
INTRODUCTION
Head and neck cancers are a heterogeneous group of tumours that originate in the the nasal cavity, paranasal sinuses, oral cavity, salivary glands, pharynx and larynx [1–4]. A large number (>90%) of these malignancies are squamous cell carcinoma (SCC) that arise from the squamous epithelium of the oral cavity and the oropharynx [2, 5–7], they are generally referred to as head and neck squamous cell carcinomas (HNSCC). HNSCC currently stands as the sixth most common cancer worldwide with 900,000 new cases per year, with about 300,000 deaths annually [1].
There is a rapid rise in the incidence of oropharyngeal cancers (OPC), a type of HNSCC, caused by the human papillomavirus type 16 (HPV-16) [8] in the USA and in the western world, whilst oral cavity cancer (OC, predominantly HPV-negative) prevalence is increasing in emerging economies [8–10]. In general, HPV-positive HNSCC patients have a better prognosis than HPV-negative patients with similar tumour burden [11, 12]. More than half of these tumours are diagnosed at an advanced stage [13] and only 50% of HPV-negative patients and 66% HPV-positive patients survive up to 5 years post diagnosis (American Cancer Society, 2015). In addition, approximately 30% of HPV-positive patients develop recurrences within 2 years of initial diagnosis, whilst HPV-negative HNSCC patients show recurrences within 1 year [14]. For both tumour types when diagnosed early (before local and distant metastasis), the 5-year survival rate is 80% compared with only 15% in late diagnosis [15]. Given the clinical and biological diffrences between these two cancer types, it is therefore important to treat them separately when developing biomarkers [16].
Due to late diagnosis, the majority of HNSCC patients show either locally advanced disease and/or metastatic disease and require multimodality therapy which includes surgery, commonly followed by postoperative radiotherapy or chemo-radiotherapy [17]. In contrast, when detected early, these tumours are treated by single modality, surgery or radiotherapy alone, reducing the side effects of combining chemo-and radiotherapy. Therefore, there is an urgent need to develop early diagnostic biomarkers for the management of HNSCC patients [18].
MicroRNAs (miRNAs) are a new class of robust, small non-coding RNAs that regulate gene expression by binding to their mRNA targets [19–22]. The strong stability and altered expression levels of miRNA in biological samples (blood, saliva and urine) suggest that they could potentially be used as diagnostic, prognostic and predictive biomarkers for a number of tumour types [23, 24]. The field has moved away from using a single diagnostic biomarker to using multi-biomarker pannels [25, 26]. Multi marker panels are used to obtain an accurate overview of the tumour heterogeneity.
In a pilot study, we have previously demonstrated that three of the miRNAs from the nine panel can discriminate a healthy control group from a HNSCC patient group [27]. However, our previous data was generated using a small subet of samples, where the control group did not include smokers and ex-smokers and the patient group did not take into consideration the HPV status as well as the majority of the HNSCC patients were from an advanced stage of cancer. In contrast, the current study addresses these limitations and we have also included an additional four miRNAs, which have been preselected as these are upregulated in tumours tissue vs normal tissue (data obtained from The Cancer Genome Atlas) [28].
We hypothesised that the salivary miRNA panel can discriminate healthy controls from HPV-negative and HPV-positive patients as well as to differentially detect HPV-negative HNSCC patients from HPV-positive patients. The aims of this study were two-fold: (i) to identify salivary miRNAs that can discriminate a healthy control group from HPV-positive and HPV-negative HNSCC patients (ii) to identify salivary miRNAs that can differentially detect HPV-positive HNSCC patients from HPV-negative HNSCC patients.
RESULTS
Population characteristics
The mean age of controls was 44.7 years (SD 11.4, range 19–79 years), HPV-positive HNSCC patients was 59.7 years (SD 11.4, range 37–87 years) and that of HPV-negative HNSCC patients was 64.3 years (SD 10.38, range 42–91 years). The two genders were equally represented in the control group but in the patient group, there were more men than women. Additionally, HNSCC patients were approximately twice as likely to be smokers or having quit within the past 12 month (61.4%) compared to controls (33.6%). Only 16.8% of HNSCC patients have never been smokers compared to 62.8% of controls. Most HPV-negative HNSCC patients were current smokers (85.1%) and the minority of them were former smokers (6.4%) while within the HPV-positive HNSCC patients, 40.7% were current smokers and 35.2% former smokers. The majority of controls and HNSCC patients were Caucasians, 72.8% and 99%, respectively.
The clinical and pathological characteristics of HNSCC patients are shown in Table 1. The cancer sites were mostly of oropharyngeal and oral cavity (56.4% and 24.8% respectively), laryngeal and hypopharyngeal were 10.9% and 1% respectively; and 6.9% from other anatomical sites in the head and neck area. HPV-negative HNSCC patients had cancers within the oral cavity (42.6%) whereas the majority of HPV-positive HNSCC patients had cancers within the oropharynx (75.9%). HPV-positive HNSCC patients were mostly diagnosed (83.3%) with stages III and IV tumours, whilst 46.8% of HPV-negative patients were diagnosed with stages III and IV tumours. This is primarily due to the higher frequency of patients with nodal neck disease that is commonly seen in HPV-positive HNSCC [29].
Table 1: Participants demographic characteristics
Controls (n = 113) |
HPV-negative HNSCC patients (n = 47) |
HPV-positive HNSCC patients |
|
|---|---|---|---|
Gender |
|||
Male |
59 (52.2) |
34 (72.3) |
49 (90.7) |
Female |
54 (47.8) |
13 (27.7) |
5 (9.3) |
Age (years) |
|||
<50 |
73 (64.6) |
5 (10.6) |
10 (18.5) |
50 - 60 |
36 (31.9) |
11 (23.4) |
16 (29.6) |
>60 |
4 (3.5) |
31 (65.9) |
28 (51.9) |
Race and ethnicity |
|||
Caucasian |
82 (72.6) |
46 (97.9) |
54 (100) |
Asian |
13 (11.5) |
1 (2.1) |
0 (0) |
Other |
18 (15.9) |
0 (0) |
0 (0) |
Smoking status |
|||
Smokers |
38 (33.6) |
40 (85.1) |
22 (40.7) |
<10 |
9 (7.9) |
6 (12.8) |
3 (5.6) |
10-20 |
21 (18.6) |
19 (40.4) |
8 (14.8) |
>20 |
8 (7.1) |
15 (31.9) |
11 (20.4) |
Ex-smoker |
4 (3.5) |
3 (6.4) |
19 (35.2) |
Non-smoker |
71 (63.7) |
4 (8.5) |
13 (24.1) |
Tumour characteristics |
|||
AJCC Stage I |
6 (12.8) |
3 (5.6) |
|
Stage II |
9 (19.1) |
6 (11.1) |
|
Stage III |
10 (21.3) |
6 (11.1) |
|
Stage IVa |
20 (42.6) |
37 (68.5) |
|
Stage IVb |
1 (2.1) |
2 (3.7) |
|
Stage IVc |
1 (2.1) |
0 (0) |
|
Tumour anatomic sites |
|||
Oral cavity |
20 (42.6) |
5 (9.3) |
|
Oropharynx |
16 (34.0) |
41 (75.9) |
|
Larynx |
9 (19.1) |
2 (3.7) |
|
Hypopharynx |
1 (2.1) |
0 (0) |
|
Neck |
1 (2.1) |
6 (11.1) |
|
Differentiation status |
|||
Well differentiated |
9 (19.1) |
2 (3.7) |
|
Well to moderately differentiated |
2 (4.3) |
1 (1.9) |
|
Moderately differentiated |
16 (34.0) |
12 (22.2) |
|
Moderately to poorly differentiated |
5 (10.6) |
7 (13.0) |
|
Poorly differentiated |
6 (12.8) |
13 (24.1) |
|
N/A |
9 (19.1) |
19 (35.2) |
|
Keratinisation status |
|||
keratinising |
13 (27.7) |
4 (7.4) |
|
non-keratinising |
34 (72.3) |
45 (83.3) |
|
others |
0 (0) |
5 (9.3) |
miRNA yields from small volumes of saliva samples
We have previously described a robust and a reproducible method to isolate high yields of miRNA from both fresh and archived saliva samples based on QIAzol (Qiagen, Valencia, CA, USA) extraction followed by solid phase enrichment of miRNAs on silica, column [27]. The amount of miRNAs isolated in 200 μL of saliva collected from healthy controls was 0.123 to 6.01 μg and from HNSCC patients was 0.21 to 19.3 μg yields.
Salivary miRNA expression levels can discriminate a control group from a HPV-negative and a HPV-positive HNSCC patient group
We have performed both univariate and multivariate statistical analysis to determine the best miRNA that can detect HPV-positive and HPV-negative HNSCC patients. Univariate analysis of individual miRNA expression levels demonstrated that miRNA-9, -196a, -196b, -210, -222, and -455 were significantly upregulated in the saliva from HPV-negative HNSCC patients compared with saliva from healthy controls; whilst the expression levels of miRNA-9, -134, -196a, -196b, -210 and -455 were significantly upregulated in the saliva from HPV-positive HNSCC patients compared with healthy controls (Figure 1).
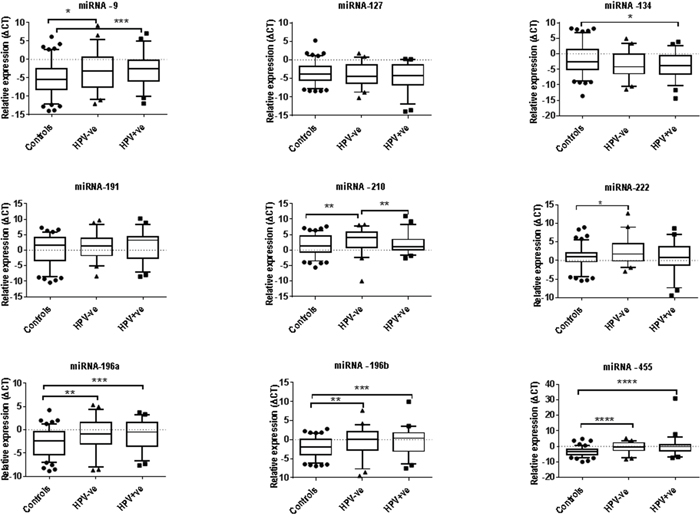
Figure 1: The expression levels of nine miRNA in saliva collected from healthy control (n=113) as well as HPV-negative (n=47) and HPV-positive (n=54) by RT-qPCR. SNORD-96A was used as a normerliser. Statistically significant differences were determined using Mann Whitney U Test. Significant differences are denoted as *P<0.05; **P<0.01; ***P<0.001 and ****P<0.0001.
We have identified a combination of salivary miRNA-9, -127, -134, -191, -222 and -455 as the most parsimonious set of candidates for identifying HPV-negative patients from healthy controls using multiple logistic regression analysis. This resulted in 60% sensitivity and 94% specificity. The combination of miRNA-9,-134, -210, and -455 and -196b was found to be the most appropriate for identifying HPV-positive patients from healthy controls. This resulted in a sensitivity of 65% and a specificity of 95% (see Table 2 and Figure 2).
Table 2: Discrimination of healthy controls from HPV-negative HNSCC patients and -positive HNSCC patients using the combined miRNA panels
Control vs HPV-patients |
Control vs HPV +patients |
|
|---|---|---|
Probability threshold |
0.45 |
0.41 |
Sensitivity |
0.60 |
0.65 |
Specificity |
0.94 |
0.95 |
Negative predictive value |
0.85 |
0.85 |
Positive predictive value |
0.82 |
0.87 |
AUC |
0.82 |
0.80 |
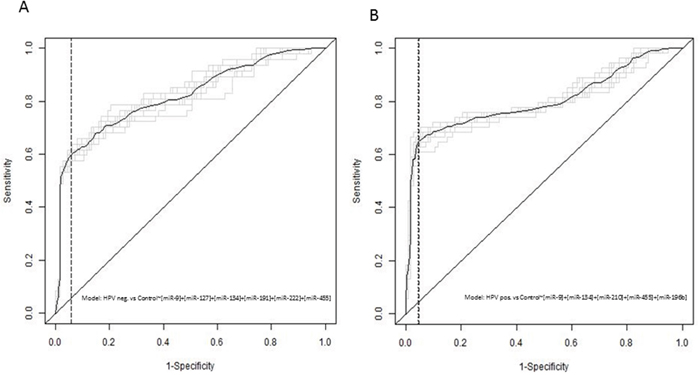
Figure 2: The receiver operator characteristics curve analysis from the independent validation study using saliva (A) HPV-negative HNSCC patients vs controls (B) HPV-positive HNSCC patients vs controls.
Salivary miRNA expression levels can discriminate HPV-positive HNSCC patients from HPV-negative HNSCC patients
Using a Mann Whitney U test, the expression level of miRNA-210 was elevated in saliva collected from HPV-negative HNSCC patients compared with HPV-positive HNSCC patients. Using multiple logistic regression analysis pipeline, we have identified the combination of miRNA-191, -196b, -210, and -222 to be the most parsimonious miRNA set for discriminating HPV-negative patients from HPV-positive patients.
Salivary miRNA expression levels could detect eraly stage HPV-negative and HPV-positive HNSCC pateints from a control group
The miRNA expression levels of -196a, -196b, -210 and -455 were found to be elevated in the saliva collected from early clinical stages (stages I and II) HPV-negative HNSCC patients compared with the saliva from healthy controls using the Mann Whitney U test. Whilst the upregulation of miRNA-9, -127, -196a, -196b, -222 and -455 were found in the saliva collected from early stage (stages I and II) HPV-positive HNSCC patients compared with healthy controls (see Figure 3 and 4).
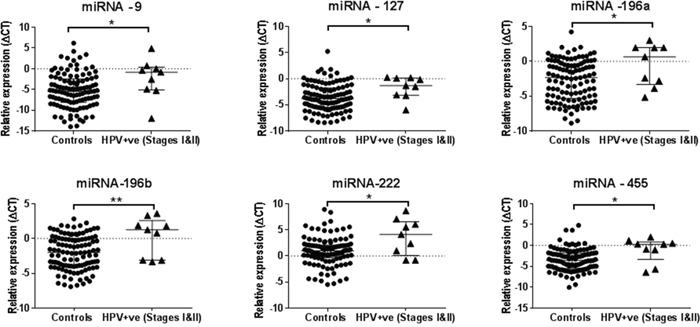
Figure 3: A set of six salivary miRNAs that can discriminate the early stage (Stages I&II) of HPV-positive HNSCC patients from the healthy control smoker and non-smoker group. *P<0.05 and **P<0.01.
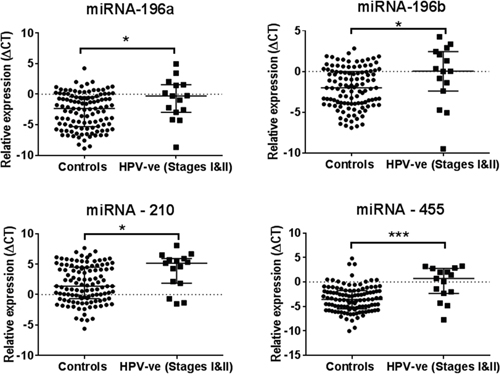
Figure 4: A set of four salivary miRNAs that can be used in discriminating healthy controls from the early stage (Stages I&II) of HPV-negative HNSCC patients. Significant differences are *P<0.05 and ***P<0.001.
DISCUSSION
Despite advanced locoregional control and reduced treatment related morbidity, the five-year survival rates for HPV-positive and HPV-negative HNSCC patients have not improved [30]. Diagnostic biomarkers are urgently needed to identify these patients earlier to improve survival rates and minimise the treatment toxicity. The rationale for improving prognosis and de-escalating therapy for disease diagnosed early is not only self-evident, it is applicable to virtually every cancer, and there is overwhelming literature evidence of better prognosis with earlier diagnosis in these patients [31, 32]. In this study, a multivariable logistic regression analysis with cross validation was used to identify the most robust salivary miRNAs that can discriminate a control group from HPV-negative and HPV-positive HNSCC patients as well as to differentially diagnose HPV-negative and HPV-positive patients. In this study, we have used a multimarker approach to minimise tumour heterogeneity and biological variability.
One of the major challenges in cancer research biomarker studies is to identify stable biomolecules which can be routinely measured in easily accessible samples [33]. Robustness and reproducibility are key requisites prior to clinical implementation of biomarkers. To increase the robustness of the identified miRNA panel, we have used a pipeline consisting of multiple logistic regression with a ROC curve analysis and a 10-fold cross-validation. We have used this statistical analysis method to increase the likelihood of clinical implementation of this miRNA panel, when it is applied to an independent cohort of patients and controls. This then reduces the risk of obtaining overly optimistic data and hence increases the likelihood of clinical translation.
Previous studies have shown that miRNA expression signatures are promising biomarkers for the diagnosis, prognosis and prediction of human cancers [34–39]. We have found elevated levels of miRNA-9 in saliva collected from HNSCC patients compared with saliva from controls, paralleling tumour tissue data for HNSCC [27, 28, 40–42]. Similarily, the overexpression of miRNA-9 has been previously observed in many other cancer types including osteosarcoma, correlated significantly with poor prognosis as a result of tumor metastasis [43].
Salivary miRNA-134 expression levels showed concordance to the tumour expression levels [28]; the upregulation of miRNA-134 in tongue tumour tissues has shown to be associated with an increase in nodal metastasis as well as mortality in HNSCC patients mediated via the downregulation of WWOX gene [44]. In line with our salivary miRNA- 196a data, previous studies have also demonstrated an upregulation of miRNA-196a in HNSCC tissues when compared to normal tissues [45–47], with miRNA-196 precursor shown to be predictive of overall survival and disease-free survival in HPV-positive oropharyngeal cancer patients [48]. Similarly, miRNA-455 levels were elevated in saliva from HPV-positive and HPV-negative patients, supported by other studies demonstrating an elavted expression levels in tumours from uvula, larynx, floor of mouth and tongue of HNSCC patients [28, 39, 49, 50].
Current diagnosis is usually made after clinical presentation of symptoms, and involves biopsy to confirm diagnosis, HPV status by p16INK4A immunostaining, and histological classification [9, 10]. These diagnostic methods are applied to advanced stage tumours with significant clinical presentation of symptoms. The treatment and clinical management also differs between HPV-negative and HPV-positive HNSCC patients. Therefore, it becomes important to discriminate between these patient groups to tailor therapy. We found that the expression levels of salivary miRNA-210 can differentiate between HPV-positive and HPV-negative HNSCC patients. In addition, infection of HPV-16/18 in organotypic raft cultures of vaginal keratinocytes increased the expression of miRNA-210 [51]. Moreover, it has been also reported that the expression levels of miRNA-127-3p is decreased in HPV-positive patients tumour tissues compared with HPV-negative patints tumour tissues [52]. Regardless of HPV status, we found that miRNA-196a, -196b and -455 were significantly overexpressed in saliva from HNSCC patients from early stages of tumour development (stages I and II). A previous study has shown that miRNA-196a plays an oncogenic role in HNSCC through deregulation of cell proliferation [47]. Similarly, another study has shown that elevated levels of miRNA-455-5p was associated with poor prognosis [53]. Albeit, our data has been generated in a small cohort of patients from stages I and II, it implies that these miRNA may have prognostic value as biomarkers for early detection of HNSCC. Therefore, a further study should be conducted to verify the predictive potential of the above markers.
One of the limitations in the current study is the low sensitivity (~60%), in contrast to a high specificity of 90%, indicating that this panel is better suited as a screening tool [54]. In addition, age as a continouus variable may affect this panel. Current literature dipicts that miRNAs are the key regulators of aging and has shown a higher expression levels in the tissues collected from older people [55]. Intriguingly, the salivary miRNAs investigated in this study didn’t show any significant changes as a result of aging (data not shown). A lager cohort with the addition of other parameters (e.g. new miRNA or other clinical variables) is warranted for a further investigation.
In summary, we have identified two miRNA panels that can discriminate healthy controls from HPV-negative (sensitivity =60%; specificity =94%) and -positive HNSCC patients (sensitivity =65%, specificity =95%). Remarkably, the salivary miRNA data strongly correlated with published TCGA data using tumour tissues obtained from HNSCC patients (international studies). Therefore, we are confident that the miRNA expression changes in saliva can be used as a proxy to determine tumour progression. Our approach of using multiple logistic regression coupled to ROC analysis with cross-fold validation has allowed us to identify salivary miRNAs with minimal biological variations in a control and a patient cohort. This opens up new avenues for exploring the utility of salivary miRNAs as either diagnostic, prognostic indicators or to determine the response to treatment. A future multi-centre confirmatory study is warranted to test the diagnostic performance of these salivary miRNA prior to clinical implementation.
MATERIALS AND METHODS
Participants
Unstimulated whole mouth saliva samples were collected from healthy individuals, including smokers and non-smokers (n=113) with no previous history of any malignancies to the head and neck areas as well as from HPV-positive (n=54) and HPV-negative (n=47) HNSCC patients at various tumour nodal metastasis (TNM) clinical stages (stages II-IV) of cancer who presented to the Head and Neck Clinic at the Princess Alexandra Hospital, Woolloongabba, Australia. Patients with early stages of tumours (stages I-II) in general do not show either local and/or distant metastasis [56]. The participants’ demographics and clinical characteristics are shown in Table 1. This study was approved by the University of Queensland Medical Ethical Institutional Board [HREC No: 2014000679 and 2014000862] and the Queensland University of technology [HREC No: 1400000617 and 1400000641] and by the Princess Alexandra Hospital Ethics Review Board [HREC Number: HREC/12/QPAH/381]. All participants gave written informed consent before sample collection.
Saliva sample collection and processing
Whole mouth resting saliva samples were collected from volunteers while seated in an upright position. Volunteers were asked to rinse their mouths with drinking water to remove food debris. They were then asked to tilt their heads down and pool saliva in the mouth for 2-5 minutes [57, 58] before drooling into sterile 50 mL Falcon tubes (Sarstedt, Australia). Saliva samples were transported to the laboratory on dry ice.
miRNA extraction and cDNA synthesis from saliva samples
The enrichment and isolation of miRNA from saliva samples was performed using the NucleoSpin miRNA kit (Machnery-Nagel, Germany) as previously published [27]. In brief, whole mouth saliva (200 μL) was added to 800 μL of QIAzol lysis reagent (Qiagen, Valencia, CA, USA). The samples were briefly vortexed and incubated for 5 minutes at room temperature, 200 μL of chloroform was added and vortexed vigorously and incubated for a further 5 minutes at RT. Samples were then centrifuged at 10,000 x g for 10 minutes at 4°C. An aliquot of the upper aqueous layer (800 μL) was transferred into a new micro centrifuge tube and a further 200 μL of chloroform was added and vortexed. Samples were then centrifuged again at 10,000 x g at 4ºC. The upper aqueous layer containing total RNA was carefully removed (800 μL) and transferred into a new micro centrifuge Eppendorff tube and 200 μL of 100% ethanol was added. The solution containing total RNA was passed through Nucleospin column (blue ring) by centrifugation at 11,000 g for 30s at RT. The eluent was collected and 800 μL of MX buffer was added.
The sample was loaded onto a Nucleospin column (green ring) and centrifuged at 11,000 g for 30 s at RT. The columns were then washed with 600 μL of MW1 buffer and centrifuged at 11,000 g for 30 s. The wash was repeated with 700 μL followed by 250 μL of MW2 buffer and centrifuged at 11,000 for 30 s. The columns were then centrifuged at 11,000g for 2 mins to remove all traces of ethanol. The miRNA was eluted in 30 μL of RNase free Water. The quantity of the isolated miRNA was determined by a Nanodrop ND-1000 spectrophotometer (Thermo scientific Wilmington DE).
The cDNA synthesis of isolated miRNA (with an input of 250 ng) was carried out using the miScript II RT Kit with the Hispec buffer (Qiagen, Valencia, CA, USA) according to the manufacturers’ instructions. In brief, the miRNAs were polyadenylated by polymerase A and transcribed into cDNA using oligo-dT primers, both processes took place in parallel in the same tube. The oligo-dT has a 3’degenerate anchor and a universal tag sequence on the 5’end allowing amplification of mature miRNA using real-time PCR. The polyadenylation and universal tag primer ensured that genomic DNA was not amplified and so it was not necessary to perform a DNase treatment in the samples.
Quantitative real-time RT-PCR (RT-qPCR) for nine miRNA panel
To validate the miRNA expression levels in saliva samples, the nine miRNA miScript™ primer PCR Assays (Qiagen, Valencia, CA, USA) were used. This miRNA PCR panel included: hsa-miRNA-210-5p (Cat. No. MS00003801); hsa-miRNA-222-3p (Cat. No. MS00007609); hsa-miRNA-134-3p (Cat. No. MS00031437); hsa-miRNA-127-5p (Cat. No. MS00008575); hsa-miRNA-191-5p (Cat. No. MS00003682); hsa-miRNA-9-5p (Cat. No. MS00010752); hsa-miRNA-196a-3p (Cat. No. MS00031563); hsa-miRNA-196b-3p (Cat. No. MS00031570) and hsa-miRNA-455-3p (Cat. No. MS00009744). Briefly, 3 ng cDNA was used as a template in PCR amplifications and PCRs were run in duplicate using miScript Syber green PCR master mix (Qiagen, Valencia, CA, USA). The PCR was performed using the QuantStudioTM 7 Flex Real-Time PCR System (Thermo Fisher Scientific, Rockford, ILUSA). The PCR reaction mixtures were incubated at 95°C for 15 min to activate hot start Taq DNA polymerase and this was followed by 40 cycles of 94°C for 15 s, 55°C for 30s and 70°C for 30s, monitored by melt curve analysis. The threshold value (Ct) was determined for each well and the Ct values were averaged for each gene according to the Minimum Information for Publication of Quantitative Real-Time PCR Experiments guidelines [59].
A panel of five miRNAs were also tested for suitability as normalisers for miRNAs detected in human saliva (see Supplementary Table 1a). These assays are wet-benched validated miScript™ primer PCR Assays from Qiagen and included RNU6.2 (Cat. No. MS00033740); SNORD68 (Cat. No. MS00033712); SNORD72 (Cat. No. MS00033719); SNORD95 (Cat. No. MS00033726) and SNORD96A (Cat. No. MS00033733). We found that SNORD-96A demonstrated minimal Ct changes between saliva collected and analysed from healthy controls and the patients. As such SNORD96A was used as a normaliser in all subsequent work. The average relative expression (ΔCt) of each targeted miRNA in controls and patients is listed in Supplementary Table 1b.
Statistical analysis
The expression levels of individual miRNAs from HPV-negative and HPV-positive HNSCC patients and the healthy controls were compared using the non-parametric Mann Whitney U test, using GraphPad Prism 5 software version 5.03 (GraphPad Software Inc., USA). The clinical utility of miRNAs as biomarkers was investigated using R [60] and RWeka [61]. A logistic regression model was fitted using RWeka [61], with the patient status as the outcome variable and the miRNAs as explanatory variables. RWeka used a variable selection procedure based on the cross validation error for selecting the most parsimonious model. This model was then used in 10 runs of 10-fold cross validation using the “train” function of the “Caret” package [62]. Since each cross validation randomly creates 10 folds (splits) of the data, the 10 runs could be considered to be different replicates of the same procedure [63]. The reader is directed to the data mining book of Witten et al., (2011) for further information. For each of these 10 runs, the predictions of this model and the performance were created and evaluated using the “predict” and “performance” functions respectively of the ROCR package [63]. Several methods have been proposed for averaging the ROCs curves [64]. In this study, threshold averaging was used, since it averaged the curves at exactly the same thresholds.
Abbreviations
Head and neck squamous cell carcinomas, HNSCC; oropharyngeal cancers, OPC; human papillomavirus type 16, HPV-16; squamous cell carcinoma, SCC; oral cavity cancers, OC; tumour nodal metastasis, TNM; Human Research Ethics Committees, HREC; MicroRNAs, miRNAs; Reverse transcription, RT; complementary DNA, cDNA; quantitative PCR, qPCR; cycle threshold, Ct; receiver operating characteristic, ROC; area under the curve, AUC;
Authors' contributions
YW performed experiments and data analysis and wrote parts of the manuscript. DV developed the multiple logistic regression analysis model with cross validation. CS performed experiments. LK analysed the clinical information and writing of clinical aspect of the manuscript. DC performed experiments and data analysis. CP contributed to the study design, concept, and writing of the manuscript.
ACKNOWLEDGMENTS
We would like to thank Professor William B. Coman for his clinical input in this study. We also thank Ms Dana Middleton and the staff at the ENT Department of the Princess Alexandra Hospital, Woolloongabba, Australia for their assistance in the recruitment of study patients and collection of clinical samples. We also thank Miss Hee Vivian Chung for technical assistance, Mr. Tony Blick and Mr. Xi Zhang for editorial assistance.
CONFLICTS OF INTEREST
CP has a PCT patent filed. The other authors disclose no potential conflicts of interest.
FUNDING
This study is funded by Queensland University of Technology Vice Chancellors Start-up grant (to CP) as well as the Queensland Centre for Head and Neck Cancer funded by Atlantic Philanthropies, the Queensland Government, and the Princess Alexandra Hospital.
REFERENCES
1. van Monsjou HS, Wreesmann VB, van den Brekel MW, Balm AJ. Head and neck squamous cell carcinoma in young patients. Oral Oncol. 2013; 49:1097-102.
2. Walden MJ, Aygun N. Head and neck cancer. Semin Roentgenol. 2013; 48:75-86.
3. Schmidt H, Kulasinghe A, Kenny L, Punyadeera C. The development of a liquid biopsy for head and neck cancers. Oral Oncol. 2016; 61:8-11.
4. Kulasinghe A, Perry C, Warkiani ME, Blick T, Davies A, O'Byrne K, Thompson EW, Nelson CC, Vela I, Punyadeera C. Short term ex-vivo expansion of circulating head and neck tumour cells. Oncotarget. 2016; 7:60101-9. https://doi.org/10.18632/oncotarget.11159.
5. Arantes LM, de Carvalho AC, Melendez ME, Carvalho AL, Goloni-Bertollo EM. Methylation as a biomarker for head and neck cancer. Oral Oncol. 2014; 50:587-92.
6. Markopoulou S, Nikolaidis G, Liloglou T. DNA methylation biomarkers in biological fluids for early detection of respiratory tract cancer. Clin Chem Lab Med. 2012; 50:1723-31.
7. Wyss A, Hashibe M, Chuang SC, Lee YC, Zhang ZF, Yu GP, Winn DM, Wei Q, Talamini R, Szeszenia-Dabrowska N, Sturgis EM, Smith E, Shangina O, et al. Cigarette, cigar, and pipe smoking and the risk of head and neck cancers: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Am J Epidemiol. 2013; 178:679-90.
8. Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the United States. J Clin Oncol. 2008; 26:612-9.
9. Chai RC, Lim Y, Frazer IH, Wan Y, Perry C, Jones L, Lambie D, Punyadeera C. A pilot study to compare the detection of HPV-16 biomarkers in salivary oral rinses with tumour p16(INK4a) expression in head and neck squamous cell carcinoma patients. BMC Cancer. 2016; 16:178.
10. Chai RC, Lambie D, Verma M, Punyadeera C. Current trends in the etiology and diagnosis of HPV-related head and neck cancers. Cancer Med. 2015; 4:596-607.
11. Trosman SJ KS, Ward MC, Al-Khudari S, Nwizu T, Greskovich JF. Effect of human papillomavirus on patterns of distant metastatic failure in oropharyngeal squamous cell carcinoma treated with chemoradiotherapy. JAMA Otolaryngol Head Neck Surg. 2015; 141:457-62.
12. O'Sullivan B, Huang SH, Su J, Garden AS, Sturgis EM, Dahlstrom K, Lee N, Riaz N, Pei X, Koyfman SA, Adelstein D, Burkey BB, Friborg J, et al. Development and validation of a staging system for HPV-related oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICON-S): a multicentre cohort study. The Lancet Oncology. 2016; 17: 440-51.
13. Menzin J, Lines LM, Manning LN. The economics of squamous cell carcinoma of the head and neck. Current Opinion in Otolaryngology & Head and Neck Surgery. 2007; 15:68-73.
14. Patel AN, Mehnert JM, Kim S. Treatment of recurrent metastatic head and neck cancer: focus on cetuximab. Clin Med Insights Ear Nose Throat. 2012; 5:1-16.
15. Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009; 45:309-16.
16. Chung CH, Gillison ML. Human papillomavirus in head and neck cancer: its role in pathogenesis and clinical implications. Clin Cancer Res. 2009; 15:6758-62.
17. Pignon JP, le Maitre A, Maillard E, Bourhis J, MACH-NC Collaborative Group. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol. 2009; 92:4-14.
18. Wang Q, Gao P, Wang X, Duan Y. The early diagnosis and monitoring of squamous cell carcinoma via saliva metabolomics. Sci Rep. 2014; 4:6802.
19. Ling H, Fabbri M, Calin GA. MicroRNAs and other non-coding RNAs as targets for anticancer drug development. Nat Rev Drug Discov. 2013; 12:847-65.
20. Janssen HL, Reesink HW, Lawitz EJ, Zeuzem S, Rodriguez-Torres M, Patel K, van der Meer AJ, Patick AK, Chen A, Zhou Y, Persson R, King BD, Kauppinen S, et al. Treatment of HCV infection by targeting microRNA. N Engl J Med. 2013; 368:1685-94.
21. Mattick JS, Makunin IV. Non-coding RNA. Hum Mol Genet. 2006; 15:R17-29.
22. Budd WT, Weaver DE, Anderson J, Zehner ZE. microRNA dysregulation in prostate cancer: network analysis reveals preferential regulation of highly connected nodes. Chem Biodivers. 2012; 9:857-67.
23. Zandberga E, Kozirovskis V, Ābols A, Andrējeva D, Purkalne G, Linē A. Cell-free microRNAs as diagnostic, prognostic, and predictive biomarkers for lung cancer. Genes Chromosomes Cancer. 2013; 52:356-69.
24. Brase JC, Wuttig D, Kuner R, Sültmann H. Serum microRNAs as non-invasive biomarkers for cancer. Mol Cancer. 2010; 9:1-9.
25. Zhang Z. An
26. Cardoso F, van’t Veer LJ, Bogaerts J, Slaets L, Viale G, Delaloge S, Pierga JY, Brain E, Causeret S, DeLorenzi M, Glas AM, Golfinopoulos V, Goulioti T, et al. 70-Gene Signature as an Aid to Treatment Decisions in Early-Stage Breast Cancer. N Engl J Med. 2016; 375:717-29.
27. Salazar C, Nagadia R, Pandit P, Cooper-White J, Banerjee N, Dimitrova N, Coman WB, Punyadeera C. A novel saliva-based microRNA biomarker panel to detect head and neck cancers. Cell Oncol (Dordr). 2014; 37:331-8.
28. Cancer Genome Atlas Network. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature. 2015; 517:576-82.
29. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tân PF, Westra WH, Chung CH, Jordan RC, Lu C, Kim H, Axelrod R, Silverman CC, et al. Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer. N Engl J Med. 2010; 363:24-35.
30. Lam L, Logan RM, Luke C, Rees GL. Retrospective study of survival and treatment pattern in a cohort of patients with oral and oropharyngeal tongue cancers from 1987 to 2004. Oral Oncol. 2007; 43:150-8.
31. Adam A, Kenny LM. Interventional oncology in multidisciplinary cancer treatment in the 21(st) century. Nat Rev Clin Oncol. 2015; 12:105-13.
32. Turner J, Yates P, Kenny L, Gordon LG, Burmeister B, Thomson D, Hughes B, McCarthy AL, Perry C, Chan RJ, Fraser A, Skerman H, Batstone M, et al. The ENHANCES study--Enhancing Head and Neck Cancer patients' Experiences of Survivorship: study protocol for a randomized controlled trial. Trials. 2014; 15:191.
33. Perez-Gracia JL, Sanmamed MF, Bosch A, Patino-Garcia A, Schalper KA, Segura V, Bellmunt J, Tabernero J, Sweeney CJ, Choueiri TK, Martin M, Fusco JP, Rodriguez-Ruiz ME, et al. Strategies to design clinical studies to identify predictive biomarkers in cancer research. Cancer Treat Rev. 2017; 53:79-97.
34. Salazar C, Calvopina D, Punyadeera C. miRNAs in human papilloma virus associated oral and oropharyngeal squamous cell carcinomas. Expert Rev Mol Diagn. 2014; 14:1033-40.
35. Courthod G, Franco P, Palermo L, Pisconti S, Numico G. The role of microRNA in head and neck cancer: current knowledge and perspectives. Molecules. 2014; 19:5704-16.
36. Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat Rev Cancer. 2006; 6:857-66.
37. Calin GA, Croce CM. MicroRNA-cancer connection: the beginning of a new tale. Cancer Res. 2006; 66:7390-4.
38. Sethi N, Wright A, Wood H, Rabbitts P. MicroRNAs and head and neck cancer: reviewing the first decade of research. Eur J Cancer. 2014; 50:2619-35.
39. Avissar M, Christensen BC, Kelsey KT, Marsit CJ. MicroRNA expression ratio is predictive of head and neck squamous cell carcinoma. Clin Cancer Res. 2009; 15:2850-5.
40. Hui AB, Lin A, Xu W, Waldron L, Perez-Ordonez B, Weinreb I, Shi W, Bruce J, Huang SH, O'Sullivan B, Waldron J, Gullane P, Irish JC, et al. Potentially prognostic miRNAs in HPV-associated oropharyngeal carcinoma. Clin Cancer Res. 2013; 19:2154-62.
41. Vojtechova Z, Sabol I, Salakova M, Smahelova J, Zavadil J, Turek L, Grega M, Klozar J, Prochazka B, Tachezy R. Comparison of the miRNA profiles in HPV-positive and HPV-negative tonsillar tumors and a model system of human keratinocyte clones. BMC Cancer. 2016; 16:382.
42. Gao G, Gay HA, Chernock RD, Zhang TR, Luo J, Thorstad WL, Lewis JS Jr, Wang X. A microRNA expression signature for the prognosis of oropharyngeal squamous cell carcinoma. Cancer. 2013; 119:72-80.
43. Xu SH, Yang YL, Han SM, Wu ZH. MicroRNA-9 expression is a prognostic biomarker in patients with osteosarcoma. World J Surg Oncol. 2014; 12:195.
44. Liu CJ, Shen WG, Peng SY, Cheng HW, Kao SY, Lin SC, Chang KW. miR-134 induces oncogenicity and metastasis in head and neck carcinoma through targeting WWOX gene. Int J Cancer. 2014; 134:811-21.
45. Lu YC, Chen YJ, Wang HM, Tsai CY, Chen WH, Huang YC, Fan KH, Tsai CN, Huang SF, Kang CJ, Chang JT, Cheng AJ. Oncogenic function and early detection potential of miRNA-10b in oral cancer as identified by microRNA profiling. Cancer Prev Res (Phila). 2012; 5:665-74.
46. Liu CJ, Tsai MM, Tu HF, Lui MT, Cheng HW, Lin SC. miR-196a overexpression and miR-196a2 gene polymorphism are prognostic predictors of oral carcinomas. Ann Surg Oncol. 2013; 20: S406-14.
47. Severino P, Bruggemann H, Andreghetto FM, Camps C, Klingbeil Mde F, de Pereira WO, Soares RM, Moyses R, Wunsch-Filho V, Mathor MB, Nunes FD, Ragoussis J, Tajara EH. MicroRNA expression profile in head and neck cancer: HOX-cluster embedded microRNA-196a and microRNA-10b dysregulation implicated in cell proliferation. BMC Cancer. 2013; 13:533.
48. Guan X, Sturgis EM, Song X, Liu Z, El-Naggar AK, Wei Q, Li G. Pre-microRNA variants predict HPV16-positive tumors and survival in patients with squamous cell carcinoma of the oropharynx. Cancer Lett. 2013; 330:233-40.
49. Cao P, Zhou L, Zhang J, Zheng F, Wang H, Ma D, Tian J. Comprehensive expression profiling of microRNAs in laryngeal squamous cell carcinoma. Head Neck. 2013; 35:720-8.
50. Tran N, O'Brien CJ, Clark J, Rose B. Potential role of micro-RNAs in head and neck tumorigenesis. Head Neck. 2010; 32:1099-111.
51. Wang X, Wang HK, Li Y, Hafner M, Banerjee NS, Tang S, Briskin D, Meyers C, Chow LT, Xie X, Tuschl T, Zheng ZM. microRNAs are biomarkers of oncogenic human papillomavirus infections. Proc Natl Acad Sci U S A. 2014; 111:4262-7.
52. Lajer CB, Nielsen FC, Friis-Hansen L, Norrild B, Borup R, Garnaes E, Rossing M, Specht L, Therkildsen MH, Nauntofte B, Dabelsteen S, von Buchwald C. Different miRNA signatures of oral and pharyngeal squamous cell carcinomas: a prospective translational study. Br J Cancer. 2011; 104:830-40.
53. Wong N, Khwaja SS, Baker CM, Gay HA, Thorstad WL, Daly MD, Lewis JS Jr, Wang X. Prognostic microRNA signatures derived from The Cancer Genome Atlas for head and neck squamous cell carcinomas. Cancer Med. 2016; 5:1619-28.
54. Altman DG. 2015. Practical Statistics for Medical Research: Chapman and Hall.
55. Machida T, Tomofuji T, Ekuni D, Maruyama T, Yoneda T, Kawabata Y, Mizuno H, Miyai H, Kunitomo M, Morita M. MicroRNAs in Salivary Exosome as Potential Biomarkers of Aging. Int J Mol Sci. 2015; 16:21294-309.
56. National Comprehensive Cancer Network. 2015. NCCN Clinical Practice Guidelines in Oncology: Head and Neck Cancers.
57. Pandit P, Cooper-White J, Punyadeera C. High-yield RNA-extraction method for saliva. Clin Chem. 2013; 59:1118-22.
58. Mohamed R, Campbell JL, Cooper-White J, Dimeski G, Punyadeera C. The impact of saliva collection and processing methods on CRP, IgE, and Myoglobin immunoassays. Clin Transl Med. 2012; 1:19.
59. Bustin SA, Shipley GL, Vandesompele J, Wittwer CT, Benes V, Garson JA, Hellemans J, Huggett J, Kubista M, Mueller R, Nolan T, Pfaffl MW. The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments. Clin Chem. 2009; 55:611-22.
60. R Core Team. 2013. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria.
61. Hornik K, Buchta C, Zeileis A. Open-source machine learning: R meets Weka. Computational Statistics. 2008; 24:225-32.
62. Kuhn M, Wing J, Weston S, Williams A, Keefer C, Engelhardt A, Cooper T, Mayer Z, Team RC, Benesty M. 2014. caret: classification and regression training. R package version 6.0-24.
63. Witten IH, Frank E. 2005. Data Mining: Practical machine learning tools and techniques: Morgan Kaufmann.
64. Sing T, Sander O, Beerenwinkel N, Lengauer T. ROCR: visualizing classifier performance in R. Bioinformatics. 2005; 21:3940-1.