
INTRODUCTION
Hepatocellular carcinoma(HCC) is the fifth most frequently diagnosed cancer worldwide and the second most frequent cause of cancer death [1], with the highest incidence in Asian and especially in China [2]. Partial hepatectomy remains the most commonly used curative therapy modality for HCC [3, 4]. Accurately prognostic prediction of HCC is important to facilitate screening of high risk patients and for the decision on adjuvant therapy. Many risk factors are associated with the prognosis of HCC which makes the tumor staging, prognosis estimation and choosing of therapy options complicated and difficult. Many clinical staging systems have been developed, taking into account tumor related characteristics, liver dysfunction, and general health status. These commonly used clinical staging systems included: (1) the 7th edition of TNM/AJCC classification (TNM 7th) [5]; (2) the Barcelona Clinic Liver Cancer (BCLC) staging system [6]; (3) the International Hepato-Pancreato-Biliary Association (IHPBA) staging system [7]; (4) the Okuda staging system [8]; (5) the Cancer of the Liver Italian Program (CLIP) staging system [9]; (6) the Groupe d’Etude et de Traitement du Carcinome He’patocellulaire (GETCH) staging system [10]; (7) the Chinese University Prognostic Index (CUPI) staging system [11]. Nevertheless, it remains controversial which of the established staging systems should be used as a universally applicable staging system to help improving the overall grim prognosis of HCC [12].
The Pretreatment Extent of Disease System (PRETEXT) was designed by the International Childhood Liver Tumor Strategy Group (SIOPEL) for staging and risk stratification of hepatoblastoma [13, 14]. It was based on the anatomy of the liver and depended on the assessment of the accuracy of imaging techniques preoperatively [15]. PRETEXT system was widely used as a relatively objective method to evaluate tumor extent at diagnosis. Moreover, the system had been proved to show good prognostic value for primary malignant liver tumors of childhood [16]. Many study groups also used the PRETEXT system to describe imaging findings and perform effective comparison among different staging systems of liver tumors in children. However, no researchers applied this effectively and objectively hepatic staging system to adult liver diseases.
The aim of the present study is to apply PRETEXT staging system in predicting survival of adult patients with HCC who underwent curative partial hepatectomy. The prognostic value of the PRETEXT staging system was also compared with those obtained from the currently and commonly used staging systems of HCC mentioned above.
RESULTS
Characteristics of the patients
The characteristics of Eastern and Western patients enrolled in two different hepatobiliary surgery units were shown in Table 1. In these three cohorts, differences among these groups were significant for most covariates. In fact, compared to the Italian, Chinese patients were younger, with predominant hepatitis B related liver disease etiology, larger tumors and better compensated liver function, while Western patients had much higher anti-hepatitis C virus (HCV) positive rate.
Table 1: Clinicopathological characteristics
Variable |
number/value(pecent) |
|||
|---|---|---|---|---|
The primary cohort (n=507) |
Internal validation cohort (n=233) |
External validation cohort (n=293) |
P values |
|
Age in yr(median range) |
49.6±11.2(10-77) |
51.2±10.8(12-70) |
63.5±9.4(40-85) |
0.001 |
Gender |
0.001 |
|||
Male |
441(87.1%) |
202(86.7%) |
227(77.5%) |
|
Female |
66(12.9%) |
31(13.3%) |
66(22.5%) |
|
HBsAg |
0.001 |
|||
Positive |
432(85.2%) |
192(82.4%) |
68(23.2%) |
|
Negative |
75(14.8%) |
41(17.6%) |
225(76.8%) |
|
HBeAg |
0.001 |
|||
Positive |
193(38.1%) |
64(27.5%) |
28(9.6%) |
|
Negative |
314(61.9%) |
169(72.5%) |
265(90.4%) |
|
Anti-HCV(+) |
0 |
0 |
202(68.9%) |
0.001 |
Liver cirrhosis |
0.098 |
|||
Yes |
367(72.4%) |
176(75.5%) |
232(79.2%) |
|
No |
140(27.6%) |
57(24.5%) |
61(20.8%) |
|
TBL(umol/l) |
15.5±8.3 |
15.1±7.3 |
16.1±8.2 |
0.462 |
ALB (g/dl) |
39.4±6.6 |
39.9±6.5 |
37.9±4.6 |
0.106 |
ALT(U/L) |
55.7±34.1 |
50.4±30.2 |
79.4±66.5 |
0.068 |
INR |
1.06±0.09 |
1.04+0.09 |
1.15+1.03 |
0.001 |
PLT(*109/L) |
120±61 |
125±58 |
137±63 |
0.142 |
ALP |
0.028 |
|||
>130 |
83(16.4%) |
30(12.9%) |
63(21.5%) |
|
≤130 |
424(83.6%) |
203(87.1%) |
230(78.5%) |
|
AFP(ng/ml) |
0.001 |
|||
≤400 |
305(60.2%) |
132(56.7%) |
224(76.5%) |
|
>400 |
202(39.8%) |
101(43.3%) |
69(23.5%) |
|
Blood transfusion |
0.364 |
|||
Yes |
128(25.3%) |
70(30.0%) |
82(28.0%) |
|
No |
379(74.7%) |
163(70.0%) |
211(72.0%) |
|
Edmondson-Steiner grade |
0.131 |
|||
III or IV |
315(62.1%) |
160(68.7%) |
198(67.6%) |
|
I or II |
192(37.9%) |
73(31.3%) |
95(32.4%) |
|
Tumor encapsulation |
0.341 |
|||
No (no or part) |
348(68.6%) |
152(65.2%) |
187(63.8%) |
|
Yes (complete) |
159(32.1%) |
81(34.8%) |
106(36.2%) |
|
Tumor diameter(<5cm) |
||||
Median diameter |
5.4±3.2(1.0-12.5) |
5.1±2.6(1.0-12.0) |
3.9±2.1(0.7-14.0) |
0.001 |
>5 cm |
217(42.8%) |
114(48.9%) |
60(20.5%) |
|
≤5 cm |
290(57.2%) |
119(51.1%) |
233(79.5%) |
|
Microvascular invasion |
0.001 |
|||
Yes |
200(39.4%) |
81(34.8%) |
78(26.6%) |
|
No |
307(60.6%) |
152(65.2%) |
215(73.4%) |
|
Tumor number |
0.296 |
|||
Multiple |
87(17.2%) |
50(21.5%) |
60(20.5%) |
|
Solitary |
420(82.8%) |
183(78.5%) |
233(79.5%) |
|
1-year survivaL rate |
84.60% |
81.40% |
83.50% |
|
3-year survivaL rate |
57.40% |
59.40% |
61.50% |
|
5-year survivaL rate |
43.50% |
43.90% |
49.40% |
|
TBL: total bilirubin; ALB: albumin; ALT: alanine aminotransferase; INR: international normalize ratio; PLT: blood platelet; AKP: alkaline phosphatase; AFP: alpha-fetoprotein.
Overall survival in the three cohorts and prognostic factors in the primary cohort
The Overall median survival times were 52.3 months(95% CI:44.4–60.2), 53.1 months(95% CI: 41.2–60.1) and 60.0 months(95% CI: 36.3–83.8) in the primary, internal and external validation cohorts, respectively. The 1-, 3-, and 5-year overall survival rates were showed in Table 1.
Univariate analysis identified that gender, liver cirrhosis, Child–Pugh classification, AFP level, the international normalized ratio(INR), tumor number, maximum tumor size, microscopic vascular invasion and PRETEXT staging system were significant prognostic factors of survival after curative resection (see Table 2). The multivariate analysis of Cox proportional hazard regression identified INR (p=0.001), microvascular invasion (p=0.042), maximum tumor size (p=0.002) and PRETEXT staging system (p=0.001) were independently predictors of overall survival.
Table 2: Cox proportional hazard regression analyses in the training cohort
Variable |
Univariate |
Multivariate |
||||
|---|---|---|---|---|---|---|
HR |
95%CI |
P value |
HR |
95%CI |
P value |
|
Age in yr(median range) |
1.003 |
0.993-1.013 |
0.581 |
|||
Male |
1.546 |
1.120-2.133 |
0.008 |
1.145 |
1.008-1.521 |
0.063 |
HBsAg |
0.881 |
0.613-1.226 |
0.493 |
|||
HBeAg |
0.851 |
0.624-1.161 |
0.309 |
|||
TBL(umol/l) |
0.991 |
0.977-1.006 |
0.231 |
|||
ALB (g/dl) |
1.159 |
0.784-1.771 |
0.459 |
|||
ALT (U/L) |
1.001 |
0.996-1.006 |
0.812 |
|||
INR |
0.078 |
0.024-0.255 |
0.001 |
0.130 |
0.039-0.432 |
0.001 |
ALP>130U/L |
1.102 |
0.923-1.215 |
0.071 |
|||
PLT(*109/L) |
1.005 |
0.992-1.010 |
0.648 |
|||
AFP>400ng/ml |
1.4 |
1.110-1.766 |
0.004 |
1.131 |
1.090-1.438 |
0.312 |
Blood transfusion |
1.055 |
0.835-1.333 |
0.653 |
|||
Edmondson-Steiner grade (3 or 4) |
1.049 |
0.840-1.310 |
0.671 |
|||
Cirrhosis |
2.946 |
2.109-4.115 |
0.001 |
1.043 |
0.096-1/457 |
0.416 |
Child–Pugh classification |
2.163 |
1.680-2.786 |
0.001 |
1.083 |
0.856-1.759 |
0.284 |
Tumour encapsulation |
0.843 |
0.656-1.084 |
0.183 |
|||
Tumour size(>5cm) |
2.262 |
1.792-2.855 |
<0.001 |
1.534 |
1.174-2.002 |
0.002 |
Microvascular invasion |
1.414 |
1.106-1.807 |
0.006 |
1.294 |
1.010-1.659 |
0.042 |
Tumor number |
1.723 |
1.301-2.281 |
<0.001 |
1.013 |
0.731-1.403 |
0.939 |
PRETEXT system |
1.849 |
1.621-2.109 |
<0.001 |
1.565 |
1.205-2.034 |
0.001 |
Staging systems in the three cohorts
Among the three different cohorts, patient stratification and estimated median survival time according to the 8 staging systems were depicted in Table 3. The majority of all patients were stratified to intermediate stages of the staging systems. When looking at the individual staging system as a whole, each showed a statistically significant association with prognosis. Figure 1 showed the Kaplan-Meier survival curves stratified according to the 8 staging systems. The detail distinction between the adjacent stages of the systems was analyzed and showed in Table 3.
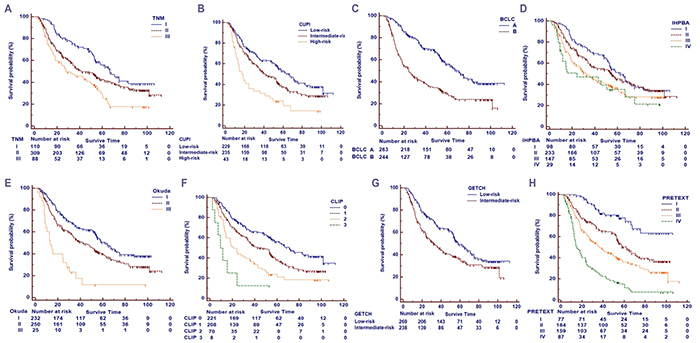
Figure 1: Kaplan-Meier survival curves of the primary cohort. A. the 7th edition of TNM/AJCC classification (TNM 7th); B. the Chinese University Prognostic Index (CUPI) staging system; C. the Barcelona Clinic Liver Cancer (BCLC) staging system; D. the International Hepato-Pancreato-Biliary Association (IHPBA) staging system; E. the Okuda staging system; F. the Cancer of the Liver Italian Program (CLIP) staging system; G. the Groupe d’Etude et de Traitement du Carcinome He’patocellulaire (GETCH) staging system; H:the PRETEXT staging systems.
Table 3: Patient distribution and estimated median survival time according to the eight staging systems
Staging system |
The primary cohort(n=507) |
Internal validation cohort(n=233) |
External validation cohort(n=293) |
|||
|---|---|---|---|---|---|---|
Median survival time(months) |
P value |
Median survival time(months) |
P value |
Median survival time(months) |
P value |
|
AJCC TNM 7th |
<0.001 |
<0.001 |
<0.001 |
|||
I |
67.8 |
I vs. II:0.010 |
61.9 |
I vs. II:0.283 |
80.3 |
I vs. II:0.094 |
II |
57.2 |
II vs. III:0.018 |
55.5 |
II vs. III:0.009 |
64.1 |
II vs. III:0.008 |
III |
42.1 |
39.5 |
36.7 |
|||
CUPI |
<0.001 |
<0.001 |
<0.001 |
|||
Low-risk |
65.2 |
Low-risk vs. Intermediate-risk:0.008 |
65.8 |
Low-risk vs. Intermediate-risk:0.005 |
77.8 |
Low-risk vs. Intermediate-risk:0.001 |
Intermediate-risk |
53.2 |
Intermediate-risk vs. High-risk:0.001 |
48.9 |
Intermediate-risk vs. High-risk:0.547 |
52.3 |
Intermediate-risk vs. High-risk:0.171 |
High-risk |
33.1 |
45.7 |
35.7 |
|||
BCLC |
<0.001 |
0.008 |
0.003 |
|||
A |
70.4 |
A vs. B:<0.001 |
60.1 |
A vs. B:0.008 |
73.8 |
A vs. B:0.003 |
B |
42.9 |
47 |
51.7 |
|||
IHPBA |
<0.001 |
<0.001 |
<0.001 |
|||
I |
75.6 |
I vs. II:0.004 |
69.8 |
I vs. II:0.269 |
88.8 |
I vs. II:0.037 |
II |
60.5 |
II vs. III:0.018 |
59.3 |
II vs. III:0.019 |
68.3 |
II vs. III:0.271 |
III |
47.3 |
III vs. IV:0.091 |
44.9 |
III vs. IV:0.243 |
59.7 |
III vs. IV:0.004 |
IV |
36.9 |
36.5 |
45.9 |
|||
Okuda |
<0.001 |
<0.001 |
0.014 |
|||
I |
62.2 |
I vs. II:0.003 |
64.6 |
I vs. II:0.017 |
80.2 |
I vs. II:0.039 |
II |
53.9 |
II vs. III:0.001 |
49.8 |
II vs. III:0.069 |
64.2 |
II vs. III:0.406 |
III |
26 |
38.5 |
53.7 |
|||
CLIP |
<0.001 |
<0.001 |
<0.001 |
|||
0 |
68.5 |
0 vs. 1:0.001 |
64.4 |
0 vs. 1:0.030 |
86.7 |
0 vs. 1:0.032 |
1 |
52.1 |
1 vs. 2:0.003 |
52.9 |
1 vs. 2:0.041 |
68.5 |
1 vs. 2:0.046 |
2 |
38.3 |
2 vs. 3:0.073 |
35.9 |
2 vs. 3:0.273 |
49.2 |
2 vs. 3:0.735 |
3 |
15.9 |
27.5 |
49 |
|||
GETCH |
<0.001 |
0.003 |
0.001 |
|||
Low |
64.3 |
Low vs. Intermediate: <0.001 |
60 |
Low vs. Intermediate: 0.003 |
76.9 |
Low vs. Intermediate: 0.001 |
Intermediate |
48.8 |
45.2 |
56.4 |
|||
PRETEXT |
<0.001 |
<0.001 |
<0.001 |
|||
I |
84.2 |
I vs. II:0.001 |
76.1 |
I vs. II:0.103 |
99.3 |
I vs. II:<0.001 |
II |
62.3 |
II vs. III:0.004 |
63 |
II vs. III:0.011 |
65.6 |
II vs. III:0.006 |
III |
51.5 |
III vs. IV:0.001 |
45.7 |
III vs. IV:0.006 |
43.4 |
III vs. IV:0.292 |
IV |
28.1 |
28.5 |
32.6 |
|||
Comparison of predictive performance of the PRETEXT system and other staging systems in the primary cohort
In the primary cohort, The performance of the PRETEXT system and the other seven conventional staging systems assessed by the likelihood ratio χ2, linear trend χ2 and the AIC test was described in Table 4. Compared with the other seven conventional staging systems, the PRETEXT system had better homogeneity (higher likelihood ratio χ2 score), discriminatory ability, and monotonicity of gradients (higher linear trend χ2 score). Also, it had a smaller AIC value, suggesting the predictive accuracy was higher. Moreover, the AUC of the PRETEXT system was 0.702 (95% CI, 0.656 to 0.747), which was higher than the other conventional staging systems for predicting survival of HCC (P<0.01, Figure 2). The AUCs of the other staging systems were 0.576 (95% CI, 0.526 to 0.626) of AJCC TNM 7th edition; 0.586 (95% CI, 0.536 to 0.636) of CUPI; 0.616 (95% CI, 0.567 to 0.665) of BCLC; 0.551 (95% CI, 0.500 to 0.601) of IHPBA; 0.593 (95% CI, 0.543 to 0.642) of Okuda; 0.624 (95% CI, 0.575 to 0.672) of CLIP and 0.553 (95% CI, 0.503 to 0.604) of GETCH.
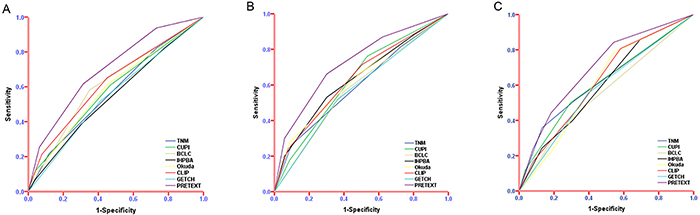
Figure 2: Predictive accuracy of PRETEXT system compared with other staging systems. ROC analysis was displaying the ability of PRETEXT system and the currently used staging systems to predict the survival in the primary cohort A. internal validation cohort B. and external validation cohort C.
Table 4: Comparison of the performance of the eight staging systems in the primary cohort
Staging system |
Discriminatory ability (Linear trend x2) |
Homogeneity (Likelihood ratio x2) |
Akaike information criterion (AIC) |
|---|---|---|---|
AJCC TNM 7th |
11.342 |
16.967 |
3238.438 |
CUPI |
14.85 |
21.48 |
3234.754 |
BCLC |
26.77 |
49.422 |
3207.742 |
IHPBA |
4.533 |
13.092 |
3242.524 |
Okuda |
17.399 |
22.991 |
3232.903 |
CLIP |
27.929 |
40.44 |
3217.915 |
GETCH |
5.67 |
13.784 |
3241.817 |
PRETEXT |
67.761 |
87.161 |
3169.021 |
Validation of predictive performance of PRETEXT system
The results from the primary cohort were verified by two validation cohorts. The PRETEXT system had significantly larger AUC than those of other staging systems in the internal validation cohort(0.725 vs. AJCC TNM 7th edition: 0.599, CUPI: 0.628, BCLC: 0.582, IHPBA: 0.635, Okuda: 0.626, CLIP: 0.638 and GETCH: 0.578, P<0.05, Figure 2) and in the external cohort(0.697 vs. AJCC TNM 7th edition: 0.621, CUPI: 0.612, BCLC: 0.561, IHPBA: 0.600, Okuda: 0.609, CLIP: 0.622 and GETCH: 0.579, P<0.05, Figure 2).
DISCUSSION
With the development of radiology and the different modalities of treatment for patients with HCC, increasing number of patients were detected HCC in relatively early stage [26], which we defined aspatients with no major vascular invasion, extrahepatic metastasis or lymph nodes spreading. Nevertheless, even in this selection of patients, the prognosis still varied since many predictors were related with the survival or the disease-free survival [27, 28]. Many staging systems had been proposed and they had been shown to have different ability to discriminate survival in HCC patients in different studies [29, 30]. Much debate still existed regarding to which prognostic staging system was the best.On the one hand, different geographic regions were attributed to various patients characteristics which led to different predictive value of the commonly used staging systems. For example, alcohol and HCV had repeatedly been identified as two leading etiologic factors for HCC in Europe studies [31], while HBV-infection was the leading etiologic factor in Chinese patients [32, 33]. On the other hand, the heterogeneity treatment options at diagnosis were associated with the lack of a consensus of different predictive value of HCC staging systems [34]. In the present study, we focused on the patients with HCC after curative partial hepatectomy, The predictive performance of the conventional staging systems were not specifically constructed for this selected group and needed to be confirmed.
After revised in 2005, PRETEXT staging system was tend to be more integral and efficient and was intended to applicable to all primary malignant liver tumor of children. It included almost all risk factors of liver tumors, such as tumor size, location, number, major vein involvement, extrahepatic abdominal disease, tumor rupture or intraperitoneal haemorrhage, distant metastases, lymph node metastases and so on [19]. More importantly, PRETEXT staging system was the only pretreatment evaluation system investigated prospectively in patients with hepatoblastoma [14]. As the widely validated effective system in predicting surgical resectability and the prognosis in liver tumor of children, we proposed to apply PRETEXT system in adult liver tumor of HCC and confirm its prognostic significance in HCC. Similarly as adult liver carcinoma TNM system used and compared with other staging systems in liver tumor of children [16, 35], we proposed to assess patients with HCC using PRETEXT system and extend it to all malignant liver tumors when its accuracy and prognostic significance were well validated in different studies. Particularly necessary to point out that since this was the first study reported PRETEXT in patients with HCC, we used the findings of perioperative exploration and the pathology report of the postoperative resection specimen rather than imaging manifestations to determine the PRETEXT staging in order to ensure the accuracy of the PRETEXT staging of patients with HCC. Meanwhile, we compared preoperative findings with the golden standard of pathologic results to further confirm the accuracy of PRETEXT staging. In the present study, we showed that 78(15.4%) of 507 tumors were incorrectly staged. This might be explained by the difficulty of distinguishing tumor and non-tumor tissues in the borderline of the different sections. The preoperative imaging findings might be used when the imaging quality and techniques improved or the error rate reduced to an acceptable range.
Our results showed that the PRETEXT system wasan independent risk factor for overall survival. Moreover, it showed superior prognostic value in both Eastern cohort and Western cohort compared with the commonly used staging systems. Multiple studies compared the staging systems in HCC and have reported different ranking of staging systems in predicting prognosis [36-39]. In our relatively selected patients, we showed that the PRETEXT staging system performed better than the conventional staging systems in the primary cohort(p<0.05), and subsequently we validated our findings in two different cohorts involving Eastern and Western patients. Among the other seven staging systems, CLIP scores showed superior performance in predicting overall survival, whereas no significance difference was observed.
There were several limitations of this study: (1) the PRETEXT system was a comprehensive and sophisticated stage for liver tumor, while we just applied part of the PRETEXT system for a selected patients with HCC. We have planned a further study to apply whole PRETEXT system to all stages of patients with HCC; (2) originally PRETEXT system was used preoperatively to evaluate prognosis of patients, thus further studies should concentrate on apply it at diagnosis; (3) since this was the first study applying PRETEXT system for patients with HCC, more studies were needed to confirm its prognostic value for HCC.
In conclusion, this study showed that the PRETEXT was a good prognostic staging system for HCC. It performed better than the conventional and commonly used staging systems in predicting survival of patients with HCC after curative partial hepatectomy.
PATIENTS AND METHODS
Patients
The inclusion criteria of patient selection were: (1) all patients submitted to hepatic resection as the initial treatment; (2) a preoperative ECOG criteria score of 0-1 [17]; (2) Child-Pugh class A and B; (4) histologically proven HCC in the resected specimen; (5) no evidence of extrahepatic metastasis was present at the time of surgery, and at pathologic examination did not present tumor invasion into a major branch of the portal or hepatic veins, direct invasion of adjacent organs, or spread to the lymph nodes of the hepatic hilum; (6) no tumor enucleations were included in the present study and all resections considered in the present analysis were curative resections at histology. The curative resection was defined as complete resection of tumor according to the criteria that was previously reported [18]. Applying these criteria, we prospectively collected data of consecutive patients with HCC received surgery by the same surgical team between February 1st, 2005 and December 30th, 2012 at the Eastern Hepatobiliary Surgery Hospital (EHBH) of Shanghai, China. After excluding patients with incomplete data, the final study ultimately consisted of 507 patients as the primary cohort. In the same time period 233 patients underwent resection by another surgical team in the same hospital enrolled as internal validation cohort according to the same including criteria. Moreover, another independent cohort including 293 patients were obtained from the Department of Surgery and Transplantation of the University of Bologna during February 2000 to November 2011 and using the similar inclusion criteria to serve as the external validation cohort of this study.
PRETEXT staging system
PRETEXT staging system, which is based exclusively on imaging at diagnosis and Couinaud’s system of segmentation of the liver, divides the liver into four parts, called sections (Figure 3). The liver segments are grouped into four sections as follows: the left lobe of the liver consisting of a left lateral section (segments 2 and 3) and the medial section (segments 4); the right lobe dividing into right anterior section (segments 5 and 8) and right posterior section (segments 6 and 7). The term section is used (where other authors use segment or sector) to avoid terminological confusion. Couinaud segment 1 was not included in the original PRETEXT system. While In the 2005 revised PRETEXT system [19], tumors limited to the caudate lobe were classified as PRETEXT II. The tumor is classified into one of the following four PRETEXT categories depending on the number of liver section that are free of tumor (Figure 3). PRETEXT I (three adjacent section free of tumor); PRETEXT II (two adjacent free of tumor); PRETEXT III (one section free of tumor or two sections in one hemi-liver and one nonadjacent section in the other hemi-liver) and PRETEXT IV (no tumor free section involved). There is no change in numbering for tumors involving the caudate lobe and any other part of the liver.
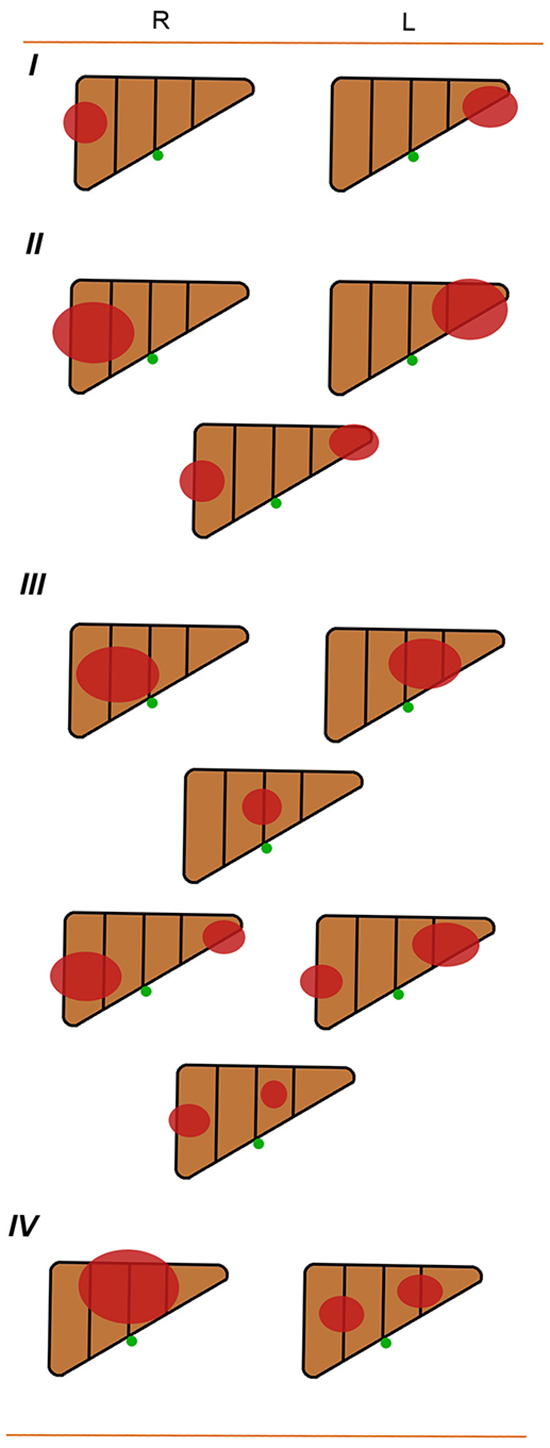
Figure 3: The Liver Tumor Study Group of the International Society of Pediatric Oncology(SIOP) SIOPEL-1: pretreatment extent of disease of grouping system. R: right; L: left.
The assessment of the extent of the primary tumor was performed by abdominal ultrasound and computed tomography (CT). Magnetic resonance imaging or hepatic angiography was only performed if thought necessary by the surgeon of local center. In this study, patients were staged to PRETEXT system according to the findings of perioperative exploration and the pathology report postoperatively, which could ensure the accuracy of the PRETEXT staging.
Clinical staging systems
Collected data was used to restage all patients. This included all patients assessed by the TNM 7th edition, BCLC, IHPBA, Okuda, CLIP, GETCH and CUPI staging systems.
Diagnosis and treatment
After a detailed history and a complete physical examination, the hepatitis B and C serology, liver function test and tumor markers examination which included alpha-fetoprotein (AFP), carbohydrate antigen 19-9 (CA19-9), and carcinoembryonic antigen (CEA) was routinely performed. Other routine investigations were chest X-ray, upper gastrointestinal endoscopy, abdominal ultrasound, contrast-enhanced computerized tomography (CT) and/or magnetic resonance imaging (MRI). A clinical diagnosis of HCC was based on the criteria of the American Association for the Study of Liver Diseases (AASLD) [20].
The type of partial hepatectomy carried out was based on the tumor size, number, location, presence/absence of cirrhosis and estimated volume of future liver remnant. As far as possible, anatomical liver resection was carried out basing on Couinaud’s liver segments, sectors and hemilivers.
Histopathological study of the resected specimens was carried out independently by three pathologists who came to a consensus by discussion if there was any discrepancy.
Follow-up
Contrast-enhanced CT scan or MRI of the abdomen was carried out once every 3 months in the first two years after surgery, and then once every 6 months thereafter. Further investigations were carried out when clinically indicated or when tumor recurrence was suspected. The diagnostic criteria for HCC recurrence were the same as used for the initial diagnosis. Overall survival (OS) was used as the primary endpoint of this study. OS was defined as the interval between partial hepatectomy and death or the last date of follow-up.
Statistical analysis
Continuous variables were expressed as mean ± SD (standard deviation) and compared using a two-tailed unpaired Student’s t test; categorical variables were compared using χ2 or Fisher analysis. Survival curves were plotted using the Kaplan–Meier method, and the log-rank test was used to determine significance [21]. Factors that were deemed of potential importance on univariate analysis were included in multivariate analyses which was performed by means of the Cox proportional-hazards model using the forward logistic regression (LR) stepwise procedure for variable selection. Homogeneity (small difference in survival among patients in the same classification within each system) was determined by likelihood ratio χ2 which was generated by the Cox proportional hazards model. The discriminatory ability of each staging system (greater difference in survival among patients in different stages within each system) was measured by linear trend χ2 [22]. Additionally, To assess potential bias in comparing prognostic systems with different numbers of stages, the Akaike information criterion (AIC) value within a Cox proportional hazard regression model was used. The AIC statistic was defined by AIC = -2 log maximum likelihood + 2*number of parameters in the model. A smaller AIC value indicated a better model for predicting outcome [23, 24]. The predictive performance of PRETEXT system and the other staging systems were measured using the area under ROC curve (AUC). AUCs were also used to compare the PRETEXT system and other staging systems using the Hanleyand McNeil method [25]. Statistical analyses were conducted with the SPSS for Windows version 18.0 release (SPSS, Inc., Chicago, IL) and ROC curve analysis were computed using MedCalcV.11.0.3.0 (MedCalc software, Mariakerke, Belgium). A value of P < 0.05 was considered significant in all the analysis.
CONFLICTS OF INTEREST
The authors who have taken part in this study declared that they have nothing to disclose regarding funding or conflict of interest with respect to this manuscript.
FINANCIAL SUPPORT
No financial support.
Author contributions
Guoliang Qiao, Long Li and Feng Shen designed the research; Alessandro Cucchetti, Jun Li, Matteo Cescon, Giorgio Ercolani, Guanghua Liu conducted acquisition of data; Guoliang Qiao and Alessandro Cucchetti performed the research and statistical analysis; Guoliang Qiao and Feng Shen wrote the paper; Alessandro Cucchetti, Antonio Daniele Pinna and Jun Ren conducted a critical revision of the manuscript.
REFERENCES
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E and Forman D. Global cancer statistics. CA Cancer J Clin. 2011; 61:69-90.
2. Ferlay J, Shin HR, Bray F, Forman D, Mathers C and Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. International journal of cancer. 2010; 127:2893-2917.
3. Torzilli G, Makuuchi M, Inoue K, Takayama T, Sakamoto Y, Sugawara Y, Kubota K and Zucchi A. No-mortality liver resection for hepatocellular carcinoma in cirrhotic and noncirrhotic patients: is there a way? A prospective analysis of our approach. Archives of surgery (Chicago, Ill : 1960). 1999; 134:984-992.
4. Arii S, Yamaoka Y, Futagawa S, Inoue K, Kobayashi K, Kojiro M, Makuuchi M, Nakamura Y, Okita K and Yamada R. Results of surgical and nonsurgical treatment for small-sized hepatocellular carcinomas: a retrospective and nationwide survey in Japan. The Liver Cancer Study Group of Japan. Hepatology (Baltimore, Md). 2000; 32:1224-1229.
5. Edge SB, Byrd DR, Compton C, Fritz A, Greene F and Trotti A. American joint committee on cancer staging manual. American Joint Committee on Cancer Staging Manual. 2010.
6. Llovet JM, Bru C and Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Seminars in liver disease. 1999; 19:329-338.
7. Makuuchi M, Belghiti J, Belli G, Fan ST, Lau JW, Ringe B, Strasberg SM, Vauthey JN, Yamaoka Y and Yamasaki S. IHPBA concordant classification of primary liver cancer: working group report. Journal of hepato-biliary-pancreatic surgery. 2003; 10:26-30.
8. Okuda K, Ohtsuki T, Obata H, Tomimatsu M, Okazaki N, Hasegawa H, Nakajima Y and Ohnishi K. Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer. 1985; 56:918-928.
9. A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients: the Cancer of the Liver Italian Program (CLIP) investigators. Hepatology (Baltimore, Md). 1998; 28:751-755.
10. Chevret S, Trinchet JC, Mathieu D, Rached AA, Beaugrand M and Chastang C. A new prognostic classification for predicting survival in patients with hepatocellular carcinoma. Groupe d’Etude et de Traitement du Carcinome Hepatocellulaire. Journal of hepatology. 1999; 31:133-141.
11. Leung TW, Tang AM, Zee B, Lau WY, Lai PB, Leung KL, Lau JT, Yu SC and Johnson PJ. Construction of the Chinese University Prognostic Index for hepatocellular carcinoma and comparison with the TNM staging system, the Okuda staging system, and the Cancer of the Liver Italian Program staging system: a study based on 926 patients. Cancer. 2002; 94:1760-1769.
12. El-Serag HB. Hepatocellular carcinoma. The New England journal of medicine. 2011; 365:1118-1127.
13. Pritchard J, Brown J, Shafford E, Perilongo G, Brock P, Dicks-Mireaux C, Keeling J, Phillips A, Vos A and Plaschkes J. Cisplatin, doxorubicin, and delayed surgery for childhood hepatoblastoma: a successful approach--results of the first prospective study of the International Society of Pediatric Oncology. Journal of clinical oncology. 2000; 18:3819-3828.
14. Brown J, Perilongo G, Shafford E, Keeling J, Pritchard J, Brock P, Dicks-Mireaux C, Phillips A, Vos A and Plaschkes J. Pretreatment prognostic factors for children with hepatoblastoma-- results from the International Society of Paediatric Oncology (SIOP) study SIOPEL 1. European journal of cancer (Oxford, England : 1990). 2000; 36:1418-1425.
15. Vos A and Kuijper CF. Primary liver tumors in children [Article in Dutch]. Nederlands tijdschrift voor geneeskunde. 1995; 139:1918-1922.
16. Aronson DC, Schnater JM, Staalman CR, Weverling GJ, Plaschkes J, Perilongo G, Brown J, Phillips A, Otte JB, Czauderna P, MacKinlay G and Vos A. Predictive value of the pretreatment extent of disease system in hepatoblastoma: results from the International Society of Pediatric Oncology Liver Tumor Study Group SIOPEL-1 study. Journal of clinical oncology. 2005; 23:1245-1252.
17. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET and Carbone PP. Toxicity and response criteria of the Eastern Cooperative Oncology Group. American journal of clinical oncology. 1982; 5:649-655.
18. Wang K, Liu J, Yan ZL, Li J, Shi LH, Cong WM, Xia Y, Zou QF, Xi T, Shen F, Wang HY and Wu MC. Overexpression of aspartyl-(asparaginyl)-beta-hydroxylase in hepatocellular carcinoma is associated with worse surgical outcome. Hepatology (Baltimore, Md). 2010; 52:164-173.
19. Roebuck DJ, Aronson D, Clapuyt P, Czauderna P, de Ville de Goyet J, Gauthier F, Mackinlay G, Maibach R, McHugh K, Olsen OE, Otte JB, Pariente D, Plaschkes J, Childs M, Perilongo G and International Childrhood Liver Tumor Strategy G. 2005 PRETEXT: a revised staging system for primary malignant liver tumours of childhood developed by the SIOPEL group. Pediatric radiology. 2007; 37:123-132; quiz 249-150.
20. Bruix J and Sherman M. Management of hepatocellular carcinoma. Hepatology (Baltimore, Md). 2005; 42:1208-1236.
21. EL K and P M. Nonparametric estimations from incomplete observations. J Am Stat Assoc. 1958; 53:457-481.
22. Forster MR. Key Concepts in Model Selection: Performance and Generalizability. Journal of Mathematical Psychology. 2000; 44:205-231.
23. Harrell FE, Jr., Califf RM, Pryor DB, Lee KL and Rosati RA. Evaluating the yield of medical tests. Jama. 1982; 247:2543-2546.
24. Hsu CY, Huang YH, Hsia CY, Su CW, Lin HC, Loong CC, Chiou YY, Chiang JH, Lee PC, Huo TI and Lee SD. A new prognostic model for hepatocellular carcinoma based on total tumor volume: the Taipei Integrated Scoring System. Journal of hepatology. 2010; 53:108-117.
25. Hanley JA. Receiver operating characteristic (ROC) methodology: the state of the art. Critical reviews in diagnostic imaging. 1989; 29:307-335.
26. Bolondi L, Sofia S, Siringo S, Gaiani S, Casali A, Zironi G, Piscaglia F, Gramantieri L, Zanetti M and Sherman M. Surveillance programme of cirrhotic patients for early diagnosis and treatment of hepatocellular carcinoma: a cost effectiveness analysis. Gut. 2001; 48:251-259.
27. Imamura H, Matsuyama Y, Tanaka E, Ohkubo T, Hasegawa K, Miyagawa S, Sugawara Y, Minagawa M, Takayama T, Kawasaki S and Makuuchi M. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. Journal of hepatology. 2003; 38:200-207.
28. Nathan H, Schulick RD, Choti MA and Pawlik TM. Predictors of survival after resection of early hepatocellular carcinoma. Annals of surgery. 2009; 249:799-805.
29. Huitzil-Melendez FD, Capanu M, O’Reilly EM, Duffy A, Gansukh B, Saltz LL and Abou-Alfa GK. Advanced hepatocellular carcinoma: which staging systems best predict prognosis? Journal of clinical oncology. 2010; 28:2889-2895.
30. Yang T, Zhang J, Lu JH, Yang LQ, Yang GS, Wu MC and Yu WF. A new staging system for resectable hepatocellular carcinoma: comparison with six existing staging systems in a large Chinese cohort. Journal of cancer research and clinical oncology. 2011; 137:739-750.
31. Greten TF, Papendorf F, Bleck JS, Kirchhoff T, Wohlberedt T, Kubicka S, Klempnauer J, Galanski M and Manns MP. Survival rate in patients with hepatocellular carcinoma: a retrospective analysis of 389 patients. British journal of cancer. 2005; 92:1862-1868.
32. Li Q, Li H, Qin Y, Wang PP and Hao X. Comparison of surgical outcomes for small hepatocellular carcinoma in patients with hepatitis B versus hepatitis C: a Chinese experience. Journal of gastroenterology and hepatology. 2007; 22:1936-1941.
33. Yuen MF, Hou JL and Chutaputti A. Hepatocellular carcinoma in the Asia pacific region. Journal of gastroenterology and hepatology. 2009; 24:346-353.
34. Chen CH, Hu FC, Huang GT, Lee PH, Tsang YM, Cheng AL, Chen DS, Wang JD and Sheu JC. Applicability of staging systems for patients with hepatocellular carcinoma is dependent on treatment method--analysis of 2010 Taiwanese patients. European journal of cancer (Oxford, England : 1990). 2009; 45:1630-1639.
35. von Schweinitz D, Hecker H, Schmidt-von-Arndt G and Harms D. Prognostic factors and staging systems in childhood hepatoblastoma. International journal of cancer. 1997; 74:593-599.
36. Cillo U, Bassanello M, Vitale A, Grigoletto FA, Burra P, Fagiuoli S, D’Amico F, Ciarleglio FA, Boccagni P, Brolese A, Zanus G and D’Amico DF. The critical issue of hepatocellular carcinoma prognostic classification: which is the best tool available? Journal of hepatology. 2004; 40:124-131.
37. Grieco A, Pompili M, Caminiti G, Miele L, Covino M, Alfei B, Rapaccini GL and Gasbarrini G. Prognostic factors for survival in patients with early-intermediate hepatocellular carcinoma undergoing non-surgical therapy: comparison of Okuda, CLIP, and BCLC staging systems in a single Italian centre. Gut. 2005; 54:411-418.
38. Kondo K, Chijiiwa K, Nagano M, Hiyoshi M, Kai M, Maehara N, Ohuchida J, Nakao H and Ohkuwa Y. Comparison of seven prognostic staging systems in patients who undergo hepatectomy for hepatocellular carcinoma. Hepato-gastroenterology. 2007; 54:1534-1538.
39. Marrero JA, Fontana RJ, Barrat A, Askari F, Conjeevaram HS, Su GL and Lok AS. Prognosis of hepatocellular carcinoma: comparison of 7 staging systems in an American cohort. Hepatology (Baltimore, Md). 2005; 41:707-716.