
INTRODUCTION
Lung cancer is the leading cause of cancer-related death and its incidence is increasing in women [1]. Gender has been shown to play a prognostic role in lung cancer. Compared to men, the proportions of adenocarcinoma histology and early-stage disease are greater in women with lung cancers [2, 3]. Women have a higher response rate to chemotherapy and a better survival rate than men, especially in adenocarcinomas [3, 4]. In addition, mutations in epidermal growth factor receptor (EGFR), which can predict sensitivity to EGFR tyrosine kinase inhibitor, are more frequently identified in women than in men [5, 6]. This suggests that lung cancer carcinogenesis should be considered, at least partly, as a distinct entity by gender.
The tumor biology of sex steroid hormone receptors, such as the estrogen receptor (ER) and the progesterone receptor (PR), has been studied, especially in breast cancers [7–12]. In human ERs, there are two isoforms (ERα and ERβ) with partial homology, yet distinct function, in normal and neoplastic cells [13]. In breast cancer patients, nuclear expression of ERα and PR has been an important and favorable prognostic biomarker with a greater response to endocrine therapy (such as tamoxifen) [7–9]. Currently, immunohistochemical assessment of ERα and PR has been part of routine clinical practice for treating breast cancers. In addition to ERα, since the discovery of a second ER—which has been identified as ERβ—its functional and prognostic importance has been also investigated in breast cancers [10–12]. Recently, in lung cancers the positive association between ER expression and EGFR mutations has been detected [14, 15], and the potential clinical impact of ERα, ERβ, and PR has also been investigated [14–23]. Despite these investigations, their prognostic value remains controversial.
The tumor immune microenvironment has a prognostic impact on solid malignancies [24–26]. Using a large cohort of stage I lung adenocarcinoma patients, we have identified forkhead box P3 (FoxP3)+/CD3+ lymphocytes infiltration index—which represents the ratio of regulatory T cells to total T cells—in tumor-related stroma, overexpression of tumoral interleukin-7 receptor (IL-7R), and loss of tumoral IL-12Rβ2 as independent prognostic factors [27]. In breast carcinomas, associations between the tumor immune microenvironment and ER status have been investigated; the number of tumor-infiltrating lymphocytes (including FoxP3+, CD8+ or CD20+ cells) is greater in ERα-negative tumors than in ERα-positive tumors [28–31] and lymphocyte infiltration contributes to better clinical outcomes in ERα-negative tumors than in ERα-positive tumors [32].
In 2011, the International Association for the Study of Lung Cancer (IASLC), the American Thoracic Society (ATS), and the European Respiratory Society (ERS) published the new lung adenocarcinoma histologic classification system [33]. Its prognostic value—which is based on predominant histologic patterns—has been confirmed in large independent cohorts worldwide [34–36]. Additionally, our group has reported molecular and radiologic correlations with histologic subtypes [37–40]. However, associations between histologic subtypes and sex steroid hormone receptors in lung adenocarcinoma have yet to be investigated.
In our study, we investigate whether ERα and PR expression predicts risk of disease recurrence and if it has any associations with clinicopathologic factors, histologic patterns, mutation status, or immune factors in stage I lung adenocarcinoma patients.
RESULTS
Patient demographics
Patient demographics are shown in Table 1. Of all (n = 913), median patient age was 69 years (range, 23–96 years). More than half of the patients were women (n = 564) and had stage IA disease (n = 636). Median tumor size was 2.0 cm (range, 0.3–5.0). During the study period, 14% (n = 130) of patients experienced recurrence and 17% (n = 136) died from any cause without documented recurrence. Median follow-up period for patients who did not experience recurrence was 38.5 months (range, 2.6–160.1 months).
Table 1: Patients demographics and its associations with nuclear ERα in all patients
Variables |
N |
Nuclear ERα, N (%) |
P |
|||
Negative |
Positive |
|||||
Age, years |
0.63 |
|||||
Median |
69* |
69* |
69* |
|||
Range |
23–96** |
23–96** |
43–87** |
|||
Sex |
0.038 |
|||||
Female |
564 |
455 |
(81) |
109 |
(19) |
|
Male |
349 |
301 |
(86) |
48 |
(14) |
|
Smoking status |
0.56 |
|||||
Never |
151 |
128 |
(85) |
23 |
(15) |
|
Former/current |
762 |
628 |
(82) |
134 |
(18) |
|
Surgery |
0.019 |
|||||
Lobectomy |
718 |
606 |
(84) |
112 |
(16) |
|
Limited resection |
195 |
150 |
(77) |
45 |
(23) |
|
Tumor size (cm) |
0.006 |
|||||
Median |
2.0* |
2.0* |
1.8* |
|||
Range |
0.3–5.0** |
0.3–5.0** |
0.5–5.0** |
|||
Pathological stage |
0.98 |
|||||
IA |
636 |
526 |
(83) |
110 |
(17) |
|
IB |
277 |
230 |
(83) |
47 |
(17) |
|
Architectural grade |
0.37 |
|||||
Low |
111 |
93 |
(84) |
18 |
(16) |
|
Intermediate |
579 |
472 |
(82) |
107 |
(18) |
|
High |
223 |
191 |
(86) |
32 |
(14) |
|
Pleural invasion |
0.26 |
|||||
Absence |
758 |
633 |
(84) |
125 |
(16) |
|
Presence |
155 |
123 |
(79) |
32 |
(21) |
|
Lymphatic invasion |
0.39 |
|||||
Absence |
622 |
510 |
(82) |
112 |
(18) |
|
Presence |
291 |
246 |
(85) |
45 |
(15) |
|
Vascular invasion |
0.45 |
|||||
Absence |
679 |
558 |
(82) |
121 |
(18) |
|
Presence |
234 |
198 |
(85) |
36 |
(15) |
|
Necrosis |
0.75 |
|||||
Absence |
761 |
632 |
(83) |
129 |
(17) |
|
Presence |
152 |
124 |
(82) |
28 |
(18) |
|
Nuclear atypia |
0.47 |
|||||
Mild |
392 |
331 |
(84) |
61 |
(16) |
|
Moderate |
315 |
255 |
(81) |
60 |
(19) |
|
Severe |
206 |
170 |
(83) |
36 |
(17) |
|
Mitotic count |
0.98 |
|||||
Low |
442 |
367 |
(83) |
75 |
(17) |
|
Intermediate |
196 |
162 |
(83) |
34 |
(17) |
|
High |
275 |
227 |
(83) |
48 |
(17) |
|
Significant P-values (<0.05) are shown in bold.
ER, estrogen receptor
*Median
**Range
ER and PR expression profiles
ERα and PR expression profiles are summarized in Table 2. Of all, nuclear ERα expression was observed in 157 (17%) patients, most of whom were focally positive (n = 138; 88%). Among nuclear ERα-positive tumors, 118 (75%) were weakly positive, 27 (17%) were moderately positive, and 12 (8%) were strongly positive (Fig. 1A). Cytoplasmic ERα expression was observed in 86 (9%) patients, most of whom were weakly (n = 80; 93%) (Fig. 1B) and focally positive (n = 74; 86%). Nuclear PR expression was observed in 119 (13%) patients, most of whom were focally positive (n = 108; 91%). Among nuclear PR-positive tumors, 93 (78%) were weakly positive, 20 (17%) were moderately positive (Fig. 1C), and 6 (5%) were strongly positive. Cytoplasmic PR expression was observed in 116 (13%) patients, more than half of whom were focally positive (n = 80; 69%). Among cytoplasmic PR-positive tumors, 87 (75%) were weakly positive, 21 (18%) were moderately positive, and 8 (7%) were strongly positive (Fig. 1D).
Table 2: ERα and PR expression profiles in all patients
Intensity |
Distribution |
||||||||||||
Marker |
Positive |
Weak |
Moderate |
Strong |
Focal |
Diffuse |
|||||||
N |
(%) |
N |
(%) |
N |
(%) |
N |
(%) |
N |
(%) |
N |
(%) |
||
ERα (n = 913) |
|||||||||||||
Nucleus |
157 |
(17) |
118 |
(75) |
27 |
(17) |
12 |
(8) |
138 |
(88) |
19 |
(12) |
|
Cytoplasm |
86 |
(9) |
80 |
(93) |
6 |
(7) |
0 |
(0) |
74 |
(86) |
12 |
(14) |
|
PR (n = 910) |
|||||||||||||
Nucleus |
119 |
(13) |
93 |
(78) |
20 |
(17) |
6 |
(5) |
108 |
(91) |
11 |
(9) |
|
Cytoplasm |
116 |
(13) |
87 |
(75) |
21 |
(18) |
8 |
(7) |
80 |
(69) |
36 |
(31) |
|
ER, estrogen receptor; PR, progesterone receptor
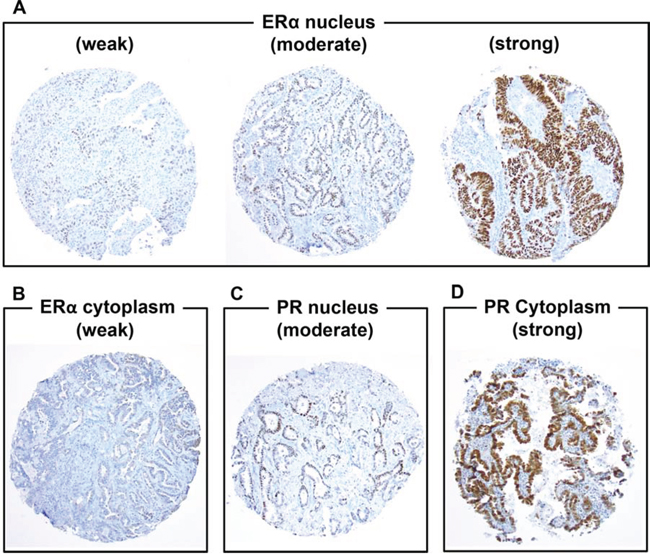
Figure 1: Immunohistochemical analyses of estrogen receptor-α (ERα) and progesterone receptor (PR) using tissue microarrays (original magnification, A–F: × 100 magnification) A. ERα is weakly, moderately, or strongly positive in tumor nuclei. B. ERα is weakly positive in tumor cytoplasm. C. PR is moderately positive in tumor nuclei. D. PR is strongly positive in tumor cytoplasm.
ERα and PR expression associations with disease recurrence and overall survival
In all patients, nuclear ERα expression was not associated with risk of recurrence (P = 0.38) (Fig. 2A). In pT1a patients, 5-year CIR of patients with nuclear ERα-positive tumors was significantly higher (n = 81; 5-year CIR, 20%) than nuclear ERα-negative tumors (n= 336; 5-year CIR, 8%; P = 0.018) (Fig. 2B). Among pT1a patients, 5-year CIR of patients with nuclear ERα-positive tumors was significantly higher (n = 24; 5-year CIR, 47%) than nuclear ERα-negative tumors in males (n = 131; 5-year CIR, 11%; P = 0.003) (Fig. 2C) while the difference was not observed in females (P = 0.55) (Fig. 2D). After excluding the wedge resection group, among T1a patients who had undergone sublobar resection or lobectomy, 5-year CIR of patients with nuclear ERα-positive tumors was still higher (n = 60; 5-year CIR, 13%) than nuclear ERα-negative tumors (n = 279; 5-year CIR, 6%); the difference was not statistically significant (P = 0.19). Among T1a patients who had undergone lobectomy only, 5-year CIR of patients with nuclear ERα-positive tumors was slightly higher (n = 53; 5-year CIR, 10%) than nuclear ERα-negative tumors (n = 249; 5-year CIR, 5%); the difference was also not statistically significant (P = 0.58). Cytoplasmic ERα, nuclear PR, and cytoplasmic PR were not associated with risk of recurrence (Table 3).
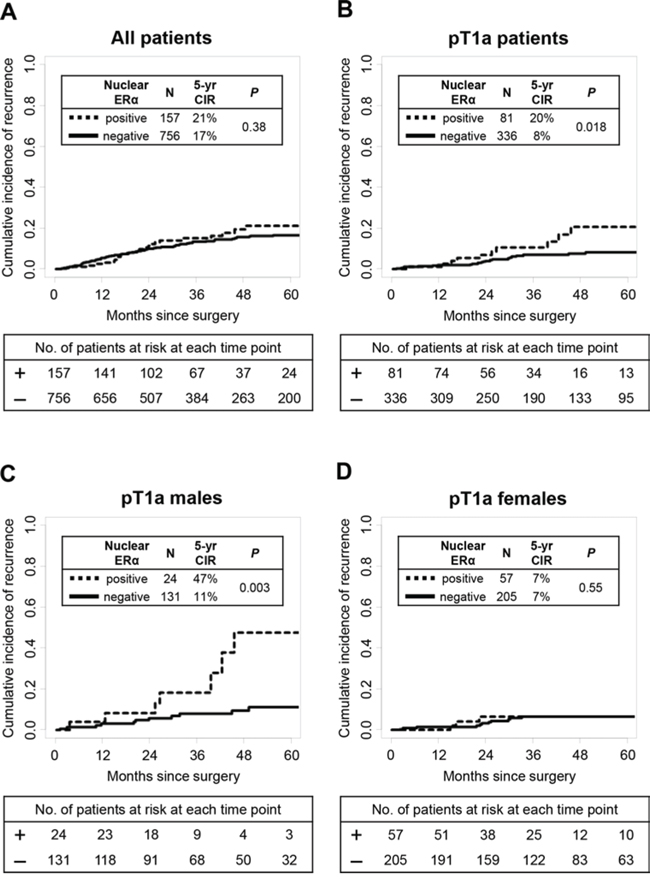
Figure 2: Estrogen receptor-α (ERα) associations with disease recurrence. A. In all patients, nuclear ERα expression was not associated with risk of recurrence (P = 0.38) B. In pT1a patients, 5-year CIR of patients with nuclear ERα-positive tumors was significantly higher (n = 81; 5-year CIR, 20%) than patients with nuclear ERα-negative tumors (n = 336; 5-year CIR, 8%; P = 0.018). C. In pT1a males, 5-year CIR of patients with nuclear ERα-positive tumors was significantly higher (n = 24; 5-year CIR, 47%) than patients with nuclear ERα-negative tumors (n = 131; 5-year CIR, 11%; P = 0.003). D. In pT1a females, nuclear ERα expression was not associated with risk of recurrence (P = 0.55).
Table 3: ERα and PR association with disease recurrence
Variables |
All patients |
Patients with pT1a disease |
||||||
N |
(%) |
5-yr CIR |
P |
N |
(%) |
5-yr CIR |
P |
|
ERα nucleus |
0.38 |
0.018 |
||||||
Negative |
756 |
(83) |
17% |
336 |
(81) |
8% |
||
Positive |
157 |
(17) |
21% |
81 |
(19) |
20% |
||
ERα cytoplasm |
0.37 |
0.14 |
||||||
Negative |
827 |
(91) |
18% |
380 |
(91) |
11% |
||
Positive |
86 |
(9) |
14% |
37 |
(9) |
5% |
||
PR nucleus |
0.18 |
0.96 |
||||||
Negative |
791 |
(87) |
17% |
347 |
(83) |
10% |
||
Positive |
119 |
(13) |
23% |
69 |
(17) |
12% |
||
PR cytoplasm |
0.42 |
0.65 |
||||||
Negative |
794 |
(87) |
18% |
348 |
(84) |
10% |
||
Positive |
116 |
(13) |
16% |
68 |
(16) |
10% |
||
Significant P-values (<0.05) are shown in bold.
ER, estrogen receptor; PR, progesterone receptor; CIR, cumulative incidence of recurrence
Although overall survival (OS) analysis was also performed, ERα and PR expression (in nuclear or cytoplasm) were not associated with OS in all and T1a patients. In pT1a patients, limited resection (vs. lobectomy; P < 0.001), high architectural grade (P < 0.001), lymphatic invasion (P = 0.001), vascular invasion (P = 0.004), tumor necrosis (P = 0.043), greater nuclear atypia (P = 0.027), and higher mitotic count (P = 0.001) were significantly associated with high risk of recurrence.
On multivariate analysis of patients with pT1a disease, nuclear ERα expression remained a significant prognostic factor of increased risk of recurrence (hazard ratio [HR] = 2.27; P = 0.03) (Table 4A). When analyzing the effect of nuclear ERα expression on recurrence in males and females separately, nuclear ERα expression was significantly associated with a higher risk of recurrence in males (HR = 3.66; P = 0.009), but not in females (HR = 1.31; P = 0.63) (Table 4B).
Table 4: Multivariate analysis for disease recurrence in patients with T1a disease
(A) In patients with pT1a disease |
||||
Variables |
Hazard Ratio |
95% CI |
P |
|
Nuclear ERα |
positive vs. negative |
2.27 |
1.08–4.77 |
0.03 |
Sex |
males vs. females |
2.19 |
1.06–4.53 |
0.035 |
Surgery |
lobectomy vs. limited resection |
3.55 |
1.69–7.49 |
<0.001 |
Architectural grade |
high vs. intermediate |
2.88 |
1.26–6.58 |
0.012 |
high vs. low |
11.67 |
1.60–84.75 |
0.015 |
|
Lymphatic Invasion |
present vs. absent |
1.18 |
0.56–2.51 |
0.67 |
Mitotic count |
intermediate vs. low |
0.67 |
0.23–1.95 |
0.46 |
high vs. low |
1.31 |
0.54–3.17 |
0.55 |
|
(B) Effect of nuclear ER in males and females with pT1a disease |
||||
Variables |
Hazard Ratio |
95% CI |
P |
|
Nuclear ERα in females |
positive vs. negative |
1.31 |
0.43–4.01 |
0.63 |
Nuclear ERα in males |
positive vs. negative |
3.66 |
1.37–9.74 |
0.009 |
Surgery |
lobectomy vs. limited resection |
3.49 |
1.65–7.36 |
0.001 |
Architectural grade |
high vs. intermediate |
2.99 |
1.25–7.15 |
0.014 |
high vs. low |
12.55 |
1.80–86.96 |
0.011 |
|
Lymphatic Invasion |
present vs. absent |
1.12 |
0.53–2.4 |
0.77 |
Mitotic count |
intermediate vs. low |
0.69 |
0.23–2.02 |
0.49 |
high vs. low |
1.33 |
0.53–3.33 |
0.54 |
|
Significant P-values (<0.05) are shown in bold.
ER, estrogen receptor; CI, confidence interval
Nuclear ER associations with patient clinicopathologic factors
In all patients, nuclear ERα-positive tumors were more frequently identified in females than in males (19% vs. 14%; P = 0.038) and they were smaller in size than nuclear ERα-negative tumors (median size, 1.8 cm vs. 2.0 cm; P = 0.019) (Table 1). However, these differences were not significant in pT1a tumors (P = 0.15 and P = 0.59, respectively). In all patients, nuclear ERα-positive tumors were slightly more frequently identified in the limited resection group than in the lobectomy group (23% vs. 16%; P = 0.019); however, this difference was not statistically significant in pT1a tumors (P = 0.15). The other aforementioned factors were not associated with nuclear ERα expression.
According to histologic subtype, nuclear ERα-positive tumors were most frequently observed in micropapillary subtype (22%) although there was no significant difference in the rate of nuclear ERα-positive tumors among non-mucinous invasive tumors (18% in lepidic subtype, 19% in acinar subtype, 18% in papillary subtype, and 16% in solid subtype) (Fig. 3). Nuclear ERα-positive tumors were not identified in mucinous subtypes (invasive mucinous or colloid subtype). Nuclear ERα-positive tumors were less frequently identified in minimally invasive subtype (11%). Among minimally invasive tumors, two mucinous cases were negative for nuclear ERα.
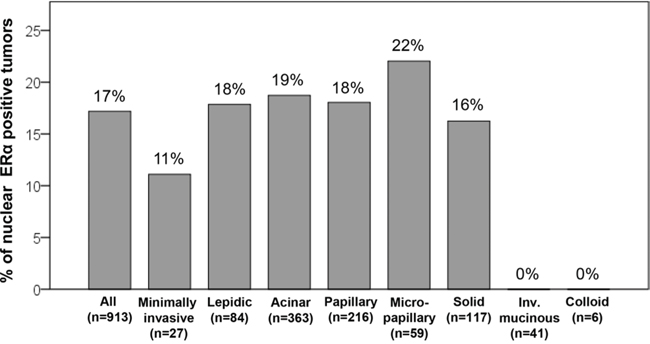
Figure 3: Percentage of nuclear estrogen receptor-α (ERα)-positive tumors according to histologic subtypes. Nuclear ERα-positive tumors were most frequently observed in micropapillary subtype (22%), although there was no significant difference in percentages of nuclear ERα-positive tumors among non-mucinous invasive tumors (18% in lepidic subtype, 19% in acinar subtype, 18% in papillary subtype, and 16% in solid subtype). Nuclear ERα-positive tumors were not identified in mucinous subtypes (invasive mucinous or colloid subtype). Nuclear ERα-positive tumors were less frequently identified in minimally invasive subtype (11%).
Associations between nuclear ERα and mutation status were also analyzed and the results showed that nuclear ERα expression was not associated with EGFR or KRAS mutations (P = 0.99 and P = 0.6, respectively).
Nuclear ER associations with prognostic immune markers
In all patients, nuclear ERα expression was positively associated with high tumoral and stromal CD3+ lymphocyte infiltration (P = 0.012 and P = 0.043, respectively), high tumoral and stromal FoxP3+ lymphocyte infiltration (P < 0.001 and P = 0.027, respectively), and high tumoral and stromal FoxP3/CD3 risk index (P < 0.001 and P = 0.006, respectively) (Table 5). In patients with pT1a disease, nuclear ERα expression was positively associated with high stromal CD3+ lymphocyte infiltration (P < 0.001), high tumoral and stromal FoxP3+ lymphocyte infiltration (P < 0.001 and P = 0.028, respectively), high tumoral FoxP3/CD3 risk index (P < 0.001), and high tumoral IL-7R expression (P = 0.022) (Table 5). In male patients with pT1a disease, nuclear ERα expression was positively associated with high tumoral CD3+ lymphocyte infiltration (P < 0.001), and high tumoral FoxP3/CD3 risk index (P = 0.001). However, these immune markers were not associated with smoking status or patient gender (data not shown).
Table 5: Associations between nuclear ERα and immune markers
Variable |
(A) All patients |
(B) Patients with pT1a disease |
||||||||
Nuclear ERα, N (%) |
P |
Nuclear ERα, N (%) |
P |
|||||||
Negative |
Positive |
Negative |
Positive |
|||||||
Tumoral CD3 |
0.012 |
0.07 |
||||||||
Low |
425 |
(86) |
72 |
(14) |
179 |
(84) |
34 |
(16) |
||
High |
314 |
(79) |
84 |
(21) |
149 |
(76) |
46 |
(24) |
||
Stromal CD3 |
0.043 |
<0.001 |
||||||||
Low |
501 |
(85) |
89 |
(15) |
235 |
(86) |
39 |
(14) |
||
High |
224 |
(79) |
59 |
(21) |
87 |
(70) |
37 |
(30) |
||
Tumoral FoxP3 |
<0.001 |
<0.001 |
||||||||
Low |
391 |
(91) |
38 |
(9) |
168 |
(92) |
15 |
(8) |
||
High |
341 |
(75) |
116 |
(25) |
155 |
(71) |
63 |
(29) |
||
Stromal FoxP3 |
0.027 |
0.028 |
||||||||
Low |
471 |
(85) |
85 |
(15) |
223 |
(84) |
44 |
(16) |
||
High |
241 |
(79) |
66 |
(21) |
98 |
(74) |
35 |
(26) |
||
Tumoral FoxP3/CD3 index |
<0.001 |
<0.001 |
||||||||
Low |
457 |
(89) |
56 |
(11) |
196 |
(88) |
26 |
(12) |
||
High |
273 |
(74) |
98 |
(26) |
127 |
(71) |
52 |
(29) |
||
Stromal FoxP3/CD3 index |
0.006 |
0.07 |
||||||||
Low |
526 |
(85) |
92 |
(15) |
236 |
(83) |
48 |
(17) |
||
High |
175 |
(77) |
53 |
(23) |
78 |
(74) |
27 |
(26) |
||
IL-7 R |
0.41 |
0.022 |
||||||||
Low |
440 |
(84) |
85 |
(16) |
228 |
(84) |
44 |
(16) |
||
High |
299 |
(81) |
68 |
(19) |
98 |
(74) |
35 |
(26) |
||
IL-12Rβ2 |
0.96 |
0.96 |
||||||||
Low |
557 |
(83) |
117 |
(17) |
238 |
(80) |
60 |
(20) |
||
High |
180 |
(82) |
39 |
(18) |
88 |
(81) |
21 |
(19) |
||
Significant P-values (<0.05) are shown in bold.
ER, estrogen receptor; FoxP3, forkhead box P3; IL-7R, interleukin-7 receptor; IL-12Rβ2, interleukin-12 receptor β2
DISCUSSION
We have demonstrated that nuclear ERα expression is an independent predictor of increased risk of recurrence in patients with pT1aN0 (≤2.0 cm) lung adenocarcinoma, especially in male patients, and positively correlates with poor prognostic immune microenvironments (CD3+ and FoxP3+ lymphocyte infiltration, and tumoral IL-7R expression).
In lung cancers, ER expression was reported to correlate with female sex, less smoking history, smaller tumor size, adenocarcinoma histology, and EGFR mutation [14, 15, 20–23]. Our results from stage I lung adenocarcinoma show that ERα expression was more frequently observed in females than males (19% vs. 14%) and correlates with smaller tumor size (1.8 cm vs. 2.0 cm); however, it was not associated with smoking history or EGFR mutation.
Previous studies have investigated the clinical impact of ER expression in lung cancer patients [14–23]; however, its prognostic significance remains controversial. Most studies have demonstrated that nuclear ERβ expression is associated with better prognosis in lung cancers [15–18], especially in male patients [16, 17]. However, other groups also have reported the unfavorable prognostic value of nuclear and cytoplasmic ERβ expression in lung cancers [20, 22]. With regard to ERα expression in lung cancers, Raso et al. and Kawai et al. reported that cytoplasmic ERα expression was associated with worse prognosis [18, 20], while Rouquette et al. found that it had favorable prognostic value [21]. Moreover, other studies did not identify any prognostic significance of nuclear or cytoplasmic ERα expression in lung cancers [14–16, 19, 22]. By contrast, the prognostic significance of ERα in resected early-stage lung adenocarcinoma remained unknown since previous study cohorts were either composed of only a small number of patients or were a heterogeneous population with regards to pathologic TNM stage (including early-stage and advanced-stage) and histology (including adenocarcinoma and squamous cell carcinoma). In our study using a large, uniform cohort (n > 900) comprised of patients with stage I lung adenocarcinoma, we have demonstrated that ERα expression is an independent risk factor of disease recurrence, especially in male patients with pT1a status (HR = 3.66).
Considering the inconsistent results of previous studies—specifically clinical correlations and the prognostic value of ER expression in lung cancers—its function may vary due to variations in patient gender (male vs. female), location of ER expression (nucleus vs. cytoplasm), ER isoforms (ERα vs. ERβ), and epitopes that each anti-ER monoclonal antibody can recognize. The two anti-ERα mouse monoclonal antibodies (ID5 and 6F11) have shown similar immunoreactivity in breast carcinomas [41] and were most frequently used in previous studies on lung carcinomas [14, 16, 19–21]. As an epitope, monoclonal antibody ID5 recognizes N-terminal of ERα while 6F11 recognizes full length of ERα [20]. More recently, anti-ERα rabid monoclonal antibody SP1—which recognizes C-terminal of ERα—has been introduced and is reported to have higher sensitivity and an 8-fold higher affinity in breast carcinomas for the detection of ERα, compared with ID5 [42]. Furthermore, in breast carcinomas, SP1 was recognized as a more reliable prognostic factor and a superior predictor of response to endocrine therapy compared with ID5 [9]. In lung adenocarcinoma, the superiority of SP1 to ID5 in the detection of tumoral ERα was also demonstrated; detection rate of ERα was significantly higher in SP1 (27%) when compared with ID5 (8%) and 6F11 (14%) [43]. In our study, we first described the unfavorable prognostic value of nuclear ERα in early-stage lung adenocarcinoma using monoclonal antibody SP1, which has high sensitivity and affinity. Use of different monoclonal antibodies in the studies may be the reason why nuclear ERα expression was not associated with smoking history or EGFR mutations in our study.
The IASLC/ATS/ERS lung adenocarcinoma classification system has powerful prognostic value [34–36] and shows molecular correlations (such as thyroid transcription factor-1, Ki-67, EGFR/KRAS mutations) [37–40]. In our study, no significant difference of ERα expression rate was observed among tumors with non-mucinous invasive subtypes. However, we found it interesting that no mucinous tumors (including mucinous minimally invasive, invasive mucinous, and colloid subtypes) showed nuclear ERα expression. Invasive mucinous adenocarcinoma (mucinous bronchioloalveolar carcinoma) has been known to correlate with KRAS mutation and harbor no EGFR mutation [44, 45]. Additionally, the recently discovered fusion gene CD74-NRG1 presented specifically in invasive mucinous lung adenocarcinoma [46, 47]. Taking this into account, invasive mucinous adenocarcinoma can be considered a distinct entity or subtype from non-mucinous adenocarcinoma of the lung, according to its molecular profile.
Estradiol-which is the most biologically active type of estrogen-was proven to stimulate lung cancer cell growth, both in vitro and in mouse models [48]. In lung cancer patients, high serum estrogen levels are an unfavorable prognostic marker [49] and hormone replacement therapy may correlate with decreases survival in women [50, 51]. Tamoxifen is an antagonist of ER and causes decreases in invasion capacity and proliferation of ER-positive human lung adenocarcinoma cell lines [52, 53]. Interestingly, highly concordant co-expression of estrogen receptors and aromatase-which is an enzyme that can catalyze androgen aromatization into estrogen-has been identified in lung cancers [54]. Additionally, Niikawa et al. reported that estradiol was locally produced, mainly by aromatase, in lung cancer cells and it played an important role in the growth of ER-positive tumors in in vitro studies, thereby suggesting that anti-estrogen therapies (such as selective ER modulators and aromatase inhibitors) may be clinically effective in patients with ER-positive lung cancers [55]. More importantly, their study also demonstrated that estradiol concentration in lung cancer tissue was significantly higher in men than in postmenopausal women [55]. This finding may explain why ERα expression in lung adenocarcinoma has had a significant prognostic impact on males but not for females in our study.
Recently, an effect of estrogen levels on regulatory T cells was investigated and it was suggested that high levels of estrogen might induce increases of regulatory T cells in peripheral blood [56, 57]. Previously, we reported high FoxP3+/CD3+ lymphocyte ratio as an independent risk factor of recurrence in stage I lung adenocarcinoma [27]. In our current study, we demonstrated that FoxP3+ regulatory T lymphocyte infiltration was positively associated with ERα expression in lung adenocarcinoma. By contrast, in breast carcinomas the degree of tumor infiltrating FoxP3+ regulatory T lymphocytes was higher in ERα-negative tumors than in ERα-positive tumors [30, 31]. This discrepancy may be due to multiple factors including variations in primary tumor location (lung vs. breast), predominant gender and exposure of the tumor microenvironment to other immunogenic proteins.
In conclusion, our study demonstrates that nuclear ERα expression is an independent predictor of increased risk of recurrence in small (pT1aN0) stage I lung adenocarcinoma, especially in males, and correlates with unfavorable prognostic immune microenvironments (FoxP3+ regulatory T lymphocyte infiltration and tumoral IL-7R overexpression). In stage I lung adenocarcinoma, nuclear ERα expression is observed in 17% of cases using monoclonal antibody SP1, which may become a potential target for anti-estrogen therapy.
MATERIALS AND METHODS
Patients
The Institutional Review Board at Memorial Sloan Kettering Cancer Center (MSK) approved our retrospective study (WA0269-08). We reviewed patients with pathologic stage I, solitary lung adenocarcinomas who had undergone surgical resection at MSK between 1995 and 2009. Tumor slides and blocks from 944 patients were available for slide review and tissue microarray construction. Of the 913 patients with high quality tissue cores, 718 had undergone lobectomy and 195 had undergone limited resection (segmentectomy [n = 65] and wedge resection [n = 130]). In our cohort of patients with T1a disease, 85% of patient had undergone lymph node dissection or sampling in addition to lung resection. Lymph nodes were not examined in this study.
Clinical data were collected from our prospectively maintained database. As of March 2013, patient medical records and the database of last follow-up were reviewed and update. Disease stage was assigned using the seventh edition of the American Joint Committee on Cancer TNM Staging Manual [58]. Of all, 497 patients had EGFR and KRAS mutation analyses results in our dataset. Subsets of the cases in this study have been used in our previous publications [27, 37–39].
Histologic evaluation
All available tumor slides were reviewed by two pathologists (K.K. and W.D.T.), both of whom were blinded to patient clinical outcomes, using an Olympus BX51 microscope (Olympus, Tokyo, Japan) with a standard 22-mm diameter eyepiece. Tumors demonstrating squamous morphology, such as keratinization or intracellular bridges, were excluded from this study. When the tumors exhibited a purely solid pattern without differentiated adenocarcinoma morphology (e.g., lepidic, acinar, or papillary patterns), those cases were proven to have intracellular mucin with mucin stains at time of original pathologic diagnosis. Tumors were classified according to the IASLC/ATS/ERS classification system [33] and were grouped into 3 architectural grades on the basis of histologic subtype-low (adenocarcinoma in situ, minimally invasive, or lepidic), intermediate (papillary or acinar), and high (micropapillary, solid, invasive mucinous, or colloid) [34, 37, 39].
Mitoses were evaluated in 50 high-power fields (HPFs) at × 400 magnification (0.237 mm2 field) in areas with highest mitotic activity and were counted as average number of mitotic figures per 10 HPFs. Mitotic count was classified as follows: low (0–1 mitotic figures/10 HPFs), intermediate (2–4 mitotic figures/10 HPFs), and high (≥5 mitotic figures/10 HPFs) [39]. Visceral pleural invasion, lymphovascular invasion, and tumor were also investigated.
Immunohistochemical analysis and scoring of ERα and PR expression
We briefly deparaffinized 4 μm-thick sections from previously constructed tissue microarray blocks [27, 38]. Each case had 2–6 tumoral cores and 2–3 stromal cores (0.6 mm in diameter). Using the standard avidin-biotin-complex peroxidase technique, sections were immunostained for anti-ERα antibody (SP1, Ventana; prediluted) and anti-PR antibody (1E2, Ventana; prediluted). Of all, 913 ERα cases and 910 PR cases had adequate tumor cores available for immunohistochemical analyses. In each tumor core, intensity score (0: no expression, 1: weak, 2: moderate, and 3: strong) and distribution (%) of ERα and PR expression were evaluated separately in tumor nuclei and cytoplasm [14, 20, 27]. Average of intensity scores and positive cell distribution within cores were used as the score for each patient. Intensity scores were classified into either negative (score 0), weakly (score 0–1), moderately (score 1–2), or strongly positive (score 2–3). Distribution was classified into focally (0–49%) and diffusely (≥50%) positive. Any level of positivity (score > 0) for ERα and PR was considered positive [14, 20].
Immunohistochemical scores (high or low) of CD3+ lymphocyte infiltration (in tumor and stroma), FoxP3+ lymphocyte infiltration (in tumor and stroma), CD3/FoxP3+ risk index (in tumor and stroma), tumoral IL-7R, and tumoral IL-12Rβ2 were obtained from the dataset used in our previous study [27].
Statistical analysis
Associations between variables were analyzed using Fisher's exact test for categorical variables and the Wilcoxon test for continuous variables. Follow-up duration was calculated from date of surgery to date of first recurrence, death from any cause, or last follow-up. Cumulative incidence of recurrence (CIR) where death from any cause other than recurrence was considered a competing event was used to estimate probability of recurrence [59]. Differences in CIR between groups were assessed using the Gray method for univariate analyses and the Fine-Gray method for multivariate analyses, after adjustment for important potential confounders [60]. Overall survival was estimated using the Kaplan–Meier method, and nonparametric group comparisons were performed using the logrank test. All P-values were determined using two-tailed statistical analyses and P < 0.05 was considered statistically significant. Statistical analyses were conducted using SAS v9.2 (SAS Institute, Cary, NC) and R (R Development Core Team, 2010), including the “survival” and “cmprsk” packages.
ACKNOWLEDGMENTS
We thank Joe Dycoco of the MSK Thoracic Surgery Service for assisting with the MSK Thoracic Surgery Service's lung cancer database; Irina Linkov of the Pathology Core Facility for technical assistance with immunohistochemistry; and Alex Torres of the MSK Thoracic Surgery Service for their editorial assistance.
FUNDING
This work was supported by grants from the National Institutes of Health (R21 CA164568-01A1, R21 CA164585-01A1, R01 CA136705-06, U54 CA137788, P30 CA008748, and P50 CA086438-13), the U.S. Department of Defense (PR101053 and LC110202), and the Mr. William H. Goodwin and Mrs. Alice Goodwin, the Commonwealth Foundation for Cancer Research, and the Experimental Therapeutics Center of Memorial Sloan Kettering Cancer Center.
CONFLICTS OF INTEREST
All authors have no conflicts of interest to disclose.
REFERENCES
1. Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011. CA Cancer J Clin. 2011; 61:212–236.
2. Minami H, Yoshimura M, Miyamoto Y, Matsuoka H, Tsubota N. Lung cancer in women: sex-associated differences in survival of patients undergoing resection for lung cancer. Chest. 2000; 118:1603–1609.
3. Sakurai H, Asamura H, Goya T, Eguchi K, Nakanishi Y, Sawabata N, Okumura M, Miyaoka E, Fujii Y. Survival differences by gender for resected non-small cell lung cancer: a retrospective analysis of 12,509 cases in a Japanese Lung Cancer Registry study. J Thorac Oncol. 2010; 5:1594–1601.
4. Wheatley-Price P, Blackhall F, Lee SM, Ma C, Ashcroft L, Jitlal M, Qian W, Hackshaw A, Rudd R, Booton R, Danson S, Lorigan P, Thatcher N, et al. The influence of sex and histology on outcomes in non-small-cell lung cancer: a pooled analysis of five randomized trials. Ann Oncol 2010; 21:2023–2028.
5. Shigematsu H, Lin L, Takahashi T, Nomura M, Suzuki M, Wistuba, II, Fong KM, Lee H, Toyooka S, Shimizu N, Fujisawa T, Feng Z, Roth JA, et al. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J Natl Cancer Inst. 2005; 97:339–346.
6. Tam IY, Chung LP, Suen WS, Wang E, Wong MC, Ho KK, Lam WK, Chiu SW, Girard L, Minna JD, Gazdar AF, Wong MP. Distinct epidermal growth factor receptor and KRAS mutation patterns in non-small cell lung cancer patients with different tobacco exposure and clinicopathologic features. Clin Cancer Res. 2006; 12:1647–1653.
7. Bardou V-J, Arpino G, Elledge RM, Osborne CK, Clark GM. Progesterone receptor status significantly improves outcome prediction over estrogen receptor status alone for adjuvant endocrine therapy in two large breast cancer databases. J Clin Oncol. 2003; 21:1973–1979.
8. Clarke M CR, Darby S, Davies C, Evans V, Godwin J, Gray R, McGale P, Peto R, Wang Y. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005; 365:1687–1717.
9. Cheang MCU, Treaba DO, Speers CH, Olivotto IA, Bajdik CD, Chia SK, Goldstein LC, Gelmon KA, Huntsman D, Gilks CB, Nielsen TO, Gown AM. Immunohistochemical detection using the new rabbit monoclonal antibody SP1 of estrogen receptor in breast cancer is superior to mouse monoclonal antibody 1D5 in predicting survival. J Clin Oncol. 2006; 24:5637–5644.
10. Esslimani-Sahla M, Simony-Lafontaine J, Kramar A, Lavaill R, Mollevi C, Warner M, Gustafsson J-Å, Rochefort H. Estrogen receptor β (ERβ) level but not its ERβcx variant helps to predict tamoxifen resistance in breast cancer. Clin Cancer Res 2004; 10:5769–5776.
11. Gruvberger-Saal SK, Bendahl P-O, Saal LH, Laakso M, Hegardt C, Edén P, Peterson C, Malmström P, Isola J, Borg Å, Fernö M. Estrogen receptor β expression is associated with tamoxifen response in ERα-negative breast carcinoma. Clin Cancer Res 2007; 13:1987–1994.
12. Honma N, Horii R, Iwase T, Saji S, Younes M, Takubo K, Matsuura M, Ito Y, Akiyama F, Sakamoto G. Clinical importance of estrogen receptor-β evaluation in breast cancer patients treated with adjuvant tamoxifen therapy. J Clin Oncol. 2008; 26:3727–3734.
13. Morani A, Warner M, Gustafsson JA. Biological functions and clinical implications of oestrogen receptors alfa and beta in epithelial tissues. J Intern Med. 2008; 264:128–142.
14. Toh CK, Ahmad B, Soong R, Chuah KL, Tan SH, Hee SW, Leong SS, Tan EH, Lim WT. Correlation between epidermal growth factor receptor mutations and expression of female hormone receptors in East-Asian lung adenocarcinomas. J Thorac Oncol. 2010; 5:17–22.
15. Nose N, Sugio K, Oyama T, Nozoe T, Uramoto H, Iwata T, Onitsuka T, Yasumoto K. Association between estrogen receptor-beta expression and epidermal growth factor receptor mutation in the postoperative prognosis of adenocarcinoma of the lung. J Clin Oncol. 2009; 27:411–417.
16. Schwartz AG, Prysak GM, Murphy V, Lonardo F, Pass H, Schwartz J, Brooks S. Nuclear estrogen receptor beta in lung cancer: expression and survival differences by sex. Clin Cancer Res. 2005; 11:7280–7287.
17. Skov BG, Fischer BM, Pappot H. Oestrogen receptor beta over expression in males with non-small cell lung cancer is associated with better survival. Lung Cancer. 2008; 59:88–94.
18. Kawai H, Ishii A, Washiya K, Konno T, Kon H, Yamaya C, Ono I, Minamiya Y, Ogawa J. Estrogen receptor alpha and beta are prognostic factors in non-small cell lung cancer. Clin Cancer Res. 2005; 11:5084–5089.
19. Ishibashi H, Suzuki T, Suzuki S, Niikawa H, Lu L, Miki Y, Moriya T, Hayashi S-i, Handa M, Kondo T, Sasano H. Progesterone receptor in non–small cell lung cancer - A potent prognostic factor and possible target for endocrine therapy. Cancer Res. 2005; 65:6450–6458.
20. Raso MG, Behrens C, Herynk MH, Liu S, Prudkin L, Ozburn NC, Woods DM, Tang X, Mehran RJ, Moran C, Lee JJ, Wistuba II. Immunohistochemical expression of estrogen and progesterone receptors identifies a subset of NSCLCs and correlates with EGFR mutation. Clin Cancer Res. 2009; 15:5359–5368.
21. Rouquette I, Lauwers-Cances V, Allera C, Brouchet L, Milia J, Nicaise Y, Laurent J, Delisle M-B, Favre G, Didier A, Mazières J. Characteristics of lung cancer in women: Importance of hormonal and growth factors. Lung Cancer. 2012; 76:280–285.
22. Stabile LP, Dacic S, Land SR, Lenzner DE, Dhir R, Acquafondata M, Landreneau RJ, Grandis JR, Siegfried JM. Combined analysis of estrogen receptor β-1 and progesterone receptor expression identifies lung cancer patients with poor outcome. Clin Cancer Res. 2011; 17:154–164.
23. Sun H-b, Zheng Y, Ou W, Fang Q, Li P, Ye X, Zhang B-b, Yang H, Wang S-y. Association between hormone receptor expression and epidermal growth factor receptor mutation in patients operated on for non-small cell lung cancer. Ann Thorac Surg. 2011; 91:1562–1567.
24. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pages C, Tosolini M, Camus M, Berger A, Wind P, Zinzindohoue F, Bruneval P, Cugnenc PH, et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science. 2006; 313:1960–1964.
25. Zhang L, Conejo-Garcia JR, Katsaros D, Gimotty PA, Massobrio M, Regnani G, Makrigiannakis A, Gray H, Schlienger K, Liebman MN, Rubin SC, Coukos G. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N Engl J Med. 2003; 348:203–213.
26. Pages F, Kirilovsky A, Mlecnik B, Asslaber M, Tosolini M, Bindea G, Lagorce C, Wind P, Marliot F, Bruneval P, Zatloukal K, Trajanoski Z, Berger A, et al. In situ cytotoxic and memory T cells predict outcome in patients with early-stage colorectal cancer. J Clin Oncol. 2009; 27:5944–5951.
27. Suzuki K, Kadota K, Sima CS, Nitadori JI, Rusch VW, Travis WD, Sadelain M, Adusumilli PS. Clinical impact of immune microenvironment in stage I lung adenocarcinoma: Tumor interleukin-12 receptor beta2 (IL-12Rbeta2), IL-7R, and stromal FoxP3/CD3 ratio are independent predictors of recurrence. J Clin Oncol. 2013; 31:490–498.
28. Mahmoud SM, Paish EC, Powe DG, Macmillan RD, Grainge MJ, Lee AH, Ellis IO, Green AR. Tumor-infiltrating CD8+ lymphocytes predict clinical outcome in breast cancer. J Clin Oncol. 2011; 29:1949–1955.
29. Mahmoud SM, Lee AH, Paish EC, Macmillan RD, Ellis IO, Green AR. The prognostic significance of B lymphocytes in invasive carcinoma of the breast. Breast Cancer Res Treat. 2012; 132:545–553.
30. Mahmoud SM, Paish EC, Powe DG, Macmillan RD, Lee AH, Ellis IO, Green AR. An evaluation of the clinical significance of FOXP3+ infiltrating cells in human breast cancer. Breast Cancer Res Treat. 2011; 127:99–108.
31. Bates GJ, Fox SB, Han C, Leek RD, Garcia JF, Harris AL, Banham AH. Quantification of regulatory T cells enables the identification of high-risk breast cancer patients and those at risk of late relapse. J Clin Oncol. 2006; 24:5373–5380.
32. Loi S, Sirtaine N, Piette F, Salgado R, Viale G, Van Eenoo F, Rouas G, Francis P, Crown JP, Hitre E, de Azambuja E, Quinaux E, Di Leo A, et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin Oncol. 2013; 31:860–867.
33. Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ, Van Schil PE, Garg K, Austin JH, Asamura H, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011; 6:244–285.
34. Yoshizawa A, Motoi N, Riely GJ, Sima CS, Gerald WL, Kris MG, Park BJ, Rusch VW, Travis WD. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol. 2011; 24:653–664.
35. Yoshizawa A, Sumiyoshi S, Sonobe M, Kobayashi M, Fujimoto M, Kawakami F, Tsuruyama T, Travis WD, Date H, Haga H. Validation of the IASLC/ATS/ERS lung adenocarcinoma classification for prognosis and association with EGFR and KRAS gene mutations: analysis of 440 Japanese patients. J Thorac Oncol. 2013; 8:52–61.
36. Warth A, Muley T, Meister M, Stenzinger A, Thomas M, Schirmacher P, Schnabel PA, Budczies J, Hoffmann H, Weichert W. The novel histologic International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification system of lung adenocarcinoma is a stage-independent predictor of survival. J Clin Oncol. 2012; 30:1438–1446.
37. Kadota K, Colovos C, Suzuki K, Rizk NP, Dunphy MP, Zabor EC, Sima CS, Yoshizawa A, Travis WD, Rusch VW, Adusumilli PS. FDG-PET SUVmax combined with IASLC/ATS/ERS histologic classification improves the prognostic stratification of patients with stage I lung adenocarcinoma. Ann Surg Oncol 2012; 19:3598–3605.
38. Kadota K, Nitadori J, Sarkaria IS, Sima CS, Jia X, Yoshizawa A, Rusch VW, Travis WD, Adusumilli PS. Thyroid transcription factor-1 expression is an independent predictor of recurrence and correlates with the IASLC/ATS/ERS histologic classification in patients with stage I lung adenocarcinoma. Cancer. 2013; 119:931–938.
39. Kadota K, Suzuki K, Kachala SS, Zabor EC, Sima CS, Moreira AL, Yoshizawa A, Riely GJ, Rusch VW, Adusumilli PS, Travis WD. A grading system combining architectural features and mitotic count predicts recurrence in stage I lung adenocarcinoma. Mod Pathol. 2012; 25(8):1117–1127.
40. Rekhtman N, Ang DC, Riely GJ, Ladanyi M, Moreira AL. KRAS mutations are associated with solid growth pattern and tumor-infiltrating leukocytes in lung adenocarcinoma. Mod Pathol. 2013; 26:1307–1319.
41. Vassallo J, Pinto GA, Alvarenga M, Zeferino LC, Chagas CA, Metze K. Comparison of immunoexpression of 2 antibodies for estrogen receptors (1D5 and 6F11) in breast carcinomas using different antigen retrieval and detection methods. Appl Immunohistochem Mol Morphol 2004; 12:177–182.
42. Huang Z, Zhu W, Szekeres G, Xia H. Development of new rabbit monoclonal antibody to estrogen receptor: Immunohistochemical assessment on formalin-fixed, paraffin-embedded tissue sections. Appl Immunohistochem Mol Morphol. 2005; 13:91–95.
43. Gomez-Fernandez C, Mejias A, Walker G, Nadji M. Immunohistochemical expression of estrogen receptor in adenocarcinomas of the lung: The antibody factor. Appl Immunohistochem Mol Morphol 2010; 18:137–141.
44. Casali C, Rossi G, Marchioni A, Sartori G, Maselli F, Longo L, Tallarico E, Morandi U. A single institution-based retrospective study of surgically treated bronchioloalveolar adenocarcinoma of the lung: clinicopathologic analysis, molecular features, and possible pitfalls in routine practice. J Thorac Oncol. 2010; 5:830–836.
45. Finberg KE, Sequist LV, Joshi VA, Muzikansky A, Miller JM, Han M, Beheshti J, Chirieac LR, Mark EJ, Iafrate AJ. Mucinous differentiation correlates with absence of EGFR mutation and presence of KRAS mutation in lung adenocarcinomas with bronchioloalveolar features. J Mol Diagn. 2007; 9:320–326.
46. Nakaoku T, Tsuta K, Ichikawa H, Shiraishi K, Sakamoto H, Enari M, Furuta K, Shimada Y, Ogiwara H, Watanabe SI, Nokihara H, Yasuda K, Hiramoto M, et al. Druggable oncogene fusions in invasive mucinous lung adenocarcinoma. Clin Cancer Res. 2014; Apr 11. [Epub ahead of print].
47. Fernandez-Cuesta L, Plenker D, Osada H, Sun R, Menon R, Leenders F, Ortiz-Cuaran S, Peifer M, Bos M, Dassler J, Malchers F, Schottle J, Vogel W, et al. CD74-NRG1 fusions in lung adenocarcinoma. Cancer Discov. 2014; 4:415–422.
48. Stabile LP, Davis AL, Gubish CT, Hopkins TM, Luketich JD, Christie N, Finkelstein S, Siegfried JM. Human non-small cell lung tumors and cells derived from normal lung express both estrogen receptor alpha and beta and show biological responses to estrogen. Cancer Res. 2002; 62:2141–2150.
49. Olivo-Marston SE, Mechanic LE, Mollerup S, Bowman ED, Remaley AT, Forman MR, Skaug V, Zheng Y-L, Haugen A, Harris CC. Serum estrogen and tumor-positive estrogen receptor-alpha are strong prognostic classifiers of non-small-cell lung cancer survival in both men and women. Carcinogenesis. 2010; 31:1778–1786.
50. Ganti AK, Sahmoun AE, Panwalkar AW, Tendulkar KK, Potti A. Hormone replacement therapy is associated with decreased survival in women with lung cancer. J Clin Oncol. 2006; 24:59–63.
51. Chlebowski RT, Schwartz AG, Wakelee H, Anderson GL, Stefanick ML, Manson JE, Rodabough RJ, Chien JW, Wactawski-Wende J, Gass M, Kotchen JM, Johnson KC, O'Sullivan MJ, et al. Oestrogen plus progestin and lung cancer in postmenopausal women (Women's Health Initiative trial): a post-hoc analysis of a randomised controlled trial. Lancet. 2009; 374:1243–1251.
52. Shen H, Yuan Y, Sun J, Gao W, Shu YQ. Combined tamoxifen and gefitinib in non-small cell lung cancer shows antiproliferative effects. Biomed Pharmacother 2010; 64:88–92.
53. Wang XY, Wang Y, Liu HC. Tamoxifen lowers the MMP-9/TIMP-1 ratio and inhibits the invasion capacity of ER-positive non-small cell lung cancer cells. Biomed Pharmacother 2011; 65:525–528.
54. Abe K, Miki Y, Ono K, Mori M, Kakinuma H, Kou Y, Kudo N, Koguchi M, Niikawa H, Suzuki S, Evans DB, Sugawara S, Suzuki T, et al. Highly concordant coexpression of aromatase and estrogen receptor β in non–small cell lung cancer. Human Pathology. 2010; 41:190–198.
55. Niikawa H, Suzuki T, Miki Y, Suzuki S, Nagasaki S, Akahira J, Honma S, Evans DB, Hayashi S, Kondo T, Sasano H. Intratumoral estrogens and estrogen receptors in human non-small cell lung carcinoma. Clin Cancer Res. 2008; 14:4417–4426.
56. Tai P, Wang J, Jin H, Song X, Yan J, Kang Y, Zhao L, An X, Du X, Chen X, Wang S, Xia G, Wang B. Induction of regulatory T cells by physiological level estrogen. J Cell Physiol. 2008; 214:456–464.
57. Xiong YH, Yuan Z, He L. Effects of estrogen on CD4(+) CD25(+) regulatory T cell in peripheral blood during pregnancy. Asian Pac J Trop Med. 2013; 6:748–752.
58. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. American Joint Committee on Cancer Cancer Staging Manual. 7th ed. New York, NY: Springer; 2009: 253–270.
59. Dignam JJ, Zhang Q, Kocherginsky M. The use and interpretation of competing risks regression models. Clin Cancer Res. 2012; 18:2301–2308.
60. Gray RJ. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Annals of Statistics. 1988; 16:1141–1154.