
INTRODUCTION
Nasopharyngeal carcinoma (NPC) is a unique malignancy with a remarkable geographic distribution, which occurs with much greater frequency in Southern China [1, 2]. The recent reported incidence of NPC in Southern China is 30–80 per 100,000 people per year [3]. The current standard regimen is radiotherapy (RT) alone for early-stage disease and concurrent chemoradiotherapy (CRT) for locally advanced disease [1]. Although NPC is mostly radiosensitive, 20–30% of patients ultimately develop distant metastasis and/or recurrence despite of treatment [4]. Currently, the prognosis for NPC patients is mainly based on TNM staging system. However, patients with the same TNM stage and similar treatment regimens often present with variable clinical outcomes, suggesting that the present staging system is not adequate for prognosis. Therefore, it is critical to define reliable prognostic factors to complement the TNM staging system to identify high-risk patients for combined and aggressive treatment.
It is reported that lipid metabolism plays an important role in the pathogenesis and progression of cancer [5–8]. Increased serum cholesterol level is associated with an increased risk for certain cancers, such as breast cancer, prostate cancer, and colon cancer [9–12]. There is a report that serum levels of triglyceridesare correlated with cancer morbidity [13]. Serum high-density lipoprotein cholesterol (HDL-C) level may be a clinical prognostic factor in gastric and lung cancers [8, 14]. Recent studies have suggested that ApoA-I, the major protein constituent of HDL-C, is a prognostic biomarker for ovarian, breast and pancreatic cancers [15–18]. Recent retrospective studies have revealed that elevated ApoA-I level is significantly associated with favorable prognosis in patients with metastatic NPC and non-small-cell lung cancer [19, 20]. However, little is known about the prognostic significance of ApoA-I in patients with non-metastatic NPC.
The aim of this study is to determine the prognostic value of serum ApoA-I in newly diagnosed non-metastatic NPC patients.
RESULTS
Patient characteristics
The clinical characteristics of the 1196 patients are shown in Table 1. These patients are men dominated. The median age was 46 years (range 11–80 years). The distribution of disease stage was: stage I, 3.4% (41 patients); stage II, 16.1% (193 patients); stage III, 50.8% (608 patients) and stage IV, 29.6% (354) patients. The mean ApoA-I level was 1.286 g/L (range 0.29–3.1 g/L). The cut-off points of baseline serum lipid and lipoprotein levels were determined by ROC curve analyses (Supplementary Figure S1). An ApoA-I value of 1.025 g/L resulted in the most appropriate sensitivity and specificity for DSS. Using 1.025 g/L as the cutoff point, we identified 183 patients (15.3%) as having decreased ApoA-I. Similarly, a triglyceride value of 1.865 mmol/L, cholesterol value of 5.045 mmol/L, HDL-C value of 1.065 mmol/L, LDL-C value of 5.715 mmol/L, and Apo-B value of 1.880 g/L were selected as the optimal cut-off points for survival analysis. Baseline clinical features of patients with elevated ApoA-I at diagnosis were compared with those of patients with decreased ApoA-I at diagnosis. No significant between-group difference was observed for age, N stage, EA/IgA, and different levels of triglyceride, LDL-C, and Apo-B. Patients with ApoA-I < 1.025 g/L at diagnosis tended to be men, presentingat later clinical stages and T stages, and receiving CRT. Patients with lower ApoA-I at diagnosis usually presented with a higher titer of VCA/IgA, and lower levels of total cholesterol and HDL-C.
Table 1: Clinical characteristics of patients according to ApoA-I levels at diagnosis
Characteristics |
ApoA-I ≥ 1.025 g/L |
ApoA-I < 1.025 g/L |
P value |
|---|---|---|---|
n (%) |
n (%) |
||
Age, years |
0.309 |
||
≤45 |
490 (48.4) |
96 (52.5) |
|
>45 |
523 (51.6) |
87 (47.5) |
|
Sex |
0.007 |
||
Female |
260 (25.7) |
30 (16.4) |
|
Male |
753 (74.3) |
153 (83.6) |
|
Clinical stage |
0.029 |
||
I/II |
209 (20.6) |
25 (13.7) |
|
III/IV |
804 (79.4) |
158 (86.3) |
|
T stage |
0.009 |
||
T1/T2 |
343 (33.9) |
44 (24.0) |
|
T3/T4 |
670 (66.1) |
139 (76.0) |
|
N stage |
0.888 |
||
N0/N1 |
609 (60.1) |
109 (59.6) |
|
N2/N3 |
404 (39.9) |
74 (40.4) |
|
VCA-IgAa |
0.006 |
||
<1:80 |
109 (11.2) |
8 (4.5) |
|
≥1:80 |
864 (88.8) |
170 (95.5) |
|
EA-IgAb |
0.498 |
||
<1:10 |
134 (14.8) |
22 (12.8) |
|
≥1:10 |
773 (85.2) |
150 (87.2) |
|
Triglyceride (mmol/L) |
0.228 |
||
<1.865 |
840 (82.9) |
145 (79.2) |
|
≥1.865 |
173 (17.1) |
38 (20.8) |
|
Cholesterol (mmol/L) |
< 0.001 |
||
<5.045 |
512 (50.5) |
122 (66.7) |
|
≥5.045 |
501 (49.5) |
61 (33.3) |
|
HDL-C (mmol/L) |
< 0.001 |
||
<1.065 |
202 (19.9) |
138 (75.4) |
|
≥1.065 |
811 (80.1) |
45 (24.6) |
|
LDL-C (mmol/L) |
0.394 |
||
<5.715 |
1000 (98.7) |
182 (99.5) |
|
≥5.715 |
13 (1.3) |
1 (0.5) |
|
Apo-B (g/L) |
0.415 |
||
<1.880 |
1004 (99.1) |
183 (100) |
|
≥ 1.880 |
9 (0.9) |
0 (0) |
|
Treatment |
0.030 |
||
CRT |
706 (69.7) |
142 (77.6) |
|
RT |
307 (30.3) |
41 (22.4) |
|
Diagnosis of diabetes |
0.344 |
||
Yes |
75 |
10 |
|
No |
936 |
173 |
|
Diagnosis of hypertension |
0.781 |
||
Yes |
219 |
38 |
|
No |
791 |
345 |
Abbreviations: ApoA-I, apolipoprotein A-I; VCA-IgA, immunoglobulin A/virus capsid antigen; EA-IgA, immunoglobulin A/early antigen; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; Apo-B, apolipoprotein B; CRT, chemoradiotherapy; RT, radiotherapy.
aComplete information on VCA-IgA was available in 1151 cases;
bComplete information on EA-IgA was available in 1079 cases.
Univariate analysis of ApoA-I as a prognostic factor for DSS, DMFS, and LRFS
The results of univariate analysis are presented in Table 2. Using 1.025 g/L as a cut-off value, serum ApoA-I level was strongly associated with DSS, DMFS, and LRFS. The 5-year estimate for DSS was 81.3% for patients with ApoA-I ≥ 1.025 g/L and 69.3% for those with ApoA-I < 1.025 g/L (P < 0.001; Figure 1A). Patients with ApoA-I < 1.025 g/L at diagnosis also had worse 5-year DMFS (83.4% vs. 67.4%, P < 0.001; Figure 1B) and worse 5-year LRFS (80.9% vs. 67.3%, P < 0.001; Figure 1C) than patients with elevated ApoA-I level at diagnosis. In addition to ApoA-I level, sex, age, clinical stage, T stage, N stage, TC, and HDL-C were significantly associated with DSS, DMFS, and LRFS.
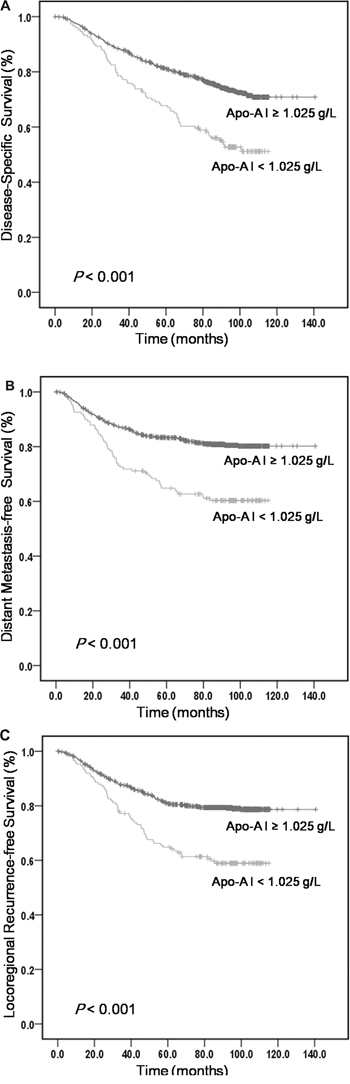
Figure 1: Kaplan-Meier curves obtained from univariate analyses (log-rank) of 1196 patients with NPC based on serum ApoA-I levels. A. DSS curves based on ApoA-I levels. B. DMFS curves based on ApoA-I levels. C. LRFS curves based on ApoA-I levels.
Table 2: Univariate analysis of prognostic factors for patients with nasopharyngeal carcinoma
Factor |
5-year disease-specific survival (%) |
5-year distant metastasis-free survival (%) |
5-year locoregional recurrence-free survival (%) |
|---|---|---|---|
Gender |
|||
Male |
76.8 |
78.9 |
76.0 |
Female |
86.9 |
87.2 |
87.0 |
P value |
0.003 |
0.004 |
0.001 |
Age (years) |
|||
≤45 |
84.3 |
84.5 |
82.8 |
>45 |
74.6 |
77.5 |
74.7 |
P vallue |
<0.001 |
<0.001 |
<0.001 |
Clinical stage |
|||
I/II |
94.8 |
94.4 |
92.6 |
III/IV |
75.7 |
77.6 |
75.3 |
P value |
<0.001 |
<0.001 |
<0.001 |
T status |
|||
T1/T2 |
90.1 |
90.6 |
87.7 |
T3/T4 |
74.3 |
76.2 |
74.4 |
P value |
<0.001 |
<0.001 |
<0.001 |
N status |
|||
N0/N1 |
83.1 |
84.8 |
82.3 |
N2/N3 |
73.9 |
75.2 |
73.4 |
P value |
<0.001 |
<0.001 |
0.001 |
VCA-IgA |
|||
<1:80 |
86.3 |
85.5 |
87.8 |
≥1:80 |
78.7 |
80.8 |
78.2 |
P value |
0.024 |
0.179 |
0.011 |
EA-IgA |
|||
<1:10 |
83.2 |
80.1 |
82.9 |
≥1:10 |
77.9 |
80.4 |
77.6 |
P value |
0.097 |
0.934 |
0.102 |
Triglyceride (mmol/L) |
|||
<1.865 |
78.7 |
79.7 |
78.0 |
≥1.865 |
82.9 |
87.0 |
82.4 |
P value |
0.201 |
0.130 |
0.285 |
Cholesterol (mmol/L) |
|||
<5.045 |
78.1 |
78.5 |
76.4 |
≥5.045 |
80.9 |
83.7 |
81.4 |
P value |
0.043 |
0044 |
0.019 |
HDL-C (mmol/L) |
|||
<1.065 |
74.2 |
75.6 |
74.2 |
≥1.065 |
81.5 |
83.1 |
80.6 |
P value |
<0.001 |
0.005 |
0.003 |
LDL-C (mmol/L) |
|||
<5.715 |
79.3 |
80.8 |
78.7 |
≥5.715 |
91.7 |
92.3 |
84.6 |
P value |
0.107 |
0.220 |
0.418 |
ApoA-I (g/L) |
|||
≥1.025 |
81.3 |
83.4 |
80.9 |
<1.025 |
69.3 |
67.4 |
67.3 |
P value |
<0.001 |
<0.001 |
<0.001 |
Apo-B (g/L) |
|||
<1.880 |
79.3 |
88.9 |
78.8 |
≥1.880 |
88.9 |
80.9 |
77.8 |
P value |
0.313 |
0.489 |
0.937 |
Treatment |
|||
CRT |
77.2 |
79.0 |
77.1 |
RT |
84.6 |
85.4 |
82.8 |
P value |
0.052 |
0.023 |
0.031 |
Abbreviations: VCA-IgA, immunoglobulin A/virus capsid antigen; EA-IgA, immunoglobulin A/early antigen; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; ApoA-I, apolipoprotein A-I; Apo-B, apolipoprotein B; CRT, chemoradiotherapy; RT, radiotherapy.
Multivariate analysis of ApoA-I as an independent prognostic factor for DSS, DMFS, and LRFS
As shown in Table 3, age, sex, clinical stage, T stage, N stage, ApoA-I, TC, HDL-C and treatment were included in the multivariate analysis. Decreased serum ApoA-I level was a significantly independent predictor for the worse prognostic measures, including DSS [hazard ratio (HR) = 1.629, 95% confidence interval (CI) = 1.227–2.163; P = 0.001], DMFS (HR = 1.888, 95% CI = 1.370–2.603; P < 0.001), and LRFS (HR = 1.750, 95% CI = 1.278–2.396; P < 0.001). The advanced T and N stages were also independent indicators for inferior DSS, DMFS, and LRFS. In addition, younger age was an independent factor for superior DSS, DMFS, and LRFS.
Table 3: Multivariate Cox proportional hazards analysis prognostic factors in non-metastatic NPC patients
Variable |
Death |
Recurrence |
Metastasis |
|||
|---|---|---|---|---|---|---|
HR (95% CI) |
P value |
HR (95% CI) |
P value |
HR (95% CI) |
P value |
|
Age, >45 vs. ≤45 years |
1.939 (1.548–2.429) |
<0.001 |
1.660 (1.295–2.128) |
< 0.001 |
1.680 (1.300–2.171) |
<0.001 |
Sex, male vs. female |
1.269 (0.962–1.674) |
0.0910 |
1.499 (1.085–2.072) |
0.014 |
1.372 (0.987–1.909) |
0.060 |
Clinical stage, IV/III vs. II/I |
2.131 (1.207–3.759) |
0.009 |
1.789 (0.979–3.268) |
0.059 |
1.746 (0.884–3.447) |
0.108 |
T stage, T4/T3 vs. T2/T1 |
2.041 (1.419–2.936) |
<0.001 |
1.715 (1.154–2.549) |
0.008 |
2.330 (1.507–3.603) |
<0.001 |
N stage, N3/N2 vs. N1/N0 |
1.472 (1.164–1.862) |
0.001 |
1.415 (1.084–1.848) |
0.011 |
1.652 (1.263–2.163) |
<0.001 |
ApoA-I (g/L), < 1.025 vs. ≥1.025 |
1.629 (1.227–2.163) |
0.001 |
1.750 (1.278–2.396) |
<0.001 |
1.888 (1.370–2.603) |
<0.001 |
Cholesterol (mmol/L), <5.045 vs. ≥5.045 |
1.198 (0.960–1.495) |
0.109 |
1.257 (0.979–1.613) |
0.073 |
1.196 (0.925–1.545) |
0.172 |
HDL-C (mmol/L), <1.065 vs. ≥1.065 |
0.899 (0.696–1.160) |
0.411 |
0.984 (0.739–1.311) |
0.914 |
1.010 (0.749–1.362) |
0.947 |
Treatment, CRT vs. RT |
1.421 (1.091–1.851) |
0.009 |
1.241 (0.911–1.689) |
0.171 |
1.337 (0.975–1.834) |
0.071 |
Abbreviations: ApoA-I, apolipoprotein A-I; HDL-C, high-density lipoprotein cholesterol.
We further classified patients within each stage level into two risk stratification groups based on ApoA-I level (Table 4). After stratification by clinical stages, ApoA-I remained a clinically and statistically significant predictor of prognosis (Figure 2).
Table 4: Five-year DSS analysis comparison of different levels of ApoA-I within each clinical stage
Clinical stage and ApoA-I level |
No. of patients |
5-year DSS (%) |
P value |
|---|---|---|---|
I/II |
|||
ApoA-I ≥ 1.025 g/L |
208 |
96.1 |
0.023 |
ApoA-I < 1.025 g/L |
25 |
84.0 |
|
III/IV |
|||
ApoA-I ≥ 1.025 g/L |
803 |
77.4 |
<0.001 |
ApoA-I < 1.025 g/L |
160 |
67.0 |
Abbreviations: DSS, disease-specific survival; ApoA-I, apolipoprotein A-I.
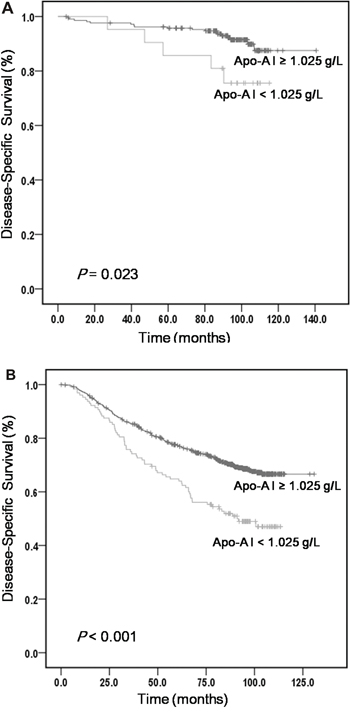
Figure 2: The five-year DSS analysis comparing serum levels of ApoA-I within different clinical stages. A. DSS curves based on ApoA-I levels in stage I/II. B. DSS curves based on ApoA-I levels in stage III/IV.
DISCUSSION
This is believed to be the first large cohort study to evaluate the prognostic significance of serum biomakers of lipid metabolism including triglyceride, cholesterol, HDL-C, LDL-C, ApoA-I, and Apo-B in non-metastatic NPC patients. The results suggested that elevated serum ApoA-I was significantly associated with superior prognosis. Serum ApoA-I level segregated patients with NPC at each level of clinical stages into two significantly distinguished risk groups. Thus, the level of serum ApoA-I could complement clinical staging for risk definition and could be useful in selecting optimal treatment for patients with NPC at different stage.
ApoA-I, which belongs to the apolipoprotein A1/A4/E family, is the main polypeptide of human plasma HDL and plays a key role in cholesterol homeostasis [21]. Synthesized in the liver and small intestine, ApoA-I reverses transport of cholesterol from tissue to the liver for excretion, transfers fatty acids and ethanolamine back to cells for reuse, and acts as a cofactor for lecithin cholesterol acyltransferase to convert cholesterol to cholesterylester [22].
Accumulating studies have suggested a strong link between ApoA-I and different types of cancer. Similarly, our study showed that elevated ApoA-I level was significantly associated with better prognosis, independent of other variables in patients with non-metastatic NPC.
The biological mechanism underlying the relationship between ApoA-I level and cancer development remains to be clarified. NPC has long been associated with EBV [23]. A previous study has suggested that EBV-encoded LMP1 mediates interleukin-6 production in epithelial cells [24]. It is reported that interleukin-6 can stimulate hepatic production and secretion of secretory nonpancreatic phospholipase A2 (sPLA2), an acute-phase protein that is increased during infection and inflammation [25]. Overexpression of sPLA2 in transgenic mice has been reported to decrease the level of ApoA-I [26, 27]. Thus, the decrease in the ApoA-I level might be due to the subsequent stimulation of acute-phase proteins by EBV infection [19]. Moreover, the systemic inflammatory responseis suggested to promote tumor metastasis and progression. A recent study has revealed a potent immunomodulatory role for ApoA-I in the tumor microenvironment, altering tumor-associated macrophages from a pro-tumor to an anti-tumor phenotype [28]. Therefore, elevated levels of ApoA-I may indicate cancer-related inflammation and predict better prognosis. Additionally, ApoA-I has been identified as a prostacyclin (PGI2)-stabilizing factor and thus may have an anticlotting effect [28]. PGI2 is reported to act as a powerful anti-metastatic agent against melanoma cells, which may result from the inhibitory effect of PGI2 on platelet aggregation. In addition, inhibitors of PGI2 synthesis may increase metastasis [29]. This suggests that the anti-tumor effects of elevated ApoA-I levels might be mediated by stabilizing PGI2. Further investigation is required to provide a better understanding of these mechanisms.
Prognostic assessment is crucial for formation of appropriate treatment choices. Various prognostic factors for NPC have been identified and evaluated retrospectively. Most of these factors were identified by immunohistochemical staining of tumor tissue, such as survivin and livin [30]. However, few of these markers are currently used in routine clinical practice. Currently, the TNM staging system is the key prognostic determinant for patients with NPC. However, large variations in the clinical outcomes of patients with the same cancer stage have been reported [31]. In our study, elevated serum ApoA-I level was predictive of superior survival in patients with NPC independent of TNM stage. Therefore, serum ApoA-I could potentially allow clinicians to identify candidates for aggressive therapy and improve treatment outcomes. Patients classified with the same TNM stage might be stratified into different disease recurrence-risk groups based on serum ApoA-I level, and thus treated with systemic approaches of different intensities. For example, in patients with early-stage disease (stages I/II) and low ApoA-I levels, CRT might be more beneficial than RT alone. However, for patients with advanced-stage disease (stages III/IV) and low ApoA-I levels, the current chemotherapy regimen might be insufficient, and a more intensive chemotherapy regimen or targeted therapy may be needed.
Our study had two main strengths: (i) all patients were newly diagnosed, which ruled out any impact on patient outcome of any possible disproportionate pretreatment; and (ii) relatively long follow-up period. However, our study also had two main limitations: (i) because of its retrospective nature, the selection bias could not be completely eliminated; and (ii) this was a retrospective study restricted to one local hospital. Therefore, a prospective study with a large number of cases is needed to confirm a correlation between ApoA-I and NPC prognosis.
In conclusion, this study suggested that the serum level of ApoA-I at diagnosis is a prognostic indicator of clinical outcome in non-metastatic NPC and may complement clinical staging for risk definition. Future prospective clinical studies are required to confirm our findings.
MATERIALS AND METHODS
Patients and data collection
We retrospectively reviewed the medical records of 1196 patients with newly diagnosed non-metastatic NPC between January 2004 and March 2007 at the Sun Yat-sen University Cancer Center, China. The criteria for case inclusion were as follows: (i) pathologically diagnosed non-metastatic NPC; (ii) Karnofsky Performance Status score ≥70; (iii) no previous treatment; and (iv) adequate clinical information and follow-up data. Patients were excluded if: (i) they were taking hormone replacement therapy or any drugs known to affect lipid metabolism; or (2) if they had previous malignancy or a second primary tumor. Each patient underwent a pre-therapeutic testing, including physical and neurological examinations, hematological and biochemistry profiles, endoscopic examination of the nasopharynx, computed tomography or magnetic resonance imaging of the head and neck, chest radiography, abdominal ultrasonography, emission computed tomography, or positron emission tomography. Clinical staging was reclassified according to the criteria of the 2002 Union International Control Cancer staging system. All pathological specimens were reviewed and reclassified by central review according to the World Health Organization criteria for pathologic diagnosis. This study was approved by the Institutional Review Board of Sun Yat-sen University Cancer Center. Informed consent for the collection of medical information was provided at the first visit of all patients.
The clinical data were collected at diagnosis, including patient demographics, Karnofsky Performance Status, the serum level of lipids and lipoproteins, and the serum antibody titers of Epstein-Barr virus (EBV) immunoglobulin A/virus capsid antigen (VCA/IgA) andimmunoglobulin A/early antigen (EA/IgA). Serum levels of triglyceride, cholesterol, HDL-C, low-density lipoprotein cholesterol (LDL-C), ApoA-I, and apolipoprotein B (Apo-B) were examined in early morning samples obtained before therapy and immediately measured using a Hitachi 7600–020 automatic biochemical analyzer (Hitachi High-Technologies, Tokyo, Japan).
Treatment and follow-up
Patients were treated with different regimens based on their clinical characteristics in line with the clinical practice guidelines for NPC in the Sun Yat-sen University Cancer Center and National Comprehensive Cancer Network guidelines. According to the clinical practice guidelines during the study period, RT alone was used for patients in stages I–IIA, radiation with concurrent platinum-based chemotherapy was used for those in stage IIB, and concurrent CRT, with or without neoadjuvant or adjuvant chemotherapy, was used for those in stages III–IV. For RT, megavoltage photons (6 MV) were used to treat the primary tumor and neck lymph nodes. RT was given five times a week at 2 Gy/day. The median radiation dose was 70 Gy (range, 60–80 Gy) to the nasopharyngeal region and 60 Gy (range, 40–72 Gy) to the initially involved cervical node. In 41 patients with stage I disease, 38 (92.7%) were treated with radiotherapy alone, 3 (7.3%) were treated with cisplatin and 5-FU based neoadjuvant (2 patients) and concurrent chemotherapy (1 patient). In193 patients with stage II disease, 130 (67.4%) were treated with radiotherapy alone and 63 (32.6%) were treated with cisplatin and/or 5-FU based neoadjuvant (13 patients) and/or concurrent chemotherapy (50 patients). In 608 patients with stage III disease, 136 (22.4%) were treated with radiotherapy alone and 472 (77.6%) were treated with cisplatin and/or 5-FU based neoadjuvant (261 patients) and/or concurrent chemotherapy (291 patients). In 354 patients with stage IV disease, 30 (8.5%) were treated with radiotherapy alone, 324 (91.5%) were treated with cisplatin and/or 5-FU based neoadjuvant (206 patients) and/or concurrent chemotherapy (200 patients). Neoadjuvant chemotherapy consisted of cisplatin with 5-fluorouracil every 3 weeks for two or three cycles. Concurrent chemotherapy that consisted of cisplatin was administered on days 1, 22, and 43 of RT.
After treatment was completed, patients were followed up every 3 months in the first 3 years and every 6 months thereafter. The last follow-up date was December 31, 2014 for all the available patients.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). The major endpoints used for assessment in the current analysis were DSS, DMFS, and LRFS. We calculated DSS from diagnosis to the date of death from disease-related causes or the date of the last follow-up visit; DMFS to the first distant relapse or the date of the last follow-up visit; and LRFS to the first locoregional relapse or the date of the last follow-up visit.
Receiver operating characteristic (ROC) curves were used to select the most appropriate cutoff points of serum lipids and lipoproteins to stratify patients at a high risk of malignancy-related death. The score closest to the point with both maximum sensitivity and specificity was selected as the cutoff value. The χ2 test was used to compare baseline clinical characteristics between different serum levels of ApoA-I. The DSS, DMFS, and LRFS rates were calculated by the Kaplan-Meier method, and survival was compared using the log-rank test. Significant variables in the univariate analysis were considered as variables for the multivariate analysis of survival. The later was performed by the Cox proportional hazards model. P < 0.05 was considered statistically significant. All P values corresponded to two-sided significance tests.
CONFLICTS OF INTEREST
The authors have declared no conflicts of interest.
GRANT SUPPORT
The work was supported by National Natural Science Foundation of China (NO.81372883, NO.81001052), Science and Technology Planning Project of Guangdong Province, China (2011B031800222), Young Talents Project of Sun Yat-sen University Cancer Center (to CaiQingqing), Young Talents Project of Sun Yat-sen University (11ykpy56, to Cai Qingqing), and the Natural Science Foundation of Guangdong Province, China (8151008901000043). Sister Institution Network Fund of MD Anderson Cancer Center (to RaoHuilan).
REFERENCES
1. Lee AW, Lin JC, Ng WT. Current management of nasopharyngeal cancer. Semin Radiat Oncol. 2012; 22:233–244.
2. Yoshizaki T, Ito M, Murono S, Wakisaka N, Kondo S, Endo K. Current understanding and management of nasopharyngeal carcinoma. Auris Nasus Larynx. 2012; 39:137–144.
3. Muir CS. Cancer Incidence in Five Continents. Classification. IARC Sci Publ. 1992; 25–30.
4. Lee AW, Lau WH, Tung SY, Chua DT, Chappell R, Xu L, Siu L, Sze WM, Leung TW, Sham JS, Ngan RK, Law SC, Yau TK, Au JS, O’Sullivan B, Pang ES, et al. Preliminary results of a randomized study on therapeutic gain by concurrent chemotherapy for regionally-advanced nasopharyngeal carcinoma: NPC-9901 Trial by the Hong Kong Nasopharyngeal Cancer Study Group. J Clin Oncol. 2005; 23:6966–6975.
5. Van Hemelrijck M, Walldius G, Jungner I, Hammar N, Garmo H, Binda E, Hayday A, Lambe M, Holmberg L. Low levels of apolipoprotein A-I and HDL are associated with risk of prostate cancer in the Swedish AMORIS study. Cancer Causes Control. 2011; 22:1011–1019.
6. Wang L, Chi PD, Chen H, Xiang J, Xia ZJ, Zhang YJ. Low level of high-density lipoprotein cholesterol correlates with poor prognosis in extranodal natural killer/T cell lymphoma. Tumour Biol. 2014; 35:2141–2149.
7. Hsieh Wu J. Lipoprotein(a) in vascular disease, cancer and longevity. Chang Gung Med J. 2011; 34:555–564.
8. Chi PD, Liu W, Chen H, Zhang JP, Lin Y, Zheng X, Dai S. High-density lipoprotein cholesterol is a favorable prognostic factor and negatively correlated with C-reactive protein level in non-small cell lung carcinoma. PLoS One. 2014; 9:e91080.
9. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003; 348:1625–1638.
10. Gaziano JM, Hennekens CH. Dietary fat and risk of prostate cancer. J Natl Cancer Inst. 1995; 87:1427–1428.
11. Michalaki V, Koutroulis G, Syrigos K, Piperi C, Kalofoutis A. Evaluation of serum lipids and high-density lipoprotein subfractions (HDL2, HDL3) in postmenopausal patients with breast cancer. Mol Cell Biochem. 2005; 268:19–24.
12. van Duijnhoven FJ, Bueno-De-Mesquita HB, Calligaro M, Jenab M, Pischon T, Jansen EH, Frohlich J, Ayyobi A, Overvad K, Toft-Petersen AP, Tjonneland A, Hansen L, Boutron-Ruault MC, Clavel-Chapelon F, Cottet V, Palli D, et al. Blood lipid and lipoprotein concentrations and colorectal cancer risk in the European Prospective Investigation into Cancer and Nutrition. Gut. 2011; 60:1094–1102.
13. Siemianowicz K, Gminski J, Stajszczyk M, Wojakowski W, Goss M, Machalski M, Telega A, Brulinski K, Magiera-Molendowska H. Serum total cholesterol and triglycerides levels in patients with lung cancer. Int J Mol Med. 2000; 5:201–205.
14. Tamura T, Inagawa S, Hisakura K, Enomoto T, Ohkohchi N. Evaluation of serum high-density lipoprotein cholesterol levels as a prognostic factor in gastric cancer patients. J Gastroenterol Hepatol. 2012; 27:1635–1640.
15. Clarke CH, Yip C, Badgwell D, Fung ET, Coombes KR, Zhang Z, Lu KH, Bast RC Jr. Proteomic biomarkers apolipoprotein A1, truncated transthyretin and connective tissue activating protein III enhance the sensitivity of CA125 for detecting early stage epithelial ovarian cancer. Gynecol Oncol. 2011; 122:548–553.
16. Han C, Zhang HT, Du L, Liu X, Jing J, Zhao X, Yang X, Tian B. Serum levels of leptin, insulin, and lipids in relation to breast cancer in china. Endocrine. 2005; 26:19–24.
17. Chang SJ, Hou MF, Tsai SM, Wu SH, Hou LA, Ma H, Shann TY, Tsai LY. The association between lipid profiles and breast cancer among Taiwanese women. Clin Chem Lab Med. 2007; 45:1219–1223.
18. Ehmann M, Felix K, Hartmann D, Schnolzer M, Nees M, Vorderwulbecke S, Bogumil R, Buchler MW, Friess H. Identification of potential markers for the detection of pancreatic cancer through comparative serum protein expression profiling. Pancreas. 2007; 34:205–214.
19. Jiang R, Yang ZH, Luo DH, Guo L, Sun R, Chen QY, Huang PY, Qiu F, Zou X, Cao KJ, Mai HQ, Guo X, Qian CN, Hong MH, Chen MY. Elevated apolipoprotein A-I levels are associated with favorable prognosis in metastatic nasopharyngeal carcinoma. Med Oncol. 2014; 31:80.
20. Cheng T, Dai X, Zhou DL, Lv Y, Miao LY. Correlation of apolipoprotein A-I kinetics with survival and response to first-line platinum-based chemotherapy in advanced non-small cell lung cancer. Med Oncol. 2015; 32:407.
21. Brewer HB Jr., Fairwell T, LaRue A, Ronan R, Houser A, Bronzert TJ. The amino acid sequence of human APOA-I, an apolipoprotein isolated from high density lipoproteins. Biochem Biophys Res Commun. 1978; 80:623–630.
22. Yui Y, Aoyama T, Morishita H, Takahashi M, Takatsu Y, Kawai C. Serum prostacyclin stabilizing factor is identical to apolipoprotein A-I (Apo A-I). A novel function of Apo A-I. J Clin Invest. 1988; 82:803–807.
23. Wei WI, Sham JS. Nasopharyngeal carcinoma. Lancet. 2005; 365:2041–2054.
24. Eliopoulos AG, Stack M, Dawson CW, Kaye KM, Hodgkin L, Sihota S, Rowe M, Young LS. Epstein-Barr virus-encoded LMP1 and CD40 mediate IL-6 production in epithelial cells via an NF-kappaB pathway involving TNF receptor-associated factors. Oncogene. 1997; 14:2899–2916.
25. Crowl RM, Stoller TJ, Conroy RR, Stoner CR. Induction of phospholipase A2 gene expression in human hepatoma cells by mediators of the acute phase response. J Biol Chem. 1991; 266:2647–2651.
26. Tietge UJ, Maugeais C, Cain W, Grass D, Glick JM, de Beer FC, Rader DJ. Overexpression of secretory phospholipase A(2) causes rapid catabolism and altered tissue uptake of high density lipoprotein cholesteryl ester and apolipoprotein A-I. J Biol Chem. 2000; 275:10077–10084.
27. Tietge UJ, Maugeais C, Lund-Katz S, Grass D, deBeer FC, Rader DJ. Human secretory phospholipase A2 mediates decreased plasma levels of HDL cholesterol and apoA-I in response to inflammation in human apoA-I transgenic mice. Arterioscler Thromb Vasc Biol. 2002; 22:1213–1218.
28. Zamanian-Daryoush M, Lindner D, Tallant TC, Wang Z, Buffa J, Klipfell E, Parker Y, Hatala D, Parsons-Wingerter P, Rayman P, Yusufishaq MS, Fisher EA, Smith JD, Finke J, DiDonato JA, Hazen SL. The cardioprotective protein apolipoprotein A1 promotes potent anti-tumorigenic effects. J Biol Chem. 2013; 288:21237–21252.
29. Honn KV, Cicone B, Skoff A. Prostacyclin: a potent antimetastatic agent. Science. 1981; 212:1270–1272.
30. Xiang Y, Yao H, Wang S, Hong M, He J, Cao S, Min H, Song E, Guo X. Prognostic value of Survivin and Livin in nasopharyngeal carcinoma. Laryngoscope. 2006; 116:126–130.
31. Liu N, Chen NY, Cui RX, Li WF, Li Y, Wei RR, Zhang MY, Sun Y, Huang BJ, Chen M, He QM, Jiang N, Chen L, Cho WC, Yun JP, Zeng J, et al. Prognostic value of a microRNA signature in nasopharyngeal carcinoma: a microRNA expression analysis. Lancet Oncol. 2012; 13:633–641.