
Introduction
Metanephric adenoma (MA) is a rare benign tumor of the kidney, accounting for 0.2% of adult renal epithelial neoplasms [1]. The tumor, which is composed of primitive metanephric cells [2], is often asymptomatic. Some authors have suggested that MA may derive from maturing nephroblastomas (Wilms tumor), since immunophenotypic findings overlap closely with those of differentiated nephroblastoma and nephrogenic rests [3]. Though it may also occur in children, it is detected mainly in adults aged between 50 and 70 and is more common (ratio 2:1) in women [2, 4, 5]. Radical nephrectomy, cryoablation and radiofrequency have been used to treat this neoplasm [5].
While the clinical course is benign, histological findings often overlap with those of malignant tumors including Wilms tumor and renal papillary neoplasms, thus prompting the need for differential diagnosis [6]. A better understanding of this benign tumor would undoubtedly aid the development of less invasive strategies. Although most authors rule out the possibility of MA becoming malignant, one case has been reported of a metanephric adenoma in association with a high-grade sarcoma (metanephric adenosarcoma) [5, 7].
Immunohistochemical analysis is a useful tool for differential diagnosis. The literature contains few reports of integrated diagnosis of MA using molecular techniques [8].
Mutation of the BRAF gene prompts constitutive activation of the ERK-mediated signaling pathway, favoring cell proliferation and differentiation.
Activation of RAF, in both its homodimer and heterodimer forms, triggers the phosphorylation of MAPK kinase (MEK), which in turns prompts the phosphorylation of extracellular signal-regulated kinase (ERK); ERK activation promotes cell proliferation and signal transformation through interaction with several molecules crucial to tumor pathogenesis [9, 10].
The specific BRAF gene mutation V600E has been reported in over half of all cutaneous melanomas and papillary thyroid carcinomas, as well as in a number of blood cancers including hairy cell leukemia; it is also present in indolent and benign tumors such as melanocytic nevus [11]. This specific mutation has also been studied in malignant neoplasms such as renal cell carcinoma in response to targeted therapies [12]. In benign neoplasms like MA, several authors have noted that testing for the BRAF V600E mutation may be a valuable tool for the diagnosis [1, 2, 11].
Results
Gross examination revealed well-circumscribed, non-encapsulated tumors measuring between 1.5 and 6 cm (mean 3.7 cm), with focal areas of blood-containing cysts and solid, in some cases presenting calcifications. Histologically, MAs were composed of small, monomorphic epithelial cells displaying no significant atypia or mitotic figures, showing papillary or acinar patterns, and edematous or hyalinized stroma with calcification (psammoma bodies) (Figure 1A). Immunohistochemical examination showed positive staining for WT1 and vimentin, and negative staining for racemase, CK7, CD10, CD57 and RCC (Figure 1B). Mutation analysis by real-time PCR revealed the BRAF gene mutation V600E in three cases and wild-type BRAF in the fourth. Based on morphological features and the findings of immunohistochemical and molecular analysis, all four cases were diagnosed as MA. Three of the patients are alive and well 12, 5 and 2 years after surgery, while the fourth died 13 years after the procedure due to other causes.
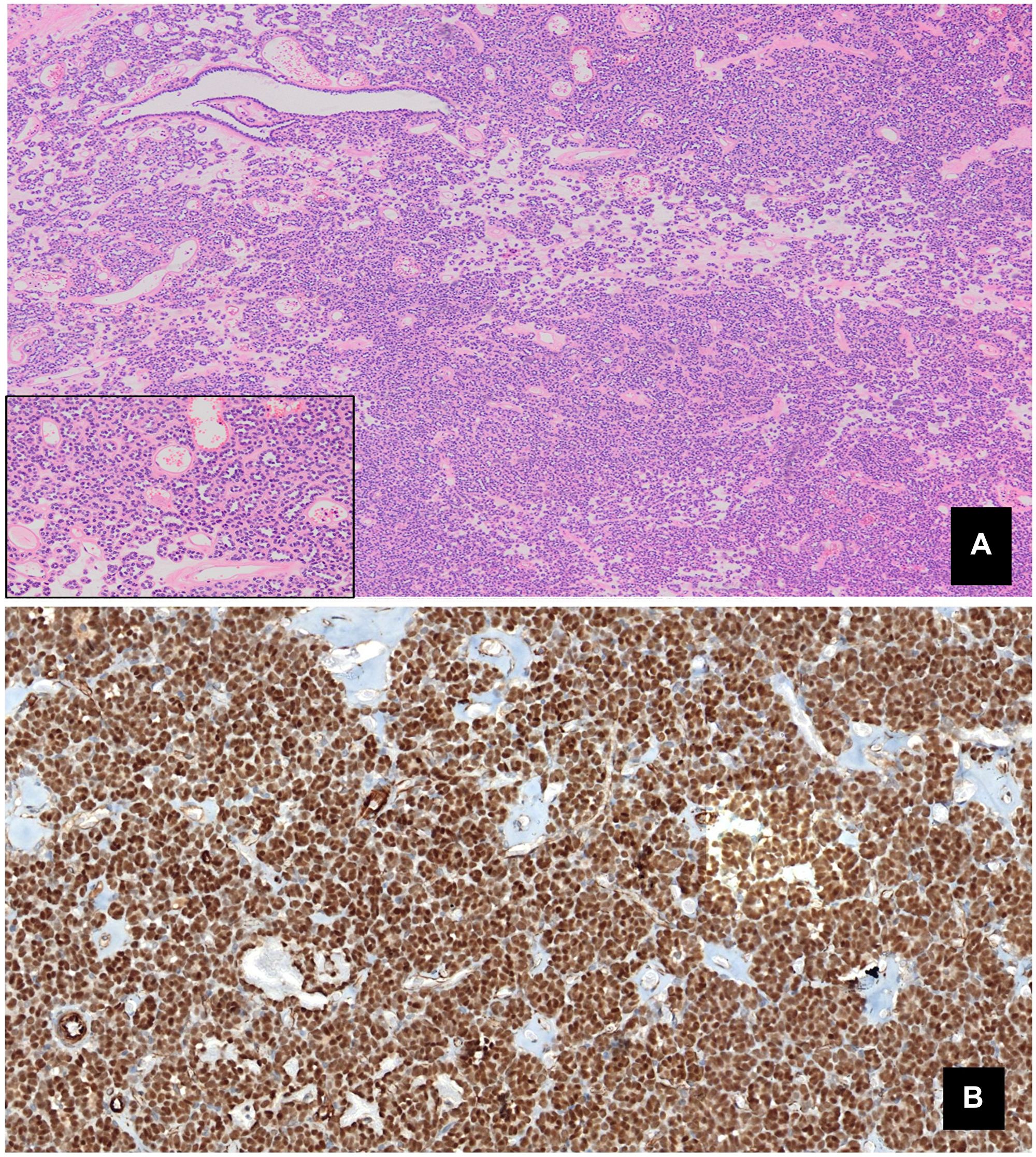
Figure 1: (A) Monomorphic epithelial proliferation, displaying no significant atypia or mitotic figures, within an edematous stroma containing psammoma bodies (Panoramic view. HE). (B) Intense positive nuclear staining for WT1.
DISCUSSION
MA is an uncommon, benign tumor of the kidney composed of spindle cells associated with epithelial cells. In 1988, Mostofi et al. [13] described MA for the first time as a distinct nosologic entity among renal neoplasms, with tubular-like epithelial cells. This tumor is currently classified among the metanephric neoplasms, which also include metanephric adenoma and metanephric stromal tumour [4]. MA, which accounts for 0.2–0.7% of adult renal epithelial neoplasms, derives from remnants of embryonic renal tissue [1, 3, 4].
At gross examination, MA appears as a well-circumscribed neoplasm with a yellowish surface, often displaying evidence of secondary changes including focal necrosis, hemorrhage and/or cystic degeneration. Coarse calcification may also be present. The tumor mass generally ranges in size between 3 and 6 cm in diameter, although tumors of up to 15 cm have been reported [4]. Histologically, it comprises an acinar arrangement of small cells. Differential diagnosis of MA includes Wilms tumor, nephrogenic rests and renal papillary neoplasms [5]. MA typically expresses WT1 and CD57, but stains negative for CK7 and racemase. Positive intense staining for WT1 was recorded in the four cases reported here, but CD57 staining was in most of them weak; so, BRAF mutation helped us to confirm the diagnosis of MA.
Oncogenic BRAF normally regulates cell division and differentiation through the MAP kinase signaling pathway. BRAF mutations, identified in several solid tumors and blood cancers, prompt the constitutive activation of the pathway, which has been widely documented in melanomas [9, 10, 14]. Most BRAF mutations involve a thymine-adenine transversion, leading to the substitution of valine by glutamic acid at codon V600 (V600E) [14].
Most reported MAs display a normal genotype, lacking the simultaneous chromosomes 7 and 17 gain and Y chromosome loss characteristic of papillary renal cell carcinoma and common in neuroblastoma.
The BRAF gene mutation V600E is reported in roughly 90% of metanephric adenomas [2, 4, 11, 15], with only 2 described cases of V600D mutation [2] and 1 of V600K [16]. Caliò [14] et al. identified the V600E mutation in 41 out of 48 MA patients (85%) with a mean age of 54, while Choueiri et al. [11] reported it in 26/29 patients (89%) also with a mean age of 54, and Ding et al. [17] described 27 MA patients with mean age of 39 years and 22 (81%) with BRAF mutation. Other authors have reported the V600E mutation in smaller series [18–21]. In our research, as shown in Table 1, the mutation was identified in three of the four patients studied (75%), aged between 19 and 65 (mean 47.5).
Table 1: BRAF mutations in metanephric adenomas: literature review
| Research and year | Number of cases | Mean age (year, range) | Gender | Tumor size (cm, range) | BRAF mutation | Type of mutation |
|---|---|---|---|---|---|---|
| Previous reports in Caliò et al., 2016 | 99 | 52 (5–84) | 71F 28M | 3.4 (1.1–8) | 87 (88%) | V600E (97) V600D (2) |
| Ding et al., 2018 | 27 | 39 (12–80) | 9F 18M | 3.1 (2–7) | 22 (81%) | V600E |
| Wobker et al., 2019 | 10 | 42 (10–62) | 6F 4M | 2.7 (1.3–3.5) | 8 (80%) | V600E |
| Catic et al., 2020 | 28 | 52 (9–73) | 17F 10M | 3 (0.5–12) | 15 (53%) | V600E |
| Chan et al., 2020 | 12 | 54 (38–76) | 11F 1M | 2.9 (1–6) | 12 (100%) | V600E |
| Lenci et al., 2021 | 1 | 73 | F | 3.2 | 1 (100%) | V600K |
| Current study | 4 | 54 (19–65) | 1F 3M | 3,7 (1.5–6) | 3 (75%) | V600E |
Several authors have drawn attention to the relationship between wild-type BRAF and MA in younger adults (i.e., under 25). Of the 29 cases reported by Choueri [11] et al., all three patients harboring wild-type BRAF were well below the mean age. By contrast, in the four pediatric cases of MA described by Chami et al. [22], only one harbored wild-type BRAF. An epidemiological analysis was carried out of the published cases of MA in which the BRAF mutation has been studied. In Table 2 it can be observed that, although the age range of presentation is similar in both groups, the mean age is 19.6 years lower in the wild-type BRAF patients (31.1 vs. 50.7). The present study detected the BRAF gene mutation V600E in patients aged between 50 and 65, while the youngest patient (aged 19) harbored wild-type BRAF.
Table 2: Comparison of age and gender incidence in mutated BRAF and wild type BRAF metanephric adenomas: literature review
| Research and year | Number of MUTATED/WT cases | Mean age MUTATED/WT (years, range) | Gender | |||
|---|---|---|---|---|---|---|
| MUTATED BRAF | WT BRAF | |||||
| Male | Female | Male | Female | |||
| Choueiri et al., 2012 | 26/3 | 54.7 (36−78)/32 (25−38) | 3 (12%) | 23 (88%) | − | 3 (100%) |
| Dadone et al., 2013 | 1/0 | 61/− | − | 1 (100%) | − | |
| Pinto et al., 2015 | 6/0 | 52/− | − | 6 (100%) | − | |
| Udager et al., 2015 | 10/1 | 51.2 (16−84)/32 | 4 (40%) | 6 (60%) | 1 (100%) | − |
| Chami et al., 2015 | 3/1 | 5.6 (4−9)/10 | 2 (67%) | 1 (33%) | 1 (100%) | − |
| Caliò A et al., 2016 | 41/7 | 57 (5−84)/33 (10−74) | 11 (27%) | 30 (73%) | 6 (86%) | 1 (14%) |
| Ding et al., 2018 | 22/5 | 40 (25−73)/29 (12−47) | 17 (77%) | 5 (23%) | 4 (80%) | 1 (20%) |
| Wobker et al., 2019 | 8/2 | 46 (19−62)/26.5 (10−43) | 3 (37%) | 5 (63%) | 1 (50%) | 1 (50%) |
| Catic et al., 2020 | 15/9 | 47 (5−75)/36 (9−71) | 7 (46%) | 8 (54%) | 3 (37%) | 5 (63%) |
| Chan et al., 2020 | 12/0 | 54 (38−76)/− | 1 (8%) | 11 (92%) | − | |
| Lenci et al., 2021 | 1/0 | 73/− | − | 1 (100%) | − | |
| Current study | 3/1 | 57 (50−65)/19 | 2 (67%) | 1 (33%) | 1 (100%) | − |
| 148 (84%)/29 (16%) | 50.7 (4−84)/31.1 (9−74) | 50 (34%) | 98 (66%) | 17 (58%) | 12 (42%) | |
A relationship that has not been previously highlighted is the higher incidence of wild-type BRAF in male patients. As described above, metanephric adenoma is more common in female patients in a 2: 1 ratio, just like in mutated BRAF MA (Table 2). By contrast, in wild-type BRAF MA, the incidence in men is higher than women with a 1.45: 1 ratio. A remarkable case is the series of 48 patients by Calio et al. [14], where the F:M ratio in mutated BRAF is 2.7: 1, while in wild-type BRAF it is 1: 6.
Therefore, mutated BRAF MA are more frequent in elderly patients and women, which is consistent with studies in other pathologies. Even with these results, it is necessary to carry out studies with a greater number of cases in order to ensure it.
Materials and Methods
This paper reports on MA in three men and one woman, aged between 19 and 65 (mean age 47.5); patient data are provided in Table 3. The diagnosis was confirmed and subsequently reviewed following WHO-recommended criteria [4]. In all cases, MA presented as a single, asymptomatic mass discovered incidentally during imaging procedures; CT scan confirmed the presence of a solitary, space-occupying, solid renal tumor. A nephrectomy was performed in all patients.
Table 3: Epidemiological data and BRAF status
| Case | Gender | Age (years) | BRAF status (V600E) |
|---|---|---|---|
| 1 | M | 19 | WT |
| 2 | F | 50 | Mut |
| 3 | M | 56 | Mut |
| 4 | M | 65 | Mut |
Immunohistochemical staining was performed on H&E- stained sections cut from paraffin blocks to assess expression of WT1, vimentin, racemase, CK7, CD10 and RCC. Testing for the BRAF gene mutation V600 was carried out by real-time PCR (Cobas® 4800) using the DNA Sample Preparation Kit and the BRAF Mutation Test (Roche), which detects the BRAF gene mutations V600E, V600K and V600D in formalin-fixed, paraffin-embedded tissue.
Conclusions
These results bear out the findings of previous studies of BRAF gene mutations in MA, showing that molecular mutation analysis may aid diagnosis in cases with atypical histological features, especially in small biopsies when non-surgical treatment is planned.
A highly accurate definitive diagnosis of MA was achieved by combining immunohistochemical and molecular analysis; mutated BRAF MA are more frequent in elderly patients and women. Accurate early diagnosis may help to avoid unnecessary aggressive treatments such as radical nephrectomy.
CONFLICTS OF INTEREST
Authors have no conflicts of interest to declare.
FUNDING
This research did not receive any specific grant from any funding agency in the public, commercial, or not-for -profit sector.
References
1. Sun Z, Kan S, Zhang L, Zhang Y, Jing H, Huang G, Yu Q, Wu J. Immunohistochemical phenotype and molecular pathological characteristics of metanephric adenoma. Int J Clin Exp Pathol. 2015; 8:6031–36. [PubMed].
2. Udager AM, Pan J, Magers MJ, Palapattu GS, Morgan TM, Montgomery JS, Weizer AZ, Hafez KS, Miller DC, Wolf JS Jr, McHugh JB, Chinnaiyan AM, Dhanasekaran SM, Mehra R. Molecular and immunohistochemical characterization reveals novel BRAF mutations in metanephric adenoma. Am J Surg Pathol. 2015; 39:549–57. https://doi.org/10.1097/PAS.0000000000000377. [PubMed].
3. Muir TE, Cheville JC, Lager DJ. Metanephric adenoma, nephrogenic rests, and Wilms’ tumor: a histologic and immunophenotypic comparison. Am J Surg Pathol. 2001; 25:1290–96. https://doi.org/10.1097/00000478-200110000-00010. [PubMed].
4. Moch H, Humphrey PA, Ulbright TM, Reuter VE. WHO Classification of Tumours of the Urinary System and Male Genital Organs. Lyon, France: International Agency for Research on Cancer; 2016.
5. Rodríguez-Zarco E, Vallejo-Benítez A, Farfán-López FJ, Vilches-Arenas Á, Pereira-Gallardo S, Vázquez-Ramírez FJ. [Adenoma metanephric: Report of 2 cases and bibliographic review]. Arch Esp Urol. 2017; 70:792–96. [PubMed].
6. Arroyo MR, Green DM, Perlman EJ, Beckwith JB, Argani P. The spectrum of metanephric adenofibroma and related lesions: clinicopathologic study of 25 cases from the National Wilms Tumor Study Group Pathology Center. Am J Surg Pathol. 2001; 25:433–44. https://doi.org/10.1097/00000478-200104000-00002. [PubMed].
7. Picken MM, Curry JL, Lindgren V, Clark JI, Eble JN. Metanephric adenosarcoma in a young adult: morphologic, immunophenotypic, ultrastructural, and fluorescence in situ hybridization analyses: a case report and review of the literature. Am J Surg Pathol. 2001; 25:1451–57. https://doi.org/10.1097/00000478-200111000-00016. [PubMed].
8. Kinney SN, Eble JN, Hes O, Williamson SR, Grignon DJ, Wang M, Zhang S, Baldrige LA, Martignoni G, Brunelli M, Wang L, Comperat E, Fan R, et al. Metanephric adenoma: the utility of immunohistochemical and cytogenetic analyses in differential diagnosis, including solid variant papillary renal cell carcinoma and epithelial-predominant nephroblastoma. Mod Pathol. 2015; 28:1236–48. https://doi.org/10.1038/modpathol.2015.81. [PubMed].
9. Beeram M, Patnaik A, Rowinsky EK. Raf: a strategic target for therapeutic development against cancer. J Clin Oncol. 2005; 23:6771–90. https://doi.org/10.1200/JCO.2005.08.036. [PubMed].
10. Garnett MJ, Rana S, Paterson H, Barford D, Marais R. Wild-type and mutant B-RAF activate C-RAF through distinct mechanisms involving heterodimerization. Mol Cell. 2005; 20:963–69. https://doi.org/10.1016/j.molcel.2005.10.022. [PubMed].
11. Choueiri TK, Cheville J, Palescandolo E, Fay AP, Kantoff PW, Atkins MB, McKenney JK, Brown V, Lampron ME, Zhou M, Hirsch MS, Signoretti S. BRAF mutations in metanephric adenoma of the kidney. Eur Urol. 2012; 62:917–22. https://doi.org/10.1016/j.eururo.2012.05.051. [PubMed].
12. Banerjee N, Sachdev E, Figlin RA. A Rare Finding of a BRAF Mutation in Renal Cell Carcinoma with Response to BRAF-Directed Targeted Therapy. Cureus. 2016; 8:e449. https://doi.org/10.7759/cureus.449. [PubMed].
13. Mostofi FK, Sesterhenn IA, Davis CJ Jr. Benign tumors of the kidney. Prog Clin Biol Res. 1988; 269:329–46. [PubMed].
14. Caliò A, Eble JN, Hes O, Martignoni G, Harari SE, Williamson SR, Brunelli M, Osunkoya AO, Wang L, Comperat E, Lopez-Beltran A, Wang M, Zhang S, et al. Distinct clinicopathological features in metanephric adenoma harboring BRAF mutation. Oncotarget. 2016; 8:54096–105. https://doi.org/10.18632/oncotarget.11117. [PubMed].
15. Pinto A, Signoretti S, Hirsch MS, Barletta JA. Immunohistochemical staining for BRAF V600E supports the diagnosis of metanephric adenoma. Histopathology. 2015; 66:901–04. https://doi.org/10.1111/his.12509. [PubMed].
16. Lenci N, Francesco P, Scarciglia E, Fiorentino V, Schino M, Palermo G, Racioppi M, Bassi P, Martini M. Metanephric adenoma with BRAF V600K mutation and a doubtful radiological imaging: pitfalls in the diagnostic process. Med Mol Morphol. 2021; 54:187–91. https://doi.org/10.1007/s00795-020-00269-z. [PubMed].
17. Ding Y, Wang C, Li X, Jiang Y, Mei P, Huang W, Song G, Wang J, Ping G, Hu R, Miao C, He X, Chen G, et al. Novel clinicopathological and molecular characterization of metanephric adenoma: a study of 28 cases. Diagn Pathol. 2018; 13:54. https://doi.org/10.1186/s13000-018-0732-x. [PubMed].
18. Catic A, Kurtovic-Kozaric A, Sophian A, Mazur L, Skenderi F, Hes O, Rohan S, Rakheja D, Kogan J, Pins MR. KANK1-NTRK3 fusions define a subset of BRAF mutation negative renal metanephric adenomas. BMC Med Genet. 2020; 21:202. https://doi.org/10.1186/s12881-020-01143-6. [PubMed].
19. Dadone B, Ambrosetti D, Carpentier X, Duranton-Tanneur V, Burel-Vandenbos F, Amiel J, Pedeutour F. A renal metanephric adenoma showing both a 2p16e24 deletion and BRAF V600E mutation: a synergistic role for a tumor suppressor gene on chromosome 2p and BRAF activation? Cancer Genet. 2013; 206:347–52. https://doi.org/10.1016/j.cancergen.2013.09.002. [PubMed].
20. Wobker SE, Matoso A, Pratilas CA, Mangray S, Zheng G, Lin MT, Debeljak M, Epstein JI, Argani P. Metanephric Adenoma-Epithelial Wilms Tumor Overlap Lesions: An Analysis of BRAF Status. Am J Surg Pathol. 2019; 43:1157–69. https://doi.org/10.1097/PAS.0000000000001240. [PubMed].
21. Chan E, Stohr BA, Croom NA, Cho SJ, Garg K, Troxell ML, Higgins JP, Bean GR. Molecular characterisation of metanephric adenomas beyond BRAF: genetic evidence for potential malignant evolution. Histopathology. 2020; 76:1084–90. https://doi.org/10.1111/his.14094. [PubMed].
22. Chami R, Yin M, Marrano P, Teerapakpinyo C, Shuangshoti S, Thorner PS. BRAF mutations in pediatric metanephric tumors. Hum Pathol. 2015; 46:1153–61. https://doi.org/10.1016/j.humpath.2015.03.019. [PubMed].