
Introduction
Breast surgery and the various oncological treatments for breast cancer (BC), treat the disease and save lives, but may nonetheless have adverse effects that may last years after diagnosis [1–3].
The physical rehabilitation after BC treatment requires a broad view of the set of problems that patients suffer from [4]. Prolonged pain defined as pain that lasts up to three months after surgery, which is felt in the breast, armpit or arm are the most common problems and occur in up to 50% of patients [5, 6]. Functional limitations occur in up to 50% of patients and affect their quality of life [2]. Pain and functional limitations are the main causes of women’s difficulty in returning to the jobs they held pre-diagnosis, and apply to up to 48% of patients [7]. Secondary lymphedema (chronic edema) due to lymph node dissection and radiation treatment may develop over months and gradually become a chronic condition with a prevalence of up to 17% [8]. Cognitive impairment and fatigue are common in up to 25% and 30% of patients, respectively [9]. The prevalence of sleep difficulties ranges between 20% and 70% [10]. Two additional symptoms are chemotherapy-induced peripheral neuropathy (30%), and cardiotoxicity 6–17% [11]. All the above symptoms affect survivors’ quality of life [12] and require long emotional and physical rehabilitation [13].
Identifying patients at risk of arm morbidity and providing rehabilitation programs can help survivors throughout their journey to recovery [14]. Therefore, the importance of understanding the risk factors and their effect on morbidity, including health behaviors, the type of oncological treatments including type of surgery, and even the patient’s emotional state, increases [15].
Several tools have been developed to assess the risk of morbidity, such as the RATE-L, which assesses the risk of lymphedema using known risk factors, including body weight, age, number of lymph nodes removed, axillary radiation therapy and chemotherapy. [16].
Other risk factors are known to affect the risk of developing a limitation in the range of motion (ROM), pain or causes a decrease in function [17, 18]. A thorough understanding of the impact of the various risk factors resulting from BC treatments and their effect on arm symptoms can empower doctors and therapists to optimize treatment protocols and identify patients who need symptom monitoring or preventive [19, 20].
We hypothesize that understanding the risk factors for arm morbidity after BC treatments, including personal characteristics, various aspects related to surgery and oncological treatments, could lead to the design of tools and programs, intend to identify patients at risk at an earlier stage and thereby provide better care [21, 22].
Therefore, the aim of this systematic review is to identify risk factors for the four most common physical symptoms by patients, namely, persistent pain, lymphedema, decreased ROM, and functional disability.
Results
After conducting electronic searches based on abstracts and titles, we identified 1242 articles. After removing duplicates, 1,153 articles were examined for full text. Sixty-nine of these articles met the criteria and were included in the review. Flow chart of the study is shown in Figure 1. The literature reviews included five systematic reviews, four RCTs and 65 studies with evidence quality levels of 1A to 2B. The classification of evidence is presented in Table 1 and the risk of bias assessments are described in Figure 2 and Figure 3 according to study type.
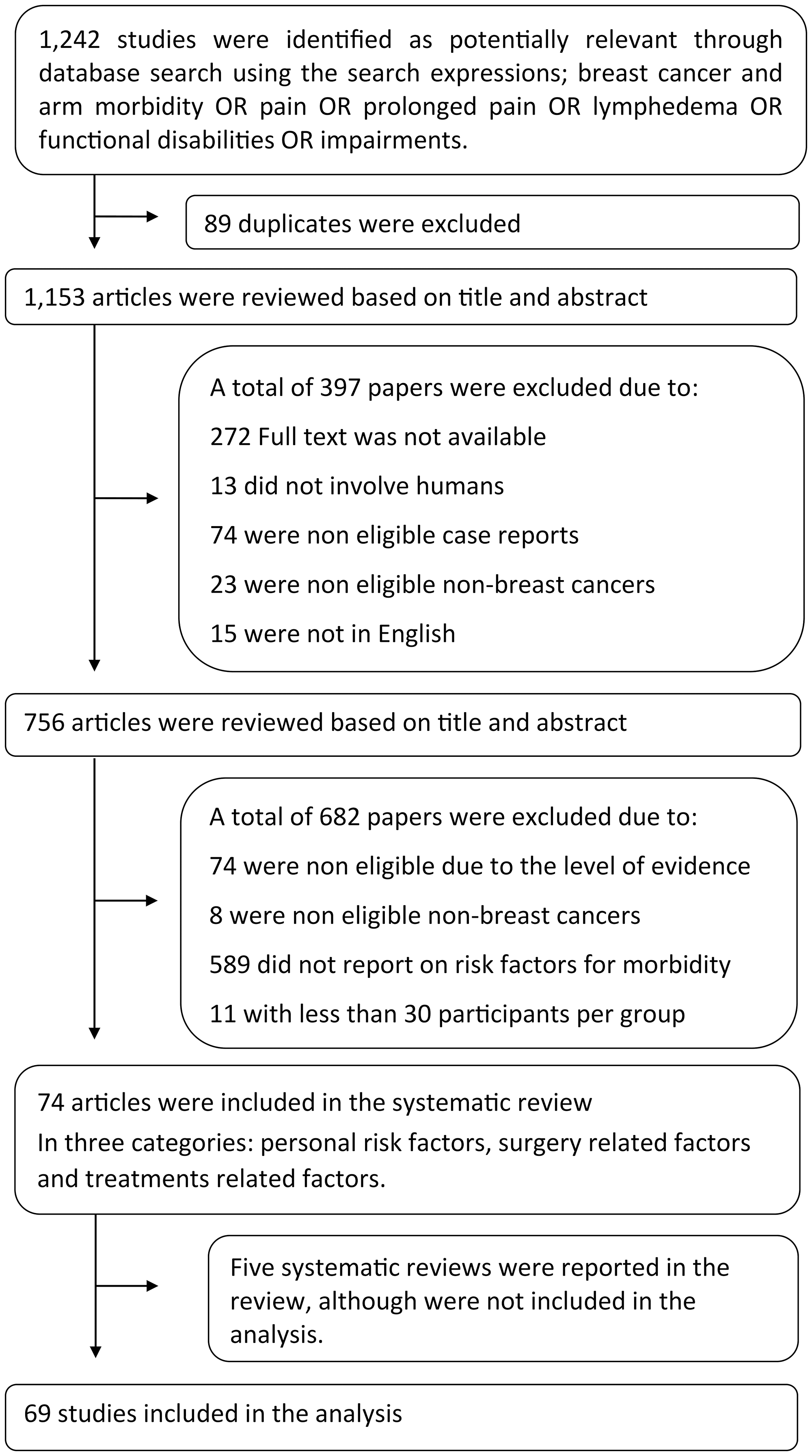
Figure 1: Flow chart of the study selection.
Search process and selection of articles according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) Guidelines [102].
Table 1: Classification of evidence system based on the Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence
| 1A | Systematic review (with homogeneity) of RCTs |
| 1B | Individual RCT (with narrow confidence intervals) |
| 2A | Systematic review (with homogeneity) of cohort studies |
| 1C | All or none study |
| 2B | Individual cohort study including low quality RCT |
| 2C | Outcomes research; ecological studies |
| 3A | Systematic review (with homogeneity) of case-control studies |
| 3B | Individual case-control study |
| 4 | Case series (and poor-quality cohort and case-control study) |
| 5 | Expert opinion without explicit critical appraisal or based on physiology bench research or “first principles” |
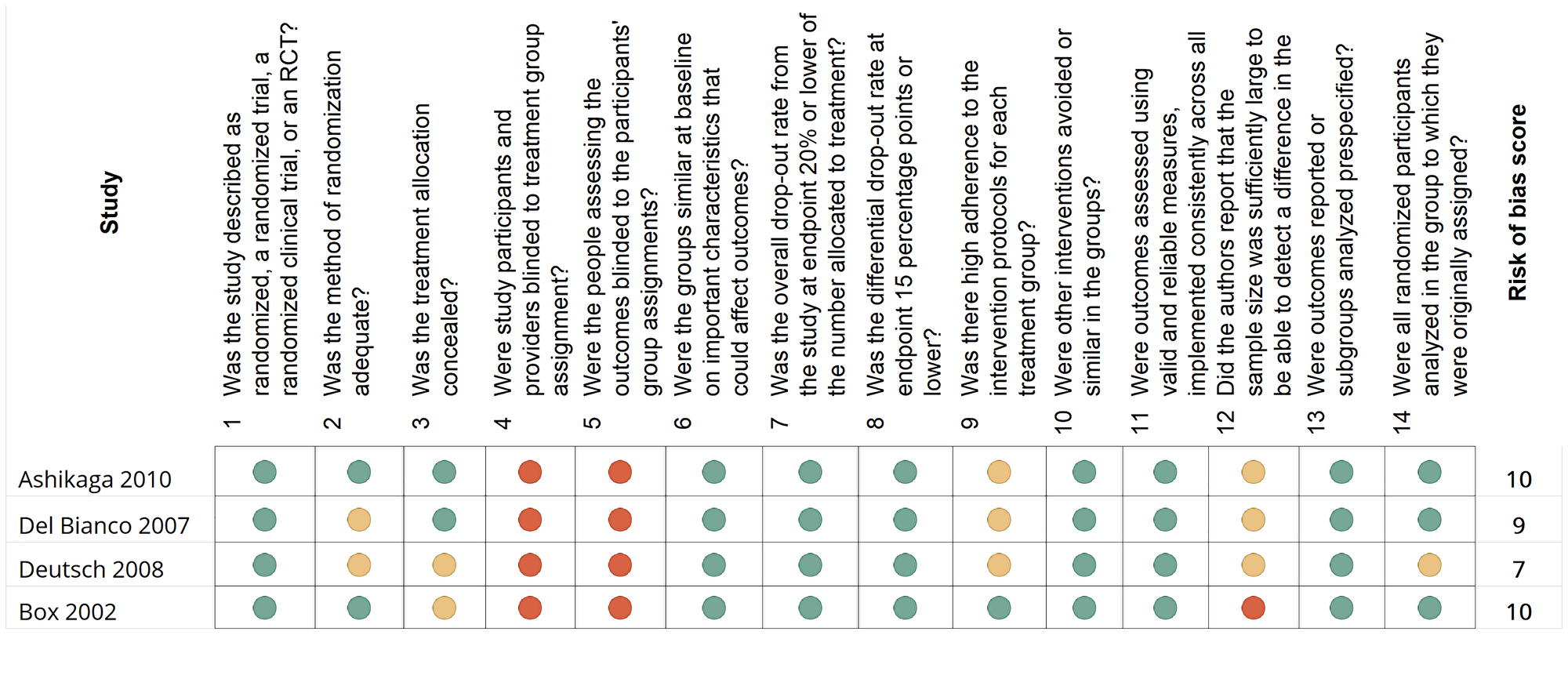
Figure 2: A summary and risk-of-bias assessment according to the National Institutes of Health quality assessment tool for randomized control studies (https://www.nih.gov/)
This figure describes the risk of bias in each of the 65 observational studies, cohort studies, and cross-sectional studies included in the review. The National Institute of Health (NIH) risk-assessment tool includes 14 questions evaluating bias risk. This diagram represents the answer options; green indicates a positive answer; red indicates a negative answer; yellow indicates questions that are cannot be determined or not.
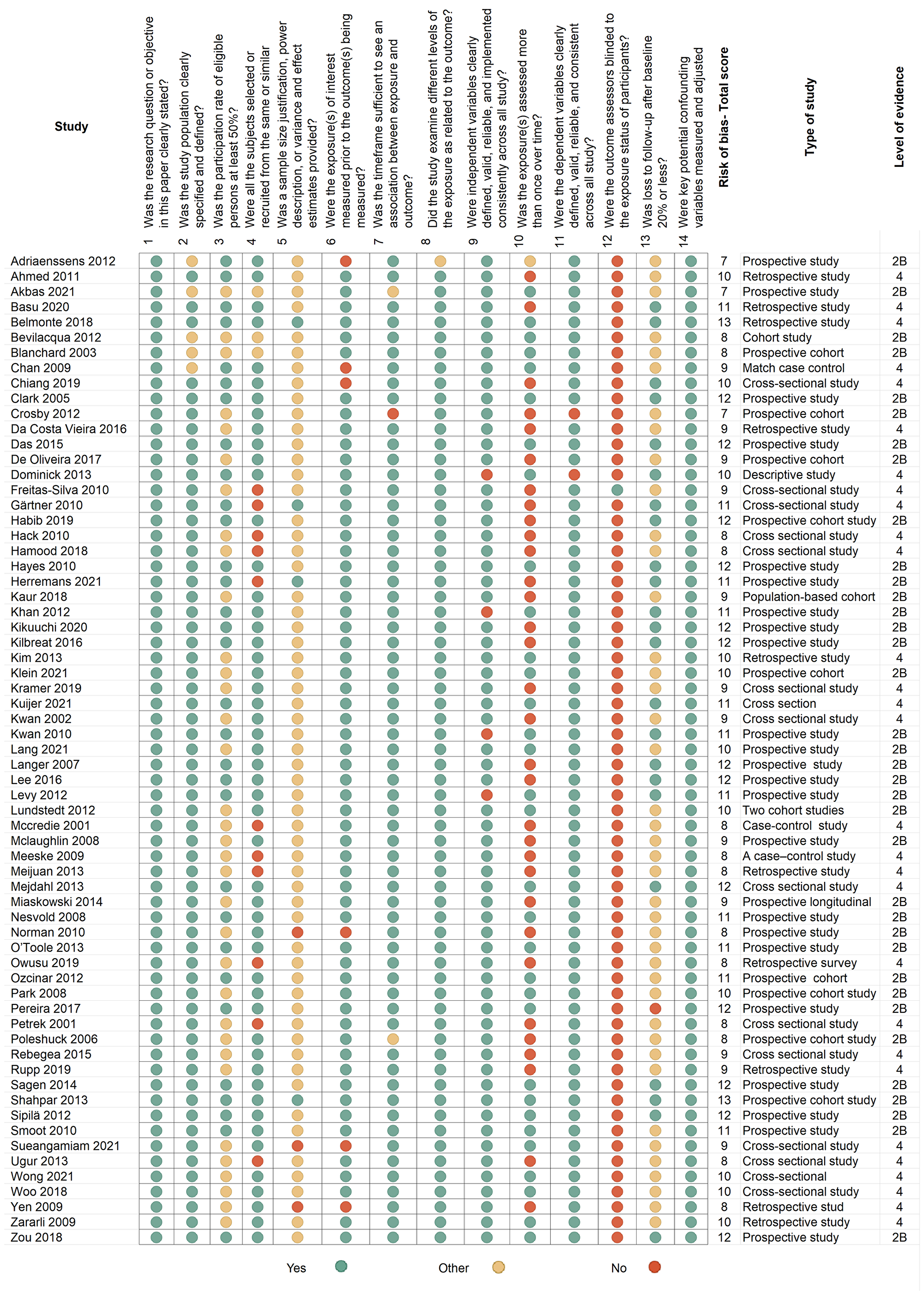
Figure 3: A summary and risk-of-bias using the quality assessment tool for observational cohort and cross-sectional studies (https://www.nih.gov/)
This figure describes the risk of bias in each of the 65 observational studies, cohort studies, and cross-sectional studies included in the review. The National Institute of Health (NIH) risk-assessment tool includes 14 questions evaluating bias risk. This diagram represents the answer options; green indicates a positive answer; red indicates a negative answer; yellow indicates questions that are cannot be determined or not applicable.
The study included articles published between 2001 and 2021, with a total of 22,886 patients and a follow-up period of between three months and ten years. The results were divided into the following three categories: (1) personal risk factors; (2) risk factors related to surgery; and (3) factors related to oncological treatments (See Tables 2–8 and Figures 4, 5).
Table 2: Young age as a risk factor for arm morbidity following breast cancer treatments
| Disability | Author | N | Follow-up | Measure | Comparison/Comments | P-value | OR/RR/HR | CI (95%) | Type of evidence | Evidence level |
|---|---|---|---|---|---|---|---|---|---|---|
| Persistent pain | Wang 2016 [25] | 11,030 | Median follow-up 12 months | VAS) | OR for every 10 years | OR = 1.36 | 1.24–1.48 | Systematic review and meta-analysis | 2A | |
| Miaskowski 2014 [23] | 398 | 6 months | ASQ and Postsurgical Pain Questionnaire | No pain Mild pain Moderate pain | <0.001 | Prospective longitudinal study | 2B | |||
| Poleshuck 2006 [26] | 95 | 3 months | NPRS | 0.004 | OR = 0.95 | 0.91–0.99 | Prospective study | 2B | ||
| Zararli 2009 [32] | 299 | AVS | Age <50 vs. >50 | 0.001 | RR = 2.493 | 1.532–4.058 | Prospective study | 2B | ||
| Lee 2016 [30] | 375 | Brief Pain Inventory and NPRS | Age <50 vs. >50 | 0.010 | OR = 2.44 | 1.24–4.79 | Prospective study | 2B | ||
| Lundstedt 2012 [31] | 1,027 | BC 3 to 20 years earlier | Based on Lundstedt questionnaire | Breast pain vs. no breast pain following radiation | RR = 0.96 | 0.94–0.98 | Two cohort studies data collection | 2B | ||
| Mejdahl 2013 [27] | 2,411 | 6 years | NPRS | With or without chronic pain | <0.001 | OR = 1.78 | 1.25–2.5 | Repeated cross-sectional study | 4 | |
| Kaur 2018 [28] | 215 | 3 months | VAS and Neuropathic Pain Symptom Inventory | <3/>3 Visual analog scale | 0.03 | Descriptive study | 4 | |||
| Meijuan 2013 [29] | 225 | - | McGill Pain Questionnaire and SF36 | <0.05 | Retrospective study | 4 | ||||
| Hamood 2018 [24] | 410 | 7.4 years | NPRS | With or without chronic pain | 0.002 | OR per one year = 0.96 | 0.94–0.99 | A cross-sectional study | 4 | |
| Functional disabilities | Zararli 2009 [32] | 299 | Physical examination | Age <50 vs. >50 | 0.048 | RR = 2.493 | 1.53–4.05 | Prospective study | 2B | |
| Khan 2012 [33] | 85 | Functional Independence Measure | <57 vs. >57 | 0.007 | Prospective study | 2B | ||||
| De Oliveira 2017 [34] | 101 | 12 months after surgery | The DASH questionnaire | <56 vs. 57< | 0.035 | 1.3–7.8 | Retrospective cross-sectional study | 4 | ||
| Lymphedema | Meeske 2009 [35] | 494 | 50 months after diagnosis | Self-report | Age 35–44, 45–54, 55–64 | OR per year of age = 0.96 | 0.93–0.99 | A case-control study | 4 | |
| Gärtner 2010 [36] | 3,253 | Self-report | Age 18–39, 40–49, 50–59, 60–69 | <0.001 | OR = 2.60 | 1.72–3.94 | cross-sectional study | 4 | ||
| Axillar web syndrome or cording | O’Toole 2013 [38] | 308 | 8 months | Perometer and the LEFT-BC questionnaire Cording by patient self-report | 0.005 | HR = 0.96 | 0.94–0.98 | Prospective study | 2B |
Table 3: Age over 50 as a risk factor for arm morbidity following breast cancer treatments
| Disability | Author | N | Follow-up | Measure | Comparison/Comments | P-value | OR/RR/HR | CI (95%) | Type of evidence | Evidence level |
|---|---|---|---|---|---|---|---|---|---|---|
| Functional disabilities | Hayes 2010 [39] | 287 | 18-months | QuickDASH | <50, 50> | <0.05 | OR = 1.94 | 1.01–3.75 | Prospective study | 2B |
| Lymphedema | Ashikaga 2010 [37] | 3,963 | 36-months | Arm volume | ALND vs. SLNB and age <49, 50< | 0.006 | OR = 1.41 | RCT | 1B | |
| Bevilacqua 2012 [42] | 1,051 | 5 years | Arm circumference measurement | Age <50/50> | 0.0485 | Prospective cohort study | 2B | |||
| Herremans 2021 [43] | 132 | 5 years | Circumference measurement and bioimpedance spectroscopy | LYMPHA technique and ALND | 0.037 | OR = 0.37 | 0.14–0.94 | Retrospective cross-sectional study | 4 | |
| Chan 2009 [41] | 202 after ALND | Arm circumference measurement | Level of lymphedema increases with age | 0.011 | OR = 1.05 | 1.01–1.10 | Matched cases control study | 3B | ||
| Persistent pain | Sipilä 2012 [44] | 489 | 6 months | NPRS | Age <39, 40–69, 70< | <0.01 | OR = 0.35 | 0.16–0.76 | Prospective study | 2B |
| Mejdahl 2013 [27] | 2,411 | Developed questionnaire | For age 60–69 | <0.001 | OR = 1.12 | 0.90–1.41 | Repeated cross-sectional study | 4 | ||
| Decreased range of motion | Woo 2018 [45] | 430 | Having restricted ROM ≥ 30° in comparison to the unaffected side | Different modalities of breast reconstructions | 0.041 | OR = 1.038 | 1.00–1.07 | Prospective study | 2B | |
| Levy 2012 [40] | 115 | 12 months | Harvard Alumni Health Study Physical Activity Questionnaire and The QuickDASH Questionnaire | Severity of limitation | 0.001 | Prospective study | 2B |
Table 4: Body mass index (BMI) as risk factor for arm morbidity following breast cancer treatments
| Disability | Author | N | Follow-up | Measure | Comparison/Comments | P-value | OR/RR/HR | CI (95%) | Type of evidence | Evidence level |
|---|---|---|---|---|---|---|---|---|---|---|
| Lymphedema | Deutsch 2008 [51] | 1,457 | Arm circumferences | 0.001 | RCT | 1B | ||||
| Box 2002 [57] | 65 | 24 months | Arm circumferences, arm volume and multi-frequency bioimpedance | 0.01 | OR = 1.21 | 1.04–1.41 | RCT | 1B | ||
| Nesvold 2008 [48] | 263 | 47 months | Volume calculation | <0.01 | OR = 1.11 | 1.04–1.19 | Prospective study | 2B | ||
| Kwan 2010 [49] | 997 | 20.9 months | Examination by a specialist | BMI 25 (healthy weight) 25–29 (overweight) >30 (obese) | HR = 1.43 | 0.88–2.31 | Prospective study | 2B | ||
| Zou 2018 [47] | 387 | 24 months | Circumference and Norman questionnaire | BMI <24/24< | 0.03 | HR = 1.1 | 1.0–1.1 | Prospective study | 2B | |
| Shahpar 2013 [50] | 410 | 3 years | Arm circumferences | Increase of 1 kg/m2 in Body mass index | <0.001 | OR = 1.09 | 1.05–1.15 | Prospective cohort study | 2B | |
| Das 2015 [55] | 199 | 2–15-year | Self-reported | BMI> = 25 treated with tamoxifen | 0.05 | OR = 2.62 | 0.99–6.93 | Prospective cohort | 2B | |
| Mclaughlin 2008 [52] | 936 | 5 years | Circumference | <0.001 | Prospective study | 2B | ||||
| Kilbreath 2016 [53] | 450 | 18-months | Bio-impedance spectroscopy | <5/>5 lymph nodes removed | 0.08 | OR = 1.9 | 0.9–3.9 | Prospective cohort | 2B | |
| Kuijer 2021 [17] | 1,037 | 1-year | Self-reported | BMI 25–30 | 0.03 | OR = 1.7 | Prospective cohort study | 2B | ||
| Bevilacqua 2012 [42] | 1,051 | 5 years | Arm circumference measurement | BMI <25/>25 | 0.001 | Prospective cohort | 2B | |||
| Chan 2009 [41] | 5 years | Arm circumference measurement | 0.007 | OR = 1.11 | 1.03–1.21 | Matched case-control study | 3B | |||
| Meeske 2009 [35] | 494 | 50 months after diagnosis | Self-report of lymphedema | OR for, BMI>30 = 2.48 | 1.05–5.84 | A case-control study | 4 | |||
| Petrek 2001 [54] | 923 | 20 years | Circumferential arm measurements | 0.08 | Cross-sectional | 4 | ||||
| Mccredie 2001 [56] | 809 | Self-reported | For BMI>30 | 0.02 | OR = 1.7 | 1.1–2.6 | Population-based study | 4 | ||
| Smoot 2010 [104] | 144 | The DASH questionnaires and circumference measurement | 0.041 | −3.68–−0.08 | Cross-sectional study | 4 | ||||
| Lymphedema BMI>25 | Nesvold 2008 [48] | 263 | 47 months | British Columbia Cancer Agency in Canada | <0.01 | OR = 1.12 | 1.04–1.19 | Prospective study | 2B | |
| Dominick 2013 [61] | 2,431 | 6 years | Norman and colleagues’ validated telephone lymphedema questionnaire | For BMI>30 | <0.01 | OR = 2.08 | 1.66–2.60 | Prospective cohort study | 2B | |
| Ugur 2013 [62] | 455 | 53 months | Tape measure | BMI <25/>25 | <0.001 | OR = 3.94 | 1.97–7.87 | Prospective study | 2B | |
| Park 2008 [63] | 450 | 24 months | Tape measure | BMI <25/>25 | 0.023 | OR = 2.01 | 1.10–3.68 | Prospective study | 2B | |
| Clark 2005 [64] | 251 | 3 years | Tape measure | BMI <25/>25 | RR = 2.02 | 1.11–3.68 | Prospective observational study | 2B | ||
| Crosby 2012 [58] | 1,117 | From medical record | Immediate breast reconstruction and BMI <25/>25 | 0.008 | OR = 2.78 | 1.30–5.94 | Retrospective study | 4 | ||
| Functional disabilities | Nesvold 2008 [48] | 263 | 47 months | British Columbia Cancer Agency in Canada | 0.001 | OR = 1.12 | 1.05–1.2 | Prospective study | 2B | |
| Hack 2010 [59] | 316 | 12 months | The DASH Questionnaire | 0.026 | Cross-sectional study | 4 | ||||
| Decreased range of motion | Kuijer 2021 [17] | 1,037 | 1-year | CARES-SF | For BMI 25–30 | 0.05 | OR = 1.5 | Multicenter prospective cohort study | 2B | |
| Levy 2012 [40] | 115 | 12 months | Harvard Alumni Health Study Physical Activity Questionnaire | BMI <25/>25 | <0.05 | Prospective study | 2B | |||
| Basu 2020 [60] | 342 | 37 months | Questionnaire was inspired by the Australian BC Family Study | BMI <25/>25 | 0.04 | HR = 1.42 | 1.6–2.4 | Retrospective study | 4 | |
| Persistent pain | Laurence 2017 [65] | 0.008 | OR = 1.34 | 1.08–1.67 | Meta analysis | 1A | ||||
| Sipilä 2012 [44] | 489 | 6 months | NPRS | BMI <25, 26–30, >30 | <0.01 | OR = 0.58 | 0.34–0.98 | Prospective study | 2B |
Table 5: Mastectomy as a risk factor for arm morbidity following breast cancer treatments
| Disability | Author | N | Follow-up | Measure | Comparison/Comments | P-value | OR/RR/HR | CI (95%) | Type of evidence | Evidence level |
|---|---|---|---|---|---|---|---|---|---|---|
| Persistent pain | Nesvold 2008 [48] | 263 | 47 months | British Columbia Cancer Agency in Canada | 0.001 | Prospective study | 2B | |||
| Pereira 2017 [69] | 506 | 12 months | Brief Pain Inventory, Pain Disability Index | Mastectomy with ALND | RR = 2.52 | 1.25–5.11 | Cohort study | 2B | ||
| Hamood 2018 [24] | 410 | 7.4 years | NPRS | With or without chronic pain | 0.005 | OR = 3.54 | 1.46–8.59 | A cross-sectional study of a random sample | 4 | |
| Paresthesia | Zararli 2009 [32] | 299 | Self-report | 0.048 | RR = 2.493 | 1.53–4.05 | Prospective | 2B | ||
| Lymphedema | Hack 2010 [59] | 316 | 24 months | Circumference and the Norman questionnaire | HR = 2.1 | 1.3–3.4 | Prospective study | 2B | ||
| Nesvold 2008 [48] | 263 | 47 months | Volume calculation | 0.02 | OR = 2.94 | 1.2–7.3 | Prospective study | 2B | ||
| Clark 2005 [64] | 251 | 3 years | Tape measure | RR = 2.04 | 1.18–3.54 | Prospective observational study | 2B | |||
| Park 2008 [63] | 450 | 24 months | Tape measure | 0.035 | OR = 7.48 | 2.38–23.85 | Prospective study | 2B | ||
| Ahmed 2011 [71] | 1,287 | Self-report | OR = 1.13 | 0.72–1.77 | Cross-sectional study | 4 | ||||
| Decreased range of motion | Nesvold 2008 [48] | 263 | 47 months | British Columbia Cancer Agency in Canada | 0.04 | OR = 2.75 | 1.37–5.5 | Prospective study | 2B | |
| Kuijer 2021 [17] | 1,037 | 1 year | CARES-SF | 0.02 | OR = 1.8 | Multicenter prospective cohort study | 2B | |||
| Freitas-Silva 2010 [77] | 70 | Goniometer (shoulder internal rotation) | Breast-conserving therapy vs modified radical mastectomy and immediate reconstruction | 0.03 | OR = 7.23 | 1.28–17.1 | Cross-sectional study | 4 | ||
| Basu 2020 [60] | 342 | 37 months | Questionnaire was inspired by the Australian BC Family Study | 0.04 | HR = 1.8 | 1.1–3.4 | Retrospective study | 4 | ||
| Ahmed 2011 [71] | 1,287 | Self-report | OR = 1.24 | 0.95–1.59 | Cross-sectional study | 4 | ||||
| Adhesive capsulitis | Wong 2021 [75] | 135 | Restricted passive ROM in 2 or more planes of movement (Goniometer), with normal radiographic findings | Mastectomy with reconstruction | 0.021 | OR = 3.93 | 1.23–12.63 | Cross-sectional observational study | 4 | |
| Functional disabilities | Hayes 2010 [39] | 287 | 18 months | QuickDASH and the Functional Assessment of Cancer Therapy Breast questionnaire | 0.006 | OR = 1.95 | 0.98–5.21 | Prospective study | 2B |
Table 6: Axillary lymph node dissection (ALND) as a risk factor for arm morbidity following breast cancer treatments
| Disability | Author | N | Follow-up | Measure | Comparison/Comments | P-value | OR/HR | CI (95%) | Type of evidence | Evidence level |
|---|---|---|---|---|---|---|---|---|---|---|
| Lymphedema | Ashikaga 2010 [37] | 3,963 | 36 months | Water displacement | <0.001 | OR = 1.90 | RCT | 1B | ||
| Del Bianco 2007 [82] | 341 | 24 months | ALND vs. SLNB | 0.01 | OR = 0.48 | 0.25–1.06 | RCT | 1B | ||
| Kilbreat 2016 [53] | 450 | 18 months | Circumference and Bioimpedance spectroscopy | >13 lymph nodes | 0.07 | OR = 2.1 | 0.9–4.9 | Prospective cohort study | 2B | |
| Kwan 2010 [49] | 997 | 20.9 months | Examination by a specialist | No. of dissected lymph nodes | HR = 1.04 | 1.02–1.07 | Prospective cohort study | 2B | ||
| Dominick 2013 [61] | 2,431 | 6 years | Norman and colleagues’ validated telephone lymphedema questionnaire | <0.01 | OR = 2.08 | 1.66–2.60 | Prospective cohort study | 2B | ||
| Park 2008 [63] | 450 | 24 months | Tape measure | 0.008 | OR = 6.61 | 1.64–26.57 | Prospective study | 2B | ||
| Kuijer 2021 [17] | 1,037 | 1 year | CARES-SF | <0.01 | OR = 3.6 | Multicenter prospective cohort study | 2B | |||
| Smoot 2010 [104] | 144 | Circumference and bioimpedance | <0.005 | −7.18–-2.43 | Prospective longitudinal study | 2B | ||||
| Sagen 2014 [83] | 391 | 2.5 years | Water Displacement | ALND vs. SLNB | 0.05 | Prospective study | 2B | |||
| Blanchard 2003 [86] | 1,253 | 12 months | Self-reported | ALND vs. SLNB | <0.001 | Prospective study | 2B | |||
| Belmonte 2018 [87] | 112 | 5 years | Circumference | ALND vs. SLNB | <0.001 | 45.8–257.3 | Prospective study | 2B | ||
| Langer 2007 [81] | 635 | 60 months | Circumference | <0.0001 | OR = 0.15 | 0.08–0.28 | Prospective study | 2B | ||
| Zou 2018 [47] | 387 | 24 months | Circumference and Norman questionnaire | 16><16 lymph nodes | 0.09 | HR = 5.2 | 1.6–17.3 | Prospective study | 2B | |
| Yen 2009 [89] | 1,338 | 4 years | Self-reported | More than 5 nodes | <0.001 | OR = 2.11 | 4.68–5.61 | Population cohort study | 2B | |
| Norman 2009 [105] | 631 | 5 years | Self-reported | HR = 2.61 | 1.77–3.84 | Prospective study | 2B | |||
| Chan 2009 [41] | 5 years | Arm circumference | 0.003 | OR = 2.97 | 1.46–6.03 | Matched case-control study | 3B | |||
| Herremans 2021 [43] | 132 | 5 years | Arm circumference and bioimpedance spectroscopy | LYMPHA technique vs. ALND | 0.036 | OR = 0.39 | 0.16–0.94 | Retrospective cross-sectional study | 4 | |
| Owusu 2019 [78] | 313 | - | - | 0.008 | A descriptive retrospective survey | 4 | ||||
| Kim 2013 [79] | 772 | 8.3 years | Circumference measurements | <0.001 | HR = 2.81 | Retrospective study | 4 | |||
| Mccredie 2001 [56] | 809 | Self-report | OR = 2.4 | 1.0–5.6 | Population-based case-control study | 4 | ||||
| Rebegea 2015 [80] | 305 | >25 nodes | <0.001 | OR = 4.88 | 2.25–10.58 | Cross-sectional study | 4 | |||
| 16–25 nodes | <0.001 | OR = 1.85 | 1.27–2.75 | |||||||
| Da Costa Vieira 2016 [3] | 622 | 10 years | Self-report | For ≥ 15 lymph nodes | 0.017 | HR = 9.12 | 1.15–72.12 | Retrospective study | 4 | |
| Ahmed 2011 [71] | 1,287 | Self-report | OR = 3.52 | 1.32–9.34 | Cross-sectional study | 4 | ||||
| Gärtner 2010 [36] | 3,104 | Self-report | <0.0001 | OR = 2.89 | 2.42–3.45 | Cross-sectional study | 4 | |||
| Crosby 2012 [58] | 1,117 | From medical records | <0.001 | OR = 6.69 | 2.59–17.29 | Retrospective study | 4 | |||
| Meeske 2009 [35] | 494 | 50 months | Self-report of lymphedema | 10 or more lymph nodes | OR = 2.16 | 1.12–4.17 | A case-control study | 4 | ||
| Langer 2007 [81] | 635 | 60 months | VAS | <0.0001 | OR = 0.33 | 0.20–0.54 | Prospective study | 2B | ||
| Persistent pain | Kramer 2019 [73] | 349 | SPADI questionnaire | OR = 0.48 | 0.23–0.98 | Cross-sectional study | 4 | |||
| Mejdahl 2013 [27] | 2,411 | Developed questionnaire | <0.001 | OR = 2.04 | 1.60–2.61 | Cross-sectional study | 4 | |||
| Chiang 2019 [74] | 201 | NPRS and Brief Pain Inventory | 0.03 | OR = 4.33 | 1.19–15.73 | Retrospective cross-sectional study | 4 | |||
| Functional disabilities | Del Bianco 2007 [82] | 341 | 24 months | - | ALND vs. SLNB at 6 months | 0.005 | OR = 0.47 | 0.27–0.79 | RCT | 1B |
| Habib 2020 [92] | 44 | 6 weeks | QuickDASH disability score | 0.010 | Prospective cohort | 2B | ||||
| Hayes 2010 [39] | 287 | 18 months | QuickDASH and Functional Assessment of Cancer Therapy Breast questionnaire | 0.02 | OR = 4.81 | 1.64–14.14 | Prospective study | 2B | ||
| Kramer 2019 [73] | 349 | SPADI questionnaire | OR = 0.99 | 0.54–1.81 | Cross-sectional study | 4 | ||||
| Decreased range of motion | Ashikaga 2010 [37] | 3,963 | 36 months | <0.001 | OR = 1.54 | RCT | 1B | |||
| Nesvold 2008 [48] | 263 | 47 months | British Columbia Cancer Agency in Canada | 0.01 | OR = 0.92 | 0.85–0.98 | Prospective study | 2B | ||
| Langer 2007 [81] | 635 | 60 months | ROM measurements | 0.0002 | OR = 0.22 | 0.15–0.56 | Prospective study | 2B | ||
| Hack 2010 [59] | 316 | 12 months | Volume measurements | 0.003 | OR = 3.62 | 8.48–1.54 | Cross-sectional study | 4 | ||
| Ahmed 2011 [71] | 1,287 | Self-report | OR = 2.38 | 1.41–4.03 | Cross-sectional study | 4 |
Table 7: Radiotherapy as a risk factor for arm morbidity following breast cancer treatments
| Disability | Author | N | Follow-up | Measure | Comparison/Comments | P-value | OR/RR/HR | CI (95%) | Type of evidence | Evidence level |
|---|---|---|---|---|---|---|---|---|---|---|
| Persistent pain | Zararli 2009 [32] | 299 | VAS | 0.006 | RR = 2.80 | 1.341–3.821 | Prospective study | 2B | ||
| Habib 2020 [92] | 124 | 12 months | NPRS | 0.03 | OR = 2.52 | 1.13–5.82 | Prospective observational study | 2B | ||
| Hamood 2018 [24] | 410 | 7.4 years | NPRS | With or without chronic pain | 0.003 | OR = 2.96 | 1.43–6.12 | A cross-sectional study of a random sample | 4 | |
| Decreased range of motion | Ashikaga 2010 [37] | 3,963 | 36 months | 0.037 | OR = 2.48 | RCT | 1B | |||
| Adriaenssens 2012 [85] | 118 | 3 months | ROM | Abduction after radiation to regional nodes | 0.0011 | RCT | 1B | |||
| Zararli 2009 [32] | 299 | Physical examination | 0.006 | RR = 2.46 | 1.290–4.466 | Prospective study | 2B | |||
| Kuijer 2021 [17] | 1,037 | 1 year | CARES-SF | 0.01 | OR = 2.4 | Multicenter prospective cohort study | 2B | |||
| Kikuuchi 2020 [68] | 223 | 3 months | ROM | 0.006 | OR = 0.34 | 0.16–0.73 | Prospective study | 2B | ||
| Basu 2020 [60] | 342 | 37 months | Questionnaire was inspired by the Australian Breast Cancer Family Study | 0.01 | HR = 1.1 | 1.5–2.6 | Retrospective study | 4 | ||
| Ahmed 2011 [71] | 1,287 | Self-report | OR = 1.72 | 1.15–2.57 | Cross-sectional study | 4 | ||||
| Lymphedema | Ashikaga 2010 [37] | 3,963 | 36 months | Water displacement | 0.007 | OR = 3.47 | RCT | 1B | ||
| Zou 2018 [47] | 387 | 24 months | Circumference and Norman questionnaire | <0.001 | HR = 3.9 | 2.0–7.5 | Prospective study | 2B | ||
| Ozcinar 2012 [98] | 218 | 24–82 months | Circumference measurements | <0.001 | Prospective observational cohort | 2B | ||||
| Kilbreat 2016 [53] | 450 | 18 months | Circumferences and Bioimpedance spectroscopy | 0.01 | OR = 3.7 | 1.6–8.7 | Prospective cohort study | 2B | ||
| Ugur 2013 [62] | 455 | 53 months | Tape measure | 0.007 | OR = 1.83 | 1.17–2.84 | Prospective study | 2B | ||
| Bevilacqua 2012 [42] | 1,051 | 5 years | Circumferences | > 6 months | 0.0001 | Prospective cohort study | 2B | |||
| Park 2008 [63] | 450 | 24 months | Tape measure | Axillary radiotherapy | <0.001 | OR = 6.73 | 2.58–17.54 | Prospective study | 2B | |
| Kuijer 2021 [17] | 1,037 | 1-year | CARES-SF | 0.05 | OR = 1.8 | Multicenter prospective cohort study | 2B | |||
| Dominick 2013 [61] | 2,431 | 6 years | Norman and colleagues’ validated telephone lymphedema questionnaire | Lumpectomy and radiation | <0.01 | OR = 1.12 | 0.91–1.37 | Prospective cohort study | 2B | |
| Mastectomy and radiation | OR = 2.02 | 1.52–2.69 | ||||||||
| Ahmed 2011 [71] | 1,287 | Self-report | OR = 1.77 | 0.92–3.40 | Cross-sectional study | 4 | ||||
| Hack 2010 [59] | 316 | 12 months | Volume measurements | 0.007 | Cross-sectional study | 4 | ||||
| Herremans 2021 [43] | 132 | 5 years | Circumferences and bioimpedance spectroscopy | LYMPHA technique VS ALND | 0.032 | OR = 0.38 | 0.15–0.91 | Retrospective cross-sectional study | 4 | |
| Kwan 2002 [84] | 744 | Self-report | <0.001 | OR = 3.1 | Cross-sectional | 4 | ||||
| Sueangamiam 2021 [88] | 308 | Circumferences | 0.046 | HR = 1.81 | 1.09–13.28 | Cross-sectional study | 4 | |||
| Da Costa Vieira 2016 [3] | 622 | 10 years | Self-report | Supra-clavicular radiation | 0.043 | HR = 1.87 | 1.02–3.45 | Retrospective study | 4 | |
| Gärtner 2010 [36] | 3104 | Self-report | 0.0005 | OR = 1.72 | 1.30–2.27 | Repeated cross-sectional study | 4 | |||
| Crosby 2012 [58] | 1117 | From medical record | Immediate breast reconstruction and BMI <25/>25 | 0.023 | OR = 2.23 | 1.12–4.89 | Retrospective study | 4 |
Table 8: Chemotherapy as a risk factor for arm morbidity following breast cancer treatments
| Disability | Author | N | Follow-up | Measure | Comparison/Comments | P-value | OR/HR | CI (95%) | Type of evidence | Evidence level |
|---|---|---|---|---|---|---|---|---|---|---|
| Persistent pain | Kramer 2019 [73] | 349 | SPADI questionnaire | OR = 0.39 | 0.18–0.83 | Cross-sectional study | 4 | |||
| Habib 2020 [92] | 0.02 | OR = 3.39 | 1.24–10.41 | Prospective observational study | 2B | |||||
| Functional disabilities | Kramer 2019 [73] | 349 | SPADI questionnaire | OR = 0.37 | 0.18–0.77 | Cross-sectional study | 4 | |||
| Khan 2012 [33] | 85 | FIM Measurement | < 0.001 | Prospective study | 2B | |||||
| Decreased range of motion | Woo 2018 [45] | 430 | Having restricted ROM ≥ 30° in compared to unaffected side | Different modalities of breast reconstructions | 0.002 | OR = 5.578 | 1.83–16.95 | Prospective study | 2B | |
| Ashikaga 2010 [37] | 3,963 | 36-months | 0.003 | OR = 0.73 | RCT | 1B | ||||
| Lymphedema | Kilbreat 2016 [53] | 450 | 18 months | Circumferences and bioimpedance spectroscopy (BIS) | Taxane-based chemotherapy | 0.04 | OR = 2.3 | 1.0–5.2 | Prospective cohort study | 2B |
| Chemotherapy | 0.08 | OR = 2.2 | 0.9–5.3 | |||||||
| Rupp 2019 [99] | 385 | LBCQ-D and SDBC-D | Adjuvant chemotherapy | 0.005 | OR = 2.5 | 0.21–0.76 | Retrospective study | 4 | ||
| Ahmed 2011 [71] | 1,287 | Self-report | OR = 3.05 | 1.75–5.30 | Cross-sectional study | 4 | ||||
| Bevilacqua 2012 [42] | 1,051 | 5 years | Circumferences | At 0–6 months | 0.0001 | Prospective cohort | 2B | |||
| Herremans 2021 [43] | 132 | 5 years | Circumferences and bioimpedance spectroscopy | LYMPHA technique VS ALND | 0.030 | OR = 0.38 | 0.15–0.90 | Retrospective cross study | 4 | |
| Da Costa Vieira 2016 [3] | 622 | 10 years | Self-report | 0.051 | HR = 0.5 | 0.21–1.17 | Retrospective study | 4 | ||
| Das 2015 [55] | 199 | Self-reported | Tamoxifen therapy only | 0.02 | OR = 2.31 | 1.13–4.71 | Cross-sectional | 4 | ||
| Gärtner 2010 [36] | 3104 | Self-report | <0.0001 | OR = 1.92 | 1.66–2.22 | Repeated cross-sectional study | 4 | |||
| Norman 2009 [105] | 631 | 5 years | Self-reported | HR = 1.46 | 1.02–2.04 | Prospective study | 2B |
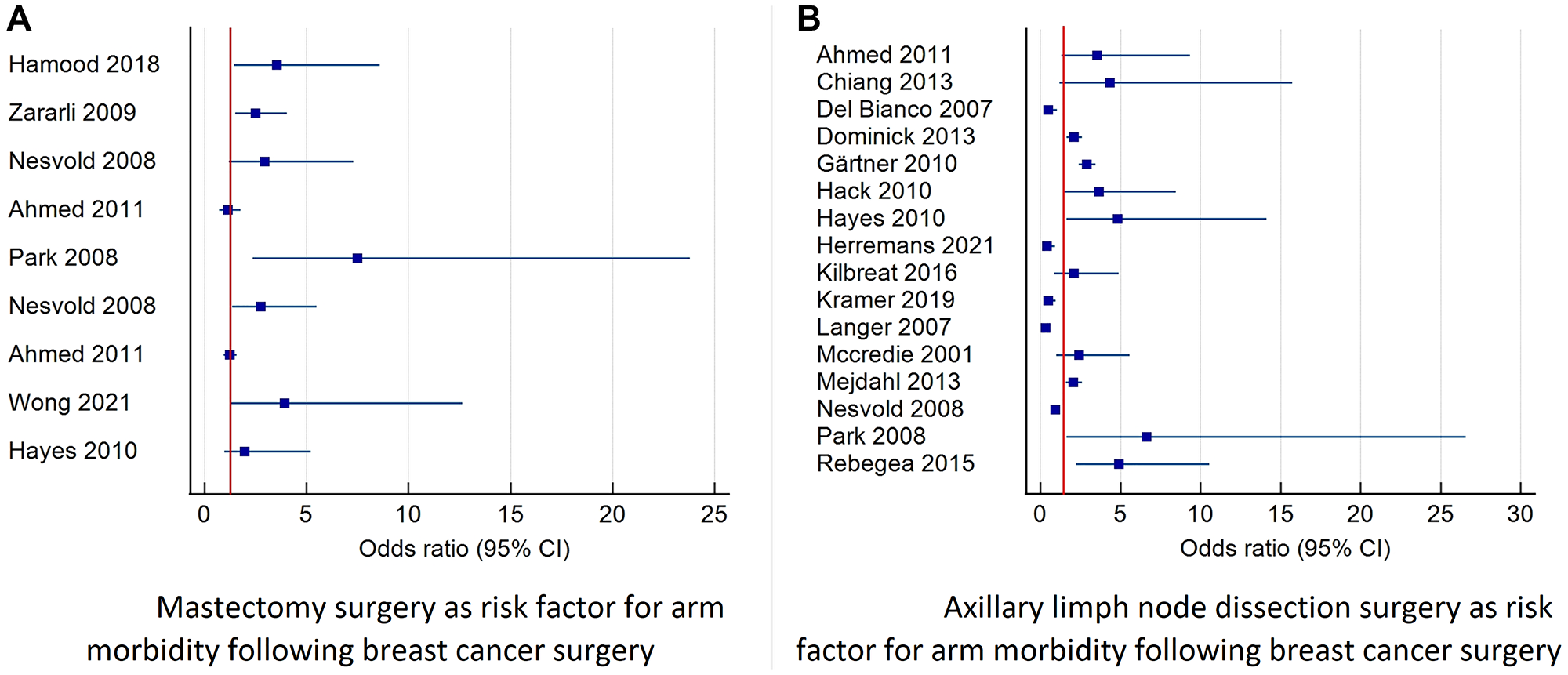
Figure 4: Forest plot diagram of odds ratio (95% CI) for surgery related factors as risk factors for prolonged arm morbidity.
This figure describes studies that reported the odds ratio and 95% confidence interval for mastectomy and axillary surgery as risk factors for combined morbidity of the arm including: pain, lymphedema, decreased function and decreased range of motion. (A) Describes the risk of morbidity after mastectomy surgery. (B) Describes the risk of morbidity after axillary lymph node dissection. Abbreviation: CI: confidence interval.
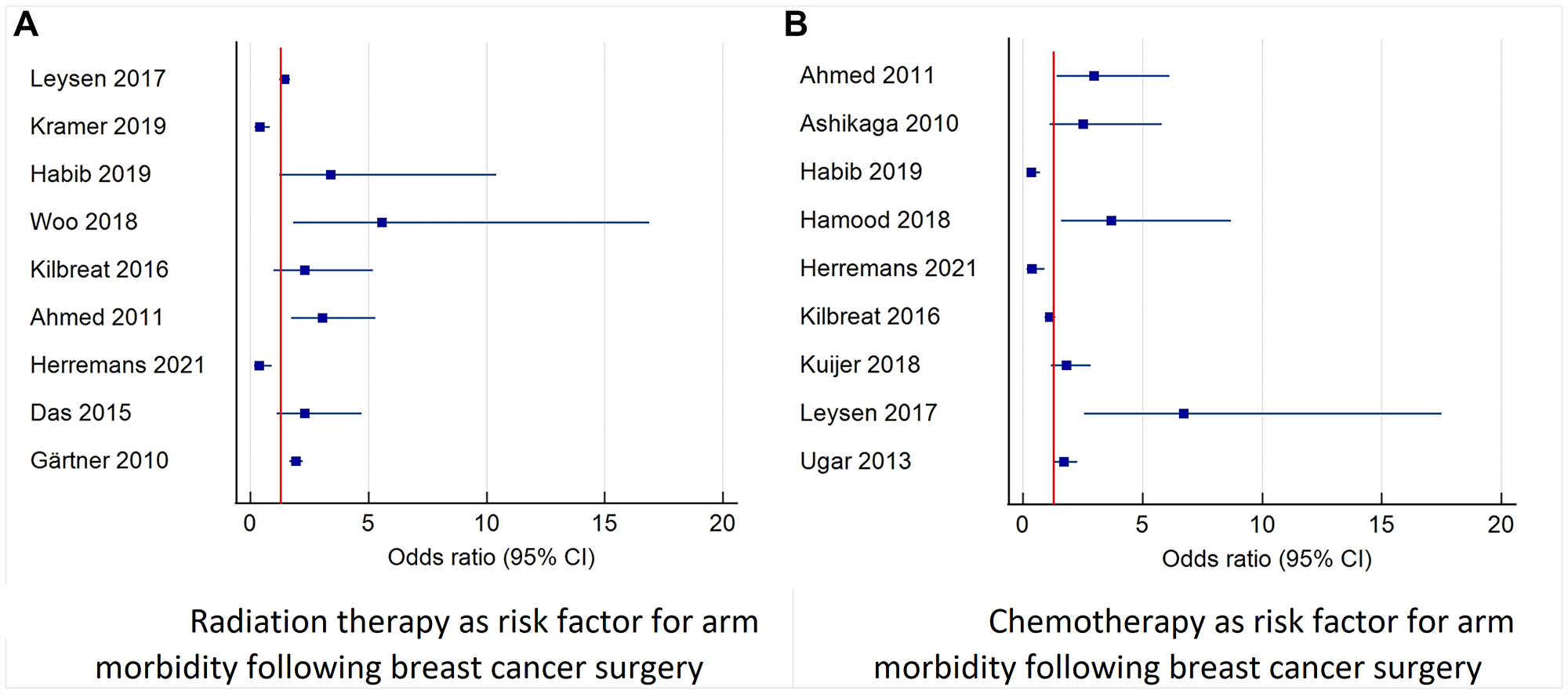
Figure 5: Forest plot diagram of odds ratio (95% CI) for risk factors for arm morbidity related to oncological treatment.
This figure describes studies that reported the odds ratio and 95% confidence interval for radiotherapy and chemotherapy as risk factors for combined morbidity of the arm including: pain, lymphedema, decreased function and decreased range of motion. (A) Describes the risk of radiation therapy morbidity. (B) Describes the risk of morbidity after chemotherapy (adjuvant and neoadjuvant). Abbreviation: CI: confidence interval.
Risk factors for the morbidity of the arm divided into three categories: personal factors, factors related to the type of surgery, and factors related to the type of oncological treatment
Personal risk factors for arm morbidities
Age
Young age was evaluated in seven studies, including 18,272 patients. Young age was found to be associated with persistent pain or more severe pain [23–29], radiation-associated pain [30, 31], paresthesia, loss of strength [32], poor functioning [33, 34] and lymphedema [35, 36]. Younger women (≤49) were found to have larger tumor sizes and were associated with having a mastectomy in contrast to a lumpectomy [37]. Furthermore, young age was found to be a risk factor for axillar web syndrome (AWS), a complication that often develops within weeks following BC surgery and may present as one or more visible or palpable tight cords of tissue in the axilla [38].
Age over 50 was evaluated in seven trials comprising 7,914 patients, and was found to be associated with functional decline [39], ROM deficit [40], lymphedema [37, 41–43], and pain six months after surgery [44]. Older women who underwent different modalities of breast reconstruction were at higher risk of limitation in ROM [45] (See Tables 2, 3).
Body mass index (BMI)
BMI was evaluated in 15 trials comprising 9,025 patients. BMI above 30 was associated with higher risk for lymphedema [17, 35, 41, 42, 46–58], functional disability [59], and decreased ROM [17]. BMI above 25 was negatively and significantly related to shoulder ROM deficit, function decline [40, 60], lymphedema [48, 61–64], and pain [65] (See Table 4).
BC history
BC history was evaluated in one trial that included 489 participants. A high number of previous operations was found to be a risk factor for persistent pain six months after surgery [44].
Preoperative ROM deficit
Preoperative ROM deficit was evaluated in two trials including 192 participants. A history of shoulder problems and restricted humeral extension preoperatively was found to be associated with persistent pain [66, 67].
Preoperative pain
Preoperative pain was evaluated in three trials including 20,459 participants. Preoperative pain in the breast area was found to associated with persistent pain and functional disability [25, 67], in addition to chronic pain conditions [44].
Functional decline before surgery
Functional decline prior to surgery may cause more functional disabilities after surgery, as well as a decrease in ROM [67].
Emotional support
Lack of emotional support was evaluated in one trial that included 316 patients. Lack of a partner was found to be associated with persistent postoperative pain six months after surgery [59].
Low educational attainment
Low educational status was found to be associated with ROM restrictions [65], and lymphedema [50, 56]. On the other hand, a different study found associations between a high level of education and lymphedema [49].
Low socioeconomic status
Defined by income was found to have an effect on upper body functional impairments [39]. In addition, patients who reported financial distress were found to be at a higher risk of lymphedema one year after surgery [17].
Follow-up by public health services
After cancer treatment, receiving care from public health services was associated with a higher degree of functional disability compared to patients treated in private clinics [34].
Treatment on the dominant side
It was found that treatment to the contralateral side can have an effect on upper body functional impairments [39] and ROM of the effected arm [68].
Breast cancer stage at diagnosis
Regionally advanced cancer was associated with chronic pain [24]. Cancer Stage III/IV was found to be a predictor of neuropathic pain [69], while more advanced disease was found to cause arm morbidity [70], including pain, limited ROM [59], and lymphedema [17, 50, 62, 63, 71]. Aggressive tumors were found to be associated with poor levels of functioning [33].
Previous smoking
Smoking was found to be a risk factor for persistent pain six months after surgery [59].
Diabetes mellitus
Diabetes was found to be a prognostic factor for arm and shoulder morbidity, including stiffness, edema, numbness, and pain [60].
A history of hypertension
Hypertension was found to be a risk factor for lymphedema [35].
Anxiety
Anxiety was found to be a predictor of neuropathic pain [69]. Additionally, arm symptoms, lower emotional functioning and insomnia presented one month following surgery were identified as significant risk factors for persistent pain [72].
African American ethnicity
African American ethnicity was associated with an increased risk of lymphedema [49] and higher pain levels [73], and radiation-associated pain [30]. Non-European ethnicity was identified as risk factors for moderate to severe persistent pain after surgery [74].
Comorbid diseases
Comorbidity were significantly correlated with the development of lymphedema [50, 71] and pain [30].
Time after surgery
The time elapsed since surgery had a significant correlation with the development of lymphedema [50].
Surgery-related risk factors for arm morbidities
The effect of a lumpectomy vs. a mastectomy surgery
The effect of the type of surgery was evaluated in 16 articles that comprised 7,392 patients. Chronic pain was found to be positively associated with a mastectomy compared to breast-conserving surgery [24, 48]. A mastectomy without reconstruction was found to be related to flexion and abduction ROM loss at 12 months after surgery [40] and functional impairments [39]. Breast-conserving surgery was associated with long-term paresthesia [32]. In addition, both radical mastectomy and modified radical mastectomy were found to be risk factors for lymphedema [47, 59, 64], with both causing restricted shoulder ROM [17, 48, 60]. A mastectomy was also found to be a risk factors for adhesive capsulitis [75]. A lumpectomy was found to be related to a decline in the level of activities of daily living [76]. Contrary to expectations, it was found that breast-conserving therapy caused a higher prevalence of restricted internal rotation compared to modified radical mastectomy and immediate breast reconstruction [77] (see Table 5 and Figure 4A).
Axillary lymph node dissection (ALND)
ALND was found to cause higher lymphedema frequency [3, 17, 42, 43, 47, 49, 56, 63, 78–82], persistent pain [27, 73, 74, 81], reduced muscle strength and restricted ROM compared to SLNB [1, 25, 39, 46, 59, 65, 66, 70, 81–87], in addition to seroma formation and infections [86]. A dissection of more than 20 lymph nodes increases the risk of lymphedema [58, 61, 88], and even 6–10 dissected nodes may cause lymphedema, pain, and ROM restrictions [35, 67, 71, 89]. In addition to breast-conserving surgery or a mastectomy, ALND was found to be a predictor for neuropathic pain [69]. Furthermore, ALND was associated with more numbness and tingling compared to SLNB [37], and a higher risk for AWS [38] (See Table 6 and Figure 4B).
Breast reconstruction surgery
Breast reconstruction surgery was evaluated in three trials comprising 766 patients. Regardless of the specific reconstructive modality, pain and functional deficits following surgery are extremally common [45, 90], and were identified as risk factors for moderate to severe persistent pain after surgery [74]. Reconstruction surgery was found to be a risk factors for adhesive capsulitis [75], but not a risk factor for lymphedema [58, 91].
Pain during hospitalization
Pain during hospitalization was evaluated in four trials comprising 597 patients. Greater acute postoperative pain was found to be an indicator of persistent pain [25, 92]. Higher pain levels in the early postoperative period were found to correlate with restricted shoulder ROM [93].
Postoperative infection
Postoperative infection was found to cause pain and functional disability [59]. Trauma or infection in the affected ipsilateral arm after surgery were found to be risk factors associated with lymphedema [41, 42, 50, 52, 54, 62], and cellulite events [46].
Axillary web syndrome (AWS)
AWS was identified as a risk factor for reduced function, ROM impairments, pain, and lymphedema at 18 months [94].
The number of positive axillar lymph nodes
The number of dissected lymph nodes was related to loss of flexion and abduction ROM [40] and lymphedema [47, 48, 50, 70, 89]. Furthermore, the number of positive nodes were found to be a cause of reduced ROM in reconstruction surgeries [45].
Lymphedema
Lymphedema was found in a meta-analysis as the most significant risk factor for chronic pain [65], diminished quality of life and functional impairments [39, 95]. In addition, early edema in the first six months postoperatively was found to be a risk factor for lymphedema [42].
Limitation in shoulder movement due to pain, and lymphedema was found to cause functional limitations [47].
Postoperative seroma was found to be a risk factor for lymphedema [42].
Capsule invasion of the tumor was found to be a risk factor for lymphedema [96].
Damage to the intercostobrachial nerve was found to be a predictor of neuropathic pain [69].
Hospital skin puncture (defined as any intentional puncture by a health professional or patient of the patient’s skin in the hand or arm on the ipsilateral side with a needle for any purpose, including finger prick glucose testing) was found to be a risk factor for lymphedema [64].
Treatment-related risk factors for arm morbidities
Radiation therapy
The effect of radiation therapy was evaluated in 25 trials including 24,195 patients and was found to be a risk factor for persistent pain [24, 32, 65, 92, 97], shoulder stiffness [32, 60, 71], decreased ROM [17, 37, 68], and lymphedema [3, 17, 36, 37, 42, 43, 46, 47, 61–63, 70, 84, 88, 98] (See Table 7 and Figure 5A).
Chemotherapy
Chemotherapy was evaluated in 13 trials including 12,406 patients. Neoadjuvant and adjuvant chemotherapy were found to be risk factors for chronic pain [65, 73, 92], functional disabilities [33, 73], and lymphedema [43, 53]. Neoadjuvant chemotherapy was found to be a risk factor for limitations in ROM in patients that had undergone different modalities of breast reconstructions [45]. Adjuvant chemotherapy was found to be a risk factor for the appearance of lymphedema [3, 42, 71, 99], especially tamoxifen [55], although taxane-based chemotherapy were not found to increase the risk of lymphedema compared to patients receiving no chemotherapy or non-taxane adjuvant chemotherapy. Those treated with docetaxel may experience mild swelling, but this does not translate into subsequent lymphedema [100] (see Table 8 and Figure 5B).
Hormonal therapy was found to be a risk factor for persistent pain [76].
A description of the number of studies found in the literature review for each risk factor, in relation to the different morbidity: lymphedema, decreased range of motion, decreased function and prolonged pain, is shown in Supplementary Figure 1.
DISCUSSION
Breast cancer surgery and treatments are known to cause long-term physical morbidity of the arm. These morbidities include prolonged pain or chronic pain [23, 29], limitations in ROM, decreased function [1, 2, 6, 59, 84] and lymphedema [8, 16, 101]. All these morbidities can last for months or even years after surgery [1, 2], and cause an additional burden on the primary cancer treatment.
Our systematic review aimed to comprehensively analyse the risk factors for these four long-term arm morbidities that are common after BC surgeries and treatments. The analysis encompassed various elements, such as surgical and oncological factors, patient medical conditions, lifestyle habits, work-related factors, family support, and emotional well-being.
This review revealed 29 primary risk factors associated with arm morbidity after BC treatment. These factors ranged from surgical procedures such as mastectomy and ALND to medical considerations like chemotherapy, radiation therapy, and cancer stage. Additionally, patient-related factors such as BMI, smoking, anxiety levels, and emotional support were found to influence the development of morbidity.
Age emerged as a significant factor impacting morbidity. Older age was found to be a risk factor for lymphedema, functional limitation and ROM deficits, while young age was found to be associated with prolonged pain, as found in a meta-analysis by Wang et al. [25]. Contrary to the report of Sipila et al., who found that older age (over 70) is associated with prolonged pain [44].
Additional risk factors contributing to prolonged arm morbidity following BC have been investigated by various researchers, each focusing on specific morbidities. Leysen et al. and Wang et al., in their systematic review and meta-analysis, identified several risk factors associated with prolonged pain, including BMI>30, lower education levels (<12–13 years), younger age, lymphedema, smoking, axillary lymph node dissection (ALND), chemotherapy, hormonal therapy, radiation, greater acute postoperative pain, and preoperative pain [25, 65].
Similarly, DiSipio et al., in their literature review and meta-analysis, reported risk factors for lymphedema, which include ALND or a greater number of lymph nodes dissected, mastectomy surgery, and being overweight or obese [101]. Torgbenu et al. also emphasized BMI>25 as a significant risk factor for lymphedema [8].
In this comprehensive review, additional risk factors were found to be associated with prolonged arm morbidity following BC treatments. These factors encompass various aspects, such as low socioeconomic level, African-American ethnicity, lack of monitoring by public health services, insufficient emotional support, anxiety, comorbidity, advanced cancer stage, preoperative functional decline, preoperative ROM deficit, postoperative infection, trauma to the affected arm, AWS, the number of positive lymph nodes, and postoperative seroma.
The identification of these diverse risk factors enhances our understanding of the multifactorial nature of arm morbidity in breast cancer patients. By acknowledging and recognizing these risk factors, healthcare providers can develop more targeted interventions and personalized treatment plans. This, in turn, leads to improved outcomes and a reduction in the burden of prolonged arm morbidity for patients. Such invaluable insights are instrumental in optimizing rehabilitation strategies and enhancing patient care, ultimately resulting in an improved quality of life for breast cancer survivors.
Our findings underscore the importance of utilizing risk factor information to create predictive tools and tailored treatment plans. By addressing these risk factors proactively, we have the potential to reduce future morbidity, improve patient outcomes, and significantly enhance the overall recovery process for breast cancer patients.
Materials and Methods
This systematic review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and meta-analysis guidelines (PRISMA) [102].
To identify relevant studies regarding risk factors for persistent pain, lymphedema, decreased range of motion (ROM) and function in cancer survivors. A systematic search of the literature was conducted in the databases PubMed, Cochrane Central Register of Controlled Trials, MEDLINE, and Pedro up to February 2022, using MeSH terms and free key words. Authors were contacted if the full texts of their studies could not be retrieved.
Search terms associated with BC-related arm morbidity were used (e.g., risk factors, arm morbidity, chronic/persistent pain, function decline, function disability, lymphedema, lymphedema, ROM deficit, decreased/diminished ROM). We searched for different risk factors, namely, BMI, age, mastectomy, axillary dissection, breast reconstructions, chemotherapy, radiotherapy, BC history, pre-operative pain, pre-operative functional decline, pre-operative ROM deficit, pain during hospitalization, comorbidity, race, socioeconomic status, education, postoperative complications such as infection or serum, emotional support, and anxiety levels.
Inclusion criteria
The inclusion criteria were as follows: (1) Studies and systematic reviews and meta-analyses published between the years 2000–2021; (2) full text in English; (3) studies that examined risk factors for arm morbidity in patients diagnosed with breast cancer (BC); (4) studies on patients who had undergone surgical and oncological treatments; and 5) articles in which the data for determining risk factors were available.
Exclusion criteria
The exclusion criteria were as follows: (1) Case reports and study protocols; (2) patients with a diagnosis of cancer recurrence; (3) subjects diagnosed with cancers other than BC; (4) articles in which persistent pain, lymphedema, decreased range of motion, ROM and function were not presented as an outcome; (5) studies with less than 30 participants; and (6) systematic reviews and meta-analyses.
Two independent reviewers (IK, DS) screened the titles and abstracts of studies identified as eligible. Articles considered potentially relevant were obtained, and the full articles were screened for inclusion by the same two independent reviewers. IK and DS resolved disagreements by consensus. The tables reported in the review represent studies in which the researchers found positive relationships between the various risk factors for long-term morbidity of the arm (including: pain, decreased function, limitation of range of motion or lymphedema).
Quality assessment
The level of evidence was evaluated according to the Levels of Evidence for Therapeutic Studies [103]. The risk of bias was evaluated using the National Institutes of Health (NIH) quality assessment tool for each type of study: for RCTs, using the Quality Assessment of Controlled Intervention Studies, for non-RCTs, using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies, both of which include 14 items.
Conclusions
In conclusion, gaining a comprehensive understanding of the risk factors associated with arm morbidity following breast cancer treatment offers invaluable insights to healthcare professionals, enabling them to optimize patient care and rehabilitation strategies effectively. By identifying and proactively addressing these risk factors, we can strive to minimize the impact of long-term physical morbidity and enhance the overall quality of life for breast cancer survivors. Through this proactive approach, we can foster better outcomes and support the well-being of those who have overcome breast cancer challenges.
The main risk factors for lymphedema include the number of removed lymph nodes, BMI, mastectomy, disease stage, radiation, chemotherapy, infection, and post-surgery trauma. Decreased ROM is linked to radiation, mastectomy, ALND, and BMI >30. Decreased function is influenced by ALND, age <50, BMI >25, and chemotherapy. Prolonged pain is associated with age <50, radiation, chemotherapy, ALND, disease stage, mastectomy, and intense preoperative pain. Future research should use these risk factors to develop predictive tools and tailored treatment protocols for improved patient outcomes.
Abbreviations
BC: Breast cancer; BMI: body mass index; PT: physical therapy; ALND: axillary lymph node dissection; SLNB: sentinel lymph node biopsy; VAS: visual analog scale; ROM: range of motion; NPRS: numeric pain rating scale; AWS: axillary web syndrome; CI: confidence interval; OR: odds ratio; HR: hazard ratio; RR: relative risk; RCT: randomize control trail; N: number.
CONFLICTS OF INTEREST
Authors have no conflicts of interest to declare.
FUNDING
No funding was used for this paper.
References
1. Kootstra JJ, Dijkstra PU, Rietman H, de Vries J, Baas P, Geertzen JH, Hoekstra HJ, Hoekstra-Weebers JE. A longitudinal study of shoulder and arm morbidity in breast cancer survivors 7 years after sentinel lymph node biopsy or axillary lymph node dissection. Breast Cancer Res Treat. 2013; 139:125–34. https://doi.org/10.1007/s10549-013-2509-y. [PubMed].
2. Hauerslev KR, Madsen AH, Overgaard J, Damsgaard TE, Christiansen P. Long-term follow-up on shoulder and arm morbidity in patients treated for early breast cancer. Acta Oncol. 2020; 59:851–58. https://doi.org/10.1080/0284186X.2020.1745269. [PubMed].
3. da Costa Vieira RA, da Costa AM, de Souza JL, Coelho RR, de Oliveira CZ, Sarri AJ, Junior RJ, Zucca-Matthes G. Risk Factors for Arm Lymphedema in a Cohort of Breast Cancer Patients Followed up for 10 Years. Breast Care (Basel). 2016; 11:45–50. https://doi.org/10.1159/000442489. [PubMed].
4. Palesh O, Scheiber C, Kesler S, Mustian K, Koopman C, Schapira L. Management of side effects during and post-treatment in breast cancer survivors. Breast J. 2018; 24:167–75. https://doi.org/10.1111/tbj.12862. [PubMed].
5. Chiu M, Bryson GL, Lui A, Watters JM, Taljaard M, Nathan HJ. Reducing persistent postoperative pain and disability 1 year after breast cancer surgery: a randomized, controlled trial comparing thoracic paravertebral block to local anesthetic infiltration. Ann Surg Oncol. 2014; 21:795–801. https://doi.org/10.1245/s10434-013-3334-6. [PubMed].
6. Smith HS, Wu SX. Persistent pain after breast cancer treatment. Ann Palliat Med. 2012; 1:182–94. https://doi.org/10.3978/j.issn.2224-5820.2012.10.13. [PubMed].
7. Lee MK, Kang HS, Lee KS, Lee ES. Three-Year Prospective Cohort Study of Factors Associated with Return to Work After Breast Cancer Diagnosis. J Occup Rehabil. 2017; 27:547–58. https://doi.org/10.1007/s10926-016-9685-7. [PubMed].
8. Torgbenu E, Luckett T, Buhagiar MA, Chang S, Phillips JL. Prevalence and incidence of cancer related lymphedema in low and middle-income countries: a systematic review and meta-analysis. BMC Cancer. 2020; 20:604. https://doi.org/10.1186/s12885-020-07079-7. [PubMed].
9. Joly F, Lange M, Dos Santos M, Vaz-Luis I, Di Meglio A. Long-Term Fatigue and Cognitive Disorders in Breast Cancer Survivors. Cancers (Basel). 2019; 11:1896. https://doi.org/10.3390/cancers11121896. [PubMed].
10. Costa AR, Fontes F, Pereira S, Gonçalves M, Azevedo A, Lunet N. Impact of breast cancer treatments on sleep disturbances - A systematic review. Breast. 2014; 23:697–709. https://doi.org/10.1016/j.breast.2014.09.003. [PubMed].
11. Houbois CP, Nolan M, Somerset E, Shalmon T, Esmaeilzadeh M, Lamacie MM, Amir E, Brezden-Masley C, Koch CA, Thevakumaran Y, Yan AT, Marwick TH, Wintersperger BJ, Thavendiranathan P. Serial Cardiovascular Magnetic Resonance Strain Measurements to Identify Cardiotoxicity in Breast Cancer: Comparison With Echocardiography. JACC Cardiovasc Imaging. 2021; 14:962–74. https://doi.org/10.1016/j.jcmg.2020.09.039. [PubMed].
12. Doege D, Thong MS, Koch-Gallenkamp L, Bertram H, Eberle A, Holleczek B, Pritzkuleit R, Waldeyer-Sauerland M, Waldmann A, Zeissig SR, Jansen L, Brenner H, Arndt V. Health-related quality of life in long-term disease-free breast cancer survivors versus female population controls in Germany. Breast Cancer Res Treat. 2019; 175:499–510. https://doi.org/10.1007/s10549-019-05188-x. [PubMed].
13. Ewertz M, Jensen AB. Late effects of breast cancer treatment and potentials for rehabilitation. Acta Oncol. 2011; 50:187–93. https://doi.org/10.3109/0284186X.2010.533190. [PubMed].
14. Falcicchio C, Di Lallo D, Fabi A, Bonucci A, Perrone M, Pace A, Corti A, Giacomelli L, Pugliese P. Use of rehabilitation pathways in women with breast cancer in the first 12 months of the disease: a retrospective study. BMC Cancer. 2021; 21:311. https://doi.org/10.1186/s12885-021-07927-0. [PubMed].
15. van Londen G, Beckjord E, Dew M, Cuijpers P, Tadic S, Brufsky A. Breast cancer survivorship symptom management: current perspective and future development. Breast Cancer Manag. 2013; 2:71–81. https://doi.org/10.2217/bmt.12.63. [PubMed].
16. Basta MN, Wu LC, Kanchwala SK, Serletti JM, Tchou JC, Kovach SJ, Fosnot J, Fischer JP. Reliable prediction of postmastectomy lymphedema: The Risk Assessment Tool Evaluating Lymphedema. Am J Surg. 2017; 213:1125–33.e1. https://doi.org/10.1016/j.amjsurg.2016.08.016. [PubMed].
17. Kuijer A, Dominici LS, Rosenberg SM, Hu J, Gelber S, Di Lascio S, Wong JS, Ruddy KJ, Tamimi RM, Schapira L, Borges VF, Come SE, Sprunck-Harrild K, et al. Arm Morbidity After Local Therapy for Young Breast Cancer Patients. Ann Surg Oncol. 2021; 28:6071–82. https://doi.org/10.1245/s10434-021-09947-3. [PubMed].
18. Ribeiro Pereira ACP, Koifman RJ, Bergmann A. Incidence and risk factors of lymphedema after breast cancer treatment: 10 years of follow-up. Breast. 2017; 36:67–73. https://doi.org/10.1016/j.breast.2017.09.006. [PubMed].
19. Stout NL, Binkley JM, Schmitz KH, Andrews K, Hayes SC, Campbell KL, McNeely ML, Soballe PW, Berger AM, Cheville AL, Fabian C, Gerber LH, Harris SR, et al. A prospective surveillance model for rehabilitation for women with breast cancer. Cancer. 2012; 118:2191–200. https://doi.org/10.1002/cncr.27476. [PubMed].
20. Bruce J, Thornton AJ, Powell R, Johnston M, Wells M, Heys SD, Thompson AM, Smith CW, Chambers AW, Scott NW, and Recovery Study Group. Psychological, surgical, and sociodemographic predictors of pain outcomes after breast cancer surgery: a population-based cohort study. Pain. 2014; 155:232–43. https://doi.org/10.1016/j.pain.2013.09.028. [PubMed].
21. Singh C, De Vera M, Campbell KL. The effect of prospective monitoring and early physiotherapy intervention on arm morbidity following surgery for breast cancer: a pilot study. Physiother Can. 2013; 65:183–91. https://doi.org/10.3138/ptc.2012-23O. [PubMed].
22. Bulley C, Coutts F, Blyth C, Jack W, Chetty U, Barber M, Tan CW. A Morbidity Screening Tool for identifying fatigue, pain, upper limb dysfunction and lymphedema after breast cancer treatment: a validity study. Eur J Oncol Nurs. 2014; 18:218–27. https://doi.org/10.1016/j.ejon.2013.10.006. [PubMed].
23. Miaskowski C, Paul SM, Cooper B, West C, Levine JD, Elboim C, Hamolsky D, Abrams G, Luce J, Dhruva A, Langford DJ, Merriman JD, Kober K, et al. Identification of patient subgroups and risk factors for persistent arm/shoulder pain following breast cancer surgery. Eur J Oncol Nurs. 2014; 18:242–53. https://doi.org/10.1016/j.ejon.2013.12.002. [PubMed].
24. Hamood R, Hamood H, Merhasin I, Keinan-Boker L. Chronic pain and other symptoms among breast cancer survivors: prevalence, predictors, and effects on quality of life. Breast Cancer Res Treat. 2018; 167:157–69. https://doi.org/10.1007/s10549-017-4485-0. [PubMed].
25. Wang L, Guyatt GH, Kennedy SA, Romerosa B, Kwon HY, Kaushal A, Chang Y, Craigie S, de Almeida CPB, Couban RJ, Parascandalo SR, Izhar Z, Reid S, et al. Predictors of persistent pain after breast cancer surgery: a systematic review and meta-analysis of observational studies. CMAJ. 2016; 188:E352–61. https://doi.org/10.1503/cmaj.151276. [PubMed].
26. Poleshuck EL, Katz J, Andrus CH, Hogan LA, Jung BF, Kulick DI, Dworkin RH. Risk factors for chronic pain following breast cancer surgery: a prospective study. J Pain. 2006; 7:626–34. https://doi.org/10.1016/j.jpain.2006.02.007. [PubMed].
27. Mejdahl MK, Andersen KG, Gärtner R, Kroman N, Kehlet H. Persistent pain and sensory disturbances after treatment for breast cancer: six year nationwide follow-up study. BMJ. 2013; 346:f1865. https://doi.org/10.1136/bmj.f1865. [PubMed].
28. Kaur N, Kumar A, Saxena AK, Gupta A, Grover RK. Postmastectomy chronic pain in breast cancer survivors: An exploratory study on prevalence, characteristics, risk factors, and impact on quality of life. Indian J Surg. 2018; 80:592–98. https://doi.org/10.1007/s12262-017-1663-6.
29. Meijuan Y, Zhiyou P, Yuwen T, Ying F, Xinzhong C. A retrospective study of postmastectomy pain syndrome: incidence, characteristics, risk factors, and influence on quality of life. ScientificWorldJournal. 2013; 2013:159732. https://doi.org/10.1155/2013/159732. [PubMed].
30. Lee E, Takita C, Wright JL, Reis IM, Zhao W, Nelson OL, Hu JJ. Characterization of risk factors for adjuvant radiotherapy-associated pain in a tri-racial/ethnic breast cancer population. Pain. 2016; 157:1122–31. https://doi.org/10.1097/j.pain.0000000000000489. [PubMed].
31. Lundstedt D, Gustafsson M, Steineck G, Malmström P, Alsadius D, Sundberg A, Wilderäng U, Holmberg E, Johansson KA, Karlsson P. Risk factors of developing long-lasting breast pain after breast cancer radiotherapy. Int J Radiat Oncol Biol Phys. 2012; 83:71–78. https://doi.org/10.1016/j.ijrobp.2011.05.065. [PubMed].
32. Zararli O, Karaman N, Özaslan C, Hüseyinova S, Altinok M. Long-term complications associated with mastectomy and axillary dissection. 2009. https://explore.openaire.eu/search/publication?articleId=tubitakulakb::9529498bf60179959710dd5298c5bbca.
33. Khan F, Amatya B, Pallant JF, Rajapaksa I. Factors associated with long-term functional outcomes and psychological sequelae in women after breast cancer. Breast. 2012; 21:314–20. https://doi.org/10.1016/j.breast.2012.01.013. [PubMed].
34. Dantas de Oliveira NP, Guedes TS, Holanda AM, Reis MA, da Silva CP, Rocha e Silva BL, Maia de Almeida GC, de Souza DL. Functional Disability in Women Submitted to Breast Cancer Treatment. Asian Pac J Cancer Prev. 2017; 18:1207–14. https://doi.org/10.22034/APJCP.2017.18.5.1207. [PubMed].
35. Meeske KA, Sullivan-Halley J, Smith AW, McTiernan A, Baumgartner KB, Harlan LC, Bernstein L. Risk factors for arm lymphedema following breast cancer diagnosis in Black women and White women. Breast Cancer Res Treat. 2009; 113:383–91. https://doi.org/10.1007/s10549-008-9940-5. [PubMed].
36. Gärtner R, Jensen MB, Kronborg L, Ewertz M, Kehlet H, Kroman N. Self-reported arm-lymphedema and functional impairment after breast cancer treatment--a nationwide study of prevalence and associated factors. Breast. 2010; 19:506–15. https://doi.org/10.1016/j.breast.2010.05.015. [PubMed].
37. Ashikaga T, Krag DN, Land SR, Julian TB, Anderson SJ, Brown AM, Skelly JM, Harlow SP, Weaver DL, Mamounas EP, Costantino JP, Wolmark N, and National Surgical Adjuvant Breast, Bowel Project. Morbidity results from the NSABP B-32 trial comparing sentinel lymph node dissection versus axillary dissection. J Surg Oncol. 2010; 102:111–18. https://doi.org/10.1002/jso.21535. [PubMed].
38. O’Toole J, Miller CL, Specht MC, Skolny MN, Jammallo LS, Horick N, Elliott K, Niemierko A, Taghian AG. Cording following treatment for breast cancer. Breast Cancer Res Treat. 2013; 140:105–11. https://doi.org/10.1007/s10549-013-2616-9. [PubMed].
39. Hayes SC, Rye S, Battistutta D, DiSipio T, Newman B. Upper-body morbidity following breast cancer treatment is common, may persist longer-term and adversely influences quality of life. Health Qual Life Outcomes. 2010; 8:92. https://doi.org/10.1186/1477-7525-8-92. [PubMed].
40. Levy EW, Pfalzer LA, Danoff J, Springer BA, McGarvey C, Shieh CY, Morehead-Gee A, Gerber LH, Stout NL. Predictors of functional shoulder recovery at 1 and 12 months after breast cancer surgery. Breast Cancer Res Treat. 2012; 134:315–24. https://doi.org/10.1007/s10549-012-2061-1. [PubMed].
41. Mak SS, Yeo W, Lee YM, Tse SM, Ho FP, Zee B, Chan E. Risk factors for the initiation and aggravation of lymphoedema after axillary lymph node dissection for breast cancer. Hong Kong Med J. 2009; 15:8–12. [PubMed].
42. Bevilacqua JL, Kattan MW, Changhong Y, Koifman S, Mattos IE, Koifman RJ, Bergmann A. Nomograms for predicting the risk of arm lymphedema after axillary dissection in breast cancer. Ann Surg Oncol. 2012; 19:2580–89. https://doi.org/10.1245/s10434-012-2290-x. [PubMed].
43. Herremans KM, Cribbin MP, Riner AN, Neal DW, Hollen TL, Clevenger P, Munoz D, Blewett S, Giap F, Okunieff PG, Mendenhall NP, Bradley JA, Mendenhall WM, et al. Five-Year Breast Surgeon Experience in LYMPHA at Time of ALND for Treatment of Clinical T1-4N1-3M0 Breast Cancer. Ann Surg Oncol. 2021; 28:5775–87. https://doi.org/10.1245/s10434-021-10551-8. [PubMed].
44. Sipilä R, Estlander AM, Tasmuth T, Kataja M, Kalso E. Development of a screening instrument for risk factors of persistent pain after breast cancer surgery. Br J Cancer. 2012; 107:1459–66. https://doi.org/10.1038/bjc.2012.445. [PubMed].
45. Woo KJ, Lee KT, Mun GH, Pyon JK, Bang SI. Effect of breast reconstruction modality on the development of postmastectomy shoulder morbidity. J Plast Reconstr Aesthet Surg. 2018; 71:1761–67. https://doi.org/10.1016/j.bjps.2018.07.033. [PubMed].
46. Gillespie TC, Sayegh HE, Brunelle CL, Daniell KM, Taghian AG. Breast cancer-related lymphedema: risk factors, precautionary measures, and treatments. Gland Surg. 2018; 7:379–403. https://doi.org/10.21037/gs.2017.11.04. [PubMed].
47. Zou L, Liu FH, Shen PP, Hu Y, Liu XQ, Xu YY, Pen QL, Wang B, Zhu YQ, Tian Y. The incidence and risk factors of related lymphedema for breast cancer survivors post-operation: a 2-year follow-up prospective cohort study. Breast Cancer. 2018; 25:309–14. https://doi.org/10.1007/s12282-018-0830-3. [PubMed].
48. Nesvold IL, Dahl AA, Løkkevik E, Marit Mengshoel A, Fosså SD. Arm and shoulder morbidity in breast cancer patients after breast-conserving therapy versus mastectomy. Acta Oncol. 2008; 47:835–42. https://doi.org/10.1080/02841860801961257. [PubMed].
49. Kwan ML, Darbinian J, Schmitz KH, Citron R, Partee P, Kutner SE, Kushi LH. Risk factors for lymphedema in a prospective breast cancer survivorship study: the Pathways Study. Arch Surg. 2010; 145:1055–63. https://doi.org/10.1001/archsurg.2010.231. [PubMed].
50. Shahpar H, Atieh A, Maryam A, Fatemeh HS, Massoome N, Mandana E, Masud Y, Hamid Reza M, Mohammad Esmaeil A. Risk factors of lymph edema in breast cancer patients. Int J Breast Cancer. 2013; 2013:641818. https://doi.org/10.1155/2013/641818. [PubMed].
51. Deutsch M, Land S, Begovic M, Sharif S. The incidence of arm edema in women with breast cancer randomized on the National Surgical Adjuvant Breast and Bowel Project study B-04 to radical mastectomy versus total mastectomy and radiotherapy versus total mastectomy alone. Int J Radiat Oncol Biol Phys. 2008; 70:1020–24. https://doi.org/10.1016/j.ijrobp.2007.07.2376. [PubMed].
52. McLaughlin SA, Wright MJ, Morris KT, Giron GL, Sampson MR, Brockway JP, Hurley KE, Riedel ER, Van Zee KJ. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: objective measurements. J Clin Oncol. 2008; 26:5213–19. https://doi.org/10.1200/JCO.2008.16.3725. [PubMed].
53. Kilbreath SL, Refshauge KM, Beith JM, Ward LC, Ung OA, Dylke ES, French JR, Yee J, Koelmeyer L, Gaitatzis K. Risk factors for lymphoedema in women with breast cancer: A large prospective cohort. Breast. 2016; 28:29–36. https://doi.org/10.1016/j.breast.2016.04.011. [PubMed].
54. Petrek JA, Senie RT, Peters M, Rosen PP. Lymphedema in a cohort of breast carcinoma survivors 20 years after diagnosis. Cancer. 2001; 92:1368–77. https://doi.org/10.1002/1097-0142(20010915)92:6<1368::aid-cncr1459>3.0.co;2-9. [PubMed].
55. Das N, Baumgartner RN, Riley EC, Pinkston CM, Yang D, Baumgartner KB. Treatment-related risk factors for arm lymphedema among long-term breast cancer survivors. J Cancer Surviv. 2015; 9:422–30. https://doi.org/10.1007/s11764-014-0416-9. [PubMed].
56. McCredie MR, Dite GS, Porter L, Maskiell J, Giles GG, Phillips KA, Redman S, Hopper JL. Prevalence of self-reported arm morbidity following treatment for breast cancer in the Australian Breast Cancer Family Study. Breast. 2001; 10:515–22. https://doi.org/10.1054/brst.2000.0291. [PubMed].
57. Box RC, Reul-Hirche HM, Bullock-Saxton JE, Furnival CM. Physiotherapy after breast cancer surgery: results of a randomised controlled study to minimise lymphoedema. Breast Cancer Res Treat. 2002; 75:51–64. https://doi.org/10.1023/a:1016591121762. [PubMed].
58. Crosby MA, Card A, Liu J, Lindstrom WA, Chang DW. Immediate breast reconstruction and lymphedema incidence. Plast Reconstr Surg. 2012; 129:789e–95e. https://doi.org/10.1097/PRS.0b013e31824a2ab1. [PubMed].
59. Hack TF, Kwan WB, Thomas-Maclean RL, Towers A, Miedema B, Tilley A, Chateau D. Predictors of arm morbidity following breast cancer surgery. Psychooncology. 2010; 19:1205–12. https://doi.org/10.1002/pon.1685. [PubMed].
60. Basu A, Mondal J, Swetha B, Chakrabarty S, Ghosh D, Gangopadhyay S, Mandel B. Patient-reported shoulder morbidity and fatigue among breast cancer survivors: An insight from a tertiary care cancer hospital. Indian J Med Paediatr Oncol. 2020; 41:825–31. https://doi.org/10.4103/ijmpo.ijmpo_257_20.
61. Dominick SA, Madlensky L, Natarajan L, Pierce JP. Risk factors associated with breast cancer-related lymphedema in the WHEL Study. J Cancer Surviv. 2013; 7:115–23. https://doi.org/10.1007/s11764-012-0251-9. [PubMed].
62. Ugur S, Arıcı C, Yaprak M, Mescı A, Arıcı GA, Dolay K, Ozmen V. Risk factors of breast cancer-related lymphedema. Lymphat Res Biol. 2013; 11:72–75. https://doi.org/10.1089/lrb.2013.0004. [PubMed].
63. Park JH, Lee WH, Chung HS. Incidence and risk factors of breast cancer lymphoedema. J Clin Nurs. 2008; 17:1450–59. https://doi.org/10.1111/j.1365-2702.2007.02187.x. [PubMed].
64. Clark B, Sitzia J, Harlow W. Incidence and risk of arm oedema following treatment for breast cancer: a three-year follow-up study. QJM. 2005; 98:343–48. https://doi.org/10.1093/qjmed/hci053. [PubMed].
65. Leysen L, Beckwée D, Nijs J, Pas R, Bilterys T, Vermeir S, Adriaenssens N. Risk factors of pain in breast cancer survivors: a systematic review and meta-analysis. Support Care Cancer. 2017; 25:3607–43. https://doi.org/10.1007/s00520-017-3824-3. [PubMed].
66. Lang AE, Murphy M, Dickerson CR, Stavness I, Kim SY. Shoulder dysfunction in breast cancer survivors: Can treatment type or musculoskeletal factors identify those at higher risk? Rehabil Oncol. 2021; 39:143–51. https://doi.org/10.1097/01.REO.0000000000000224.
67. Klein I, Kalichman L, Chen N, Susmallian S. A comprehensive approach to risk factors for upper arm morbidities following breast cancer treatment: a prospective study. BMC Cancer. 2021; 21:1251. https://doi.org/10.1186/s12885-021-08891-5. [PubMed].
68. Kikuuchi M, Akezaki Y, Nakata E, Yamashita N, Tominaga R, Kurokawa H, Hamada M, Aogi K, Ohsumi S, Tsuji T, Sugihara S. Risk factors of impairment of shoulder function after axillary dissection for breast cancer. Support Care Cancer. 2021; 29:771–78. https://doi.org/10.1007/s00520-020-05533-7. [PubMed].
69. Pereira S, Fontes F, Sonin T, Dias T, Fragoso M, Castro-Lopes J, Lunet N. Neuropathic Pain After Breast Cancer Treatment: Characterization and Risk Factors. J Pain Symptom Manage. 2017; 54:877–88. https://doi.org/10.1016/j.jpainsymman.2017.04.011. [PubMed].
70. Albert US, Koller M, Kopp I, Lorenz W, Schulz KD, Wagner U. Early self-reported impairments in arm functioning of primary breast cancer patients predict late side effects of axillary lymph node dissection: results from a population-based cohort study. Breast Cancer Res Treat. 2006; 100:285–92. https://doi.org/10.1007/s10549-006-9247-3. [PubMed].
71. Ahmed RL, Schmitz KH, Prizment AE, Folsom AR. Risk factors for lymphedema in breast cancer survivors, the Iowa Women’s Health Study. Breast Cancer Res Treat. 2011; 130:981–91. https://doi.org/10.1007/s10549-011-1667-z. [PubMed].
72. Moloney N, Sung JM, Kilbreath S, Dylke E. Prevalence and risk factors associated with pain 21 months following surgery for breast cancer. Support Care Cancer. 2016; 24:4533–39. https://doi.org/10.1007/s00520-016-3292-1. [PubMed].
73. Kramer N, Ramjith J, Shamley D. Prevalence of shoulder morbidity after treatment for breast Cancer in South Africa. Support Care Cancer. 2019; 27:2591–98. https://doi.org/10.1007/s00520-018-4540-3. [PubMed].
74. Chiang DLC, Rice DA, Helsby NA, Somogyi AA, Kluger MT. The Prevalence, Impact, and Risk Factors for Persistent Pain After Breast Cancer Surgery in a New Zealand Population. Pain Med. 2019; 20:1803–14. https://doi.org/10.1093/pm/pnz049. [PubMed].
75. Wong CJ, Tay MRJ, Aw HZ. Prevalence and Risk Factors of Adhesive Capsulitis in Asian Breast Cancer Patients Undergoing an Outpatient Community Cancer Rehabilitation Program. Arch Phys Med Rehabil. 2021; 102:843–48. https://doi.org/10.1016/j.apmr.2020.10.105. [PubMed].
76. Hidding JT, Beurskens CH, van der Wees PJ, van Laarhoven HW, Nijhuis-van der Sanden MW. Treatment related impairments in arm and shoulder in patients with breast cancer: a systematic review. PLoS One. 2014; 9:e96748. https://doi.org/10.1371/journal.pone.0096748. [PubMed].
77. Freitas-Silva R, Conde DM, de Freitas-Júnior R, Martinez EZ. Comparison of quality of life, satisfaction with surgery and shoulder-arm morbidity in breast cancer survivors submitted to breast-conserving therapy or mastectomy followed by immediate breast reconstruction. Clinics (Sao Paulo). 2010; 65:781–87. https://doi.org/10.1590/s1807-59322010000800007. [PubMed].
78. Owusu Sekyere M, Basson P, Uys C, Armer JM. Incidence of and risk factors for arm lymphoedema following breast cancer treatment: A study in ghana. J Lymphoedema. 2019; 14:41–45.
79. Kim M, Kim SW, Lee SU, Lee NK, Jung SY, Kim TH, Lee ES, Kang HS, Shin KH. A model to estimate the risk of breast cancer-related lymphedema: combinations of treatment-related factors of the number of dissected axillary nodes, adjuvant chemotherapy, and radiation therapy. Int J Radiat Oncol Biol Phys. 2013; 86:498–503. https://doi.org/10.1016/j.ijrobp.2013.02.018. [PubMed].
80. Rebegea L, Firescu D, Dumitru M, Anghel R. The incidence and risk factors for occurrence of arm lymphedema after treatment of breast cancer. Chirurgia (Bucur). 2015; 110:33–37. [PubMed].
81. Langer I, Guller U, Berclaz G, Koechli OR, Schaer G, Fehr MK, Hess T, Oertli D, Bronz L, Schnarwyler B, Wight E, Uehlinger U, Infanger E, et al. Morbidity of sentinel lymph node biopsy (SLN) alone versus SLN and completion axillary lymph node dissection after breast cancer surgery: a prospective Swiss multicenter study on 659 patients. Ann Surg. 2007; 245:452–61. https://doi.org/10.1097/01.sla.0000245472.47748.ec. [PubMed].
82. Del Bianco P, Zavagno G, Burelli P, Scalco G, Barutta L, Carraro P, Pietrarota P, Meneghini G, Morbin T, Tacchetti G, Pecoraro P, Belardinelli V, De Salvo GL, and GIVOM. Morbidity comparison of sentinel lymph node biopsy versus conventional axillary lymph node dissection for breast cancer patients: results of the sentinella-GIVOM Italian randomised clinical trial. Eur J Surg Oncol. 2008; 34:508–13. https://doi.org/10.1016/j.ejso.2007.05.017. [PubMed].
83. Sagen A, Kaaresen R, Sandvik L, Thune I, Risberg MA. Upper limb physical function and adverse effects after breast cancer surgery: a prospective 2.5-year follow-up study and preoperative measures. Arch Phys Med Rehabil. 2014; 95:875–81. https://doi.org/10.1016/j.apmr.2013.12.015. [PubMed].
84. Kwan W, Jackson J, Weir LM, Dingee C, McGregor G, Olivotto IA. Chronic arm morbidity after curative breast cancer treatment: prevalence and impact on quality of life. J Clin Oncol. 2002; 20:4242–48. https://doi.org/10.1200/JCO.2002.09.018. [PubMed].
85. Adriaenssens N, Vinh-Hung V, Miedema G, Versmessen H, Lamote J, Vanhoeij M, Lievens P, van Parijs H, Storme G, Voordeckers M, De Ridder M. Early contralateral shoulder-arm morbidity in breast cancer patients enrolled in a randomized trial of post-surgery radiation therapy. Breast Cancer (Auckl). 2012; 6:79–93. https://doi.org/10.4137/BCBCR.S9362. [PubMed].
86. Blanchard DK, Donohue JH, Reynolds C, Grant CS. Relapse and morbidity in patients undergoing sentinel lymph node biopsy alone or with axillary dissection for breast cancer. Arch Surg. 2003; 138:482–88. https://doi.org/10.1001/archsurg.138.5.482. [PubMed].
87. Belmonte R, Messaggi-Sartor M, Ferrer M, Pont A, Escalada F. Prospective study of shoulder strength, shoulder range of motion, and lymphedema in breast cancer patients from pre-surgery to 5 years after ALND or SLNB. Support Care Cancer. 2018; 26:3277–87. https://doi.org/10.1007/s00520-018-4186-1. [PubMed].
88. Sueangamiam K, Rongsriyam K. The prevalence of arm lymphedema after radiation treatment in patients with breast cancer. J Radiother Pract. 2023; 22:E7. https://doi.org/10.1017/S1460396921000418.
89. Yen TW, Fan X, Sparapani R, Laud PW, Walker AP, Nattinger AB. A contemporary, population-based study of lymphedema risk factors in older women with breast cancer. Ann Surg Oncol. 2009; 16:979–88. https://doi.org/10.1245/s10434-009-0347-2. [PubMed].
90. Nelson JA, Lee IT, Disa JJ. The Functional Impact of Breast Reconstruction: An Overview and Update. Plast Reconstr Surg Glob Open. 2018; 6:e1640. https://doi.org/10.1097/GOX.0000000000001640. [PubMed].
91. Siotos C, Sebai ME, Wan EL, Bello RJ, Habibi M, Cooney DS, Manahan MA, Cooney CM, Seal SM, Rosson GD. Breast reconstruction and risk of arm lymphedema development: A meta-analysis. J Plast Reconstr Aesthet Surg. 2018; 71:807–18. https://doi.org/10.1016/j.bjps.2018.01.012. [PubMed].
92. Habib AS, Kertai MD, Cooter M, Greenup RA, Hwang S. Risk factors for severe acute pain and persistent pain after surgery for breast cancer: a prospective observational study. Reg Anesth Pain Med. 2019; 44:192–99. https://doi.org/10.1136/rapm-2018-000040. [PubMed].
93. Akbas A, Dagmura H, Daldal E, Dasiran FM, Deveci H, Okan I. Association between Shoulder Range of Motion and Pain Catastrophizing Scale in Breast Cancer Patients after Surgery. Breast Care (Basel). 2021; 16:66–71. https://doi.org/10.1159/000506922. [PubMed].
94. Koehler LA, Hunter DW, Blaes AH, Haddad TC. Function, Shoulder Motion, Pain, and Lymphedema in Breast Cancer With and Without Axillary Web Syndrome: An 18-Month Follow-Up. Phys Ther. 2018; 98:518–27. https://doi.org/10.1093/ptj/pzy010. [PubMed].
95. Kibar S, Dalyan Aras M, Ünsal Delialioğlu S. The risk factors and prevalence of upper extremity impairments and an analysis of effects of lymphoedema and other impairments on the quality of life of breast cancer patients. Eur J Cancer Care (Engl). 2017; 26. https://doi.org/10.1111/ecc.12433. [PubMed].
96. Iyigun ZE, Duymaz T, Ilgun AS, Alco G, Ordu C, Sarsenov D, Aydin AE, Celebi FE, Izci F, Eralp Y, Ozmen V. Preoperative Lymphedema-Related Risk Factors in Early-Stage Breast Cancer. Lymphat Res Biol. 2018; 16:28–35. https://doi.org/10.1089/lrb.2016.0045. [PubMed].
97. Andersen KG, Kehlet H. Persistent pain after breast cancer treatment: a critical review of risk factors and strategies for prevention. J Pain. 2011; 12:725–46. https://doi.org/10.1016/j.jpain.2010.12.005. [PubMed].
98. Ozcinar B, Guler SA, Kocaman N, Ozkan M, Gulluoglu BM, Ozmen V. Breast cancer related lymphedema in patients with different loco-regional treatments. Breast. 2012; 21:361–65. https://doi.org/10.1016/j.breast.2012.03.002. [PubMed].
99. Rupp J, Hadamitzky C, Henkenberens C, Christiansen H, Steinmann D, Bruns F. Frequency and risk factors for arm lymphedema after multimodal breast-conserving treatment of nodal positive breast Cancer - a long-term observation. Radiat Oncol. 2019; 14:39. https://doi.org/10.1186/s13014-019-1243-y. [PubMed].
100. Swaroop MN, Ferguson CM, Horick NK, Skolny MN, Miller CL, Jammallo LS, Brunelle CL, O’Toole JA, Isakoff SJ, Specht MC, Taghian AG. Impact of adjuvant taxane-based chemotherapy on development of breast cancer-related lymphedema: results from a large prospective cohort. Breast Cancer Res Treat. 2015; 151:393–403. https://doi.org/10.1007/s10549-015-3408-1. [PubMed].
101. DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013; 14:500–15. https://doi.org/10.1016/S1470-2045(13)70076-7. [PubMed].
102. Moher D, Liberati A, Tetzlaff J, Altman DG, and PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009; 151:264–69. https://doi.org/10.7326/0003-4819-151-4-200908180-00135. [PubMed].
103. Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg. 2011; 128:305–10. https://doi.org/10.1097/PRS.0b013e318219c171. [PubMed].
104. Smoot B, Paul SM, Aouizerat BE, Dunn L, Elboim C, Schmidt B, Hamolsky D, Levine JD, Abrams G, Mastick J, Topp K, Miaskowski C. Predictors of Altered Upper Extremity Function During the First Year After Breast Cancer Treatment. Am J Phys Med Rehabil. 2016; 95:639–55. https://doi.org/10.1097/PHM.0000000000000455. [PubMed].
105. Norman SA, Localio AR, Potashnik SL, Simoes Torpey HA, Kallan MJ, Weber AL, Miller LT, Demichele A, Solin LJ. Lymphedema in breast cancer survivors: incidence, degree, time course, treatment, and symptoms. J Clin Oncol. 2009; 27:390–97. https://doi.org/10.1200/JCO.2008.17.9291. [PubMed].