
BACKGROUND
Papillary thyroid cancer (PTC) is the most common endocrine malignancy, which constitutes the primary component of the rapid rise in the incidence of thyroid cancer widely seen in recent decades [1, 2]. In general, PTC is an indolent cancer with a high curability and excellent prognosis, but a subgroup of patients have aggressive disease with a poor prognosis. Given this heterogeneity of the disease prognosis, it is often debatable on how to appropriately manage individual cases of PTC when the goal is to optimize the balance between aggressively treating the cancer to prevent disease recurrence and patient mortality and conservatively limiting the treatment extent to reduce the risk of treatment-associated complications [2–4]. To overcome this challenge will rely on improved risk stratifications to more accurately identify the patients who most likely have a poor prognosis. This can be helped with better understanding of the molecular pathogenesis and identification of useful prognostic molecular markers in PTC.
BRAF V600E mutation, the most common oncogene in PTC, is such a potential prognostic molecular marker. By aberrantly activating the MAP kinase signaling pathway, this mutation plays an important role in the tumorigenesis of many human cancers, including thyroid cancer [5–7]. Many studies reported a role of BRAF V600E mutation in poorer clinicopathological outcomes of PTC [8–13]. There were other studies, however, that failed to demonstrate such a role of BRAF mutation and its prognostic usefulness [14–16]. In a previous relatively small study from our group, BRAF mutation was found to be associated with poor clinicopathological outcomes even in papillary thyroid microcarcinoma (PTMC) [17]. Clearly, new large studies with robust power are needed to help reconcile this controversy on the role of BRAF mutation in PTC.
Two somatic mutations, chr5:1,295,228C > T and chr5:1,295,250C > T (termed here as C228T and C250T, respectively), in the promoter of the gene for telomerase reverse transcriptase (TERT) were found to be associated with poor clinicopathological outcomes of PTC, including aggressive tumor behaviors and increased disease recurrences, making them potentially useful new prognostic molecular makers for PTC [18–22]. TERT is the catalytic subunit of telomerase, which plays an important role in cell immortalization and tumorigenesis. The two TERT promoter mutations were shown to be mutually exclusive and able to increase TERT expression [23, 24]. They were also shown to be associated with aggressiveness of other human cancers, such as melanoma, brain tumor and bladder cancer [25–27]. The prevalence of TERT promoter mutations in PTC varied between 7.5%–27% in previous studies [18–22, 28–30]. Some studies showed an association between BRAF V600E and TERT promoter mutations [19, 21, 28]. One study demonstrated that coexistence of the two mutations was associated with the worst clinicopathololgical outcomes of PTC [21]. These recent findings on TERT promoter mutations in thyroid cancer are exciting, but they remain to be confirmed and generalized by further and high-power studies, ideally in different ethnic populations.
In recent years, the incidence of thyroid carcinoma in the Eastern China region has been rising rapidly, with a rate well above the national average in China [31–33]. It is not clear what the genetic patterns are in thyroid cancer in this region. In the present study, we used a large cohort of PTC patients from this region to particularly investigate BRAF V600E and TERT promoter mutations and their role in the clinicopathological outcomes of PTC.
RESULTS
Demographic features of patients and BRAF V600E and TERT promoter mutations in PTC
Among the cohort of 653 patients with PTC, there were 503 (77.0%) female patients. The mean age ± SD of the patients was 46.5 ± 12.4 years. Most of the cases (58.3%) had a tumor size > 1.0 cm and the mean ± SD of the tumor size in the entire cohort was 1.52 ± 0.91 cm. The rest of the demographic information is presented in Supplementary Table 1. Among the entire cohort of the PTC cases, 416 (63.7%) were found to be positive for BRAF V600E mutation. Both TERT C228T and C250T mutations were found in this cohort of PTC (Supplementary Figure 1) and they were mutually exclusive and collectively found in 27/653 (4.1%) cases. When only tumors ≥ 1.5 cm were analyzed in the present cohort of PTC, the prevalence of TERT promoter mutations was 9.8%.
Our PTC cases were included from 2009 to 2014. As shown in Figure 1, there was an interesting increase in the prevalence of BRAF mutation from the early to the recent years in this period of time. As shown in Figure 2, TERT C228T and C250T were mutually exclusive from each other, with the former being dominant, and they were both associated with BRAF V600E mutation. Specifically, among the 27 cases that were positive for TERT promoter mutations, 22 (81.5%) were also positive for BRAF mutation and the prevalence of TERT promoter mutations were 5.3% in the BRAF mutation-positive group versus 2.1% in the wild-type BRAF group (P = 0.05).
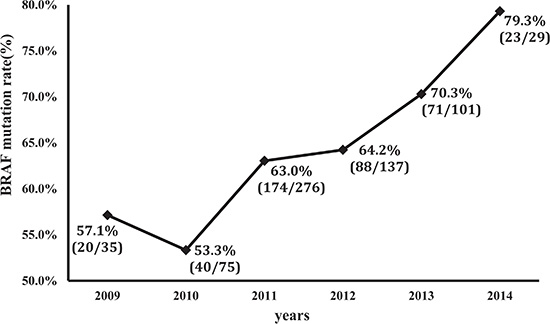
Figure 1: Increasing prevalence of BRAF V600E mutation over the time period from 2009 to 2014. The indicated number of papillary thyroid cancer tumors were tested for BRAF V600E mutation from the indicted years. Percentages represent the prevalence of BRAF mutation. In the brackets, the denominator represents the total cases tested and numerator represents the cases positive for BRAF mutation.
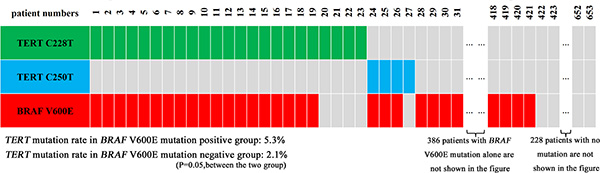
Figure 2: Distribution of BRAF V600E and TERT promoter C228T and C250T mutations and their relationship in papillary thyroid cancer. A total of 653 cases of papillary thyroid cancer were tested for the indicated mutations. Shown are the case numbers and the corresponding mutation status. There was no overlap between the two TERT promoter mutations but there was a considerable overlap between BRAF V600E and the TERT promoter mutations.
Relationship of BRAF V600E and TERT promoter mutations with clinicopathological features of PTC
As shown in Table 1, when the entire cohort of the 653 PTC cases was divided into two genotype groups—a BRAF V600E mutation group and a wild-type BRAF group, the BRAF mutation group was significantly associated with older patient age (P = 0.031), larger tumor size (P = 0.006), capsular invasion (P = 0.027), extrathyroidal invasion (P = 0.004), lymph node metastasis (LNM) (P = 0.035), advanced stage (P = 0.005) and higher MAICS score (P < 0.001). Interestingly, Hashimoto’s thyroiditis (HT) was more commonly seen in patients with wild-type BRAF tumors (P < 0.001). There was no significant association between BRAF mutation and patient sex, tumor multifocality (Table 1).
Table 1: Relationship between BRAF V600E mutation and clinicopathological characteristics of papillary thyroid cancer
Characteristics |
BRAF status, Number (%) |
|
|
|---|---|---|---|
Wild-type (n = 237) |
V600E mutation (n = 416) |
P-value |
|
Age at diagnosis, y |
|
|
|
Mean ± SD |
45.1 ± 12.6 |
47.4 ± 12.2 |
0.031 |
< 45 y |
115 (48.5) |
162 (38.9) |
0.017 |
≥ 45 y |
122 (51.5) |
254 (61.1) |
|
Gender |
|
|
|
Female |
182 (76.8) |
321 (77.2) |
0.914 |
Male |
55 (23.2) |
95 (22.8) |
|
Tumor size in mm |
|
|
|
Mean ± SD |
1.37 ± 0.78 |
1.60 ± 0.97 |
0.006 |
≤ 1 cm |
112 (47.3) |
160 (38.5) |
0.028 |
> 1 cm |
125 (52.7) |
256 (61.5) |
|
Hashimoto’s thyroiditis |
116 (48.9) |
112 (26.9) |
< 0.001 |
Multifocality |
74 (31.2) |
129 (31.0) |
0.955 |
Capsular invasion |
40 (16.9) |
101 (24.3) |
0.027 |
Extrathyroidal invasion |
25 (10.5) |
80 (19.2) |
0.004 |
Lymph node metastasis |
147 (65.3)* |
284 (73.4)* |
0.035 |
AJCC disease stage |
|
|
|
I + II |
168 (70.9) |
249 (59.9) |
0.005 |
III + IV |
69 (29.1) |
167 (40.1) |
|
TERT promoter mutation |
5 (2.1) |
22 (5.3) |
0.050 |
MAICS score |
4.3 ± 0.9 |
4.6 ± 1.0 |
< 0.001 |
*The percentage was calculated only in patients with neck dissection.
Similarly, when the entire cohort of the 653 PTC cases was divided into two genotype groups—a TERT promoter mutation group and a wild-type TERT group, a significant association was observed between the TERT promoter mutation group and high-risk clinicopathological features of PTC (Table 2). Specifically, TERT promoter mutations were significantly associated with older patient age (P < 0.001), larger tumor size (P < 0.001), capsular invasion (P < 0.001), extrathyroidal invasion (P < 0.001), advanced disease stage (P = 0.003), and higher MAICS score (P < 0.001). No association was observed between TERT promoter mutations and patient sex, HT, tumor multifocality and LNM.
Table 2: Relationship between TERT promoter mutation and clinicopathological characteristics of papillary thyroid cancer
Characteristics |
TERT mutation status, Number (%) |
|
|
|---|---|---|---|
Wild-type (n = 626) |
Mutation (n = 27) |
P-value |
|
Age at diagnosis, y |
|
|
|
Mean ± SD |
46.0 ± 12.0 |
59.2 ± 13.8 |
< 0.001 |
< 45 y |
272 (43.5) |
5 (18.5) |
0.010 |
≥ 45 y |
354 (56.5) |
22 (81.5) |
|
Gender |
|
|
|
Female |
484 (77.3) |
19 (70.4) |
0.401 |
Male |
142 (22.7) |
8 (29.6) |
|
Tumor size in cm |
|
|
|
Mean ± SD |
1.46 ± 0.84 |
2.80 ± 1.52 |
< 0.001 |
≤ 1 cm |
270 (43.1) |
2 (7.4) |
< 0.001 |
> 1 cm |
356 (56.9) |
25 (92.6) |
|
Hashimoto’s thyroiditis |
220 (35.1) |
8 (29.6) |
0.556 |
Multifocality |
192 (30.7) |
11 (40.7) |
0.268 |
Capsular invasion |
125 (20.0) |
16 (59.3) |
< 0.001 |
Extrathyroidal invasion |
91 (14.5) |
14 (51.9) |
< 0.001 |
Lymph node metastasis |
411 (70.1)* |
20 (76.9)* |
0.458 |
AJCC disease stage |
|
|
|
I + II |
407 (65.0) |
10 (37.0) |
0.003 |
III + IV |
219 (35.0) |
17 (63.0) |
|
BRAF V600E mutation |
394 (62.9) |
22 (81.5) |
0.050 |
MAICS score |
4.4 ± 0.9 |
6.2 ± 1.4 |
< 0.001 |
*The percentage was calculated only in patients with neck dissection.
Relationship of BRAF V600E alone or TERT promoter mutation alone or their coexistence with clinicopathological characteristics of PTC
As shown in Table 3, compared with the group harboring neither BRAF V600E nor TERT promoter mutation, the group harboring BRAF mutation alone (no TERT promoter mutation) had a significant association with a number of high-risk clinicopathological characteristics. Specifically, BRAF mutation alone was associated with older patient age (≥ 45 years) (P = 0.042), larger tumor size (P = 0.032), extrathyroidal invasion (P = 0.012), advanced stage (P = 0.022), and higher MAICS score (P = 0.002). BRAF mutation was significantly less common in patients with HT than patients without HT (P < 0.001). Compared with the group harboring neither BRAF V600E nor TERT promoter mutation, the group harboring TERT promoter mutation alone (no BRAF V600E mutation) had a significant yet modest association with capsular invasion (P = 0.035) and higher MAICS score (P = 0.040). There was no significant association between TERT promoter mutation alone and other clinicopathological characteristics. Strikingly, the group simultaneously harboring both BRAF V600E and TERT promoter mutations showed a sharply more common association with much higher significance (lower P values) for all the above high-risk clinicopathological features. This association of coexistence of BRAF V600E and TERT promoter mutations with aggressive clinicopathological features of PTC was far more robust than either mutation alone, with a P value being < 0.001 in most cases (Table 3).
Table 3: Relationship of BRAF V600E alone or TERT promoter mutation alone or their coexistence with clinicopathological characteristics of papillary thyroid cancer
|
No mutation |
TERT mutation only |
P value |
BRAF mutation only |
P value |
TERT+ BRAF mutations |
P value |
|---|---|---|---|---|---|---|---|
Age at diagnosis, y |
|
|
|
|
|
|
|
Mean ± SD |
44.9 ± 12.3 |
53.4 ± 23.0 |
0.361 |
46.6 ± 11.8 |
0.104 |
60.5 ± 11.2 |
< 0.001 |
Range |
11–78 |
25–81 |
|
18–79 |
|
41–80 |
|
≥ 45 y |
119 (51.3) |
3 (60.0) |
1.000 |
235 (59.6) |
0.042 |
19 (86.4) |
0.002 |
Gender (Female) |
178 (76.7) |
4 (80.0) |
1.000 |
306 (77.7) |
0.786 |
15 (68.2) |
0.370 |
Tumor size in cm |
|
|
|
|
|
|
|
Mean ± SD |
1.36 ± 0.78 |
1.80 ± 0.95 |
0.247 |
1.52 ± 0.86 |
0.032 |
3.03 ± 1.55 |
< 0.001 |
Range |
0.1–4.3 |
0.5–2.8 |
|
0.3–5.0 |
|
0.6–7.0 |
|
> 1 cm |
121 (52.2) |
4 (80.0) |
0.435 |
235 (59.6) |
0.068 |
21 (95.5) |
< 0.001 |
HT |
114 (49.1) |
2 (40.0) |
1.000 |
106 (26.9) |
< 0.001 |
6 (27.3) |
0.050 |
Multifocality |
74 (31.9) |
0 (0.0) |
0.328 |
118 (29.9) |
0.610 |
11 (50.0) |
0.085 |
Capsular invasion |
37 (15.9) |
3 (60.0) |
0.035 |
88 (22.3) |
0.054 |
13 (59.1) |
< 0.001 |
Extrathyroidal invasion |
23 (9.9) |
2 (40.0) |
0.088 |
68 (17.3) |
0.012 |
12 (54.5) |
< 0.001 |
LNM |
144 (65.5)* |
3 (60.0)* |
1.000 |
267 (73.0)* |
0.055 |
17 (81.0)* |
0.150 |
Late stage (III + IV) |
68 (29.3) |
1 (20.0) |
1.000 |
151 (38.3) |
0.022 |
16 (72.7) |
< 0.001 |
MAICS score |
4.3 ± 0.8 |
5.5 ± 1.7 |
0.040 |
4.5 ± 0.9 |
0.002 |
6.4 ± 1.3 |
< 0.001 |
Footnotes: Data are expressed as number (percentage). Comparisons were performed between the no mutation group and each of the other three groups (TERT promoter mutation only; BRAF mutation only; TERT + BRAF mutation); P value refers to the comparison of the no mutation group with the group in the column immediately left to the P value column. *The percentage is calculated only in patients with neck dissection. HT, Hashimoto’s thyroiditis; LNM: lymph node metastasis.
DISCUSSION
In this largest study on TERT promoter mutation in PTC, we demonstrated a significant role of TERT promoter mutations in the development of aggressive clinicopathological features of PTC. This study on a Chinese cohort of PTC patients confirmed the findings in some previous studies in other ethnic populations [18–22] and expanded this newly emerged exciting area of thyroid cancer research. Given the controversies on the role of BRAF V600E in clinicopathological aggressiveness of PTC, we also took the advantage of this large new cohort of PTC to further address this issue. We demonstrated a significant role of BRAF V600E mutation in the development of aggressive features of PTC, confirming the findings in some previous studies. With the large size, the present study provides new robust evidence helping reconcile the controversies on this role of BRAF mutation.
Several previous studies reported an association between BRAF V600E mutation and TERT promoter mutations in PTC [19, 21, 28]. One previous study demonstrated that coexistence of BRAF V600E and TERT promoter mutations was even more strongly associated with poor clinicopathological outcomes of PTC [21]. Inconsistent results on this phenomenon, however, were reported by other studies. For example, in several studies the association between BRAF V600E and TERT promoter mutations was not significant [18, 22, 34]. Another study even reported a significant inverse relationship between BRAF V600E and TERT promoter mutations in PTC [29]. Data on the clinicopathological significance of coexisting BRAF V600E and TERT promoter mutations were also inconsistent; two studies showed no particularly aggressive role of coexisting BRAF and TERT promoter mutations in the pathogenesis of PTC [20, 22]. These studies, however, were all relatively small. Consequently, the number of cases with coexisting BRAF and TERT promoter mutations in these studies was all particularly small—too small to provide sufficient statistical power. Thus, this is currently an important unresolved issue on the role of TERT promoter mutations in thyroid cancer. Resolution of this controversy would rely on studies of large patient cohorts. Indeed, in the present study—the largest on TERT promoter mutation so far, we were able to observe a significant association between BRAF V600E and TERT promoter mutations and demonstrate a robust cooperative role of coexisting BRAF V600E and TERT promoter mutations in the development of clinicopatholoical aggressiveness of PTC, providing strong new evidence reconciling the controversy. The present findings, together with previous studies [21], thus firmly establish that coexisting BRAF V600E and TERT promoter mutations represent a unique robust genetic mechanism that identifies the most aggressive group of PTC and thus has an important prognostic value. This role of coexisting BRAF V600E and TERT promoter mutations in the clinicopathological aggressiveness of PTC is consistent with the hypothesis that BRAF V600E mutation, through constitutively activating the MAP kinase pathway, can promote the expression of TERT when TERT mutations are created and can thus bind with ETS transcription factors, leading to tumorigenesis-promoting cellular activities [23, 24].
A prevalence of 63.7% for BRAF V600E mutation in PTC found in this study seemed to be somehow higher than generally reported, which was averaged around 45–50% [35–37]. One possible explanation is the relatively high dietary iodine intake from rich sea foods in the eastern coastal regions in China where the study was conducted. This possibility is consistent with a previous report of the association between BRAF V600E mutation and high dietary iodine intake [38]. Another explanation is that the present study included a large number of patients from recent years, in which there was an increasing prevalence of BRAF V600E mutation as demonstrated in the present study (Figure 1). This finding is consistent with other similar reports, including the one of Mathur et al. in which the prevalence of BRAF mutation was significantly higher in the recent 5 years compared with earlier years [39]. The lower prevalence of BRAF mutation in PTC in an early study from our group seems to be also consistent with this idea [17].
In contrary to the high prevalence of BRAF V600E mutation, we found a relatively low prevalence of 4.1% for TERT promoter mutations compared with other studies [18–22, 28–30]. One explanation is the high proportion of small tumors in our study; the average tumor size was smaller than those in many previous studies and up to 67.2% of our patients had tumor size < 1.5 cm. Since the present study and previous studies demonstrated an association of TERT promoter mutations with larger tumor size of PTC, the large number of small tumors included in our study presumably resulted in an overall low prevalence of TERT promoter mutations. This idea is strongly supported by the fact that when only tumors ≥ 1.5 cm were analyzed in the present cohort of PTC, the prevalence of TERT promoter mutations rose to 9.8%.
Our study also found an interesting inverse association between the BRAF V600E mutation and HT; the prevalence of BRAF mutation in PTC was significantly lower in patients with coexisting HT compared with those without HT. This is consistent with similar findings in several previous studies [40, 41]. Interestingly, consistent with an aggressive role of BRAF mutation in PTC, PTC associated with HT (and hence lower prevalence of BRAF mutation) was associated with a better prognosis in these studies. Microenvironment in which the BRAF V600E derives pathogenic molecular changes plays an important role in the pathogenesis of PTC (43–45). It remains to be investigated whether this mechanism may play a role in the interplay among HT, BRAF V600E, and clinicopathological features of PTC.
CONCLUSIONS
This is the largest study on TERT promoter mutation in PTC, which demonstrates a significant role of TERT promoter mutations and their association with BRAF V600E as well as their cooperation in driving the clinicopathological aggressiveness of PTC. This study on a large cohort of PTC also provides new and robust evidence demonstrating an aggressive role of BRAF V600E mutation in PTC. These results help reconcile some of the controversies on the roles of BRAF V600E and TERT promoter mutations in the pathogenesis and progression of PTC and establish their unique prognostic values. As such, this study has important clinical and biological implications for PTC.
METHODS
Patients and thyroid cancer samples
A total of 653 PTC patients with complete clinical and pathological data were included in this study, who were treated with thyroidectomy at the First and Third Affiliated Hospitals of Wenzhou Medical University (481 and 172 patients, respectively) from May 2009 to July 2014., Most of these patients were long-term residents living in the coastal Eastern China. Of these patients, there were 503 (77.0%) females. With the ethic committee’s approval at the First and Third Affiliated Hospital of Wenzhou Medical University and informed patient consent, fresh PTC specimens were collected from 481 patients undergoing thyroidectomy at the First Affiliated Hospital. Samples were snap-frozen in liquid nitrogen immediately after surgical resection and subsequently stored at a −80°C freezer. Formalin fixed and paraffin-embedded PTC tumor specimens, originally from 172 patients at the Third Affiliated Hospital, were collected for DNA extraction. Histopathological slides were reviewed retrospectively for all cases to confirm the histological diagnosis and to ensure abundant cancer content of the tumor by two pathologists. Disease stages were classified according to the American Joint Committee on Cancer (AJCC) staging system. The MACIS prognostic scoring system was used for predicting PTC patients prognosis as previously described [42].
In our study cohort, there were 88 (13.5%) patients with the age > 60 years at the diagnosis, 132 (20.2%) patients with the tumor > 2 cm, and 612 (93.7%) patients with lymph node dissection, of which 279 (45.6%) were N1a and 152 (24.8%) were N1b. For papillary thyroid cancer (PTMC), central lymph node dissection (CLND) was controversial in our institution. Most physicians performed prophylactic CLND and others did not. For non-PTMC, prophylactic CLND was routinely performed. All lateral lymph node dissection was therapeutic. In this study, no lymph node dissection was performed in 41 patients. None of the patients in this study had distant metastasis. As PTC variants (such as conventional, tall-cell or follicular variant) are not routinely specifically defined in our institution, we report all PTC cases here collectively as PTC. None of the patients had distant metastasis.
DNA extraction and mutation analysis
For fresh thyroid specimens, genomic DNA was extracted by standard phenol-chloroform extraction and ethanol precipitation procedures. For paraffin-embedded specimens, DNA extraction was performed using the QIAamp DNA FFPE Tissue Kit (QIAGEN) according to the manufacturer’s instructions. Exon 15 of BRAF was amplified by polymerase chain reaction (PCR) using the following primers: 5′-TCATAATGCTTGCTCTGATAGGA-3′ (sense) and 5′-GGCCAAAAATTTAATCAGTGGA-3′ (antisense). The PCR condition included an initial denaturation step at 94°C for 3 min, followed by 35 cycles of 94°C denaturation for 30 s, 55°C annealing for 30 s, 72°C elongation for 1 min and a final elongation step at 72°C for 5 min. A fragment of the TERT promoter, containing the C228T and C250T mutation sites, was amplified by PCR using the GC-RICH PCR System (Roche Applied Science) and primers: 5′-CCAGGACCGCGCTTCCCAC-3′ (sense) and 5′-GGGAGCGCGCGGCATCG-3′ (antisense). The PCR condition included an initial denaturation step at 95°C for 3 min, 10 cycles of 95°C denaturation for 30 s, 60°C annealing for 30 s, 72°C elongation for 30 s, followed by 30 cycles of running at 95°C for 30 s, 58°C for 30 s, and 72°C for 35 s and a final elongation step at 72°C for 7 min. The quality of the PCR products was confirmed by 2% agarose gel electrophoresis. The PCR products were sequenced using a Big Dye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems) on an ABI PRISM 3730XL DNA Analyzer (Applied Biosystems) to identify the mutation. When a mutation was observed, another independent PCR reaction and sequencing analysis were performed to confirm the mutation.
Statistical analysis
The results are expressed as mean ± SD for continuous data and percentage (%) for categorical data. Mann–Whitney U test was used for comparison of continuous variables. Pearson χ2 test or Fisher’s exact test was used for comparison of categorical variables. The SPSS statistical software (version 19.0) was used for all analyses. A P value ≤ 0.05 was considered to be significant.
ACKNOWLEDGMENTS
This study was supported by the National High Technology Research and Development Program of China (863 Program) (2012AA02A210) and the Zhejiang Provincial Natural Science Foundation of China (LY13H160034).
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare.
REFERENCES
1. Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg. 2014; 140:317–322.
2. La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F, Negri E. Thyroid cancer mortality and incidence: A global overview. International journal of cancer. 2015; 136:2187–2195.
3. Morris LG, Sikora AG, Tosteson TD, Davies L. The increasing incidence of thyroid cancer: the influence of access to care. Thyroid. 2013; 23:885–891.
4. Brito JP, Morris JC, Montori VM. Thyroid cancer: zealous imaging has increased detection and treatment of low risk tumours. Bmj. 2013; 347:f4706.
5. Cohen Y, Xing M, Mambo E, Guo Z, Wu G, Trink B, Beller U, Westra WH, Ladenson PW, Sidransky D. BRAF mutation in papillary thyroid carcinoma. Journal of the National Cancer Institute. 2003; 95:625–627.
6. Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fagin JA. High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer research. 2003; 63:1454–1457.
7. Soares P, Trovisco V, Rocha AS, Lima J, Castro P, Preto A, Maximo V, Botelho T, Seruca R, Sobrinho-Simoes M. BRAF mutations and RET/PTC rearrangements are alternative events in the etiopathogenesis of PTC. Oncogene. 2003; 22:4578–4580.
8. Xing M, Westra WH, Tufano RP, Cohen Y, Rosenbaum E, Rhoden KJ, Carson KA, Vasko V, Larin A, Tallini G, Tolaney S, Holt EH, Hui P, et al. BRAF mutation predicts a poorer clinical prognosis for papillary thyroid cancer. The Journal of clinical endocrinology and metabolism. 2005; 90:6373–6379.
9. Elisei R, Ugolini C, Viola D, Lupi C, Biagini A, Giannini R, Romei C, Miccoli P, Pinchera A, Basolo F. BRAF(V600E) mutation and outcome of patients with papillary thyroid carcinoma: a 15-year median follow-up study. The Journal of clinical endocrinology and metabolism. 2008; 93:3943–3949.
10. Oler G, Cerutti JM. High prevalence of BRAF mutation in a Brazilian cohort of patients with sporadic papillary thyroid carcinomas: correlation with more aggressive phenotype and decreased expression of iodide-metabolizing genes. Cancer. 2009; 115:972–980.
11. Elisei R, Viola D, Torregrossa L, Giannini R, Romei C, Ugolini C, Molinaro E, Agate L, Biagini A, Lupi C, Valerio L, Materazzi G, Miccoli P, et al. The BRAF(V600E) Mutation Is an Independent, Poor Prognostic Factor for the Outcome of Patients with Low-Risk Intrathyroid Papillary Thyroid Carcinoma: Single-Institution Results from a Large Cohort Study. J Clin Endocr Metab. 2012; 97:4390–4398.
12. Xing M, Alzahrani AS, Carson KA, Viola D, Elisei R, Bendlova B, Yip L, Mian C, Vianello F, Tuttle RM, Robenshtok E, Fagin JA, Puxeddu E, et al. Association between BRAF V600E mutation and mortality in patients with papillary thyroid cancer. Jama. 2013; 309:1493–1501.
13. Xing M, Alzahrani AS, Carson KA, Shong YK, Kim TY, Viola D, Elisei R, Bendlova B, Yip L, Mian C, Vianello F, Tuttle RM, Robenshtok E, et al. Association between BRAF V600E mutation and recurrence of papillary thyroid cancer. Journal of clinical oncology. 2015; 33:42–50.
14. Ito Y, Yoshida H, Maruo R, Morita S, Takano T, Hirokawa M, Yabuta T, Fukushima M, Inoue H, Tomoda C, Kihara M, Uruno T, Higashiyama T, et al. BRAF mutation in papillary thyroid carcinoma in a Japanese population: its lack of correlation with high-risk clinicopathological features and disease-free survival of patients. Endocrine journal. 2009; 56:89–97.
15. Nam JK, Jung CK, Song BJ, Lim DJ, Chae BJ, Lee NS, Park WC, Kim JS, Jung SS, Bae JS. Is the BRAF(V600E) mutation useful as a predictor of preoperative risk in papillary thyroid cancer? American journal of surgery. 2012; 203:436–441.
16. Fugazzola L, Puxeddu E, Avenia N, Romei C, Cirello V, Cavaliere A, Faviana P, Mannavola D, Moretti S, Rossi S, Sculli M, Bottici V, Beck-Peccoz P, et al. Correlation between B-RAFV600E mutation and clinico-pathologic parameters in papillary thyroid carcinoma: data from a multicentric Italian study and review of the literature. Endocr Relat Cancer. 2006; 13:455–464.
17. Lin KL, Wang OC, Zhang XH, Dai XX, Hu XQ, Qu JM. The BRAF Mutation Is Predictive of Aggressive Clinicopathological Characteristics in Papillary Thyroid Microcarcinoma. Annals of surgical oncology. 2010; 17:3294–3300.
18. Liu T, Wang N, Cao J, Sofiadis A, Dinets A, Zedenius J, Larsson C, Xu D. The age- and shorter telomere-dependent TERT promoter mutation in follicular thyroid cell-derived carcinomas. Oncogene. 2014; 33:4978–4984.
19. Liu X, Qu S, Liu R, Sheng C, Shi X, Zhu G, Murugan AK, Guan H, Yu H, Wang Y, Sun H, Shan Z, Teng W, et al. TERT promoter mutations and their association with BRAF V600E mutation and aggressive clinicopathological characteristics of thyroid cancer. The Journal of clinical endocrinology and metabolism. 2014; 99:E1130–1136.
20. Melo M, da Rocha AG, Vinagre J, Batista R, Peixoto J, Tavares C, Celestino R, Almeida A, Salgado C, Eloy C, Castro P, Prazeres H, Lima J, et al. TERT promoter mutations are a major indicator of poor outcome in differentiated thyroid carcinomas. The Journal of clinical endocrinology and metabolism. 2014; 99:E754–765.
21. Xing M, Liu R, Liu X, Murugan AK, Zhu G, Zeiger MA, Pai S, Bishop J. BRAF V600E and TERT promoter mutations cooperatively identify the most aggressive papillary thyroid cancer with highest recurrence. Journal of clinical oncology. 2014; 32:2718–2726.
22. Muzza M, Colombo C, Rossi S, Tosi D, Cirello V, Perrino M, De Leo S, Magnani E, Pignatti E, Vigo B, Simoni M, Bulfamante G, Vicentini L, et al. Telomerase in differentiated thyroid cancer: promoter mutations, expression and localization. Molecular and cellular endocrinology. 2015; 399:288–295.
23. Huang FW, Hodis E, Xu MJ, Kryukov GV, Chin L, Garraway LA. Highly recurrent TERT promoter mutations in human melanoma. Science. 2013; 339:957–959.
24. Horn S, Figurel A, Rachakonda PS, Fischer C, Sucker A, Gast A, Kadel S, Moll I, Nagore E, Hemminki K, Schadendorf D, Kumar R. TERT promoter mutations in familial and sporadic melanoma. Science. 2013; 339:959–961.
25. Killela PJ, Reitman ZJ, Jiao YC, Bettegowda C, Agrawal N, Diaz LA, Friedman AH, Friedman H, Gallia GL, Giovanella BC, Grollman AP, He TC, He YP, et al. TERT promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal. Proc Natl Acad Sci USA. 2013; 110:6021–6026.
26. Rachakonda PS, Hosen I, de Verdier PJ, Fallah M, Heidenreich B, Ryk C, Wiklund NP, Steineck G, Schadendorf D, Hemminki K, Kumar R. TERT promoter mutations in bladder cancer affect patient survival and disease recurrence through modification by a common polymorphism. Proc Natl Acad Sci USA. 2013; 110:17426–17431.
27. Griewank KG, Murali R, Puig-Butille JA, Schilling B, Livingstone E, Potrony M, Carrera C, Schimming T, Moller I, Schwamborn M, Sucker A, Hillen U, Badenas C, et al. TERT Promoter Mutation Status as an Independent Prognostic Factor in Cutaneous Melanoma. Journal of the National Cancer Institute. 2014; 106.
28. Liu X, Bishop J, Shan Y, Pai S, Liu D, Murugan AK, Sun H, El-Naggar AK, Xing M. Highly prevalent TERT promoter mutations in aggressive thyroid cancers. Endocrine-related cancer. 2013; 20:603–610.
29. Landa I, Ganly I, Chan TA, Mitsutake N, Matsuse M, Ibrahimpasic T, Ghossein RA, Fagin JA. Frequent somatic TERT promoter mutations in thyroid cancer: higher prevalence in advanced forms of the disease. The Journal of clinical endocrinology and metabolism. 2013; 98:E1562–1566.
30. Vinagre J, Almeida A, Populo H, Batista R, Lyra J, Pinto V, Coelho R, Celestino R, Prazeres H, Lima L, Melo M, da Rocha AG, Preto A, et al. Frequency of TERT promoter mutations in human cancers. Nature communications. 2013; 4:2185.
31. Zheng W, Zhang Z. An analysis of cancer incidence in 2005 in Lucheng District, Wenzhou City, Zhejiang Province. Bulletin of Chinese Cancer. 2007; 16:306–308.
32. Gong W, Hu R, Luo S, Jin P, Fei F, He Q, Zhang Z, min Y. Analysis on incidence and mortality characteristics of thyroid cancer during 2007 to 2011 in Zhejiang Province. Zhejiang Prev Med. 2014; 26:433–437.
33. Yang L, Zheng R, Wang N, Zhang S, Chen W. Analysis of incidence and mortality of thyroid cancer in China, 2010. Zhonghua yu fang yi xue za zhi [Chinese journal of preventive medicine]. 2014; 48:663–668.
34. Cancer Genome Atlas Research N. Integrated genomic characterization of papillary thyroid carcinoma. Cell. 2014; 159:676–690.
35. Kim TH, Park YJ, Lim JA, Ahn HY, Lee EK, Lee YJ, Kim KW, Hahn SK, Youn YK, Kim KH, Cho BY, Park do J. The association of the BRAF(V600E) mutation with prognostic factors and poor clinical outcome in papillary thyroid cancer: a meta-analysis. Cancer. 2012; 118:1764–1773.
36. Lee JH, Lee ES, Kim YS. Clinicopathologic significance of BRAF V600E mutation in papillary carcinomas of the thyroid: a meta-analysis. Cancer. 2007; 110:38–46.
37. Tufano RP, Teixeira GV, Bishop J, Carson KA, Xing M. BRAF mutation in papillary thyroid cancer and its value in tailoring initial treatment: a systematic review and meta-analysis. Medicine. 2012; 91:274–286.
38. Guan HX, Ji MJ, Bao R, Yu HY, Wang YG, Hou P, Zhang Y, Shan ZY, Teng WP, Xing MZ. Association of High Iodine Intake with the T1799A BRAF Mutation in Papillary Thyroid Cancer. J Clin Endocr Metab. 2009; 94:1612–1617.
39. Mathur A, Moses W, Rahbari R, Khanafshar E, Duh QY, Clark O, Kebebew E. Higher rate of BRAF mutation in papillary thyroid cancer over time: a single-institution study. Cancer. 2011; 117:4390–4395.
40. Kim SJ, Myong JP, Jee HG, Chai YJ, Choi JY, Min HS, Lee KE, Youn YK. Combined effect of Hashimoto’s thyroiditis and BRAF mutation status on aggressiveness in papillary thyroid cancer. Head & neck. 2014 Sep 12. doi: 10.1002/hed.23854.
41. Kwak HY, Chae BJ, Eom YH, Hong YR, Seo JB, Lee SH, Song BJ, Jung SS, Bae JS. Does papillary thyroid carcinoma have a better prognosis with or without Hashimoto thyroiditis? Int J Clin Oncol. 2015; 20:463–473.
42. Hay ID, Bergstralh EJ, Goellner JR, Ebersold JR, Grant CS. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery. 1993; 114:1050–1057.
43. Nucera C, Porrello A, Antonello ZA, Mekel M, Nehs MA, Giordano TJ, Gerald D, Benjamin LE, Priolo C, Puxeddu E, Finn S, Jarzab B, Hodin RA, et al. B-Raf(V600E) and thrombospondin-1 promote thyroid cancer progression. Proc Natl Acad Sci USA. 2010; 107:10649–10654.
44. Nucera C, Lawler J, Parangi S. BRAF(V600E) and microenvironment in thyroid cancer: a functional link to drive cancer progression. Cancer Res. 2011; 71:2417–2422.
45. Nucera C. Targeting thyroid cancer microenvironment:basic research and clinical applications. Front Endocrinol (Lausanne). 2013; 4:167.