
INTRODUCTION
The introduction of reduced intensity (RIC) allogeneic stem cell transplantation into the mainstay of clinical management of older patients with acute lymphoblastic leukemia (ALL) more than a decade ago [1] represented a significant paradigm change for clinicians treating this challenging segment of the acute leukemia field. As is the case for younger ALL patients, an allogeneic stem cell transplant endeavors to provide older patients with the best possibility for disease control, while remaining cognizant of the overarching principals of therapy for this unique patient population, namely minimizing treatment related toxicity and mortality [1–3]. Whereas standard chemotherapy based approaches have yielded for the most part disappointing results in this age group with long term survival of only 6–21% [4–8], transplant is increasingly being used in an attempt to improve on these suboptimal results. Yet, the benefit of transplantation in this age group is not as evident as that seen for younger patients, for example those at the 18–39 year age group where 5 year overall survival rates of 66% surpass by far the reported 22% survival rate for patients 60–69, as published recently by the Dutch cancer registry [9]. Moreover, given the substantial transplant related mortality and morbidity reported by several groups [2, 10–13], it remains unclear which patients derive the most benefit from a transplant based approach. Thus, defining specific patient subsets who would specifically benefit from transplantation is of utmost importance for patients and clinicians alike. Using the multicenter registry of the acute leukemia working party (ALWP) of the European Society of Blood and Marrow Transplantation (EBMT) we provide a current assessment of the clinical landscape for older ALL patients over the age of 60 undergoing allogeneic stem cell transplantation after a RIC regimen.
RESULTS
Patient, disease and transplant characteristics
In all, 142 patients were identified and their baseline clinical and laboratory data are summarized in Table 1. The median age of patients on the cohort was 62 (range 60–76 years) with a median follow-up period of 36 months (range 2–123 months). Notably, a little more than half of the cohort analyzed was Philadelphia chromosome positive. Fludarabine based regimens were the most frequently used approaches for conditioning prior to transplant whereas PB was the most commonly used source for stem cell grafts (135 patients; 95%). Donor was matched sibling for 66 patients, and 10/10 HLA matched unrelated donors for 76 patients. Of note, most Philadelphia chromosome positive patients were treated with tyrosine kinase inhibitors (TKI) prior to transplant (45 patients; 70%), and 20 patients received TKI post-transplant indicated either for prophylaxis (7 patients), positive minimal residual disease (MRD) studies (5 patients) or because of relapse (8 patients).
Table 1: Baseline characteristics of study population
Parameter |
N = 142 |
|---|---|
Follow up duration in m, median (range) |
36 (1.8–123.4 ) |
Age in years, median (range) |
62 (60–76) |
Gender, n (%) |
|
Male |
65 (45.7) |
Female |
77 (54.2) |
ALL type |
|
B-ALL |
126 (88.7) |
T-ALL |
11 (7.7) |
Other |
5 (3.5) |
Philadelphia Chromosome |
|
Ph negative |
59 (41.5) |
Ph positive |
83 (58.4) |
Donor type, n (%) |
|
Identical sibling |
66 (46.4) |
Matched unrelated |
76 (53.5) |
Stem cell source, n (%) |
|
Peripheral blood |
135 (95) |
Bone marrow |
7 (4.9) |
Conditioning regimen, n (%) |
|
Flu/Mel |
28 (19.7) |
Flu/Bu |
58 (40.8) |
Cy/Thio |
1 (0.7) |
Flu/Treo |
2 (1.4) |
Bu/Clo |
6 (4.2) |
Cy/Flu |
3 (2.1) |
Flu/Thio/BCNU |
11 (7.7) |
Cy/Treo |
1 (0.7) |
TBI |
32 (22.5) |
Donor-recipient CMV match, n (%) |
|
CMV D−/R− |
33 (23.4) |
CMV D+/R− |
13 (9.2) |
CMV D−/R+ |
39 (27.6) |
CMV D+/R+ |
56 (39.7) |
Missing |
1 |
Karnofsky score at transplant |
|
< 90 |
45 (33.8) |
≥ 90 |
88 (66.1) |
Missing |
9 |
HCT-CI |
|
0 |
41 (42.7) |
1–2 |
25 (26) |
≥ 3 |
30 (31.2) |
Missing |
46 |
Abbreviations: CMV, cytomegalovirus; Flu/Mel, fludarabine and melphalan; Flu/Bu, fludarabine and busulfan; Cy/Thio, cyclophosphamide and thiotepa; TBI, total body irradiation; HCT-CI, Hematopoietic Stem Cell Transplant Comorbidity Index.
Acute and chronic GVHD
The cumulative incidence of grade II-IV acute GVHD at 100 days was 29% (95% CI: 21%–37%) while the incidence of grade III-IV acute GVHD was 9% (95% CI: 5%–15%). As shown in the univariate analysis presented in Supplementary Table 1, patients transplanted from matched unrelated donors had significantly worse grade II-IV acute GVHD rates compared to patients transplanted from matched sibling donors (39% versus 16%; P = 0.001). As detailed in the multivariate analysis shown in Table 2, patients transplanted from URD experienced increased grade II-IV acute GVHD compared to patients receiving grafts from MSD (HR = 3.7, 95% CI, 1.75–7.8; P = 0.0005). Conversely, CMV D+/R+ status was also associated with a trend towards a higher rate of grade II-IV acute GVHD (HR = 1.79, 95% CI, 0.93–3.41; P = 0.07).
Table 2: Multivariate analysis of factors impacting on clinical outcome
Outcome |
Hazard ratio (95% CI) |
P |
|---|---|---|
RI |
||
URD versus MSD |
0.72 (0.39–1.31) |
0.28 |
Philadelphia chromosome positive ALL |
0.64 (0.35–1.15) |
0.14 |
NRM |
||
CMV D+/R+ versus others |
2.25 (1.09–4.66) |
0.028 |
LFS |
||
CMV D+/R+ versus others |
1.62 (1.01–2.6) |
0.045 |
OS |
||
CMV D+/R+ versus others |
1.78 (1.09–2.89) |
0.02 |
GRFS |
||
CMV D+/R+ versus others |
1.33 (0.89–1.99) |
0.15 |
Grade II-IV acute GVHD |
||
URD versus MSD |
3.7 (1.75–7.8) |
0.0005 |
CMV D+/R+ versus others |
1.79 (0.93–3.41) |
0.07 |
Abbreviations: CR, complete remission; GVHD, graft versus host disease; GRFS,GVHD-free/relapse-free survival; CMV, cytomegalovirus; URD, unrelated donor; MDS, matched sibling donor.
RI and NRM
At 3 years the cumulative incidence of relapse was 40% (95% CI: 32%–48%) whereas the rate of NRM at 3 years was 23% (95% CI: 16%–30%). With univariate analysis (Supplementary Table 2), we observed that in male patients receiving grafts from female donors there was a trend suggesting increased relapse rates (61% versus 36%; P = 0.072). In multivariate analysis, RI was not significantly affected by donor source nor by Philadelphia chromosome positivity (Table 2). NRM was significantly affected by the CMV status in both donor and patient whereby D+/R+ patients experienced increased NRM rates (HR = 2.25, 95% CI, 1.09–4.66; P = 0.028).
GRFS, LFS and OS
Patients in the analyzed cohort had 3 year OS and LFS rates of 42% and 35% respectively. The most frequent causes of death in the analyzed cohort were leukemia relapse (41 patients; 49%), infection (18 patients, 21%), and GVHD (14 patients, 16%). Results of a univariate analysis are summarized in Supplementary Table 1. In multivariate analysis, LFS and OS rates were significantly influenced by CMV D+/R+ status whereby CMV D+/R+ (HR = 1.62, 95% CI, 1.01–2.6; P = 0.045, and HR = 1.78, 95% CI, 1.09–2.89; P = 0.02) conferred inferior rates for both clinical indices. The GRFS rate was not significantly impacted by any of the abovementioned factors. Philadelphia chromosome status did not significantly impact on clinical outcome (Figure 1).
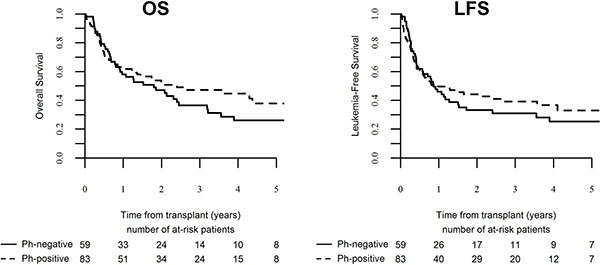
Figure 1: Outcome of ALL patients over the age of 60 following transplantation in CR1 per Philadelphia chromosome status. (A)- OS, (B)- LFS.
DISCUSSION
Older patients with ALL are a uniquely challenging patient population where clinicians are faced with the need to maintain a finely tuned balance between treating leukemia optimally while minimizing the attendant treatment related toxicity. In this analysis we present our recent experience with a large group of older ALL patients undergoing transplant with a curative intent. Our data indicate that a significant subset of patients will be alive and disease free at 3 years following transplant (42% and 35%, respectively), furthermore we show that the traditionally designated high risk Ph+ patients experience equivalent clinical outcome to Ph- patients in terms of both leukemia control and transplant associated toxicity.
While outcome of adult patients as a whole has decidedly improved over the past decade [14], selection of the older ALL patient most suitable for undergoing HSCT remains a difficult and challenging clinical decision. Indeed, this is reflected in a wide variation in practice, where for example a recent survey conducted among Canadian hematologists revealed that only half of them would recommend upfront transplant for ALL patients over the age of 35 [15] while on the other hand published data from the Netherlands indicates that 19% of patients between the ages of 60–69 were transplanted between the years 2007–2012 [9]. The justified concerns of transplant related morbidity and mortality in the inherently vulnerable population of older patients must be contrasted with the realization of the poor outcome associated with non-transplant approaches yielding a five year overall survival rate of only 21% for non-transplanted adults over the age of 55 as observed for instance in the MRC UKALL XII/ECOG E2993 [6, 16]. In our current analysis we found that older patients attained survival rates of more than 40%, in agreement with recently published data in older ALL patients [17, 18], and probably in concurrence also with the MRC UKALL XII/ECOG E2993 [6] and the Japanese experience [19] which evaluated survival at different time points (5 and 2 years respectively).
Our results confirm that the transformative role of TKI in Ph+ ALL also extends to the segment of older Ph+ patients undergoing transplantation. Indeed, our data suggests that for older patients with Philadelphia chromosome positive ALL, prognosis equates with that of Philadelphia chromosome negative patients. Accordingly, it may possible to consider that in older Ph+ patients fit for transplant, Philadelphia chromosome status no longer designates patients as having higher risk disease, a designation which was based on the historical poor outcomes in this patient population [20, 21].
Data from our group [22] and others [13, 17, 23] have established the non-inferiority of RIC and myeloablative conditioning in terms of relapse incidence. Yet, the optimal RIC regimen has yet to be determined. Most of the centers in our cohort used reduced intensity fludarabine based regimens with either melphalan or busulfan, a pattern shared with the experience reported by others [11, 18, 19]. Kanamori and colleagues suggested that fludarabine/busulfan was superior to fludarabine/melphalan although their results did not reach statistical significance [19]. As of now, no data exist to demonstrate a definitive advantage in using a given conditioning regimen. Our retrospective study was not designed to assess the differences between the various conditioning regimens and thus the optimal conditioning regimen to use in this setting remains an open question.
An unexpected finding in our analysis pertained to the clinical impact of CMV donor-recipient matching. We found CMV D+/R+ to be significantly associated with inferior overall survival and leukemia free survival coupled with increased non-relapse mortality. In an earlier EBMT analysis from the 1990s [24] looking at a large cohort of acute leukemia and chronic myeloid leukemia patients, those patients receiving grafts from CMV-seropositive HLA-identical sibling donors had the same survival as patients grafted from seronegative donors. Notably, in that study patients receiving unrelated donor grafts from CMV-seropositive donors had an improved 5-year survival. This issue was recently readdressed with data showing that for patients undergoing myeloablative conditioning, CMV D+/R+ donor-recipient status correlated with improved overall survival compared with CMV D-/R+. This effect was absent in the reduced-intensity conditioning cohort of the analysis [25]. Of note no distinction was made in this study between ALL and AML. A recently published analysis from the EBMT [26] on 5158 ALL patients seem to be in line with our data, indicating that CMV seropositivity of the donor and/or the recipient is significantly associated with decreased 2-year leukemia-free survival and overall survival, and increased non-relapse mortality. Why donor-recipient CMV matching would impact significantly on clinical outcome is still unclear, though some preclinical observations suggest that CMV infection modulates the NK cell repertoire following transplantation thus impacting on acute myeloid leukemia relapse [27].
Owing to the multicenter retrospective nature of our analysis, interpretation of our results needs to be undertaken cautiously. Several factors which were not captured by our registry, including measurable residual disease (MRD) data as well as depth of molecular remission (in Philadelphia chromosome positive patients) prior to transplant, would undoubtedly would have further informed our analysis. In addition, we acknowledge that the cohort analyzed was a select group of patients fit for transplant which may not be completely characteristic of the complete older ALL patient population.
MATERIALS AND METHODS
Study design and data collection
This is a retrospective multicenter analysis based on the registry data of the ALWP of the EBMT. The EBMT is a voluntary working group comprising more than 500 transplant centers that are required to report all consecutive stem cell transplantations and follow-ups once a year. Audits are routinely performed to determine the accuracy of the data. This study was approved by the ALWP institutional review board. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All patients provided written informed consent authorizing the use of their personal information for research purposes. Eligibility criteria for this analysis included adult ALL patients over 60 years of age who underwent RIC HSCT in first remission between 2005 and 2014. Intensity of conditioning was determined according to published criteria [28]. Stem cell graft consisted of either bone marrow (BM) or G-CSF mobilized peripheral blood (PB). All donors were HLA-matched according to standard criteria (locus-A, -B, -C, DRB1, -DQB1). Exclusion criteria were: previous allogeneic, cord blood or haploidentical transplantation, ex vivo T cell depleted stem cell graft. Comorbidity scores were evaluated by the modified EBMT score [29] and the HCT-CI [30]. Grading of acute GVHD and chronic GVHD was performed using established criteria [31, 32].
Statistical analysis
Clinical outcomes were evaluated as follows: (i) non-relapse mortality (NRM), defined as death without previous relapse; (ii) relapse incidence (RI), defined on the basis of morphological evidence of leukemia in bone marrow or other extramedullary organs; (iii) leukemia-free survival (LFS), defined as the time from transplantation to first event (either relapse or death in complete remission); (iv) GVHD-free/relapse-free survival (GRFS), defined as events including grade 3–4 acute GVHD, extensive chronic GVHD, relapse, or death in the first post-HCT year [33]; and (v) overall survival. Cumulative incidence curves were used for RI and NRM in a competing risks setting, since death and relapse are competing. Probabilities of OS, LFS, and LFS were calculated using the Kaplan–Meier estimate. Univariate analyses were done using the Gray’s test for cumulative incidence functions and the log rank test for OS, GRFS, and LFS. Multivariate analyses were performed by stepwise selection of variables associated with p < 0.15 in univariate analysis. All tests were two-sided with the type I error rate fixed at 0.05. Statistical analyses were performed with SPSS 19 (SPSS Inc, Chicago, IL, USA) and R 2.13.2 (R Development Core Team, Vienna, Austria) software packages.
CONCLUSIONS
Taken as a whole, our findings indicate that allogeneic stem cell transplantation is older patients with ALL is feasible and offers the possibility of a long term disease free state in some patients regardless of Philadelphia chromosome status. Patients in first remission, with matched sibling donors, and with CMV donor-recipient matching other than CMV D+/R+ probably fare better than other patients. As we expect novel therapeutics to form the centerpiece of management of ALL patients in the near future, it is cautiously anticipated and hoped that the outcome of older patients with ALL will further improve.
Abbreviations
ALL: Acute lymphoblastic leukemia; EBMT: European Society for Blood and Marrow Transplantation; ALWP: Acute leukemia working party; GVHD: Graft versus host disease; GRFS: GVHD-free/relapse-free survival; LFS: Leukemia free survival; OS: Overall survival; RI: Relapse incidence.
Author contributions
GRG, JC, AR, ML, AN, and MM designed the research and/or analyzed the data. JC, GRG, ML, AR, AN, and MM wrote the manuscript. JF, JJC, NF, GS, MR, MP, AG, HV, JYC, MC, YB, and SG provided clinical data and commented on manuscript. All authors read and approved the final manuscript.
ACKNOWLEDGMENTS
We thank all the European Society for Blood and Marrow Transplantation (EBMT) centers and national registries for contributing patients to the study and data managers for their excellent work. Supplementary information is available at the EBMT Web site.
CONFLICTS OF INTEREST
None.
FUNDING
None.
REFERENCES
1. Mohty M, Labopin M, Tabrizzi R, Theorin N, Fauser AA, Rambaldi A, Maertens J, Slavin S, Majolino I, Nagler A, Blaise D, Rocha V, Acute Leukemia Working Party; European Group for Blood and Marrow Transplantation. Reduced intensity conditioning allogeneic stem cell transplantation for adult patients with acute lymphoblastic leukemia: a retrospective study from the European Group for Blood and Marrow Transplantation. Haematologica. 2008; 93:303–6. https://doi.org/10.3324/haematol.11960.
2. Bachanova V, Verneris MR, DeFor T, Brunstein CG, Weisdorf DJ. Prolonged survival in adults with acute lymphoblastic leukemia after reduced-intensity conditioning with cord blood or sibling donor transplantation. Blood. 2009; 113:2902–5. https://doi.org/10.1182/blood-2008-10-184093.
3. Ram R, Storb R, Sandmaier BM, Maloney DG, Woolfrey A, Flowers ME, Maris MB, Laport GG, Chauncey TR, Lange T, Langston AA, Storer B, Georges GE. Non-myeloablative conditioning with allogeneic hematopoietic cell transplantation for the treatment of high-risk acute lymphoblastic leukemia. Haematologica. 2011; 96:1113–20. https://doi.org/10.3324/haematol.2011.040261.
4. Moorman AV, Chilton L, Wilkinson J, Ensor HM, Bown N, Proctor SJ. A population-based cytogenetic study of adults with acute lymphoblastic leukemia. Blood. 2010; 115:206–14. https://doi.org/10.1182/blood-2009-07-232124.
5. Juliusson G, Karlsson K, Hallbook H. Population-based analyses in adult acute lymphoblastic leukemia. Blood. 2010; 116:1011; author reply 2. https://doi.org/10.1182/blood-2010-03-272724.
6. Sive JI, Buck G, Fielding A, Lazarus HM, Litzow MR, Luger S, Marks DI, McMillan A, Moorman AV, Richards SM, Rowe JM, Tallman MS, Goldstone AH. Outcomes in older adults with acute lymphoblastic leukaemia (ALL): results from the international MRC UKALL XII/ECOG2993 trial. Br J Haematol. 2012; 157:463–71. https://doi.org/10.1111/j.1365-2141.2012.09095.x.
7. Larson RA, Dodge RK, Burns CP, Lee EJ, Stone RM, Schulman P, Duggan D, Davey FR, Sobol RE, Frankel SR. A five-drug remission induction regimen with intensive consolidation for adults with acute lymphoblastic leukemia: cancer and leukemia group B study 8811. Blood. 1995; 85:2025–37.
8. Larson RA, Dodge RK, Linker CA, Stone RM, Powell BL, Lee EJ, Schulman P, Davey FR, Frankel SR, Bloomfield CD, George SL, Schiffer CA. A randomized controlled trial of filgrastim during remission induction and consolidation chemotherapy for adults with acute lymphoblastic leukemia: CALGB study 9111. Blood. 1998; 92:1556–64.
9. Dinmohamed AG, Szabo A, van der Mark M, Visser O, Sonneveld P, Cornelissen JJ, Jongen-Lavrencic M, Rijneveld AW. Improved survival in adult patients with acute lymphoblastic leukemia in the Netherlands: a population-based study on treatment, trial participation and survival. Leukemia. 2016; 30:310–7. https://doi.org/10.1038/leu.2015.230.
10. Stein AS, Palmer JM, O’Donnell MR, Kogut NM, Spielberger RT, Slovak ML, Tsai NC, Senitzer D, Snyder DS, Thomas SH, Forman SJ. Reduced-intensity conditioning followed by peripheral blood stem cell transplantation for adult patients with high-risk acute lymphoblastic leukemia. Biol Blood Marrow Transplant. 2009; 15:1407–14. https://doi.org/10.1016/j.bbmt.2009.07.003.
11. Cho BS, Lee S, Kim YJ, Chung NG, Eom KS, Kim HJ, Min CK, Cho SG, Kim DW, Lee JW, Min WS, Kim CC. Reduced-intensity conditioning allogeneic stem cell transplantation is a potential therapeutic approach for adults with high-risk acute lymphoblastic leukemia in remission: results of a prospective phase 2 study. Leukemia. 2009; 23:1763–70. https://doi.org/10.1038/leu.2009.102.
12. Nishiwaki S, Inamoto Y, Imamura M, Tsurumi H, Hatanaka K, Kawa K, Suzuki R, Miyamura K. Reduced-intensity versus conventional myeloablative conditioning for patients with Philadelphia chromosome-negative acute lymphoblastic leukemia in complete remission. Blood. 2011; 117:3698–9. https://doi.org/10.1182/blood-2011-01-329003.
13. Marks DI, Wang T, Perez WS, Antin JH, Copelan E, Gale RP, George B, Gupta V, Halter J, Khoury HJ, Klumpp TR, Lazarus HM, Lewis VA, et al. The outcome of full-intensity and reduced-intensity conditioning matched sibling or unrelated donor transplantation in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia in first and second complete remission. Blood. 2010; 116:366–74. https://doi.org/10.1182/blood-2010-01-264077.
14. Giebel S, Labopin M, Socie G, Beelen D, Browne P, Volin L, Kyrcz-Krzemien S, Yakoub-Agha I, Aljurf M, Wu D, Michallet M, Arnold R, Mohty M, et al. Improving results of allogeneic hematopoietic cell transplantation for adults with acute lymphoblastic leukemia in first complete remission: an analysis from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Haematologica. 2017; 102:139–49. https://doi.org/10.3324/haematol.2016.145631.
15. Paulson K, Szwajcer D, Raymond CB, Seftel MD. The role of hematopoietic cell transplantation in adult ALL: clinical equipoise persists. Leuk Res. 2014; 38:176–9. https://doi.org/10.1016/j.leukres.2013.10.021.
16. Rowe JM, Buck G, Burnett AK, Chopra R, Wiernik PH, Richards SM, Lazarus HM, Franklin IM, Litzow MR, Ciobanu N, Prentice HG, Durrant J, Tallman MS, et al. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. Blood. 2005; 106:3760–7. https://doi.org/10.1182/blood-2005-04-1623.
17. Bachanova V, Marks DI, Zhang MJ, Wang H, de Lima M, Aljurf MD, Arellano M, Artz AS, Bacher U, Cahn JY, Chen YB, Copelan EA, Drobyski WR, et al. Ph+ ALL patients in first complete remission have similar survival after reduced intensity and myeloablative allogeneic transplantation: impact of tyrosine kinase inhibitor and minimal residual disease. Leukemia. 2014; 28:658–65. https://doi.org/10.1038/leu.2013.253.
18. Rosko AE, Wang HL, de Lima M, Sandmaier B, Khoury HJ, Artz A, Brammer J, Bredeson C, Farag S, Kharfan-Dabaja M, Lazarus HM, Marks DI, Martino Bufarull R, et al. Reduced intensity conditioned allograft yields favorable survival for older adults with B-cell acute lymphoblastic leukemia. Am J Hematol. 2017; 92:42–9. https://doi.org/10.1002/ajh.24575.
19. Kanamori H, Mizuta S, Kako S, Kato H, Nishiwaki S, Imai K, Shigematsu A, Nakamae H, Tanaka M, Ikegame K, Yujiri T, Fukuda T, Minagawa K, et al. Reduced-intensity allogeneic stem cell transplantation for patients aged 50 years or older with B-cell ALL in remission: a retrospective study by the Adult ALL Working Group of the Japan Society for Hematopoietic Cell Transplantation. Bone Marrow Transplant. 2013; 48:1513–8. https://doi.org/10.1038/bmt.2013.140.
20. Moorman AV, Harrison CJ, Buck GA, Richards SM, Secker-Walker LM, Martineau M, Vance GH, Cherry AM, Higgins RR, Fielding AK, Foroni L, Paietta E, Tallman MS, et al. Karyotype is an independent prognostic factor in adult acute lymphoblastic leukemia (ALL): analysis of cytogenetic data from patients treated on the Medical Research Council (MRC) UKALLXII/Eastern Cooperative Oncology Group (ECOG) 2993 trial. Blood. 2007; 109:3189–97. https://doi.org/10.1182/blood-2006-10-051912.
21. Dombret H, Gabert J, Boiron JM, Rigal-Huguet F, Blaise D, Thomas X, Delannoy A, Buzyn A, Bilhou-Nabera C, Cayuela JM, Fenaux P, Bourhis JH, Fegueux N, et al. Outcome of treatment in adults with Philadelphia chromosome-positive acute lymphoblastic leukemia--results of the prospective multicenter LALA-94 trial. Blood. 2002; 100:2357–66. https://doi.org/10.1182/blood-2002-03-0704.
22. Mohty M, Labopin M, Volin L, Gratwohl A, Socie G, Esteve J, Tabrizi R, Nagler A, Rocha V, Acute Leukemia Working Party of EBMT. Reduced-intensity versus conventional myeloablative conditioning allogeneic stem cell transplantation for patients with acute lymphoblastic leukemia: a retrospective study from the European Group for Blood and Marrow Transplantation. Blood. 2010; 116:4439–43. https://doi.org/10.1182/blood-2010-02-266551.
23. Tanaka J, Kanamori H, Nishiwaki S, Ohashi K, Taniguchi S, Eto T, Nakamae H, Minagawa K, Miyamura K, Sakamaki H, Morishima Y, Kato K, Suzuki R, et al. Reduced-intensity vs myeloablative conditioning allogeneic hematopoietic SCT for patients aged over 45 years with ALL in remission: a study from the Adult ALL Working Group of the Japan Society for Hematopoietic Cell Transplantation (JSHCT). Bone Marrow Transplant. 2013; 48:1389–94. https://doi.org/10.1038/bmt.2013.68.
24. Ljungman P, Brand R, Einsele H, Frassoni F, Niederwieser D, Cordonnier C. Donor CMV serologic status and outcome of CMV-seropositive recipients after unrelated donor stem cell transplantation: an EBMT megafile analysis. Blood. 2003; 102:4255–60. https://doi.org/10.1182/blood-2002-10-3263.
25. Ljungman P, Brand R, Hoek J, de la Camara R, Cordonnier C, Einsele H, Styczynski J, Ward KN, Cesaro S, Infectious Diseases Working Party of the European Group for Blood and Marrow Transplantation. Donor cytomegalovirus status influences the outcome of allogeneic stem cell transplant: a study by the European group for blood and marrow transplantation. Clin Infect Dis. 2014; 59:473–81. https://doi.org/10.1093/cid/ciu364.
26. Schmidt-Hieber M, Labopin M, Beelen D, Volin L, Ehninger G, Finke J, Socie G, Schwerdtfeger R, Kroger N, Ganser A, Niederwieser D, Polge E, Blau IW, et al. CMV serostatus still has an important prognostic impact in de novo acute leukemia patients after allogeneic stem cell transplantation: a report from the Acute Leukemia Working Party of EBMT. Blood. 2013; 122:3359–64. https://doi.org/10.1182/blood-2013-05-499830.
27. Bjorklund AT, Clancy T, Goodridge JP, Beziat V, Schaffer M, Hovig E, Ljunggren HG, Ljungman PT, Malmberg KJ. Naive Donor NK Cell Repertoires Associated with Less Leukemia Relapse after Allogeneic Hematopoietic Stem Cell Transplantation. J Immunol. 2016; 196:1400–11. https://doi.org/10.4049/jimmunol.1501434.
28. Bacigalupo A, Ballen K, Rizzo D, Giralt S, Lazarus H, Ho V, Apperley J, Slavin S, Pasquini M, Sandmaier BM, Barrett J, Blaise D, Lowski R, et al. Defining the intensity of conditioning regimens: working definitions. Biol Blood Marrow Transplant. 2009; 15:1628–33. https://doi.org/10.1016/j.bbmt.2009.07.004.
29. Terwey TH, Hemmati PG, Martus P, Dietz E, Vuong LG, Massenkeil G, Dorken B, Arnold R. A modified EBMT risk score and the hematopoietic cell transplantation-specific comorbidity index for pre-transplant risk assessment in adult acute lymphoblastic leukemia. Haematologica. 2010; 95:810–8. https://doi.org/10.3324/haematol.2009.011809.
30. Sorror ML, Maris MB, Storb R, Baron F, Sandmaier BM, Maloney DG, Storer B. Hematopoietic cell transplantation (HCT)-specific comorbidity index: a new tool for risk assessment before allogeneic HCT. Blood. 2005; 106:2912–9. https://doi.org/10.1182/blood-2005-05-2004.
31. Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, Thomas ED. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995; 15:825–8.
32. Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR, Lee SJ, Martin P, Chien J, Przepiorka D, Couriel D, Cowen EW, Dinndorf P, Farrell A, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005; 11:945–56. https://doi.org/10.1016/j.bbmt.2005.09.004.
33. Holtan SG, DeFor TE, Lazaryan A, Bejanyan N, Arora M, Brunstein CG, Blazar BR, MacMillan ML, Weisdorf DJ. Composite end point of graft-versus-host disease-free, relapse-free survival after allogeneic hematopoietic cell transplantation. Blood. 2015; 125:1333–8. https://doi.org/10.1182/blood-2014-10-609032.