
INTRODUCTION
Malignant pleural mesothelioma(MPM) is a rare but highly aggressive asbestos-induced malignancy, with a poor prognosis and increasing incidence [1]. Although the surgery and combination chemotherapy are proved effective, the median overall survival of MPM remains poor [2]. Therefore, it is necessary to identify prognostic markers to help with the survival of MPM. Mesothelin is a 40 kDa cell surface glycoprotein, and highly expressed in several human cancers, including mesotheliomas, pancreatic cancers and ovarian cancers [3]. Although mesothelin bounds to cell membrane, a circulating form termed soluble mesothelin can be detected in the blood and pleural effusion by using enzyme-linked immunosorbent assay (ELISA) [4]. Soluble mesothelin is a useful biomarker, which can not only play an important role in the diagnosis [5, 6], but also be beneficial to monitor the progression and treatment response of MPM [7]. Recently, some studies have reported that high soluble mesothelin level can be considered as a negative prognostic factor in patients with MPM [8-12]. On the other hand, some studies show that the prognostic value of soluble mesothelin in MPM is not conclusive and needs further evaluation [13-15]. Despite numerous published studies, the prognostic value of soluble mesothelin remains controversial. Additionally, the correlation between the survival of MPM patients and clinicpathological characteristics such as age, gender, tumor histology and tumor stage are uncertain. To evaluate the prognostic value of soluble mesothelin and the effect of clinicopathological characteristics on the survival of MPM patients, we performed a meta-analysis.
RESULTS
Characteristics of eligible studies
A total of 1285 records were identified through database searching. Six hundred and twelve records were excluded for duplication. After browsing the titles and abstracts, 16 studies that might meet the inclusion criteria were screened out to read full texts. These studies were carefully reviewed. Finally, 8 eligible studies including 579 patients were selected for this meta-analysis (Figure 1). The characteristics of eligible studies were summarized in Table 1. The size of sample in each study ranged from 36 to 107 and all of the patients were Caucasian. The most common tumor site of the patients was pleural. The mestothelin level was tested using serum specimen in 7 studies. In the rest 1 study, the samples were from pleural effusion. Two Mesomark ELISA kits (Mesomark kit by Fujirebio Diagnostics, Malvern, Pennsylvania, USA or by Cisbio International, Gif-Sur-Yvette, France) were used in eligible studies to measure mesothelin level. The mesothelin level was expressed in nanomoles per liter (nmol/L) in the eligible studies. Six studies provided available HR with 95%CI. The other 2 studies had their HRs and 95%CIs calculated from Kaplan- Meier survival curves.
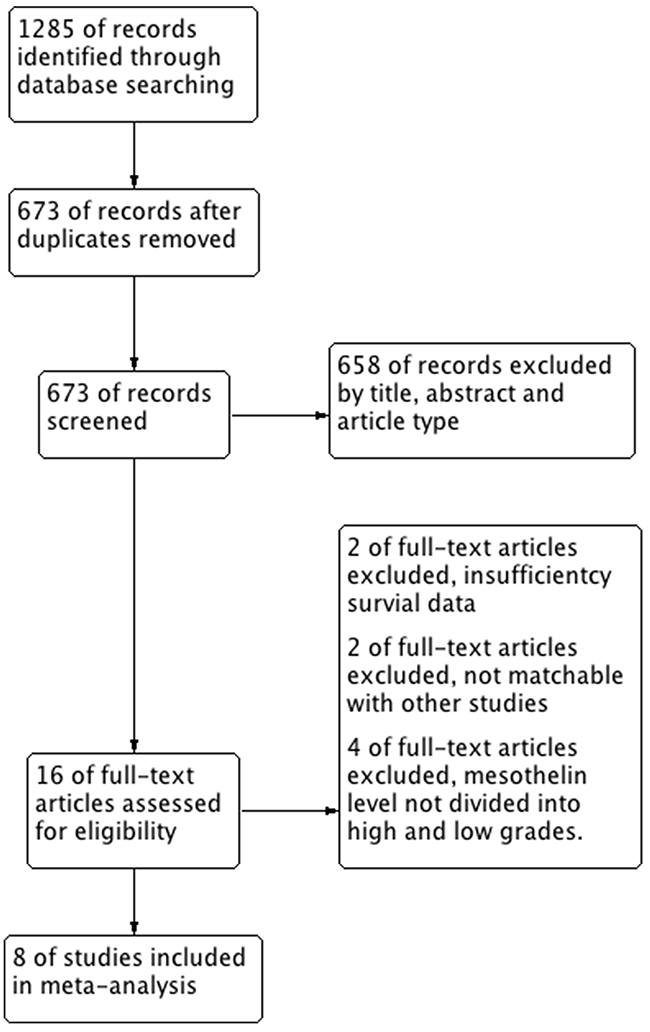
Figure 1: Flow chart of study selection in this meta-analysis.
Table 1: Main characteristics and results of the eligible studies
Author (year) |
Country |
Study |
No. of |
Ethnicity |
Tumor |
Tumor |
Tumor |
Treatment |
Specimen |
Cut-off |
Method |
Source |
Multivariate |
Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Linch et al. |
UK |
P |
53 |
Caucasian |
Ple/Per |
46/1/5/1 |
NA |
CT/BSC |
Serum |
2.7 |
ELISAa |
Reported |
No |
7 |
Dipalma et al. (2011) [11] |
Italy |
P |
36 |
Caucasian |
pleural |
29/4/3/0 |
16/6/3/11 |
NA |
Serum |
1.2 |
ELISAb |
Reported |
No |
7 |
Creaney et al. (2011) [10] |
Australia |
P |
95 |
Caucasian |
pleural |
68/9/18/0 |
NA |
CT/ BSC /Surg/RT |
Serum |
5 |
ELISAa |
Reported |
Yes |
9 |
Grigoriu et al. (2009) [29] |
France |
R |
40 |
Caucasian |
pleural |
35/3/2/0 |
NA |
CT/BSC/GT |
Serum |
NA |
ELISAc |
Estimated |
No |
6 |
Schneider et al. 2008) [12] |
Germany |
P |
100 |
Caucasian |
pleural |
66/12/15/7 |
I/II/III/IV/II-III |
CT/Surg/RT/BSC/Un |
Serum |
3.5 |
ELISAa |
Reported |
Yes |
8 |
Grigoriu et al. (2007) [9] |
France |
P |
96 |
Caucasian |
pleural |
73/10/13/0 |
11/21/32/19 |
CT/BSC /Surg |
Serum |
3.5 |
ELISAb |
Reported |
Yes |
8 |
Cristaudo et al. (2007) [8] |
Italian |
P |
107 |
Caucasian |
pleural |
72/10/7/18 |
I-II/III-IV/NOS* 43/45/19 |
NA |
Serum |
1 |
ELISAb |
Reported |
Yes |
9 |
Creaney et al. (2007) [13] |
Australia |
P |
52 |
Caucasian |
NA |
15/9/5/23 |
NA |
NA |
PE |
26 |
ELISAa |
Estimated |
No |
7 |
P: prospective; R: retrospective; Ple: pleural; Per: peritoneal; Epi: epithelial; Sar: Sarcomatoid; Bip: Biphasic; NA: not available; Un: unknown; NOS*: not otherwise specified; PE: pleural effusion; CT: chemotherapy; RT: radiotherapy; BSC: best supportive care; Surg: surgery; GT: immunotherapy.
ELISAa: tested by the MESOMARK kit (Fujirebio Diagnostics); ELISAb: tested by the MESOMARK kit (Cisbio International); ELISAc: tested by the MESOMARK kit (Fujirebio Diagnostics or Cisbio International).
Prognostic impact of soluble mesothelin in MPM
The main meta-analysis results, the correlation between soluble mesothelin and the survival of MPM, were summarized in Figure 2. The pooled HR for all eligible studies which evaluated soluble mesothelin in MPM patients was 1.958 (95%CI 1.531-2.504). The results showed that high soluble mesothelin level was statistically significant correlated with the overall survival of MPM (p = 0.000) with a low heterogeneity (I2 = 1.1%, p = 0.421). To detect the potential heterogeneity, subgroup analysis stratified by specimen type, cut-off value, sample size, source of HR and survival analysis mode were applied. The results of subgroup analysis indicated that patients with high soluble mesothelin level had poorer overall survival compared with patients with low soluble mesothelin level in the following subgroups: serum subgroup (HR = 2.016; 95% CI =1.571-2.588; p = 0.000), cut-off value <5 subgroup (HR = 1.980; 95% CI = 1.516-2.586; p = 0.000), sample size <50 subgroup (HR = 4.970; 95% CI = 1.633- 15.131; p = 0.005), sample size ≥50 subgroup (HR = 1.866; 95% CI = 1.450- 2.402; p = 0.000), HR reported subgroup (HR = 2.016; 95% CI = 1.569-2.591; p = 0.000), multivariate analysis subgroup (HR = 1.925; 95% CI = 1.466-2.528; p = 0.000), non-multivariate analysis subgroup (HR = 2.111; 95% CI = 1.188-3.752; p = 0.011). The results of subgroup analysis revealed some possible contributors to the heterogeneity: sample size, specimen type, source of HR and survival analysis mode. The detailed results of subgroup analysis were summarized in Table 2.
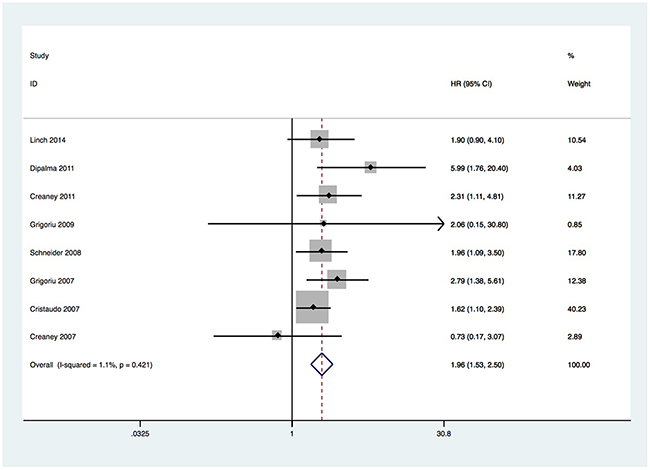
Figure 2: Forest plots for the correlation between soluble mesothelin and overall survival.
Table 2: Pooled hazard ratio (HR) of soluble mesothelin (high vs low level) for overall survival according to subgroup analysis
Subgroup |
No. of studies |
Effects model |
HR(95%CI) |
Significance |
Heterogeneity test |
||
|---|---|---|---|---|---|---|---|
Chi2 |
I2 (%) |
p-Value |
|||||
Overall |
8 |
Fixed |
1.958 (1.531, 2.504) |
p = 0.000 |
7.08 |
1.1 |
0.421 |
Specimen |
|||||||
Serum |
7 |
Fixed |
2.016 (1.571, 2.588) |
p = 0.000 |
5.24 |
0.0 |
0.514 |
Pleural effusion |
1 |
- |
0.73 (0.17, 3.07) |
- |
- |
- |
- |
Cut-off value (nmol/L) |
|||||||
<5 |
5 |
Fixed |
1.980 (1.516, 2.586) |
p = 0.000 |
5.09 |
21.4 |
0.278 |
≥5 |
2 |
Fixed |
1.826 (0.949, 3.511) |
p = 0.071 |
1.94 |
48.4 |
0.164 |
NA |
1 |
- |
2.02 (0.14, 29.97) |
- |
- |
- |
- |
Sample size |
|||||||
<50 |
2 |
Fixed |
4.970 (1.633, 15.131) |
p = 0.005 |
0.51 |
0.0 |
0.475 |
≥50 |
6 |
Fixed |
1.866 (1.450, 2.402) |
p = 0.000 |
3.74 |
0.0 |
0.587 |
Source of HR |
|||||||
Reported |
6 |
Fixed |
2.016 (1.569, 2.591) |
p = 0.000 |
5.24 |
4.5 |
0.388 |
Estimated |
2 |
Fixed |
0.925 (0.259, 3.297) |
p = 0.904 |
0.45 |
0.0 |
0.502 |
Multivariate analysis |
|||||||
Yes |
4 |
Fixed |
1.925 (1.466, 2.528) |
p = 0.000 |
2.07 |
0.0 |
0.558 |
No |
4 |
Fixed |
2.111 (1.188, 3.752) |
p = 0.011 |
4.93 |
39.1 |
0.177 |
Correlation between clinicopathological characteristics and the survival of MPM
The main meta-analysis results of the correlation between clinicopathological characteristics and the survival of MPM patients were summarized in Table 3. The clinicopathological characteristics included age, gender, tumor histology and tumor stage. The results showed that not all the clinicopathologicl characteristics were significantly correlated with the survival of MPM patients. The pooled HR for age, gender, tumor histology and tumor stage were, respectively, 1.256(95% CI =0.907-1.739; p = 0.170), 0.932(95% CI =0.168-5.17; p = 0.936), 3.214(95% CI = 2.071-4.988; p = 0.000), 2.007(95% CI = 1.477-2.727; p = 0.000). No significant correlations were found between the survival of MPM patients and age or gender. However, tumor histology and tumor stage were significantly related to the survival of MPM patients with no heterogeneity.
Table 3: Main results of correlation between clinicopathological characteristics and the survival of MPM patients
Clinical characteristics |
No. of studies |
Effects model |
Pooled HR(95%CI) |
Significance |
Heterogeneity test |
||
|---|---|---|---|---|---|---|---|
Chi2 |
I2 (%) |
p-Value |
|||||
Age |
Random |
1.256 (0.907, 1.739) |
p = 0.170 |
6.76 |
70.4 |
0.034 |
|
Gender |
Random |
0.932 (0.168, 5.17) |
p = 0.936 |
9.04 |
88.9 |
0.003 |
|
Tumor histology |
Fixed |
3.214 (2.071, 4.988) |
p = 0.000 |
0.95 |
0.0 |
0.623 |
|
Tumor stage |
Fixed |
2.007 (1.477, 2.727) |
p = 0.000 |
0.07 |
0.0 |
0.966 |
|
Sensitivity analysis and publication bias
Sensitivity analysis was used to estimate the influence by omitting one study at a time and calculate the combined HR. The result indicated that no individual study had a significant influence on the observed effect size (pooled HR) for overall survival (Figure 3). Begg’s funnel plot with pseudo 95 % confidence limits was performed to estimate the publication bias of the eight studies included about overall survival (Figure 4). There was no significant publication bias observed with the Begg’s tests of overall survival (p = 0.711). To validate the result, the nonparametric trim and fill method was further used to evaluate the impact of this bias and the pooled HR for overall survival. The results indicated no significant publication bias among studies and the pooled HR remained significant. Collectively, the result of this meta-analysis was robust and statistically reliable.
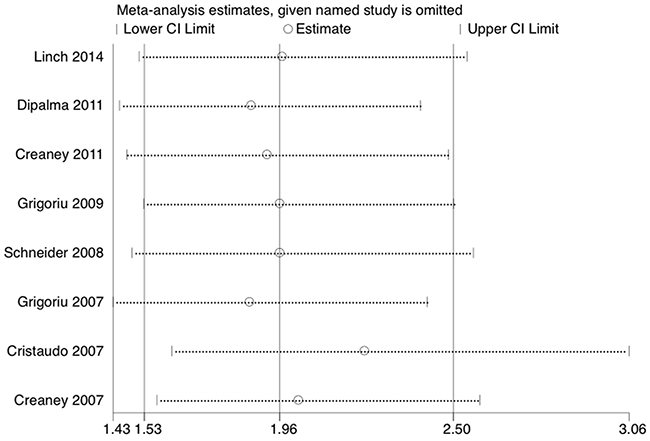
Figure 3: Sensitivity analysis on the correlation between soluble mesothelin and overall survival.
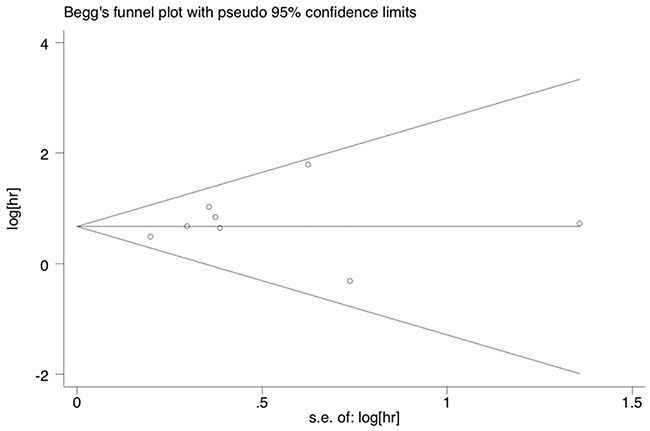
Figure 4: Funnel plots of publication bias on the correlation between soluble mesothelin and overall survival.
DISCUSSION
To our best knowledge, this meta-analysis is the first study to evaluate the prognostic value of soluble mesothelin and effect of clinicopathological characteristics on the survival of MPM patients.
Mesothelin was firstly studied as a prognostic indicator in MPM by Cristaudo et al. [8], who reported a significant inverse correlation between mesothelin level and the overall survival of MPM. Grigoriu et al. [9] also found high mesothelin level was negatively correlated with the survival of MPM patients in both univariate and multivariate analysis. Another study, conducted by Yamada et al. [16], indicated that pleural effusion mesothelin level also had a prognostic effect the survival of MPM patients. However, in two studies conducted by Hollevoet et al. [17, 18], finding serum mesothelin was not an effective predictor for the survival of MPM patients. By the result of our meta-analysis, we found that high mesothelin level is a negative prognostic factor for MPM patients. Moreover, in the subgroup analysis, which survival analysis was conducted by multivariate analysis, the high mesothelin level was still significantly related to the survival of MPM patients. Data above indicated that mesothelin might be an independent prognostic factor in MPM patients. In addition, some clinicopathdological characteristics such as age, gender, tumor histology and tumor stage were also reported to have prognostic effects on the survival of MPM Patients. Recent studies showed old age, male gender, non-epithelioid histology and advanced tumor stage were significantly related to poor survival of MPM patients [19-22]. The results of our meta-analysis indicated that the survival of MPM patients was significantly correlated with tumor histology and tumor stage, which suggested that non-epithelioid histology and advanced tumor stage were significant negative predictors of the survival in MPM patients. However, neither age nor gender was found to be significantly related with the survival of MPM patients in our meta-analysis. There are some other independent prognostic factors proposed for MPM patients, such as white blood cell count, C-reactive protein level, hemoglobin level, neutrophil-to-lymphocyte ratio, lactate dehydrogenase, performance status, comorbidity, weight loss and breathlessness [20, 23-26]. Moreover, the therapies also contributed to the survival of MPM patients. Patients treated with chemotherapy had significantly longer survival than those treated with best supportive care [26]. Chemotherapy and radiation to port sites independently and in combination were associated with improved overall survival in MPM patients [27]. Absence of adjuvant therapy and non-curative surgery were significantly related to poor survival [19].
The mechanisms responsible for the association between high mesothelin level and poor survival of MPM patients remain unclear. More and more studies have showed that soluble mesothein level was closely associated with disease progression, disease status and tumor burden [17, 28, 29]. Additionally, Mesothelin contributes to further understanding of the biology of MPM, because it participates in cell adherence, cell proliferation and tumor invasion of MPM [30, 31]. Mesothelin is a suitable candidate for drug therapy and a potential target for designing novel therapeutic strategies [32]. Recent studies have indicated that antimesothelin immunotoxins, such as SS1P and RG7787, are well tolerated and exhibits significant antitumor activity in patients with MPM [33, 34]. Amatuximab is tolerable in MPM patients with a disease control rate of 90% when given with pemetrexed and cisplatin [35, 36]. The exposure of amatuximab is associated with overall survival, higher amatuximab exposure accompanied with longer overall survival [37]. Mesothelin gene silencing has an antitumor effect on cell lines overexpressing mesothelin deriving from MPM, which means mesothelin could be considered as a key molecular target for novel gene-based targeted therapies of MPM [38]. Collectively, mesothelin participates in cell adherence, cell proliferation, tumor invasion of MPM, and plays an important role in monitoring the treatment response, the disease progression and the prognosis in MPM patients. Mesothelin is also a suitable potential target for drug therapy.
There are some limitations in this meta-analysis. Firstly, both the number of included studies and the simple size of each study were relatively small. Secondly, not all of the HRs with 95% CI were directly extracted from the studies, the reconstructed HR calculated via Kaplan-Meier survival curves unavoidably brought some unexpected errors. Thirdly, the ethnicities of the patients in our analysis were Caucasian, there might be ethnic bias existed. Fourthly, not all of the survival analyses of the eligible studies were conducted by the multivariate analysis, there might be some confounding factors existed. Fifth, though no significant heterogeneity among studies was found in our study, we could not fully neglect the potential heterogeneity. The subgroup analysis was used to assess the sources of heterogeneity. The results of subgroup analysis revealed that sample size, specimen type, source of HR and survival analysis mode might contribute to the heterogeneity. Therefore, more eligible studies are needed to explore the sources of heterogeneity. Moreover, the stability of our results was confirmed by sensitivity analysis.
In conclusion, the survival of MPM is significantly correlated with tumor histology and tumor stage. Furthermore, high soluble mesothelin level may lead to a poor prognosis for MPM patients. Therefore, it is appropriate to regard soluble mesothelin as an independent prognostic marker and a novel potential therapeutic target for MPM patients.
MATERIALS AND METHODS
This meta-analysis was performed according to the statement of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [39].
Search strategy
Two investigators independently searched the Medline (via OvidSP), Embase(via OvidSP), COCENTRAL and Pubmed for studies that investigated the prognosis with soluble mesothelin in MPM. Studies were examined, and an updated search was conducted on November 2016. The search terms were as follows: mesothelin and mesothelioma. The title and abstract of each identified study were browsed to exclude any irrelevant publications. The full texts of all potentially eligible studies were retrieved, and their references were carefully browsed to find other studies that met the criteria. Disagreements between two investigators were settled by discussion.
Inclusion and exclusion criteria
Studies eligible for inclusion in this meta-analysis met the following criteria: (1) evaluated the prognostic value of soluble mesothelin, either in blood or pleural effusion(PE); (2) soluble mesothelin level was divided into high and low grades; (3) the literature should be published with full texts. Exclusion criteria included: (1) articles published as reviews, conference abstracts or comments;(2) studies with insufficient survival data for which HR and CI could not be determined;
Data extraction and quality assessment
Two investigators extracted useful information from eligible studies independently. The following information was recorded: first author surname, publication year, country, study type, number of patients, ethnicity, tumor site, tumor histology, tumor stage, treatment, specimen, method, cut-off value, source of HR (95% CI), survival analysis mode. Hazard ratio was the most appropriate statistic to analyze time-to-event outcomes, because both the number of events and time of events were taken into account. When the HR with 95% was available from the original article, we used the data directly. Otherwise we extracted data from the Kaplan-Meier survival curves by the software Engauge Digitizer Version 4.1 (http://digitizer.sourceforge.net/). The method proposed by Tierney et al. was used to calculated the HR and 95%CI [40]. When both univariate and multivariate analysis were conducted in the studies, we preferred the results based on multivariate analysis. Disagreements were settled by discussion. The Newcastle-Ottawa Scale (NOS) was used to evaluate the quality of each individual study [41]. The NOS consists of three parameters of quality: selection (there terms: representativeness of the exposed cohort, selection of the non exposed cohort, selection of the non exposed cohort, demonstration that outcome of interest was not present at start of study?), comparability (one term: comparability of cohorts on the basis of the design or analysis), and outcome assessment (three terms: assessment of outcome, was follow-up long enough for outcomes to occur? adequacy of follow up of cohorts). The NOS score was ranged from 0 to 9, and the study with an NOS score ≥ 6 was considered as a high quality study.
Statistical analysis
Hazard ratio (HR) with 95% CI was performed to estimate the prognostic value of soluble mesothelin and the effect of clinicopathological characteristics on the survival of MPM patients. Cochrane’s Q test (Chi-squared test) and I2 metric were performed to calculate the statistical heterogeneity of the pooled HR with 95% CI [42]. For I2 statistics, I2<25% indicates there is a low heterogeneity, I2= 25%-50% indicates there is a moderate heterogeneity and I2 >50% indicates there is a significant heterogeneity [43]. The fixed-effect model was adopted in the meta-analysis when no statistically significant heterogeneity was observed between studies (p≥0.1 or I2 <50%), otherwise the random-effect model was used. When HR >1, a poor prognosis for MPM patients was indicated by high soluble mesothelin level. If there was no overlap between 95% CI and 1, it would be considered that the impact of soluble mesothein on survival was statistically significant. Subgroup analysis was stratified by specimen type, cut-off value, sample size, source of HR and survival analysis mode. The sensitivity analysis was performed using the leave-one-out method to explore the influence of each individual study on the pooled HR for overall survival. Publication bias was evaluated by funnel plot(qualitative) and Begg’s test(quantitative). When publication bias existed, the nonparametric trim and fill method was applied to re-estimate a corrected effect size after adjustment for publication bias [44]. All p values were based on two-sided test, p value < 0.05 was considered to be statistically significant. STATA 11.0 software (Stata Corporation, College Station, TX) was used to conduct all statistical analysis.
Author contributions
(1) Conception and design: Long Tian.
(2) Administrative support: Guowei Che.
(3) Provision of study materials or patients: Mingming Wang.
(4) Collection and assembly of data: Xin Wang, Yutian Lai.
(5) Data analysis and interpretation: Rujun Zeng, Cheng Shen.
(6) Manuscript writing: Long Tian, Rujun Zeng.
(7) Final approval of manuscript: All authors.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the reviewers for their helpful comments on this paper.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
FUNDING
This study was supported by Foundation of Science and Technology support plan Department of Sichuan Province (2014SZ0148, 2015SZ0158).
REFERENCES
1. Robinson BW, Musk AW, Lake RA. Malignant mesothelioma. Lancet. 2005; 366: 397-408. doi: 10.1016/s0140-6736(05)67025-0.
2. Vogelzang NJ, Rusthoven JJ, Symanowski J, Denham C, Kaukel E, Ruffie P, Gatzemeier U, Boyer M, Emri S, Manegold C, Niyikiza C, Paoletti P. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol. 2003; 21: 2636-44. doi: 10.1200/jco.2003.11.136.
3. Chang K, Pastan I. Molecular cloning of mesothelin, a differentiation antigen present on mesothelium, mesotheliomas, and ovarian cancers. Proc Natl Acad Sci U S A. 1996; 93: 136-40. doi: 10.1073/pnas.93.1.136.
4. Sapede C, Gauvrit A, Barbieux I, Padieu M, Cellerin L, Sagan C, Scherpereel A, Dabouis G, Gregoire M. Aberrant splicing and protease involvement in mesothelin release from epithelioid mesothelioma cells. Cancer Sci. 2008; 99: 590-4. doi: 10.1111/j.1349-7006.2007.00715.x.
5. Hollevoet K, Reitsma JB, Creaney J, Grigoriu BD, Robinson BW, Scherpereel A, Cristaudo A, Pass HI, Nackaerts K, Rodriguez Portal JA, Schneider J, Muley T, Di Serio F, et al. Serum mesothelin for diagnosing malignant pleural mesothelioma: an individual patient data meta-analysis. J Clin Oncol. 2012; 30: 1541-9. doi: 10.1200/jco.2011.39.6671.
6. Cui A, Jin XG, Zhai K, Tong ZH, Shi HZ. Diagnostic values of soluble mesothelin-related peptides for malignant pleural mesothelioma: updated meta-analysis. BMJ Open. 2014; 4: e004145. doi: 10.1136/bmjopen-2013-004145.
7. Franko A, Dolzan V, Kovac V, Arneric N, Dodic-Fikfak M. Soluble mesothelin-related peptides levels in patients with malignant mesothelioma. Dis Markers. 2012; 32: 123-31. doi: 10.3233/dma-2011-0866.
8. Cristaudo A, Foddis R, Vivaldi A, Guglielmi G, Dipalma N, Filiberti R, Neri M, Ceppi M, Paganuzzi M, Ivaldi GP, Mencoboni M, Canessa PA, Ambrosino N, et al. Clinical significance of serum mesothelin in patients with mesothelioma and lung cancer. Clin Cancer Res. 2007; 13: 5076-81. doi: 10.1158/1078-0432.ccr-07-0629.
9. Grigoriu BD, Scherpereel A, Devos P, Chahine B, Letourneux M, Lebailly P, Gregoire M, Porte H, Copin MC, Lassalle P. Utility of osteopontin and serum mesothelin in malignant pleural mesothelioma diagnosis and prognosis assessment. Clin Cancer Res. 2007; 13: 2928-35. doi: 10.1158/1078-0432.ccr-06-2144.
10. Creaney J, Francis RJ, Dick IM, Musk AW, Robinson BW, Byrne MJ, Nowak AK. Serum soluble mesothelin concentrations in malignant pleural mesothelioma: relationship to tumor volume, clinical stage and changes in tumor burden. Clin Cancer Res. 2011; 17: 1181-9. doi: 10.1158/1078-0432.ccr-10-1929.
11. Dipalma N, Luisi V, Di Serio F, Fontana A, Maggiolini P, Licchelli B, Mera E, Bisceglia L, Galise I, Loizzi M, Pizzigallo MA, Molinini R, Vimercati L. Biomarkers in malignant mesothelioma: diagnostic and prognostic role of soluble mesothelin-related peptide. Int J Biol Markers. 2011; 26: 160-5. doi: 10.5301/jbm.2011.8614.
12. Schneider J, Hoffmann H, Dienemann H, Herth FJ, Meister M, Muley T. Diagnostic and prognostic value of soluble mesothelin-related proteins in patients with malignant pleural mesothelioma in comparison with benign asbestosis and lung cancer. J Thorac Oncol. 2008; 3: 1317-24. doi: 10.1097/JTO.0b013e318187491c.
13. Creaney J, Yeoman D, Naumoff LK, Hof M, Segal A, Musk AW, De Klerk N, Horick N, Skates SJ, Robinson BW. Soluble mesothelin in effusions: a useful tool for the diagnosis of malignant mesothelioma. Thorax. 2007; 62: 569-76. doi: 10.1136/thx.2006.068114.
14. Linch M, Gennatas S, Kazikin S, Iqbal J, Gunapala R, Priest K, Severn J, Norton A, Ayite B, Bhosle J, O’Brien M, Popat S. A serum mesothelin level is a prognostic indicator for patients with malignant mesothelioma in routine clinical practice. BMC Cancer. 2014; 14: 674. doi: 10.1186/1471-2407-14-674.
15. Creaney J, Dick IM, Meniawy TM, Leong SL, Leon JS, Demelker Y, Segal A, Musk AW, Lee YC, Skates SJ, Nowak AK, Robinson BW. Comparison of fibulin-3 and mesothelin as markers in malignant mesothelioma. Thorax. 2014; 69: 895-902. doi: 10.1136/thoraxjnl-2014-205205.
16. Yamada S, Tabata C, Tabata R, Fukuoka K, Nakano T. Clinical significance of pleural effusion mesothelin in malignant pleural mesothelioma. Clin Chem Lab Med. 2011; 49: 1721-6. doi: 10.1515/cclm.2011.242.
17. Hollevoet K, Nackaerts K, Gosselin R, De Wever W, Bosquee L, De Vuyst P, Germonpre P, Kellen E, Legrand C, Kishi Y, Delanghe JR, van Meerbeeck JP. Soluble mesothelin, megakaryocyte potentiating factor, and osteopontin as markers of patient response and outcome in mesothelioma. J Thorac Oncol. 2011; 6: 1930-7. doi: 10.1097/JTO.0b013e3182272294.
18. Hollevoet K, Nackaerts K, Thas O, Thimpont J, Germonpre P, De Vuyst P, Bosquee L, Legrand C, Kellen E, Kishi Y, Delanghe JR, van Meerbeeck JP. The effect of clinical covariates on the diagnostic and prognostic value of soluble mesothelin and megakaryocyte potentiating factor. Chest. 2012; 141: 477-84. doi: 10.1378/chest.11-0129.
19. Pass HI, Giroux D, Kennedy C, Ruffini E, Cangir AK, Rice D, Asamura H, Waller D, Edwards J, Weder W, Hoffmann H, van Meerbeeck JP, Rusch VW. Supplementary prognostic variables for pleural mesothelioma: a report from the IASLC staging committee. J Thorac Oncol. 2014; 9: 856-64. doi: 10.1097/jto.0000000000000181.
20. Nojiri S, Gemba K, Aoe K, Kato K, Yamaguchi T, Sato T, Kubota K, Kishimoto T. Survival and prognostic factors in malignant pleural mesothelioma: a retrospective study of 314 patients in the west part of Japan. Jpn J Clin Oncol. 2011; 41: 32-9. doi: 10.1093/jjco/hyq159.
21. Ceresoli GL, Grosso F, Zucali PA, Mencoboni M, Pasello G, Ripa C, Degiovanni D, Simonelli M, Bruzzone A, Dipietrantonj C, Piccolini E, Beretta GD, Favaretto AG, et al. Prognostic factors in elderly patients with malignant pleural mesothelioma: results of a multicenter survey. Br J Cancer. 2014; 111: 220-6. doi: 10.1038/bjc.2014.312.
22. Komurcuoglu B, Cirak AK, Kirakli SC, Polat G, Yucel N, Usluer O, Erer O, Balci G, Gayaf M, Guldaval F, Aktogu S, Guclu S, Ozsoz A, Halilcolar H. Prognostic factors affecting survival in malignant pleural mesothelioma: analysis of 125 subjects. Tumori. 2014; 100: 55-9. doi: 10.1700/1430.15816.
23. Kao SC, Vardy J, Chatfield M, Corte P, Pavlakis N, Clarke C, van Zandwijk N, Clarke S. Validation of prognostic factors in malignant pleural mesothelioma: a retrospective analysis of data from patients seeking compensation from the New South Wales Dust Diseases Board. Clin Lung Cancer. 2013; 14: 70-7. doi: 10.1016/j.cllc.2012.03.011.
24. Suzuki H, Hirashima T, Kobayashi M, Okamoto N, Matsuura Y, Tamiya M, Morishita N, Okafuji K, Shiroyama T, Morimura O, Morita S, Kawase I. Prognostic factors in malignant pleural mesothelioma: a retrospective study. Intern Med. 2012; 51: 707-10.
25. Ak G, Metintas S, Metintas M, Yildirim H, Erginel S, Kurt E, Alatas F, Cadirci O. Prognostic factors according to the treatment schedule in malignant pleural mesothelioma. J Thorac Oncol. 2009; 4: 1425-30. doi: 10.1097/JTO.0b013e3181ba2033.
26. Gonlugur U, Gonlugur TE. Prognostic factors for 100 patients with malignant pleural mesothelioma. Arch Environ Occup Health. 2010; 65: 65-9. doi: 10.1080/19338240903390271.
27. Al-Alao BS, Parissis H, Rychlik IJ, Graham A, McGuigan J. Prognostic factors in malignant pleural mesothelioma: role of talc pleurodesis. Asian Cardiovasc Thorac Ann. 2012; 20: 443-9. doi: 10.1177/0218492312449633.
28. Bonotti A, Simonini S, Pantani E, Giusti L, Donadio E, Mazzoni MR, Chella A, Marconi L, Ambrosino N, Lucchi M, Mussi A, Cristaudo A, Foddis R. Serum mesothelin, osteopontin and vimentin: useful markers for clinical monitoring of malignant pleural mesothelioma. Int J Biol Markers. 2016: 32: e126-31. doi: 10.5301/jbm.5000229.
29. Grigoriu BD, Chahine B, Vachani A, Gey T, Conti M, Sterman DH, Marchandise G, Porte H, Albelda SM, Scherpereel A. Kinetics of soluble mesothelin in patients with malignant pleural mesothelioma during treatment. Am J Respir Crit Care Med. 2009; 179: 950-4. doi: 10.1164/rccm.200807-1125OC.
30. Servais EL, Colovos C, Rodriguez L, Bograd AJ, Nitadori J, Sima C, Rusch VW, Sadelain M, Adusumilli PS. Mesothelin overexpression promotes mesothelioma cell invasion and MMP-9 secretion in an orthotopic mouse model and in epithelioid pleural mesothelioma patients. Clin Cancer Res. 2012; 18: 2478-89. doi: 10.1158/1078-0432.ccr-11-2614.
31. Tang Z, Qian M, Ho M. The role of mesothelin in tumor progression and targeted therapy. Anticancer Agents Med Chem. 2013; 13: 276-80.
32. Wang K, Bodempudi V, Liu Z, Borrego-Diaz E, Yamoutpoor F, Meyer A, Woo RA, Pan W, Dudek AZ, Olyaee MS, Esfandyari T, Farassati F. Inhibition of mesothelin as a novel strategy for targeting cancer cells. PLoS One. 2012; 7: e33214. doi: 10.1371/journal.pone.0033214.
33. Hassan R, Sharon E, Thomas A, Zhang J, Ling A, Miettinen M, Kreitman RJ, Steinberg SM, Hollevoet K, Pastan I. Phase 1 study of the antimesothelin immunotoxin SS1P in combination with pemetrexed and cisplatin for front-line therapy of pleural mesothelioma and correlation of tumor response with serum mesothelin, megakaryocyte potentiating factor, and cancer antigen 125. Cancer. 2014; 120: 3311-9. doi: 10.1002/cncr.28875.
34. Zhang J, Khanna S, Jiang Q, Alewine C, Miettinen M, Pastan I, Hassan R. Efficacy of anti-mesothelin immunotoxin RG7787 plus nab-paclitaxel against mesothelioma patient derived xenografts and mesothelin as a biomarker of tumor response. Clin Cancer Res. 2016. doi: 10.1158/1078-0432.ccr-16-1667.
35. Reck M, Hassan R, Jahan T, Kindler HL, Bazhenova L, Fatato P, Heyburn JW, Parno J, Maltzman JD, Wallin B. A multi-center phase II clinical trial of the chimeric anti-mesothelin monoclonal antibody amatuximab in combination with chemotherapy for frontline therapy of malignant pleural mesothelioma: updated clinical outcomes and correlative studies. Ann Oncol. 2012; 23: ix493. doi.org/10.1093/annonc/mds415.
36. Hassan R, Kindler HL, Jahan T, Bazhenova L, Reck M, Thomas A, Pastan I, Parno J, O’Shannessy DJ, Fatato P, Maltzman JD, Wallin BA. Phase II clinical trial of amatuximab, a chimeric antimesothelin antibody with pemetrexed and cisplatin in advanced unresectable pleural mesothelioma. Clin Cancer Res. 2014; 20: 5927-36. doi: 10.1158/1078-0432.ccr-14-0804.
37. Gupta A, Hussein Z, Hassan R, Wustner J, Maltzman JD, Wallin BA. Population pharmacokinetics and exposure-response relationship of amatuximab, an anti-mesothelin monoclonal antibody, in patients with malignant pleural mesothelioma and its application in dose selection. Cancer Chemother Pharmacol. 2016; 77: 733-43. doi: 10.1007/s00280-016-2984-z.
38. Melaiu O, Stebbing J, Lombardo Y, Bracci E, Uehara N, Bonotti A, Cristaudo A, Foddis R, Mutti L, Barale R, Gemignani F, Giamas G, Landi S. MSLN gene silencing has an anti-malignant effect on cell lines overexpressing mesothelin deriving from malignant pleural mesothelioma. PLoS One. 2014; 9: e85935. doi: 10.1371/journal.pone.0085935.
39. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010; 8: 336-41. doi: 10.1016/j.ijsu.2010.02.007.
40. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007; 8: 16. doi: 10.1186/1745-6215-8-16.
41. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010; 25: 603-5. doi: 10.1007/s10654-010-9491-z.
42. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002; 21: 1539-58. doi: 10.1002/sim.1186.
43. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327: 557-60. doi: 10.1136/bmj.327.7414.557.
44. Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000; 56: 455-63.