
Introduction
Peritoneal dialysis (PD) is a renal replacement therapy commonly used around the world. PD uses the peritoneal membrane (PM) as semipermeable barrier for water and solute exchange. Ultrafiltration failure (UFF) along with acute peritonitis are major causes of the technique dropout [1].
The factors associated to PM failure include chronic and acute peritoneal inflammation caused by bacteria, glucose degradation products, advanced glycation end-products, acidic pH from PD fluids (PDF), and hemoperitoneum [2, 3]. Activated inflammatory cells subsequently drive fibrotic and pro-angiogenic factors and stimulates mesothelial cells (MCs) to start trans-differentiation. This process is so-called mesothelial-to-mesenchymal transition (MMT), in which MCs acquire a fibroblast-like phenotype [4], lose their basoapical and basolateral polarity and acquire migratory capacity towards the submesothelium, where they synthesize extracellular matrix (ECM) and vascular endothelial growth factor (VEGF), thus contributing to PM structural damage. Not surprisingly, numerous efforts have been made to improve the PDF biocompatibility and to investigate drugs capable of neutralizing the PM damage [3].
The CMs monolayer is the first barrier exposed to different peritoneal aggressions. Its injury provokes aberrant expression of several genes, making these cells protagonists of peritoneal damage [5]
β-adrenergic receptors (β-AR) are a class of G protein-coupled receptors that are targets of catecholamines (noradrenaline and epinephrine). Many cells including pleural MCs [6] express these receptors, which participate in many biological functions and its blockade might be beneficial in fibrosis pathway [7].
β-AR blockers were introduced into the market more than four decades ago in order to control cardiac arrhythmias and blood pressure in cardiac and hypertensive patients. In PD patients their use was limited due to possible development of severe secondary effects, such as peritoneal sclerosis and UFF [8, 9]. One of the suggested reasons for UFF was the splanchnic arteriolar vasoconstriction especially associated with non-selective β-blockers administration. The consequence of splanchnic arteriolar vasoconstriction is the reduction in portal venous pressure and the PD ultrafiltration rate. In fact it is the rationale for prescribing β-AR blockers to cirrhosis patients with bleeding esophageal varices [10, 11]. Since then, new indications for β-blockers have been restored. Robust studies [12] have shown that patients suffering from heart failure and/or ischemic heart disease have a higher survival rate using β-blockers.
For these reasons and given that cardiovascular diseases are very frequent in renal replacement therapy patients [13], the use of b-blockers, especially those of new generation, must be reconsidered [14].
Nebivolol, is a highly selective β1-adrenergic receptor (β1-AR) blocker, whose mechanism of action is to increase nitric oxide (NO) release by endothelial cells, promoting a vasodilator effect and reducing the vascular resistance [14]. Nebivolol also decreased collagen synthesis, angiogenesis and shows an anti-oxidant effect [15] [16]. Recently it has been demonstrated that pleural MCs express β-AR [6], which participates not only in the tissue fibrosis inhibition but also in pleural fluid transport such as pleural lymphatic flow effusions [7]. Therefore, it is plausible that peritoneal MCs express β-ARs and that Nebivolol could protect the PM from the changes induced by PD (MMT, fibrosis, angiogenesis and UFF).
Herein, we demonstrate for the first time that human MCs express the β1-AR. Using a PD mice model [17], we observed that, though the blockade of this receptor with Nebivolol. Some deleterious effects associated with PD are reduced, such as MMT, PM fibrosis, angiogenesis and UFF, with an increase in the MCs fibrinolytic capacity.
Results
Human omentum derived mesothelial cells (HOMCs) express b1-AR and its blockade with Nebivolol partially inhibits the MMT
Herein, we demonstrate for the first time that HOMCs show β1-AR (Figure 1A, 1B) and that Nebivolol (10 nM) decreased its expression. Recent publications show that β1-AR blockade is generally associated with anti-fibrotic and anti-angiogenic effects [18, 19]. Given that both effects are commonly associated to MMT and PM failure, we decided to explore the effect of Nebivolol on HOMCs stimulated with TGF-β. We measured the expression of genes that are usually altered during the MMT process (down-regulation of E-cadherin and up-regulation of Snail, fibronectin, pro-collagen and α-SMA, among others) [4].
The co-treatment with Nebivolol (10 nM) and TGF-β (1 ng/ml) did not inhibit the MMT phenotype (Figure 1C), however, this drug kept the E-cadherin expression at the level of 60% of its control value (Figure 1D). Likewise Nebivolol inhibited the up-regulation of Snail, fibronectin, pro-collagen and alpha smooth muscle actin (α-SMA), in a dose dependent manner (Figure 1E-1H).
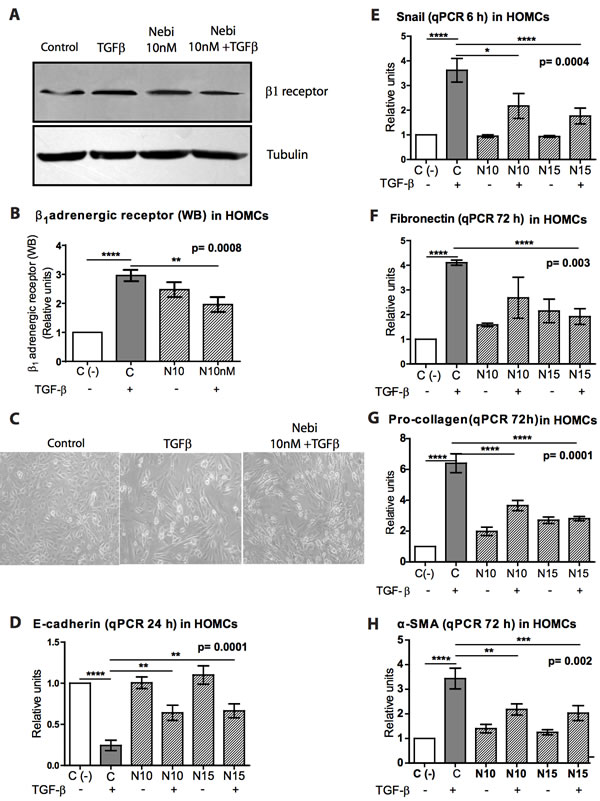
Figure 1: Effect of Nebivolol on b1-adrenergic receptor of HOMCs. A. Immunoblotting analysis of β1-adrenergic receptor in reference to tubulin in protein lysates from omentum cells cultures treated, or not, with Nebivolol at 10 nM with or without TGF-β (1 ng/ml). B. The corresponding graph is shown. C. Representative pictures from cultures of omentum (control), TGF-β- and TGF-β + Nebivolol-treated cells D.-H. qPCR analyses of mRNA expressions of different MMT from omentum cell treated, or not, with Nebivolol at different concentrations (N10 = 10 nM or N15 = 15 nM) with or without TGF-β (1 ng/ml). (D) E-Cadherin (24 h), (E) Snail (6 h), (F) fibronectin (72 h), (G) pro-collagen (72 h) and (H) α-SMA (72 h). The markers were analyzed at different time points taking into consideration that the time of their high expression varies among them. Bars graphics represent means ± SE (n = 3).
Nebivolol improved the fibrinolytic capacity and decreased the VEGF and IL-6 levels in HOMCs and human effluent derived mesothelial cells (HEMCs)
The fibrinolytic capacity of MCs is essential to maintain the production/degradation balance of extracellular matrix components in order to avoid the formation of peritoneal adhesions and fibrosis. Experimentally, the MMT induced by TGF-β1 was also associated to increase in plasminogen activator inhibitor-1 (PAI-1) level which is a strong anti-fibrinolytic molecule. Nebivolol tend to decrease PAI values in HOMCs supernatant, although this decrease does not reach statistical difference (Figure 2A). Moreover, the levels of its natural inhibitor, the tissue-type plasminogen activator (tPA), the most potent fibrinolytic factor known, were decreased upon TGF-β1 treatment. Nebivolol tended to restore the tPA baseline levels in HOMCs (Figure 2B) increasing tPA/PAI-ratio, a commonly used clinical marker for fibrinolytic capacity (Figure 2C).
Similar and even more powerful effects were observed in transdifferentiated HEMCs treated with Nebivolol. This pro-fibrinolytic effect also showed a dose-dependent pattern (Figure 2G to 2I).
TGF-β is a master molecule in both MMT induction and fibrosis pathogenesis. Therefore, we measured TGF-β levels in transdifferentiated HEMCs supernatant treated with Nebivolol. We did not find significant effect of Nebivolol on TGF-β supernatant levels (Figure 2F). VEGF and IL-6 are molecules related to angiogenesis and inflammation respectively. Treatment with Nebivolol decreased both VEGF and IL-6 supernatant levels in TGF-β-stimulated HOMCs (Figure 2D and 2E). These results suggest that Nebivolol improves the fibrinolytic capacity and might have an anti-angiogenic and anti-inflammatory effect.
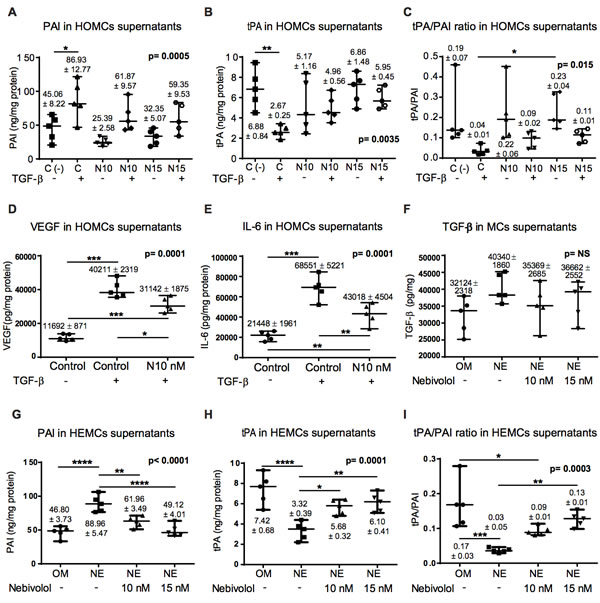
Figure 2: Effect of Nebivolol on fibrinolytic capacity, cytokines and growth factors in HOMCs and HEMCs. A., B. Expression of the fibrinolytic factors PAI and tPA by HOMCs treated or not with TGF-ß and with different doses of Nebivolol (10 or 15nM) during 48 h. C. The tPA/PAI ratio as fibrinolytic capacity marker was also determined. D. and E. VEGF and IL-6 supernatant levels in HOMCs treated with TGF-ß. F. TGF-ß levels in transdifferentiated HEMCs supernatant. G. and H. Expression of the fibrinolytic factors PAI and tPA by HEMCs treated with different doses of Nebivolol (10 or 15nM) during 48 h. I. Levels of tPA/PAI ratio in HEMCs. The levels of these factors were measured in HOMCs and HEMCs supernatants by ELISA and results are depicted as nanograms per milligrams of total cellular proteins. Data point graphics represent the absolute value of each determination and lines the median, lower and upper range. Numbers on the top of graphics represent the mean ± SE (n = 5). P values < 0.05 are considered statistically significant using one-way Anova test, and are depicted in the graphs. To account for multiple comparisons, the Bonferroni post-test was used to compare all pairs of means. The symbols represent the statistical differences between the groups (*p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001). NE = non epithelioid HEMCs; NS = no significant.
Nebivolol ameliorated peritoneal membrane alterations induced by dialysis fluid exposure in a PD model in mouse
We analyzed whether Nebivolol might prevent the PM deterioration in PD mice exposed to PDF. Histological analysis of parietal peritoneal biopsies from PDF group (six in each group) showed a loss of MCs monolayer (cytokeratin positive) and increased PM thickness when compared with control mice group. Interestingly, oral administration of Nebivolol to PD-treated mice (PDF + Nebivolol group) significantly reduced the PM thickness and prevented the loss of MCs monolayer mesothelial (Figure 3A, 3B).
Another histological characteristic of the peritoneum during PD was the accumulation of fibroblasts expressing α-SMA in the submesothelial compact zone; some of them co-expressed cytokeratin (CK), indicating their mesothelial origin (MMT). In PDF group we found an important accumulation of MCs with double positive staining for CK (red) and α-SMA (green) located in the superficial and submesothelial areas (see arrows). In control and PDF + Nebivolol groups, co-stained cells were almost undetectable (Figure 3C).
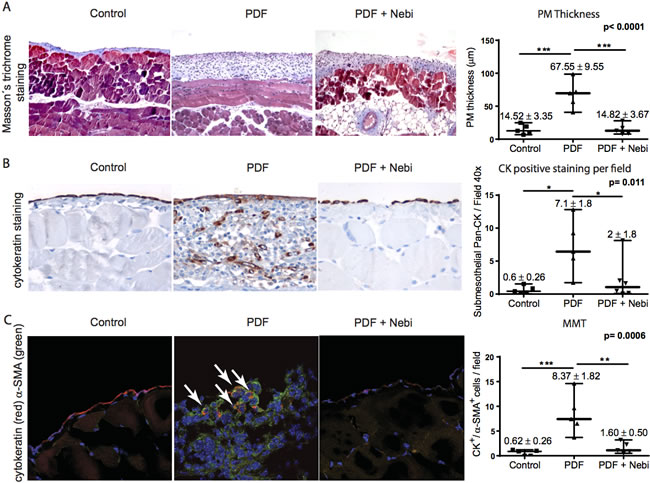
Figure 3: In vivo analysis of the peritoneal membrane alterations. C57BL/6 female mice were treated or not with PDF or PDF + Nebivolol for 30 days (six mice per group). A. Fibrosis assessment by Masson’s Trichrome staining. Blue staining indicates collagen depositions. Quantification of peritoneal fibrosis is shown in the corresponding graph. B. Immunohistochemistry staining of cytokeratin and quantification of the total cytokeratin positive stained cells in the peritoneal membrane. C. Immunofluorescence microscopy analysis of parietal peritoneal tissue sections, stained for cytokeratin (red), and α-smooth muscle actin (α-SMA) (green) and cells nuclei with 4,6-diamidino-2-phenylindole (DAPI) (blue) counterstaining. Number of double positive cells for α-SMA and cytokeratin as per field are shown. Ten randomized calculations per mouse were performed. Data point graphics represent the absolute value of each determination and lines the median, lower and upper range. Numbers on the top of graphics represent the mean ± SE. P values < 0.05 are considered statistically significant (one-way Anova test). To account for multiple comparisons, the Bonferroni post-test was used to compare all pairs of means. The symbols represent the statistical differences between the groups (*p < 0.05, **p < 0.01, ***p < 0.001).
Nebivolol decreased the peritoneal angiogenesis and maintained the water and solutes transport capacity
Angiogenesis is an important component for PM failure and it is associated with alterations in the peritoneal water transport [1]. Recently it has been reported that Nebivolol can regulate the blood vessels formation in cardiovascular system [20]. Herein, we analyzed the effect of Nebivolol on PM angiogenesis and peritoneal water and solute transport. PDF group showed a higher number of CD31+ cells in the submesothelial area, indicating an intense neovascularization compared to control and Nebivolol group (Figure 4A, 4B).
In relation to peritoneal transport, after the exposure of the mice peritoneal cavity to 2 ml of PDF during 30 minutes, the PDF group showed an important reduction in UF rate compared to the remaining groups (Figure 4C). However, we did not observe statistical significant differences over time in peritoneal solute transport (urea, creatinine and glucose) among the groups (Figure 4E, 4F, 4G). Likewise, VEGF levels were similar between groups (Figure 4D).
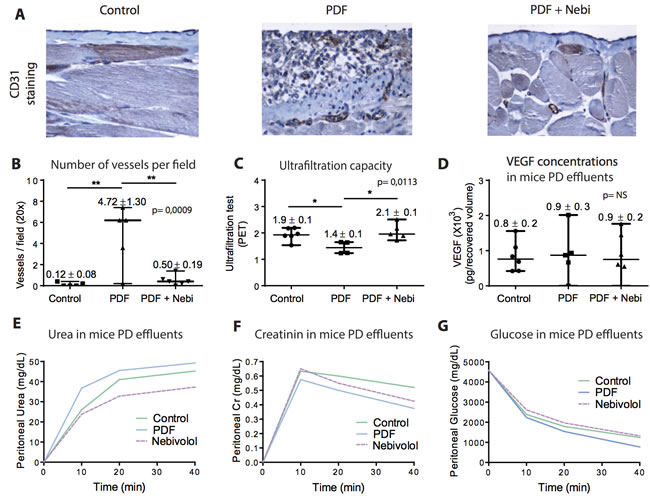
Figure 4: In vivo analysis of the alterations related to angiogenesis and the ultrafiltration capacity of the peritoneal membrane. A. Immunohistochemistry staining of CD31 (vessels) and B. quantification of the total CD31 positive stained cells in the peritoneal membrane. C. Ultrafiltration capacity analysis (PET test) (30 minutes) after injecting mice with PDF in the last day of the experiment. D. Concentrations of VEGF (pg/recovered volume) measured by ELISA in the peritoneal effluents of mice. No significant (NS) differences were observed. E.-G. Kinetic curves of urea, creatinine and glucose, respectively, in the different groups of mice measured at 10, 20 and 40 minutes. Data point graphics represent the absolute value of each determination and lines the median, lower and upper range. Numbers on the top of graphics represent the mean ± SE. P values < 0.05 are considered statistically significant using one-way Anova test, and are depicted in the graphs. To account for multiple comparisons, the Bonferroni post-test was used to compare all pairs of means. NE: MCs with non-epithelioid phenotype. The symbols represent the statistical differences between the groups (*p < 0.05, **p < 0.01, ***p < 0.001).
Nebivolol improved the fibrinolytic capacity in the peritoneal cavity in a PD mice model
Given the improvement of the fibrinolytic capacity found in HOMCs and transdifferentiated HEMCs cultured with Nebivolol or Nebivolol + TGF-β (Figure 2), we measured PAI and tPA concentrations in mice PD effluents after 30 days in PD. PDF exposure was associated to increase PAI (Figure 5A) and decrease tPA levels (Figure 5B), leading to a decrease in fibrinolytic capacity in the peritoneal cavity. In contrast, mice treated with Nebivolol maintained or improved fibrinolytic capacity in the peritoneal cavity.
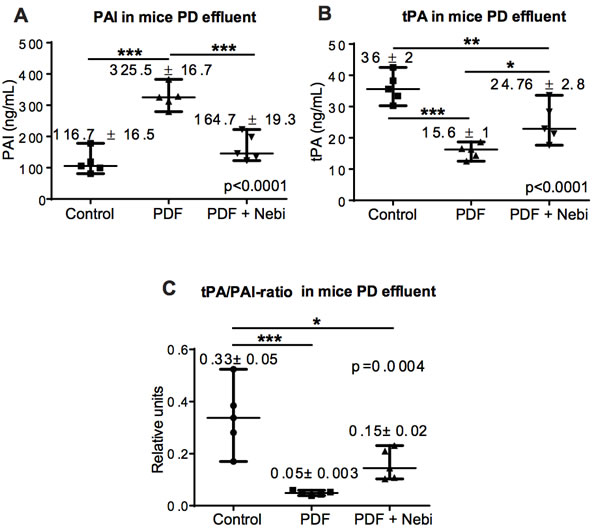
Figure 5: Fibrinolytic capacity in vivo. A.-B. Expression of the fibrinolytic factors PAI and tPA in the different mice groups. The levels of these factors were measured in the effluents by ELISA and results are depicted as ng/mL. C. The tPA/PAI ratio, an important marker of fibrinolytic capacity, is also shown. Data point graphics represent the absolute value of each determination and lines the median, lower and upper range. Numbers on the top of graphics represent the mean ± SE. P values < 0.05 are considered statistically significant using one-way Anova test, and are depicted in the graphs. To account for multiple comparisons, the Bonferroni post-test was used to compare all pairs of means. The symbols represent the statistical differences between the groups (*p < 0.05, **p < 0.01, ***p < 0.001).
Nebivolol partially restored the inflammatory status in the peritoneal cavity from mice treated with PD
Inflammation in peritoneal cavity is one of the most important factors that trigger MMT and PM damage. Bioincompatible PDFs, peritonitis and/or hemoperitoneum are primarily responsible for peritoneal immune activation [2, 3]. Given that Nebivolol seems to have an anti-inflammatory effect on cardiovascular system [21], we decided to measure inflammatory markers in the peritoneal cavity of mice treated with PD. We did not find differences in total peritoneal cells, pro-inflammatory cytokines (IL-6) and anti-inflammatory cytokines (TGF-β and IL-10) between the groups treated or not with Nebivolol. Total cell count, PDF vs. PDF + Nebovilol (7.5 ± 0.4 vs. 8.8 ± 1.5 x 106 total cell, NS), IL-6 (135 ± 48 vs. 30 ± 14 x103 pg/recovered volume, p = 0.07), TGF-β (8785 ± 3810 vs. 8297 ± 4295 pg/recovered volume, NS) and IL10 (7.5 ± 4.2 vs. 4.6 ± 2.5 x 103 pg/recovered volume, NS), respectively. However, Nebivolol treatment prevented the increase in IL8 values associated to PDF exposure, (674.9 ± 228.6 vs. 165.5 62.1 pg/recovered volume, p = 0.02).
Nebivolol did not modify the NO3- levels in the peritoneal cavity of mice treated with PD
Nebivolol treatment has generally been associated with increased NO synthesis [22]. NO is a potent vasodilator and stimulates tissue angiogenesis via VEGF and HIF dependent pathway [23]. However, we did not find differences in NO3- (a marker of NO levels) concentration in mice PD effluent among the groups. PDF vs. PDF + Nebovilol groups (175.3 ± 29.8 vs. 139.7 ± 45.2 mm/mL, NS, respectively).
Discussion
PD technique is based on the ultrafiltration capacity and solute clearance of the PM, but its exposure to PDFs leads to PM deterioration. This damage starts with inflammation and MMT of MCs in the PM surface, causing MCs migration, fibrosis, angiogenesis and, consequently, UFF. PD patient´s survival frequently depends on maintaining the PM integrity, so its preservation through the employment of more biocompatible PDFs or pharmacological agents, preventing their deleterious effects, is essential for the maintenance of the PD technique [2].
For this purpose and considering that Nebivolol has shown positive cardiovascular effects in non-uremic patients [13], we conduct the present research.
The use of the first β-AR blockers in patients undergoing PD had to be limited due to the possible risk of developing functional and structural PM complications [8, 9]. However there is no clinical experience with the use of new β-AR blockers in PD Patients that contrary seem to have very beneficial systemic effects. The protective effects of Nebivolol on cardiovascular functions have been associated to NO release by endothelial cells, and by its anti-oxidant and anti-fibrotic effects, associated with collagen synthesis reduction and its anti-angiogenic capacity [15]. These protective properties are regulated by the β-AR modulation [16]. Herein, we demonstrate for the first time that peritoneal MCs express β1-AR.
Recent data indicate that MCs are very versatile because they express a large number of receptors such as estrogen, PPAR-γ or angiotensin-II [24-26]. Since pleural and peritoneal MCs have the same phylogenetic origin, the discovery of β2-AR in pleural MCs is consistent with our results [6] and opens new therapeutic opportunities.
Given the central role of the MMT process in the initiation and progression of peritoneal injury in PD patients [7], [8], [34], we have analyzed the effects of Nebivolol on the MMT of MCs in vitro and in a mice PD model. We found that Nebivolol did not inhibit totally the MMT in vitro but decreased the ECM synthesis. In addition, it partially prevented the down-regulation of E-cadherin and up-regulation of Snail when MCs were treated with TGF-β (Figure 1).
The loss of fibrinolytic capacity and MCs migration are usually associated with MMT [24]. The following sentence should be: Recently, Shan T. et al. [27] demonstrated that the natural agonist of β-AR, norepinephrine, inducesepithelial-to-mesenchymal transition (EMT) in a gastric adenocarcinoma cell lines, so the blockade of β-AR could inhibit this process.
Herein we demonstrated that Nebivolol treatment increased the tPA-levels in HOMCs and HEMCs supernatant, and effluent of mice in PD. tPA is a natural inhibitor of PAI and its balance maintains an anti-adherent surface. Moreover, elevation of tPA makes a more fluid matrix surface increasing the cell migratory by MMP2 up-regulation, and is also able to inhibit the MMT via increases in HGF levels [28]. HGF and BMP7 are natural inhibitors of TGF-β, the master molecule of tissue fibrosis and maximum initiator of the EMT [29].
One would think that the increase in cell migratory ability to submesothelium is a negative phenomenon, but the first requirement to migrate is suffer MMT and tPA blocks MMT via HGF / BMP7 increment [28], therefore tPA increase is always positive.
We demonstrated that Nebivolol also improved the fibrinolytic capacity of MCs mediated by an increase in tPA levels, which is essential to maintain an adequate balance of extracellular matrix components, thereby protecting from the tissue fibrosis and peritoneal adhesions formation. Our results in HEMCs and HOMCs stimulated with TGF-β1 indicate that tPA production, a powerful fibrinolytic factor, decreased together with an increase in PAI, its antagonist. Interestingly, treatments with Nebivolol restored the tPA basal levels or even increased its synthesis above the basal level, decreased the PAI levels and restored the tPA / PAI-ratio. These findings are consistent with the results of Tarighi et al, [30] who found an improvement in the fibrinolytic serum profile of hypertensive patients treated with Nebivolol.
Another way by which Nebivolol would inhibit MMT or its deleterious effects is increasing NO [31]. Although we did not observe significant differences in the levels of NO in the mice PD effluent, another possible route by which Nebivolol could inhibit the MMT is increasing the NO synthesis. In mesangial cell culture, a link between NO and regulation of genes related to ECM production has been proposed [32]. NO is able to down-regulate the mRNA and protein levels secretion of modular calcium-binding protein-1 (SMOC-1), and its silencing led to a significant reduction in the expression of TGF-β, PAI-1 and other genes involved in tissue fibrosis and EMT. The downregulation of SMOC-1 was also linked with a disruption in TGF-β signaling by preventing from binding of Smad proteins to the Smad binding element in DNA [31]. In endothelial cells, NO has also been shown to inhibit TGF-β gene expression, through interference with Smad signaling. NO inhibited Smad-2 phosphorylation and nuclear translocation and led to Smad-2 degradation via the ubiquitin proteasome pathway. Moreover, it has recently been demonstrated that Nebivolol exerts an anti-inflammatory, anti-fibrotic and anti-migratory effects blocking the same signaling pathway (TGF-ß, MMP-2 and MMP9)[21, 33].
Peritoneal inflammation is crucial for the development of PM fibrosis and EMT [1]. Although in this study we observed no statistically significant reduction neither in the pro-inflammatory cytokine IL-6 production nor in the number of total cells in PD-effluent from Nebivolol-treated mice. We did observe differences in IL8 concentrations; this fact and the sum of the sum of pleiotropic effects of Nebivolol may explain its protective effect on PM.
Angiogenesis is another component from PM failure. We found a small number of submesothelial vessels in the group of PD mice treated with Nebivolol. To our knowledge Nebivolol is not considered an anti-angiogenic agent, but it might indirectly attenuate vessels formation through a decrease in tissue fibrosis and MMT. In addition β-AR blockade is associated with anti-angiogenic effects [34, 35].
Since the 80s decade the use of β-blockers in PD patients has been controversial for their association with ultrafiltration rate reduction by decreasing splanchnic blood flow (vasoconstriction) and, possibly, by peritoneal fibrosis induction [8, 9]. However the third generation of β-blockers such as Nebivolol does not produce such effects, in fact Nebivolol increases endothelial NO release inducing vasodilation, anti-oxidation and improving the systemic fibrinolytic capacity [36, 37]. Robust clinical evidences favor that Nebivolol could be approved in US to treat hypertension and in Europe to treat hypertension and heart failure with reduced ejection fraction [37].
Cardiovascular disease remains the leading cause of death in patients on dialysis [38]. The exact causes for this premature vascular aging are complex and include major incidence of hypertension, dyslipidemia, diabetes, oxidative stress, systemic inflammation and tendency to the formation of vascular thrombi with decreased endothelial fibrinolytic capacity. This network has as common factor: the endothelial dysfunction [39], which is associated with deficit of NO by accumulation of a uremic toxin called NG monomethyl-L-arginine (L-NMMA) and asymmetric dimethylarginine (ADMA) [40].
Both ADMA and L-NMMA are the result of posttranscriptional methylation of L-arginine residues by protein arginine methyltransferases and are released in their free form following protein hydrolysis. ADMA production is about 10-fold that of L-NMMA and is elevated in patients with chronic renal failure [40]. Plasma levels of ADMA predict adverse cardiovascular events in uremic patients [41], therefore ADMA has been classified as a “uremic toxin” and exhibits adverse cardiovascular effects [39].
published an interesting review and meta-analysis where they analyze the effects of beta-adrenergic antagonists in patients with chronic kidney disease concluding that the beta-blockers treatment in patients with chronic renal failure and chronic systolic heart failure improved all-cause mortality. We believe that in the case of Nebivolol this effect could be due to improvement in the NO synthesis, in the endothelial fibrinolytic capacity and its anti-oxidant and anti-hypertensive effect.
Considering the results presented here and existing pharmacological evidence regarding the cardiovascular protective effects of Nebivolol, we can suggest that this drug may be an excellent candidate for use in PD patients as PM and cardiovascular protector. Future studies with a prospective design, matched and double-blind (if possible) should analyze its therapeutic potential in uremic patients.
Conclusions
Nebivolol displays a protective effect against PM damage induced by PD fluids. This protection involves a partial anti-MMT, anti-fibrotic, anti-angiogenic and pro-fibrinolytic effects. Importantly, the protective cardiovascular effects of this drug make it a very attractive candidate to be used in PD patients.
Materials and Methods
Isolation, culture and treatment of HOMCs and HEMCs
HOMCs were obtained from omental samples taken from patients undergoing elective abdominal surgery and from effluents of PD patients as described previously [42-45].
HEMCs were isolated from a PD overnight exchange of patients with more than 3 months in PD as previously described by us [46].
The purity of the omentum- and effluent-derived MCs cultures was determined by the expression of the standard mesothelial markers: intercellular adhesion molecule (ICAM)-1, calretinin and cytokeratins. These MCs cultures were negative for von-Willebrand factor and CD45, ruling out any contamination by endothelial cells or macrophages [43-45].
To induce MMT ex vivo, HOMCs were seeded on wells coated with collagen I (50 mg/ml, Roche Diagnostics GmbH) and treated for 48 h with human-recombinant TGF-β1 (1 ng/ml, R&D Systems), a commonly used in vitro model of MMT [26, 43-45, 47].
To evaluate the effect of β-AR blockade on MMT prevention, HOMCs were co-treated with TGF-β and Nebivolol (Menarini, Italy) at of 10 and 15 nM during 6, 48 and 72 hours, as referred by others [48]. We also analyzed the effect of Nebivolol on spontaneously transdiffferentiated mesothelial cells isolated from peritoneal effluent of PD patients; HEMCs were also treated with Nebivolol (10 and 15 nM) and analyzed at 48 hours. These cells were characterized by non-epitheliod morphology, E-cadherin down-regulation and Snail and mesenchymal markers up-regulated.
The present study adjusts to the Declaration of Helsinki and was approved by the Ethics Committee of the Hospital Universitario de La Princesa, Madrid, Spain. Informed written consent was obtained from all the patients (PD effluent and omentum donors).
Western blot analysis and quantitative RT-PCR
For western blotting, MCs cultures were lysed in a buffer containing 1% sodium deoxycholate and 0.1% sodium dodecyl sulfate (SDS). The total protein was quantified using a protein assay kit (Bio-Rad). Total cell protein (50 mg) was resolved on 8-10% SDS-polyacrylamide gels and transferred onto nitrocellulose membranes, which were then blocked with fat-free milk and probed with specific antibodies against b1 adrenergic receptor (Santa Cruz Biotechnology). Images of the blots were acquired with a LAS-1000 Charge Coupled Device camera (Fujifilm).
For quantitative RT-PCR analysis, MCs were lysed in TRI Reagent (Ambion), and RNA was extracted according to manufacturer’s instructions. Complementary-DNA was synthesized from 2 µg of total RNA by reverse transcription (RNA PCR Core Kit, Applied Biosystems). Quantitative PCR was carried out in a Light Cycler 2.0 using a SYBR Green Kit (Roche Diagnostics GmbH) and specific primers sets for human Snail, E-cadherin, fibronectin, pro-collagen-I, α-SMA and histone H3. Samples were normalized with respect to the value obtained for H3. All experiments were repeated at least three times. For RT-PCR determinations in each experiment it was assigned a value of one to a control omentum (C-) from which the relative values of the remaining groups were calculated. The primer sets used are depicted in Table S1.
Fibrinolytic capacity and enzyme-linked immunoassays in HOMCs and HEMCs
To evaluate the effect of Nebivolol on fibrinolytic capacity, HOMCs and HEMCs were cultured with TGF-β Nebivolol 10 and 15 nM during 48 hours. The plasminogen activator inhibitor type-1 (PAI-1) and tissue-type plasminogen activator (tPA) concentration were measured in culture supernatants by ELISA kits (PAI-1, BioVentor Laboratorni Medicina, a.s. Karasek, Czech Republic) and (R&D Systems Inc; Minneapolis, USA), respectively.
Using the same technique we also measure VEGF-A, TGF-β and IL-6 in MCs culture supernatants (VEGF-A and TGF-β; R&D Systems Inc; Minneapolis, USA and IL-6: BD Biosciences Pharmingen, San Diego, CA).
Peritoneal dialysis fluid exposure model in mice
This study was performed in 21 non-uremic female C57BL/6 mice (N = 18, aged 12-14 weeks; Harlan Interfauna Iberica, Spain). The experimental protocol was approved by the Animal Ethics Committee of the Unidad de Cirurgía Experimental of Hospital La Paz, Madrid, Spain. The animals had free access to food and water. A customized peritoneal catheter (Access Technologies) was surgically placed in all mice as previously described by González-Mateo, et al [17]. After one week, animals were divided into three groups: 6 controls (exposed to the catheter alone), 6 animals to receive daily infusions of 2 ml of 4,25% glucose PDF (Stay Safe, Fresenius Medical Care) and 6 animals to receive 2 ml PDF peritoneal infusions and Nebivolol diluted in water (8 mg/kg/day in 15 µL of volume) orally. The dropout animals were mainly due to catheter displacement (one from each group).
Histological analysis
Peritoneum fragments were fixed in Bouin’s fixative for 24 h and then embedded in paraffin. 5 µm sections were stained with Masson’s Trichrome for submesothelial thickness determination. Thickness was measured microscopically every 60 mm for the whole length of the biopsy (Leica CTR6000 with LAS-AF6000; Leica Microsystems).
For immunofluorescence stainings, tissue was embedded in OCT (Optimal Cutting Temperature) medium and cut into 5 mm sections. The frozen sections were fixed for 15 minutes in 4% formaldehyde in PBS and blocked with 10% horse serum for 1 hour in PBS with 0.3% Triton X-100. Then samples were stained with primary antibodies anti-pan cytokeratin (CK), α-SMA (Sigma-Aldrich, Saint Louis, Missouri, USA) and CD31 (Beckton Dickinson). Afterwards, they were conjugated with zenon compounds (Invitrogen). Nuclei were stained with DAPI. Micrography was performed with a fluorescence microscope (Leica CTR6000 with LAS-AF6000).
For immunohistochemistry stainings, biopsies were fixed in paraformaldehyde, embedded in paraffin and cut into 3 µm sections. After paraffin remotion with xylol treatment, samples were heated to expose any masked antigens using a Real Target Retrieval Solution containing citrate buffer (pH 6.0, Dako). Samples were pre-treated with Real Peroxidase-Blocking Solution (Dako) to block the endogenous peroxidase. Tissue sections were stained with anti-pan cytokeratin or anti-CD31 and counterstained with nuclear hematoxylin. Images were analyzed by computerized digital image analysis (AnalySIS, Soft Imaging System). Positive staining was counted and expressed as the mean of 10 independent counts for each animal, quantified at 20x using the analysis program Image-J 1.37c (National Institute of Health, USA).
Peritoneal function assessment
After the 30-days treatment, 2 ml of PDF were instilled into the peritoneal cavity and after 10, 20 and 40 minutes, 300 µl of effluent were obtained through direct puncture of the abdominal wall for urea, Creatinine and glucose dosing (Servicio de Bioquímica Clínica from Laboratorio de Bioquímica from Hospital Universitario La Paz, Madrid, Spain). On next day, 2 ml of PDF were infused into the peritoneal cavity and after 30 minutes animals were anesthetized by halothane inhalation and sacrificed by cervical dislocation. Total peritoneal effluent volume was collected and weighed on a precision balance for the evaluation of ultrafiltration capacity. Afterwards, effluents were centrifuged and total cells were counted. Effluents were stored at -80ºC to later analyze different parameters.
Evaluation of the fibrinolytic capacity in of HOMCs, HEMCs and mice mouse PD effluent
To evaluate the fibrinolytic capacity of human MCs (HOMCs and HEMCs), these cells were co-cultured with TGF-β1 and Nebivolol 10 and 15 nM during another 48 h Cell culture supernatants were collected and stored to -80ºC. Concentrations of plasminogen activator inhibitor type-1 (PAI-1, BioVentor Laboratorni Medicina, a.s. Karasek, Czech Republic) and of tissue-type plasminogen activator (tPA, R&D Systems) were measured using ELISA kit following manufacturer’s instructions. The values in supernatant are expressed in ng/mg protein. Mice PD effluent samples were collected after 30 days of PD. In PD mice effluent, PAI and tPA were also determined using the same Elisa Kits. The values are expressed in ng/mL (UF volume).
Enzyme-linked immunoassays (ELISA) and nitrates (NO3-) in MCs cultures and mice PD effluents
TGF-β1, VEGF and IL-6 protein levels were measured in human MCs supernatants by ELISA according to manufacturer´s instructions. In mice, PD effluent samples were collected after 30 days in PD. VEGF-A, TGF-β1, IL-6, IL-8 and IL-10 were measured by ELISA, (VEGF-A and IL-8: Bender Med Systems, Vienna, Austria; TGF-β1: R&D Systems, Minneapolis, USA; and IL-6 and IL-10: BD Biosciences Pharmingen, San Diego, CA). NO3- was also determined in MCs supernatant and PD effluent by capillary electrophoresis as described [49]. The values are expressed in pg/total recovered volume.
Statistical analysis
In Figure 1, the results (qPCR) are presented as mean ± SE in bars graphics. In Figures 2 to 5 the results are showed in data point graphics representing the absolute value of each determination and lines the median, lower and upper range. Numbers on the top of graphics represent the mean ± SE. The difference between the two groups was calculated using the nonparametric Mann-Whitney rank sum. The global difference between tree groups was calculated using ANOVA one way and Bonferroni post-hoc test. We used the SPSS statistic package version 14.5 (Chicago, IL) and GraphPad Prism version 5.0 (La Jolla, CA). P < 0.05 was considered statistically significant.
Funding
This work was supported by Menarini Spain, grants PI 12/01175 from Fondo de Investigaciones Sanitarias (FIS) Instituto Carlos-III to A.A.; SAF2013-47611R from the Ministerio de Economía y Competitividad and grant S2010/BMD-2321 (FIBROTEAM Consortium) from Comunidad Autónoma de Madrid to M.L.-C.; G.L. was fully supported from the European EuTRiPD Marie Curie project.
Acknowledgments
We thank Marta Ramirez for the assistance in MCs culture, Vanessa Fernández and Luiz Stark for the assistance with mouse experiments.
conflicts of interest
Nothing to disclose
References
1. Krediet RT, Lindholm B and Rippe B. Pathophysiology of peritoneal membrane failure. Perit Dial Int. 2000; 20 Suppl 4:S22-42.
2. Margetts PJ and Bonniaud P. Basic mechanisms and clinical implications of peritoneal fibrosis. Perit Dial Int. 2003; 23:530-541.
3. Aroeira LS, Aguilera A, Sanchez-Tomero JA, Bajo MA, del Peso G, Jimenez-Heffernan JA, Selgas R and Lopez-Cabrera M. Epithelial to mesenchymal transition and peritoneal membrane failure in peritoneal dialysis patients: pathologic significance and potential therapeutic interventions. J Am Soc Nephrol. 2007; 18:2004-2013.
4. Yanez-Mo M, Lara-Pezzi E, Selgas R, Ramirez-Huesca M, Dominguez-Jimenez C, Jimenez-Heffernan JA, Aguilera A, Sanchez-Tomero JA, Bajo MA, Alvarez V, Castro MA, del Peso G, Cirujeda A, Gamallo C, Sanchez-Madrid F and Lopez-Cabrera M. Peritoneal dialysis and epithelial-to-mesenchymal transition of mesothelial cells. N Engl J Med. 2003; 348:403-413.
5. Lopez-Cabrera M. Mesenchymal Conversion of Mesothelial Cells Is a Key Event in the Pathophysiology of the Peritoneum during Peritoneal Dialysis. Adv Med. 2014; 2014:473134.
6. Sironi C, Bodega F, Armilli M, Porta C, Zocchi L and Agostoni E. beta2-Adrenergic receptors and G-protein-coupled receptor kinase 2 in rabbit pleural mesothelium. Respiratory physiology & neurobiology. 2010; 173:189-191.
7. Zocchi L. Physiology and pathophysiology of pleural fluid turnover. The European respiratory journal. 2002; 20:1545-1558.
8. Stegmayr BG. Beta-blockers may cause ultrafiltration failure in peritoneal dialysis patients. Perit Dial Int. 1997; 17:541-545.
9. Brown P, Baddeley H, Read AE, Davies JD and McGarry J. Sclerosing peritonitis, an unusual reaction to a beta-adrenergic-blocking drug (practolol). Lancet. 1974; 2:1477-1481.
10. Garcia-Tsao G, Sanyal AJ, Grace ND and Carey W. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007; 46:922-938.
11. Kroeger RJ and Groszmann RJ. Increased portal venous resistance hinders portal pressure reduction during the administration of beta-adrenergic blocking agents in a portal hypertensive model. Hepatology. 1985; 5:97-101.
12. Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW and Yancy CW. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009; 119:e391-479.
13. Go AS, Chertow GM, Fan D, McCulloch CE and Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004; 351:1296-1305.
14. J C. A review of the safety and efficacy of nebivolol in the mildly hypertensive patient. Vasc Health Risk Manag 2007; 3:909-917.
15. Mason RP, Jacob RF, Corbalan JJ, Szczesny D, Matysiak K and Malinski T. The favorable kinetics and balance of nebivolol-stimulated nitric oxide and peroxynitrite release in human endothelial cells. BMC Pharmacol Toxicol. 2013; 14:2050-6511.
16. Cole SW and Sood AK. Molecular pathways: beta-adrenergic signaling in cancer. Clin Cancer Res. 2012; 18:1201-1206.
17. Gonzalez-Mateo GT, Loureiro J, Jimenez-Hefferman JA, Bajo MA, Selgas R, Lopez-Cabrera M and Aroeira LS. Chronic exposure of mouse peritoneum to peritoneal dialysis fluid: structural and functional alterations of the peritoneal membrane. Perit Dial Int. 2009; 29:227-230.
18. Yucel S, Bahcivan M, Gol MK, Erenler BH, Kolbakir F and Keceligil HT. Reduced intimal hyperplasia in rabbits via medical therapy after carotid venous bypass. Tex Heart Inst J. 2009; 36:387-392.
19. Pires MJ, Rodriguez-Pena AB, Arevalo M, Cenador B, Evangelista S, Esteller A, Sanchez-Rodriguez A, Colaco A and Lopez-Novoa JM. Long-term nebivolol administration reduces renal fibrosis and prevents endothelial dysfunction in rats with hypertension induced by renal mass reduction. J Hypertens. 2007; 25:2486-2496.
20. Mason RP, Jacob RF, Corbalan JJ, Szczesny D, Matysiak K and Malinski T. The favorable kinetics and balance of nebivolol-stimulated nitric oxide and peroxynitrite release in human endothelial cells. BMC Pharmacol Toxicol. 2013; 14:48.
21. Celik T, Iyisoy A, Kardesoglu E and Fici F. The anti-inflammatory effects of nebivolol in human coronary smooth muscle cells: clinical implications. International journal of cardiology. 2009; 133:415-416.
22. Agabiti-Rosei E, Porteri E and Rizzoni D. Arterial stiffness, hypertension, and rational use of nebivolol. Vasc Health Risk Manag. 2009; 5:353-360.
23. Hu T, Beattie WS, Mazer CD, Leong-Poi H, Fujii H, Wilson DF, Tsui AK, Liu E, Muhammad M, Baker AJ and Hare GM. Treatment with a highly selective beta(1) antagonist causes dose-dependent impairment of cerebral perfusion after hemodilution in rats. Anesth Analg. 2013; 116:649-662.
24. Loureiro J, Sandoval P, del Peso G, Gonzalez-Mateo G, Fernandez-Millara V, Santamaria B, Bajo MA, Sanchez-Tomero JA, Guerra-Azcona G, Selgas R, Lopez-Cabrera M and Aguilera AI. Tamoxifen ameliorates peritoneal membrane damage by blocking mesothelial to mesenchymal transition in peritoneal dialysis. PloS one. 2013; 8.
25. Kiribayashi K, Masaki T, Naito T, Ogawa T, Ito T, Yorioka N and Kohno N. Angiotensin II induces fibronectin expression in human peritoneal mesothelial cells via ERK1/2 and p38 MAPK. Kidney Int. 2005; 67:1126-1135.
26. Sandoval P, Loureiro J, Gonzalez-Mateo G, Perez-Lozano ML, Maldonado-Rodriguez A, Sanchez-Tomero JA, Mendoza L, Santamaria B, Ortiz A, Ruiz-Ortega M, Selgas R, Martin P, Sanchez-Madrid F, Aguilera A and Lopez-Cabrera M. PPAR-gamma agonist rosiglitazone protects peritoneal membrane from dialysis fluid-induced damage. Lab Invest. 2010; 90:1517-1532.
27. Shan T, Cui X, Li W, Lin W, Li Y, Chen X and Wu T. Novel regulatory program for norepinephrine-induced epithelial-mesenchymal transition in gastric adenocarcinoma cell lines. Cancer Sci. 2014; 105:847-856.
28. Wahab NA and Mason RM. A critical look at growth factors and epithelial-to-mesenchymal transition in the adult kidney. Interrelationships between growth factors that regulate EMT in the adult kidney. Nephron Experimental nephrology. 2006; 104:e129-134.
29. Liu Y. Epithelial to mesenchymal transition in renal fibrogenesis: pathologic significance, molecular mechanism, and therapeutic intervention. J Am Soc Nephrol. 2004; 15:1-12.
30. Tarighi B, Kurum T, Demir M and Azcan SN. The effects of nebivolol on fibrinolytic parameters in mild and moderate hypertensive patients. Can J Cardiol. 2007; 23:651-655.
31. Dreieicher E, Beck KF, Lazaroski S, Boosen M, Tsalastra-Greul W, Beck M, Fleming I, Schaefer L and Pfeilschifter J. Nitric oxide inhibits glomerular TGF-beta signaling via SMOC-1. J Am Soc Nephrol. 2009; 20:1963-1974.
32. Eberhardt W, Beeg T, Beck KF, Walpen S, Gauer S, Bohles H and Pfeilschifter J. Nitric oxide modulates expression of matrix metalloproteinase-9 in rat mesangial cells. Kidney Int. 2000; 57:59-69.
33. Ceron CS, Rizzi E, Guimaraes DA, Martins-Oliveira A, Gerlach RF and Tanus-Santos JE. Nebivolol attenuates prooxidant and profibrotic mechanisms involving TGF-beta and MMPs, and decreases vascular remodeling in renovascular hypertension. Free Radic Biol Med. 2013; 65:47-56.
34. Chen H, Liu D, Yang Z, Sun L, Deng Q, Yang S, Qian L, Guo L, Yu M, Hu M, Shi M and Guo N. Adrenergic signaling promotes angiogenesis through endothelial cell-tumor cell crosstalk. Endocr Relat Cancer. 2014; 21:783-795.
35. Sharifpanah F, Saliu F, Bekhite MM, Wartenberg M and Sauer H. beta-adrenergic receptor antagonists inhibit vasculogenesis of embryonic stem cells by downregulation of nitric oxide generation and interference with VEGF signalling. Cell Tissue Res. 2014; 358:443-452.
36. Chatterjee S, Biondi-Zoccai G, Abbate A, D’Ascenzo F, Castagno D, Van Tassell B, Mukherjee D and Lichstein E. Benefits of beta blockers in patients with heart failure and reduced ejection fraction: network meta-analysis. BMJ. 2013; 346:f55.
37. Fongemie J and Felix-Getzik E. A Review of Nebivolol Pharmacology and Clinical Evidence. Drugs. 2015; 75:1349-1371.
38. Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ, Parfrey P, Pfeffer M, Raij L, Spinosa DJ and Wilson PW. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension. 2003; 42:1050-1065.
39. Vanholder R, De Smet R, Glorieux G, Argiles A, Baurmeister U, Brunet P, Clark W, Cohen G, De Deyn PP, Deppisch R, Descamps-Latscha B, Henle T, Jorres A, Lemke HD, Massy ZA, Passlick-Deetjen J, et al. Review on uremic toxins: classification, concentration, and interindividual variability. Kidney Int. 2003; 63:1934-1943.
40. Vallance P, Leone A, Calver A, Collier J and Moncada S. Accumulation of an endogenous inhibitor of nitric oxide synthesis in chronic renal failure. Lancet. 1992; 339:572-575.
41. Ravani P, Tripepi G, Malberti F, Testa S, Mallamaci F and Zoccali C. Asymmetrical dimethylarginine predicts progression to dialysis and death in patients with chronic kidney disease: a competing risks modeling approach. J Am Soc Nephrol. 2005; 16:2449-2455.
42. Stylianou E, Jenner LA, Davies M, Coles GA and Williams JD. Isolation, culture and characterization of human peritoneal mesothelial cells. Kidney Int. 1990; 37:1563-1570.
43. Aroeira LS, Aguilera A, Selgas R, Ramirez-Huesca M, Perez-Lozano ML, Cirugeda A, Bajo MA, del Peso G, Sanchez-Tomero JA, Jimenez-Heffernan JA and Lopez-Cabrera M. Mesenchymal conversion of mesothelial cells as a mechanism responsible for high solute transport rate in peritoneal dialysis: role of vascular endothelial growth factor. Am J Kidney Dis. 2005; 46:938-948.
44. Lopez-Cabrera M, Aguilera A, Aroeira LS, Ramirez-Huesca M, Perez-Lozano ML, Jimenez-Heffernan JA, Bajo MA, del Peso G, Sanchez-Tomero JA and Selgas R. Ex vivo analysis of dialysis effluent-derived mesothelial cells as an approach to unveiling the mechanism of peritoneal membrane failure. Perit Dial Int. 2006; 26:26-34.
45. Loureiro J, Aguilera A, Selgas R, Sandoval P, Albar-Vizcaino P, Perez-Lozano ML, Ruiz-Carpio V, Majano PL, Lamas S, Rodriguez-Pascual F, Borras-Cuesta F, Dotor J and Lopez-Cabrera M. Blocking TGF-beta1 protects the peritoneal membrane from dialysate-induced damage. J Am Soc Nephrol. 2011; 22:1682-1695.
46. Diaz C, Selgas R, Castro MA, Bajo MA, Fernandez de Castro M, Molina S, Jimenez C, Ortiz A and Vara F. Ex vivo proliferation of mesothelial cells directly obtained from peritoneal effluent: its relationship with peritoneal antecedents and functional parameters. Adv Perit Dial. 1998; 14:19-24.
47. Strippoli R, Benedicto I, Perez Lozano ML, Cerezo A, Lopez-Cabrera M and del Pozo MA. Epithelial-to-mesenchymal transition of peritoneal mesothelial cells is regulated by an ERK/NF-kappaB/Snail1 pathway. Dis Model Mech. 2008; 1:264-274.
48. Brehm BR, Wolf SC, Bertsch D, Klaussner M, Wesselborg S, Schuler S and Schulze-Osthoff K. Effects of nebivolol on proliferation and apoptosis of human coronary artery smooth muscle and endothelial cells. Cardiovasc Res. 2001; 49:430-439.
49. Jariego CM and Hernanz A. Determination of organic acids by capillary electrophoresis in screening of organic acidurias. Clin Chem. 1996; 42:477-478.