
INTRODUCTION
Primary ovarian, fallopian tube, and peritoneal carcinoma (OC) remains the most lethal gynecological malignancy [1], because most women with OC are diagnosed at an advanced stage. Although most cases of OC are sporadic, at least 10% of patients with OC have a genetic predisposition [2]. Identifying individuals at risk for hereditary cancer syndrome with OC predisposition enables targeted prevention, early detection, and effective treatment of this disease.
Hereditary breast and ovarian cancer (HBOC) and Lynch syndrome comprise two common hereditary cancer syndromes associated with increased likelihood of OC; these are caused by pathogenic germline variants in BRCA1 and BRCA2 (BRCA1/2) and mismatch repair (MMR) genes including MLH1, MSH2, MSH6, and PMS2, respectively. Pathogenic germline variants in other genes (e.g., genes from the BRCA-Fanconi-anemia pathway, such as BRIP1 and RAD51) have also been associated with an elevated risk of OC [3, 4]. Analysis of these genes may therefore be useful for identifying individuals with an OC predisposition for effective prevention strategies, early diagnosis, and prediction of therapeutic efficacy such as for poly(ADP-ribose) polymerase inhibitors (PARPi). Although recent findings have indicated that approximately 10–20% of OC cases are associated with pathogenic germline variants in cancer susceptibility genes [4–7], most patients in those studies were Caucasian. Conversely, the frequency of pathogenic germline variants in cancer susceptibility genes (including BRCA1/2) in unselected patients with OC is largely unknown in the Japanese population. In BRCA1/2, for example, data on the frequency of pathogenic germline variants may be important for estimating the rate of patients with OC who may benefit from treatment with a PARPi before the drug is approved in Japan. Furthermore, pathogenic germline BRCA1/2 variants are associated with high-grade serous carcinoma (HGSC), which is less frequently found in East Asian populations (including Japanese) compared with Caucasian populations [8]; thus, the frequency of pathogenic germline variants in Japanese patients with OC may differ from that in Caucasians.
Accordingly, this study was conducted to determine the prevalence of pathogenic germline variants of OC-associated genes including known predisposing genes in an unselected group of 230 Japanese patients with OC, using next-generation sequencing (NGS)-based comprehensive targeted panel sequencing (TPS) for 75 or 79 candidate genes. The putative pathogenic variants were interpreted based on a database from Myriad Genetics [9] and a well-evaluated classification of variants in guidelines from the American College of Medical Genetics and Genomics (ACMG) [10].
RESULTS
Description of the study population
In total, 230 germline DNA samples from unselected patients with OC that had been stored in the Keio Women’s Health Biobank (KWB) in Keio University School of Medicine (Tokyo, Japan) were analyzed by targeted resequencing, using panels of 75 or 79 candidate OC-associated genes (Supplementary Table 1). The clinicopathological characteristics of the patients are shown in Table 1. The median (range) age at diagnosis was 54 (27–87) years. Histological subtyping revealed that 74/230 (32.2%) and 71/230 (30.9%) cases were HGSC and clear cell carcinoma, respectively.
Table 1: Characteristics of the patients included in this study
Characteristic |
n |
% |
|---|---|---|
Total |
230 |
|
Age, years |
||
median (range) |
54 (27–87) |
|
<40 |
18 |
0.4 |
40–49 |
70 |
30.4 |
50–59 |
64 |
27.8 |
60–69 |
52 |
22.6 |
70–79 |
22 |
9.6 |
≥80 |
4 |
1.7 |
Disease site |
||
Ovary |
217 |
94.3 |
Peritoneal |
5 |
2.2 |
Fallopian tube |
8 |
3.5 |
Histological subtype |
||
High-grade serous |
74 |
32.2 |
Low-grade serous |
3 |
1.3 |
Endometrioid |
58 |
25.2 |
Clear cell |
71 |
30.9 |
Mucinous |
18 |
7.8 |
Others |
6 |
2.6 |
Stage |
||
I |
107 |
46.5 |
II |
25 |
10.9 |
III |
80 |
34.8 |
IV |
18 |
7.8 |
Personal history (n = 180) |
||
Proband had breast cancer |
6 |
3.3 |
Family history (n = 180) |
||
First or second-degree relative had breast cancer |
26 |
14.4 |
First or second-degree relative had ovarian cancer |
13 |
7.2 |
Pathogenic germline variant |
||
BRCA1 |
19 |
8.3 |
BRCA2 |
8 |
3.5 |
MLH1 |
1 |
0.4 |
MSH2 |
1 |
0.4 |
MSH6 |
2 |
0.9 |
PMS2 |
2 |
0.9 |
RAD51D |
3 |
1.3 |
ATM |
2 |
0.9 |
MRE11A |
1 |
0.4 |
FANCC |
1 |
0.4 |
GABRA2 |
1 |
0.4 |
Pathogenic germline variants identified in the cohort of patients with OC
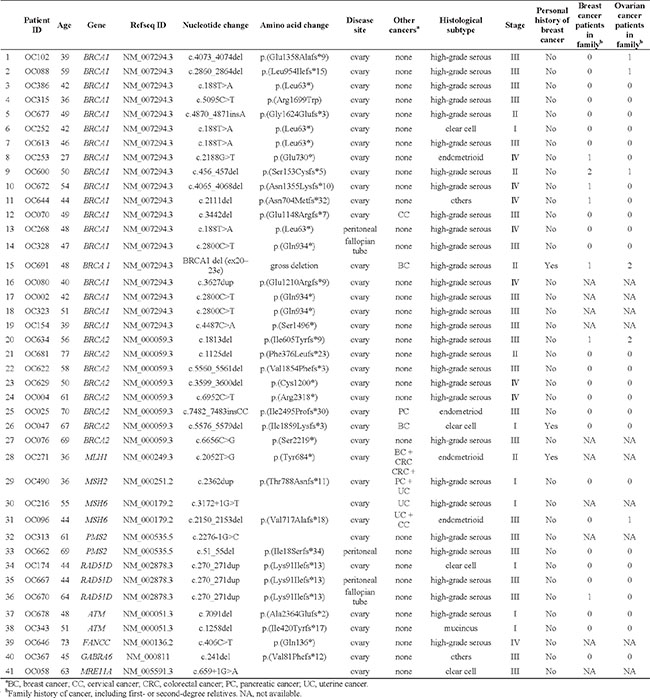
For all coding exons of the 75 or 79 genes selected for study, single-nucleotide variants (SNVs), short insertions/deletions (InDels), and copy-number variations (CNVs) were simultaneously detected using data from TPS. Pathogenic or likely pathogenic germline variants in the tested genes, as classified by the ACMG guidelines, are listed in Table 2 [10]. Of 230 patients, 19 (8.3%) and 8 (3.5%) cases carried germline BRCA1 and BRCA2 pathogenic variants, respectively, of which only 1 had a gross deletion covering more than 1 exon in BRCA1. No variants of uncertain significance in the BRCA1/2 genes were detected in our analysis, based on the Myriad Genetics database [9]. In addition, 6 patients (2.6%) carried pathogenic variants of MMR genes, which may increase the risk of developing Lynch syndrome-related tumors, including 1 in MLH1, 1 in MSH2, 2 in MSH6, and 2 in PMS2. Furthermore, various pathogenic variants were found in several other genes including 3 (1.3%) in RAD51D, 2 (0.9%) in ATM, 1 (0.4%) in MRE11A, 1 in FANCC, and 1 in GABRA6. In total, 41/230 (17.8%) women with OC had pathogenic germline variants in 11 OC-associated genes.
Table 2: List of pathogenic germline variants in tested genes and clinicopathological features of patients with OC
Association between clinicopathological characteristics and pathogenic germline variants
Clinicopathological features for patients with pathogenic germline variants are described in Table 2 and Table 3. Patients with OC and pathogenic germline variants of BRCA1/2 or any other tested genes were diagnosed at a younger age compared with patients lacking pathogenic variants in those genes.
Table 3: Correlation between patient characteristics and pathogenic germline variants in BRCA1/2 or any tested genes among 230 patients with OCa
Clinicopathological features |
n |
Pathogenic BRCA1/2 mutation |
P valueb |
Pathogenic mutations in any tested gene |
P valueb |
||
|---|---|---|---|---|---|---|---|
Positive |
Negative |
Positive |
Negative |
||||
Age |
|||||||
<55 |
117 |
20 |
97 |
0.0132 |
28 |
89 |
0.0159 |
≥55 |
113 |
7 |
106 |
13 |
100 |
||
Histologic subtypec |
|||||||
HGSC |
74 |
22 |
52 |
<0.0001 |
30 |
44 |
<0.0001 |
Non-HGSC |
156 |
5 |
151 |
11 |
145 |
||
Stage |
|||||||
I |
107 |
11 |
96 |
0.5460 |
21 |
86 |
0.6050 |
II - IV |
123 |
16 |
107 |
20 |
103 |
||
Personal history of breast cancera |
|||||||
Diagnosed with breast cancer |
6 |
2 |
4 |
0.1480 |
3 |
3 |
0.0714 |
Not diagnosed with breast cancer |
224 |
25 |
199 |
38 |
186 |
||
One or more family members with breast cancera,d |
|||||||
Present |
26 |
5 |
21 |
0.3260 |
6 |
20 |
0.4040 |
Absent |
154 |
17 |
137 |
25 |
129 |
||
One or more family members with ovarian cancera,d |
|||||||
Present |
13 |
6 |
7 |
0.0017 |
7 |
6 |
0.0019 |
Absent |
167 |
16 |
151 |
24 |
143 |
||
One or more family members with ovarian or breast cancera,c |
|||||||
Present |
32 |
7 |
25 |
0.0775 |
9 |
23 |
0.1180 |
Absent |
148 |
15 |
133 |
22 |
126 |
||
aAmong 230 patients, a detailed family history was available for 180 patients.
bFisher’s exact test.
cHGSC, high-grade serous carcinoma.
dFamily history of cancer, including first- or second-degree relatives.
The frequency of histological OC subtypes among our patient cohort differed from that in Caucasian patients [4–7]; thus, we studied the association between the histological subtypes and pathogenic germline variants in our cohort. Although the major histological subtype of BRCA1/2-associated tumors was HGSC (22/27 cases, 81.5%), pathogenic germline BRCA1/2 variants were also found in patients with other subtypes including endometrioid and clear cell carcinomas. The prevalence of pathogenic germline variants of BRCA1/2 was much higher in patients with HGSC (22/74 , 29.7%) than in those with clear cell carcinoma (2/71, 2.8%) or endometrioid carcinoma (2/58, 3.4%).
In some Asian countries including Japan, genetic counseling and genetic testing have hitherto been offered to patients with OC and a family history of OC or breast cancer [11]. In our cohort, the frequencies of family history of HBOC-related and Lynch syndrome-related cancers were similar between pathogenic germline mutation-positive cases and negative cases (Supplementary Table 2). Therefore, we next focused on OC and breast cancer for family history analysis. Among 180 patients with available detailed family history, 32 had first or second-degree relatives with OC or breast cancer. Carriers of pathogenic germline BRCA1/2 variants and any OC-associated gene variants were more likely to have first or second-degree relatives with OC (P = 0.0017 and 0.0019, respectively; Fisher’s exact test). Individuals with OC and a personal history of breast cancer tended to carry pathogenic germline variants of BRCA1/2 or other OC-associated genes, although the result did not reach statistical significance owing to the small number of such individuals available to be studied.
Descriptive statistical analysis showed that younger age, HGSC, and OC family history were significantly associated with positive pathogenic variant status of either BRCA1/2 or any genes tested (Table 3). Therefore, logistic regression analysis was applied to model the relationship between these variables and pathogenic germline variants of BRCA1/2 or any tested genes. After adjustment for these variables, only the HGSC subtype and OC family history remained as independent predictive factors for pathogenic germline BRCA1/2 variants, whereas all 3 factors remained as independent predictive factors for pathogenic germline variants of any tested genes (Table 4). Because a detailed family history was not obtained from 50 of the 230 subjects, we also examined the association between variables excluding family history and pathogenic germline variants. By applying multiple logistic regression with stepwise variable selection, using P values as a selection criterion, the HGSC subtype and personal history of breast cancer remained as independent predictive factors for both pathogenic germline variants of BRCA1/2 and any tested genes (Supplementary Table 3).
Table 4: Multivariate analysis to determine predictive clinicopathological factors of pathogenic germline variants of BRCA1/2 or any tested genes in 180 patients with OC and a detailed family historya
Variable |
Pathogenic BRCA1/2 variant |
Pathogenic variant in any tested gene |
||||
|---|---|---|---|---|---|---|
Odds ratio |
95% CIb |
Adjusted P valuec |
Odds ratio |
95% CIb |
Adjusted P valuec |
|
Age |
||||||
<55 vs. ≥55 |
2.62 |
0.862–7.970 |
0.0893 |
3.48 |
0.13–9.31 |
0.0129 |
One or more family members with ovarian cancerd |
||||||
Present vs. absent |
6.58 |
1.52–28.60 |
0.0119 |
5.22 |
1.3–21.00 |
0.0201 |
Histologic subtype of OCe |
||||||
HGSC vs non-HGSC |
12.3 |
3.97–38.40 |
<0.0001 |
10.4 |
4.05–26.80 |
<0.0001 |
aMultiple logistic regression was conducted using 3 variables that showed significant correlations with the mutations presented in Table 2.
bCI, confidence interval.
cBold face text denotes statistically significant results.
dFamily history of cancer including first- or second-degree relatives.
eHGSC, high-grade serous carcinoma.
DISCUSSION
In this study, we performed TPS using a multigene panel to estimate the frequency of pathogenic germline variant carriers among Japanese patients with OC. Because this was not a large study, selection bias may have affected the study outcomes. However, the prevalence of pathogenic germline BRCA1/2 variants in unselected Japanese patients with OC (27/230, 11.7%) did not show a large difference compared with that in other ethnicities, regardless of a large difference in prevalence of clear cell carcinoma, which showed a low frequency of pathogenic germline BRCA1/2 variants, between Caucasian and East Asian populations (including Japanese) [8, 12–22]. Pathogenic variants in OC-associated genes other than BRCA1/2 were also detected in 14 patients: 6 in 4 MMR genes and 8 in 5 other OC-associated genes. These pathogenic variants were also frequently observed in HGSC (8/74, 10.8%) compared with clear cell (2/71, 2.8%) and endometrioid (2/58, 3.4%) carcinomas. Because all genes with pathogenic variants in patients with OC except GABRA6 are associated with DNA repair functions, individuals carrying pathogenic germline variants in DNA repair genes appear to be at risk for OC. Although the prevalence and penetrance of pathogenic germline variants differed among the DNA repair genes and the clinical utility of interventions in individuals with moderate-penetrance gene variants associated with OC risk remains unknown [23], multigene panel-based genetic testing, rather than single-gene testing, is an alternative tool for screening hereditary OC that enables more accurate genetic counseling [24].
Prediction of inherited risk in patients with OC is crucial for selecting patients who should be offered genetic risk evaluation by multigene panel-based genetic testing. As an independent risk variable, the age at OC diagnosis had not been generally associated with the likelihood of harboring an inherited pathogenic variant or with the gene in which a pathogenic variant was found [4]. In the patients with OC among our cohort, however, younger age (<55 years old) at the time of diagnosis was associated with positive pathogenic variants of BRCA1/2 or any of the other tested genes. In terms of familial history, in addition, individuals with any first- or second-degree relatives with OC were associated with positive pathogenic variants of BRCA1/2 or any of the other tested genes in the present study, although most individuals with positive pathogenic variants of BRCA1/2 (15/22, 68.2%) or any of the other tested genes (22/29, 71.0%) did not have a family history of breast cancer/OC. Data in several previous reports also demonstrated that patients with OC and pathogenic germline BRCA1/2 variants frequently lack a family history of breast cancer/OC [4, 13, 17]. Pathogenic germline BRCA1/2 variants may predispose women to OC, particularly HGSC, through defective homologous recombination repair (HRR) function. Consistent with this hypothesis, pathogenic germline variants in other HRR-related genes including PALB2, RAD51, RAD50, BARD1, CHEK2, and BRIP1 have been previously detected in serous OC [4, 25, 26]. Thirdly, in our study, patients with OC classified as HGSC were associated with positive pathogenic variants of BRCA1/2 or any of the other tested genes.
Multiple logistic regression using these 3 variables revealed that the most significant predictors for germline variants in BRCA1/2 or any of the other tested genes were the HGSC subtype and family history of OC. Predictive significance of the serous histologic subtype for pathogenic BRCA1/2 variant-positive patients with OC was also reported in another Asian population [11]. Identifying pathogenic germline variant carriers among patients with OC will enable appropriate genetic counseling and will also enable these patients, especially those with pathogenic BRCA1/2 variant-positive OC, to benefit from targeted therapy. However, pathogenic germline variants of BRCA1/2, other HRR-related genes, and MMR genes were also observed in non-HGSC subtypes (Table 3). Taken together, these data indicate that all patients with OC may be eligible for a cost-effective multigene testing using TPS, although those with inherited pathogenic variants could be predicted according to their clinicopathological features, such as age, family history of OC, and histologic subtype.
Individuals with pathogenic variants in MMR genes are predisposed to Lynch syndrome; moreover, OC is a Lynch syndrome-related cancer [27]. Among the MMR genes MLH1, MSH2, MSH6, and PMS2, defects in MLH1 and MSH2 account for most cases of Lynch syndrome and predominate in colon cancer [28]. In the present study, however, pathogenic variants were more frequently observed in MSH6 and PMS2 compared with MLH1 and MSH2 (Table 1). A similar finding was reported in a cohort of 1,915 unselected patients with OC that included 1,681 Caucasians: pathogenic variants were observed in MSH6 in 3 cases and in PMS2 in 4 cases, in contrast to 1 case with an MLH1 pathogenic variant and no cases with a pathogenic variant in MSH2 [28]. Collectively, MSH6 and PMS2 among the MMR genes appeared to be more strongly associated with OC compared with MLH1 and MSH2, irrespective of ethnicity. Notably, OC in all cases with pathogenic germline PMS2 variants in the present study (2/2 cases) and in a previous study (4/4 cases) [7] belonged to the HGSC subtype, whereas OC in some pathogenic germline MSH6 variant cases in the present study (1/2 cases) and a previous study (2/3 cases) [7] was classified as endometrioid carcinoma. Therefore, MSH6 and PMS2 might be associated with different histologic subtypes of OC.
Several limitations of this study should be noted. The frequency of pathogenic variants may have been underestimated in this series of patients because we included only variants with a clearly damaging impact on protein function. Although we evaluated BRCA1/2 variants according to a database from Myriad Genetics [9], some not-yet-characterized missense variants may prove damaging in OC-associated genes other than BRCA1/2. The frequency of patients with a personal history of breast cancer and a family history of various cancers may also have been underestimated, considering that we used samples from our biobank (KWB) and that it is difficult to obtain recent personal and family histories from patients who died or who were not followed-up in our hospital. A limited statistical power owing to the relatively small size of our cohort may also have prevented detection of the true association between pathogenic germline variants and clinicopathological features. In addition, the absence of an association does not necessarily imply the absence of a causal relationship between genetic predisposition and clinicopathological factors in patients with OC. Further studies are needed to clarify the prevalence and relevance of pathogenic germline variants in Japanese patients with OC.
In summary, our data suggest that the prevalence of pathogenic BRCA1/2 variants and all tested OC-associated genes in Japanese patients with OC is similar to that in other ethnic groups, and that at least the HGSC subtype and OC family history may be useful for predicting the risk of genetic predisposition of Japanese patients with OC and referring high-risk patients for genetic counseling and testing.
MATERIALS AND METHODS
Study subjects and genomic DNA extraction
This study was approved by the Keio University School of Medicine Ethics Committee. All patients provided written, informed consent.
In total, 230 patients with OC treated in Keio University Hospital from 2001 to 2015 were enrolled for this analysis (Table 1). This study excluded the 102 patients with OC who had been recruited for our previous study, in which reported the correlation between family history and BRCA1/2 status [29].
The histological subtypes included high-grade serous (n = 74), low-grade serous (n = 3), endometrioid (n = 58), clear cell (n = 71), mucinous (n = 18) and other cancers (n = 6). Histological diagnosis was performed by 2 independent pathologists and confirmed by 1 pathologist who specializes in gynecologic oncology (H.T.). Clinicopathological factors including familial cancer histories were collected and regularly updated through follow-up and questionnaires.
Germline DNA was isolated from whole blood samples using the QIAamp DNA Blood Kit (Qiagen, Hilden, Germany) and stored in the KWB. DNA concentrations were measured using a Qubit® instrument (Thermo Fisher Scientific Inc., Waltham, MA, USA).
Library construction, hybridization, and massively parallel sequencing
For TPS, 200 ng of genomic DNA from each patient was sheared using a Covaris S220 System sample-preparation instrument (Covaris, Woburn, MA, USA). After assessing the quality of the sheared DNA using a Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA), paired-end libraries were prepared and hybridized with a custom pool of oligonucleotides targeting 75 or 79 genes (Supplementary Table 1) using the SureSelect XT Target Enrichment System (Agilent Technologies) according to the manufacturer’s protocols. Following capture, samples were pooled for multiplexed sequencing and sequenced with 2 × 150 bp paired-end reads on a MiSeq (Illumina, San Diego, CA, USA).
Bioinformatics analysis
Sequenced reads were mapped to the human genome reference (hg19) and SNVs, InDels, and CNVs were detected using SureCall Software v2.1/v3.5 (Agilent Technologies) and our pipeline for NGS data analysis, as described elsewhere [30–32], with a minor modification owing to a software update specific for a bioinformatics pipeline [32]. Minor-allele frequency data were referenced using the 1000 Genomes Project Database (http://www.1000genomes.org/), the NHLBI GO Exome Sequencing Project (ESP6500, http://evs.gs.washington.edu/EVS/), the Human Genetic Variation Database (HGVD, http://www.genome.med.kyoto-u.ac.jp/SnpDB/), and the Integrative Japanese Genome Variation Database (iJGVD, https://ijgvd.megabank.tohoku.ac.jp/). Pathogenic or likely pathogenic variants were validated by Sanger sequencing.
The detected variants in BRCA1/2 were interpreted using a variant classification program according to the ACMG recommendations [10] and the database of Myriad Genetic Laboratories (Salt Lake City, UT, USA), which were developed with supporting linkage, biomedical, clinical, functional, and statistical data used for specific missense and intronic alterations based on over a million samples tested [9].
Statistical analysis
Statistical analysis was performed using Prism 7 (GraphPad Software, La Jolla, CA, USA) or the R software package (version 3.3.2, https://www.r-project.org/). Fisher’s exact test was performed to identify associations between categorical variables. For statistical purposes, family history of breast or ovarian cancer was limited to the first- and second-degree relatives only. A subset of variables, which showed a significant association (P < 0.05), or all variables, which were used for stepwise variable selection using P values as selection criteria, were studied by multivariate analysis to calculate the logarithm of odds of carrying pathogenic germline variants, using logistic regression. All statistical analyses were two-sided, and P values < 0.05 were considered statistically significant.
Author contributions
AH and II contributed equally to this work. AH and II designed the study, analyzed the data, and wrote the manuscript. II provided critical review and comments. II, TN, and KM interpreted the data. TA, WY, HN, and NS contributed to the biobanking and data management. HT performed the central pathological review. DA supervised the study.
ACKNOWLEDGMENTS
We thank the patients and the supporting medical staff for making this study possible. We are grateful to FALCO Biosystems Ltd. for providing scientific and technical advice. We also thank Professor Kenjiro Kosaki, Dr. Kokichi Sugano, Dr. Arisa Ueki, and Ms. Kumiko Misu for their support in the genetic counseling clinic. We are also grateful to Ms. Tomomi Noda, Ms. Mika Okabe, and Ms. Atsuko Fukushima for their biobank and data management.
CONFLICTS OF INTEREST
None.
FUNDING
This study was supported in part by AstraZeneca Externally Sponsored Scientific Research (ESR), Japan Society for the Promotion of Science (JSPS) KAKENHI grant numbers 17K19611 and 16K15618, JSPS Bilateral programs, Keio Gijuku Academic Development Funds from Keio University, and the Japan Agency for Medical Research and Development grant; Public Understanding and Information Sharing on Research Ethics (Ethical, legal and social issues on the practical application of genome medicine).
REFERENCES
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2015; 67:7–30.
2. American College of Obstetricians and Gynecologists; ACOG Committee on Practice Bulletins-Gynecology; ACOG Committee on Genetics; Society of Gynecologic Oncologists. ACOG Practice Bulletin No. 103: hereditary breast and ovarian cancer syndrome. Obstet Gynecol. 2009; 113:957–966.
3. Toss A, Tomasello C, Razzaboni E, Contu G, Grandi G, Cagnacci A, Schilder RJ, Cortesi L. Hereditary ovarian cancer: not only BRCA 1 and 2 genes. Biomed Res Int. 2015; 2015:341723.
4. Walsh T, Casadei S, Lee MK, Pennil CC, Nord AS, Thornton AM, Roeb W, Agnew KJ, Stray SM, Wickramanayake A, Norquist B, Pennington KP, Garcia RL, et al. Mutations in 12 genes for inherited ovarian, fallopian tube, and peritoneal carcinoma identified by massively parallel sequencing. Proc Natl Acad Sci USA. 2011; 108:18032–18037.
5. The Cancer Genome Atlas Research Network. Integrated genomic analyses of ovarian carcinoma. Nature. 2011; 474:609–615.
6. Kanchi KL, Johnson KJ, Lu C, McLellan MD, Leiserson MD, Wendl MC, Zhang Q, Koboldt DC, Xie M, Kandoth C, McMichael JF, Wyczalkowski MA, Larson DE, et al. Integrated analysis of germline and somatic variants in ovarian cancer. Nat Commun. 2014; 5:3156.
7. Norquist BM, Harrell MI, Brady MF, Walsh T, Lee MK, Gulsuner S, Zhang Q, Koboldt DC, Xie M, Kandoth C, McMichael JF, Wyczalkowski MA, Larson DE, et al. Inherited mutations in women with ovarian carcinoma. JAMA Oncol. 2016; 2:482–490.
8. Yamagami W, Nagase S, Takahashi F, Ino K, Hachisuga T, Aoki D, Katabuchi H. Clinical statistics of gynecologic cancers in Japan. J Gynecol Oncol. 2017; 28:e32.
9. Eggington JM, Bowles K, Moyes K, Manley S, Esterling L, Sizemore S, Rosenthal E, Theisen A, Saam J, Arnell C, Pruss D, Bennett J, Burbidge LA, et al. A comprehensive laborator-ybased program for classification of variants of uncertain significance in hereditary cancer genes. Clin Genet. 2014; 86:229–237.
10. Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, Grody WW, Hegde M, Lyon E, Spector E, Voelkerding K, Rehm HL; ACMG Laboratory Quality Assurance Committee. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015; 17:405–424.
11. Hasmad HN, Lai KN, Wen WX, Park DJ, Nguyen-Dumont T, Kang PC, Thirthagiri E, Ma’som M, Lim BK, Southey M, Woo YL, Teo SH. Evaluation of germline BRCA1 and BRCA2 mutations in a multi-ethnic Asian cohort of ovarian cancer patients. Gynecol Oncol. 2016; 141:318–322.
12. Sarantaus L, Vahteristo P, Bloom E, Tamminen A, Unkila-Kallio L, Butzow R, Nevanlinna H. BRCA1 and BRCA2 mutations among 233 unselected Finnish ovarian carcinoma patients. Eur J Hum Genet. 2001; 9:424–430.
13. Soegaard M, Kjaer SK, Cox M, Wozniak E, Høgdall E, Høgdall C, Blaakaer J, Jacobs IJ, Gayther SA, Ramus SJ. BRCA1 and BRCA2 mutation prevalence and clinical characteristics of a population-based series of ovarian cancer cases from Denmark. Clin Cancer Res. 2008; 14:3761–3767.
14. Chao A, Chang TC, Lapke N, Jung SM, Chi P, Chen CH, Yang LY, Lin CT, Huang HJ, Chou HH, Liou JD, Chen SJ, Wang TH, Lai CH. Prevalence and clinical significance of BRCA1/2 germline and somatic mutations in Taiwanese patients with ovarian cancer. Oncotarget. 2016; 7:85529–85541. https://doi.org/10.18632/oncotarget.13456.
15. Zhang S, Royer R, Li S, McLaughlin JR, Rosen B, Risch HA, Fan I, Bradley L, Shaw PA, Narod SA. Frequencies of BRCA1 and BRCA2 mutations among 1,342 unselected patients with invasive ovarian cancer. Gynecol Oncol. 2011; 121:353–357.
16. Brozek I, Ochman K, Debniak J, Morzuch L, Ratajska M, Stepnowska M, Stukan M, Emerich J, Limon J. High frequency of BRCA1/2 germline mutations in consecutive ovarian cancer patients in Poland. Gynecol Oncol. 2008; 108:433–437.
17. Alsop K, Fereday S, Meldrum C, deFazio A, Emmanuel C, George J, Dobrovic A, Birrer MJ, Webb PM, Stewart C, Friedlander M, Fox S, Bowtell D, et al. BRCA mutation frequency and patterns of treatment response in BRCA mutation-positive women with ovarian cancer: a report from the Australian Ovarian Cancer Study Group. J Clin Oncol. 2012; 30:2654–2663.
18. Pal T, Permuth-Wey J, Betts JA, Krischer JP, Fiorica J, Arango H, LaPolla J, Hoffman M, Martino MA, Wakeley K, Wilbanks G, Nicosia S, Cantor A, et al. BRCA1 and BRCA2 mutations account for a large proportion of ovarian carcinoma cases. Cancer. 2005; 104:2807–2816.
19. Rodríguez AO, Llacuachaqui M, Pardo GG, Royer R, Larson G, Weitzel JN, Narod SA. BRCA1 and BRCA2 mutations among ovarian cancer patients from Colombia. Gynecol Oncol. 2012; 124:236–243.
20. Liede A, Malik IA, Aziz Z, Rios Pd Pde L, Kwan E, Narod SA. Contribution of BRCA1 and BRCA2 mutations to breast and ovarian cancer in Pakistan. Am J Hum Genet. 2002; 71:595–606.
21. Shi T, Wang P, Xie C, Yin S, Shi D, Wei C, Tang W, Jiang R, Cheng X, Wei Q, Wang Q, Zang R. BRCA1 and BRCA2 mutations in ovarian cancer patients from China: ethnic-related mutations in BRCA1 associated with an increased risk of ovarian cancer. Int J Cancer. 2017; 140:2051–2059.
22. Einbeigi Z, Bergman A, Meis-Kindblom JM, Flodin A, Bjursell C, Martinsson T, Kindblom LG, Wahlström J, Wallgren A, Nordling M, Karlsson P. Occurrence of both breast and ovarian cancer in a woman is a marker for the BRCA gene mutations: a population-based study from western Sweden. Fam Cancer. 2007; 6:35–41.
23. Ramus SJ, Song H, Dicks E, Tyrer JP, Rosenthal AN, Intermaggio MP, Fraser L, Gentry-Maharaj A, Hayward J, Philpott S, Anderson C, Edlund CK, Conti D, et al. Germline mutations in the BRIP1, BARD1, PALB2, and NBN genes in women with ovarian cancer. J Natl Cancer Inst. 2015; 107.
24. Swisher EM. Usefulness of multigene testing: catching the train that’s left the station. JAMA Oncol. 2015; 1:951–952.
25. Cunningham JM, Cicek MS, Larson NB, Davila J, Wang C, Larson MC, Song H, Dicks EM, Harrington P, Wick M, Winterhoff BJ, Hamidi H, Konecny GE, et al. Clinical characteristics of ovarian cancer classified by BRCA1, BRCA2, and RAD51C status. Sci Rep. 2014; 4:4026.
26. Rigakos G, Razis E. BRCAness: finding the Achilles heel in ovarian cancer. Oncologist. 2012; 17:956–962.
27. Lynch HT, Snyder CL, Shaw TG, Heinen CD, Hitchins MP. Milestones of Lynch syndrome: 1895–2015. Nat Rev Cancer. 2015; 15:181–194.
28. Pérez-Carbonell L, Ruiz-Ponte C, Guarinos C, Alenda C, Payá A, Brea A, Egoavil CM, Castillejo A, Barberá VM, Bessa X, Xicola RM, Rodríguez-Soler M, Sánchez-Fortún C, et al. Comparison between universal molecular screening for Lynch syndrome and revised Bethesda guidelines in a large population-based cohort of patients with colorectal cancer. Gut. 2012; 61:865–872.
29. Hirasawa A, Masuda K, Akahane T, Ueki A, Yokota M, Tsuruta T, Nomura H, Kataoka F, Tominaga E, Banno K, Makita K, Susumu N, Sugano K, et al. Family history and BRCA1/BRCA2 status among Japanese ovarian cancer patients and occult cancer in a BRCA1 mutant case. Jpn J Clin Oncol. 2014; 44:49–56.
30. Okamoto N, Naruto T, Kohmoto T, Komori T, Imoto I. A novel PTCH1 mutation in a patient with Gorlin syndrome. Hum Genome Var. 2014; 1:14022.
31. Watanabe M, Hayabuchi Y, Ono A, Naruto T, Horikawa H, Kohmoto T, Masuda K, Nakagawa R, Ito H, Kagami S, Imoto I. Detection of 1p36 deletion by clinical exome-first diagnostic approach. Hum Genome Var. 2016; 3:16006.
32. Watanabe M, Nakagawa R, Naruto T, Kohmoto T, Suga K, Goji A, Kagami S, Masuda K, Imoto I. A novel missense mutation of COL5A2 in a patient with Ehlers–Danlos syndrome. Hum Genome Var. 2016; 3:16030.