
INTRODUCTION
Papillary thyroid carcinoma (PTC) is the most common thyroid malignancy in adults, the incidence of which has been soaring in recent decades [1–3]. Over the past 20 years, new discoveries in the pathogenesis of PTC have given insight into better diagnostic, prognostic, and therapeutic procedures for patients with thyroid cancer [2, 4, 5]. Previous genetic studies have reported point mutations of the BRAF and the RAS genes, as well as fusions involving the RET and NTRK1 tyrosine kinases [6]. More recently, Integrated Genomic Characterization of PTC by the Cancer Genome Atlas (TCGA) project reduced the proportion of PTC cases with unknown oncogenic driver from 25% to 3.5% [7]. Nearly all of these driver mutations are mutually exclusive thus accounting for the classification of PTC in several genetically defined subgroups. Therefore,understanding genetic lesions is necessary for elucidating distinct clinicopathological characteristics,such as clonal evolution, risk stratification, and therapeutic targets.
With the advent of next-generation sequencing (NGS), a more complete biological characterization of a tumor can be attained at the molecular level by allowing simultaneous analysis of large regions of the genome, and offering high-sensitivity detection of mutations, and quantitative assessment of mutant alleles [8, 9]. Recently, molecular genetics of PTC have been studied on a different scale including whole-genome sequencing, whole-exome sequencing, and whole-transcriptome sequencing [7, 9]. These methodologies are complementary to each other and are essential for genetic discovery projects. Further, targeted sequencing of multiple specific genomic regions may offer an easier and less expensive alternative strategy in routine molecular diagnostics of cancer allowing a more detailed cancer genetic lesions to be obtained [10, 11].
In the present study, we developed a targeted, massively paralleled sequencing assay for 244 cancer-related genes and 20 fusion genes by a homebred Thyroid Cancer Panel (ThyGenCapTM panel),designed as a comprehensive diagnostic test for mutations and gene rearrangements of PTC in an efficient and cost-effective manner. Our assay has allowed improvements on earlier approaches, most importantly by expanding the spectrum of mutations and including complex genomic rearrangements that are potentially detectable by the assay [9, 12].
RESULTS
Quality assessment of the targeted sequencing data
Patient characteristics are described in Supplementary Table 1. Paired specimens of PTC and matched blood samples were used for analysis. The mean value of raw variant coverage was 18489435 reads for each sample, and the variant coverage ranged from 1354085 to 84293424 reads. On average 97.58% of all reads could be mapped back to the genome and 60.48% of all reads were mapped to our designed target regions (43.89%-73.89%). This indicated a high capture efficiency of the probes. The mean read length was 150 base pairs and the mean coverage of the 138 samples analyzed was 288×(124×-928×).
Somatic mutations in PTC
The number of mutated genes per tumor was 1.39 (range 0–4). Overall, 203 somatic mutations including 181 SNVs (1 splicing, 3 stopgain, and 177 nonsynonymous), 17 deletions, and 4 insertions in 77 genes were identified in the PTC samples. Somatic mutations with mutant allele frequency greater than 10% were all confirmed by Sanger sequencing. Point mutations were most frequently observed in BRAF (80 mutations in 138 patients,58.0%), BRAF V600E mutation accounted for all the affected cases except for one case that showed BRAF V601K. The mutational frequency of other mutations was lower than 5%. A list of the genes that occurred in at least 2 PTC patients is shown in Figure 1. The majority of the tumors (95/138, 68.8%) harbored at least one driver-gene mutation (Supplementary Table 3), 57.2% (79/138) showed concurrent mutations in two or more genes (Figure 1 and Supplementary Table 3), and 24 (18.16%) tumors showed no somatic mutation in the 244 genes analyzed.
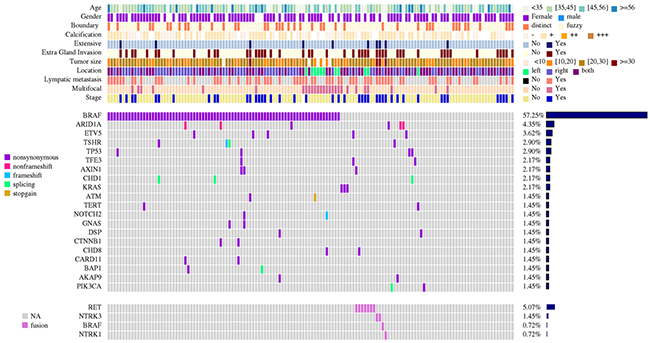
Figure 1: Detailed description of mutation and gene rearrangement landscape of 138 cases of papillary thyroid carcinoma. Genes mutated in two or more cases are listed vertically in decreasing order of prevalence. Colored rectangles indicate mutation categories observed in a given gene and tumor. Results of gene rearrangement analysis are shown in the bottom panel. Patient demographics as well as tumor classifications and molecular features, such as age, gender, boundary, calcification, extensive metastasis, extragland invasion, and lymphatic metastasis, are indicated in the boxes on the right.
Detection and validation of fusion genes
We identified both known and novel fusions, i.e. new partners of previously described fusions, in 11 (7.97 %) of the 138 informative cases (Table 1 and Figure 2). Among them, UEVLD-RET, OSBPL9-BRAF and SQSTM1-NTRK3 were three novel fusion genes. RET fusions were the most frequent (7/138, 4.35%), including three previously reported partners and one novel unique RET fusions (Table 1 and Figure 2). Sequencing analysis of the PCR products confirmed the presence of fused genes on DNA and transcription level in the corresponding tumors; an example for UEVLD-RET fusion gene is shown in Figure 2B. Finally, the presence of the fusion between these two genes was confirmed by two-color FISH using probes corresponding to 5’ and 3’ of the breakpoints. Figure 2C showed the representative validation by FISH involving threenovel candidate fusion genes UEVLD-RET, OSBPL9-BRAF and SQSTM1-NTRK3.
Table 1: Fusion genes identified from 138 PTC
Patient |
Gender |
Age |
Gene fusion |
Novel or |
DNA |
RNA |
FISH |
Reference |
|---|---|---|---|---|---|---|---|---|
14 |
Female |
47 |
SPECC1L-RET |
No |
Yes |
Yes |
Yes |
25 |
76 |
Male |
30 |
UEVLD-RET |
Yes |
Yes |
Yes |
Yes |
NEW |
94 |
Female |
51 |
CCDC6-RET |
No |
Yes |
Yes |
Yes |
20 |
130 |
Male |
40 |
CCDC6-RET |
No |
Yes |
Yes |
Yes |
20 |
98 |
Female |
52 |
CCDC6-RET |
No |
Yes |
Yes |
Yes |
20 |
125 |
Male |
40 |
CCDC6-RET |
No |
Yes |
Yes |
Yes |
20 |
124 |
Female |
29 |
CCDC186-RET |
No |
Yes |
Yes |
Yes |
23 |
138 |
Male |
19 |
IRF2BP2-NTRK1 |
No |
Yes |
ND |
Yes |
22 |
135 |
Female |
37 |
SQSTM1-NTRK3 |
Yes |
Yes |
ND |
Yes |
NEW |
133 |
Female |
44 |
EML4-NTRK3 |
No |
Yes |
ND |
Yes |
21 |
89 |
Male |
25 |
OSBPL9-BRAF |
Yes |
Yes |
Yes |
Yes |
NEW |
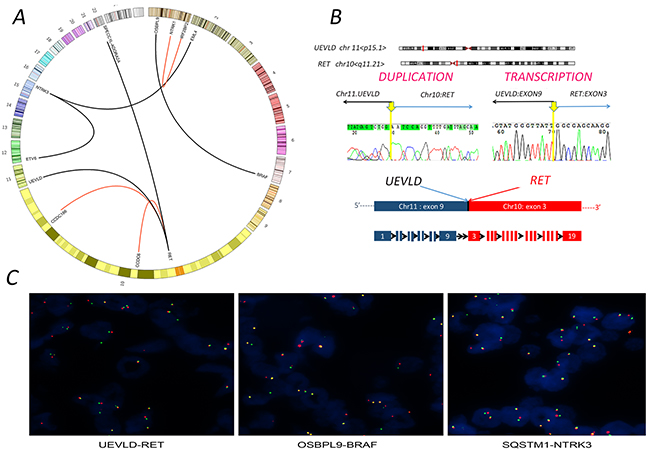
Figure 2: Gene fusions identified from papillary thyroid carcinoma (PTC) cases. (A) Circos plot of eleven fusion genes in tracks with chromosomes circularly arranged. The corresponding genes are labeled inside the circus. Red lines represent novel fusion genes, and black lines represent already reported ones. (B) Validation of novel candidate fusion genes UEVLD-RET by fusion-specific DNA and RNA sequencing. Chromosomal ideograms show UEVLD-RET gene fusions between UEVLD (chr.11 p15.1) and RET (chr.10 q11.21). Sanger sequencing chromatograms show breakpoint regions on gene-level with exact single-base resolution fusion point indicated (Hg19 coordinates) and confirmation of the in-frame fusion of UEVLD (exon 9) and RET (exon 3) by fusion-specific transcription. The arrowheads indicate RET fusion points between UEVLD and RET gene sequences and the genomic coordinates of the RNA fusion junction localized at Chr11:18541431/Chr1043101044. Each gene in the fusion plot is drawn 5’ to 3’. The breakpoints of RET are exons 3, which allow the fusion to harbor the kinase domain of RET. Predicted chimeric protein structure of rearrangements inferred from genomic and transcription data are displayed under electropherograms. (C) Three novel fusions, UEVLD-RET, OSBPL9-BRAF, and SQSTM1-NTRK3, validated by break-apart fluorescence in situ hybridization (FISH) assay. FISH reveals separations of the 5’ probe (red) from the 3’ probe (green) signals. The yellow signal indicating of a rearrangement in tumor cells.
Correlation between MAPK pathway, BRAF, and fusion genes and clinicalpathological characteristics
We observed that 69.6% of the PTC cases had genetic alterations leading to constitutive activation of the MAPK pathway, including point mutations of BRAF (80, 58.0%),KRAS genes and HRAS genes (4, 2.9%), RET genes (1, 0.7%), as well as gene fusions involving the RET (7, 5.1%), BRAF (1, 0.7%), and NTRK1 and NTRK3 tyrosine kinases (3, 2.2%) (Figure 3). These mutations were almost mutually exclusive, suggesting that activation of a single effector of this pathway is sufficient for cell transformation. We further analyzed the correlation between MAPK pathway alteration and the clinicopathological features of PTC. As shown in Table 2, MAPK pathway alteration was significantly associated with advanced tumor stage III/IV (P<0.05). Interestingly, the fusion genes were strongly associated with distinct clinicopathological characteristics, including younger age at diagnosis (P=0.013), extensive metastasis (P=0.025), local invasion (P=0.048), large tumor size (P=0.003), and disease stage (P=0.035) (Table 2).
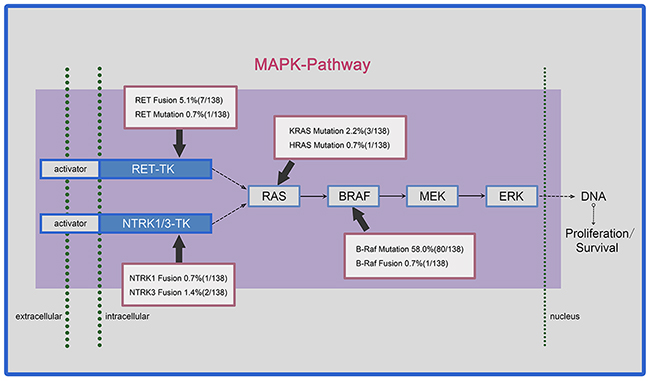
Figure 3: Prevalence of somatic mutations and chromosomal rearrangements in papillary thyroid carcinoma (PTC) affecting the MAPK pathway. The MAPK pathway is driven by activating mutations, including RET, BRAF and RAS mutations; and gene arrangements, including the RET gene, the NTRK1/3 gene, and the BRAF gene. Both ways of alterations constitutively activate the downstream components of the MAPK pathway, resulting in multiple responses at the transcriptional level and leading to the expression of factors promoting cell proliferation and survival.
Table 2: MAPK pathway, BRAF and fusion genes analysis with clinicopathology indexes
Variables |
MAPK pathwaya |
Fusion genesc |
BRAF mutationd |
P valuesb |
|||||
|---|---|---|---|---|---|---|---|---|---|
YES |
NO |
P valuesb |
YES |
NO |
P valuesb |
YES |
NO |
||
Total |
96 |
42 |
11 |
127 |
80 |
58 |
|||
Gender |
0.393 |
0.139 |
0.844 |
||||||
Male |
26 |
8 |
5 |
29 |
19 |
15 |
|||
Female |
70 |
34 |
6 |
98 |
61 |
43 |
|||
Age(years) |
0.872 |
0.013 |
0.055 |
||||||
≤30 |
9 |
5 |
4 |
10 |
5 |
9 |
|||
>30 |
86 |
38 |
7 |
117 |
75 |
49 |
|||
Lymphatic metastasis |
0.137 |
0.112 |
0.733 |
||||||
Metastasis |
49 |
15 |
10 |
54 |
37 |
27 |
|||
Non-metastasis |
47 |
27 |
1 |
73 |
43 |
31 |
|||
Extensive metastasise |
0.276 |
0.025 |
0.648 |
||||||
Non-extensive |
88 |
41 |
8 |
121 |
75 |
54 |
|||
Extensive |
8 |
1 |
3 |
6 |
5 |
4 |
|||
Extraglandular invasionf |
0.177 |
0.048 |
0.870 |
||||||
Non-invasion |
58 |
31 |
4 |
86 |
54 |
36 |
|||
Invasion |
37 |
11 |
7 |
41 |
26 |
22 |
|||
Borderg |
0.842 |
0.172 |
0.513 |
||||||
Clearance |
28 |
14 |
1 |
42 |
27 |
16 |
|||
Obscure |
67 |
28 |
10 |
85 |
53 |
42 |
|||
Tumor size(mm) |
0.258 |
0.003 |
0.673 |
||||||
≤10 |
35 |
22 |
0 |
55 |
32 |
23 |
|||
>10 |
61 |
20 |
11 |
72 |
48 |
35 |
|||
Calcificationg |
0.2 |
0.71 |
0.181 |
||||||
Non-calcification |
16 |
15 |
3 |
28 |
14 |
17 |
|||
Calcification |
79 |
28 |
8 |
99 |
66 |
41 |
|||
Multifocal or unifocalh |
0.358 |
0.45 |
0.79 |
||||||
Unifocal |
75 |
36 |
8 |
103 |
63 |
48 |
|||
Multifocal |
21 |
6 |
3 |
24 |
17 |
10 |
|||
Stage |
0.047 |
0.035 |
0.629 |
||||||
Stage I,II |
61 |
34 |
4 |
91 |
53 |
43 |
|||
Stage III,IV |
35 |
8 |
7 |
36 |
27 |
15 |
|||
a MAPK pathway concludes BRAF mutation(for example, BRAF V600E), any fusion genes detected of MAPK pathways and RAS, RET mutation.
b P values derived from Fisher exact test.
c Any fusion genes detected = yes.
d BRAF mutation (for example, BRAF V600E) detected
e Extensive metastasis referred to extensive lymphatic metastasis of neck nodes (for instance, II, III, IV and V region).
f Border observed under ultrasound was classified into clear and obscure ones.
g Calcification observed under ultrasound.
h Multifocal = multi primary foci of papillary thyroid cancer.
DISCUSSION
In this study, we carried a targeted massively paralleled sequencing assay in a large series of PTC cases. Being cost-efficient, significantly sensitive and accurate, ThyGenCapTM is a promising tool for better understanding thyroid carcinogenesis and clinical genotyping of PTC.
The occurrence of BRAF mutations was 58% (80/138) and it ranked as the highest mutational frequency. Most other mutational frequencies were lower than 5%, consistent with the low mutation frequency found in PTC as reported previously [7]. Chromosomal rearrangements and translocations are the common feature ofPTC and contribute to its pathogenesis. We identified both known and novel fusions in 11 (7.8%) of the 138 informative cases. This is a little lower than what was found in a recent multiple platform analysis of 484 cases (15.3%) [7].
In accordance with previous reports, the most common chromosomal rearrangements involve the RETprotooncogene, as well as NTRK3,NTRK1, and BRAF genes, although with a significantly lower prevalence [14–17]. Since the identification of the first RET partner in a chromosomal rearrangement in 1990 [14], at least 25 different 5’-fusion partner genes of RET have been described so far, with CCDC6–RET (also known for historical reasons as RET/PTC1) being the most common [17]. Remarkably, all breakpoints of the already known RET rearrangements occurred within intron 11 or occasionally in intron 10 [17, 18]. Of possible interest is the fact that UEVLD-RET in this study, unlike the majority of RET rearrangements, occurred in intron 2 of RET, resulting in longer rearrangements than the most common RET rearrangements.
The prevalence of fusion genes in PTC was more frequent in patients who had been diagnosed at a young age and showed a tendency toward a more malignant behavior of PTC [17, 19]. This at least in part explained the fact that younger patients commonly have clinically more advanced disease at presentation with extensive lymph node metastasis and, sometimes, distant metastasis [20, 21]. In our study, we did not find any relationship between BRAF mutation and aggressive histopathological or clinical characteristics of PTC. However, results from other laboratories indicated that BRAF mutation, as well as the MAPK pathway were associated with worse prognosis [6], although the association of BRAF V600E with more aggressive clinicopathologic features and worse outcome has been under debate [22–24]. The discrepancies may be attributed to methodological differences, tumors from different geographical areas, different PTC variants, and tumor heterogeneity [25]. A large multicenter study with all centers using the same methodology should resolve this issue.
Notably, it has been previously reported that TERT promoter mutation is infrequent in PTC but has been identified as an indicator of the worst prognosis of PTC [26]. Although we only detected 2 samples harboring this mutation, both cases suffered from lymph node metastasis recurrence in less than 2 years after total thyroidectomy with lymph node dissection. Remarkably, TERT and BRAF mutations were coexistent in both patients. Seemingly, either TERT alone or the synergistic effect of the two mutations affected the clinical outcome. Our observation supported the recent report that the concomitance of TERT and BRAF mutations was significantly associated with poorer clinicopathological features [27–29]. Nevertheless, the number of patients included in our subgroups was too limited to draw a definitive conclusion.
Another promising application to improve efficacy of therapy is to pursue a mutational-profile-guided targeted therapy for aggressive and metastatic PTC. The knowledge of alterations in the MAPK pathway, such as RET/PTC rearrangements and BRAF mutations, will provide oportunities for clinical development of novel treatment strategies for this cancer. Among the new therapeutic approaches, the most promising compounds have been the BRAF inhibitors (i.e., vemurafenib) [4, 30] and RET-kinase inhibitors (i.e., vandetanib) [31]. Clinical trials for additional agents directed against specific genes or mutations are currently underway and are expected to progressively increase the repertoire of available targeted therapies for cancer [32].
In summary, targeted sequencing assay permits the detection of a large panel of genomic mutations, from point mutations to structural rearrangements. The detection is very sensitive even in the context of tumor heterogeneity or sample impurity as they could be overcome by in-depth sequencing. Further, this approach will prove to be valuable as a discovery tool enabling development of new therapeutic agents or providing prognostic information. Therefore, the Thyroid Cancer Panel method is cost-effective and robust enough to be integrated into routine clinical care for PTC.
MATERIALS AND METHODS
Patient and clinicopathological data collection
We carried out a retrospective, single-center study including 138 patients with PTC who were treated with total thyroidectomy between 2012 and 2014 at Beijing Cancer Hospital. This study received ethical approval from the Institutional Review Board of the Peking University School of Oncology, China, and the study was carried out in accordance with approved guidelines. Blood samples from each patient were paired with the tumor samples and served as normal controls to discriminate somatic mutations from germline variations. We retrospectively reviewed the clinical records of these patients. Experienced pathologists made histological diagnosis based on specimens stained with hematoxylin and eosin. Demographic and clinicopathological data of these 138 patients with PTC were summarized in Supplementary Table 1.
Detection of point mutations and gene fusions by ThyGenCapTM panel
A ThyGenCapTM panel was designed to target 244 cancer-related genes and 20 genes often rearranged in thyroid carcinoma. Details of the genes are provided in Supplementary Table 2. Gene sets were selected based on search results of the literature, the COSMIC database, and the TCGA database.
The amplified DNA was captured by GenCapTM Technologyfrom MyGenostics(Beijing, China). For 244 cancer-related genes, the DNA probes were designed to tile along the exon regions of the target genes, as well as the two most common mutations in TERTpromoter, C228T and C250T,upstream of the TERT ATG site. For 20 genes often rearranged in thyroid carcinoma,the DNA probes were covered whole potential rearranged gene, including introns. The capture experiment was conducted according to manufacturer’s protocol. The whole-genomic libraries were hybridized with these probes, adsorbed onto the beads via biotin and streptavidin magnetic beads, and the uncaptured DNA fragments were removed by washing. Then the eluted fragments containing the target genes were enriched by 18 cycles of PCR to generate libraries for sequencing. Libraries were quantified and sequenced for paired-end 100bp using the Illumina HiSeq 2000 sequencer (Illumina Inc., San Diego, CA, USA). The Illumina clean reads were mapped to human genome (GRCh37/hg19) using the BWA program. The paired-end read, uniquely mapped with one end to a target gene and the other to another target gene, is identified as a discordant read pair. If a specific position has three or more discordant read pairs, it would be considered as a potential fusion site. The fusion sites were annotated according to human genome (GRCh37/hg19) from the UCSC database.
Only those mutations that had an allele frequency ≥5% were scored as positive for the mutation. All variants identified by next-generation sequencing with mutant allele frequency greater than 10% were validated by Sanger sequencing. For gene rearrangements, the presence of at least 3 high-quality reads spanning the fusion point of the two split genes confirmed by PCR and Sanger sequencing was required to consider the sample positive for the rearrangement.
Verification and validation of fusion genes by Sanger sequencing
According to the 5’ and 3’ sequences flanking the breakpoints, respectively,we traced its position on chromosome via UCSC genome and then as a sequence to design proper primers. PCR and Sanger sequencing confirmed the spliced sites.
Furthermore, after breakpoints were validated on DNA level, exons were put together by prediction according to exons spanning the breakpoints. RNA was extracted from tissues and followed by RT-PCR. Specific primers for each fusion gene were designed according to exons put together flanking the breakpoints, respectively. RNA sequences spanning two disparate genes and where the coding frame was predicted were to be maintained in the fusion transcript.
Fusion gene break-apart fluorescence in situ hybridization (FISH) assay
FISH was done on formalin-fixed and paraffin-embedded tumor tissues using probes encompassing the genomic region of all potential gene rearrangement loci (Supplementary Figure 1). The probes used in this study were purchased from Jin Lu Biotechnology Co., Ltd, Shaoxing, China), and the probe clones were from C.H.O.R.I., Children´s Hospital, Oakland Research Institute). Labeling with fluorescein using Nick Translation Kit were purchased from Abbott Molecular, Abbott Park, IL, USA). FISH-positive cases were defined as >15% tumor cells showing classic split signals as previously described [13].
Statistical analysis
Clinicalpathological characteristics associated with mitogen-activated protein kinase (MAPK) pathway alteration, BRAF mutations and fusion genes were evaluated using Pearson's chi-square test or Fisher's exact test. Statistical analysis was conducted using SPSS version 13.0 (SPSS, Chicago, IL, USA). All statistical tests were two-sided at the 0.05 significance level.
Author contributions
Conception and design: Z. Lu, W. Yang, B. Liu; Development of methodology: Z. Lu, Y. Zhang; Acquisition of data: Y. Zhang, D. Feng, J. Sheng; Analysis and interpretation of data: Z. Lu, Y. Zhang; Writing, review, and/or revision of the manuscript: Z. Lu, Y. Zhang, W. Yang; Clinical or sample support: Y. Zhang, D. Feng, J. Sheng, B. Liu; Study supervision: Z. Lu.
CONFLICTS OF INTEREST
The authors declare no competing financial interests.
GRANT SUPPORT
This work was supported by Beijing Natural Science Foundation (Grant No 7171001 to ZL); Beijing Municipal Science & Technology Commission (Grant No Z171100001017136 to ZL); Natural Science Foundation of China (Grant No 81441078 to ZL; Grant No 81672649 to BL).
REFERENCES
1. McLeod DS, Sawka AM, Cooper DS. Controversies in primary treatment of low-risk papillary thyroid cancer. Lancet. 2013; 381:1046-1057.
2. Jung CK, Little MP, Lubin JH, Brenner AV, Wells SA, Sigurdson AJ, Nikiforov YE. The increase in thyroid cancer incidence during the last four decades is accompanied by a high frequency of BRAF mutations and a sharp increase in RAS mutations. J Clin Endocrinol Metab. 2014; 99:E276-E285.
3. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014; 64:9-29.
4. Cabanillas ME, Dadu R, Hu MI, Lu C, Gunn GB, Grubbs EG, Lai SY, Williams MD. Thyroid gland malignancies. Hematol Oncol Clin North Am. 2015; 29:1123-1143.
5. Viola D, Valerio L, Molinaro E, Agate L, Bottici V, Biagini A, Lorusso L, Cappagli V, Pieruzzi L, Giani C, Sabini E, Passannati P, Puleo L, et al. Treatment of advanced thyroid cancer with targeted therapies: ten years of experience. Endocr Relat Cancer. 2016; 23:R185-205.
6. Xing M. Molecular pathogenesis and mechanisms of thyroid cancer. Nat Rev Cancer. 2013; 13:184-199.
7. Cancer Genome Atlas Research Network. Integrated genomic characterization of papillary thyroid carcinoma. Cell. 2014; 159:676-690.
8. Nikiforova MN, Wald AI, Roy S, Durso MB, Nikiforov YE. Targeted next-generation sequencing panel (ThyroSeq) for detection of mutations in thyroid cancer. J Clin Endocrinol Metab. 2013; 98:E1852-1860.
9. Nikiforov YE, Carty SE, Chiosea SI, Coyne C, Duvvuri U, Ferris RL, Gooding WE, LeBeau SO, Ohori NP, Seethala RR, Tublin ME, Yip L, Nikiforova MN. Impact of the multi-gene ThyroSeq next-generation sequencing assay on cancer diagnosis in thyroid nodules with atypia of undetermined significance/follicular lesion of undetermined significance cytology. Thyroid. 2015; 25:1217-1223.
10. Mukherjee S, Ma Z, Wheeler S, Sathanoori M, Coldren C, Prescott JL, Kozyr N, Bouzyk M, Correll M, Ho H, Chandra PK, Lennon PA. Chromosomal microarray provides enhanced targetable gene aberration detection when paired with next generation sequencing panel in profiling lung and colorectal tumors. Cancer Genet. 2016; 209:119-129.
11. Joosten SE, Retel VP, Coupe VM, van den Heuvel MM, van Harten WH. Scenario drafting for early technology assessment of next generation sequencing in clinical oncology. BMC Cancer. 2015; 16:66.
12. Nikiforov YE, Carty SE, Chiosea SI, Coyne C, Duvvuri U, Ferris RL, Gooding WE, Hodak SP, LeBeau SO, Ohori NP, Seethala RR, Tublin ME, Yip L, Nikiforova MN. Highly accurate diagnosis of cancer in thyroid nodules with follicular neoplasm/suspicious for a follicular neoplasm cytology by ThyroSeq v2 next-generation sequencing assay. Cancer. 2014; 120:3627-3634.
13. Lindeman NI, Cagle PT, Beasley MB, Chitale DA, Dacic S, Giaccone G, Jenkins RB, Kwiatkowski DJ, Saldivar JS, Squire J, Thunnissen E, Ladanyi M; College of American Pathologists International Association for the Study of Lung Cancer and Association for Molecular Pathology. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Mol Diagn. 2013; 15:415-453.
14. Grieco M, Santoro M, Berlingieri MT, Melillo RM, Donghi R, Bongarzone I, Pierotti MA, Della Porta G, Fusco A, Vecchio G. PTC is a novel rearranged form of the ret proto-oncogene and is frequently detected in vivo in human thyroid papillary carcinomas. Cell. 1990; 60:557-563.
15. Pfarr N, Stenzinger A, Penzel R, Warth A, Dienemann H, Schirmacher P, Weichert W, Endris V. High-throughput diagnostic profiling of clinically actionable gene fusions in lung cancer. Genes Chromosomes Cancer. 2016; 55:30-44.
16. Lu Z, Sheng J, Zhang Y, Deng J, Li Y, Lu A, Zhang J, Yu H, Zhang M, Xiong Z, Yan H, Diplas BH, Lu Y, Liu B. Clonality analysis of multifocal papillary thyroid carcinoma by using genetic profiles. J Pathol. 2016; 239:72-83.
17. Romei C, Ciampi R, Elisei R. A comprehensive overview of the role of the RET proto-oncogene in thyroid carcinoma. Nat Rev Endocrinol. 2016; 12:192-202.
18. Tsai TH, Wu SG, Hsieh MS, Yu CJ, Yang JC, Shih JY. Clinical and prognostic implications of RET rearrangements in metastatic lung adenocarcinoma patients with malignant pleural effusion. Lung Cancer. 2015; 88:208-214.
19. Prensner JR, Chinnaiyan AM. Oncogenic gene fusions in epithelial carcinomas. Curr Opin Genet Dev. 2009; 19:82-91.
20. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985-1995. Cancer. 1998; 83:2638-2648.
21. Mitelman F, Johansson B, Mertens F. The impact of translocations and gene fusions on cancer causation. Nat Rev Cancer. 2007; 7:233-245.
22. Xing M. Prognostic utility of BRAF mutation in papillary thyroid cancer. Mol Cell Endocrinol. 2010; 321:86-93.
23. Gandolfi G, Sancisi V, Piana S, Ciarrocchi A. Time to re-consider the meaning of BRAF V600E mutation in papillary thyroid carcinoma. Int J Cancer. 2015; 137:1001-1011.
24. Li F, Chen G, Sheng C, Gusdon AM, Huang Y, Lv Z, Xu H, Xing M, Qu S. BRAFV600E mutation in papillary thyroid microcarcinoma: a meta-analysis. Endocr Relat Cancer. 2015; 22:159-168.
25. Almendro V, Marusyk A, Polyak K. Cellular heterogeneity and molecular evolution in cancer. Ann Rev Pathol. 2013; 8:277-302.
26. Vinagre J, Almeida A, Populo H, Batista R, Lyra J, Pinto V, Coelho R, Celestino R, Prazeres H, Lima L, Melo M, da Rocha AG, Preto A, et al. Frequency of TERT promoter mutations in human cancers. Nat Commun. 2013; 4:2185.
27. Liu R, Xing M. TERT promoter mutations in thyroid cancer. Endocr Relat Cancer. 2016; 23:R143-155.
28. Xing M, Liu R, Liu X, Murugan AK, Zhu G, Zeiger MA, Pai S, Bishop J. BRAF V600E and TERT promoter mutations cooperatively identify the most aggressive papillary thyroid cancer with highest recurrence. J Clin Oncol. 2014; 32:2718-2726.
29. Liu X, Bishop J, Shan Y, Pai S, Liu D, Murugan AK, Sun H, El-Naggar AK, Xing M. Highly prevalent TERT promoter mutations in aggressive thyroid cancers. Endocr Relat Cancer. 2013; 20:603-610.
30. Pyo JS, Kang G, Kim DH, Chae SW, Park C, Kim K, Do SI, Lee HJ, Kim JH, Sohn JH. Activation of nuclear factor-kappaB contributes to growth and aggressiveness of papillary thyroid carcinoma. Pathol Res Pract. 2013; 209:228-232.
31. Leboulleux S, Bastholt L, Krause T, de la Fouchardiere C, Tennvall J, Awada A, Gomez JM, Bonichon F, Leenhardt L, Soufflet C, Licour M, Schlumberger MJ. Vandetanib in locally advanced or metastatic differentiated thyroid cancer: a randomised, double-blind, phase 2 trial. Lancet Oncol. 2012; 13:897-905.
32. Bible KC, Ryder M. Mutated BRAF and personalised medicine in differentiated thyroid cancer. Lancet Oncol. 2016; 17:1181-1183.