
INTRODUCTION
Interleukin-6 (IL-6) is one of the most widely recognized cytokines. It can regulate immune responses and cell proliferation and differentiation [1]. IL-6 was originally studied as an inflammatory factor, which was later found to be closely related to tumorigenesis, invasion and metastasis [2]. High expression of IL-6 is associated with different cancer types, such as esophageal cancer, non-small cell lung cancer, endometrial cancer, breast cancer, prostate cancer, lung cancer, chronic lymphocytic leukemia and diffuse large B-cell lymphoma [2–5]. Therefore, IL-6 is closely related to tumor occurrence and development, and understanding the genetic diversity of IL-6 will be helpful for cancer risk prediction and gene therapy.
The human IL-6 gene is located on chromosome 7p21 which is identified as pro-inflammatory cytokine [6], and plays an important role in the pathogenesis of several types of cancers. The single nucleotide polymorphisms (SNPs) at the 50 flanking region of the IL-6 gene promoter (rs1800795, rs1800796 and rs1800797) can effect on IL-6 expression [7–9]. However, previous studies have conflicting results between IL-6 promoter (rs1800795, rs1800796 and rs1800797) and cancer susceptibility [10–99] and prognosis [40, 47, 53, 57, 63, 100-106].
To confirm whether IL-6 promoter polymorphisms are related to cancer risk, we performed this meta-analysis, aiming to measure the correlation between IL-6 promoter polymorphisms and cancer susceptibility and prognosis.
RESULTS
Characteristics of published studies
A flow chart was carefully identified of the search process in Figure 1. After duplicates removed, 16843 studies were retrieved (PubMed: 16457, Embase: 18324). Finally, ninety-seven studies were chosen, and the data was extracted. Seventy-eight studies reported the association between rs1800795 and cancer risk, twenty-one studies reported the association between rs1800796 and cancer risk, seventeen studies reported the association between rs1800797 and cancer risk, and twelve studies reported the association between IL-6 promoter polymorphisms and cancer prognosis. The genotype frequencies of IL-6 promoter in controls of each study met the HWE expectation (P > 0.05). The genotype distributions of all studies are summarized in Supplementary Tables 1–6.
Meta-analysis of rs1800795 polymorphism and cancer risk
Seventy-eight studies reported the association between rs1800795 and cancer risk. Our results showed that rs1800795 was significantly associated with increased cancer risk in allelic, dominant, recessive and additive models (OR = 1.05, 95% CI: 1.01, 1.09, P = 0.007, allelic models respectively) (Table 1). Subgroup analysis indicated that rs1800795 was associated with a significantly higher risk of cancer in Asia (OR = 1.05, 95% CI: 1.01, 1.10, P = 0.003, allelic models respectively) (Table 2) and Caucasian (OR= 1.04, 95% CI: 1.02, 1.06, P < 0.001, allelic models respectively) (Table 2) in all four gene model. Meanwhile, rs1800795 was significantly associated with increased risk of cervical cancer (OR = 1.13, 95% CI: 1.05, 1.21, P = 0.004, allelic models respectively) (Table 3), colorectal cancer (OR = 1.10, 95% CI: 1.02, 1.19, P = 0.014, allelic models respectively) (Table 3), breast cancer (OR = 1.08, 95% CI: 1.01, 1.19, P = 0.013, allelic models respectively) (Table 3), prostate cancer (OR = 1.08, 95% CI: 1.03, 1.13, P = 0.005, allelic models respectively) (Table 3), lung cancer(OR = 1.08, 95% CI: 1.02, 1.15, P = 0.003, allelic models respectively) (Table 3), glioma (OR = 1.28, 95% CI: 1.13, 1.46, P < 0.001, allelic models respectively) (Table 3), non-hodgkin’s lymphoma (OR = 1.25, 95% CI: 1.01, 1.51, P = 0.049, allelic models respectively) (Table 3) and hodgkin’s lymphoma (OR = 1.22, 95% CI: 1.02, 1.45, P = 0.030, allelic models respectively) (Table 3) but not gastric cancer (OR = 0.95, 95% CI: 0.83, 1.08, P = 0.435, allelic models respectively)(Table 3) and multiple myeloma (OR = 1.06, 95% CI: 0.88, 1.30, P = 0.559, allelic models respectively) (Table 3) in all four gene model.
Table 1: Meta-analysis of IL-6 promoter polymorphisms and cancer susceptibility
Genetic model |
No.of studies |
Heterogeneity |
OR |
95% CI |
P value |
Model |
|
|---|---|---|---|---|---|---|---|
I2 |
P value |
||||||
rs1800795 |
78 (46096/56969) |
||||||
G vs. C |
55.5% |
0.000 |
1.05 |
1.01,1.09 |
0.007 |
Random-effects model |
|
GG+ GC vs. CC |
38.4% |
0.000 |
1.04 |
1.01,1.08 |
0.021 |
Fixed-effects model |
|
GG vs. GC+CC |
55.1% |
0.000 |
1.08 |
1.03,1.13 |
0.001 |
Random-effects model |
|
GG vs. GC |
53.4% |
0.000 |
1.06 |
1.00,1.14 |
0.035 |
Random-effects model |
|
rs1800796 |
21 (9930/13080) |
||||||
C vs. G |
47.2% |
0.008 |
1.11 |
1.04,1.18 |
< 0.001 |
Fixed-effects model |
|
CC+ CG vs. GG |
34.4% |
0.059 |
1.12 |
1.02,1.21 |
0.029 |
Fixed-effects model |
|
CC vs. CG+GG |
50.6% |
0.003 |
1.09 |
1.03,1.16 |
0.045 |
Random-effects model |
|
CC vs. CG |
44.5% |
0.013 |
1.04 |
1.01,1.09 |
0.010 |
Fixed-effects model |
|
rs1800797 |
17 (9162/12724) |
||||||
G vs. A |
0.0% |
0.901 |
1.04 |
1.01,1.08 |
0.007 |
Fixed-effects model |
|
GG+ GA vs. AA |
0.0% |
0.904 |
1.07 |
1.02,1.13 |
0.007 |
Fixed-effects model |
|
GG vs. GA+AA |
0.0% |
0.493 |
1.06 |
1.03,1.09 |
0.004 |
Fixed-effects model |
|
GG vs. GA |
38.0% |
0.020 |
1.03 |
1.00,1.08 |
0.035 |
Fixed-effects model |
|
Table 2: Meta-analysis of IL-6 promoter polymorphisms and cancer risk in ethnicity
rs1800795 |
No.of studies |
Heterogeneity |
OR |
95% CI |
P value |
Model |
|
|---|---|---|---|---|---|---|---|
Ethnicity |
I2 |
P value |
|||||
Asian |
3 (1090/1482) |
||||||
G vs. C |
75.5% |
0.017 |
1.05 |
1.01,1.10 |
0.003 |
Random-effects model |
|
GG+ GC vs. CC |
47.1% |
0.151 |
1.03 |
1.01,1.06 |
< 0.001 |
Fixed-effects model |
|
GG vs. GC+CC |
66.8% |
0.049 |
1.07 |
1.03,1.12 |
< 0.001 |
Random-effects model |
|
GG vs. GC |
56.7% |
0.100 |
1.06 |
1.01,1.12 |
0.002 |
Random-effects model |
|
Caucasian |
75 (44895/55402) |
||||||
G vs. C |
49.7% |
0.000 |
1.04 |
1.02,1.06 |
< 0.001 |
Fixed-effects model |
|
GG+ GC vs. CC |
34.0% |
0.001 |
1.05 |
1.02,1.09 |
0.004 |
Fixed-effects model |
|
GG vs. GC+CC |
51.4% |
0.000 |
1.10 |
1.06,1.15 |
< 0.001 |
Random-effects model |
|
GG vs. GC |
51.6% |
0.000 |
1.08 |
1.03,1.14 |
0.004 |
Random-effects model |
|
rs1800796 |
|||||||
Asian |
12 (3574/4423) |
||||||
C vs. G |
52.9% |
0.013 |
1.08 |
1.03,1.14 |
< 0.001 |
Random-effects model |
|
CC+ CG vs. GG |
28.3% |
0.160 |
1.12 |
1.05,1.20 |
< 0.001 |
Fixed-effects model |
|
CC vs. CG+GG |
54.9% |
0.009 |
1.15 |
1.06,1.25 |
0.009 |
Random-effects model |
|
CC vs. CG |
53.2% |
0.012 |
1.06 |
1.02,1.11 |
0.018 |
Random-effects model |
|
Caucasian |
9 (5679/8001) |
||||||
C vs. G |
0.0% |
0.651 |
1.05 |
1.01,1.10 |
0.003 |
Fixed-effects model |
|
CC+ CG vs. GG |
5.2% |
0.392 |
1.05 |
1.02,1.09 |
< 0.001 |
Fixed-effects model |
|
CC vs. CG+GG |
15.2% |
0.299 |
1.06 |
1.02,1.11 |
0.002 |
Fixed-effects model |
|
CC vs. CG |
29.9% |
0.180 |
1.04 |
1.02,1.06 |
< 0.001 |
Fixed-effects model |
|
rs1800797 |
|||||||
Asian |
2 (187/495) |
||||||
G vs. A |
0.0% |
0.637 |
1.23 |
0.79,2.04 |
0.326 |
Fixed-effects model |
|
GG+ GA vs. AA |
0.0% |
0.954 |
4.38 |
1.21,15.9 |
0.025 |
Fixed-effects model |
|
GG vs. GA+AA |
0.0% |
0.589 |
0.86 |
0.48,1.34 |
0.405 |
Fixed-effects model |
|
GG vs. GA |
0.0% |
0.377 |
0.38 |
0.21,0.68 |
0.001 |
Fixed-effects model |
|
Caucasian |
14 (8298/11573) |
||||||
G vs. A |
0.0% |
0.806 |
1.04 |
1.01,1.08 |
0.041 |
Fixed-effects model |
|
GG+ GA vs. AA |
0.0% |
0.900 |
1.06 |
1.02,1.11 |
0.034 |
Fixed-effects model |
|
GG vs. GA+AA |
3.1% |
0.418 |
1.06 |
1.01,1.11 |
0.014 |
Fixed-effects model |
|
GG vs. GA |
25.9% |
0.122 |
1.03 |
1.01,1.06 |
0.002 |
Fixed-effects model |
|
Table 3: Subground of analyses of rs1800795 polymorphism and cancer risk
rs1800795 |
No.of studies |
Heterogeneity |
OR |
95% CI |
P value |
Model |
|
|---|---|---|---|---|---|---|---|
Cancer type |
I2 |
P value |
|||||
Cervical cancer |
7 (1734/2272) |
||||||
G vs. C |
70.1% |
0.003 |
1.13 |
1.05,1.21 |
0.004 |
Random-effects model |
|
GG+ GC vs. CC |
58.5% |
0.025 |
1.16 |
1.06,1.27 |
0.039 |
Random-effects model |
|
GG vs. GC+CC |
58.7% |
0.024 |
1.21 |
1.08,1.34 |
0.002 |
Random-effects model |
|
GG vs. GC |
44.0% |
0.098 |
1.19 |
1.08,1.30 |
0.003 |
Fixed-effects model |
|
Colorectal cancer |
14 (7399/9808) |
||||||
G vs. C |
63.7% |
0.000 |
1.10 |
1.02,1.19 |
0.014 |
Random-effects model |
|
GG+ GC vs. CC |
0.0% |
0.515 |
1.13 |
1.04,1.22 |
0.003 |
Fixed-effects model |
|
GG vs. GC+CC |
63.6% |
0.000 |
1.11 |
1.01,1.22 |
0.047 |
Random-effects model |
|
GG vs. GC |
54.6% |
0.006 |
1.07 |
1.01,1.19 |
0.019 |
Random-effects model |
|
Gastric cancer |
4 (672/1614) |
||||||
G vs. C |
0.0% |
0.776 |
0.95 |
0.83,1.08 |
0.435 |
Fixed-effects model |
|
GG+ GC vs. CC |
0.0% |
0.573 |
1.03 |
0.81,1.32 |
0.799 |
Fixed-effects model |
|
GG vs. GC+CC |
0.0% |
0.874 |
0.87 |
0.72,1.06 |
0.181 |
Fixed-effects model |
|
GG vs. GC |
0.0% |
0.409 |
0.85 |
0.69,1.05 |
0.122 |
Fixed-effects model |
|
Breast cancer |
13 (9532/15064) |
||||||
G vs. C |
57.8% |
0.011 |
1.08 |
1.01,1.19 |
0.013 |
Random-effects model |
|
GG+ GC vs. CC |
61.6% |
0.004 |
1.19 |
1.04,1.34 |
0.011 |
Random-effects model |
|
GG vs. GC+CC |
60.5% |
0.005 |
1.20 |
1.06,1.25 |
0.028 |
Random-effects model |
|
GG vs. GC |
57.2% |
0.012 |
1.11 |
1.06,1.17 |
0.009 |
Random-effects model |
|
Prostate cancer |
5 (12169/13116) |
||||||
G vs. C |
31.0% |
0.203 |
1.08 |
1.03,1.13 |
0.005 |
Fixed-effects model |
|
GG+ GC vs. CC |
32.4% |
0.193 |
1.11 |
1.04,1.18 |
0.003 |
Fixed-effects model |
|
GG vs. GC+CC |
24.0% |
0.254 |
1.13 |
1.05,1.22 |
0.008 |
Fixed-effects model |
|
GG vs. GC |
15.4% |
0.315 |
1.07 |
1.02,1.12 |
0.003 |
Fixed-effects model |
|
Lung Cancer |
4 (3203/3332) |
||||||
G vs. C |
0.0% |
0.817 |
1.08 |
1.02,1.15 |
0.003 |
Fixed-effects model |
|
GG+ GC vs. CC |
0.0% |
0.912 |
1.06 |
1.01,1.11 |
0.002 |
Fixed-effects model |
|
GG vs. GC+CC |
25.4% |
0.258 |
1.07 |
1.03,1.12 |
<0.001 |
Fixed-effects model |
|
GG vs. GC |
0.0% |
0.745 |
1.10 |
1.03,1.17 |
0.003 |
Fixed-effects model |
|
Glioma |
3 (1082/1701) |
||||||
G vs. C |
0.0% |
0.482 |
1.28 |
1.13,1.46 |
< 0.001 |
Fixed-effects model |
|
GG+ GC vs. CC |
67.6% |
0.046 |
1.15 |
1.05,1.26 |
0.021 |
Random-effects model |
|
GG vs. GC+CC |
77.9% |
0.011 |
1.50 |
1.03,2.17 |
0.035 |
Random-effects model |
|
GG vs. GC |
88.7% |
0.000 |
1.55 |
1.05,2.72 |
0.012 |
Random-effects model |
|
Multiple myeloma |
5 (6013/6471) |
||||||
G vs. C |
0.0% |
0.901 |
1.06 |
0.88,1.30 |
0.559 |
Fixed-effects model |
|
GG+ GC vs. CC |
0.0% |
0.987 |
1.00 |
0.66,1.53 |
0.992 |
Fixed-effects model |
|
GG vs. GC+CC |
0.0% |
0.617 |
0.95 |
0.70,1.28 |
0.733 |
Fixed-effects model |
|
GG vs. GC |
0.0% |
0.737 |
1.01 |
0.73,1.38 |
0.961 |
Fixed-effects model |
|
Non-Hodgkin’s lymphoma |
4 (5609/5649) |
||||||
G vs. C |
60.9% |
0.053 |
1.25 |
1.01,1.51 |
0.049 |
Random-effects model |
|
GG+ GC vs. CC |
11.2% |
0.337 |
1.26 |
1.03,1.54 |
0.022 |
Fixed-effects model |
|
GG vs. GC+CC |
50.3% |
0.110 |
1.20 |
1.04,1.40 |
0.015 |
Random-effects model |
|
GG vs. GC |
20.1% |
0.289 |
1.15 |
1.08,1.35 |
0.008 |
Fixed-effects model |
|
Hodgkin’s lymphoma |
3 (533/484) |
||||||
G vs. C |
16.7% |
0.301 |
1.22 |
1.02,1.45 |
0.030 |
Fixed-effects model |
|
GG+ GC vs. CC |
0.0% |
0.460 |
1.25 |
1.02,1.73 |
0.043 |
Fixed-effects model |
|
GG vs. GC+CC |
0.0% |
0.434 |
1.32 |
1.02,1.73 |
0.037 |
Fixed-effects model |
|
GG vs. GC |
0.0% |
0.601 |
1.28 |
1.08,1.68 |
0.013 |
Fixed-effects model |
|
Meta-analysis of rs1800796 polymorphism and cancer risk
Twenty-one studies reported the association between rs1800796 and cancer risk. Our results showed that rs1800796 was significantly associated with increased cancer risk in allelic, dominant, recessive, and additive models (OR = 1.11, 95% CI: 1.04, 1.18, P < 0.001, allelic models respectively) (Table 1). Subgroup analysis indicated that rs1800796 was significantly associated with increased risk of lung cancer (OR = 1.23, 95% CI: 1.11, 1.36, P = 0.002, allelic models respectively) (Table 4), prostate cancer (OR = 1.13, 95% CI: 1.04, 1.23, P = 0.002, allelic models respectively) (Table 4) and colorectal cancer (OR = 1.07, 95% CI: 1.04, 1.23, P < 0.001, allelic models respectively) (Table 4) but not gastric cancer (OR = 1.03, 95% CI: 0.82, 1.29, P = 0.786, allelic models respectively) (Table 4) in all four gene model. Furthermore, rs1800796 was associated with a significantly risk of cancer in Asia (OR = 1.08, 95% CI: 1.03, 1.14, P < 0.001, allelic models respectively) (Table 2) and Caucasian (OR = 1.05, 95% CI: 1.01, 1.10, P-0.003, allelic models respectively) (Table 2) in all four gene model.
Table 4: Subground of analyses of rs1800796 polymorphism and cancer risk
rs1800796 |
No.of studies |
Heterogeneity |
OR |
95% CI |
P value |
Model |
|
|---|---|---|---|---|---|---|---|
Cancer type |
I2 |
P value |
|||||
Lung cancer |
6 (1974/2879) |
||||||
C vs. G |
55.6% |
0.046 |
1.23 |
1.11,1.36 |
0.002 |
Random-effects model |
|
CC+ CG vs. GG |
57.4% |
0.039 |
1.17 |
1.09,1.26 |
0.012 |
Random-effects model |
|
CC vs. CG+GG |
62.0% |
0.022 |
1.15 |
1.05,1.26 |
0.012 |
Random-effects model |
|
CC vs. CG |
66.2% |
0.011 |
1.18 |
1.11,1.27 |
0.008 |
Random-effects model |
|
Prostate cancer |
5 (2360/3872) |
||||||
C vs. G |
0.0% |
0.803 |
1.13 |
1.04,1.23 |
0.002 |
Fixed-effects model |
|
CC+ CG vs. GG |
0.0% |
0.623 |
1.18 |
1.09,1.25 |
0.018 |
Fixed-effects model |
|
CC vs. CG+GG |
0.0% |
0.493 |
1.19 |
1.07,1.32 |
0.015 |
Fixed-effects model |
|
CC vs. CG |
13.5% |
0.328 |
1.16 |
1.06,1.28 |
0.014 |
Fixed-effects model |
|
Colorectal cancer |
2 (2581/3363) |
||||||
C vs. G |
0.0% |
0.826 |
1.07 |
1.03,1.12 |
< 0.001 |
Fixed-effects model |
|
CC+ CG vs. GG |
0.0% |
0.859 |
1.08 |
1.02,1.15 |
< 0.001 |
Fixed-effects model |
|
CC vs. CG+GG |
0.0% |
0.865 |
1.10 |
1.02,1.19 |
0.006 |
Fixed-effects model |
|
CC vs. CG |
0.0% |
0.905 |
1.15 |
1.04,1.27 |
0.009 |
Fixed-effects model |
|
Gastric cancer |
2 (365/395) |
||||||
C vs. G |
0.0% |
0.910 |
1.03 |
0.82,1.29 |
0.786 |
Fixed-effects model |
|
CC+ CG vs. GG |
0.0% |
0.380 |
1.05 |
0.62,1.80 |
0.848 |
Fixed-effects model |
|
CC vs. CG+GG |
0.0% |
0.602 |
1.04 |
0.78,1.38 |
0.807 |
Fixed-effects model |
|
CC vs. CG |
26.6% |
0.256 |
1.05 |
0.78,1.41 |
0.757 |
Fixed-effects model |
|
Meta-analysis of rs1800797 polymorphism and cancer risk
Seventeen studies reported the association between rs1800797 and cancer risk. Our results showed that rs1800797 was significantly associated with increased cancer risk in allelic, dominant, recessive, and additive models (OR = 1.04, 95% CI: 1.01, 1.08, P = 0.002, allelic models respectively) (Table 1). Subgroup analysis indicated that rs1800797 has significant association in breast cancer (OR = 1.14, 95% CI: 1.06, 1.23, P = 0.002, allelic models respectively) (Table 5), non-Hodgkin’s lymphoma (OR = 1.09, 95% CI: 1.03, 1.05, P = 0.006, allelic models respectively) (Table 5), B-NHL (OR= 1.10, 95% CI: 1.03, 1.18, P = 0.006, allelic models respectively) (Table 5) and DLCBL (OR = 1.10, 95% CI: 1.01, 1.20, P = 0.006, allelic models respectively) (Table 5) but not gastric cancer (OR = 1.04, 95% CI: 0.93, 1.15, P = 0.530, allelic models respectively) (Table 5) in all four gene model. Besides, rs1800797 was associated with a significantly higher risk of cancer in Caucasian (OR= 1.04, 95% CI: 1.01, 1.08, P = 0.041, allelic models respectively) (Table 2) but not in Asia (OR = 1.23, 95% CI: 0.79, 2.04, P = 0.326, allelic models respectively) (Table 2) in all four gene model.
Table 5: Subground of analyses of rs1800797 polymorphism and cancer risk
rs1800797 |
No.of studies |
Heterogeneity |
OR |
95% CI |
P value |
Model |
|
|---|---|---|---|---|---|---|---|
Cancer type |
I2 |
P value |
|||||
Breast Cancer |
2 (1164/1388) |
||||||
G vs. A |
0.0% |
0.705 |
1.14 |
1.06,1.23 |
0.002 |
Fixed-effects model |
|
GG+ GA vs. AA |
0.0% |
0.923 |
1.09 |
1.02,1.16 |
< 0.001 |
Fixed-effects model |
|
GG vs. GA+AA |
0.0% |
0.454 |
1.17 |
1.09,1.15 |
0.003 |
Fixed-effects model |
|
GG vs. GA |
0.0% |
0.365 |
1.06 |
1.02,1.11 |
0.003 |
Fixed-effects model |
|
Gastric cancer |
2 (286/316) |
||||||
G vs. A |
0.0% |
0.879 |
1.04 |
0.93,1.15 |
0.530 |
Fixed-effects model |
|
GG+ GA vs. AA |
0.0% |
0.692 |
1.01 |
0.82,1.24 |
0.936 |
Fixed-effects model |
|
GG vs. GA+AA |
0.0% |
0.662 |
1.06 |
0.92,1.23 |
0.429 |
Fixed-effects model |
|
GG vs. GA |
4.0% |
0.353 |
0.99 |
0.72,1.35 |
0.934 |
Fixed-effects model |
|
Non-Hodgkin’s lymphoma |
4 (5729/6036) |
||||||
G vs. A |
0.0% |
0.554 |
1.09 |
1.03,1.15 |
0.006 |
Fixed-effects model |
|
GG+ GA vs. AA |
0.0% |
0.497 |
1.07 |
1.02,1.13 |
0.002 |
Fixed-effects model |
|
GG vs. GA+AA |
32.2% |
0.219 |
1.12 |
1.04,1.21 |
0.008 |
Fixed-effects model |
|
GG vs. GA |
67.6% |
0.026 |
1.19 |
1.06,1.32 |
0.015 |
Random-effects model |
|
B-cell lymphoma |
3 (2161/2018) |
||||||
G vs. A |
0.0% |
0.736 |
1.10 |
1.03,1.18 |
0.006 |
Fixed-effects model |
|
GG+ GA vs. AA |
0.0% |
0.389 |
0.83 |
0.50,1.37 |
0.462 |
Fixed-effects model |
|
GG vs. GA+AA |
0.0% |
0.603 |
1.39 |
1.12,1.67 |
0.007 |
Fixed-effects model |
|
GG vs. GA |
58.3% |
0.091 |
1.52 |
1.21,1.84 |
0.018 |
Random-effects model |
|
DLCBL |
4 (5388/7026) |
||||||
G vs. A |
6.3% |
0.344 |
1.10 |
1.01,1.20 |
0.006 |
Fixed-effects model |
|
GG+ GA vs. AA |
0.0% |
0.759 |
1.06 |
1.01,1.12 |
< 0.001 |
Fixed-effects model |
|
GG vs. GA+AA |
0.0% |
0.683 |
1.13 |
1.03,1.24 |
0.003 |
Fixed-effects model |
|
GG vs. GA |
0.0% |
0.830 |
1.16 |
1.05,1.28 |
0.006 |
Fixed-effects model |
|
DLCBL: diffuse large B-cell lymphoma.
Table 6: Meta-analysis of IL-6 promoter polymorphisms and cancer prognosis
Genetic model |
No.of studies |
Heterogeneity |
HR |
95% CI |
P value |
Model |
|
|---|---|---|---|---|---|---|---|
I2 |
P value |
||||||
rs1800795 |
10 (7640/8361) |
||||||
GG vs. GC+CC |
0.088 |
43.6% |
1.17 |
1.07,1.36 |
< 0.001 |
Fixed-effects model |
|
CC VS. GC+GG |
0.610 |
0.0% |
1.51 |
1.09,2.13 |
< 0.001 |
Fixed-effects model |
|
rs1800796 |
2 (452/538) |
||||||
GG vs. GC+CC |
0.326 |
0.0% |
1.16 |
1.07,2.42 |
< 0.001 |
Fixed-effects model |
|
rs1800797 |
3 (892/951) |
||||||
GG vs. GA+AA |
0.416 |
0.0% |
1.23 |
1.11,1.37 |
< 0.001 |
Fixed-effects model |
|
Meta-analysis of IL-6 promoter polymorphisms and cancer prognosis
Twelve studies reported the association between IL-6 promoter polymorphisms and cancer prognosis. Prognostic meta-analyses were performed in a double gene model: CC vs. GC+GG and GG vs. GC+CC in rs1800795, GG vs. GC+CC in rs1800796 and GG vs. GA+AA in rs1800797. Our results showed that rs1800795, rs1800796 and rs1800797 were significantly associated with cancer prognosis (Table 6).
Sensitivity analysis
Sensitivity analysis was conducted to assess the stability of the results. The results show four genetic model were stable in Supplementary Figures 1–3.
Publication bias
Each study in this meta-analysis was performed to evaluate the publication bias by both Begg’s funnel plot and Egger’s test. The results show no obvious evidence of publication bias was found in allelic, dominant, recessive or additive genetic model in Table 7.
Table 7: Publication bias analysis of the meta-analysis
Genetic model |
Test |
t |
95% CI |
P |
|---|---|---|---|---|
rs1800795 |
||||
G vs. C |
Begg’s test |
0.853 |
||
Egger’s test |
-1.49 |
-3.43,0.48 |
0.139 |
|
GG+ GC vs. CC |
Begg’s test |
0.272 |
||
Egger’s test |
-4.09 |
-0.84,-027 |
0.125 |
|
GG vs. GC+CC |
Begg’s test |
0.472 |
||
Egger’s test |
-3.27 |
-5.21,1.11 |
0.086 |
|
GG vs. GC |
Begg’s test |
0.791 |
||
Egger’s test |
-1.74 |
-0.48,6.99 |
0.403 |
|
rs1800796 |
||||
C vs. G |
Begg’s test |
0.602 |
||
Egger’s test |
-4.82 |
-2.60,1.17 |
0.130 |
|
CC+ CG vs. GG |
Begg’s test |
0.117 |
||
Egger’s test |
-9.04 |
-0.09,0.02 |
0.070 |
|
CC vs. CG+GG |
Begg’s test |
0.602 |
||
Egger’s test |
-5.03 |
-3.15,1.36 |
0.125 |
|
CC vs. CG |
Begg’s test |
0.602 |
||
Egger’s test |
-5.22 |
-2.82,1.17 |
0.121 |
|
rs1800797 |
||||
G vs. A |
Begg’s test |
0.713 |
||
Egger’s test |
-1.23 |
-8.24,2.07 |
0.230 |
|
GG+ GA vs. AA |
Begg’s test /p> |
0.890 |
||
Egger’s test |
-1.29 |
-0.87,0.20 |
0.211 |
|
GG vs. GA+AA |
Begg’s test |
0.931 |
||
Egger’s test |
-0.86 |
-17.0,6.89 |
0.395 |
|
GG vs. GA |
Begg’s test |
0.973 |
||
Egger’s test |
2.28 |
0.73,14.4 |
0.531 |
DISCUSSION
Cancer is now a public health crisis, affecting millions of people in both developed and developing countries. By 2020, the disease is forecasted to be the major cause of morbidity and mortality in most developing nations [107]. To improve this embarrassing situation, risk factors concerning cancer should be identified timely and controlled effectively. The etiology of cancer involves both genetic and environmental factors. Therefore, understanding the impact of genetic factors on cancer will help to prevent cancer. IL-6 is a confirmed pleiotropic pro-inflammatory cytokine associated with cardiovascular diseases. Elevated expression of IL-6 and its major effector have been implicated in the different stages of cancer development, including initiation, promotion, malignant conversion, invasion, and metastasis [2].
Several recent meta-analysis have focused on the association between IL-6 promoter polymorphisms and cancer risk. Two meta-analysis showed that rs1800795 polymorphism increased the risk of prostate cancer and cervical cancer [108, 109]. Though, the result same with ours, it still exist some problems. On the one hand, single case-control studies with small sample sizes may have weak statistical power, thereby interfering with the precision of their results. On the another hand, the quantity of SNPs involving in their meta-analysis was smaller, which weak the persuasive power of their research. Additionally, no meta-analyses concerning the relationship between IL-6 promoter polymorphisms and cancer prognosis.
In this current meta-analysis was based on 97 case-control study, with 80361 cases and 78712 control from sixteen countries, thus, this meta-analysis provides the most up-to-date epidemiological evidence supporting IL-6 promoter polymorphisms were significantly associated with the susceptibility and prognosis of cancer. To our knowledge, this is the first complete study to identify the potential association between IL-6 promoter and cancer risk and prognosis. However, we also found rs1800795 was not associated with gastric cancer and multiple myeloma, this may be due to tumor heterogeneity or insufficient statistical power to check an association. therefore, a greater number of original case-control studies must be performed to further evaluate the association between the IL-6 promoter polymorphisms and different cancer types.
Although, we performed this meta-analysis very carefully, however, some limitations must be considered in the current meta-analysis. Firstly, we performed stratification only by ethnicity and cancer type, without referring other factors. Further research should be conducted in different sex of population. Secondly, we only select literature that written by English, other language should be chosen in the further. Thirdly, a lack of original data limited further evaluations of the potential gene-gene and gene-environment interactions.
In conclusion, our findings underscore the notion that IL-6 promoter polymorphisms were significantly associated with the susceptibility and prognosis of cancer. In the future, large-scale case-control and population based association studies must be performed in the future to validate the risk identified in the current meta-analysis, and investigate the effect of potential gene-gene and gene-environment interactions on cancer risk.
MATERIALS AND METHODS
Search strategy and selection criteria
The selection process is shown in the flow chart (Figure 1). We searched PubMed and Embase databases up to April, 2017, with keywords including “IL-6” or “interleukin-6” and “single nucleotide polymorphism” or “SNP” and “cancer” or “tumor”. Eligible studies were choosing and other relevant publications were also examined.
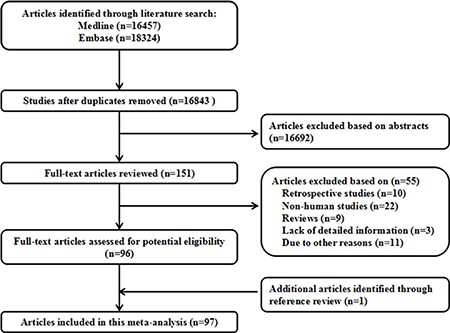
Figure 1: Flow diagram of the study selection process.
Data extraction
The following information in studies were investigated by two independent researchers: (1) first author; (2) publication year; (3) country; (4) cancer type; (5) cases and controls sample size; (6) genotype.
Statistical analysis
STATA software 12.0 (STATA Corp, College Station, TX, USA) was used to evaluate the relationships between IL-6 promoter polymorphisms and cancer risk and prognosis. Studies were assessed by chi-square in control group under Hardy-Weinberg equilibrium (HWE) to calculate frequencies of IL-6 promoter, and if P < 0.05, study was considered to be disequilibrium. The strength of the relationship between IL-6 promoter polymorphisms and the risk of cancer were evaluated by odd ratios with corresponding 95% confidence intervals. The correlation between IL-6 promoter polymorphisms and prognosis of cancer were measured by hazard ratios (HRs). By using Q test and I2 statistic to assess heterogeneity among studies in rs1800795 in the allelic (G vs. C), dominant (GG+ GC vs. CC), recessive (GG vs. GC+CC) and additive (GG vs. GC), in rs1800796 in the allelic (C vs. G), dominant (CC+CG vs. GG), recessive (CC vs. CC+GG), and additive (CC vs. CG) genetic models and in rs1800797 in the allelic (G vs. A), dominant (GG+GA vs. AA), recessive (GG vs.GA+AA, and additive (GG vs. GA) genetic models. Random-effect model was chosen if PQ<0.10 or I2 >50%, otherwise, fixed-effect mode was applied. Sensitivity analysis was conducted to assess the stability of the results. Begg’s and Egger’s tests were used to assess the publication bias of each study.
Author contributions
Xingchun Peng, Jun Shi and Ming Sang performed search, Wanqun Sun, Xiaodong Sun and Jue Wang prepared tables and figures, Bin Li wrote the manuscript and performed power calculation.
ACKNOWLEDGMENTS AND FUNDING
No financial support and sponsorship support this work.
CONFLICTS OF INTERESTS
No conflicts of financail interests is stated by authors.
REFERENCES
1. Kishimoto T. Interleukin-6: from basic science to medicine--40 years in immunology. Annu Rev Immunol. 2005; 23:1–21.
2. Tchirkov A, Khalil T, Chautard E, Mokhtari K, Veronese L, Irthum B, Vago P, Kemeny JL, Verrelle P. Interleukin-6 gene amplification and shortened survival in glioblastoma patients. Br J Cancer. 2007; 96:474–6.
3. Blay JY, Farcet JP, Lavaud A, Radoux D, Chouaib S. Serum concentrations of cytokines in patients with Hodgkin’s disease. Eur J Cancer. 1994; 30A:321–4.
4. Winther KV, Jess T, Langholz E, Munkholm P, Binder V. Survival and cause-specific mortality in ulcerative colitis: follow-up of a population-based cohort in Copenhagen County. Gastroenterology. 2003; 125:1576–82.
5. Terry CF, Loukaci V, Green FR. Cooperative influence of genetic polymorphisms on interleukin 6 transcriptional regulation. J Biol Chem. 2000; 275:18138–44.
6. Bowcock AM, Kidd JR, Lathrop GM, Daneshvar L, May LT, Ray A, Sehgal PB, Kidd KK, Cavalli-Sforza LL. The human “interferon-beta 2/hepatocyte stimulating factor/interleukin-6” gene: DNA polymorphism studies and localization to chromosome 7p21. Genomics. 1988; 3:8–16.
7. Jones SA, Horiuchi S, Topley N, Yamamoto N, Fuller GM. The soluble interleukin 6 receptor: mechanisms of production and implications in disease. FASEB J. 2001; 15:43–58.
8. Vickers MA, Green FR, Terry C, Mayosi BM, Julier C, Lathrop M, Ratcliffe PJ, Watkins HC, Keavney B. Genotype at a promoter polymorphism of the interleukin-6 gene is associated with baseline levels of plasma C-reactive protein. Cardiovasc Res. 2002; 53:1029–34.
9. Tartour E, Gey A, Sastre-Garau X, Pannetier C, Mosseri V, Kourilsky P, Fridman WH. Analysis of interleukin 6 gene expression in cervical neoplasia using a quantitative polymerase chain reaction assay: evidence for enhanced interleukin 6 gene expression in invasive carcinoma. Cancer Res. 1994; 54:6243–8.
10. Chakraborty B, Vishnoi G, Gowda SH, Goswami B. Interleukin-6 gene-174 G/C promoter polymorphism and its association with clinical profile of patients with multiple myeloma. Asia Pac J Clin Oncol. 2017; 13:e402–07.
11. Ennas MG, Moore PS, Zucca M, Angelucci E, Cabras MG, Melis M, Gabbas A, Serpe R, Madeddu C, Scarpa A, Cocco P. Interleukin-1B (IL1B) and interleukin-6 (IL6) gene polymorphisms are associated with risk of chronic lymphocytic leukaemia. Hematol Oncol. 2008; 26:98–103.
12. Hulkkonen J, Vilpo J, Vilpo L, Koski T, Hurme M. Interleukin-1 beta, interleukin-1 receptor antagonist and interleukin-6 plasma levels and cytokine gene polymorphisms in chronic lymphocytic leukemia: correlation with prognostic parameters. Haematologica. 2000; 85:600–6.
13. Lan Q, Zheng T, Rothman N, Zhang Y, Wang SS, Shen M, Berndt SI, Zahm SH, Holford TR, Leaderer B, Yeager M, Welch R, Boyle P, et al. Cytokine polymorphisms in the Th1/Th2 pathway and susceptibility to non-Hodgkin lymphoma. Blood. 2006; 107:4101–8.
14. Mazur G, Bogunia-Kubik K, Wrobel T, Karabon L, Polak M, Kuliczkowski K, Lange A. IL-6 and IL-10 promoter gene polymorphisms do not associate with the susceptibility for multiple myeloma. Immunol Lett. 2005; 96:241–6.
15. Rausz E, Szilagyi A, Nedoszytko B, Lange M, Niedoszytko M, Lautner-Csorba O, Falus A, Aladzsity I, Kokai M, Valent P, Marschalko M, Hidvegi B, Szakonyi J, et al. Comparative analysis of IL6 and IL6 receptor gene polymorphisms in mastocytosis. Br J Haematol. 2013; 160:216–9.
16. Rothman N, Skibola CF, Wang SS, Morgan G, Lan Q, Smith MT, Spinelli JJ, Willett E, De Sanjose S, Cocco P, Berndt SI, Brennan P, Brooks-Wilson A, et al. Genetic variation in TNF and IL10 and risk of non-Hodgkin lymphoma: a report from the InterLymph Consortium. Lancet Oncol. 2006; 7:27–38.
17. Vasku JA, Vasku A, Goldbergova M, Vasku V. Heterozygote AG variant of -596 A/G IL-6 gene polymorphism is a marker for cutaneous T-cell lymphoma (CTCL). Clin Immunol. 2004; 113:256–60.
18. Wang SS, Cerhan JR, Hartge P, Davis S, Cozen W, Severson RK, Chatterjee N, Yeager M, Chanock SJ, Rothman N. Common genetic variants in proinflammatory and other immunoregulatory genes and risk for non-Hodgkin lymphoma. Cancer Res. 2006; 66:9771–80.
19. Zheng C, Huang DR, Bergenbrant S, Sundblad A, Osterborg A, Bjorkholm M, Holm G, Yi Q. Interleukin 6, tumour necrosis factor alpha, interleukin 1beta and interleukin 1 receptor antagonist promoter or coding gene polymorphisms in multiple myeloma. Br J Haematol. 2000; 109:39–45.
20. Deans C, Rose-Zerilli M, Wigmore S, Ross J, Howell M, Jackson A, Grimble R, Fearon K. Host cytokine genotype is related to adverse prognosis and systemic inflammation in gastro-oesophageal cancer. Ann Surg Oncol. 2007; 14:329–39.
21. Kamangar F, Abnet CC, Hutchinson AA, Newschaffer CJ, Helzlsouer K, Shugart YY, Pietinen P, Dawsey SM, Albanes D, Virtamo J, Taylor PR. Polymorphisms in inflammation-related genes and risk of gastric cancer (Finland). Cancer Causes Control. 2006; 17:117–25.
22. El-Omar EM, Rabkin CS, Gammon MD, Vaughan TL, Risch HA, Schoenberg JB, Stanford JL, Mayne ST, Goedert J, Blot WJ, Fraumeni JF Jr, Chow WH. Increased risk of noncardia gastric cancer associated with proinflammatory cytokine gene polymorphisms. Gastroenterology. 2003; 124:1193–201.
23. Crusius JB, Canzian F, Capella G, Pena AS, Pera G, Sala N, Agudo A, Rico F, Del Giudice G, Palli D, Plebani M, Boeing H, Bueno-de-Mesquita HB, et al. Cytokine gene polymorphisms and the risk of adenocarcinoma of the stomach in the European prospective investigation into cancer and nutrition (EPIC-EURGAST). Ann Oncol. 2008; 19:1894–902.
24. Ognjanovic S, Yamamoto J, Saltzman B, Franke A, Ognjanovic M, Yokochi L, Vogt T, Decker R, Le Marchand L. Serum CRP and IL-6, genetic variants and risk of colorectal adenoma in a multiethnic population. Cancer Causes Control. 2010; 21:1131–8.
25. Tsilidis KK, Helzlsouer KJ, Smith MW, Grinberg V, Hoffman-Bolton J, Clipp SL, Visvanathan K, Platz EA. Association of common polymorphisms in IL10, and in other genes related to inflammatory response and obesity with colorectal cancer. Cancer Causes Control. 2009; 20:1739–51.
26. Wilkening S, Tavelin B, Canzian F, Enquist K, Palmqvist R, Altieri A, Hallmans G, Hemminki K, Lenner P, Forsti A. Interleukin promoter polymorphisms and prognosis in colorectal cancer. Carcinogenesis. 2008; 29:1202–6.
27. Kury S, Buecher B, Robiou-du-Pont S, Scoul C, Colman H, Le Neel T, Le Houerou C, Faroux R, Ollivry J, Lafraise B, Chupin LD, Sebille V, Bezieau S. Low-penetrance alleles predisposing to sporadic colorectal cancers: a French case-controlled genetic association study. BMC Cancer. 2008; 8:326.
28. Vogel U, Christensen J, Dybdahl M, Friis S, Hansen RD, Wallin H, Nexo BA, Raaschou-Nielsen O, Andersen PS, Overvad K, Tjonneland A. Prospective study of interaction between alcohol, NSAID use and polymorphisms in genes involved in the inflammatory response in relation to risk of colorectal cancer. Mutat Res. 2007; 624:88–100.
29. Slattery ML, Wolff RK, Herrick J, Caan BJ, Samowitz W. Tumor markers and rectal cancer: support for an inflammation-related pathway. Int J Cancer. 2009; 125:1698–704.
30. Theodoropoulos G, Papaconstantinou I, Felekouras E, Nikiteas N, Karakitsos P, Panoussopoulos D, Lazaris A, Patsouris E, Bramis J, Gazouli M. Relation between common polymorphisms in genes related to inflammatory response and colorectal cancer. World J Gastroenterol. 2006; 12:5037–43.
31. Gunter MJ, Canzian F, Landi S, Chanock SJ, Sinha R, Rothman N. Inflammation-related gene polymorphisms and colorectal adenoma. Cancer Epidemiol Biomarkers Prev. 2006; 15:1126–31.
32. Landi S, Moreno V, Gioia-Patricola L, Guino E, Navarro M, de Oca J, Capella G, Canzian F, and Bellvitge Colorectal Cancer Study Group. Association of common polymorphisms in inflammatory genes interleukin (IL)6, IL8, tumor necrosis factor alpha, NFKB1, and peroxisome proliferator-activated receptor gamma with colorectal cancer. Cancer Res. 2003; 63:3560–6.
33. Gangwar R, Mittal B, Mittal RD. Association of interleukin-6 -174G>C promoter polymorphism with risk of cervical cancer. Int J Biol Markers. 2009; 24:11–6.
34. Cacev T, Jokic M, Loncar B, Krizanac S, Kapitanovic S. Interleukin-6-174 G/C polymorphism is not associated with IL-6 expression and susceptibility to sporadic colon cancer. DNA Cell Biol. 2010; 29:177–82.
35. Vasku A, Vokurka J, Bienertova-Vasku J. Obesity-related genes variability in Czech patients with sporadic colorectal cancer: preliminary results. Int J Colorectal Dis. 2009; 24:289–94.
36. Shi WJ, Liu H, Wu D, Tang ZH, Shen YC, Guo L. Stratification analysis and case-control study of relationships between interleukin-6 gene polymorphisms and cervical cancer risk in a Chinese population. Asian Pac J Cancer Prev. 2014; 15:7357–62.
37. Nogueira de Souza NC, Brenna SM, Campos F, Syrjanen KJ, Baracat EC, Silva ID. Interleukin-6 polymorphisms and the risk of cervical cancer. Int J Gynecol Cancer. 2006; 16:1278–82.
38. Lima SF, Tavares MM, Macedo JL, Oliveira RS, Heraclio SA, Maia MM, Souza PR, Moura R, Crovella S. Influence of IL-6, IL-8, and TGF-beta1 gene polymorphisms on the risk of human papillomavirus-infection in women from Pernambuco, Brazil. Mem Inst Oswaldo Cruz. 2016; 111:663–9.
39. Grimm C, Watrowski R, Baumuhlner K, Natter C, Tong D, Wolf A, Zeillinger R, Leodolter S, Reinthaller A, Hefler L. Genetic variations of interleukin-1 and -6 genes and risk of cervical intraepithelial neoplasia. Gynecol Oncol. 2011; 121:537–41.
40. Hohaus S, Giachelia M, Di Febo A, Martini M, Massini G, Vannata B, D’Alo F, Guidi F, Greco M, Pierconti F, Larocca LM, Voso MT, Leone G. Polymorphism in cytokine genes as prognostic markers in Hodgkin’s lymphoma. Ann Oncol. 2007; 18:1376–81.
41. Duch CR, Figueiredo MS, Ribas C, Almeida MS, Colleoni GW, Bordin JO. Analysis of polymorphism at site -174 G/C of interleukin-6 promoter region in multiple myeloma. Braz J Med Biol Res. 2007; 40:265–7.
42. Andrie E, Michos A, Kalampoki V, Pourtsidis A, Moschovi M, Polychronopoulou S, Athanasiadou-Piperopoulou F, Kalmanti M, Hatzakis A, Paraskevis D, Nieters A, Petridou ET. Genetic variants in immunoregulatory genes and risk for childhood lymphomas. Eur J Haematol. 2009; 83:334–42.
43. Aladzsity I, Kovacs M, Semsei A, Falus A, Szilagyi A, Karadi I, Varga G, Fust G, Varkonyi J. Comparative analysis of IL6 promoter and receptor polymorphisms in myelodysplasia and multiple myeloma. Leuk Res. 2009; 33:1570–3.
44. Madeleine MM, Johnson LG, Malkki M, Resler AJ, Petersdorf EW, McKnight B, Malone KE. Genetic variation in proinflammatory cytokines IL6, IL6R, TNF-region, and TNFRSF1A and risk of breast cancer. Breast Cancer Res Treat. 2011; 129:887–99.
45. Joshi N, Kannan S, Kotian N, Bhat S, Kale M, Hake S. Interleukin 6 -174G>C polymorphism and cancer risk: meta-analysis reveals a site dependent differential influence in Ancestral North Indians. Hum Immunol. 2014; 75:901–8.
46. Dossus L, Kaaks R, Canzian F, Albanes D, Berndt SI, Boeing H, Buring J, Chanock SJ, Clavel-Chapelon F, Feigelson HS, Gaziano JM, Giovannucci E, Gonzalez C, et al. PTGS2 and IL6 genetic variation and risk of breast and prostate cancer: results from the Breast and Prostate Cancer Cohort Consortium (BPC3). Carcinogenesis. 2010; 31:455–61.
47. Cherel M, Campion L, Bezieau S, Campone M, Charrier J, Gaschet J, Ricolleau G, Gouraud W, Charbonnel C, Jezequel P. Molecular screening of interleukin-6 gene promoter and influence of -174G/C polymorphism on breast cancer. Cytokine. 2009; 47:214–23.
48. Slattery ML, Curtin K, Sweeney C, Wolff RK, Baumgartner RN, Baumgartner KB, Giuliano AR, Byers T. Modifying effects of IL-6 polymorphisms on body size-associated breast cancer risk. Obesity (Silver Spring). 2008; 16:339–47.
49. Slattery ML, Curtin K, Baumgartner R, Sweeney C, Byers T, Giuliano AR, Baumgartner KB, Wolff RR. IL6, aspirin, nonsteroidal anti-inflammatory drugs, and breast cancer risk in women living in the southwestern United States. Cancer Epidemiol Biomarkers Prev. 2007; 16:747–55.
50. Slattery ML, Wolff RK, Curtin K, Fitzpatrick F, Herrick J, Potter JD, Caan BJ, Samowitz WS. Colon tumor mutations and epigenetic changes associated with genetic polymorphism: insight into disease pathways. Mutat Res. 2009; 660:12–21.
51. Vogel U, Christensen J, Wallin H, Friis S, Nexo BA, Raaschou-Nielsen O, Overvad K, Tjonneland A. Polymorphisms in genes involved in the inflammatory response and interaction with NSAID use or smoking in relation to lung cancer risk in a prospective study. Mutat Res. 2008; 639:89–100.
52. Balasubramanian SP, Azmy IA, Higham SE, Wilson AG, Cross SS, Cox A, Brown NJ, Reed MW. Interleukin gene polymorphisms and breast cancer: a case control study and systematic literature review. BMC Cancer. 2006; 6:188.
53. Snoussi K, Strosberg AD, Bouaouina N, Ben Ahmed S, Chouchane L. Genetic variation in pro-inflammatory cytokines (interleukin-1beta, interleukin-1alpha and interleukin-6) associated with the aggressive forms, survival, and relapse prediction of breast carcinoma. Eur Cytokine Netw. 2005; 16:253–60.
54. Hefler LA, Grimm C, Lantzsch T, Lampe D, Leodolter S, Koelbl H, Heinze G, Reinthaller A, Tong-Cacsire D, Tempfer C, Zeillinger R. Interleukin-1 and interleukin-6 gene polymorphisms and the risk of breast cancer in caucasian women. Clin Cancer Res. 2005; 11:5718–21.
55. Litovkin KV, Domenyuk VP, Bubnov VV, Zaporozhan VN. Interleukin-6 -174G/C polymorphism in breast cancer and uterine leiomyoma patients: a population-based case control study. Exp Oncol. 2007; 29:295–8.
56. Smith KC, Bateman AC, Fussell HM, Howell WM. Cytokine gene polymorphisms and breast cancer susceptibility and prognosis. Eur J Immunogenet. 2004; 31:167–73.
57. Pierce BL, Biggs ML, DeCambre M, Reiner AP, Li C, Fitzpatrick A, Carlson CS, Stanford JL, Austin MA. C-reactive protein, interleukin-6, and prostate cancer risk in men aged 65 years and older. Cancer Causes Control. 2009; 20:1193–203.
58. Brenner AV, Butler MA, Wang SS, Ruder AM, Rothman N, Schulte PA, Chanock SJ, Fine HA, Linet MS, Inskip PD. Single-nucleotide polymorphisms in selected cytokine genes and risk of adult glioma. Carcinogenesis. 2007; 28:2543–7.
59. Smallwood L, Allcock R, van Bockxmeer F, Warrington N, Palmer LJ, Iacopetta B, Norman PE. Polymorphisms of the interleukin-6 gene promoter and abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. 2008; 35:31–6.
60. Gonzalez-Zuloeta Ladd AM, Arias Vasquez A, Witteman J, Uitterlinden AG, Coebergh JW, Hofman A, Stricker BH, van Duijn CM. Interleukin 6 G-174 C polymorphism and breast cancer risk. Eur J Epidemiol. 2006; 21:373–6.
61. Abuli A, Fernandez-Rozadilla C, Alonso-Espinaco V, Munoz J, Gonzalo V, Bessa X, Gonzalez D, Clofent J, Cubiella J, Morillas JD, Rigau J, Latorre M, Fernandez-Banares F, et al, and Gastrointestinal Oncology Group of the Spanish Gastroenterological Association. Case-control study for colorectal cancer genetic susceptibility in EPICOLON: previously identified variants and mucins. BMC Cancer. 2011; 11:339.
62. Pooja S, Chaudhary P, Nayak LV, Rajender S, Saini KS, Deol D, Kumar S, Bid HK, Konwar R. Polymorphic variations in IL-1beta, IL-6 and IL-10 genes, their circulating serum levels and breast cancer risk in Indian women. Cytokine. 2012; 60:122–8.
63. Pohjanen VM, Koivurova OP, Makinen JM, Karhukorpi JM, Joensuu T, Koistinen PO, Valtonen JM, Niemela SE, Karttunen RA, Karttunen TJ. Interleukin 6 gene polymorphism -174 is associated with the diffuse type gastric carcinoma. Genes Chromosomes Cancer. 2013; 52:976–82.
64. Totaro F, Cimmino F, Pignataro P, Acierno G, De Mariano M, Longo L, Tonini GP, Iolascon A, Capasso M. Impact of interleukin-6 -174 G>C gene promoter polymorphism on neuroblastoma. PLoS One. 2013; 8:e76810.
65. Mandal S, Abebe F, Chaudhary J. -174G/C polymorphism in the interleukin-6 promoter is differently associated with prostate cancer incidence depending on race. Genet Mol Res. 2014; 13:139–51.
66. Oduor CI, Chelimo K, Ouma C, Mulama DH, Foley J, Vulule J, Bailey JA, Moormann AM. Interleukin-6 and interleukin-10 gene promoter polymorphisms and risk of endemic Burkitt lymphoma. Am J Trop Med Hyg. 2014; 91:649–54.
67. Gu X, Shen Y, Fu L, Zuo HY, Yasen H, He P, Guo XH, Shi YW, Yusufu M. Polymorphic variation of inflammation-related genes and risk of non-Hodgkin lymphoma for Uygur and Han Chinese in Xinjiang. Asian Pac J Cancer Prev. 2014; 15:9177–83.
68. Talaat RM, Abdel-Aziz AM, El-Maadawy EA, Abdel-Bary N. CD38 and interleukin 6 gene polymorphism in egyptians with diffuse large B-cell lymphoma (DLBCL). Immunol Invest. 2015; 44:265–78.
69. Chen CH, Gong M, Yi QT, Guo JH. Role of interleukin-6 gene polymorphisms in the development of prostate cancer. Genet Mol Res. 2015; 14:13370–4.
70. Zidi S, Stayoussef M, Alsaleh BL, Gazouani E, Mezlini A, Ebrahim BH, Yacoubi-Loueslati B, Almawi WY. Relationships between Common and Novel Interleukin-6 Gene Polymorphisms and Risk of Cervical Cancer: a Case-Control Study. Pathol Oncol Res. 2017; 23:385–92.
71. Pu X, Gu Z, Wang X. Polymorphisms of the interleukin 6 gene and additional gene-gene interaction contribute to cervical cancer susceptibility in Eastern Chinese women. Arch Gynecol Obstet. 2016; 294:1305–10.
72. Ozgen AG, Karadeniz M, Erdogan M, Berdeli A, Saygili F, Yilmaz C. The (-174) G/C polymorphism in the interleukin-6 gene is associated with risk of papillary thyroid carcinoma in Turkish patients. J Endocrinol Invest. 2009; 32:491–4.
73. Schonfeld SJ, Bhatti P, Brown EE, Linet MS, Simon SL, Weinstock RM, Hutchinson AA, Stovall M, Preston DL, Alexander BH, Doody MM, Sigurdson AJ. Polymorphisms in oxidative stress and inflammation pathway genes, low-dose ionizing radiation, and the risk of breast cancer among US radiologic technologists. Cancer Causes Control. 2010; 21:1857–66.
74. Ahirwar D, Kesarwani P, Manchanda PK, Mandhani A, Mittal RD. Anti- and proinflammatory cytokine gene polymorphism and genetic predisposition: association with smoking, tumor stage and grade, and bacillus Calmette-Guerin immunotherapy in bladder cancer. Cancer Genet Cytogenet. 2008; 184:1–8.
75. Basturk B, Yavascaoglu I, Vuruskan H, Goral G, Oktay B, Oral HB. Cytokine gene polymorphisms as potential risk and protective factors in renal cell carcinoma. Cytokine. 2005; 30:41–5.
76. Berkovic MC, Jokic M, Marout J, Radosevic S, Zjacic-Rotkvic V, Kapitanovic S. IL-6–174 C/G polymorphism in the gastroenteropancreatic neuroendocrine tumors (GEP-NETs). Exp Mol Pathol. 2007; 83:474–9.
77. Campa D, Hung RJ, Mates D, Zaridze D, Szeszenia-Dabrowska N, Rudnai P, Lissowska J, Fabianova E, Bencko V, Foretova L, Janout V, Boffetta P, Brennan P, Canzian F. Lack of association between polymorphisms in inflammatory genes and lung cancer risk. Cancer Epidemiol Biomarkers Prev. 2005; 14:538–9.
78. Cordano P, Lake A, Shield L, Taylor GM, Alexander FE, Taylor PR, White J, Jarrett RF. Effect of IL-6 promoter polymorphism on incidence and outcome in Hodgkin’s lymphoma. Br J Haematol. 2005; 128:493–5.
79. Seifart C, Plagens A, Dempfle A, Clostermann U, Vogelmeier C, von Wichert P, Seifart U. TNF-alpha, TNF-beta, IL-6, and IL-10 polymorphisms in patients with lung cancer. Dis Markers. 2005; 21:157–65.
80. Kesarwani P, Ahirwar DK, Mandhani A, Mittal RD. Association between -174 G/C promoter polymorphism of the interleukin-6 gene and progression of prostate cancer in North Indian population. DNA Cell Biol. 2008; 27:505–10.
81. Malaponte G, Polesel J, Candido S, Sambataro D, Bevelacqua V, Anzaldi M, Vella N, Fiore V, Militello L, Mazzarino MC, Libra M, Signorelli SS. IL-6-174 G > C and MMP-9-1562 C > T polymorphisms are associated with increased risk of deep vein thrombosis in cancer patients. Cytokine. 2013; 62:64–9.
82. Michaud DS, Daugherty SE, Berndt SI, Platz EA, Yeager M, Crawford ED, Hsing A, Huang WY, Hayes RB. Genetic polymorphisms of interleukin-1B (IL-1B), IL-6, IL-8, and IL-10 and risk of prostate cancer. Cancer Res. 2006; 66:4525–30.
83. Ognjanovic S, Yuan JM, Chaptman AK, Fan Y, Yu MC. Genetic polymorphisms in the cytokine genes and risk of hepatocellular carcinoma in low-risk non-Asians of USA. Carcinogenesis. 2009; 30:758–62.
84. Vairaktaris E, Yapijakis C, Serefoglou Z, Avgoustidis D, Critselis E, Spyridonidou S, Vylliotis A, Derka S, Vassiliou S, Nkenke E, Patsouris E. Gene expression polymorphisms of interleukins-1 beta, -4, -6, -8, -10, and tumor necrosis factors-alpha, -beta: regression analysis of their effect upon oral squamous cell carcinoma. J Cancer Res Clin Oncol. 2008; 134:821–32.
85. Bushley AW, Ferrell R, McDuffie K, Terada KY, Carney ME, Thompson PJ, Wilkens LR, Tung KH, Ness RB, Goodman MT. Polymorphisms of interleukin (IL)-1alpha, IL-1beta, IL-6, IL-10, and IL-18 and the risk of ovarian cancer. Gynecol Oncol. 2004; 95:672–9.
86. Hwang IR, Hsu PI, Peterson LE, Gutierrez O, Kim JG, Graham DY, Yamaoka Y. Interleukin-6 genetic polymorphisms are not related to Helicobacter pylori-associated gastroduodenal diseases. Helicobacter. 2003; 8:142–8.
87. Bai L, Yu H, Wang H, Su H, Zhao J, Zhao Y. Genetic single-nucleotide polymorphisms of inflammation-related factors associated with risk of lung cancer. Med Oncol. 2013; 30:414.
88. Bao S, Yang W, Zhou S, Ye Z. Relationship between single nucleotide polymorphisms in -174G/C and -634C/G promoter region of interleukin-6 and prostate cancer. J Huazhong Univ Sci Technolog Med Sci. 2008; 28:693–6.
89. Chen J, Liu RY, Yang L, Zhao J, Zhao X, Lu D, Yi N, Han B, Chen XF, Zhang K, He J, Lei Z, Zhou Y, et al. A two-SNP IL-6 promoter haplotype is associated with increased lung cancer risk. J Cancer Res Clin Oncol. 2013; 139:231–42.
90. Kang JM, Kim N, Lee DH, Park JH, Lee MK, Kim JS, Jung HC, Song IS. The effects of genetic polymorphisms of IL-6, IL-8, and IL-10 on Helicobacter pylori-induced gastroduodenal diseases in Korea. J Clin Gastroenterol. 2009; 43:420–8.
91. Kiyohara C, Horiuchi T, Takayama K, Nakanishi Y. Genetic polymorphisms involved in the inflammatory response and lung cancer risk: a case-control study in Japan. Cytokine. 2014; 65:88–94.
92. Liang J, Liu X, Bi Z, Yin B, Xiao J, Liu H, Li Y. Relationship between gene polymorphisms of two cytokine genes (TNF-alpha and IL-6) and occurring of lung cancers in the ethnic group Han of China. Mol Biol Rep. 2013; 40:1541–6.
93. Lim WY, Chen Y, Ali SM, Chuah KL, Eng P, Leong SS, Lim E, Lim TK, Ng AW, Poh WT, Tee A, Teh M, Salim A, Seow A. Polymorphisms in inflammatory pathway genes, host factors and lung cancer risk in Chinese female never-smokers. Carcinogenesis. 2011; 32:522–9.
94. Sun J, Hedelin M, Zheng SL, Adami HO, Bensen J, Augustsson-Balter K, Chang B, Adolfsson J, Adams T, Turner A, Meyers DA, Isaacs WB, Xu J, Grönberg H. Interleukin-6 sequence variants are not associated with prostate cancer risk. Cancer Epidemiol Biomarkers Prev. 2004; 13:1677–9.
95. Tang S, Yuan Y, He Y, Pan D, Zhang Y, Liu Y, Liu Q, Zhang Z, Liu Z. Genetic polymorphism of interleukin-6 influences susceptibility to HBV-related hepatocellular carcinoma in a male Chinese Han population. Hum Immunol. 2014; 75:297–301.
96. Wang MH, Helzlsouer KJ, Smith MW, Hoffman-Bolton JA, Clipp SL, Grinberg V, De Marzo AM, Isaacs WB, Drake CG, Shugart YY, Platz EA. Association of IL10 and other immune response- and obesity-related genes with prostate cancer in CLUE II. Prostate. 2009; 69:874–85.
97. Seow A, Ng DP, Choo S, Eng P, Poh WT, Ming T, Wang YT. Joint effect of asthma/atopy and an IL-6 gene polymorphism on lung cancer risk among lifetime non-smoking Chinese women. Carcinogenesis. 2006; 27:1240–4.
98. Castro FA, Haimila K, Sareneva I, Schmitt M, Lorenzo J, Kunkel N, Kumar R, Forsti A, Kjellberg L, Hallmans G, Lehtinen M, Hemminki K, Pawlita M. Association of HLA-DRB1, interleukin-6 and cyclin D1 polymorphisms with cervical cancer in the Swedish population--a candidate gene approach. Int J Cancer. 2009; 125:1851–8.
99. Markkula A, Simonsson M, Ingvar C, Rose C, Jernstrom H. IL6 genotype, tumour ER-status, and treatment predicted disease-free survival in a prospective breast cancer cohort. BMC Cancer. 2014; 14:759.
100. DeMichele A, Martin AM, Mick R, Gor P, Wray L, Klein-Cabral M, Athanasiadis G, Colligan T, Stadtmauer E, Weber B. Interleukin-6 -174G-->C polymorphism is associated with improved outcome in high-risk breast cancer. Cancer Res. 2003; 63:8051–6.
101. Ghesquieres H, Maurer MJ, Casasnovas O, Ansell SM, Larrabee BR, Lech-Maranda E, Novak AJ, Borrel AL, Slager SL, Brice P, Allmer C, Brion A, Ziesmer SC, et al. Cytokine gene polymorphisms and progression-free survival in classical Hodgkin lymphoma by EBV status: results from two independent cohorts. Cytokine. 2013; 64: 523–31.
102. Iacopetta B, Grieu F, Joseph D. The -174 G/C gene polymorphism in interleukin-6 is associated with an aggressive breast cancer phenotype. Br J Cancer. 2004; 90:419–22.
103. Lagmay JP, London WB, Gross TG, Termuhlen A, Sullivan N, Axel A, Mundy B, Ranalli M, Canner J, McGrady P, Hall B. Prognostic significance of interleukin-6 single nucleotide polymorphism genotypes in neuroblastoma: rs1800795 (promoter) and rs8192284 (receptor). Clin Cancer Res. 2009; 15:5234–9.
104. Matsusaka S, Hanna DL, Cao S, Zhang W, Yang D, Ning Y, Sunakawa Y, Okazaki S, Berger MD, Miyamato Y, Parekh A, Stintzing S, Loupakis F, Lenz HJ. Prognostic Impact of IL6 Genetic Variants in Patients with Metastatic Colorectal Cancer Treated with Bevacizumab-Based Chemotherapy. Clin Cancer Res. 2016; 22:3218–26.
105. Ruzzo A, Catalano V, Canestrari E, Giacomini E, Santini D, Tonini G, Vincenzi B, Fiorentini G, Magnani M, Graziano F. Genetic modulation of the interleukin 6 (IL-6) system in patients with advanced gastric cancer: a background for an alternative target therapy. BMC Cancer. 2014; 14:357.
106. Skerrett DL, Moore EM, Bernstein DS, Vahdat L. Cytokine genotype polymorphisms in breast carcinoma: associations of TGF-beta1 with relapse. Cancer Invest. 2005; 23:208–14.
107. Wang H, Naghavi M, Allen C, Barber RM, Bhutta ZA, Carter A, Casey DC, Charlson FJ, Chen AZ, Coates MM, Coggeshall M, Dandona L, Dicker DJ, et al, and GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016; 388:1459–544.
108. Liu TZ, Guo ZQ, Wang T, Cao Y, Huang D, Wang XH. Meta-analysis of the role of IL-6 rs1800795 polymorphism in the susceptibility to prostate cancer: evidence based on 17 studies. Medicine (Baltimore). 2017; 96:e6126.
109. Liu H, Lyu D, Zhang Y, Sheng L, Tang N. Association Between the IL-6 rs1800795 Polymorphism and the Risk of Cervical Cancer: A Meta-Analysis of 1210 Cases and 1525 Controls. Technol Cancer Res Treat. 2017; 16:662–67.