs2234593 variant is a prognostic factor in normal karyotype acute myeloid leukemia. Ann Hematol. 2015. [Epub ahead of print].
18. Zhang DY, Yan H, Cao S, Zhang W, Li XL, Zeng H, Chen XP. Wilms Tumor 1 rs16754 predicts favorable clinical outcomes for acute myeloid leukemia patients in South Chinese population. Leuk Res. 2015;39:568-574.
19. Maurer U, Brieger J, Weidmann E, Mitrou PS, Hoelzer D, Bergmann L. The Wilms’ tumor gene is expressed in a subset of CD34+ progenitors and downregulated early in the course of differentiation in vitro. Exp Hematol. 1997;25:945-950.
20. Cilloni D, Renneville A, Hermitte F, Hills RK, Daly S, Jovanovic JV, Gottardi E, Fava M, Schnittger S, Weiss T, Izzo B, Nomdedeu J, van der Heijden A, et al. Real-time quantitative polymerase chain reaction detection of minimal residual disease by standardized WT1 assay to enhance risk stratification in acute myeloid leukemia: a European LeukemiaNet study. J Clin Oncol. 2009;27:5195-5201.
21. Ujj Z, Buglyó G, Udvardy M, Beyer D, Vargha G, Biró S, Rejtó L. WT1 Expression in Adult Acute Myeloid Leukemia: Assessing its Presence, Magnitude and Temporal Changes as Prognostic Factors. Pathol Oncol Res. 2015. [Epub ahead of print].
22. Casalegno-Garduño R, Schmitt A, Spitschak A, Greiner J, Wang L, Hilgendorf I, Hirt C, Ho AD, Freund M, Schmitt M. Immune responses to WT1 in patients with AML or MDS after chemotherapy and allogeneic stem cell transplantation. Int J Cancer. 2015. doi: 10.1002/ijc.29909.
23. Zhong L, Wei L, Chen J, Huang X, Gong Y, Lu Y. WT1 Expression in Circulating RNA as a Minimal Residual Disease Marker for AML Patients After Stem-Cell Transplantation. Mol Diagn Ther. 2015;19:205-212.