
Introduction
The number of breast cancer patients is increasing every year, and the incidence of breast cancer is the highest (1 in 11 [9%]) among Japanese women according to the Center for Cancer Control and Information Services of the National Cancer Center [1]. In general, approximately 5%–10% of all breast cancers develop because of a genetic predisposition [2, 3].
Individuals with hereditary breast and ovarian cancer syndrome (HBOC), which is caused by germline pathogenic variants of BRCA1 or BRCA2, have an increased risk for breast cancer, ovarian cancer, prostate cancer, and pancreatic cancer [4–8]. In hereditary cancer, racial differences are important. For example, in persons of Ashkenazi Jewish heritage, three germline variants are observed: c.68_69delAG (BRCA1), c.5266dupC (BRCA1), and c.5946delT (BRCA2) [9]. As many as one in 40 Ashkenazi Jews have one of these three variants. A founder mutation is defined by the National Cancer Institute as “a gene mutation observed with high frequency in a group that is or was geographically or culturally isolated, in which one or more of the ancestors was a carrier of the mutant gene” [10]. Some reports on founder mutations of HBOC have been published from studies performed in Asia. From the Korean Hereditary Breast Cancer study [11] performed in Korea, one BRCA2 pathogenic variant (c.7480C>T) was identified as the Korean founder mutation using data from over 3,000 breast cancer patients [12]. Furthermore, using data from 651 breast cancer patients in Southern China, one BRCA1 pathogenic variant (c.981_982delAT) and three BRCA2 pathogenic variants (c.3109C>T, c.7436_7805del370, and c.9097_9098insA) were analyzed and reported as Chinese founder mutations [13]. In Japan, only a few reports on founder mutations of HBOC have been published [14–16]. The c.188T>A (307T>A) variant, which causes the amino acid change L63X, was reported as the Japanese founder mutation in breast cancer and ovarian cancer. BRCA1 L63X mutation was detected in Eastern Japan according to a previous report [15]. However, the data of these studies were not obtained from large study populations.
Recently, the Japanese HBOC consortium was established [16]. In this study, we aimed to analyze and report the clinical characteristics of breast cancer patients with BRCA1 L63X mutation, which is one of the BRCA1 founder mutations in the Japanese population, using the Japanese HBOC consortium trial registration data.
Results
We collected the data of 827 patients (752 breast and/or ovarian cancer patients and 75 patients without these cancers) who had undergone genetic testing in this trial registration through August 2015. The data showed 88 BRCA1 carriers, 76 BRCA2 carriers, one carrier of both BRCA1 and BRCA2, 54 variants of uncertain significance, and 608 non-carriers. We detected 46 independent pathogenic variants (including pathogenic and probably pathogenic variants) of BRCA1 and 52 independent pathogenic variants (including pathogenic and probably pathogenic variants) of BRCA2 (Figure 1). The BRCA1 pathogenic variants identified in three or more patients were c.188T>A (L63X), c.2800C>T, c.2389delGA, and c.3441delG (Table 1). The BRCA1 L63X mutation was detected in 26 patients (30.6% of BRCA1 carriers and 16.3% of BRCA1/2 carriers). The BRCA2 pathogenic variants identified in three or more patients were c.5576_5579delTAA, c.1278delA, c.8504C>A, c.9117G>A, c.6952C>T, and c.8589insA (Table 2).
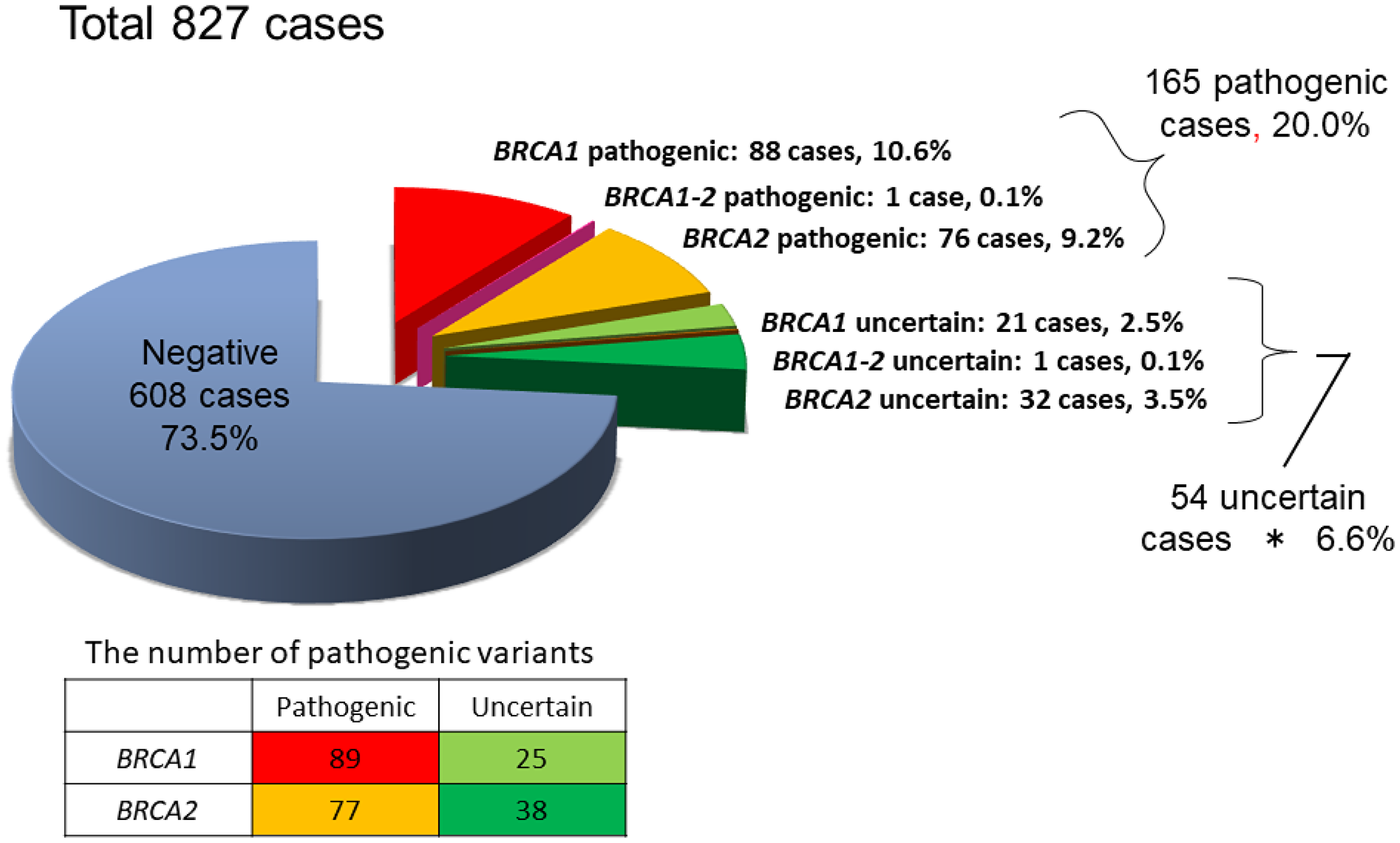
Figure 1: Results of BRCA1/2 genetic testing of 827 patients.
Table 1: BRCA1 pathogenic variants (identified in ≥three or more patients)
| Exon | AA change | BIC nomenclature | HGVS nomenclature | Effect on AA | Mutation pattern | Number |
|---|---|---|---|---|---|---|
| 5 | L63X | 307T>A | c.188T>A | p.Leu63Ter | nonsense | 26 |
| 11C | Q934X | 2919C>T | c.2800C>T | p.Glu934Ter | nonsense | 6 |
| 11B | STOP799 | 2508delGA | c.2389delGA | p.Glu797Thrfs*3 | deletion | 4 |
| 11D | STOP1154 | 3561delG | c.3442delG | p.Glu1148Argfs*7 | deletion | 4 |
Table 2: BRCA2 pathogenic variants (identified in ≥three or more patients)
| Exon | AA change | BIC nomenclature | HGVS nomenclature | Effect on AA | Mutation pattern | Number |
|---|---|---|---|---|---|---|
| 11E | STOP1862 | 5804del4 | c.5576_5579delTTAA | p.lle1859Lysfs | Deletion | 8 |
| 10 | STOP429 | 1506delA | c.1278delA | p.Asn433Glnfs | Deletion | 5 |
| 20 | S2835X | 8732C>A | c.8504C>A | p.Ser2835Ter | Nonsense | 4 |
| 23 | P3039P | 9345G>A | c.9117G>A | p.Pro3039Pro | Silent | 4 |
| 12 | R2318X | 7180C>T | c.6952C>T | p.Arg2318Ter | Nonsense | 3 |
| 20 | STOP2868 | 8817insA | c.8589dupA | p.Ala2864Serfs*5 | Insertion | 3 |
To clarify the BRCA1 L63X founder mutation, we compared the three groups (BRCA1 L63X, other BRCA1 mutations, and BRCA2 mutations) of breast cancer patients (Table 3). Comparison between the development and type of breast cancer and ovarian cancer in the probands showed that patients with both breast and ovarian cancers were observed only in the other BRCA1 mutation-positive group, although no significant difference was observed. The age at breast cancer onset was 40.3 years, 40.4 years, and 41.6 years in the BRCA1 L63X mutation-positive group, other BRCA1 mutation-positive group, and BRCA2 mutation-positive group, respectively. In general, although patients with BRCA1 mutation-positive breast cancer were younger than those with BRCA2 mutation-positive breast cancer [4], there was no significant difference in the age of onset and the status of breast cancer between the three groups. In addition, with regard to the breast cancer type, multifocal breast cancer was observed only in the BRCA2 mutation group, and there was no significant difference among the three groups. The results of the comparison of the breast cancer subtypes between the three groups were as follows: triple-negative breast cancer accounted for 89% of the BRCA1 L63X mutation group, 64.4% of other BRCA1 group, and 21.2% of BRCA2 group (p < 0.001). Significant differences in nuclear grade was also observed among the three groups (p < 0.001). During genetic counseling, we asked the patients about a family cancer history up to at least second-degree relatives. In the West, it was reported that the ovarian cancer risk was higher in the BRCA1 mutation group than in the BRCA2 mutation group, while the prostate cancer risk was higher in the BRCA2 group than in the BRCA1 group. However, no significant difference was observed between groups in terms of family cancer histories.
Table 3: Characteristics of three groups of breast cancer patients
| BRCA1 L63X n = 25a | Other BRCA1 mutation n = 59 | BRCA2 mutation n = 76a | p-value | BRCA1/2 negativeccn = 590 | |
|---|---|---|---|---|---|
| Cancer development | |||||
| BC only (%) | 22 (88) | 53 (89.8) | 73 (96.1) | 577 (97.8) | |
| OC only (%) | 3 (12) | 2 (3.4) | 3 (3.9) | 8 (1.4) | |
| BC+OC (%) | 0 | 4 (6.8) | 0 | 5 (0.8) | |
| NS | |||||
| BC onset | |||||
| Age | 40.3 | 40.4 | 41.6 | 45.2 | |
| (range) | (28–74) | (23–71) | (19–71) | (22–85) | |
| NS | |||||
| BC situationb | |||||
| Single BC (%) | 21 (95.5) | 55 (96.5) | 65 (90.3) | 468 (81.0) | |
| Bilateral BC (%) | 1 (4.5) | 2 (3.5) | 3 (4.2) | 87 (15.1) | |
| Multiple BC (%) | 0 | 0 | 4 (5.6) | 23 (3.9) | |
| NS | |||||
| BC subtypeb | |||||
| Luminal (%) | 2 (11) | 9 (20) | 23 (44.2) | 311 (62.4) | |
| Luminal+HER2 (%) | 0 | 2 (4.4) | 6 (11.5) | 42 (8.4) | |
| HER2 (%) | 0 | 0 | 1 (1.9) | 28 (5.6) | |
| Triple negative (%) | 16 (89) | 29 (64.4) | 11 (21.2) | 117 (23.5) | |
| p = < 0.001 | |||||
| BC nuclear gradeb | |||||
| 1 | 0 | 3 (8.3) | 21 (37.5) | 227 (59.3) | |
| 2 | 5 (31.2) | 5 (13.9) | 18 (32.1) | 121 (31.6) | |
| 3 | 11 (68.8) | 28 (77.8) | 17 (30.4) | 135 (35.2) | |
| p = < 0.001 | |||||
| Family history | |||||
| BC (average number) | 2.31 | 2 | 2.75 | 0.97 | |
| (range) | (0–5) | (1-6) | (0-6) | (0-5) | |
| OC (average number) | 0.54 | 0.81 | 0.36 | 0.15 | |
| (range) | (0-3) | (0-4) | (0-3) | (0-3) | |
| PC (average number) | 0.154 | 0.145 | 0.2 | 0.1 | |
| (range) | (0–1) | (0–2) | (0–2) | (0–2) | |
| NS |
DISCUSSION
BRCA1 was discovered in 1994 and BRCA2 in 1995 [18, 19]. In the United States, BRCA1/2 clinical testing started in 1996. However, this clinical testing started in 2006 in Japan, although testing had been performed in research studies. Compared to Western countries, because an HBOC medical treatment system started later in Japan, only a few reports on HBOC from Japan were obtained. Sugano et al. [20] reported that 36 of the 135 proband patients were BRCA1/2 mutation carriers including five BRCA1 L63X mutation carriers. It also described the prevalence and clinical characteristics of HBOC in Japan in 2008. Nakamura et al. [21] reported that 80 of the 260 proband patients were BRCA1/2 mutation carriers including 10 BRCA1 L63X mutation carriers and described the prevalence and differentiation of HBOC. Our study included the largest number of HBOC patients reported in Japan. The BRCA1 L63X mutation, which was reported only in Asians in the Breast Cancer Information Core database [22], was identified as a Japanese founder mutation of ovarian cancer in haplotype analysis. In our study, we used multi-facility trial registration data; thus, we have not performed haplotype analysis, but it is suggested that it is a common ancestor. Considering that it is the most frequent HBOC founder mutation among Japanese people, previous analytical studies did not have large sample sizes (Table 4). In this study, we aimed to confirm that a high proportion of Japanese HBOC patients showed the BRCA1 L63X mutation.
Table 4: Comparison of reports on the BRCA1 L63X mutation
| Institution | Number of BRCA genetic testing | Number of BRCA1 mutations | Number of BRCA1 L63X | Analysis | Results | |
|---|---|---|---|---|---|---|
| Ikeda 1997 [14] | Osaka Univ. | 113 | 15 | 4 | Haplotype analysis | Common ancestors |
| Sekine 2001 [15] | Niigata Univ. | 82 | 24 | 7 | Clinicopathological Analysis | Lower proportion of advanced |
| Nagata 2001 [17] | Niigata Univ. | 45 (BRCA1 only) | 24 | 7 | Haplotype analysis (Data not shown) | Common ancestors |
| Momozawa 2018 [34] | Biobank Japan | BC case: 7,051 Control: 11,241 | 102 | 26 | Allele frequency | 26% in BRCA1 mutations |
| Our data | HBOC consortium | 827 | 89 | 25 | Clinicopathological analysis | Higher of TN proportion |
Considering that hereditary cancer differs according to ethnicity, a founder mutation is an important element and leads to questions such as “How many founder mutations are observed in a related gene?” and “What kinds of effects does the genotype of a founder mutation have on cancer phenotype?” Identification of a founder mutation and knowledge of its prevalence in each population provides important information for genetic counseling, cancer risk assessment, and the development of a cost-effective screening strategy. Many hypotheses concerning Japanese ancestry have been proposed. Recently, using the Y chromosome, which does not undergo genetic recombination, haplotype research, and a genome-wide single nucleotide polymorphism database, the Japanese were believed to be a mixed population that descended from the Jomon people (hunters), who originated in Southeast Asia 10,000 years ago and settled in the Japanese archipelago, and the Yayoi people (farmers), who emigrated from the East Asian continent 2,000 to 3,000 years ago [22–26]. The Japanese population is the largest in the world to have inherited the haplotype of the Jomon people, which is not seen in Chinese and Korean populations [27]. This might be because Japan could be considered as an island country at the outskirts of the eastern countries. As a result, we could consider that the frequency of the BRCA1 L63X mutation might be very high in the Japanese population (Table 5). However, the Japanese population might be mixed: one c.7480C>T BRCA2 variant (the Korean founder mutation) and one c.470-471delCT BRCA1 variant (the Southern Chinese founder mutation) were observed in this registry [16].
Table 5: Proportions of founder mutations according to race
| Race | Founder mutation | BRCA1/2 carriers | Proportion of founder mutation (%) |
|---|---|---|---|
| Korea [12] | BRCA2 c. 7480C>T | 148 | 18 (12.2) |
| Southern Chinese [13] | BRCA1 c.981_982delAT | 69 | 2 (2.9) |
| BRCA2 c.3109C>T | 10 (14.5) | ||
| BRCA2 c.7436_7805del370 | 2 (2.9) | ||
| BRCA2 c.9097_9098insA | 2 (2.9) | ||
| Mainland Chinese [28] | BRCA1 c.981_982delAT | 566 | 18 (3.2) |
| BRCA2 c.3195_3198delTAAT | 5 (0.9) | ||
| BRCA2 c.5576_5579delTTAA | 5 (0.9) | ||
| Japanese (our study) | BRCA1 c.188 T>A | 161 | 26 (16.1) |
In general, the population-adjusted age distribution of breast cancer patients in Japan showed two distinct peaks, one for patients in their late 40s and another for patients in their early 60s [29]. However, according to the Surveillance, Epidemiology, and End Results database [30], between 2009 and 2013, in the age distribution of newly diagnosed breast cancer patients in the USA, there was only one peak for patients in their early 60s; in contrast, there was one peak for patients in their 40s in this age distribution in South Korea [31]. These findings indicated that there are two mixed peaks in Japan: one in patients in their 40s, similar to East Asian women, and another in patients in their early 60s, similar to Western women. In our result, the average age at breast cancer onset between the BRCA1 group and BRCA2 group was nearly equal.
According to the Consortium of Investigators of Modifiers of BRCA1/2, regarding the pathology of breast cancer with BRCA1/2 mutations [32], triple-negative breast cancer accounted for 69% of BRCA1 mutations and 16% of BRCA2 mutations, and the nuclear grades (grade 1, grade 2, and grade 3 [%]) were 3%, 20%, and 77% for BRCA1 mutations and 7%, 43%, and 50% for BRCA2 mutations, respectively. Although the pathological features of BRCA1 breast cancer and BRCA2 breast cancer reported in our study were similar to that of Western studies, the rate of triple-negative breast cancer was very high (89%) in the BRCA1 L63X mutation group. The proportion of patients with triple negative breast cancer among those who were BRCA1/2 negative in this study was 28.9% (173/597), which is higher than that of 15.4% found in the registered data of the Japan Breast Cancer Society [33]. The triple negative subtype appeared to be a part of the BRCA genetic testing criteria; however, the proportion of patients with triple negative breast cancer in those with an L63X and BRCA1 positive status in our study was much higher than that in those who were BRCA 1/2 negative. This trend was also seen in research published overseas. Because of modifiers (including genetic background and environmental factors), the characteristics of breast cancer harboring a BRCA1/2 mutation in the Japanese population might be different from that of other races. Hence, we need to create a Japanese HBOC database and elucidate the realities of HBOC breast cancer in Japan.
The association between the type and location of BRCA1 and BRCA2 mutations was published in 2015 by Rebbeck et al. [34], and they identified that breast cancer cluster regions (BCCR) were locations where carriers had a tendency to develop breast cancer mutations. The BRCA1 L63X mutation is located in the putative BCCR1 region, which has been reported in the juvenile-onset region in this study [34]. However, in this study, data obtained from the Asian population entailed that only 0.2% of individuals were BRCA1 carriers.
Recently, germline pathogenic variants of 11 breast cancer genes were explored in Japanese breast cancer patients using the samples from Biobank Japan, which is a multi-institutional hospital-based registry that collects DNA from peripheral blood leukocytes of patients with various common diseases, including breast cancer regardless of the possibility for HBOC [35]. They also found recurrent BRCA1 L63X founder mutation in BRCA1 pathogenic variants (26/102: 26% OR = 20.8) in the unselected breast cancer patients. This tendency might be found not only in East Japan but also in Japan as a whole.
In this trial registration, some selection bias might have occurred. Because the registration committee members of three hospitals belonged to the breast cancer division, we might have had a tendency to register more breast cancer patients than ovarian cancer patients. In this registration, although most patients matched the criteria for genetic testing according to the National Comprehensive Cancer Network guidelines [36], no standards were indicated in the registry. This might have affected the comparison studies including those on the age of onset, development and type of breast and ovarian cancer, clinical characteristics of breast cancer, and family cancer history.
In conclusion, the founder mutation BRCA1 L63X was observed in approximately 30% of BRCA1 carriers and is frequently observed among Japanese patients. This could be attributed to the fact that Japan is an island. The clinical characteristics of breast cancer in patients with the BRCA1 L63X mutation might not differ from those caused by other BRCA1 or BRCA2 mutations, except the subtype and nuclear grade of the resultant cancer. Further investigation is required to appropriately validate and obtain the data. Hence, we started a nationwide registration in March 2016 [37].
Materials and Methods
This investigation has been conducted in accordance with the ethical standards, the Declaration of Helsinki, and national and international guidelines. This study was approved by the Ethical Review Boards of the Japanese HBOC Consortium and each medical institution. Informed consent has been obtained in principle [16]. The Japanese HBOC consortium was established in 2012, following another study conducted by the Japanese Breast Cancer Society (2010–2012). This consortium aimed to raise awareness of HBOC in Japan and to provide an effective healthcare system for HBOC patients and their families. Their activities included constructing the Japanese HBOC database, promoting educational activities about HBOC, and developing HBOC guidelines and research. At first, for constructing the Japanese HBOC database, a trial registration was conducted by the registration committee members of four hospitals, namely, Hoshi General Hospital (Fukushima), Showa University Hospital (Tokyo), Cancer Institute Hospital (Tokyo), and St. Luke’s International Hospital (Tokyo) (Figure 2). We registered patients who underwent genetic testing at these four hospitals [16].
Figure 2: Trial registration committee members of four hospitals. As shown in the map, the four hospitals are located in Eastern Japan.
During the registration, the following data were collected: family identification number, birthdate, sex, age at death, development and type of breast cancer and ovarian cancer, history of other cancers, age during first childbirth, age at menarche, age at menopause, cause of death, data about breast cancer (age at onset, location, discovery opportunities, treatments, operative method, operation date, pathological histology, tumor size, nuclear grade, estrogen receptor status, progesterone receptor status, human epidermal growth factor receptor 2 status, and Ki-67 index score), data about ovarian cancer (age at onset, date of treatment initiation, treatment result, location, treatments, operative method, operation date, pathological histology, stage, and nuclear grade), date of genetic testing, result of genetic testing, genotype, prophylactic surgery, and family history (at least till second-degree relatives). The registration data were updated annually. All genetic tests were performed by FALCO HOLDINGS, which signed an exclusive contract with Myriad Genetics (United States) and holds the BRCA1/2 genetic testing patent in Japan. Genetic testing for BRCA1/2 was performed via direct sequencing and multiplex ligation-dependent probe amplification.
From all the registered patients, we evaluated the age at breast cancer onset, pathological features, clinical features, and family history of breast cancer patients, and we compared the difference between those with the BRCA1 L63X mutation, other BRCA1 mutations, and BRCA2 mutations using the Chi-square test.
ACKNOWLEDGMENTS
The authors acknowledge the members of the HBOC consortium.
CONFLICTS OF INTEREST
The authors declare that they have no competing interests.
FUNDING
This work was supported by Health, Labour and Welfare Sciences Research Grants (H26-policy for cancer general-012 for MA).
References
1. Cancer Information Service, National Cancer Center. Cancer Statistics in Japan. 2018. http://ganjoho.jp/reg_stat/statistics/stat/summary.html.
2. Claus EB, Schildkraut JM, Thompson WD, Risch NJ. The genetic attributable risk of breast and ovarian cancer. Cancer. 1996; 77:2318–2324. https://doi.org/10.1002/(SICI)1097-0142(19960601)77:11<2318::AID-CNCR21>3.0.CO;2-Z. [PubMed].
3. Edlich RF, Winters KL, Lin KY. Breast cancer and ovarian cancer genetics. J Long Term Eff Med Implants. 2005; 15:533–545. https://doi.org/10.1615/JLongTermEffMedImplants.v15.i5.60. [PubMed].
4. Chen S, Parmigiani G. Meta-analysis of BRCA1 and BRCA2 penetrance. J Clin Oncol. 2007; 25:1329–1333. https://doi.org/10.1200/JCO.2006.09.1066. [PubMed].
5. Mocci E, Milne RL, Méndez-Villamil EY, Hopper JL, John EM, Andrulis IL, Chung WK, Daly M, Buys SS, Malats N, Goldgar DE. Risk of pancreatic cancer in breast cancer families from the breast cancer family registry. Cancer Epidemiol Biomarkers Prev. 2013; 22:803–811. https://doi.org/10.1158/1055-9965.EPI-12-0195. [PubMed].
6. Liede A, Karlan BY, Narod SA. Cancer risks for male carriers of germline mutations in BRCA1 or BRCA2: a review of the literature. J Clin Oncol. 2004; 22:735–742. https://doi.org/10.1200/JCO.2004.05.055. [PubMed].
7. Ford D, Easton DF, Stratton M, Narod S, Goldgar D, Devilee P, Bishop DT, Weber B, Lenoir G, Chang-Claude J, Sobol H, Teare MD, Struewing J, et al. Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. The Breast Cancer Linkage Consortium. Am J Hum Genet. 1998; 62:676–689. https://doi.org/10.1086/301749. [PubMed].
8. Mavaddat N, Peock S, Frost D, Ellis S, Platte R, Fineberg E, Evans DG, Izatt L, Eeles RA, Adlard J, Davidson R, Eccles D, Cole T, et al; EMBRACE. Cancer risks for BRCA1 and BRCA2 mutation carriers: results from prospective analysis of EMBRACE. J Natl Cancer Inst. 2013; 105:812–822. https://doi.org/10.1093/jnci/djt095. [PubMed].
9. Struewing JP, Hartge P, Wacholder S, Baker SM, Berlin M, McAdams M, Timmerman MM, Brody LC, Tucker MA. The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N Engl J Med. 1997; 336:1401–1408. https://doi.org/10.1056/NEJM199705153362001. [PubMed].
10. National Cancer Institute Dictionary of Genetics Terms. http://www.cancer.gov/publications/dictionaries/genetics-dictionary?cdrid=570712.
11. Han SA, Park SK, Ahn SH, Lee MH, Noh DY, Kim LS, Noh WC, Jung Y, Kim KS, Kim SW; Korean Breast Cancer Study Group. The Korean Hereditary Breast cancer (KOHBRA) study: protocols and interim report. Clin Oncol (R Coll Radiol). 2011; 23:434–441. https://doi.org/10.1016/j.clon.2010.11.007. [PubMed].
12. Kang E, Kim SW. The Korean hereditary breast cancer study: review and future perspective. J Breast Cancer. 2013; 16:245–253. https://doi.org/10.4048/jbc.2013.16.3.245. [PubMed].
13. Kwong A, Ng EK, Wong CL, Law FB, Au T, Wong HN, Kurian AW, West DW, Ford JM, Ma ES. Identification of BRCA1/2 founder mutations in Southern Chinese breast cancer patients using gene sequencing and high resolution DNA melting analysis. PLoS One. 2012; 7:e43994. https://doi.org/10.1371/journal.pone.0043994. [PubMed].
14. Ikeda N, Miyoshi Y, Yoneda K, Shiba E, Sekihara Y, Kinoshita M, Noguchi S. Frequency of BRCA1 and BRCA2 germline mutations in Japanese breast cancer families. Int J Cancer. 2001; 91:83–88. https://doi.org/10.1002/1097-0215(20010101)91:1<83::AID-IJC1013>3.0.CO;2-5. [PubMed].
15. Sekine M, Nagata H, Tsuji S, Hirai Y, Fujimoto S, Hatae M, Kobayashi I, Fujii T, Nagata I, Ushijima K, Obata K, Suzuki M, Yoshinaga M, et al; Japanese Familial Ovarian Cancer Study Group. Mutational analysis of BRCA1 and BRCA2 and clinicopathologic analysis of ovarian cancer in 82 ovarian cancer families: two common founder mutations of BRCA1 in Japanese population. Clin Cancer Res. 2001; 7:3144–3150. [PubMed].
16. Arai M, Yokoyama S, Watanabe C, Yoshida R, Kita M, Ohkawa M, Sakurai A, Sekine M, Yotsumoto J, Nomura H, Akama Y, Inuzuka M, Nomizu T, et al. Genetic and clinical characteristics in Japanese hereditary breast and ovarian cancer: first report after establishment of HBOC registration system in Japan. J Hum Genet. 2018; 63:447–457. https://doi.org/10.1038/s10038-017-0355-1. [PubMed].
17. Nagata H, Sekine M, Tsuji S. Haplotypes of BRCA1 mutation alleles in Japanese ovarian and breast-ovarian cancer families: a novel method for detecting BRCA1 associated ovarian cancer. Acta Med Biol (Niigata). 2002; 50:33–42.
18. Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, Harshman K, Tavtigian S, Liu Q, Cochran C, Bennett LM, Ding W. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science. 1994; 266:66–71. https://doi.org/10.1126/science.7545954. [PubMed].
19. Wooster R, Bignell G, Lancaster J, Swift S, Seal S, Mangion J, Collins N, Gregory S, Gumbs C, Micklem G. Identification of the breast cancer susceptibility gene BRCA2. Nature. 1995; 378:789–792. https://doi.org/10.1038/378789a0. [PubMed].
20. Sugano K, Nakamura S, Ando J, Takayama S, Kamata H, Sekiguchi I, Ubukata M, Kodama T, Arai M, Kasumi F, Hirai Y, Ikeda T, Jinno H, et al. Cross-sectional analysis of germline BRCA1 and BRCA2 mutations in Japanese patients suspected to have hereditary breast/ovarian cancer. Cancer Sci. 2008; 99:1967–1976. https://doi.org/10.1111/j.1349-7006.2008.00944.x. [PubMed].
21. Nakamura S, Takahashi M, Tozaki M, Nakayama T, Nomizu T, Miki Y, Murakami Y, Aoki D, Iwase T, Nishimura S, Yamauchi H, Ohsumi S, Baba S, et al. Prevalence and differentiation of hereditary breast and ovarian cancers in Japan. Breast Cancer. 2015; 22:462–468. https://doi.org/10.1007/s12282-013-0503-1. [PubMed].
22. Breast Cancer Information Core. https://research.nhgri.nih.gov/bic/.
23. Tajima A, Hayami M, Tokunaga K, Juji T, Matsuo M, Marzuki S, Omoto K, Horai S. Genetic origins of the Ainu inferred from combined DNA analyses of maternal and paternal lineages. J Hum Genet. 2004; 49:187–193. https://doi.org/10.1007/s10038-004-0131-x. [PubMed].
24. Hammer MF, Karafet TM, Park H, Omoto K, Harihara S, Stoneking M, Horai S. Dual origins of the Japanese: common ground for hunter-gatherer and farmer Y chromosomes. J Hum Genet. 2006; 51:47–58. https://doi.org/10.1007/s10038-005-0322-0. [PubMed].
25. Nonaka I, Minaguchi K, Takezaki N. Y-chromosomal binary haplogroups in the Japanese population and their relationship to 16 Y-STR polymorphisms. Ann Hum Genet. 2007; 71:480–495. https://doi.org/10.1111/j.1469-1809.2006.00343.x. [PubMed].
26. Yamaguchi-Kabata Y, Nakazono K, Takahashi A, Saito S, Hosono N, Kubo M, Nakamura Y, Kamatani N. Japanese population structure, based on SNP genotypes from 7003 individuals compared to other ethnic groups: effects on population-based association studies. Am J Hum Genet. 2008; 83:445–456. https://doi.org/10.1016/j.ajhg.2008.08.019. [PubMed].
27. Jinam T, Nishida N, Hirai M, Kawamura S, Oota H, Uemetsu K, Kimura R, Ohashi J, Tajima A, Yamamoto T, Tanabe H, Mano S, et al; Japanese Archipelago Human Population Genetics Consortium. The history of human populations in the Japanese Archipelago inferred from genome-wide SNP data with a special reference to the Ainu and the Ryukyuan populations. J Hum Genet. 2012; 57:787–795. https://doi.org/10.1038/jhg.2012.114. [PubMed].
28. Kim YC, Zhao L, Zhang H, Huang Y, Cui J, Xiao F, Downs B, Wang SM. Prevalence and spectrum of BRCA germline variants in mainland Chinese familial breast and ovarian cancer patients. Oncotarget. 2016; 7:9600–9612. https://doi.org/10.18632/oncotarget.7144. [PubMed].
29. Kurebayashi J, Miyoshi Y, Ishikawa T, Saji S, Sugie T, Suzuki T, Takahashi S, Nozaki M, Yamashita H, Tokuda Y, Nakamura S. Clinicopathological characteristics of breast cancer and trends in the management of breast cancer patients in Japan: Based on the Breast Cancer Registry of the Japanese Breast Cancer Society between 2004 and 2011. Breast Cancer. 2015; 22:235–244. https://doi.org/10.1007/s12282-015-0599-6. [PubMed].
30. National Cancer Institute Surveillance, Epidemiology, and End Results Program. http://seer.cancer.gov/statfacts/html/breast.html.
31. Kim Z, Min SY, Yoon CS, Lee HJ, Lee JS, Youn HJ, Park HK, Noh DY, Hur MH, Korean Breast Cancer Society. The basic facts of Korean breast cancer in 2011: results of a nationwide survey and breast cancer registry database. J Breast Cancer. 2014; 17:99–106. https://doi.org/10.4048/jbc.2014.17.2.99. [PubMed].
32. Mavaddat N, Barrowdale D, Andrulis IL, Domchek SM, Eccles D, Nevanlinna H, Ramus SJ, Spurdle A, Robson M, Sherman M, Mulligan AM, Couch FJ, Engel C, et al; Consortium of Investigators of Modifiers of BRCA1/2. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol Biomarkers Prev. 2012; 21:134–147. https://doi.org/10.1158/1055-9965.EPI-11-0775. [PubMed].
33. Iwase H, Kurrebayashi J, Tsuda H, Ohta Y, Kurosumi M, Miyamoto K, Yamamoto Y, Iwase T. Clinicopathological analyses of triple negative breast cancer using surveillance data from the Registration Committee of the Japanese Breast Cancer Society. Breast Cancer. 2010; 17:118–124. https://doi.org/10.1007/s12282-009-0113-0. [PubMed].
34. Rebbeck TR, Mitra N, Wan F, Sinilnikova OM, Healey S, McGuffog L, Mazoyer S, Chenevix-Trench G, Easton DF, Antoniou AC, Nathanson KL, Laitman Y, Kushnir A, et al; CIMBA Consortium. Association of type and location of BRCA1 and BRCA2 mutations with risk of breast and ovarian cancer. JAMA. 2015; 313:1347–1361. https://doi.org/10.1001/jama.2014.5985. [PubMed].
35. Momozawa Y, Iwasaki Y, Parsons M, Komatani Y, Takahashi A, Tamura C, Katagiri T, Yoshida T, Nakamura S, Sugano K, Miki Y, Hirata M, Matsuda K, et al. Germline pathogenic variants of 11 breast cancer genes in 7,051 Japanese Patients and 11,241 controls. Nat Commun. 2018; 9:4083. https://doi.org/10.1038/s41467-018-06581-8. [PubMed].
36. NCCN Guidelines version 2.2016 Genetic/Familial High-Risk Assessment: Breast and Ovarian. https://www.nccn.org/professionals/physician_gls/pdf/genetics_screening.pdf.
37. Yamauchi H, Okawa M, Yokoyama S, Nakagawa C, Yoshida R, Suzuki K, Nakamura S, Arai M. High rate of occult cancer found in prophylactic mastectomy specimens despite through presurgical assessment with MRI and ultrasound: findings from the Hereditary Breast and Ovarian Cancer Registration 2016 in Japan. Breast Cancer Res Treat. 2018; 172:679–687. https://doi.org/10.1007/s10549-018-4953-1. [PubMed].