
INTRODUCTION
Hepatocellular carcinoma (HCC) was the fourth leading cause of global cancer deaths in 2012 [1-3]. Depending on the extent of the disease and the underlying liver status, patients may be treated with local, locoregional, and/or systemic therapy. Several clinical trials have indicated that radiotherapy (RT) can play a meaningful role in the management of HCC [4-8]. Although there is no high level evidence from randomized controlled trial, the efficacy and safety of RT in HCC has been shown by several prospective or retrospective trials using modern RT techniques, especially in Asia-Pacific, where have higher incidence of HCC than other areas [9, 10]. In the 5th Asia-Pacific Primary Liver Cancer Expert Meeting (APPLE 2014), a consensus on the utility and efficacy of RT in the treatment of HCC according to different cancer stage have been made: in early and intermediate stage HCC, if standard treatment is not compatible, RT, including EBRT and SIRT can be considered. In locally advanced stage HCC, combined EBRT with transarterial chemoembolization or hepatic arterial infusion chemotherapy, and SIRT can be considered [9].
The goals of cancer staging are to predict prognosis and to provide therapeutic guidelines; they are also useful to stratify patients enrolled in clinical trials. A variety of new HCC staging systems are emerging. There are currently 10 different staging systems relevant to HCC. These include the Okuda staging system [11], Cancer of the Liver Italian Program (CLIP) prognostic score [12, 13], Barcelona Clinic Liver Cancer (BCLC) classification system [14], France staging system [15], Chinese University Prognostic Index (CUPI) [16], Japan Integrated Staging (JIS) score [17], American Joint Committee on Cancer (AJCC) 1997 Tumor-Node-Metastasis (TNM) staging system [18], AJCC 2002 TNM staging system [19], AJCC 2010 TNM staging system [20] and the Chinese Guangzhou 2001 staging system [21]. No other single cancer has such a large number of proposed staging systems, which reflects a general sense that the current HCC staging systems are less than satisfactory. Furthermore, there are even more newly proposed staging systems for HCC patients.
However, few staging systems are based on radiotherapy. To date, only Jensen Seong et al. have addressed this [22]. Most existing staging systems are proposed based on surgery rather than radiotherapy. Therefore, the purpose of our study was to assess the validity of the 10 staging systems in HCC patients receiving radiotherapy in our cohort.
RESULTS
Baseline characteristics and 249 HCC patient distribution by staging system
A total of 249 patients were included in the analyses; their performance status and liver function are shown in Table 1. The patients’ disease classifications based on different cancer staging systems are shown in Table 2. More than 50% of patients were classified as Okuda stage I, BCLC stage C, France stage B, CUPI low-risk group, JIS score 1, AJCC 1997 TNM staging system stage T1, AJCC 2002 TNM staging system stage T1, AJCC 2010 TNM staging system stage T1 and Guangzhou 2001 stage II. No patient was classified as CLIP score 5, France stage C, JIS score 0, 4, 5. According to the Okuda staging and CUPI, 95% of patients were classified as early and middle stage. Among 249 patients, the median survival time was 15 months. The overall survival rates at 1, 2, 3, 4 and 5 years were 58%, 37%, 31%, 25% and 20%, respectively.
Table 1: Clinical characteristics of 249 eligible HCC patients undergoing RT
Variables |
No. of patients |
% |
Age (year) Median(range) Sex (Male) Symptoms (Yes) Abdominal pain (Yes) Weight loss (Yes) Alcohol (Yes) HBV (Positive) Cirrhosis (Yes) Splenomegaly (Yes) Tumor size (≤5cm) Tumor number 1 ≥2 AFP(>400ng/ml) Tumor thrombosis (Yes) Vascular invasion (Yes) Total dose of RT Median(range) Fraction dose of RT Median(range) Total times of RT Median(range, day) Times per week 3 4 5 Interventional therapy |
48(23-82) 218 208 167 58 64 205 145 83 48 214 35 143 69 99 52Gy(32Gy-72Gy) 4.6Gy(1.8Gy-8Gy) 12(6-35) 220 19 10 154 |
87.6 83.5 67.1 23.3 25.7 82.3 58.2 33.3 19.3 85.9 14.1 57.4 27.7 39.8 88.4 7.6 4 61.8 |
Survival analysis by the Okuda staging system
The median survival times for patients with Okuda stages I, II and III were 18, 9, 53 months, respectively (log-rank p value = 0.015; C-index = 0.5504, standard error (se) = 0.0181). As shown in Figure 1A, Okuda stage I patients had a significantly longer survival than those patients with Okuda stage II (p value = 0.004). Because only one patient was classified as Okuda stage III, the difference between stage II and stage III could not be evaluated. For patients with early and middle stage HCC who underwent radiotherapy, the Okuda staging system predicted survival well in this cohort.
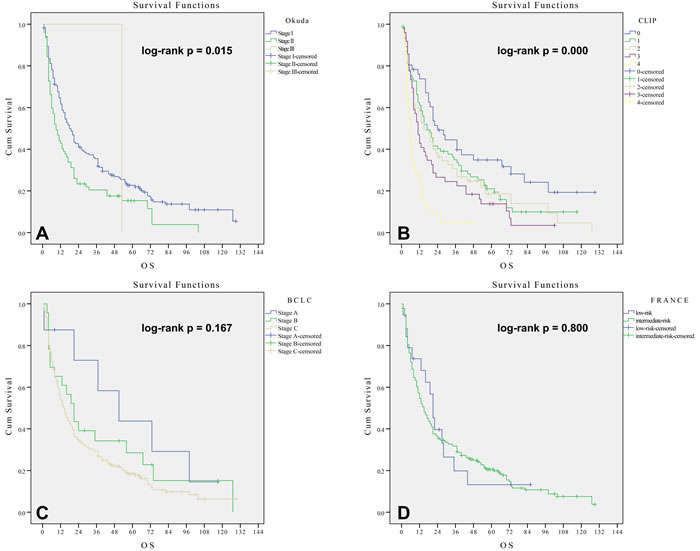
Figure 1: Kaplan-Meier method estimates of cumulative survival curves by the Okuda staging system A., CLIP prognostic score B., BCLC classification system C. and France staging system D. in 249 patients undergoing RT.
Survival analysis by the CLIP prognostic score
The median survival times for CLIP scores 0, 1, 2, 3 and 4 were 24, 17, 15, 11 and 6 months, respectively (log-rank p value = 0.000; C-index = 0.5834, se = 0.0225). As shown in Figure 1B, there was no significant difference in survival among patients with CLIP scores 1 to 3 points (p > 0.05). Significant differences in OS were observed when comparing patient groups with CLIP scores of 0, 3 and 4 (p = 0.009). Therefore, the CLIP prognostic score shows some limitations in predicting prognosis in this cohort.
Survival analysis by BCLC classification system
The median survival times for BCLC stages A, B and C were 51, 21 and 14 months, respectively (log-rank p value = 0.167; C-index = 0.5225, se = 0.0138). As shown in Figure 1C, there was no significant difference in OS between patients with BCLC stages A and B or between patients with BCLC stages B and C (p > 0.05). Therefore, the BCLC classification system had no discriminative power in predicting prognosis in this cohort.
Survival analysis by France staging system
The median survival times for the France low-risk group and intermediate-risk group were 21 and 15 months, respectively (log-rank p value = 0.800; C-index = 0.5050, se = 0.0108). There was no significant difference in OS between the low-risk and intermediate-risk groups (p > 0.05), Figure 1D. This result suggested that the France staging system had no discriminative power in stratifying patients and predicting prognosis in this cohort.
Survival analysis by Chinese university prognostic index
The median survival times for the CUPI low-risk group, intermediate-risk group and high-risk group were 20, 8 and 4 months, respectively (log-rank p value = 0.000; C-index = 0.5746, se = 0.0181). As shown in Figure 2A, CUPI low-risk group patients had a significantly longer survival than did intermediate-risk group patients (p = 0.01). CUPI intermediate-risk group patients had a significantly longer survival than did high-risk group patients (p = 0.011). For HCC patients undergoing radiotherapy, CUPI was a good predictor of overall survival in this cohort.
Survival analysis by Japan integrated staging
The median survival times for JIS scores 1, 2 and 3 were 19, 12 and 8 months, respectively (log-rank p value = 0.056; C-index = 0.5495, se = 0.0204). There was no significant difference in OS between scores of 2 and 3 points (p > 0.05). A difference was observed when comparing patient groups with JIS scores of 1 and 2 points (p = 0.037), Figure 2B. Therefore, JIS shows some limitations in predicting prognosis in this cohort.
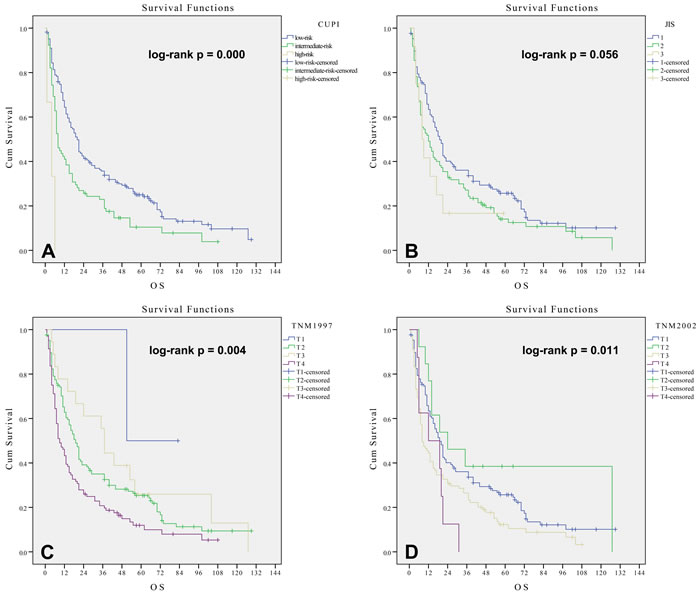
Figure 2: Kaplan-Meier method estimates of cumulative survival curves by the CUPI system A., JIS system B., TNM 1997 system C. and TNM 2002 system D. in 249 patients undergoing RT.
Survival analysis by AJCC 1997 TNM staging system
The median survival times for AJCC 1997 TNM stages T2, T3 and T4 were 19, 37 and 9 months, respectively (log-rank p value = 0.004; C-index = 0.5649, se = 0.0208). Only the difference in OS between stages T3 and T4 was significant (p = 0.011), with the median survival time of T3 longer than that of T2. This result is not common sense, as shown in Figure 2C. The AJCC 1997 TNM staging system had no discriminative power in stratifying patients and predicting prognosis in this cohort.
Table 2: 249 HCC patient distribution by different staging systems.
Staging systems |
Stage |
No. of patients |
% |
The Okuda Staging System Cancer of the Liver Italian Program prognostic score Barcelona Clinic Liver Cancer Classification System The France Staging System Chinese University Prognostic Index Japan Integrated Staging TNM staging system (1997) TNM staging system (2002) TNM staging system (2010) Guangzhou2001 |
I II III 0 1 2 3 4 A B C A B Low-risk group Intermediate-risk group High-risk group 1 2 3 T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4 I II III |
171 77 1 46 78 55 49 21 8 23 218 19 230 168 78 3 127 110 12 2 125 18 104 127 13 101 8 127 13 101 8 40 185 24 |
68.7 30.9 0.4 18.5 31.2 22.1 19.7 8.4 3.2 9.2 87.6 7.6 92.4 67.5 31.3 1.2 51 44.2 0.8 0.8 50.2 7.2 41.8 51 5.2 40.6 3.2 51 5.2 40.6 3.2 16.1 74.3 9.6 |
Survival analysis by AJCC 2002 TNM staging system
The median survival times for AJCC 2002 TNM stages T1, T2, T3 and T4 were 19, 24, 8 and 12 months, respectively (log-rank p value = 0.011; C-index = 0.5578, se = 0.0207). Stage T2 patients had significantly longer survival times than stage T3 patients (p < 0.05). However, there was no significant difference in OS either among patients with T1 and T2 or among patients with T3 and T4 (p > 0.05). In addition, the median survival time of T2 was longer than that of T1 and was longer for T4 than for T3, Figure 2D. The AJCC 2002 TNM staging system could not predict prognosis well in this cohort.
Survival analysis by AJCC 2010 TNM staging system
The median survival times for AJCC 2010 TNM stages T1, T2, T3a, T3b and T4 were 19, 24, 37, 8 and 12 months, respectively (log-rank p value = 0.003; C-index = 0.5673, se = 0.0210). T1 patients had shorter median survival times than did T2 and T3a patients, and T3a patients had the longest median survival time. Obviously, this is not common sense. As shown in Figure 3A, the AJCC 2010 TNM staging failed to predict prognosis in the HCC patients in this cohort.
Survival analysis by the Chinese Guangzhou 2001 staging system
The median survival times for Guangzhou 2001 stages I, II and III were 57, 13 and 12 months, respectively (log-rank p value = 0.000; C-index = 0.5789, se = 0.0182). As shown in Figure 3B, Guangzhou 2001 stage I patients had a significantly longer survival than stage II (p = 0.000). Patients with stages II and III had similar survival times (p = 0.301). For early and intermediate stage HCC patients undergoing radiotherapy, the Guangzhou 2001 staging system was a good predictor of overall survival.
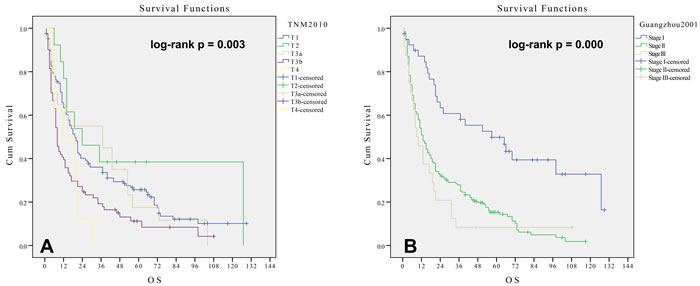
Figure 3: Kaplan-Meier method estimates of cumulative survival curves by the TNM 2010 A. and Chinese Guangzhou 2001 staging system B. in 249 patients undergoing RT.
DISCUSSION
The Okuda staging system was one of the first developed [11]. Although it does not consider tumor factors in detail, it does account for liver function status, which plays an important role in predicting prognosis [15]. In our study, Okuda stage I patients had a significantly longer survival than Okuda stage II patients (p = 0.004). Although the difference between stages II and III could not be evaluated because only one patient was classified as Okuda stage III, the Okuda staging system was successful in predicting survival for early and intermediate stage HCC patients.
The CLIP prognostic score accounts for liver function status and detailed tumor factors [12, 13]. However, several retrospective analyses showed that a significant difference was present among some stages. Levy found that the CLIP prognostic score can identify the patients with a significantly better prognosis or a significantly worse prognosis, when he studied on the prognosis of 257 HCC patients [23]. Our study showed similar results; survival differences were found only among CLIP scores 0, 3 and 4 (p = 0.009). The result of our study is similar to that of Korea [22]. The assessment of prognosis using the CLIP prognostic score needs improvement.
The BCLC [14] classification system was reported to be the best therapeutic guideline, especially for early liver cancer patients who can receive radical surgery [23, 24]. However, it had some deficits: (1) scoring is complex and requires more parameters; and (2) it is not feasible to obtain information on values such as performance score (PS) and portal hypertension for a retrospective clinical study. Our studies showed that there was no statistical differentiation among all stages.
The variables of France staging system [15] are liver function status, performance status test (PST) and portal vein cancerous thrombosis. Both it and the BCLC classification system include subjective factors such as PST. Our study showed that there was no significant difference in overall survival between the low- and intermediate-risk groups (p = 0.800).
Our study found that CUPI [16] was good at predicting overall survival for HCC patients undergoing radiotherapy. CUPI was constructed for patients with HCC based on large numbers of patients. However, almost all of the patients had HBV-related HCC (79%). Europe and the United States populations are more typically infected with the HCV virus, while the Asian population is more commonly infected with the HBV virus; perhaps it can be said that CUPI applies to patients with HBV-related liver cancer to predict the prognosis of overall survival. This study found that CUPI was able to better predict patient survival prognosis that could not be excluded precisely because of this feature; an American scholar demonstrated that CUPI showed a better prognostic ability with HCC patients undergoing transcatheter arterial chemoembolization (TACE) [25]. The limitations of our study were mainly due to the unbalanced distribution of different stage HCC patients, which makes it impossible to compare all patients. Therefore, further studies should expand the sample size to balance patients among different stages.
The JIS scoring system [17] was proposed based on the integrated Japanese TNM staging system and Child-Pugh class. The Liver Cancer Study Group of Japan indicated that the JIS scoring system was more discriminative than Japanese TNM. However, a separate trend of Kaplan-Meier survival curves between JIS scores 1 and 2 was not obvious. Hence, JIS shows some limitations in predicting prognosis.
The AJCC TNM staging system was considered the best staging system in solid tumors and was adopted for clinical practice. The AJCC 1997 TNM staging system [18] indicated that some tumor features such as tumor size, tumor number, vascular infusion, lymph node metastasis and distant metastasis had the same prognostic value. However, some studies have demonstrated that they were not all the same [26, 27]. The AJCC 2002 TNM staging system lacked liver function status; the AJCC 2002 TNM staging system then combined liver function scoring to enhance the prognostic ability [19]. However, in our study, all AJCC TNM staging systems were far from satisfactory. Vauthey LN and the International Collaborative Group obtained similar results [19, 25]. The AJCC TNM staging system had low approval for the following reasons: (1) lack of liver function status; (2) difficult to clear vascular infusion, especially microvascular infusion; and (3) difficult to compare and evaluate because each edition of AJCC TNM staging system changed tremendously.
The Guangzhou 2001 staging system was based on hepatectomy [21, 28]. It is debatable whether it is valid regarding treatment strategy beyond surgery. Some Chinese scholars considered the Guangzhou 2001 staging system to be more suitable for Chinese HCC patients. Our study showed that a separate trend of Kaplan-Meier survival curves between stages I and II was extremely obvious. For early and intermediate HCC patients undergoing radiotherapy, the Guangzhou 2001 staging system did well in predicting overall survival in HCC patients undergoing radiotherapy.
However, the manuscript has the following limitations: First, it is a retrospective study. In this retrospective analysis, we only consider the different clinical stage, not fully consider all possible confounding factors that potentially impact on patients’ overall survival, such as other treatment methods before or after radiotherapy. But, we think that it does not badly affect our results. Take Okuda staging system for example, total 88 HCC patients received transcatheter arterial chemoembolization (TACE), the proportion of patients received TACE is balanced between Okuda stage 1 and stage 2 (p = 0.757). Besides radiotherapy or TACE, a few patients have received the biotherapy and other treatment. The diversity of treatments may introduce unpredictable confounding factors. Additionally, only Child-Pugh A HCC patients were included in this study, which further limits the representativeness of the conclusion. In fact, all of the C-index were too small, with limited value, it well proved that the existing staging systems for liver cancer are flawed, and need to be improved.
In conclusion, our study demonstrated that the Okuda staging system, CUPI and the Chinese Guangzhou 2001 staging system were more discriminate than the other staging systems in prognostic stratification for early and middle stage HCC patients treated with radiotherapy. The others (CLIP prognostic score, BCLC classification system, the France staging system, JIS score, AJCC 1997 TNM staging system, AJCC 2002 TNM staging system and AJCC 2010 TNM staging system) performed poorly in stratifying the liver cancer patients undergoing radiotherapy in our study.
METHODS AND MATERIALS
Patients
Between April 1999 and March 2012, 249 eligible liver cancer patients who had not undergone curative resection were identified from the patient files of the Cancer Hospital of Guangxi Medical University and were included in the study. Patients with HCC were diagnosed based on the clinical diagnostic criteria proposed by the Chinese Society of Liver Cancer and the Chinese Anti-Cancer Association (CACA) in 2011 [28] or based on a pathologic diagnosis. Patients with primary HCC received radiotherapy using the three-dimensional conformal radiation therapy (3-DCRT) technique as the main treatment approach were included. Total dose of RT should be more than 30 Gy, Fraction dose of RT should not be less than 1.8 Gy/fraction. Patients with cirrhosis of the liver have been identified as being an independent risk for HCC, and HCC is the principal cause of death in patients with cirrhosis [29, 30], so liver cancer patients with cirrhosis were included in the study. The Child-Pugh Grade was also an independent prognostic factor for HCC [4]. We only included HCC patients with Child-Pugh Grade A in our study, considering the potential influence of the Child-Pugh Grade [31]. Whether Child-Pugh Grade B patients can accept radiation therapy is controversial, Child-Pugh Grade C is not suitable for radiotherapy. Thus, Child-Pugh Grade B and Child-Pugh Grade C HCC patients were excluded. Patients with extrahepatic metastasis were excluded. This study was approved by the Institutional Review Board of Cancer Hospital of Guangxi Medical University, which waived the requirement for informed consent. The abstract of this paper was presented as a poster at the American Society for Radiation Oncology 56th Annual Meeting, October 28-31, 2012, in Boston, Massachusetts.
Staging criteria
Two experienced reviewers independently reviewed the stages for all eligible patients following different staging systems and resolved controversies by discussion. The 10 staging systems included the Okuda staging system, Cancer of the Liver Italian Program (CLIP) prognostic score, Barcelona Clinic Liver Cancer (BCLC) classification system, the France staging system, Chinese University Prognostic Index (CUPI), Japan Integrated Staging (JIS) score, American Joint Committee on Cancer (AJCC) 1997 Tumor-Node-Metastasis (TNM) staging system, AJCC 2002 TNM staging system, AJCC 2010 TNM staging system and the Chinese Guangzhou 2001 staging system. Data were collected to compare the validity of the different staging systems in HCC patients undergoing 3-DCRT.
Tumor morphology was determined based on computerized tomography (CT). Vascular invasion was assessed using dynamic CT and angiography. The maximum diameter of the tumor was measured using CT or ultrasonography. Lymph node metastasis and distant metastases were assessed using conventional anatomic imaging, such as ultrasound, dynamic CT scans and X-rays.
Treatment
All patents underwent a planning CT scan to facilitate three-dimensional treatment planning using the Topslane planning system (Topslane Medical Corp., Shanghai, China) or the Precise planning system (Elekta Corp., Sweden). The gross volumes (GTV) were defined as the radiographically abnormal areas presented on the diagnostic CT and/or magnetic resonance imaging. The planning target volume (PTV) was defined by adding 0.5-1.5 cm to GTV. Liver motion was considered, with additional margins added to account for motion. The fraction sizes and total doses were determined based on the individual physician’s professional judgment.
Follow up
Patients were followed up every 3 months for 1 year and then every 6 months after treatment until death or the termination of this study (March 2016). The date of death was obtained from either patient records or death registers or family dependents. In patients with local recurrences of the primary lesion or with development of new lesions, a new treatment strategy was usually planned and performed. Length of survival was calculated from the date when the radiotherapy commenced.
Statistical analysis
All statistical analyses were performed with SPSS version 16.0 (SPSS Inc., Chicago, IL, USA) and R (version: 3.3.1). The cumulative survival rate was calculated using the Kaplan-Meier method. Survival curves were statistically compared using the log-rank test; univariate cox regression was performed and the Harrell’s concordance index (c-index) was calculated in the R software. A two-tailed p < 0.05 was considered statistically significant.
Author contributions
Conception and design: Shi-Xiong Liang. Collection and assembly of data: Zhi-Rui Zhou, Min Liu and Shi-Xiong Liang. Data analysis and interpretation: Zhi-Rui Zhou and Shi-Xiong Liang. Manuscript writing: all authors. Final approval of manuscript: all authors. Financial support: Shi-Xiong Liang.
Conflicts of Interest
The authors declare no conflicts of interest.
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65:87-108.
2. Monsour HP Jr, Asham E, McFadden RS, Victor DW III, Muthuswamy B, Zaheer I. Hepatocellular carcinoma: the rising tide from east to west—a review of epidemiology, screening and tumor markers. Translational Cancer Research. 2013; 2:492-506.
3. Zaccagna F, Anzidei M, Sandolo F, Cavallo Marincola B, Palla C, Leonardi A, Caliolo G, Andreani F, De Soccio V, Catalano C, Napoli A. MRgFUS for liver and pancreas cancer treatments: the Umberto I hospital experience. Translational Cancer Research. 2014; 3:430-441.
4. Liang SX, Jiang GL, Zhu XD, Fu XL, Li FX, Huang QF, Wang AY, Chen L, Lu HJ. [Prognostic factor of primary liver cancer treated by hypofractionated three-dimensional conformal radiotherapy]. [Article in Chinese]. Zhonghua Zhong Liu Za Zhi. 2005; 27:613-615.
5. Liang SX, Zhu XD, Lu HJ, Pan CY, Li FX, Huang QF, Wang AY, Chen L, Fu XL, Jiang GL. Hypofractionated three-dimensional conformal radiation therapy for primary liver carcinoma. Cancer. 2005; 103:2181-2188.
6. Yoon HI, Jung I, Han KH, Seong J. The effect of radiotherapy in liver-confined but non-resectable Barcelona Clinic Liver Cancer stage C large hepatocellular carcinoma. Oncotarget. 2016; 7:62715-62725. doi: 10.18632/oncotarget.10908.
7. Dionisi F, Guarneri A, Dell’Acqua V, Leonardi M, Niespolo R, Macchia G, Comito T, Amichetti M, Franco P, Cilla S, Caravatta L, Alongi F, Mantello G. Radiotherapy in the multidisciplinary treatment of liver cancer: a survey on behalf of the Italian Association of Radiation Oncology. Radiol Med. 2016; 121:735-743.
8. Cha H, Park HC, Yu JI, Kim TH, Nam TK, Yoon SM, Yoon WS, Kim JW, Kim MS, Jang HS, Choi Y, Kim JH, Kay CS, et al. Clinical Practice Patterns of Radiotherapy in Patients with Hepatocellular Carcinoma: A Korean Radiation Oncology Group study (KROG 14-07). Cancer Res Treat. 2016.
9. Park HC, Yu JI, Cheng JC, Zeng ZC, Hong JH, Wang ML, Kim MS, Chi KH, Liang PC, Lee RC, Lau WY, Han KH, Chow PK, Seong J. Consensus for Radiotherapy in Hepatocellular Carcinoma from The 5th Asia-Pacific Primary Liver Cancer Expert Meeting (APPLE 2014): Current Practice and Future Clinical Trials. Liver Cancer. 2016; 5:162-174.
10. Yoon HI, Seong J. Optimal Selection of Radiotherapy as Part of a Multimodal Approach for Hepatocellular Carcinoma. Liver Cancer. 2016; 5:139-151.
11. Okuda K, Ohtsuki T, Obata H, Tomimatsu M, Okazaki N, Hasegawa H, Nakajima Y, Ohnishi K. Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer. 1985; 56:918-928.
12. Investigators TCotLIPC. A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients: the Cancer of the Liver Italian Program (CLIP) investigators. Hepatology. 1998; 28:751-755.
13. Investigators TCotLIPC. Prospective validation of the CLIP score: a new prognostic system for patients with cirrhosis and hepatocellular carcinoma. The Cancer of the Liver Italian Program (CLIP) Investigators. Hepatology. 2000; 31:840-845.
14. Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999; 19:329-338.
15. Chevret S, Trinchet JC, Mathieu D, Rached AA, Beaugrand M, Chastang C. A new prognostic classification for predicting survival in patients with hepatocellular carcinoma. Groupe d’Etude et de Traitement du Carcinome Hepatocellulaire. J Hepatol. 1999; 31:133-141.
16. Leung TW, Tang AM, Zee B, Lau WY, Lai PB, Leung KL, Lau JT, Yu SC, Johnson PJ. Construction of the Chinese University Prognostic Index for hepatocellular carcinoma and comparison with the TNM staging system, the Okuda staging system, and the Cancer of the Liver Italian Program staging system: a study based on 926 patients. Cancer. 2002; 94:1760-1769.
17. Kudo M, Chung H, Osaki Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J Gastroenterol. 2003; 38:207-215.
18. Sobin LH, Fleming ID. TNM Classification of Malignant Tumors, fifth edition (1997). Union Internationale Contre le Cancer and the American Joint Committee on Cancer. Cancer. 1997; 80:1803-1804.
19. Vauthey JN, Lauwers GY, Esnaola NF, Do KA, Belghiti J, Mirza N, Curley SA, Ellis LM, Regimbeau JM, Rashid A, Cleary KR, Nagorney DM. Simplified staging for hepatocellular carcinoma. J Clin Oncol. 2002; 20:1527-1536.
20. Farges O, Fuks D, Le Treut YP, Azoulay D, Laurent A, Bachellier P, Nuzzo G, Belghiti J, Pruvot FR, Regimbeau JM. AJCC 7th edition of TNM staging accurately discriminates outcomes of patients with resectable intrahepatic cholangiocarcinoma: By the AFC-IHCC-2009 study group. Cancer. 2011; 117:2170-2177.
21. Association TCSoLCatCA-C. The clinical diagnosis and staging criteria of PLC. Chin J Hepatobiliary Surg. 2004; 12:67-68.
22. Seong J, Shim SJ, Lee IJ, Han KH, Chon CY, Ahn SH. Evaluation of the prognostic value of Okuda, Cancer of the Liver Italian Program, and Japan Integrated Staging systems for hepatocellular carcinoma patients undergoing radiotherapy. Int J Radiat Oncol Biol Phys. 2007; 67:1037-1042.
23. Levy I, Sherman M. Staging of hepatocellular carcinoma: assessment of the CLIP, Okuda, and Child-Pugh staging systems in a cohort of 257 patients in Toronto. Gut. 2002; 50:881-885.
24. Wang JH, Changchien CS, Hu TH, Lee CM, Kee KM, Lin CY, Chen CL, Chen TY, Huang YJ, Lu SN. The efficacy of treatment schedules according to Barcelona Clinic Liver Cancer staging for hepatocellular carcinoma - Survival analysis of 3892 patients. Eur J Cancer. 2008; 44:1000-1006.
25. Georgiades CS, Liapi E, Frangakis C, Park JU, Kim HW, Hong K, Geschwind JF. Prognostic accuracy of 12 liver staging systems in patients with unresectable hepatocellular carcinoma treated with transarterial chemoembolization. J Vasc Interv Radiol. 2006; 17:1619-1624.
26. Izumi R, Shimizu K, Ii T, Yagi M, Matsui O, Nonomura A, Miyazaki I. Prognostic factors of hepatocellular carcinoma in patients undergoing hepatic resection. Gastroenterology. 1994; 106:720-727.
27. Grieco A, Pompili M, Caminiti G, Miele L, Covino M, Alfei B, Rapaccini GL, Gasbarrini G. Prognostic factors for survival in patients with early-intermediate hepatocellular carcinoma undergoing non-surgical therapy: comparison of Okuda, CLIP, and BCLC staging systems in a single Italian centre. Gut. 2005; 54:411-418.
28. The Chinese Society of Liver Cancer and the Chinese Anti-Cancer Association. The clinical diagnosis and staging criteria of PLC. Chinese J Clin Oncol. 2011; 10:929-946.
29. Colombo M, de Franchis R, Del Ninno E, Sangiovanni A, De Fazio C, Tommasini M, Donato MF, Piva A, Di Carlo V, Dioguardi N. Hepatocellular carcinoma in Italian patients with cirrhosis. N Engl J Med. 1991; 325:675-680.
30. El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med. 1999; 340:745-750.
31. Liang SX, Huang XB, Zhu XD, Zhang WD, Cai L, Huang HZ, Li YF, Chen L, Liu MZ. Dosimetric predictor identification for radiation-induced liver disease after hypofractionated conformal radiotherapy for primary liver carcinoma patients with Child-Pugh Grade A cirrhosis. Radiother Oncol. 2011; 98:265-269.