
INTRODUCTION
Non-small cell lung cancer(NSCLC) is the leading cause of cancer-related mortality worldwide. NSCLC patients are at high risk for brain metastases (BMs) with reported rates ranging from approximately 20% to 40% [1, 2]. Life expectancy for these patients is poor, with a median survival of only 3.4 months [3]. Moreover, many will suffer considerable loss of autonomy due to neurocognitive and functional deficits, as well as medication associated morbidity (such as steroid and antiepileptic drugs).
The outcomes of brain metastasis from NSCLC are both unfavorable and lacking in effective treatment options. Surgical resection is generally reserved for patients with a good prognosis, limited extracranial metastases, and a single brain lesion. Numerous trials have investigated chemotherapy in BMs patients, however, due to the inability of drugs to cross brain–blood barrier (BBB), there has been no categorically proven survival benefit [4, 5]. Whole brain radiotherapy (WBRT) has long been a mainstay of treatment for BMs but it is limited by long term side-effects. Recently, stereotactic radiosurgery (SRS) has become an alternative approach for patients with BMs; this procedure involves delivering a high dose of radiation, which allows for precise tumor targeting while minimizing the irradiation to the adjacent normal tissue [6, 7].
One previous meta-analysis demonstrated that adding SRS to WBRT improved survival in patients with one brain metastasis, and improved local tumor control and functional independence in all patients [8]. Nevertheless, three randomized trials consistently found that compared with SRS alone, the use of WBRT plus SRS did not improve survival for patients with BMs [9–11]. In addition, Xue et al. investigated the safety of radiotherapy and found that WBRT resulted in a higher incidence of radiation-related toxicities than SRS [12]. Overall, evidence is in favor of SRS as an effective therapy in BMs patients despite differences in patient selection and treatment design.
Several reports have shown that the special tyrosine kinase inhibitor (TKI) of the epidermal growth factor receptor (EGFR), is capable of reducing BMs in NSCLC, sometimes with a highly dramatic response [13–15]. The status of EGFR mutation has been reported to be associated not only with improved survival for patients with BMs [16], but also with the response rate of radiotherapy [17]. However, a recent prospective study showed the addition of TKI to WBRT+SRS in NSCLC patients with 1 to 3 brain metastases did not improve survival and may even have had a deleterious effect [18]. The contradictory results of this study and the others, detailed above, involving WBRT in combination with SRS raise the question of whether TKI alone should be the primary treatment option, with SRS reserved only as a salvage method in patients with symptomatic BMs. Herein, We report the results of the addition of SRS (X-knife) to TKI (gefitinib) therapy in EGFR mutated NSCLC patients with symptomatic BMs to evaluate its’ safety and efficacy.
MATERIALS AND METHODs
Patient characteristics
We retrospectively retrieved the medical records of seven consecutive patients who were diagnosed as NSCLC with severe symptomatic BMs at Guangdong 999 Brain Hospital between 1 January 2012 and 31 August 2014. This study was reviewed and approved by the ethics committee. Included patients must have had pathologically confirmed NSCLC with EGFR gene mutation, and medical image confirmed brain metastasis. Conventional therapy included gefitinib, with SRS(X-knife) reserved as the salvage method. Contrast-enhanced CT and positron emission tomography CT (PET-CT) were performed for evaluation. Staging was designated by the 7th edition of the tumor, node, metastasis (TNM) classification.
Samples and EGFR mutation detection
All patients had adequate tumor tissue or biopsy samples for molecular analysis. The EGFR Mutation Detection Kit (Amoy Diagnostics, Xiamen, China), which is based on the amplification mutation refractory system(AMRS) technology, was used to detect the 29 most common types of EGFR mutations and the T790M mutation. All experiments were performed according to the user manual. Tissues came from operations in three patients (one from the lung, two from the head), and biopsy of the lung in the other four. Though not all samples were from the BMs, a previous Chinese study identified an accordance rate of 93.3% in the EGFR mutation status between the primary tumor and BMs [19]. Hence, primary tumor EGFR status is a very good surrogate for EGFR mutation status of the BMs.
Treatment procedures
EGFR TKI (Gefitinib) was used as the standard treatment as soon as the mutation was diagnosed. X-knife image fusion software (Radionics RT2, Burlington, MA) was used to fuse all treatment images and data to a reference CT image (initial CT before the first SRS treatment). Cumulative and individual doses to each lesion, the whole brain, the optic chasm, and the right and left optic nerves were determined for each patient with the X-knife planning software. The system included a 6-MV dedicated linac with fixed circular cones (Varian 600C/D); this was used with the X-knife forward-planning system.
Follow-up evaluations and primary outcomes
Changes in the neurological symptoms, such as paresis, aphasia, sensory and visual disturbances, were examined before and after treatment in all patients. The severity of symptoms was divided into four grades based on the activities of daily living determined according to the medical care accreditation criteria: Grade 0: no trouble (able to perform the activities without help), Grade 1: slightly impaired (able to perform/complete? activities with some difficulty), Grade 2: moderately affected (needing partial support), and Grade 3: severely affected (unable to function in normal daily life and needing total support). In addition, the improvement of symptoms was defined as an increase by one grade or more.
A Magnetic Resonance Imaging(MRI) or CT-scan were performed before treatment and every one to four months thereafter, to define the tumor response and local control. The primary end point of the study was overall survival (OS) calculated from the start of gefitinib treatment to the date of death. Secondary end points included progression-free survival (PFS) defined as the time elapsed between gefitinib treatment and disease progression. The activity of daily living was assessed using Karnofsky performance status(KPS) index.
RESULTS
Patient characteristics and radiologic and pathologic findings
A total of seven patients’ (two males and five females) clinical data were analyzed in the present study. Patient age ranged from 44 to 62. All patients were pathologically diagnosed as adenocarcinoma according to the 7th lung cancer classification. In regard to EGFR mutation, five patients had 19 deletion and two had 20 deletion. No T790M mutation was found. Among the included patients, five had more than four BMs, one had one BM (size of 6.0*3.0cm), and one had widely reinforced in pia mater. Preoperative KPS score ranged from 30 to 90. The details are listed in Table 1.
Table 1: Patient characteristics and radiologic and pathologic findings
Patient ID |
Gender |
Age |
Smoke |
Region of specimen |
EGFR mutation |
Neurological manifestation (Grade0,1,2,3) |
Number of lesions in brain (the size of the biggest one) |
Location of lesions |
|---|---|---|---|---|---|---|---|---|
1 |
Female |
59 |
No |
Biopsy |
19 del+ |
3 |
Widely reinforcement in pia mater (2.0*1.5cm) |
Pia mater |
2 |
Male |
44 |
No |
Biopsy |
19 del+ |
2 |
6 (3.7*3.3cm) |
Bilateral frontal lobe, parietal lobe on the right side, and four ventricle on the rim |
3 |
Female |
44 |
No |
Biopsy |
19 del+ |
2 |
6 (5.2*3.1cm) |
Bilateral frontal occipital lobe |
4 |
Male |
58 |
No |
Surgery |
20 del+ |
0 |
12 (3.0*2.5cm) |
Bilateral cerebral hemisphere, cerebellar hemisphere and the left cerebral peduncle |
5 |
Female |
50 |
No |
Biopsy |
19 del+ |
2 |
4 (5.2*4.1cm) |
Bilateral frontal, temporal, parietal lobe, left occipital lobe, cerebellum awning and bilateral cerebral hemisphere pia mater |
6 |
Female |
62 |
No |
Surgery |
19 del+ |
0 |
1 (6.0*3.0cm) |
Right parietal, occipital lobe, |
7 |
Female |
53 |
No |
Surgery |
20 del+ |
2 |
20 (1.29*1.22cm) |
Bilateral cerebral hemisphere, cerebellar vermis, bilateral basal ganglia region |
Treatment efficacy and safety
In the present study, two of the included patients received gefitinib as second line treatment. Two of the patient received the surgery for brain metastasis first, then received SRS, then received gefitinib. The others received biopsy first, then received gefitinib, then received SRS. Duration of Gefitinib usage ranged from two to thirteen months. X-knife was performed in all patients. Steroids were used after radio-surgery and stopped within one week. Median overall survival was 16 months, and median PFS was 10 months (Figure 1). Patients were found to tolerate treatment well. The KPS score ranged from 70 to 90 one week after X-knife therapy. Demographic details, and radio-surgical data for all patients are summarized in Table 2.
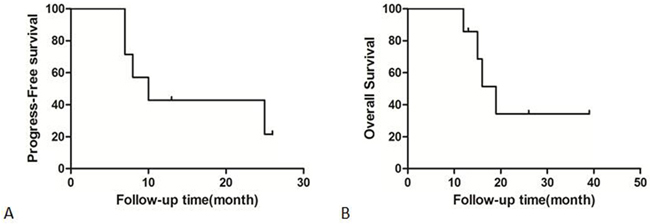
Figure 1: A. The progress-free survival of included patients. B. The overall survival of included patients.
Table 2: Treatment efficacy and safety
Patient ID |
Reason to use SRS |
SRS treatment strategies |
Usage of corticosteroid after SRS treatment |
Duration of gefitinib treatment |
Neurological manifestation after SRS (Grade0,1,2,3) |
KPS score before SRS treatment |
KPS score after SRS treatment |
PFS (months) |
OS (months) |
|---|---|---|---|---|---|---|---|---|---|
1 |
Brain edema |
One isocentre with 1000cgy dose on one lesion |
Stop at seven days after SRS |
9 |
1 |
30 |
60 |
7 |
12 |
2 |
Ventrcles compression |
First time: one isocentre with 1000cgy dose on one lesion; Second time: five isocentres with 1200cgy on four lesions |
Stop at five days after SRS |
2 |
0 |
60 |
90 |
8 |
19 |
3 |
Brain edema |
Seven isocentres with 1300cgy on six lesions |
Stop at seven days after SRS |
6 |
1 |
70 |
80 |
7 |
15 |
4 |
Brain edema |
First time: nine isocentres with 1000-1400cgy on nine lesions; Second time: nine isocentres with 1000-1400cgy on nine lesions |
Stop at seven days after SRS |
10 |
1 |
80 |
80 |
10 |
16 |
5 |
Brain edema |
Eight isocentres with 1400cgy on eight lesions |
Stop at five days after SRS |
12 |
1 |
60 |
90 |
26+ |
26+ |
6 |
Ventrcles compression |
One isocentre with 1000cgy dose on one lesion |
Stop at five days after SRS |
13 |
1 |
90 |
90 |
13+ |
13+ |
7 |
Brain edema |
Nine isocentres with 1000-1400cgy on nine lesions |
Stop at seven days after SRS |
12 |
2 |
70 |
80 |
25 |
39+ |
DISCUSSION
BMs is a common and lethal complication of NSCLC, which portends a poor prognosis. Radiotherapy has been applied to inoperable BMs as a therapeutic or palliative option. The use of drugs targeting the proteins of mutated EGFR has become a standard of care in the systemic treatment of metastatic NSCLC as well [20]. While the simultaneous presence of BMs and EGFR mutations are common , the efficacy and safety of the additional use of SRS to TKI in symptomatic NSCLC patients remains unclear. In the present study, we demonstrated that the functional autonomy (KPS) and survival could be improved by SRS(X-knife) as a salvage approach in symptomatic BMs patients.
SRS delivers a single high dose of radiation to the target volume while avoiding the surrounding normal tissues. Hall and colleagues reported that BMs patients treated with SRS alone have similar overall survival and receive more cost-effective care than those treated with SRS+WBRT [21]. Another study by Soffietti et al. concluded patients who received WBRT experienced worse health related quality of life (HRQOL), particularly during the early follow-up period, compared with patients treated with surgery or SRS alone [22]. As a result, SRS has been confirmed to be an effective and less invasive therapy. In the present study, SRS was performed as a salvage therapy for patients with complications, including encephaledema and compression of ventricles, and all patients were diagnosed with lung adenocarcinoma and severe BMs,. In addition, all included patients received EGFR TKI before SRS and the total radiation doses received were well tolerated. After SRS treatment, the KPS scores of all patients increased. Postoperative MRI examination also revealed either stable or smaller tumor lesions (Figure 2).
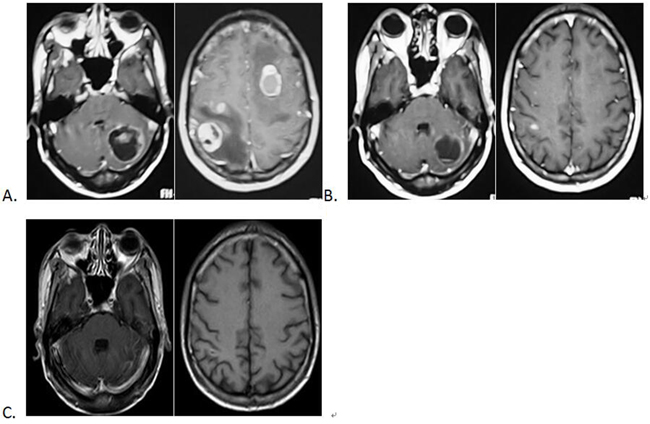
Figure 2: MRI images showing brain metastases of NSCLC. A. Before the SRS treatment; B. One month after SRS treatment; C. Four months after SRS treatment.
EGFR mutation status is associated with improved survival among patients with BMs [16]. The study from Cai et al. reported that administration of TKI agents with WBRT/SRS/surgery might be beneficial for OS and PFS of intracranial disease and PFS of extracranial disease in NSCLC patients with BMs independent of EGFR mutations [23]. However, Sperduto and colleagues found that the addition of TKI to WBRT+SRS in NSCLC patients with 1 to 3 brain metastases did not improve survival and possibly had a deleterious effect [18]. In our study, the seven included patients had primary tumor tissues or BMs diagnosed, EGFR mutation(5, 19 deletion/2, 20 deletion) and received gefitinib as primary treatment. The median OS was 16 months and the median PFS was 10 months.
In general, BMs are resistant to systemic chemotherapy due to the inability of drugs to cross brain–blood barrier (BBB) [4, 5]. Recently, the remarkable response and mild toxicity of EGFR TKI treatment makes it an attractive option for NSCLC patients with BMs and EGFR mutations [24]. One prospective study of Gefitinib on NSCLC patients with BMs reported that the response rate (RR) of TKI use in BMs patients was 10%, with a median duration of response of 13.5 months and median OS of 5 months [15]. However, another study consisting of 15 patients reported that the RR of TKI use in BMs was 60%, with a median duration of response of 8.7 months [25]. The increased RR is most likely attributed to previous radiation therapy. In addition, erlotinib seems to produce higher CSF levels than gefinitib [26], and therefore might be preferable. Another limitation is that the EGFR mutation detection kit we used can only detect three kinds of EGFR exon 20 insertion.
In conclusion, SRS(X-knife) with concurrent gifitinib therapy in NSCLC patients with symptomatic BMs, and EGFR mutation produced reliable improvement of KPS and survival. Given the small sample size, further prospective studies with a greater number of patients are warranted to confirm our results.
CONFLICTS OF INTEREST
None.
FUNDING/SUPPORT
None.
REFERENCES
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015; 65: 5-29.
2. Barnholtz-Sloan JS, Sloan AE, Davis FG, Vigneau FD, Lai P, Sawaya RE. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. Journal of clinical oncology. 2004; 22: 2865-72.
3. Lagerwaard FJ, Levendag PC, Nowak PJ, Eijkenboom WM, Hanssens PE, Schmitz PI. Identification of prognostic factors in patients with brain metastases: a review of 1292 patients. International journal of radiation oncology, biology, physics. 1999; 43: 795-803.
4. Shapiro WR, Shapiro JR. Principles of brain tumor chemotherapy. Seminars in oncology. 1986; 13: 56-69.
5. Greig NH, Soncrant TT, Shetty HU, Momma S, Smith QR, Rapoport SI. Brain uptake and anticancer activities of vincristine and vinblastine are restricted by their low cerebrovascular permeability and binding to plasma constituents in rat. Cancer chemotherapy and pharmacology. 1990; 26: 263-8.
6. Andrews DW, Scott CB, Sperduto PW, Flanders AE, Gaspar LE, Schell MC, Werner-Wasik M, Demas W, Ryu J, Bahary JP, Souhami L, Rotman M, Mehta MP, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet. 2004; 363: 1665-72.
7. Sneed PK, Suh JH, Goetsch SJ, Sanghavi SN, Chappell R, Buatti JM, Regine WF, Weltman E, King VJ, Breneman JC, Sperduto PW, Mehta MP. A multi-institutional review of radiosurgery alone vs. radiosurgery with whole brain radiotherapy as the initial management of brain metastases. International journal of radiation oncology, biology, physics. 2002; 53: 519-26.
8. Stafinski T, Jhangri GS, Yan E, Menon D. Effectiveness of stereotactic radiosurgery alone or in combination with whole brain radiotherapy compared to conventional surgery and/or whole brain radiotherapy for the treatment of one or more brain metastases: a systematic review and meta-analysis. Cancer treatment reviews. 2006; 32: 203-13.
9. Aoyama H, Shirato H, Tago M, Nakagawa K, Toyoda T, Hatano K, Kenjyo M, Oya N, Hirota S, Shioura H, Kunieda E, Inomata T, Hayakawa K, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. Jama. 2006; 295: 2483-91.
10. Chang EL, Wefel JS, Hess KR, Allen PK, Lang FF, Kornguth DG, Arbuckle RB, Swint JM, Shiu AS, Maor MH, Meyers CA. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial. The Lancet Oncology. 2009; 10: 1037-44.
11. Kocher M, Soffietti R, Abacioglu U, Villà S, Fauchon F, Baumert BG, Fariselli L, Tzuk-Shina T, Kortmann RD, Carrie C, Ben Hassel M, Kouri M, Valeinis E, et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952-26001 study. Journal of clinical oncology. 2011; 29: 134-41.
12. Xue J, Kubicek GJ, Grimm J, LaCouture T, Chen Y, Goldman HW, Yorke E. Biological implications of whole-brain radiotherapy versus stereotactic radiosurgery of multiple brain metastases. Journal of neurosurgery. 2014; 121: 60-8.
13. Chiu CH, Tsai CM, Chen YM, Chiang SC, Liou JL, Perng RP. Gefitinib is active in patients with brain metastases from non-small cell lung cancer and response is related to skin toxicity. Lung cancer. 2005; 47: 129-38.
14. Hotta K, Kiura K, Ueoka H, Tabata M, Fujiwara K, Kozuki T, Okada T, Hisamoto A, Tanimoto M. Effect of gefitinib (’Iressa’, ZD1839) on brain metastases in patients with advanced non-small-cell lung cancer. Lung cancer. 2004; 46: 255-61.
15. Ceresoli GL, Cappuzzo F, Gregorc V, Bartolini S, Crino L, Villa E. Gefitinib in patients with brain metastases from non-small-cell lung cancer: a prospective trial. Annals of oncology. 2004; 15: 1042-7.
16. Eichler AF, Kahle KT, Wang DL, Joshi VA, Willers H, Engelman JA, Lynch TJ, Sequist LV. EGFR mutation status and survival after diagnosis of brain metastasis in nonsmall cell lung cancer. Neuro-oncology. 2010; 12: 1193-9.
17. Gow CH, Chien CR, Chang YL, Chiu YH, Kuo SH, Shih JY, Chang YC, Yu CJ, Yang CH, Yang PC. Radiotherapy in lung adenocarcinoma with brain metastases: effects of activating epidermal growth factor receptor mutations on clinical response. Clinical cancer research. 2008; 14: 162-8.
18. Sperduto PW, Wang M, Robins HI, Schell MC, Werner-Wasik M, Komaki R, Souhami L, Buyyounouski MK, Khuntia D, Demas W, Shah SA, Nedzi LA, Perry G, et al. A phase 3 trial of whole brain radiation therapy and stereotactic radiosurgery alone versus WBRT and SRS with temozolomide or erlotinib for non-small cell lung cancer and 1 to 3 brain metastases: Radiation Therapy Oncology Group 0320. International journal of radiation oncology, biology, physics. 2013; 85: 1312-8.
19. Luo D, Ye X, Hu Z, Peng K, Song Y, Yin X, Zhu G, Ji Q, Peng Y. EGFR mutation status and its impact on survival of Chinese non-small cell lung cancer patients with brain metastases. Tumour biology. 2014; 35: 2437-44.
20. Ettinger DS, Akerley W, Borghaei H, Chang AC, Cheney RT, Chirieac LR, D’Amico TA, Demmy TL, Govindan R, Grannis FW Jr, Grant SC, Horn L, Jahan TM, et al. Non-small cell lung cancer, version 2.2013. Journal of the National Comprehensive Cancer Network : JNCCN. 2013; 11: 645-53; quiz 53.
21. Hall MD, McGee JL, McGee MC, Hall KA, Neils DM, Klopfenstein JD, Elwood PW. Cost-effectiveness of stereotactic radiosurgery with and without whole-brain radiotherapy for the treatment of newly diagnosed brain metastases. Journal of neurosurgery. 2014; 121 Suppl: 84-90.
22. Soffietti R, Kocher M, Abacioglu UM, Villa S, Fauchon F, Baumert BG, Fariselli L, Tzuk-Shina T, Kortmann RD, Carrie C, Ben Hassel M, Kouri M, Valeinis E, et al. A European Organisation for Research and Treatment of Cancer phase III trial of adjuvant whole-brain radiotherapy versus observation in patients with one to three brain metastases from solid tumors after surgical resection or radiosurgery: quality-of-life results. Journal of clinical oncology. 2013; 31: 65-72.
23. Cai L, Zhu JF, Zhang XW, Lin SX, Su XD, Lin P, Chen K, Zhang LJ. A comparative analysis of EGFR mutation status in association with the efficacy of TKI in combination with WBRT/SRS/surgery plus chemotherapy in brain metastasis from non-small cell lung cancer. Journal of neuro-oncology. 2014; 120: 423-30.
24. Park SJ, Kim HT, Lee DH, Kim KP, Kim SW, Suh C, Lee JS. Efficacy of epidermal growth factor receptor tyrosine kinase inhibitors for brain metastasis in non-small cell lung cancer patients harboring either exon 19 or 21 mutation. Lung cancer. 2012; 77: 556-60.
25. Namba Y, Kijima T, Yokota S, Niinaka M, Kawamura S, Iwasaki T, Takeda Y, Kimura H, Okada T, Yamaguchi T, Nakagawa M, Okumura Y, Maeda H, et al. Gefitinib in patients with brain metastases from non-small-cell lung cancer: review of 15 clinical cases. Clinical lung cancer. 2004; 6: 123-8.
26. Masuda T, Hattori N, Hamada A, Iwamoto H, Ohshimo S, Kanehara M, Ishikawa N, Fujitaka K, Haruta Y, Murai H, Kohno N. Erlotinib efficacy and cerebrospinal fluid concentration in patients with lung adenocarcinoma developing leptomeningeal metastases during gefitinib therapy. Cancer chemotherapy and pharmacology. 2011; 67: 1465-9.