
INTRODUCTION
Echinococcosis, also called hydatid disease, is a zoonotic parasitic disease associated with economic losses in the livestock industry and serious human health risks [1]. There are over 1 million people infected with echinococcosis worldwide at any given time [2]. Cystic echinococcosis (CE) caused by Echinococcus granulosus is the most common form identified in humans in the global context [3]. According to data from the WHO, CE was found to be widely distributed in most pastoral and rangeland areas worldwide, and associated with a burden.
Human echinococcosis has a long incubation period and complicated transmission routes [4]. Common definitive hosts include dogs, wolves, fox and other carnivorous animals [5]. Large numbers of adult hydatid parasites are often identified in the small intestine of definitive host animals. Gravid proglottides, or eggs produced by adult parasites, are released from the body via the host’s droppings. Intermediate hosts, which include herbivorous and omnivorous animals [6], eat eggs or proglottid from polluted soil, water, pasture, etc. Humans are accidental intermediate hosts and, similar to other intermediate hosts, acquire infection via the fecal-oral route; however, humans do not participate in the transmission cycle [7].
A recent meta-analysis [8] showed that present studies on CE have identified the following predictive factors: source of infection, such as “dog ownership”; route of transmission, such as food- and water-borne transmission; and socio-cultural, such as age, income, gender and education level. A systematic review [9] summarized the epidemiological factors associated with increased risk of echinococcosis infection in dogs and intermediate hosts and reported that being fed raw viscera, lacking anthelmintic treatment, and having owners that lack health education and were impoverished were risk factors. Khazaei et al. [10] analyzed the characteristics of patients with hydatid cysts and suggested that it is necessary to identify infection sources among people at high risk.
China has the highest prevalence rate of human echinococcosis worldwide [11, 12]. The major epidemic areas are provinces in western China and the border areas of the Qinghai-Tibet Plateau [13]. An analysis of the endemic status of echinococcosis in China showed that 10 790 cases of echinococcosis were reported in China from 2004 to 2008, 87.3% of which were identified in patients from the Xinjiang Uygur Autonomous Region, Tibet Autonomous Region, and Gansu, Sichuan and Qinghai Provinces. [14]
Several studies have evaluated echinococcosis risk factors in China in recent years. Bai Y et al. [15] surveyed 451 Tibetans students living in rural Tianzhou County in Gansu Province and suggested that age, gender and hunting status had an effect on the disease infection. Schantz PM et al. [16] surveyed 3703 volunteers in Qinghai Province from June 1997 to June 1998, and the results of the multivariate analysis suggested that potential risk factors included livestock ownership, age > 25 years, female gender, herding occupation and nomadic status. Li TY et al. [17] conducted a study in Shiqu County, Sichuan Province, which has been reported to have the highest human echinococcosis prevalence in the world [18], and found that risk factors included age, gender, dog ownership and sources of drinking water. However, thus far, these studies have had some limitations that should be considered, as most of the studies occurred in an individual city or county, and none of the studies analyzed the influence of intervention measures on human echinococcosis, which, at present, mainly include sheep immunization, dog deworming and health education in China [19].
Thus, the China Animal Health and Epidemiology Center (CAHEC) of Ministry of Agriculture of the People’s Republic of China (MoA) conducted this study to obtain a greater understanding of the prevalence of human echinococcosis in western China, identify the factors associated with the disease infection and evaluate the current measures.
RESULTS
Participant characteristics
The characteristics of the 1211 herding families are presented in Table 1. The average number of family members was 4.8±1.6, which was higher than the national average (3.02, 2015) [20]. More than 90% of the investigated families were dog owners, and the average number of dogs owned was 1.2. A total of 90 patients with CE were identified which were distributed among 90 families.
Table 1: Demographic characteristics of herding families surveyed
Type |
N (%) |
Mean±SD |
|---|---|---|
Male |
1022 (84.4) |
|
Age (year) |
46.2±11.8 |
|
Below the junior middle school education |
1073 (88.6) |
|
Family population |
4.8±1.6 |
|
Religions |
||
Buddhism |
805 (66.5) |
|
Islam |
243 (20.1) |
|
Others |
163(13.5) |
|
Languages most often spoken |
||
Chinese |
275(22.7) |
|
Tibetan language |
770 (63.6) |
|
Others |
166 (13.7) |
|
Raising livestock |
1211 (100) |
|
Cattle restock |
19.5±22.4 |
|
Sheep restock |
135.1±171.5 |
|
Households owned dogs |
1114 (91.9) |
|
The number of domestic dogs |
1.2±0.9 |
|
The reasons for keeping dogs |
||
Help graze |
784 (64.7) |
|
As a pet |
603 (49.8) |
|
Housesitting |
35 (2.9) |
|
Others |
712 (58.8) |
|
Producing activity and living environment |
||
The sheep immunization |
413(34.05) |
|
Domestic dogs deworming |
537(44.30) |
|
Dog free to roam |
819(67.52) |
|
Slaughter at home |
547(45.09) |
|
Feed dogs with viscera |
765(63.07) |
|
Drink unboiled water |
892(73.54) |
|
Eat raw vegetables |
518(42.70) |
|
Do not wash hands before meals |
1011(83.35) |
|
Often see stray dogs near habitations |
783(64.55) |
|
Often see wild animals near habitations |
416(34.30) |
|
Being concerned about the livestock echinococcosis |
495(40.81) |
|
Being concerned about family members echinococcosis |
494(40.73) |
Prevalence of human echinococcosis
Ninety patients who had been diagnosed with human echinococcosis were identified among the surveyed families. When the number of households surveyed × average household size (5813) was used as the denominator value, the average CE prevalence was 1.55%. The prevalence rates of CE in different provinces are shown in Table 2.
Table 2: The prevalence of CE in different province
Provinces and regions |
The no. of patients |
The no. of population |
Prevalence (%) |
χ2 |
P |
|---|---|---|---|---|---|
Xinjiang Uygur Autonomous Region |
14 |
1365 |
1.03 |
||
Tibet Autonomous Region |
25 |
996 |
2.51 |
11.53 |
0.020 |
Gansu Province |
11 |
1123 |
0.98 |
||
Sichuan Province |
21 |
1258 |
1.67 |
||
Qinghai Province |
19 |
1072 |
1.77 |
||
Total |
90 |
5813 |
1.55 |
The results of the chi-square test suggested that the presence of significant between province difference in the prevalence of CE (p<0.05). Tibet had the highest prevalence, which was 2.51%.
Single factor analysis of CE infection
The presence of CE patients in a family was used as the dependent variable, and the influences of 11 predictor variables, including “immunizing sheep”, “feeding dogs with viscera”, and “allowing dogs to roam free”, et. Al., were analyzed using single factor logistic regression analysis. All of these variables were binary variables. The results are shown in Table 3.
Table 3: Factors related to having CE patients in a family: single factor analysis
Variables |
β |
Wald |
P |
OR |
95% CI |
|
|---|---|---|---|---|---|---|
Lower |
Upper |
|||||
The sheep immunization |
- 1.05 |
16.59 |
0.000 |
0.35 |
0.21 |
0.58 |
Domestic dogs deworming |
- 0.90 |
0.11 |
0.739 |
0.91 |
0.54 |
1.55 |
Allowing dogs to roam free |
1.16 |
19.15 |
0.000 |
3.18 |
1.89 |
5.33 |
Slaughter at home |
1.12 |
18.44 |
0.000 |
3.02 |
1.83 |
5.01 |
Feeding dogs with viscera |
1.24 |
18.75 |
0.000 |
3.46 |
1.97 |
6.07 |
Drinking non-boiled water |
0.78 |
8.31 |
0.004 |
2.18 |
1.28 |
3.71 |
Eating raw vegetables |
0.62 |
5.81 |
0.016 |
1.86 |
1.12 |
3.08 |
Not washing hands before meals |
1.11 |
12.71 |
0.000 |
3.04 |
1.65 |
5.59 |
Often seeing stray dogs near habitations |
0.97 |
8.87 |
0.003 |
2.63 |
1.39 |
4.98 |
Often seeing wild animals near habitations |
0.65 |
6.59 |
0.010 |
1.91 |
1.16 |
3.12 |
Being concerned about family members echinococcosis |
- 0.73 |
6.71 |
0.010 |
0.48 |
0.28 |
0.84 |
Multiple factor analysis of CE infection
Variables identified as statistically significantly in the single factor analysis were included in the multifactor logistic regression analysis. The analysis results, which are presented in Table 4, showed that the sheep immunization and being concerned about family members echinococcosis were associated with reduced the risk of infection, while two dog-related factors (allowing dogs to roam free, feeding dogs with viscera), four living habit-related factors (slaughter at home, drinking non-boiled water, eating raw vegetables, not washing hands before meals), and two living condition-related factors (often seeing stray dogs or wild animals near habitations) were significantly associated (p<0.05) with increased risk of human echinococcosis.
Table 4: Factors related to having CE patients in a family: multiple factor analysis
Variables |
β |
Wald |
P |
OR |
95% CI |
|
|---|---|---|---|---|---|---|
Lower |
Upper |
|||||
The sheep immunization |
-1.05 |
16.59 |
0.000 |
0.35 |
0.21 |
0.58 |
Allowing dogs to roam free |
1.15 |
19.09 |
0.000 |
3.17 |
1.89 |
5.31 |
Feeding dogs with viscera |
1.11 |
18.60 |
0.000 |
3.04 |
1.83 |
5.03 |
Slaughter at home |
1.26 |
20.25 |
0.000 |
3.53 |
2.04 |
6.12 |
Drinking non-boiled water |
0.77 |
8.20 |
0.004 |
2.15 |
1.28 |
3.63 |
Eat raw vegetables |
0.63 |
5.95 |
0.015 |
1.87 |
1.13 |
3.10 |
Not washing hands before meals |
1.12 |
13.16 |
0.000 |
3.08 |
1.68 |
5.65 |
Often seeing stray dogs near Habitations |
0.96 |
8.76 |
0.003 |
2.60 |
1.38 |
4.91 |
Often seeing wild animals near habitations |
0.65 |
6.69 |
0.010 |
1.92 |
1.17 |
3.14 |
Being concerned about family members echinococcosis |
-0.72 |
6.62 |
0.010 |
0.49 |
0.28 |
0.84 |
Constant |
-4.87 |
126.53 |
0.000 |
0.08 |
- |
- |
DISCUSSION
According to the WHO, incidence of human CE may exceed 50/100 000 in endemic regions. The results of a national survey regarding the hydatid disease epidemic that was conducted in 2012 showed that the average prevalence of human echinococcosis was 0.24% in the 263 counties in western China. We identified a higher prevalence in the study (1.55%). We identified a higher prevalence in the study (1.55%). Echinococcosis is an often neglected disease with a long incubation period [21]. This prevalence is likely to increase because more patients may be detected as awareness of the harms associated with echinococcosis increases among herdsmen and relevant national health support policy is implemented.
Dogs are the most common definitive host, and dogs have been identified as the primary source of human CE infection [22]. One previous study [23] showed that keeping dogs was associated with increased risk of human echinococcosis.
In our study, the results of the multiple regression result showed that “allowing dogs to roam free”, which may artificially accelerate the transmission cycle of echinococcosis, may increase the risk of infection. For example, a recent study showed that [24] the dog seropositivity rate was as high as 64.56% in Qinghai Province. Free dogs infected with adult hydatid parasites have been found to defecate openly, resulting in the dissemination of hydatid eggs into the surrounding areas. In addition, the main purpose reported for keeping dogs by herding families in our analysis to help graze according to our survey. For example, dogs stay with sheep during the grazing process. Wool may be contaminated with hydatid eggs from dog feces. Herders come into close contact with eggs during milking, shearing and other production activities and are likely to become patients.
“Feeding dogs with viscera” was also associated with increased likelihood of human infection. Surveys [25, 26] previously performed in these areas have shown that the seropositivity rate of cattle and sheep ranged from 5% to 30%. Offal from those cattle and sheep may be fed to dogs. Hydatid eggs may be consumed by dogs and gradually develop into adult parasites in the small intestine. Thus, a new cycle of echinococcosis transmission begins.
Previous studies [27, 28] have identified slaughterhouses as possible influencing echinococcus risk. This is consistent with our findings. Livestock has been found to serve as an intermediate host [29, 30]. We estimated that “slaughtering at home” may increase the risk of human echinococcosis because offal from sick animals are usually fed to domestic or stray dogs by herdsmen rather than safely disposing of these viscera during slaughter, directly contributing to increased risk of human echinococcus.
As previously mentioned, humans become “victims” because of consuming proglottid or eggs in contaminated food or water. The results of this study showed that some factors related to the living habits, such as “’not washing hands before meals”, “drinking non-boiled water” and “eating raw vegetables” may contribute to increased risk, results that were consistent with those of previous studies [16, 31, 32].
In pastoral areas, herdsmen often drink non-boiled water from rivers or lakes, and animals also drink from the same water sources while grazing. Eating raw vegetables or other foods is also very common. Tsampa, which is often consumed with the fingers, is the important component of the diet of herding families. However, members of these families are often unable to wash their hands before eating due to a lack of water or being busy with production activities. Echinococcosis eggs in the external environment can go enter the body through these bad habits.
The following two environmental-related factors were identified: often seeing stray dogs and often seeing wild animals near habitations. These variables were included in analysis, and both of these variables were identified as potential risk factors for infection. This finding was similar to the results of a previous study that found that living environment has an effect on human echinococcosis [32]. Another study found that similar to dogs, common wildlife species such as wolves and foxes may act as disease vectors [29]. This finding suggested that governing stray dogs and keeping habitations away from stray dogs and wild animals may reduce the risk of echinococcosis.
To determine whether prevention and control measures have positively impacted the occurrence of echinococcosis infection among herdsmen, we evaluated and attempted to analyze the etiology of infection. Although 44.30% of the surveyed herding families could provide dogs with anti-parasitic agents, the deworming of domestic dogs had no effect on human infection in our study. Similar to Gerardo AJ’s study [33], the effect of this variable was not significant. This finding may be related to the difficulties in completely deworming identified during our field observations and interviews. First, it is difficult to deworm drugs at the recommended frequency (every dog, every month). Additionally, being busy with production activities or psychological indifferent made feeding the deworming tablets according to recommendations more difficult. Second, safe disposal of feces from dogs after deworming was also a challenge. When feces are not deeply buried or burned, hydatid eggs may survive.
Osbom PJ’s study showed that [34] resistance to immunization among sheep spines ball larva may effectively resist various fine grained spines ball larva and reduce the incidence of sheep echinococcosis infection. Control of sheep infection is beneficial to cut off the transmission chain of cystic echinococcosis [30]. The results of the regression analysis showed that herding families who immunized their sheep were 0.35 times less likely to develop echinococcosis than those who did not immunize their sheep. The “national animal disease compulsory immunization program 2016” [35] issued by the Chinese Ministry of Agriculture stated that the immunization strategy used for echinococcosis should be independently selected by animal husbandry and veterinary departments and other relevant departments at the provincial level according to the actual needs in highly endemic areas. This recommendation suggests that it may be necessary to revise immunization processes in these areas to ensure the prevention and control of echinococcus in the future.
Being concerned about echinococcosis in livestock or family members served as a reflection of the herdsmen’s health education regarding the prevention and control of echinococcosis. Craig PS’s study [36] analyzed echinococcosis interventions in various countries and regions around the world from 1986 to 2002 and found that health education had little effect on the risk of echinococcosis transmission. Similar results were identified in our research. Further study of the effect of health education on human echinococcosis in the evaluated western provinces and regions is the next objective of this research group.
Our study has several strengths. China has the largest human hydatid disease epidemic, especially in the western provinces and autonomous regions. Carrying out epidemiological surveys that includes the populated areas instead of just individual provinces will be necessary to obtain a better understanding of this disease. The 15 counties surveyed in this study were distributed in five provinces in western China. Using the data obtained from these surveys, we briefly described the prevalence of human echinococcosis in five provinces, including the Tibet Autonomous Region, which had not been assessed previously. In addition to evaluating host factors, living habits and living environment, existing prevention and control measures were also analyzed. Because of these advantages, our results could be utilized to support the prevention and control of hydatid disease in China according to the local conditions.
This study had two limitations. First, individual characteristics that may have effected infection, such as gender and level of education, were not included in the models. These variables were excluded because our analysis focused on the herding family unit and, specifically, the life styles, living environments and prevention and control measures there in. Furthermore, we included a limited number of affected families, and an analysis of whether different provinces have different risk factors could not be performed in this study. More in-depth investigations and comparative analyses will be carried out in 2017.
In conclusion, the prevention and control of echinococcosis is a priority in western China. Immunizing sheep and appropriately managing domestic and stray dogs should serve aseffective measures for controlling CE at present. Efforts to improve living environments and behaviors should consider the natural conditions, characteristics of production and the lives of herdsmen’s families. Further studies are needed to clarify the importance of health education.
MATERIALS AND METHODS
Ethics statement
The research protocol was approved by the CAHEC of MoA (Nong Fa [2016] No. 11). The questionnaire survey received ethics approval from the Division of Epidemiology Survey within CAHEC [37]. All participants must sign a written informed consent when they were informed about the purpose and procedures of the study. In case of anyone not understanding Chinese, investigators from the local veterinary station explained in minority language. There were no animal samples taken as part of our study.
Participants
For the number of echinococcosis families in western provinces and regions is unclear at present, π=0.5, allowable error δ=0.03, ɑ= 0.05. 1067 is the smallest unit of observation in the calculation of sample size. In our study, 1500 herding families were screened in Xinjiang Uygur Autonomous Region, Tibet Autonomous Region, and Gansu, Sichuan and Qinghai Provinces. Considering the vast and sparse population in these areas, a combination of probability and convenience sampling were used. The full process of sample selection was as follows: three animal husbandry counties were selected by Animal Diseases Control and Prevention Centers in each of the 5 provinces according to the probability of investigative work; then, 100 families were randomly selected in each county by computer. According to the information provided by the county veterinary department, the SPSS software was used to achieve a completely random. The steps were: data - select cases - random sample of cases and the definition sample size = 100.
Study area
The research was conducted in 15 counties (Figure 1. Vector map filecame from Resources and Environment Science Data Center, Chinese Academy of Sciences and was performed with ArcGIS10.2 software). The terrain of these areas is complex, especially in the Tibet, Sichuan and Qinghai areas, and the average altitude in the surveyed counties was above 3000 meters. Animal husbandry is the main form of agricultural production in these areas.
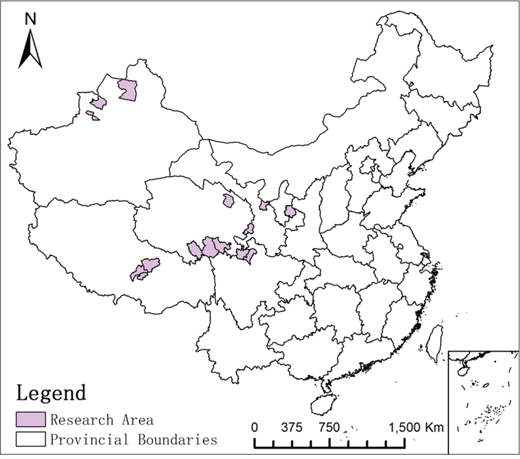
Figure 1: 15 counties conducted in the research.
Method and content
The survey was carried out from May 1, 2016 to November 31, 2016. Data were collected using questionnaires that included the following 5 parts: sociodemographic characteristics, echinococcosis infection in family members, livestock breeding situation, production activity and living environment. The questionnaire was used in Chinese. The staffs from the county veterinary department were responsible for the translation of minority languages and Chinese between the investigators and the subjects when they were not familiar with Chinese. The head of the household, which was defined as the person who in charge of the household and any dependents [38], was responsible for completing the questionnaire. Case confirmed was based on the results of the investigation of the family’s active medical treatment or the health examination that has been carried out in these areas. Respondents were asked to provide relevant diagnostic material to confirm the presence of human echinococcosis among family members. The diagnostic materials include two types: the diagnosis certificate issued by the hospital; the results of the imaging examination. When the answer of respondent is “yes” for the question of “whether or not there is a family member (including oneself) suffering from hydatid disease”, we ask one of the two. The design of the survey questionnaire and training of investigators were completed by the CAHEC.
Statistical analysis
Overall, 1213 completed questionnaires were collected and the completion rate was 80.87%. Two families located in Sichuan Province with alveolar echinococcosis (AE) patients were excluded. AE was caused by Echinococcus multilocularis. It is well-known that life-cycles of Echinococcus granulosus and E. multilocularis are quite different [39]. As a result, 1211 were analyzed, Statistical analysis was performed using SPSS 20.0. The demographic data for the heads of household and characteristics herding families were analyzed by using descriptive statistics and chi-squared test. Binary logistic regression with forced entry was performed to explore the risk factors for human echinococcosis. In all statistical analyses, p<0.05 was considered statistically significant.
Author contributions
RXY and CHY had full access to all of the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis. CHY, XDS, RXY, QGX, PL and HRW designed the study. XDS, RXY, QGX, HZ and HRW performed the study. RXY, HZ, LG and DH acquired and analyzed the data. RXY and HZ drafted the manuscript. All authors critically revised the manuscript. CHY and XDS had guarantor.
ACKNOWLEDGMENTS
We are grateful to Baoxu Huang, Youming Wang, Jingli Kang, Jinhua Li, Ailing Liu and Wen Zhao (China Animal Health and Epidemiology Center, Qingdao) for championing the preparation of this manuscript. We are grateful to Animal Diseases Control and Prevention Centers in Xinjiang, Tibet, Gansu, Sichuan and Qinghai for field research. Finally, the authors would like to thank Meng Fan and Xinmiao Rong (School of Mathematics and Statistics, Northeast Normal University, Changchun) for involving in the investigation. This work was also supported by Yanfeng Zhou (Tongji Medical College, HUST, Wuhan) and Chao Zhang (Center for Evidence-Based Medicine and Clinical Research, Taihe Hospital, Hubei University of Medicine, Shiyan).
CONFLICTS OF INTEREST
All authors report there are no conflicts of interest related to the present article.
FUNDING
This study was supported by the National Key Research and Development Program of China (No.2017YFC 1200502) and the National Natural Science Foundation of China (No.81773552, 81273179). The fundings had no roles in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
REFERENCES
1. Cadavid RA, Yang YR, McManus DP, Gray DJ, Giraudoux P, Barnes TS, Williams GM, Soares MR, Hamm NA, Clements AC. The landscape epidemiology of echinococcoses. Infect Dis Poverty. 2016; 5:13.
2. World-Health-Organization. Echinococcosis: Factsheet. Available from: http://www.who.int/mediacentre/factsheets/fs377/en/.
3. McManus DP, Gray DJ, Zhang W, Yang Y. Diagnosis, treatment, and management of echinococcosis. BMJ. 2012; 344:e3866.
4. Eckert J, Thompson RC. Historical aspects of echinococcosis. Adv Parasitol. 2017; 95:1-64.
5. Eckert J, Deplazes P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev. 2004; 17:107-135.
6. Kachani M, Heath D. Dog population management for the control of human echinococcosis. Acta Trop. 2014; 139:99-108.
7. Moro P, Schantz PM. Echinococcosis: a review. Int J Infect Dis. 2009; 13:125-133.
8. Possenti A, Manzano-Roman R, Sanchez-Ovejero C, Boufana B, La Torre G, Siles-Lucas M, Casulli A. Potential risk factors associated with human cystic echinococcosis: systematic review and meta-analysis. PLoS Negl Trop Dis. 2016; 10:e5114.
9. Lightowlers MW, Heath DD. Immunity and vaccine control of Echinococcus granulosus infection in animal intermediate hosts. Parassitologia. 2004; 46:27-31.
10. Khazaei S, Rezaeian S, Khazaei Z, Goodarzi E, Khazaei S, Mohammadian M, Salehiniya H, Ayubi E, Mohammadian-Hafshejani A. Epidemiological and clinical characteristics of patients with hydatid cysts in Khorasan Razavi province, from 2011 to 2014. Iran J Parasitol. 2016; 11:364-370.
11. Torgerson PR, Keller K, Magnotta M, Ragland N. The global burden of alveolar echinococcosis. PLoS Negl Trop Dis. 2010; 4:e722.
12. Budke CM, Deplazes P, Torgerson PR. Global socioeconomic impact of cystic echinococcosis. Emerg Infect Dis. 2006; 12:296-303.
13. Wang Q, Huang Y, Huang L, Yu W, He W, Zhong B, Li W, Zeng X, Vuitton DA, Giraudoux P, Craig PS, Wu W. Review of risk factors for human echinococcosis prevalence on the Qinghai-Tibet Plateau, China: a prospective for control options. Infect Dis Poverty. 2014; 3:3.
14. Wang LY, Wu WP, Zhu XH. [The endemic status of hydatidosis in China from 2004 to 2008]. [Article in Chinese]. Chinese J Zoonoses. 2010; 26:699-702.
15. Bai Y, Cheng N, Wang Q, Cao D. An epidemiological survey of cystic echinococcosis among Tibetan school pupils in West China. Ann Trop Paediatr. 2001; 21:235-238.
16. Schantz PM, Wang H, Qiu J, Liu FJ, Saito E, Emshoff A, Ito A, Roberts JM, Delker C. Echinococcosis on the Tibetan Plateau: prevalence and risk factors for cystic and alveolar echinococcosis in Tibetan populations in Qinghai Province, China. Parasitology. 2003; 127:S109-S120.
17. Tiaoying L, Jiamin Q, Wen Y, Craig PS, Xingwang C, Ning X, Ito A, Giraudoux P, Wulamu M, Wen Y, Schantz PM. Echinococcosis in Tibetan populations, western Sichuan Province, China. Emerg Infect Dis. 2005; 11:1866-1873.
18. Li T, Chen X, Zhen R, Qiu J, Qiu D, Xiao N, Ito A, Wang H, Giraudoux P, Sako Y, Nakao M, Craig PS. Widespread co-endemicity of human cystic and alveolar echinococcosis on the eastern Tibetan Plateau, northwest Sichuan/southeast Qinghai, China. Acta Trop. 2010; 113:248-256.
19. Ministry of Agriculture of the People’s Republic of China. BeiJing; [cited 2016 Oct 27]. “the National Development Program of the Veterinary Health (2016-2020)”. Available from: http://www.moa.gov.cn/zwllm/ghjh/201610/t20161027_5323267.htm.
20. National Health and Family Planning Commission of the People’s Republic of China. BeiJing; [cited 2015 May 15]. “Chinese family Development Report 2016”. Available from: http://www.nhfpc.gov.cn/zhuz/index.shtml.
21. World-Health-Organization. The control of neglected zoonotic diseases: community-based interventions for prevention and control. Geneva: WHO/HTM/NTD/NZD/2011.1; 2011.
22. Craig PS, Rogan MT, Campos-Ponce M. Echinococcosis: disease, detection and transmission. Parasitology. 2003; 127:S5-S20.
23. Campos-Bueno A, Lopez-Abente G, Andres-Cercadillo AM. Risk factors for Echinococcus granulosus infection: a case-control study. Am J Trop Med Hyg. 2000; 62:329-334.
24. Liu P, Cai JS, Li JH, Kang JL. [Pilot survey on prevention and control of echinococcus in Qinghai province]. [Article in Chinese]. China AHI. 2016; 33:7-9.
25. Yang AG, Guo L, Deng YQ, Hong W, Wen H, Chen D, Zhou MZ, Mao GQ, Chen B. [The epidemiology of Livestock Echinococcosis in Sichuan province, China]. [Article in Chimese]. Vet Orient. 2016; 8:155-156.
26. Fu YJ, Wang SX, Lin YQ, Li XY. [Echinococcosis in cattle and sheep in QingHai province, China]. [Article in Chinese]. Animal Husband Vet Med. 2015; 47:150-151.
27. Carmona C, Perdomo R, Carbo A, Alvarez C, Monti J, Grauert R, Stern D, Perera G, Lloyd S, Bazini R, Gemmell MA, Yarzabal L. Risk factors associated with human cystic echinococcosis in Florida, Uruguay: results of a mass screening study using ultrasound and serology. Am J Trop Med Hyg. 1998; 58:599-605.
28. Wang YH, Rogan MT, Vuitton DA, Wen H, Bartholomot B, Macpherson CN, Zou PF, Ding ZX, Zhou HX, Zhang XF, Luo J, Xiong HB, Fu Y, et al. Cystic echinococcosis in semi-nomadic pastoral communities in north-west China. Trans R Soc Trop Med Hyg. 2001; 95:153-158.
29. McManus DP, Zhang W, Li J, Bartley PB. Echinococcosis. Lancet. 2003; 362:1295-1304.
30. Deplazes P, Rinaldi L, Alvarez RC, Torgerson PR, Harandi MF, Romig T, Antolova D, Schurer JM, Lahmar S, Cringoli G, Magambo J, Thompson RC, Jenkins EJ. Global distribution of alveolar and cystic echinococcosis. Adv Parasitol. 2017; 95:315-493.
31. Yang YR, Sun T, Li Z, Zhang J, Teng J, Liu X, Liu R, Zhao R, Jones MK, Wang Y, Wen H, Feng X, Zhao Q, et al. Community surveys and risk factor analysis of human alveolar and cystic echinococcosis in Ningxia Hui Autonomous Region, China. Bull World Health Organ. 2006; 84:714-721.
32. Harandi MF, Moazezi SS, Saba M, Grimm F, Kamyabi H, Sheikhzadeh F, Sharifi I, Deplazes P. Sonographical and serological survey of human cystic echinococcosis and analysis of risk factors associated with seroconversion in rural communities of Kerman, Iran. Zoonoses Public Health. 2011; 58:582-588.
33. Acosta-Jamett G, Weitzel T, Boufana B, Adones C, Bahamonde A, Abarca K, Craig PS, Reiter-Owona I. Prevalence and risk factors for echinococcal infection in a rural area of northern Chile: a household-based cross-sectional study. PLoS Negl Trop Dis. 2014; 8:e3090.
34. Osborn PJ, Heath DD. Immunisation of lambs against Echinococcus granulosus using antigens obtained by incubation of oncospheres in vitro. RES VET SCI. 1982; 33:132-133.
35. Ministry of Agriculture of the People’s Republic of China. BeiJing; [cited 2017 Mar 20]. “The National Plan for Compulsory Immunization of Animal Epidemic 2017”. Available from: http://www.moa.gov.cn/zwllm/ghjh/201703/t20170320_5530358.htm.
36. Craig PS, McManus DP, Lightowlers MW, Chabalgoity JA, Garcia HH, Gavidia CM, Gilman RH, Gonzalez AE, Lorca M, Naquira C, Nieto A, Schantz PM. Prevention and control of cystic echinococcosis. Lancet Infect Dis. 2007; 7:385-394.
37. Zhou X, Li Y, Wang Y, Edwards J, Guo F, Clements AC, Huang B, Magalhaes RJ. The role of live poultry movement and live bird market biosecurity in the epidemiology of influenza A (H7N9): a cross-sectional observational study in four eastern China provinces. J Infect. 2015; 71:470-479.
38. Hassan OA, Affognon H, Rocklöv J, Mburu P, Sang R, Ahlm C, Evander M. The One Health approach to identify knowledge, attitudes and practices that affect community involvement in the control of Rift Valley fever outbreaks. PLoS Neglect Trop Dis. 2017; 11:e5383.
39. Bagrade G, Deksne G, Ozolina Z, Howlett SJ, Interisano M, Casulli A, Pozio E. Echinococcus multilocularis in foxes and raccoon dogs: an increasing concern for Baltic countries. Parasit Vectors. 2016; 9:615.