
INTRODUCTION
The World Health Organization has defined clear cell carcinoma (CCC) of the ovary as a distinct histological type since 1973 [1]. This tumor type accounts for 15% of all epithelial ovarian cancer (EOC) cases [2], and the incidence might be even higher among Asian women [3-5]. CCC is one of the most aggressive and malignant types of tumors, and it has a poorer clinical outcome than other types of EOC due to its resistance to platinum-based chemotherapy, particularly in patients with advanced or recurrent disease [2, 6-8]. The Gynecologic Cancer Intergroup (GCIG) initiated a meta-analysis in 2010 and demonstrated that the median overall survival (OS) for stage III/IV CCC was only 21.3 months [9]. The 5-year OS rate for patients with recurrent CCC was as low as 22.5%, and the mean OS was only 25.3 months [10], consistent with our previous studies [11]. CCC has a unique developmental pathway and possibly originates from endometriosis [4]. However, a management and efficacy monitoring strategy specifically for ovarian CCC has not been established, in part due to the relative rarity of this tumor type. Therefore, ovarian CCC is treated and monitored in the same way as other histological subtypes of EOC.
Carbohydrate antigen 125 (CA-125) is a glycoprotein antigen that is a predominantly used in the clinical setting to evaluate tumor response and to predict relapse in patients with EOC [12-16]. However, the prognostic value of CA-125 in patients with ovarian CCC has seldom been addressed in the literature [17-19], and the conclusions have been controversial. In the present study, we investigated the clinical implications of pre- and post-treatment serum CA-125 levels in patients with ovarian CCC to provide useful information for the improvement of monitoring strategies for this lethal disease.
RESULTS
Clinico-pathological characteristics
A total of 375 women met the eligibility criteria during the study period and were included in this analysis, and 164 of these patients who developed recurrent or persistent disease after primary treatment were described previously [11]. Table 1 shows the demographic and clinico-pathological characteristics of the 375 women. The mean age at initial diagnosis was 50.8 years, and 191 of the cases (50.9%) were premenopausal. Ascites and EAOC were present in 139 (37.1%) and 132 (35.2%) patients, respectively. The FIGO staging was distributed as follows: 180 cases (45%) were stage I (Ia: 63; Ib: 4; Ic: 113), 43 cases (11.5%) were stage II (IIa: 9; IIb: 13; IIc: 21), 132 cases (35.2%) were stage III, and 20 cases (5.3%) were stage IV. Initial pelvic and para-aortic lymphadenectomy was performed in 259 patients (69.1%). Node involvement was present in 74 patients, including one woman who had a positive left supraclavicular lymph node and was exempted from lymphadenectomy. Thirty-eight patients (10.1%) had macroscopic residual disease (residual tumor > 1 cm) within the abdominopelvic cavity after the initial surgery. Platinum/taxane chemotherapy was performed on 264 patients (70.4%) as the front-line therapy, and the remaining 111 patients received conventional platinum-based regimens.
Table 1: Clinicopathologic characteristics of the 375 patients with ovarian clear cell carcinoma (CCC)
Parameter |
Number of patient |
Percent (%) |
|
|---|---|---|---|
Age(Mean;range) |
50.8 ± 10.7 ; (29–85) |
||
≤45 |
128 |
34.1 |
|
>45 |
247 |
65.9 |
|
FIGO Stage at diagnosis |
|||
I |
180 |
45.0 |
|
II |
43 |
11.5 |
|
III |
132 |
35.2 |
|
IV |
20 |
5.3 |
|
Endometriosis |
|||
+ |
132 |
35.2 |
|
− |
243 |
64.8 |
|
Ascites |
|||
+ |
139 |
37.1 |
|
− |
236 |
62.9 |
|
Initial CRSa |
|||
Optimal |
337 |
89.9 |
|
Suboptimal |
38 |
10.1 |
|
Initial lymphadenectomy |
|||
+ |
259 |
69.1 |
|
− |
116 |
30.9 |
|
LNMb |
|||
+ |
74 |
28.6 |
|
− |
185 |
71.4 |
|
First line chemotherapy |
|||
Taxane and platinum |
264 |
70.4 |
|
Conventinal platinum-based regimen |
111 |
29.6 |
|
Pretreatment CA-125 (U/mL) (mean;range) |
1066.1 ± 1945.2; (1.9-17171.5) |
||
≤ 35 |
79 |
21.1 |
|
> 35 |
296 |
78.9 |
|
Disease status at completion of primary chemotherapy |
|||
NEDc |
343 |
91.5 |
|
Persistent disease |
Stable |
25 |
8.5 |
Progressive |
7 |
||
Relapse interval (month)( mean;range) |
21.5 ± 24.3; (2-153) |
||
RFSd time(month)( mean;range) |
41.3 ±39.3; (1-201) |
||
OSe time(month)( mean;range) |
47.4±39.3; (1-201) |
||
Status at the last contact |
|||
NED |
225 |
60.0 |
|
AWDf |
80 |
31.3 |
|
DODg |
70 |
18.7 |
|
Note: a: cytoreductive surgery; b:Lymph node metastasis; c: No evidence of disease; d: relapse-free survival; e: Overall survival; f: Alive with disease; g: Dead of disease.
The relationship between pretreatment (prechemotherapy) CA-125 levels and clinico-pathological characteristics
Pretreatment CA-125 levels were elevated in the majority (78.9%) of patients with CCC. The median value was 1066.1 U/mL ± 1945.2, although this value ranged widely, from 1.9 to 17171.5 U/mL. Table 2 shows potential risk factors related to pretreatment CA-125 elevation. Patients with early-stage (stages I and II) disease and EAOC without residual tumors (≤ 1 cm) exhibited a significantly lower risk of elevated pretreatment CA-125 values (> 35 U/mL) compared to patients with advanced stage (stages III and IV), negative EAOC, and positive residual tumors (> 1 cm) (p < 0.001, p < 0.001 and p = 0.001, respectively).
Table 2: The association between pretreatment CA-125 levels and clinico-pathologic characteristics for patients with CCC
Parameter |
Pretreatment CA-125 |
P valuea |
|
|---|---|---|---|
Elevated |
Normal |
||
Age(Mean;range) |
|||
≤45 |
99 |
29 |
0.587 |
>45 |
197 |
50 |
|
FIGO Stage at diagnosis |
|||
I+II |
158 |
65 |
<0.001 |
III+ IV |
138 |
14 |
|
Endometriosis |
|||
+ |
65 |
67 |
<0.001 |
− |
231 |
12 |
|
Ascites |
|||
+ |
103 |
36 |
0.078 |
− |
193 |
43 |
|
Initial surgery |
|||
Optimal |
259 |
78 |
0.001c |
Suboptimal |
37 |
1 |
|
Initial lymphadenectomy |
|||
+ |
207 |
52 |
0.483 |
− |
89 |
27 |
|
LNM |
|||
+ |
61 |
13 |
0.477 |
− |
146 |
40 |
|
Note: a: Chi-square test; b: Logistic regression analysis; CI: Confidence intervals; d: Fisher’s exact test.
The median pretreatment CA-125 levels of patients with early-stage CCC, negative residual tumors, and EAOC were significantly lower than patients with advanced stage disease, positive residual tumors, and negative EAOC (early vs. advanced stage: 881.3 U/mL vs. 1337.1 U/mL, p < 0.001; negative vs. positive residual tumor: 925.5 U/mL vs. 2312.7 U/mL, p < 0.001; positive vs. negative EAOC: 738.6 U/mL vs. 1243.9 U/mL, p = 0.035).
Status at last contact
Thirty-two (19.5%) patients had persistent disease, including stable disease (25 cases) and progressive disease (7 cases), after the completion of primary treatment. The remaining 342 patients showed no evidence of disease upon imaging examination. A total of 132 (7.0%) patients relapsed during the follow-up period (47.4 ± 39.3 months). The relapse interval was 21.5± 24.3 months and ranged from 2 to 153 months. The sites of recurrent and persistent disease included the abdomen or pelvis (109 patients), liver (49), lymph nodes (21), vaginal stump (20), spleen (19), chest cavity (5), lung (5), and other sites (38). Salvage treatments for the 164 patients with recurrent and persistent disease consisted of repeated CRS, salvage chemotherapy, and radiotherapy, which were performed in 86 (53.7%), 164 (100%), and 21 (12.8%) cases, respectively, and 14 (8.5%) of these patients regained tumor control. Seventy (18.7%) women had died of the disease by last contact. Eighty (31.3%) patients were alive but still had tumors, and 16 patients had end-stage cancer. A total of 225 (60.0%) cases survived without any evidence of residual tumor at the time of the last visit. These data were described in detail previously [11].
Patient CA-125 levels normalized either before chemotherapy (76 cases), between cycles 1 and 2 (69 cases), between cycles 2 and 3 (63 cases), between cycles 3 and 4 (50 cases), between cycles 4 and 6 (48 cases), or after 6 cycles (44 cases). A lack of normalization by the completion of primary treatment was exhibited in 25 patients.
The prognostic significance of pretreatment CA-125 levels and CA-125 normalization in ovarian CCC
The 5- and 10-year RFS rates were 56.0% and 49.7%, respectively, and the 5- and 10-year OS rates were 78.8% and 69.4%, respectively, for the entire series. Residual tumor and stage significantly impacted relapse rates in the univariate survival analysis (both p < 0.001; Table 3). Residual tumor, stage, and LNM were identified as risk factors for survival (P < 0.001, < 0.001 and = 0.039, respectively). Multivariate analysis revealed that stage was the only significant prognostic factor for relapse (P < 0.001). Residual tumor and advanced stage (P = 0.001, and < 0.001, respectively) were identified as adverse factors for survival in the multivariate analysis (Table 3 and Figure 1-a, b and 1c). The 5-year RFS rate in the advanced stage subgroup was as low as 12.1% vs. 78.5% in the early-stage subgroup. The 5-year OS rate for patients with advanced stage diseases and residual tumors was 37.7% compared with 94.5% for patients with early-stage diseases.
Table 3: Risk factors related to EFS and OS for patients with ovarion CCC
Parameter |
Relapsea |
P valueb |
P valuec |
HRd (95% CIe) |
DOD |
P valueb |
P valuec |
HRd (95% CI) |
||
|---|---|---|---|---|---|---|---|---|---|---|
+ |
− |
+ |
− |
|||||||
Age |
||||||||||
≤50 |
45 |
74 |
0.944 |
28 |
100 |
0.297 |
||||
>50 |
87 |
135 |
42 |
205 |
||||||
Optimal CRS |
||||||||||
Optimal |
111 |
207 |
<0.001 |
47 |
290 |
<0.001 |
0.001 |
2.48 (1.46-2.41) |
||
Suboptimal |
21 |
2 |
23 |
15 |
||||||
FIGO Stage |
||||||||||
I+II |
43 |
180 |
<0.001 |
<0.001 |
7.79 (5.36-11.33) |
14 |
209 |
<0.001 |
<0.001 |
6.91 (3.72-12.84) |
III+IV |
89 |
29 |
56 |
96 |
||||||
Endometriosis |
||||||||||
+ |
39 |
86 |
0.058 |
18 |
114 |
0.072 |
||||
− |
93 |
123 |
52 |
191 |
||||||
Ascites |
||||||||||
+ |
53 |
76 |
0.129 |
24 |
115 |
0.897 |
||||
− |
79 |
133 |
46 |
190 |
||||||
Lymphadenectomy |
||||||||||
+ |
92 |
144 |
0.827 |
46 |
213 |
0.407 |
||||
− |
40 |
65 |
24 |
92 |
||||||
LNM |
||||||||||
+ |
31 |
38 |
0.129 |
20 |
54 |
0.039 |
||||
− |
61 |
107 |
26 |
160 |
||||||
First line chemotherapy |
||||||||||
Taxane and platinum |
96 |
144 |
0.557 |
50 |
214 |
0.835 |
||||
Other regimens |
36 |
65 |
20 |
91 |
||||||
Pretreatment CA-125 (U/mL) |
||||||||||
≤35 |
23 |
55 |
0.060 |
11 |
68 |
0.176 |
||||
>35 |
109 |
154 |
59 |
237 |
||||||
Note: a:Thirty-two patients with persisitent disease were not included in this analysis;b: Log rank test; c: Cox proportional hazards model; d: Hazard ratios; e: Confidence intervals.
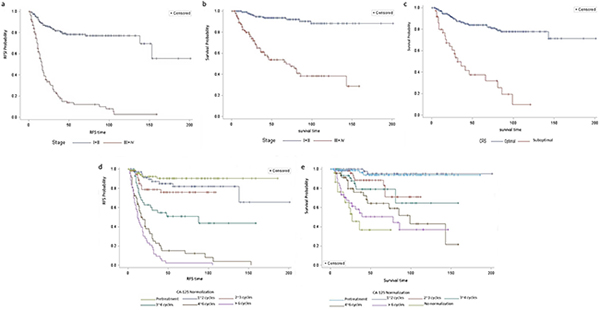
Figure 1: Risk factors related to relapse and survival. Stage was the only significant prognostic factor for relapse (P < 0.001, panel a). Residual tumor and advanced stage (P = 0.001, and < 0.001, respectively; panel b and c) were identified as adverse factors for survival in the multivariate analysis. Serial CA-125 measurements during chemotherapy cycles were prognostic of disease progression and survival (panels d and e). The 5-year RFS rates were 90.1% and 82.1%, and the 5-year OS rates were 94.0% and 95.2% (RFS: p = 0.327; OS: p = 0.654), respectively, for patients whose CA-125 levels normalized prior to chemotherapy or between cycles 1 and 2. These two parameters successively decreased from 82.1% to 2.3% and from 95.2% to 50.1% in patients whose CA-125 levels normalized after cycles 2 ~ 6 cycles, respectively. The 5-year OS rate was as low as 36.7% for patients who never attained normalized CA-125 levels.
Pretreatment CA-125 levels and EAOC were not identified as significant predictors of RFS and OS. The clinical outcome of patients with elevated CA-125 levels was slightly inferior to that of patients with normal CA-125 levels (5-year RFS: 53.7% vs. 63.8%, p = 0.060; 5-year OS: 76.9% vs. 86.1, p = 0.176). By contrast, the prognosis for patients with positive EAOC was slightly better than for patients with negative EAOC (5-year RFS: 66.5% vs. 51.3%, p = 0.058; 5-year OS: 85.9% vs. 75.0, p = 0.072).
Pretreatment CA-125 levels were not associated with patient prognosis. However, serial CA-125 measurements during chemotherapy cycles were prognostic of disease progression and survival (Table 4, Figure 1-d and 1e, and Figure 2). Patients whose CA-125 levels normalized between cycles 1 and 2 had a similar prognosis (RFS: p = 0.327; OS: p = 0.654) as patients whose CA-125 normalized prior to chemotherapy. By contrast, patients whose CA-125 levels normalized between cycles 2 and 3, between cycles 3 and 4, between cycles 4 and 6, after 6 cycles, or never normalized were significantly more likely to experience disease progression. The 5-year RFS rates were 90.1% and 82.1%, and the 5-year OS rates were 94.0% and 95.2%, respectively, for patients whose CA-125 levels normalized prior to chemotherapy or between cycles 1 and 2. These two parameters successively decreased from 82.1% to 2.3% and from 95.2% to 50.1% in patients whose CA-125 levels normalized after cycles 2 ~ 6 cycles, respectively. The 5-year OS rate was as low as 36.7% for patients who never attained normalized CA-125 levels.
Table 4: The prognostic significance of CA-125 normalization in ovarian CCC
CA-125 normalization |
No. (%) |
FIGO stage (%) |
CRS (%) |
RFS |
OS |
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
I+II |
III+IV |
P valuea |
Optimal |
Suboptimal |
P valueb |
5-year RFS(%) |
P valuec |
5-year OS(%) |
P valuec |
||
Pretreament |
76 (20.3) |
63 (82.9) |
13 (17.1) |
Referrence |
76 (100) |
0 (0) |
Referrence |
90.1 |
Referrence |
94.0 |
Referrence |
Between cycles 1 and 2 |
69 (18.4) |
55 (79.7) |
14 (20.3) |
0.623 |
66 (95.7) |
3 (4.3) |
0.103 |
82.1 |
0.327 |
95.2 |
0.654 |
Between cycles 2 and 3 |
63 (16.8) |
42 (66.7) |
21 (33.3) |
0.027 |
57 (90.5) |
6 (9.5) |
0.008 |
76.2 |
0.013 |
88.7 |
0.030 |
Between cycles 3 and 4 |
50 (13.3) |
30 (60.0) |
20 (40.0) |
0.004 |
45 (90.0) |
5 (10.0) |
0.009 |
51.0 |
<0.001 |
79.0 |
0.003 |
Between cycles 4 and 6 |
48 (12.8) |
21 (43.8) |
27 (56.1) |
<0.001 |
42 (87.5) |
6 (12.5) |
0.003 |
15.2 |
<0.001 |
64.4 |
<0.001 |
After 6 cycles |
44 (11.7) |
12 (27.3) |
32 (72.7) |
<0.001 |
38 (86.4) |
6 (13.6) |
0.002 |
2.3 |
<0.001 |
50.1 |
<0.001 |
No normalized |
25 (6.7) |
0 (0) |
25 (100) |
<0.001b |
13 (52.0) |
12 (48.0) |
<0.001 |
- |
- |
36.7 |
<0.001 |
Note: a: Chi-square test; b: Fisher’s exact test; C: Log rank test.
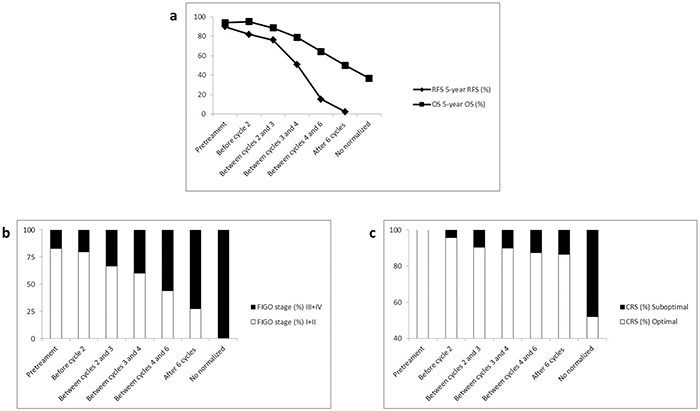
Figure 2: CA-125 normalization before the second cycle of chemotherapy is an inflection point when predicting relapse and survival in patients with CC. Number of chemotherapy cycles for CA-125 normalization was positively correlated with advanced stage (r = 0.97, P = 0.001) and residual tumor (r = 0.81, P = 0.027), whereas it was negatively correlated with 5-year RFS (r = -0.97, P = 0.002) and 5-year OS (r = -0.97, P = 0.001; Figure 2). CA-125 normalization before chemotherapy cycle 2 was associated with a significantly higher rate of early-stage disease and negative residual tumor, which were identified as favorable factors for relapse and survival.
The rates of early-stage disease and negative residual tumor were markedly higher in patients whose CA-125 levels normalized before chemotherapy or between cycles 1 and 2 compared with patients who normalized after chemotherapy cycle 2 and failed to normalize during first-line chemotherapy, when the data were stratified by CA-125 normalization after chemotherapy. Linear correlation analysis also demonstrated that the number of chemotherapy cycles for CA-125 normalization was positively correlated with advanced stage (r = 0.97, P = 0.001) and residual tumor (r = 0.81, P = 0.027), whereas it was negatively correlated with 5-year RFS (r = -0.97, P = 0.002) and 5-year OS (r = -0.97, P = 0.001; Figure 2). CA-125 normalization before chemotherapy cycle 2 was associated with a significantly higher rate of early-stage disease and negative residual tumor, which were identified as favorable factors for relapse and survival. Therefore, CA-125 normalization before chemotherapy cycle 2 is a useful predictor for improved RFS and OS.
DISCUSSION
Clinico-pathological factors associated with elevated pretreatment CA-125 levels
Pretreatment CA-125 levels were elevated in the majority (78.9%) of patients with CCC in our series, which was consistent with the study by Tian and colleagues [17]. The potential risk factors related to elevated pretreatment CA-125 levels included advanced-stage disease, residual tumors after initial CRS and negative EAOC. For patients with these high-risk factors, the elevation rate and absolute value of pretreatment CA-125 levels were significantly higher compared with patients with early-stage disease, negative residual tumor and positive EAOC.
FIGO stage and optimal initial CRS are the two most important prognostic factors for patients with ovarian CCC [17, 24], similar to other cell types of EOC. Based on our data, the 5-year RFS rates and 5-year OS rates were 56.0% and 78.8%, respectively, for the entire series. The 5-year RFS rate for patients with advanced disease was as low as 12.1% compared with 78.5% for patients with early-stage disease when stratified by FIGO stage. The 5-year OS rate for patients with advanced stage diseases and positive residual tumors after initial CRS was only 37.7% compared with 94.5% for patients with early-stage disease. Kim et al. [19] also demonstrated that elevated CA-125 levels were a useful marker for predicting advanced stage disease, suboptimal debulking and platinum-resistance in patients with ovarian CCC, consistent with our analysis.
Ovarian CCC is one of the most common histological subtypes of EOC that is associated with endometriosis, with a frequency that ranges widely from 9% to 70% [22, 25-30], and endometriosis may increase the risk for this disease [26, 31-33]. EAOC presented in 35.2% of patients in our series. The present analysis confirmed our previous study [24] showing that EAOC negatively impacts the risk of elevated CA-125 and the absolute value of this biomarker in patients with CCC. The prognostic implications of endometriosis in ovarian CCC are controversial. Orezzoli [22] and Komiyama [28] found that patients with EAOC tended to have a favorable prognosis. Additionlly, the patient group in their study was likely younger with earlier stage disease [22]. Erzen et al. [25] demonstrated that EAOC exhibited lower stages at presentation and a better clinical outcome in patients with various histological subtypes of EOC, including CCC. This increased survival was evident in all age groups and all histological subtypes, and it could not be explained by better stage specific survival in any FIGO stage. Patients with EAOC in this analysis experienced slightly more favorable clinical outcomes compared with patients with negative EAOC (5-year RFS: 66.5% vs. 51.3%; 5-year OS: 85.9% vs. 75.0). However, this difference was not statistically significant (p = 0.058 and p = 0.072, respectively), consistent with our previous study [24]. Cutt et al. [26] also claimed that endometriosis per se is not predictive of prognosis in ovarian CCC. Therefore, the prognostic implication of endometriosis for ovarian CCC remains unclear, and further investigation will be necessary.
The prognostic value of CA-125 normalization in ovarion CCC
The likelihood of elevated pretreatment CA-125 as well as pretreatment CA-125 levels themselves both increased significantly in patients with adverse prognostic factors, including advanced stage and positive residual tumor, whereas they decreased in patients with EAOC, a potentially favorable factor. However, absolute value of pretreatment CA-125 level was not identified as a predictor of relapse and survival based on our data or previous reports [17, 19]. Serial CA-125 measurements during chemotherapy treatment were indeed prognostic, and normalization before the second cycle of chemotherapy was associated with a significantly decreased risk of relapse and death. By contrast, patients with CA-125 levels that normalized after the completion of cycle 1 or never normalized were significantly more likely to experience disease progression. The 5-year RFS and OS rates in the current study were 90.1% and 94.0%, respectively, for patients whose CA-125 level normalized either before chemotherapy or before cycle 2. These two parameters successively decreased from 82.1% and 95.2% to 2.3% and 50.1% when CA-125 normalized before cycle 2 compared with after cycle 6, respectively. These two parameters successively decreased respectively from 82.1% and 95.2% to 2.3% and 50.1% in patients whose CA-125 levels normalized after cycles 2 ~ 6 cycles, respectively. Furthermore, the 5-year OS rate was as low as 36.7% for patients who never normalized their CA-125 levels. No normalization of CA-125 after the completion of first-line chemotherapy was a sufficient condition for persistent disease. Therefore, this patient group was excluded from RFS-related analysis.
The prognostic value of CA-125 normalization before and after chemotherapy is well characterized in patients with EOC. Meyer et al. [34] concluded that CA-125 normalization at the third cycle of chemotherapy carried the greatest prognostic significance of any measurement during the treatment of primary disease. Zorn et al. [35] demonstrated that CA-125 normalization prior to chemotherapy was an independent predictor of PFS in patients with advanced EOC, particularly when tumors were debulked to a microscopic residual tumor and in the serous or endometrioid subtypes. Finally, CA-125 normalization before the second cycle of chemotherapy was associated with a decreased risk of death in an ancillary analysis of a phase III study of women with advanced serous ovarian carcinoma [16].
CA-125 normalization before the second cycle of chemotherapy is an inflection point when predicting relapse and survival in patients with CCC
The prognostic value of CA-125 normalization in patients with ovarian CCC has not been well studied. Tian et al. [17] compared clinical outcome in patients with advanced CCC whose CA125 levels normalized to patients whose CA125 levels failed to normalize by the end of treatment. They concluded that CA-125 normalization by the end of treatment could be a valid indicator of RFS and OS, and likely reflected the degree of inherent chemosensitivity. However, the predictive role of CA-125 normalization was not stratified or compared with different cycles of chemotherapy in that study, likely due to their relatively small sample size (only 77 patients had CA-125 data recorded during treatment). Our analysis revealed that patient outcome grew worse as CA-125 normalization came later and later in the chemotherapy cycles. Indeed, CA-125 normalization before chemotherapy cycle 2 was a distinct inflection point for RFS and OS.
The rates of early-stage disease and negative residual tumor were markedly higher in patients whose CA-125 levels normalized before chemotherapy cycle 2 than in patients who normalized after the completion of chemotherapy cycle 1, when stratified by CA-125 normalization after chemotherapy. Linear correlation analysis also demonstrated that CA-125 normalization was positively correlated with advanced stage and suboptimal CRS, whereas it was negatively correlated with 5-year RFS and 5-year OS. CA-125 normalization before chemotherapy cycle 2 was associated with significantly higher rates of early-stage disease and negative residual tumor, which were identified as favorable factors for relapse and survival. Therefore, CA-125 normalization before chemotherapy cycle 2 may be a useful predictor for improved RFS and OS.
This analysis included results from 375 cases with ovarian CCC, making it one of the largest studies on this rare disease, despite its retrospective nature. Patient clinico-pathological data and follow-up information in the present study were relatively complete. These strengths enabled us to perform a robust analysis to evaluate the prognosis-predicting value of CA-125 normalization, and our findings provide useful information to improve monitoring strategies for this lethal tumor.
MATERIALS AND METHODS
The medical records of all CCC patients diagnosed and treated at Peking Union Medical College Hospital (PUMCH) and Beijing Chao-Yang Hospital between 1993 and 2013 were collected and reviewed. Patients whose tumor specimens from the initial surgery were histologically confirmed as pure-type ovarian CCC were included for further analysis. Patients suffering from a primary malignant tumor in another part of the body or other malignant ovarian cell types were also excluded. Patient information, including demographic and pathological characteristics, surgery, subsequent systemic chemotherapy, and disease status at last contact, were collected and evaluated.
Serum CA-125 levels were measured using a radioimmunoassay kit (Roche F170 Modular system). Rising CA-125 levels were defined as a progressive increase in three consecutive serum antigen values above 35 U/mL, which is the commonly accepted normal upper limit for CA-125. Serum CA-125 served as both a pre- and post-operative tumor marker, and levels were evaluated within one week prior to staging surgery or cytoreductive surgery (CRS), prior to each cycle of chemotherapy, and at each contact during the follow-up period.
The surgical procedures, subsequent systemic chemotherapy, and the follow-up strategy after the completion of treatment were carried out as previously described [11]. Briefly, the predominant initial surgical procedure consisted of cytoreductive surgery or staging surgery. Ascites or washings were routinely collected before surgery, and cytological data were evaluated for all of the patients. Lymphadenectomy was not mandatory. Two independent pathologists with extensive experience in gynecological pathology reviewed all of the pathological slides for this analysis, and these pathologists were blinded to patient outcome. Disease staging was re-assigned using the exact FIGO staging criteria [20]. Optimal CRS was defined as abdominopelvic residual disease ≤1 cm after debulking surgery. Endometriosis-associated ovarian carcinoma (EAOC) was defined as the co-existence of CCC with endometriosis in the same and/or contralateral ovary and/or the co-existence of CCC with extraovarian endometriosis [21, 22].
Taxane/platinum or conventional cis/carboplatin-based chemotherapy (6 to 9 cycles) were administered as the post-operative first-line treatment. Responses to the systemic agents were recorded using version 1.1 of the Response Evaluation Criteria in Solid Tumors (RECIST) [23]. GCIG CA-125 response criteria [12] were used in the absence of measurable disease.
Relapse was documented using histological evidence of disease from tumor biopsies or fine-needle biopsies and/or the appearance of new lesions during imaging examinations. Relapse-free survival (RFS) times were calculated as the period between the date of initial surgery and the date of relapse. Women who were disease free at the time of their last visit were censored. OS times were calculated in months from the date of the initial surgery to the date of patient death from the disease. Patients who died from other conditions as well as patients surviving at the time of their last visit were censored.
Patient records and information were anonymized and de-identified prior to analysis; therefore consent was not necessary. The study protocol was approved by the ethics committee respectively at PUMCH and Beijing Chao-Yang Hospital, Beijing, China.
Statistical analysis
All statistical analyses were performed using SAS® Version 9.2 (SAS Institute, Cary, NC). All of the tests were 2 sided, and P < 0.05 was considered statistically significant. Chi square or Fisher exact tests was performed to identify high-risk factors for elevated serum CA-125 levels. The two-tailed independent-sample Wilcoxon Rank Sum test was used to compare serum CA-125 levels between subgroups. The Kaplan-Meier method was used to analyze relapse and survival. A log rank test was used to compare the different survival curves. A Cox proportional hazards model was applied to all parameters that were significant in the univariate analysis. Simple lineal regression analysis was used to estimate linear correlations between CA-125 normalization and prognostic predictors.
CONCLUSIONS
FIGO stage and residual tumor after initial CRS were the most important prognostic factors for ovarian CCC. CA-125 elevation rate and absolute value increased significantly in patients with advanced stage and residual tumor after initial CRS and decreased in patients with EAOC, which is itself a contested favorable factor for prognosis. However, CA-125 levels at pretreatment were not useful for predicting patient clinical outcome. CA-125 levels after treatment was a valid indicator for treatment monitoring. CA-125 normalization after the completion of cycle 1 of chemotherapy was a distinct inflection point for decreased RFS and OS.
ACKNOWLEDGMENTS
This work is supported by Major projects of Science and Technology Program of Beijing Scientific Committee (No. D151100001915004) and National High Technology Research and Development Program of China (No. 2012AA02A507; No. 2014AA020606).
Source of the study
1 Peking Union Medical College Hospital, Chinese Academy of Medical Sciences Peking Union Medical College;
2 Beijing Chao-Yang Hospital, Capital Medical University.
Authors’ contributions
HM B, ZY Z, and K S: Conception and design of the study, assembly, analysis and interpretation of the data, manuscript writing. The other authors: Provision of study material or patients, analysis and interpretation of the data.
REFERENCES
1. Correa P, O’Conor GT, Berard CW, Axtell LM and Myers MH. International comparability and reproducibility in histologic subclassification of Hodgkin’s disease. Journal of the National Cancer Institute. 1973; 50:1429-1435.
2. Pather S and Quinn MA. Clear-cell cancer of the ovary-is it chemosensitive? International journal of gynecological cancer. 2005; 15:432-437.
3. Davis M, Rauh-Hain JA, Andrade C, Boruta DM, 2nd, Schorge JO, Horowitz NS, May T and del Carmen MG. Comparison of clinical outcomes of patients with clear cell and endometrioid ovarian cancer associated with endometriosis to papillary serous carcinoma of the ovary. Gynecologic oncology. 2014; 132:760-766.
4. Anglesio MS, Carey MS, Kobel M, Mackay H and Huntsman DG. Clear cell carcinoma of the ovary: a report from the first Ovarian Clear Cell Symposium, June 24th, 2010. Gynecologic oncology. 2011; 121:407-415.
5. Chan JK, Teoh D, Hu JM, Shin JY, Osann K and Kapp DS. Do clear cell ovarian carcinomas have poorer prognosis compared to other epithelial cell types? A study of 1411 clear cell ovarian cancers. Gynecologic oncology. 2008; 109:370-376.
6. Pectasides D, Fountzilas G, Aravantinos G, Kalofonos C, Efstathiou H, Farmakis D, Skarlos D, Pavlidis N, Economopoulos T and Dimopoulos MA. Advanced stage clear-cell epithelial ovarian cancer: the Hellenic Cooperative Oncology Group experience. Gynecologic oncology. 2006; 102:285-291.
7. Ho CM, Huang YJ, Chen TC, Huang SH, Liu FS, Chang Chien CC, Yu MH, Mao TL, Wang TY and Hsieh CY. Pure-type clear cell carcinoma of the ovary as a distinct histological type and improved survival in patients treated with paclitaxel-platinum-based chemotherapy in pure-type advanced disease. Gynecologic oncology. 2004; 94:197-203.
8. Mahdi H, Moslemi-Kebria M, Levinson KL, Gojayev A, Lockhart D, Ali-Fehmi R and Munkarah AR. Prevalence and prognostic impact of lymphadenectomy and lymph node metastasis in clinically early-stage ovarian clear cell carcinoma. International journal of gynecological cancer. 2013; 23:1226-1230.
9. Mackay HJ, Brady MF, Oza AM, Reuss A, Pujade-Lauraine E, Swart AM, Siddiqui N, Colombo N, Bookman MA, Pfisterer J and du Bois A. Prognostic relevance of uncommon ovarian histology in women with stage III/IV epithelial ovarian cancer. International journal of gynecological cancer. 2010; 20:945-952.
10. Kajiyama H, Shibata K, Mizuno M, Yamamoto E, Fujiwara S, Umezu T, Suzuki S, Nakanishi T, Nagasaka T and Kikkawa F. Postrecurrent oncologic outcome of patients with ovarian clear cell carcinoma. International journal of gynecological cancer. 2012; 22:801-806.
11. Bai H, Sha G, Cao D, Yang J, Chen J, Wang Y, Lang J, Shen K and Zhang Z. Salvage Chemotherapy for Patients With Recurrent or Persistent Ovarian Clear Cell Carcinoma: A Retrospective Study of 164 Cases. Medicine. 2015; 94:e1121.
12. Rustin GJ, Vergote I, Eisenhauer E, Pujade-Lauraine E, Quinn M, Thigpen T, du Bois A, Kristensen G, Jakobsen A, Sagae S, Greven K, Parmar M, Friedlander M, Cervantes A and Vermorken J. Definitions for response and progression in ovarian cancer clinical trials incorporating RECIST 1.1 and CA 125 agreed by the Gynecological Cancer Intergroup (GCIG). International journal of gynecological cancer. 2011; 21:419-423.
13. Rustin GJ, Timmers P, Nelstrop A, Shreeves G, Bentzen SM, Baron B, Piccart MJ, Bertelsen K, Stuart G, Cassidy J and Eisenhauer E. Comparison of CA-125 and standard definitions of progression of ovarian cancer in the intergroup trial of cisplatin and paclitaxel versus cisplatin and cyclophosphamide. Journal of clinical oncology. 2006; 24:45-51.
14. Juretzka MM, Barakat RR, Chi DS, Iasonos A, Dupont J, Abu-Rustum NR, Poynor EA, Aghajanian C, Spriggs D, Hensley ML and Sabbatini P. CA125 level as a predictor of progression-free survival and overall survival in ovarian cancer patients with surgically defined disease status prior to the initiation of intraperitoneal consolidation therapy. Gynecologic oncology. 2007; 104:176-180.
15. Fader AN, Java J, Ueda S, Bristow RE, Armstrong DK, Bookman MA and Gershenson DM. Survival in women with grade 1 serous ovarian carcinoma. Obstetrics and gynecology. 2013; 122(2 Pt 1):225-232.
16. Fader AN, Java J, Krivak TC, Bristow RE, Tergas AI, Bookman MA, Armstrong DK, Tanner EJ and Gershenson DM. The prognostic significance of pre- and post-treatment CA-125 in grade 1 serous ovarian carcinoma: a gynecologic Oncology Group study. Gynecologic oncology. 2014; 132:560-565.
17. Tian C, Markman M, Zaino R, Ozols RF, McGuire WP, Muggia FM, Rose PG, Spriggs D and Armstrong DK. CA-125 change after chemotherapy in prediction of treatment outcome among advanced mucinous and clear cell epithelial ovarian cancers: a Gynecologic Oncology Group study. Cancer. 2009; 115:1395-1403.
18. Eltabbakh GH, Mount SL, Beatty B, Simmons-Arnold L and Cooper K. Clinical and molecular differences between clear cell and papillary serous ovarian carcinoma. Journal of surgical oncology. 2006; 93:379-386.
19. Kim HS, Choi HY, Lee M, Suh DH, Kim K, No JH, Chung HH, Kim YB and Song YS. Systemic Inflammatory Response Markers and CA-125 Levels in Ovarian Clear Cell Carcinoma: A Two Center Cohort Study. Cancer Res Treat. 2016; 48:250-8.
20. Prat J. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. International journal of gynaecology and obstetrics. 2014; 124:1-5.
21. Wang S, Qiu L, Lang JH, Shen K, Yang JX, Huang HF, Pan LY and Wu M. Clinical analysis of ovarian epithelial carcinoma with coexisting pelvic endometriosis. American journal of obstetrics and gynecology. 2013; 208:413.e411-415.
22. Orezzoli JP, Russell AH, Oliva E, Del Carmen MG, Eichhorn J and Fuller AF. Prognostic implication of endometriosis in clear cell carcinoma of the ovary. Gynecologic oncology. 2008; 110:336-344.
23. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, Kaplan R, Lacombe D and Verweij J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). European journal of cancer. 2009; 45:228-247.
24. Ye S, Yang J, You Y, Cao D, Bai H, Lang J, Chen J and Shen K. Comparative study of ovarian clear cell carcinoma with and without endometriosis in People’s Republic of China. Fertility and sterility. 2014; 102:1656-1662.
25. Erzen M, Rakar S, Klancnik B and Syrjanen K. Endometriosis-associated ovarian carcinoma (EAOC): an entity distinct from other ovarian carcinomas as suggested by a nested case-control study. Gynecologic oncology. 2001; 83:100-108.
26. Cuff J and Longacre TA. Endometriosis does not confer improved prognosis in ovarian carcinoma of uniform cell type. The American journal of surgical pathology. 2012; 36:688-695.
27. Kumar S, Munkarah A, Arabi H, Bandyopadhyay S, Semaan A, Hayek K, Garg G, Morris R and Ali-Fehmi R. Prognostic analysis of ovarian cancer associated with endometriosis. American journal of obstetrics and gynecology. 2011; 204:63.e61-67.
28. Komiyama S, Aoki D, Tominaga E, Susumu N, Udagawa Y and Nozawa S. Prognosis of Japanese patients with ovarian clear cell carcinoma associated with pelvic endometriosis: clinicopathologic evaluation. Gynecologic oncology. 1999; 72:342-346.
29. Ogawa S, Kaku T, Amada S, Kobayashi H, Hirakawa T, Ariyoshi K, Kamura T and Nakano H. Ovarian endometriosis associated with ovarian carcinoma: a clinicopathological and immunohistochemical study. Gynecologic oncology. 2000; 77:298-304.
30. Rauh-Hain JA, Davis M, Clemmer J, Clark RM, Growdon WB, Goodman AK, Boruta DM, 2nd, Schorge JO and del Carmen MG. Prognostic determinants in patients with uterine and ovarian clear cell carcinoma: a SEER analysis. Gynecologic oncology. 2013; 131:404-409.
31. Kim HS, Kim TH, Chung HH and Song YS. Risk and prognosis of ovarian cancer in women with endometriosis: a meta-analysis. British journal of cancer. 2014; 110:1878-1890.
32. Pearce CL, Templeman C, Rossing MA, Lee A, Near AM, Webb PM, Nagle CM, Doherty JA, Cushing-Haugen KL, Wicklund KG, Chang-Claude J, Hein R, Lurie G, Wilkens LR, Carney ME, Goodman MT, et al. Association between endometriosis and risk of histological subtypes of ovarian cancer: a pooled analysis of case-control studies. The Lancet Oncology. 2012; 13:385-394.
33. Nagle CM, Olsen CM, Webb PM, Jordan SJ, Whiteman DC and Green AC. Endometrioid and clear cell ovarian cancers: a comparative analysis of risk factors. European journal of cancer. 2008; 44:2477-2484.
34. Meyer T and Rustin GJ. Role of tumour markers in monitoring epithelial ovarian cancer. British journal of cancer. 2000; 82:1535-1538.
35. Zorn KK, Tian C, McGuire WP, Hoskins WJ, Markman M, Muggia FM, Rose PG, Ozols RF, Spriggs D and Armstrong DK. The prognostic value of pretreatment CA 125 in patients with advanced ovarian carcinoma: a Gynecologic Oncology Group study. Cancer. 2009; 115:1028-1035.