
INTRODUCTION
With society’s trending toward aging and unhealthy lifestyle changes (such as high heat, high fat food intake increase and reduction in physical activity), the prevalence rate of essential hypertension (EH) and osteoporosis (OP) increases every year, and these have become two of the most common diseases in the world [1–3]. Research has shown that the number of fractures related to osteoporosis has reached approximately 1500000 each year in the United States [4, 5]. In China, the population of people over 60 years old has been estimated as high as one hundred thirty-two million, and of these, approximately 90000000 patients have been diagnosed with osteoporosis [6, 7]. Osteoporosis fracture is a serious consequence of osteoporosis that can lead to the increased risk of mortality and morbidity. In addition, treating and nursing patients with osteoporosis and osteoporosis fracture requires not only an investment in manpower and material resources but is also expensive. This high cost is not conducive to a society’s goal of a harmonious and stable development; thus, identifying risk factors to prevent osteoporosis has become one of the hot issues.
Numerous studies have indicated that age, gender, smoking, drinking coffee, coronary heart disease, diabetes, essential hypertension and decreased estrogen levels are risk factors for osteoporosis [8–10]. Hypertension is one of the common diseases found in the clinic. Research results have shown that hypertension and osteoporosis are a common occurrence. Both hypertension and osteoporosis are age-related diseases and result from the interaction of genetic and environmental factors. However, there is still a controversy concerning whether a correlation exists between hypertension and osteoporosis. Several studies [11, 12] have indicated that hypertension is negatively correlated with bone mineral density. Cappuccio F P [11] and his colleague conducted a prospective study of 3676 women, and they found that high blood pressure in elderly white women is associated with increased bone loss at the femoral neck. This association may reflect greater calcium losses associated with high blood pressure, which may contribute to the risk of hip fractures. Similarly, Yang S and his colleagues published a longitudinal study in 2014 with 1,032 men and 1,701 women aged 50 years and older who had participated in the Dubbo Osteoporosis Epidemiology Study. Their results found that women with hypertension had lower BMD at the femoral neck (0.79 versus 0.82 g/cm(2)) than those without hypertension. After adjusting for confounding factors, hypertension was an independent risk factor for fragility fracture (HR: 1.49; 95% CI: 1.13–1.96). In men, hypertension was associated with higher femoral neck BMD (0.94 versus 0.92 g/cm(2)), but no significant association was found between hypertension and fracture risk. Alternatively, some studies [13, 14] have suggested that there is no correlation between essential hypertension and bone density. Fahad Javed F and his colleagues conducted a retrospective, cross-sectional study with 965 participants. The result found that the proportion of patients with both osteopenia and osteoporosis was similar in those with and without hypertension (osteopenia: 50% versus 50%, p = .95; osteoporosis: 18% versus 19%, p = 0.95).
Therefore, we conducted this meta-analysis to evaluate the relationship between essential hypertension and bone mineral density and to provide a theoretical basis for early prevention of osteoporosis.
RESULTS
Literature search
Following the development of our search strategy, 2325 articles were retrieved. After excluding the duplicates and articles that did not meet the inclusion criteria, we reviewed 34 possible relevant studies in full-text. A total of 17 studies [12–28] were excluded for the following reasons: six were narrative reviews, four were not related to the outcome of interest, one described the same population, and six reported the association. Finally, a total of 17 articles were included in our meta-analysis (Figure 1).
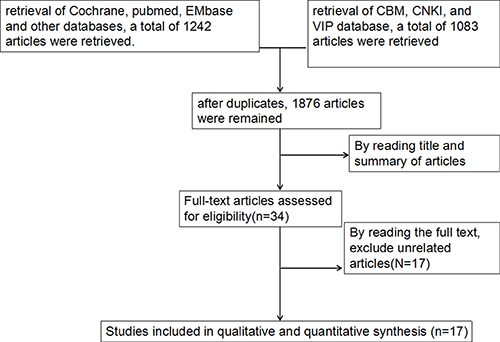
Figure 1: Flow diagram of selection of studies included in the meta-analysis.
Study characteristics
Table 1 shows the descriptive data for all 17 included studies, representing a total of 39,491 patients, Of this total, 13,375 were patients with essential hypertension, and 26116 were patients without essential hypertension. These studies were published from 2001 to 2015. In each study, the number of essential hypertension patients ranged from 13 to 6,636 and the number of patients without essential hypertension ranged from 13 to 18,195 without essential hypertension. Thirteen studies were conducted in China, one in the North America, one in Australia and one in Korea.
Table 1: Characteristic of case-control studies included in the meta-analysis
researcher |
year |
country |
hypertension (yes/no) |
Male/female |
age |
measuring position |
measuring instrument |
|---|---|---|---|---|---|---|---|
Chen K15 |
2009 |
China |
138/324 |
0/462 |
Population of 40-80 years old |
lumbar spine (1-4), femoral neck, large femoral rotor, Ward’s zone |
Dual energy X-ray |
He L16 |
2008 |
China |
103/135 |
0/238 |
Population of 30-80 years old |
lumbar spine, femoral neck, Ward’s zone, Large femoral rotor |
Dual energy X-ray |
Wang QP17 |
2009 |
China |
34/16 |
0/50 |
Population of 74.0±13.8 years old |
lumbar spin, femoral neck |
Dual energy X-ray |
Lin QM18 |
2011 |
China |
37/21 |
58/0 |
Population of 60-83 years old |
lumbar spine (2-4), femoral neck, Large femoral rotor, Ward’s zone |
Dual energy X-ray |
Liu Y19 |
2013 |
China |
78/104 |
unclear |
Population of Over 60 year old |
lumbar spine, femoral neck, Ward’s zone, oblique eminence of cuboid bone |
Dual energy X-ray |
Lu DH20 |
2015 |
China |
82/80 |
unclear |
Population of 61-71 years old |
lumbar spine, whole body |
Dual energy X-ray |
Yan LY21 |
2011 |
China |
13/28 |
unclear |
Population of 52-64 years old |
lumbar spin (1-4), femur |
Dual energy X-ray |
Wang X22 |
2001 |
China |
121/90 |
108/103 |
Population of 32-65 years old |
lumbar spin (1-4), femoral neck, Ward’s zone, oblique eminence of cuboid bone |
Dual energy X-ray |
xiang H23 |
2011 |
China |
311/291 |
293/309 |
Population of 44-79 years old |
lumbar spin (L2-L4), femoral neck, Ward’s zone, oblique eminence of cuboid bone |
Dual energy X-ray |
Yue RR24 |
2014 |
China |
256/205 |
unclear |
Population over 40 years of age |
lumbar spin (L1-L4) |
Dual energy X-ray |
Javed13 |
2012 |
America |
631/334 |
0/965 |
Women over 65 years of age |
lumbar spin (L1-L4), femoral neck |
Dual energy X-ray |
Yang11 |
2014 |
Australia |
660/2093 |
1032/1701 |
People over 50 years of age |
lumbar spin, femoral neck |
Dual energy X-ray |
Tsuda25 |
2001 |
Japan |
31/14 |
0/45 |
Women over 55 years of age |
lumbar spin (L2-L4) |
Dual energy X-ray |
Lee26 |
2015 |
Korea |
4089/4350 |
unclear |
Population over 50 years of age |
femoral neck |
Dual energy X-ray |
Perez14 |
2003 |
Spain |
82/40 |
0/122 |
postmenopausal women of 36-76 years old |
lumbar spin (L2-L4) |
Dual energy X-ray |
Xu JR27 |
2003 |
china |
60/60 |
60/60 |
Population of 63.6±10.2 years old |
forearm distal |
Dual energy X-ray |
Shi DZ28 |
2012 |
china |
115/91 |
206/0 |
Population of 64.87±3.4 years old |
forearm distal |
Dual energy X-ray |
Quality evaluation of included studies
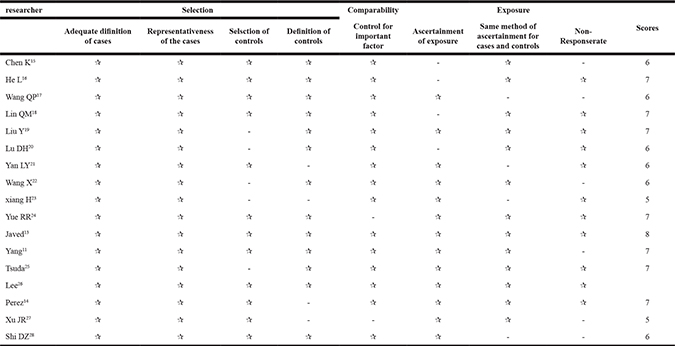
The methodological quality of the included studies was generally good. The NOS scores ranged from five to eight (Table 2). The median NOS score was 6.05.
Table 2 : Quality assessment of eligible studies based on newcastle-ottawa scale
Lumbar spine and femur rotor
The association between essential hypertension and bone mineral density of the lumbar spine was investigated in 15 studies [11–27]. The combined standard mean difference (SMD) was -0.05 (95% CI: −0.08~0.01, P = 0.006), with significant heterogeneity (Pfor heterogeneity = 0.000; I2 = 93.7%). The association between essential hypertension and bone mineral density of the femur rotor was investigated in 3 studies [15, 16, 18]. The combined standard mean difference (SMD) was 0.09 (95% CI: −0.07~0.24, P = 0.273) with significant heterogeneity (Pfor heterogeneity = 0.001; I2 = 86.5%) (Figure 2). In subgroup and sensitivity analysis of the lumbar spine (Asian and non-Asian), essential hypertension obviously reduced bone density of the lumbar spine (95%CI: −0.11~−0.03, p = 0.000) in Asian populations, but showed no association with bone density of the lumbar spine in non-Asian populations (95% CI: −0.04~0.11, p = 0.346) (Figure 3).
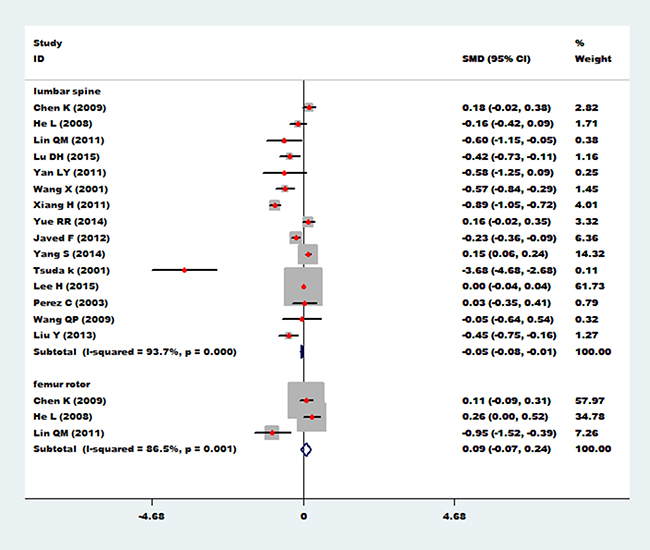
Figure 2: Forest plot of bone mineral density of lumbar spine and femur rotor with essential hypertension.
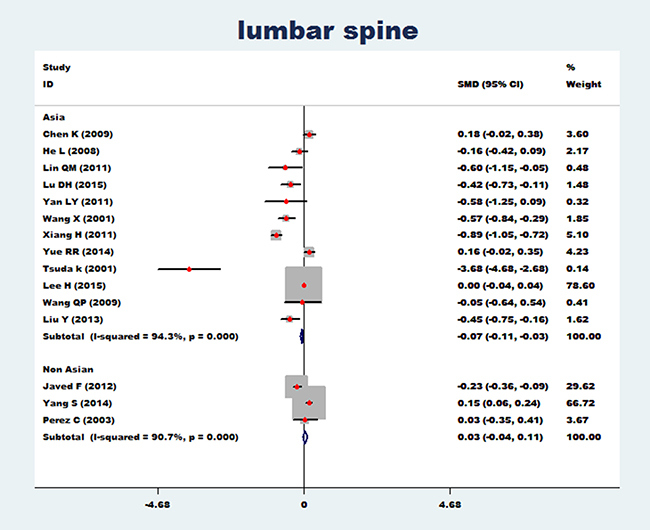
Figure 3: Forest plot of bone mineral density of lumbar spine with essential hypertension (Asian and non-Asian).
Femoral neck and ward’s triangle
The association between essential hypertension and the bone mineral density of femoral neck was investigated in 11 studies [12, 13–19, 21–23, 26]. The combined standard mean difference (SMD) was −0.06 (95%CI: −0.09~−0.02, p = 0.001), with significant heterogeneity (Pfor heterogeneity = 0.000; I2 = 96.7%). The association between essential hypertension and bone mineral density at Ward’s triangle was investigated in 6 studies [15, 16, 18, 19, 22, 23]. The combined standard mean difference (SMD) was −0.35 (95% CI: −0.45~−0.25, p = 0.000), with small heterogeneity (Pfor heterogeneity = 0.164; I2 = 36.4%) (Figure 4). In subgroup and sensitivity analysis of the femoral neck (Asian and non-Asian), essential hypertension obviously reduced bone density of the femoral neck in Asian populations (95% CI: −0.15~−0.07, p = 0.000) and non-Asian populations (95% CI: −0.15~−0.07, p = 0.002) (Figure 5).
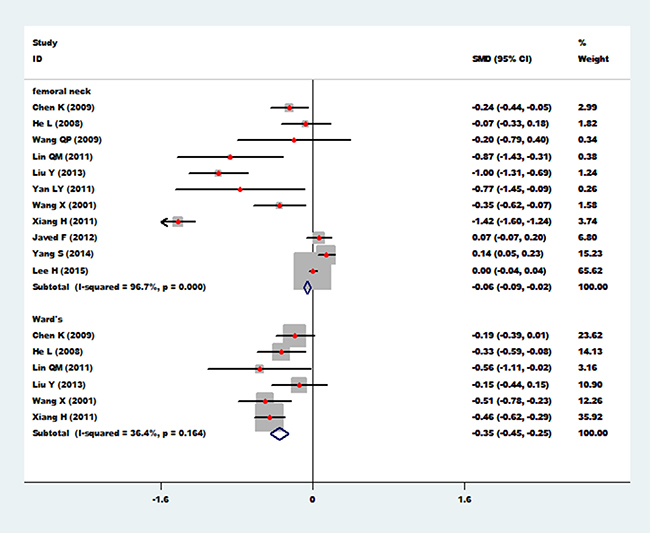
Figure 4: Forest plot of bone mineral density of femoral neck and Ward’s triangle with essential hypertension.
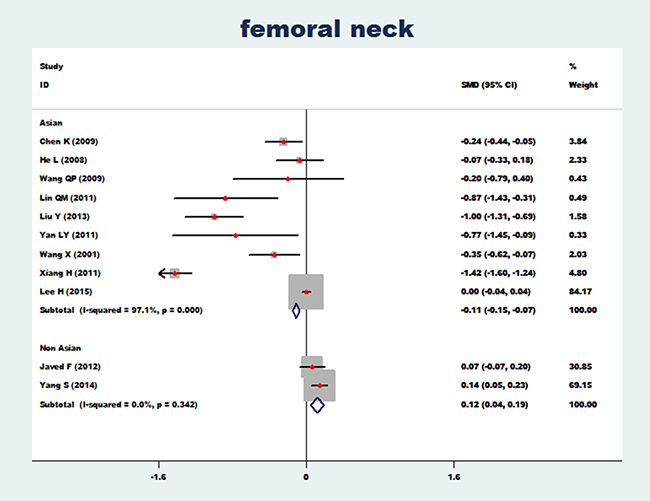
Figure 5: Forest plot of bone mineral density of femoral neck with essential hypertension (Asian and non-Asian).
Femoral intertrochanteric, calcaneus and forearm distal
The association between essential hypertension and bone mineral density of the femoral intertrochanteric region was investigated in 3 studies [19, 22, 23]. The combined standard mean difference (SMD) was −0.77 (95% CI: −0.90~−0.64, P= 0.000), with significant heterogeneity (Pfor heterogeneity = 0.000; I2 = 92.9%). The association between essential hypertension and bone mineral density of the calcaneus was investigated in 2 studies [27, 28]. The combined standard mean difference (SMD) was −0.24 (95% CI: −0.31~−0.18, P = 0.000), with significant heterogeneity (Pfor heterogeneity = 0.000; I2 = 99.2%). The relationship between essential hypertension and bone mineral density of the distal forearm was investigated in 3 studies [14, 27, 28]. The combined standard mean difference (SMD) was −0.06 (95% CI: −0.09~-0.03, P = 0.000), with significant heterogeneity (Pfor heterogeneity = 0.002; I2 = 83.9%) (Figure 6). Because of the limited number of studies, we failed to conduct subgroup and sensitivity analyses on these associations.
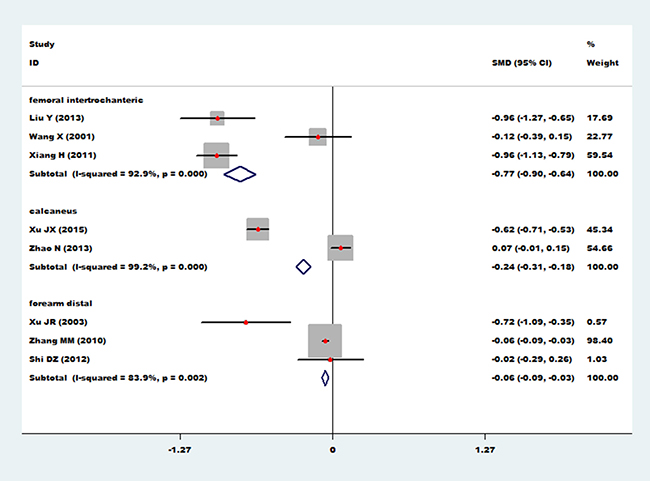
Figure 6: Forest plot of bone mineral density of femoral intertrochanteric, calcaneus, and distal forearm with essential hypertension.
Publication bias
Funnel plots were performed on the large heterogeneity of the results. The funnel plot of bone mineral density of the lumbar spine and essential hypertension is shown in Figure 7. The funnel plot of bone mineral density of the femoral neck and essential hypertension is shown in Figure 8. The funnel plot of bone mineral density at Ward’s triangle and essential hypertension is shown in Figure 9. As we can see from the funnel plot above, there is a certain bias in the articles included. Next, a meta-regression was conducted. Egger’s test was used to show that no significant publication bias was found (Table 3).
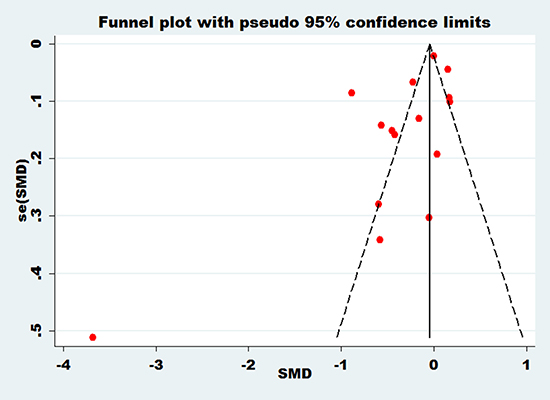
Figure 7: Funnel plot of bone mineral density of lumbar spine with essential hypertension.
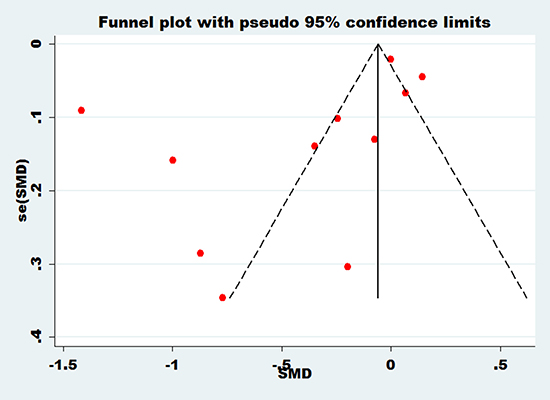
Figure 8: Funnel plot of bone mineral density of femoral neck with essential hypertension.
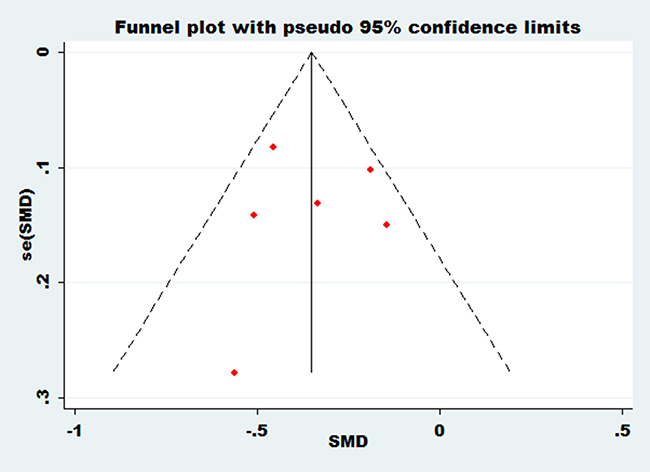
Figure 9: Funnel plot of bone mineral density at Ward’s triangle with essential hypertension.
Table 3: Publication bias (Egger’s test)
Std. Err |
t |
P |
95% CI |
|
|---|---|---|---|---|
lumbar spine |
1.281335 |
−2.20 |
0.047 |
[−5.584, −0.048] |
femoral neck |
2.152489 |
−1.82 |
0.102 |
[−8.789, 0.948] |
femur rotor |
3.229358 |
−1.68 |
0.342 |
[−46.445, 35.619] |
Ward’s |
1.779999 |
−0.02 |
0.982 |
[−4.983, 4.900] |
femoral intertrochanteric |
9.907325 |
0.59 |
0.663 |
[−120.079, 131.690] |
forearm distal |
2.083957 |
−0.87 |
0.545 |
[−28.288, 24.669] |
DISCUSSION
In contemporary society facing acceleration of population aging, the incidence of osteoporosis (OP) has been increasing every year [29, 30]. OP is a systemic, metabolic disease that exhibits primary clinical manifestations of low back pain and decreased activity [31, 32]. Patients with severe osteoporosis may even appear to have a short height, which places them at risk of spinal deformity and fragility fractures. Additionally, the pain caused by osteoporosis can cause serious decline of patient’s daily life quality. Skeletal deformation, as well as rising pulmonary infection rates, can cause disability and significantly increase mortality. At present, the clinical treatment of OP primarily, uses the method of drug therapy to intervene. However, there is currently no specific drug to reverse the development of OP [33, 34]. Therefore, early prevention is one of the fundamental methods to treat OP. In search for the early prevention methods for osteoporosis, researchers have conducted a large number of experimental studies [35, 36]. In current research, one of the hot-button topics is how to identify the risk factors in the early stages OP. Epidemiological studies have observed a large number of risk factors for OP, such as old age, low body mass, coronary heart disease, diabetes and poor blood glucose control, high blood ALP, essential hypertension and low estrogen levels.
Our study used meta-analysis to evaluate the relationship between essential hypertension and bone mineral density. Our results showed that essential hypertension can significantly reduce bone mineral density of the human body, including the lumbar spine (95% CI: −0.08~0.01), femoral neck (95% CI: −0.09~−0.02), Ward’s triangle (95% CI: −0.45~−0.25), femoral intertrochanteric region (95% CI: −0.90~−0.64), calcaneus (95% CI: −0.31~−0.18) and distal forearm (95% CI: -0.09~-0.03), but not including the femur rotor (95% CI: -0.07~0.24). Our meta-analysis results are consistent with Shi DZ [28] and Gotoh. Gotoh [37] studied the relationship between bone density, blood pressure and serum osteocalcin. The results showed that the bone density of hypertensive patients was significantly lower than that of the control group, and the relationship between bone density and systolic blood pressure was negative (r=-0.385). Furthermore, the results indicated that essential hypertension might be a factor that causes decreasing bone density.
Our study also found that essential hypertension had different effects on bone mineral density at different sites. The mechanism may be that ① different parts of body differ in skeletal muscle strength and exhibit inconsistent activity, which leads to varied effects on bone mineral density at different sites [38–40]. Ward’s triangle is primarily composed of cancellous bone, has a local blood supply that is poor, and is prone to fracture; therefore, Ward’s triangle is a sensitive region for detecting bone mineral density. The main function of the lumbar spine is to bear weight of the body. Because of this, the local calcium and phosphorus shape is good; thus, the bone density is less affected by high blood pressure. The femur rotor plays an important role in the process of standing and walking, so the local blood supply is good, which is favorable for promoting active osteoblasts and reducing the activity of osteoclasts. ② Antihypertensive drugs have different effects on different target organs. Many research results show that calcium channels exist not only in vascular smooth muscle, cardiac muscle and skeletal muscle cell membrane but also exist in skeletal muscle cells [41–45]. With antihypertensive drugs, calcium antagonists can also act on calcium channels in skeletal cells when they are acting on calcium channels in the vascular smooth muscle cells. Calcium channels of both skeletal muscle cells and cardiac muscle cells are L-type, which are voltage-dependent channels. All of these channels can be blocked by calcium antagonists and then affect the calcium metabolism of bone cells. Conducting an experiment in rabbits, Durieze [46] showed that nifedipine can cause cancellous bone loss, a decline in epiphyseal bone formation, decreased mineral deposition rate, and bone plate thinning. However, human studies showed that compared with BMD (lumbar [L2-L4], femur, radius), bone metabolic markers (including alkaline phosphatase, urine calcium/creatine, oxoprolinase/creatine) and regulating hormones (including testosterone, PTH, 1,25 (OH) 2D3, calcitonin), there have no significant difference between the nifedipine group and the control group [47, 48]. Therefore, further trials are needed to confirm these results.
In this study, we investigated the corresponding reasons for the heterogeneity and carried out a subgroup analysis and meta-regression, Egger’s test showed that no significant publication bias was tested (all P > 0.05). Thus, the results of this systematic meta-analysis are highly reliable.
MATERIALS AND METHODS
Literature search
A comprehensive literature search was performed to identify articles about the significance of essential hypertension and bone mineral density. The PubMed, EMBASE, Cochrane Library, CNKI, CBM and VIP databases (last update October 2016) were used to search for relevant articles with the following combination of search terms: “Bone Densities”, “Density, Bone”, “Bone Mineral Density”, “Bone Mineral Densities”, “Density, Bone Mineral”, “Bone Mineral Content”, “Bone Mineral Contents”, “Osteoporoses”, “Osteopenia”, “bone loss”, “Hypertension”, “Blood Pressure, High”, “Blood Pressures, High”, “High Blood Pressure” and “High Blood Pressures”. To expand our search, the bibliographies of articles that remained after the selection process were screened for additional suitable studies.
Study selection
Inclusion criteria for studies were as follows: (i) conducted on essential hypertension and bone mineral density in the last ten years; (ii) divided participants into a case group and a control group; (iii) reported the specific value of bone density or could be obtained by calculating the reported OR and 95% CI; (iv) published or accessible before October 2016; (v) selected participants in accordance with the WHO/ISH essential hypertension diagnostic criteria; (vi) did not exclude participants on the basis of gender; and (vi) measured bone mineral density using dual-energy x-ray absorptiometry.
Two reviewers (Ziliang Ye and Haili Lu) independently reviewed the titles and abstracts of the retrieved articles, applying the inclusion and exclusion criteria mentioned above. Articles were rejected if they were clearly ineligible. These two reviewers then independently reviewed the full-text versions of the remaining articles to determine their eligibility for inclusion. Disagreements were resolved by consensus.
Data extraction
Two reviewers (Ziliang Ye and Peng Liu) independently extracted the relevant data from each article and recorded these data on a standardized form. Any difference was resolved by consensus. The following data were extracted from these studies: an animal experiment; a cross-sectional study of the literature; a review, letters, and other non-essential literature; a non-randomized case-control study; information is not complete; OR and 95% CI values are not reported; and bone mineral density was measured by ultrasonic bone density instrument.
Quality assessment
Two reviewers (Ziliang Ye and Haili Lu) independently assessed the risk of bias using the Newcastle-Ottawa Scale (NOS), which consists of three factors: patient selection, comparability of the study groups, and assessment of outcome. A score of 0–9 (represented by stars) was allocated to each study. The studies achieving six or more stars were considered to be of high quality.
Statistical analysis
The odds ratio (OR) with a 95% confidence interval (CI) was used to express the pooled effect on discontinuous variables. The summary estimates of continuous variables were presented as standard mean differences (SMD) with 95% CI. Heterogeneity was quantified using the I2 statistic, where I2 > 50% represented between-study inconsistency. When there was no between-study inconsistency, fixed-effects meta-analyses were conducted to pool these outcomes across the included trials. When heterogeneity existed, the random-effects model was used. Publication bias was evaluated using a funnel plot. The results were considered statistically significant if P < 0.05. The pooled analyses were performed with Stata 11.0 software.
Limitations
There are several limitations in this study. (1) A total of 17 studies were included in this study, and most of these studies have some limitations. This study’s inclusion criteria resulted in more studies concentrated in Asia, and a small portion of trials from other areas. Under these circumstances, our findings may only apply to Asian populations and is not applicable to other populations due to genes, the environment, or diet. (2) The studies included in this meta-analysis did not clearly report the patients’ stage of hypertension or whether they were taking antihypertensive agents. (3) The sample size of this study was small, and the patient population mainly came from Asian countries, so some associations could not undergo subgroup analysis by country or nation.
In our meta-analysis, we found that essential hypertension may be a risk factor for osteoporosis. However, due to the quantity and quality of the included literature, confirmation of this conclusion still requires further .
Author contributions
Conceived and designed the experiments: Ziliang Ye and Haili Lu. Performed the experiments: Peng Liu. Analyzed the data: Haili Lu. Contributed reagents/materials/analysis tools: Peng Liu. Wrote the manuscript: Ziliang Ye. Reviewed/edited the manuscript: Peng Liu.
ACKNOWLEDGMENTS
This work was supported by the National Natural Science Foundation of China (No: 31160222 and No: 31360259), key projects of science and technology research in Universities of 2015 in Guangxi (KY2015ZD024) and Guangxi Colleges and Universities Key Laboratory of Human Development and Disease Research (0102402214009C), Guangxi Medical University 2016 undergraduate training program for innovation and Entrepreneurship (national level) (201610598004), Guangxi Medical University 2016 undergraduate training program for innovation and Entrepreneurship (school level) (201610598116), innovative training program for college students in 2017 (201710598036) and innovative training program for college students in 2018 (201710598030).
CONFLICTS OF INTEREST
The authors have declared that they have no competing interests exist.
REFERENCES
1. Svedbom A, Hernlund E, Ivergård M, Compston J, Cooper C, Stenmark J, Mccloskey EV, Jönsson B, Kanis JA. Osteoporosis in the European Union: a compendium of country-specific reports. Arch Osteoporos. 2013; 8:137.
2. Willson T, Nelson SD, Newbold J, Nelson RE, Lafleur J. The clinical epidemiology of male osteoporosis: a review of the recent literature. Clinical Epidemiology. 2015; 2015:65–76.
3. Peterlik M, Kállay E, Cross HS. Calcium nutrition and extracellular calcium sensing: relevance for the pathogenesis of osteoporosis, cancer and cardiovascular diseases. Nutrients. 2013; 5:302–27.
4. Wright NC, Looker AC, Saag KG, Curtis JR, Delzell ES, Randall S, Dawson-Hughes B. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J Bone Miner Res. 2014; 29:2520–6.
5. Madimenos FC, Liebert MA, Cepon-Robins TJ, Snodgrass JJ, Sugiyama LS. Determining osteoporosis risk in older Colono adults from rural Amazonian Ecuador using calcaneal ultrasonometry. Am J Hum Biol. 2015; 27:139–42.
6. Zhang Z, Liu Z, Shi S, Yanning LI. A retrospective literature study of osteoporosis incidence based on- 2. 5 SD criteria in mainland China. Chinese Journal of Osteoporosis. 2015; 21:1–24.
7. Epidemiological studies of Osteoporotic Hip Fracture in Hangzhou. Chinese Journal of Traditional Medical Traumatology & Orthopedics. 2013.
8. Shi S, Chen J, Wang YJ. Analysis of the risk factors of the elderly osteoporotic fracture after fracture. Jilin Medicine. 2013.
9. Yang TT, Xiao-Hong LV, Ren FH. Intervention study and influential factors of elder osteoporotic fracture. Mod Prev Med. 2012; 39.
10. Afshinnia F, Chacko S, Zahedi T. Association of lower serum cholesterol levels with higher risk of osteoporosis in type 2 diabetes. Endocr Pract. 2007; 13:620–8.
11. Cappuccio FP, Meilahn E, Zmuda JM, Cauley JA. High blood pressure and bone-mineral loss in elderly white women: a prospective study. Study of Osteoporotic Fractures Research Group. Lancet. 1999; 354:971.
12. Yang S, Nguyen ND, Center JR, Eisman JA, Nguyen TV. Association between hypertension and fragility fracture: a longitudinal study. Osteoporos Int. 2014; 25:97–103.
13. Javed F, Khan SA, Ayers EW, Aziz EF, Akram MS, Nadkarni GN, Sabharwal MS, Ahmad Z, Benjo AM, Herzog E. Association of hypertension and bone mineral density in an elderly African American female population. J Natl Med Assoc. 2012; 104:172–8.
14. Zhang M, Yagang L, Ying L, Xuena P, Binbin L, Zhong G, Qiang L. Study on the influencing factors for bone mineral density among 24831 people in Changchun. Chinese Journal of Osteoporosis. 2012; 2:125–27.
15. Chen K, Lai Y, Xue L. Study on the effect of hypertension on bone mineral density in postmenopausal women. Chinese Journal of Osteoporosis. 2009.
16. Lin HE, Li H. Correlation between hypertension and primary osteoporosis. Journal of Beijing University of Traditional Chinese Medicine. 2008.
17. Wang QP. Effects of metabolic syndrome on bone mineral density in postmenopausal women. Chinese Journal of Osteoporosis & Bone Mineral Research. 2009; 15:1141–50.
18. Lin QM, Chen F. Bone mineral density in elderly male patients with hypertension. Chinese J Hypertens. 2011.
19. Liu Y, Song CW, Du D. Study on the relationship between essential hypertension and bone mineral density and bone metabolism disorders in the elderly. Chinese Journal of laboratory diagnosis. 2014.
20. Lu DH, Lin Y, Zhang F. relationship between essential hypertension and bone mineral density in the elderly. Chinese medicine science. 2015.
21. Yan LY, Liu X, Ding L. Effects of diabetes and hypertension on bone mass. Anhui Medical & Pharmaceutical Journal. 2011.
22. Wang X. mechanism of bone mass reduction in essential hypertension patients. Journal of Capital Medical University. 2001.
23. Xiang H, Yuqin LI, Yuan H. The relationship between 25-OH-vitamin D and osteoporosis in patients with essential hypertension. Chinese Journal of Osteoporosis. 2011.
24. Yue RR. Correlation between essential hypertension and bone mineral density in middle aged and old male patients. Dalian Medical University. 2014.
25. Tsuda K, Nishio I, Masuyama Y. Bone mineral density in women with essential hypertension. Am J Hypertens. 2001; 14:704–07.
26. Lee HT, Shin J, Min SY, Lim YH, Kim KS, Kim SG, Kim JH, Lim HK. The relationship between bone mineral density and blood pressure in the Korean elderly population: the Korea National Health and Nutrition Examination Survey, 2008-2011. Clin Exp Hypertens. 2014; 9:101–9.
27. Xu JR, Zhong Q, Xin Z. The changes and significance of bone mineral density in patients with essential hypertension and serum osteocalcin. Journal of Guangdong Medical College. 2003.
28. Shi DZ, Wang XY. The relationship between the hypertetion and osteoporosis in middle aged male. China Practical Medicine. 2012.
29. Cosman F, Beur SJ, Leboff MS, Lewiecki EM, Tanner B, Randall S, Lindsay R. Erratum to: clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int. 2015; 26:2045–47.
30. Wallace T, Weaver C, Alexander D, Boushey C, Dawsonhughes B, Lappe J, Leboff M, Looker A. Calcium Plus Vitamin D Supplementation and Risk of Fractures: An Updated Meta-Analysis from NOF. Forensic Sci Int. 2014; 238:68–82.
31. Engelke K, Adams JE, Armbrecht G, Augat P, Bogado CE, Bouxsein ML, Felsenberg D, Ito M, Prevrhal S, Hans DB, Lewiecki EM. Clinical Use of Quantitative Computed Tomography and Peripheral Quantitative Computed Tomography in the Management of Osteoporosis in Adults: The 2007 ISCD Official Positions. J Clin Densitom. 2008; 11:123–62.
32. Miller PD. Bone Disease in CKD: A Focus on Osteoporosis Diagnosis and Management. Am J Kidney Dis. 2014; 64:290–304.
33. Watts NB, Lewiecki EM, Miller PD, Baim S. National Osteoporosis Foundation 2008 Clinician's Guide to Prevention and Treatment of Osteoporosis and the World Health Organization Fracture Risk Assessment Tool (FRAX): what they mean to the bone densitometrist and bone technologist. Journal of Clinical Densitometry the Official Journal of the International Society for Clinical Densitometry. 2008; 11:473–7.
34. Cranney A, Adachi JD, Guyatt G, Papaioannou A, Robinson VA, Shea BJ, Tugwell P, Waldegger LM, Weaver B, Wells G. Risedronate for the prevention and treatment of postmenopausal osteoporosis. John Wiley & Sons, Ltd. 2003.
35. Ahn E, Lee J, Yong SP, Noh HM, Bo HK. Association between delivery at an advanced maternal age and osteoporosis in elderly Korean women. J Bone Miner Metab. 2015; 33:666–73.
36. Preiss D, Welsh P, Murphy SA, Ho JE, Waters DD, Demicco DA, Cannon CP, Sabatine MS, Seshasai SRK, Barter P. Osteoporosis prevention, diagnosis, and therapy. 2001.
37. Naitoh M, Hirukawa A, Katsumata A, Ariji E. Prospective study to estimate mandibular cancellous bone density using large-volume cone-beam computed tomography. Clin Oral Implants Res. 2010; 21:1309–13.
38. Maeda S, Miyaki A, Sasai H, Tsujimoto T, So R, Tanaka K. Lifestyle Modification Decreases Arterial Stiffness in Overweight and Obese Men: Dietary Modification vs. Exercise Training. Int J Sport Nutr Exerc Metab. 2015; 25:69–77.
39. Strong WB, Malina RM, Blimkie CJ, Daniels SR, Dishman RK, Gutin B, Hergenroeder AC, Must A, Nixon PA, Pivarnik JM, Rowland T, Trost S, Trudeau F. Evidence based physical activity for school-age youth. J Pediatr. 2005; 146:732–7.
40. Guiying LI, Bo LV, Bin DI. Effect of type 2 diabetes mellitus on osteoporosis incidence and analysis of osteoporosis-related risk factors. Chinese Journal of Osteoporosis. 2009.
41. Vestergaard P, Rejnmark L, Mosekilde L. Osteoarthritis and risk of fractures. Calcif Tissue Int. 2009; 84:249–56.
42. Mancilla EE, Galindo M, Fertilio B, Herrera M, Salas K, Gatica H, Goecke A. L-type calcium channels in growth plate chondrocytes participate in endochondral ossification. J Cell Biochem. 2007; 101:389–98.
43. Zhou S, Shen Y, Wang L, Li P. Epithelial-mesenchymal transition and mesenchymal-epithelial transition response during differentiation of growth-plate chondrocytes in endochondral ossification. Int J Clin Exp Med. 2015; 8:12076–85.
44. Poiraudeau S, Lieberherr M, Kergosie N, Corvol MT. Different mechanisms are involved in intracellular calcium increase by insulin-like growth factors 1 and 2 in articular chondrocytes: voltage-gated calcium channels, and/or phospholipase C coupled to a pertussis-sensitive G-protein. J Cell Biochem. 1997; 64:414–22.
45. Wang ZM, Messi ML, Renganathan M, Delbono O. Insulin-like growth factor-1 enhances rat skeletal muscle charge movement and L-type Ca2+ channel gene expression. J Physiol. 1999; 516:331–41.
46. Duriez J, Flautre B, Blary MC, Hardouin P. Effects of the calcium channel blocker nifedipine on epiphyseal growth plate and bone turnover: A study in rabbit. Calcif Tissue Int. 1993; 52:120–4.
47. Matta C, Zákány R, Mobasheri A. Voltage-dependent calcium channels in chondrocytes: roles in health and disease. Curr Rheumatol Rep. 2015; 17:43.
48. Perezcastrillon JL, Justo I, Sanzcantalapiedra A, Pueyo C, Hernandez G, Duenas A. Effect of the Antihypertensive Treatment on the Bone Mineral Density and Osteoporotic Fracture. Curr Hypertens Rev. 2005; 1:61–66.