
INTRODUCTION
POEMS syndrome, also called as Crow-Fukase syndrome or Takatsuki syndrome, is a rare paraneoplastic syndrome characterized by polyneuropathy, organomegaly, endocrinopathy, mono-clonal gammopathy, and skin changes [1, 2]. It’s associated with an underlying clonal plasma cell dyscrasia [1, 2]. Other important manifestations include Castleman’s disease, sclerotic bone lesions, papilledema, thrombocytosis, polycythemia, extravascular volume overload, pulmonary hypertension, clubbing, weight loss, thrombotic diatheses and vitamin B12 deficiency [1, 3, 4]. Although the pathogenesis of POEMS syndrome is still unclear, the overproduction of vascular endothelial growth factor (VEGF), as one of the major diagnostic criteria of POEMS syndrome [1], may contribute to most of the above clinical manifestations and correlates with the disease activity and response to therapy [5, 6]. VEGF targets vessel endothelial cell by increasing vascular permeability and promoting angiogenesis [7-9], which may result in arterial or venous thrombosis [10, 11]. Recently, ischemic stroke is attracting increasing attention as a less-recognized manifestation of POEMS syndrome and its 5-years risk is reported to be 13.4% [12]. However, only a few patients have been reported to have ischemic stroke. The multi-vessel anomaly was documented in several studies [13-16], but the pathogenesis of cerebral vasculopathy is not clear.
In the current study, we presented a case of ischemic stroke and cerebral vasculitis diagnosed by the radiographic feature of vasculitis pathophysiology using magnetic resonance vessel-wall imaging technique in a female patient with POEMS syndrome. Subsequently, a comprehensive analysis of published literature was undertaken to study the clinical features and pathogenesis of ischemic stroke in POEMS syndrome.
CASE REPORT
A 65-year-old female from China was initially admitted to our hospital with a 2-year history of numbness and mild weakness in the distal of low extremities. She experienced chest tightness, cough, fatigue and edema in low extremities for three years with a diagnosis made by a local hospital involving serous pericarditis, multiple lymphadenopathies, bronchiectasis and silent lacunar infarction. She was receiving aspirin, furosemide and spironolactone daily after discharge. She had no relevant family history and medical history of diabetes mellitus, hypertension, hypercholesteremia, alcohol consumption, cigarette smoking and drug abuse. Noteworthy features were found in the review of systems including a 12kg weight loss and pigmentation of skin in the neck, chest, back and limbs during the past two years. The tentative diagnosis of distal symmetrical sensorimotor polyneuropathies was made after nerve conduction studies and the neurological examination on admission. Meanwhile the initial treatment of aspirin, atorvastatin and oral mecobalamin started. On the third hospital day, acute respiratory infection occured, then empirical antibiotics treatment, including penicillin and levofloxacin, was initiated for this patient.
She developed sudden onset of dysarthria and right hemiplegia on the midnight of the seven days after hospitalization. Positive physical examination revealed marasmus, splenomegaly, clubbed-finger, pitting edema in both lower extremities, bilateral papilledema and hyperpigmentation in neck, chest and four limbs. Several nontender enlarged lymph nodes were palpable in the fossa axillary, inguinal area, neck region and left postauricular region. Neurological examination was notable for dysarthria, right hemiplegia with Grade III muscle strength, absent tendon reflexes, and signs of distal symmetrical sensorimotor polyneuropathies in extremities.
Routine laboratory tests, including blood routine, biochemistry test and coagulation function test, were performed and the results were listed in Table 1. It was noteworthy for moderate anemia (Red blood cell count 3.24×1012/L, hemoglobin 85 g/L), thrombocytosis (Platelet count 512×109/L), hyperhomocysteinemia (21.3 umol/L), hypoalbuminemia (35 g/L), hyperuricemia (525 umol/L), hyperfibrinogenemia (5.96 g/L), and increased blood urea nitrogen concentration (12.24 mg/L). Hypersensitive C-reactive protein (Hs-CRP, 15.82 mg/L) was slightly increasing, but the erythrocyte sedimentation rate was normal. Serum tumor marks and autoimmune antibodies were all negative. Serum hormone test was noteworthy for hypothyroidism (Free triiodothyronine (FT3, 1.73 pg/ml), free thyroxine (FT4, 0.78 ng/dl), thyroid stimulating hormone (TSH, 8.3 mIU/L) with negative antibody (thyroglobulin antibody, thyroid peroxidase antibody and thyrotrophin receptor antibody), elevated adrenocorticotropic hormone (ACTH, 150.00 pg/ml) and decreased 24-hours urine free cortisol (81.2 nmol/24h). Glycosylated hemoglobin and oral glucose tolerance test were normal. The opening pressure of cerebrospinal fluid notably increased to 300 mmH2O. Cerebrospinal fluid examination demonstrated elevated protein level (1.95 g/L) and elevated IgG level (29.0 mg/dL) with normal cell content, normal concentration of chloride and glucose, and negative oligoclonal band.
Table 1: Summary of laboratory findings in the present case
Laboratory tests |
Normal/negative |
Abnormal finding |
Routine blood test |
||
White blood cell count |
Normal |
|
Red blood cell test |
RBC 3.24×1012/L, range: 3.5-5.0×1012/L. Hemoglobin 85 g/L, range: 110-150 g/L. Hematocrit 0.27, range: 0.37-0.47. MCV 83 fl, range: 80-100 fl. MCH 26.1 pg, range: 27-34 pg. MCHC 314 g/L, range: 320-360 g/L. |
|
Platelet count |
Thrombocytosis ( 512X109/L, range: 100-300×109/L) |
|
Reticulocytes |
Mile increased (1.6%, range: 0.5-1.5 %) |
|
Test for anemia |
Mild increased erythropoietin (22.29 IU/L, range: 15-20 IU/L) Decreased serum transferrin (120 mg/dL, range: 200-340 mg/dl ) Decreased serum iron (6.20 μmol/L, range: 9-27 μmol/L ) Decreased total iron binding capacity (40.8 μmol/L, range: 50-77 μmol/L ) |
|
Hs-CRP |
Elevated (15.82 mg/L, range: 0-3 mg/L) |
|
Liver function tests |
Hypoalbuminemia (35 g/L, range: 40-55 g/L) Decreased serum prealbumin (112 mg/L, range: 200-400 mg/L ) |
|
Renal function tests |
Increased serum urea nitrogen ( 12.24 mmol/L, range: 2.8-8.2 mmol/L) |
|
Serum uric acid |
Increased (525 umol/L, range: 90-357 umol/L) |
|
Plasma homocysteine level |
Hyperhomocystinemia (21.3 umol/L, range: 5-15 umol/L) |
|
Lipid profile |
Normal |
|
Troponin T |
Normal |
|
Serum folate level |
Decreased (3.39 ng/ml, range: 3.7-19.8 ng/ml) |
|
Serum Vitamin B12 level |
Decreased (101 pg/ml, range: 180-914 pg/ml) |
|
ESR |
Normal |
|
Antiphospholipid antibody |
Negative |
|
Serum tumor marks |
Negative |
|
ANA and ENA antibodies |
Negative |
|
ANCA antibodies |
Negative |
|
Complement C3 and C4 |
Negative |
|
ASO and RF |
Negative |
|
Coagulation test |
Hyperfibrinogenemia (5.96 g/L, range: 2-4 g/L) |
|
Serum cystatin C level |
Normal |
|
Hepatitis panels |
Negative |
|
HIV antibodies and TPPA |
Negative |
|
Cerebrospinal fluid |
Increased CSF pressure (300 mmH2O, range: 80-180 mmH2O) Increased protein (1.95 g/L,range: 0-0.4 g/L) and IgG (29 mg/dl, range: 0.4-5.8 mg/dL) |
|
Oligoclonal band |
Negative |
|
Thyriod function |
Decreased free T3 (1.73 pg/ml, range: 2.30-4.20 pg/ml) Decreased free T4 (0.78 ng/dl, range: 0.90-1.80 ng/dl) Increased TSH (8.3 mIU/L, range: 0.55-4.78 mIU/L) |
|
Anti-thyroid antibodies |
Negative |
|
Endocrinopathy panels |
Increased ACTH (150.00 pg/ml, range: 7.2-63.3 pg/ml ) Decreased 24-hours urinary free cortisol (81.2 nmol/24h, range: 129.7-303.6 nmol/L) |
|
TORCH panels |
Negative |
|
Serum immunofixation |
IgG kappa monoclonal protein |
|
Urine immunofixation |
Tiny amount of IgG kappa monoclonal protein |
|
Serum VEGF |
Significantly increased (7712 pg/ml, range:100-720 pg/ml) |
MCV: mean corpuscular volume. MCH: mean corpuscular hemoglobin.
MCHC: mean corpuscular hemoglobin contentration.
Serum tumor marks: CEA, AFP, CA125, CA199, CYRFA21-1, SCC, NSE.
ANA: antinuclear antibodies. ENA: extractable nuclear antigen antibodies.
RF: rheumatoid factor. TPPA: treponema pallidum particle agglutination assay.
TSH: thyroid stimulating hormone. ACTH: adrenocorticotropic hormone.
TORCH: Toxoplasmosis, other diseases(including HIV, syphilis, and measles),rubella, cytomegalovirus and herpes simplex.
VEGF: vascular endothelial growth factor.
The nerve conduction study and electromyogram revealed diffuse distal sensorimotor polyneuropathies including both axonal and demyelinating neuropathies. Splenomegaly, lymphadenopathy, moderate ascites were confirmed by sonography. CT scan showed multiple mediastinal lymphadenectasis, right pleural effusion and bronchiectasis in the right middle lobe and left upper lobe (Figure 1). No evidence of sclerotic bone lesions was found in whole bone scan. Serum vascular endothelial growth factor was dramatically increasing (7712 pg/mL). To detect monoclonal gammopathy, serum and urine immunofixation electrophoresis were performed. It was noteworthy in serum for an IgG kappa monoclonal protein with increased IgG and free kappa chain (Figure 2). The presence of a very tiny amount of IgG kappa monoclonal protein was detected in urine immunofixation.
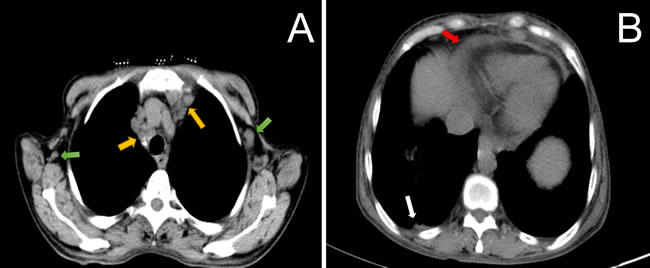
Figure 1: CT scan of the thorax showed multiple axillary (Figure 1A, green arrow), and mediastinal lymphadenopathy (Figure 1A, yellow arrow) in combination with right pleural effusion (Figure 1B, white arrow) and pericardial effusion (Figure 1B, red arrow).
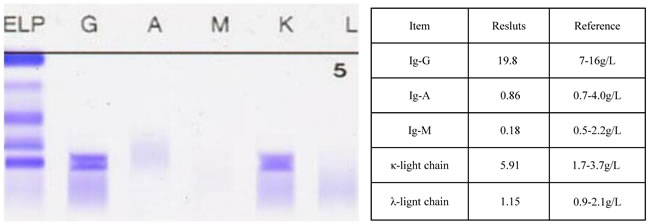
Figure 2: Serum immunofixation electrophoresis revealed an IgG kappa monoclonal protein(Figure 2A) with increased IgG and free kappa chain (Figure 2B).
The brain magnetic resonance imaging (MRI) was done three days after stroke onset. The diffusion-weighted imaging showed multiple acute infarction lesions in end artery border-zone of the left cerebral hemisphere (Figure 3). Transthoracic echocardiography revealed a moderate pulmonary arterial hypertension with a systolic pressure of 53 mmHg and mild pericardial effusion of 4 mm thickness without the presence of abnormal valvular structure and decreased left ventricular ejection fraction. There was no evidence for foramen ovale, atrial myxoma, left atrial appendage thrombus and any aortic pathologies in transesophageal echocardiography. Transcranial doppler, Holter monitoring, and carotid artery ultrasound failed to detect the embolic source. CT angiography showed a great aortic arch and normal artery except diffuse and moderate stenosis in the large vessels from the origin of left internal carotid artery (ICA) to the M1 segment of the left middle cerebral artery (MCA) (Figure 4). Strong enhancement of thickened vessel wall in left ICA was observed with high-resolution black-blood gadolinium-enhanced T1-weighted images, suggestive of vasculitis (Figure 5).
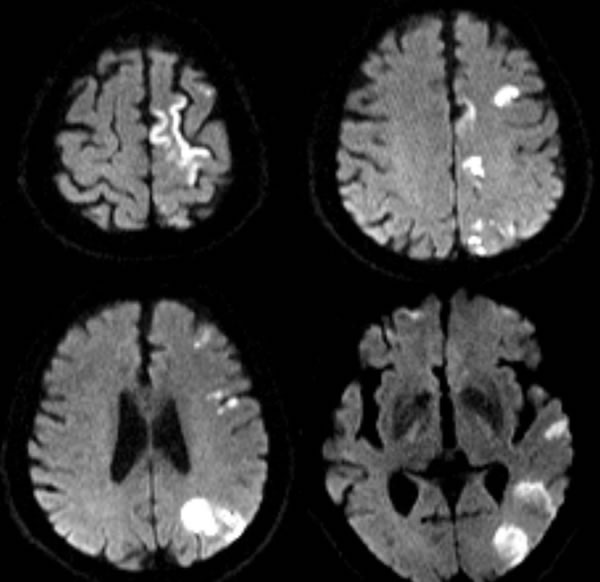
Figure 3: Axial DWI sequences showed multiple acute infarction lesions in end artery border-zone of left cerebral hemisphere.
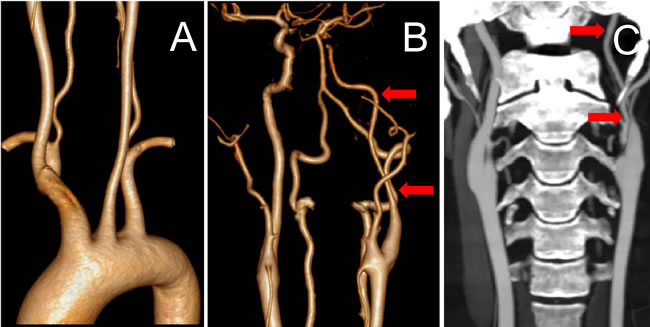
Figure 4: CT angiography showed a great aortic arch and normal artery (Figure 4A) except diffuse and moderate stenosis in the large vessels from the origin of left ICA to the M1 segment of the left MCA (Figure 4B and 4C, red arrow).
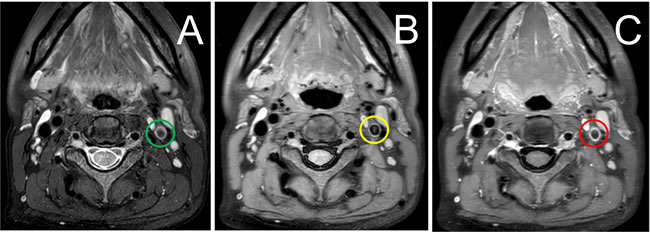
Figure 5: High-resolution T2-weighted imaging showed concentric hyperintensity and thickening in the vessel wall of left ICA and (Figure 5A, green circle). High-resolution, black-blood MRI before (Figure 5B, yellow circle) and after (Figure 6C, red circle) gadolinium injection demonstrating a strong, smooth, and concentric vessel wall enhancement in left ICA.
Multicentric plasma cell variant of Castleman’s disease was diagnosed with biopsy of a cervical lymph node (Figure 6). Bone marrow biopsy in the back of the pelvic demonstrated slightly increased plasma cell (about 4% of marrow elements) with a small account of atypical cells which were positive for CD3, CD38, CD138, CD79a, CD43, Ki-67 and kappa light chain and negative for CD20 and CD56. But it failed to provide adequate evidence of a definitized myeloma.
We diagnosed her with POEMS syndrome, Castleman’s disease and ischemic stroke due to cerebral vasculitis. Since single antiplatelet therapy showed no effect on stopping ischemic recurrence in many previous reports, we changed the initial single antiplatelet therapy into dual antiplatelet therapy with aspirin (100 mg/day) and clopidogrel (75 mg/day) for 14 days, and then switched to aspirin 100 mg/day. After refusing autologous stem cell transplantation, the treatment with mecobalamin (1000 ug/day), dexamethasone (20 mg/day on day 1, 8, 15, and 22 of each 28-day cycle) and thalidomide (100 mg/day in first week, 150 mg/day in second week, then 200 mg/day) was started. The symptoms of dysarthria and right hemiparesis relieved after a week without any side effects of drugs. At a 6-month follow-up, we observed clinical improvement of numbness, weakness, edema and no recurrence of stroke with a reduced VEGF level (1324 pg/L).
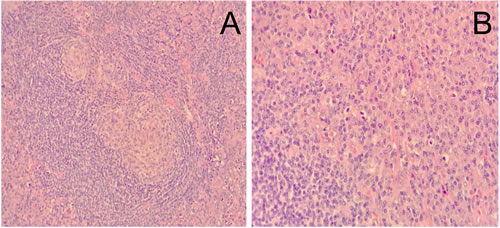
Figure 6: Histological examination of cervical lymph node revealed infiltration of plasma cells in the interfollicular area (original magnification A: ×200, B: ×400).
LITERATURE SEARCH
To retrieve all relevant studies on correlation between POEMS syndrome and ischemic stroke, we conducted a comprehensive search of Pubmed, Web of Science, EMBASE, China National Knowledge Infrastructure (CNKI), Wanfang Database and China Scientific Journal Database (VIP) using the terms “POEMS syndrome” (OR “Crow-Fukase syndrome”, “Takatsuki syndrome”) and “ischemic stroke” (OR “cerebral infarction”, “brain infarction”, “brain ischemia”, “transient ischemic attack”). The studies including case report and case series published from database inception to February 2017 were included without any language restriction. In addition, articles which didn’t have a decomposition of case series into a pattern in which cases could be analyzed individually were excluded, because we should obtain the clinical data such as age, gender, age of stroke onset, initial symptoms, time intervals between stroke onset and POEMS syndrome onset, the location of cerebral infarction, offending vessel, laboratory tests, MRI or CT image, angiography, biopsy, treatment and outcome data from each case. “Symptom improved” was used as good prognosis measure because it was the most common terms used by authors to describe the patient’s outcome, while “died” or “deterioration” was used as poor prognosis measure. Every literature was reviewed by two researchers independently.
RESULTS
To the best of our knowledge, 24 reports, including three small series and 21 single reports describing 28 cases of POEMS syndrome complicated with ischemic stroke, were identified after exclusion of the reports with incomplete data or duplicate data. All the available data were summarized in Table 2a-2d by reviewing the full texts of eligible reports. The comparison of clinical feature in the present study and two previous series was showed in Table 3.
Table 2a: Basic characteristics in patients with POEMS syndrome and ischemic stroke
Lesprit et al. 1996 [14] |
Hori et al. 1999 [38] |
Zhang et al. 2002 [39] |
Kang et al. 2003 [21] |
Erro et al. 2003 [20] |
|||
Age (years) |
53 |
51 |
44 |
42 |
48 |
52 |
65 |
Sex |
Female |
Female |
Male |
Male |
Female |
Female |
Female |
Initial symptoms |
Organomegaly |
Lymphadenopathy |
Skin changes |
N.A. |
N.A. |
Polyneuropathy |
N.A. |
POEMS to Stroke time |
24 months |
11 years |
12 months |
N.A. |
N.A. |
4 months |
29 months |
Symptoms of stroke |
Monocular blindness |
Aphasia and right hemiplegia |
Left hemiplegia |
Dysarthria Right arm monoparesis |
Weakness of all limbs |
Slurred speech |
Right monocular blindness |
Infraction territory |
Right ICA territory |
Left MCA territory |
Right MCA territory |
left MCA end BZI Left MCA/PCA BZI |
Bilateral end artery BZI Bilateral PCA territory |
Left MCA/PCA BZI |
Right ICA territory |
Cerebral vasculopathy |
Right ICA occlusion Left ICA stenosis |
Bilateral ICA occlusion |
Right MCA occlusion Diffuse vessels stenosis |
Inceased MFV of left ACA, MCA and right ICA |
Left MCA stenosis |
Left ICA stenosis |
Right ICA occlusion |
Vessels evaluation methods |
DSA |
DSA |
Ultrasonography |
TCD |
MRA |
MRA |
MRA |
Extracerebral vasculopathy |
SMA and left SA stenosis |
N.A. |
- |
Coronary artery |
Lower extremity artery |
N.A. |
Pulmonary artery |
Events (TIA, Stroke) |
1 |
1 |
1 |
1 |
1 |
1 |
2 |
Risk factors |
- |
Hypertension |
- |
Smoking |
- |
Hypertension |
- |
Relevant comorbidities |
- |
- |
- |
Myocardial infarction |
Left foot gangrene |
- |
Pulmonary embolism |
Medications before stroke |
- |
Cyclophosphamide and prednisone |
Dexamethasone |
Aspirin |
N.A. |
- |
Oral anticoagulation IVIg and prednisone |
Polyneuropathy |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
Monoclonal protein |
IgA-λ |
IgG-λ |
IgA-λ |
- |
+ |
+ |
IgG-λ |
Castleman disease |
Not performed |
+ |
Not performed |
Not performed |
+ |
Not performed |
Not performed |
Scleroticbone lesions |
+ |
- |
+ |
- |
- |
- |
- |
Organomegaly |
Hepatosplenomegaly Lymphadenopathy |
Hepatosplenomegaly Lymphadenopathy |
Hepatomegaly |
Hepatosplenomegaly Lymphadenopathy |
Hepatomegaly Lymphadenopathy |
- |
Splenomegaly |
Extravascular volume overload |
Pleural effussion Ascites Peripheral edema |
Peripheral edema |
Peripheral edema |
- |
Ascites |
Pericardial effusion |
- |
Endocrinopathy |
Glucose intolerance |
Hypothyroidism Amenorrhoea |
Gynaecomastia Hyperprolactinemia |
Hypothyroidism |
Hypothyroidism |
Hypothyroidism |
Hypothyroidism |
Skin changes |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
Papilledema |
- |
- |
- |
- |
- |
- |
- |
Thrombocytosis |
1000×109/L |
- |
612×109/L |
695×109/L |
- |
- |
560×109/L |
Hyperfibrinogenemia |
- |
- |
- |
6.03g/L |
5.94g/L |
3.61g/L |
- |
Antibodies |
- |
- |
- |
- |
- |
- |
- |
Other abnormalities |
Elevated IL-1B |
Mild anaemia Elevated CSF protein Elevated CSF pressure Elevated ESR Decreased Ccr |
Polycythemia Elevated CSF protein Weight loss (15kg in 12 months) |
Elevated CRP |
Elevated CRP |
Elevated CRP Pulmonary hypertension |
Elevated CSF protein Pulmonary hypertension |
Stroke treatment |
Aspirin and bypass graft |
Aspirin |
Aspirin |
N.A. |
N.A. |
N.A. |
Oral anticoagulation and aspirin |
POMES treatment |
Cyclophosphamide |
Melphalan and prednisolone |
Dexamethasone |
N.A. |
N.A. |
N.A. |
Azathioprine and prednisone |
Response to treatment |
Deteriorated |
Improved |
Deteriorated |
N.A. |
N.A. |
N.A. |
N.A. |
Survival time |
Died after 2 years |
N.A. |
Died 12 months later |
N.A. |
N.A. |
N.A. |
N.A. |
POEMS to Stroke time: Time from POEMS syndrome onset to stroke onset.
ICA: internal carotid artery. MCA: middle cerebral artery. ACA: anterior cerebral artery. PCA: posterior cerebral artery. BZI: border-zone infarction.
SA: subclavian artery. SMA: superior mesenteric artery.
DSA: digital subtraction angiography. MRA: magnetic resonance angiography. CTA: computed tomography angiography. TCD: transcranial doppler. MFV: mean flow velocity.
Ccr: endogenous creatinine clearance rate. IVIg: Intravenous immune globulin.
N.A.: not available.
Table 2b: Basic characteristics in patients with POEMS syndrome and ischemic stroke
Rolsser et al. 2004 [22] |
Wang et al. 2006 [30] |
Garcia et al. 2007 [13] |
Huang et al. 2007 [23] |
Lee et al. 2007 [14] |
Du et al. 2008 [31] |
||
Age (years) |
32 |
61 |
49 |
50 |
42 |
41 |
65 |
Sex |
Female |
Male |
Male |
Female |
Female |
Male |
Female |
Initial symptoms |
Edema in limbs |
Polyserositis |
Polyneuropathy |
N.A |
Diarrhea |
Polyneuropathy |
Skin changes |
POEMS to Stroke time |
6 months |
12 months |
24 months |
12 months |
5 months |
16 months |
24 months |
Symptoms of stroke |
Right hemiplegia |
Left hemiplegia |
Aphasia Right hemianesthesia |
Left hemianesthesia |
Left hemiplegia Coma |
Dysarthria Left hemiparesis |
Right hemiplegia |
Infraction territory |
Left basal ganglia |
Right MCA BZI |
Left MCA end artery |
Multiple bilateral infractions |
Rihgt ICA and Left ACA |
Right MCA territory |
Left MCA BZI |
Cerebral vasculopathy |
Left MCA occlusion Left ACA stenosis |
Normal |
Left MCA occlusion Right MCA and ACA stenosis |
Multiple bilateral arteries stenosis |
N.A. |
Bilateral MCA stenosis Right ICA stenosis |
Normal |
Vessels evaluation methods |
DSA |
Ultrasonography |
DSA |
DSA |
N.A. |
MRA |
Ultrasonography |
Extracerebral vasculopathy |
N.A. |
– |
N.A. |
Vegetation or thrombus in aortic outflow region |
N.A. |
SMA stenosis Left renal artery stenosis |
– |
Events (TIA, Stroke) |
10 TIAs, 2 infractions |
1 |
2 |
at least 3 |
1 |
1 |
1 |
Risk factors |
Hypertension |
– |
Hypertension Hyperlipidemia |
Hypertension Diabetes, smoking |
– |
– |
– |
Relevant comorbidities |
– |
– |
Ischemic stroke |
– |
– |
– |
– |
Medications before stroke |
Antihypertensive Levothyrocine |
Diuretic |
Aspirin |
Aspirin, prednisone and cyclophosphamide |
Antithyroid drugs |
Prednisolone |
Diuretic |
Polyneuropathy |
– |
– |
– |
– |
– |
– |
– |
Monoclonal protein |
IgA-λ |
IgG-λ |
IgA-λ |
IgG-λ |
IgA-κ |
IgA-λ |
λ-light chain |
Castleman disease |
– |
Not performed |
– |
– |
– |
– |
Not performed |
Scleroticbone lesions |
– |
– |
– |
– |
– |
– |
– |
Organomegaly |
Hepatosplenomegaly Lymphadenopathy |
Splenomegaly Lymphadenopathy |
Splenomegaly Lymphadenopathy |
Lymphadenopathy |
Hepatosplenomegaly Lymphadenopathy |
Hepatosplenomegaly Lymphadenopathy |
Splenomegaly Lymphadenopathy |
Extravascular volume overload |
Pericardial effusion Pleural effusion Peripheral edema |
Pericardial effusion Pleural effusion Ascites Peripheral edema |
Pericardial effusion Pleural effusion Ascites |
Peripheral edema |
Pericardial effusion Ascites Peripheral edema |
Ascites Peripheral edema Pericardial effusion |
Pericardial effusion Pleural effusion Ascites Peripheral edema |
Endocrinopathy |
Hypothyroidism |
Gynaecomastia Hyperprolactinemia |
Hypogonadism Hypothyroidism |
– |
Hyperthyroidism |
Hypogonadism Hypothyroidism |
– |
Skin changes |
– |
– |
– |
– |
– |
– |
– |
Papilledema |
– |
– |
– |
– |
– |
– |
+ |
Thrombocytosis |
– |
374×109/L |
– |
– |
– |
511×109/L |
– |
Hyperfibrinogenemia |
– |
– |
– |
– |
4.12g/L |
– |
– |
Antibodies |
– |
– |
ANA 1:160 peckled pattern |
ANA |
– |
– |
– |
Other abnormalities |
Hyperhomocystinemia Elevated CSF protein |
Elevated CSF Protein Positive CSF oligoclonal bands |
Elevated CRP and ESR Elevated CSF Protein Vitamin B12 deficiency Elevated VEGF and IL-6 Weight loss |
Pancytopenia Hypoalbuminemia Elevated triglycerides Elevated ESR, D-dimer |
Hypoalbuminemia Hyperglobulinemia Weight loss |
Elevated CRP and ESR Elevated serum creatine |
Positive CSF oligoclonal bands |
Stroke treatment |
First heparin Then clopidogrel and phenprocoumon |
Aspirin |
Aspirin |
Aspirin then clopidogrel |
N.A. |
Anticoagulants (not specified) |
Defibrase,then ozagrel, then aspirin |
POMES treatment |
First prednisone and chlorambucil, then VAD, then cyclophosphamide |
Prednisone |
First corticosteroids and rituximab, then dexamethasone and cyclophosphamide |
First Prednisone and cyclophosphamide, then rituximab and methylprednisolone |
Dexamethasone |
Prednisone and melphalan |
Prednisone |
Response to treatment |
Improved after cyclophosphamide |
Deteriorated |
Improved |
Deteriorated |
Improved |
Deteriorated |
Deteriorated |
Survival time |
At least 2 years |
Died 6 months later |
N.A. |
N.A. “gradual |
N.A. |
Died 4 weeks later |
Died 6 months later |
POEMS to Stroke time: Time from POEMS onset to stroke onset.
ICA: internal carotid artery. MCA: middle cerebral artery. ACA: anterior cerebral artery. PCA: posterior cerebral artery. SMA: superior mesenteric artery.
BZI: border-zone infarction. DSA: digital subtraction angiography. MRA: magnetic resonance angiography. TCD: transcranial doppler.
ANA: antinuclear antibody.
VAD: vincristin + doxorubicin + dexamethasone. IVIg: Intravenous immune globulin.
N.A.: not available.
Table 2c: Basic characteristics in patients with POEMS syndrome and ischemic stroke
Zheng et al. 2008 [32] |
Shi et al. 2010 [33] |
Jing et al. 2011 [34] |
Sommer et al. 2012 [24] |
Dacci et al. 2013 [25] |
Akyol et al. 2014 [15] |
||
Age (years) |
52 |
58 |
40 |
54 |
49 |
46 |
47 |
Sex |
Male |
Male |
Male |
Female |
Male |
Male |
Female |
Initial symptoms |
Impotence |
Polyserositis |
Skin changes |
Polyneuropathy |
Ischemic stroke |
Ischemic stroke |
Polyneuropathy |
POEMS to Stroke time |
3 years |
60 months |
More than 2 years |
2 months |
12 months preceded POEMS onset |
1 month preceded POEMS onset |
2.5 months |
Symptoms of stroke |
Left upper limb palsy |
Vertigo Left hemiplegia |
Right hemiplegia |
Right hemiparesis Global aphasia |
Aphasia Right hemiparesis |
Left facio-brachial palsy |
Dysarthria Right-sided hemiparesis |
Infraction territory |
Right MCA territory |
Right MCA territory |
Multiple bilateral infractions |
Left MCA and left MCA-ACA BZI |
Left MCA BZI |
Right PCA BZI |
Bilateral parietal lobes |
Cerebral vasculopathy |
Bilateral carotid atherosclerosis |
Normal |
Left MCA occlusion |
– |
– |
N.A. |
Left ICA stenosisBilateral MCA occlusion |
Vessels evaluation methods |
MRA |
Ultrasonography |
DSA |
Ultrasonography |
Ultrasonography |
N.A. |
MRA |
Extracerebral vasculopathy |
– |
– |
– |
Coronary artery |
N.A. |
N.A. |
Pulmonary artery |
Events (TIA,Stroke) |
1 |
1 |
10 |
2 |
1 |
2 |
4-5 times per day |
Risk factors |
– |
– |
– |
Hypertension, diabetes |
Smoking |
– |
Hypertension, diabetes,hyperlipidemia |
Relevant comorbidities |
– |
– |
– |
Myocardial infarction |
PFO (underwent closure) |
– |
Hashimoto thyroiditis Pulmonary embolism |
Medications before stroke |
Prednisolone |
Melphalan and prednisolone |
Aspirin |
Aspirin |
N.A. |
N.A. |
Warfarin, aspirin, atorvastatin, gliclazide |
Polyneuropathy |
– |
– |
– |
– |
– |
– |
– |
Monoclonal protein |
– |
IgA-λ |
IgG-κ |
IgG-λ |
IgA-λ |
IgG-λ |
– |
Castleman disease |
Not performed |
Not performed |
– |
Not performed |
Not performed |
Not performed |
Not performed |
Scleroticbone lesions |
– |
– |
– |
– |
– |
– |
– |
Organomegaly |
Hepatosplenomegaly |
Splenomegaly |
Lymphadenopathy |
Hepatosplenomegaly |
Hepatosplenomegaly |
Splenomegaly |
Hepatosplenomegaly |
Extravascular volume overload |
Pleural effusionPeripheral edema |
Pericardial effusion Pleural effusion Peripheral edema |
Pleural effusion Peripheral edema |
Pleural effusion |
– |
Pleural effusion |
Pericardial effusion Peripheral edema |
Endocrinopathy |
Hypothyroidism Gynaecomastia Low testosterone Hyperprolactinemia |
Hyperprolactinemia Low testosterone Hypercortisolism |
Impotence |
Hypothyroidism |
– |
– |
Subclinical hypothyroidism |
Skin changes |
– |
– |
– |
– |
– |
– |
– |
Papilledema |
– |
– |
– |
– |
– |
– |
– |
Thrombocytosis |
386×109/L |
– |
– |
– |
511x×109/L |
483×109/L |
687×109/L |
Hyperfibrinogenemia |
– |
– |
6.32g/L |
– |
– |
– |
4.18g/L |
Antibodies |
– |
– |
– |
– |
– |
– |
– |
Other abnormalities |
Elevated CSF protein Elevated CSF pressure Glucose intolerance |
Hyperglobulinemia Hypoalbuminemia Microalbuminuria |
Polycythemia Hyperglobulinemia Albuminuria |
Weight loss (10kg) |
Hyperhomocystinemia Elevated CSF protein |
Elevated serum VEGF Elevated CSF protein Elevated CRP andESR |
Orthostatic hypotension Elevated CSF protein Pulmonary hypertension Severe tricuspid regurgitation |
Stroke treatment |
Aspirin |
N.A. |
Aspirin |
Aspirin and clopidogrel |
Aspirin |
Aspirin |
Warfarin, aspirin, atorvastatin |
POMES treatment |
First prednisone, then prednisone and azathioprine |
Melphalan and prednisone |
Corticosteroids |
Prednisone and radiotherapy |
Prednisone and IVIg,then ASCT |
First PE and IVIg,then Rev/Dex, then ASCT |
Melphalan and prednisone, then cyclophosphamide |
Response to treatment |
Deteriorated |
Improved |
Improved |
Deteriorated |
Improved |
Improved |
Deteriorated |
Survival time |
Died 1 year later |
N.A. |
N.A. |
Die 1 day later |
at least 12 months |
at least 6 months |
Sudden cardiac death after two cycles treatment |
POEMS to Stroke time: Time from POEMS onset to stroke onset.
ICA: internal carotid artery. MCA: middle cerebral artery. ACA: anterior cerebral artery. PCA: posterior cerebral artery. BZI: border-zone infarction.
DSA: digital subtraction angiography. MRA: magnetic resonance angiography.
IVIg: Intravenous immune globulin. ASCT: autologous stem cell transplant. PE:plasma-exchange. Rev/Dex: lenalidomide and dexamethasone.
N.A.: not available.
Table 2d: Basic characteristics in patients with POEMS syndrome and ischemic stroke
Yu et al. 2015 [26] |
Sun et al. 2015 [36] |
Han et al. 2016 [27] |
Rajan et al. 2016 [16] |
Yagihi et al. 2016 [28] |
Liu et al. 2016 [37] |
Wang et al. 2016 [29] |
|
Age |
24 |
46 |
33 |
36 |
32 |
37 |
68 |
Sex |
Male |
Female |
Male |
Female |
Male |
Male |
Male |
Initial symptoms |
Fever and polyserositis |
Polyneuropathy |
Skin changes and impotence |
Polyneuropathy |
Headaches |
Polyneuropathy |
Ischemic stroke |
POEMS to Stroke time |
2 months |
9 months |
12 months |
3 months |
11 months preceded POEMS onset |
35 months |
1 month preceded POEMS onset |
Symptoms of stroke |
Numbness of the upper extremities Blurred vision |
Acute cognitive impairment |
Intermittent amaurosis of left eye |
Aphasia Left facial palsy |
Right monocular blindness |
Left monocular blindness Right side hemiparesis |
Right hemiparesis |
Infraction territory |
First left ventricle,then right ventricle |
Bilateral end artery BZI |
Left ICA territory |
Left MCA end artery and BZI |
RightMCA internal BZI Ophthalmic artery |
Left MCA BZI and ophthalmic artery |
Left MCA-ACA BZI |
Cerebral vasculopathy |
N.A. |
Right ICA occlusion Left ACA stenosis Right ICA stenosis |
Left ICA occlussion |
Bilateral ICA stenosis Left PCA occlusion |
Right ICA occlusion |
Left ICA stenosis |
Normal |
Vessels evaluation methods |
N.A. |
MRA |
CTA |
MRA |
DSA |
MRA |
CTA |
Extracerebral vasculopathy |
– |
– |
– |
– |
Splenic artery |
– |
– |
Events (TIA, Stroke) |
At least 4 times |
1 |
1 |
1 |
More than 4 times |
1 |
3 |
Risk factors |
– |
– |
– |
– |
Smoking |
– |
– |
Relevant comorbidities |
– |
– |
– |
– |
– |
– |
– |
Medications before stroke |
Antitubercular agents |
Corticosteroids |
– |
– |
– |
Radiotherapy |
Aspirin and atorvastatin |
Polyneuropathy |
– |
– |
– |
– |
– |
– |
– |
Monoclonal protein |
– |
IgG-λ |
λ-light chain |
IgA-λ |
IgA-λ |
IgG-λ |
IgA-λ |
Castleman disease |
– |
Not performed |
– |
Not performed |
– |
Not performed |
Not performed |
Scleroticbone lesions |
– |
– |
– |
– |
– |
– |
– |
Organomegaly |
Lymphadenopathy |
Splenomegaly Lymphadenopathy |
Splenomegaly Lymphadenopathy |
Hepatosplenomegaly |
Hepatosplenomegaly Lymphadenopathy |
– |
Splenomegaly Lymphadenopathy |
Extravascular volume overload |
Pericardial effusion Pleural effusion Peripheral edema |
Pleural effussion |
– |
Ascites Peripheral edema |
Ascites Peripheral edema Pericardial effusion |
Pericardial effusion Peripheral edema |
Peripheral edema |
Endocrinopathy |
Hypothyroidism Gynecomastia Hypotestosterone Hyperprolactinemia |
Hypothyroidism |
Hypothyroidism Hyperprolactinemia |
– |
Hypothyroidism Hypogonadism Low testosterone |
Gynaecomastia Impotence Hyperprolactinemia |
Hypothyroidism Low testosterone Hyperprolactinemia |
Skin changes |
– |
+ |
– |
– |
– |
+ |
– |
Papilledema |
– |
– |
– |
– |
– |
– |
– |
Thrombocytosis |
565×109/L |
427×109/L |
329×109/L |
697×109/L |
700×109/L |
379×109/L |
452×109/L |
Hyperfibrinogenemia |
– |
– |
– |
– |
– |
– |
– |
Antibodies |
– |
– |
– |
– |
– |
– |
– |
Other abnormalities |
Elevated serum creatine Elevated CSF protein Elevated CSF pressure Weight loss (15kg in 60 days) |
Elevated CRP and ESR Elevated serum VEGF Elevated CSF Protein Weight loss (3kg in 1 month) |
Polycythemia Hyperuricemia Dyslipidemia Hyperphosphatemia Microalbuminuria |
Polycythemia Elevated CSF protein |
Elevated CRP and ESR Elevated serum VEGF Elevated CSF Protein Proteinuria Weight loss |
PolycythemiaLeukocytosis Elevated CRP Elevated CSF Protein |
Elevated serum VEGF Elevated ESR Weight loss (3kg in 2 months) |
Stroke treatment |
N.A. |
Aspirin |
Low molecular heparin |
Antiplatelet drug |
Aspirin and verapamil |
Aspirin |
Aspirin, clopidogrel atorvastatin |
POMES treatment |
Lenalidomideand dexamethasone |
Lenalidomide and dexamethasone |
Dexamethasone and melphalan |
Thalidomide and dexamethasone |
Methylprednisolone,then prednisone,then prednisone and cyclophosphamide |
First melphalan-based chemotherapy,then ASCT |
Melphalan and prednisone |
Response to treatment |
Deteriorated |
Improved |
N.A. |
N.A. |
Deteriorated |
Improved |
Improved |
Survival time |
Died two weeks later |
At least 12 months |
At least 6 months |
N.A. |
Died 2 years later |
At least 12 months |
At least 24 months |
POEMS to Stroke time: Time from POEMS onset to stroke onset.
ICA: internal carotid artery. MCA: middle cerebral artery. ACA: anterior cerebral artery. PCA: posterior cerebral artery. BZI: border-zone infarction.
DSA: digital subtraction angiography. MRA: magnetic resonance angiography. CTA: computed tomography angiography.
ASCT: autologous stem cell transplant.
N.A.: not available.
Table 3: Comparison of clinical feature in the present study and two previous series
Characteristics |
Present study N = 28 |
Li [18] N = 99 |
Dispenzieri [41] N = 99 |
Age (median, years) |
47 |
45 |
51 |
Male sex |
14 (50%) |
58 (58%) |
62 (62%) |
Initial symptoms |
|||
Polyneuropathy |
8 (33%) |
41 (41%) |
N.A. |
Peripheral edema |
1 (4%) |
27 (27%) |
N.A. |
Skin changes |
4 (19%) |
15 (15%) |
N.A. |
Serositis |
3 (14%) |
4 (4%) |
N.A. |
Organomegaly |
2 (10%) |
3 (3%) |
N.A. |
Ischemic stroke |
4 (19%) |
0 (0%) |
N.A. |
Polyneuropathy |
28 (100%) |
98 (99%) |
99 (100%) |
Elevated CSF protein |
15 (94%) |
69 (96%) |
99 (100%) |
Organomegaly |
26 (93%) |
85 (86%) |
N.A. |
Hepatomegaly |
14 (50%) |
47 (47%) |
24 (24%) |
Splenomegaly |
21 (75%) |
70 (71%) |
22 (22%) |
Lymphadenopathy |
17 (61%) |
74 (75%) |
26 (26%) |
Castleman’s Disease |
7 (64%) |
25 (58%) |
11 (73%) |
Endocrinopathy |
23 (82%) |
N.A. |
73 (74%) |
Thyroid dysfunction |
16 (57%) |
66 (66%) |
26 (26%) |
Impaired glucose metabolism |
3 (11%) |
21 (21%) |
3 (3%) |
Monoclonal plasma cell dyscrasia |
25 (89%) |
99 (100%) |
99 (100%) |
IgA-λ |
10 (40%) |
65 (71%) |
44 (52%) |
IgG-λ |
8 (32%) |
20 (22%) |
40 (48%) |
IgM-λ |
0 (0%) |
0 (0%) |
1 (1%) |
λ |
2 (8%) |
4 (4%) |
0 (0%) |
IgG-κ |
1 (4%) |
2 (2%) |
0 (0%) |
IgA-κ |
1 (4%) |
1 (1%) |
0 (0%) |
Skin changes |
26 (93%) |
89 (90%) |
67 (68%) |
Papilledema |
7 (25%) |
56 (64%) |
29 (29%) |
Extravascular volume overload |
24 (86%) |
87 (88%) |
29 (29%) |
Peripheral edema |
18 (64%) |
84 (85%) |
24 (24%) |
Pleural effusion |
12 (43%) |
43 (43%) |
3 (3%) |
Pericardial effusion |
12 (43%) |
64 (65%) |
1 (1%) |
Ascites |
9 (32%) |
54 (55%) |
7 (7%) |
Sclerotic bone lesions |
12 (43%) |
19 (19%) |
46 (46%) |
Other features |
|||
Thrombocytosis |
17 (61%) |
54 (55%) |
53 (54%) |
Polycythemia |
5 (18%) |
9 (9%) |
18 (18%) |
Hyperfibrinogenemia |
6 (21%) |
N.A. |
N.A. |
Pulmonary hypertension |
3 (11%) |
36 (36%) |
5 (5%) |
Renal impairment |
3 (11%) |
37 (37%) |
4 (4%) |
Elevated VEGF |
5 (100%) |
28(70%) |
N.A. |
Surival rate |
8a (44%) |
86b (83%) |
64c (75%) |
Values are given as number (percent), unless otherwise indicated. The percentages for subcategories are demonstrated as the percentage of patients with the abnormality among those patients who finished the test .
N.A.: not available.
a longest follow-up time of 2 years b median follow-up time of 26 months
c median follow-up time of 70.6 months
GENERAL CHARACTERISTICS
There were 14 males and 14 females, and the male to female ratio was 1:1. The age of ischemic stroke onset ranged from 24 to 68 years (median age=47 years) without a significant difference between male and female (p=0.303). The median time interval between stroke onset and POEMS syndrome onset was six months. The time interval ranged from 12 months preceded the onset of POEMS syndrome to 11 years after the onset of POEMS syndrome. There were no relevant data in two cases. The data of initial symptom was not documented in 4 cases. The most common initial symptom was polyneuropathy (8, 33.3%). Other initial symptoms included ischemic stroke (4, 16.7%), skin changes (4, 16.7%), polyserositis (3, 12.5%), organomegaly (2, 8.3%), impotence (1, 4.2%), diarrhea (1, 4.2%) and headache (1, 4.2%). Most patients (18, 64.3%) had no risk factors of stroke. Meanwhile, twenty-one patients (75.0%) had not any relevant comorbidities of stroke, only a small proportion of patients complained of hypertension (7, 25.0%), smoking (4, 14.3%), diabetes mellitus (3, 10.7%), hyperlipidemia (2, 7.1%), pulmonary embolism (2, 7.1%), myocardial infarction (1, 3.6%), foot gangrene (1, 3.6%), patent foramen ovale (1, 3.6%), Hashimoto’s thyroiditis (1, 3.6%), and previous ischemic stroke (1, 3.6%). Medications before stroke onset which might influence on the risk of ischemic stroke included aspirin (7, 25.0%), glucocorticoids (8, 28.6%) and oral anticoagulants (2, 7.1%).
POEMS FEATURES
All the patients had slight to severe symptoms and signs of polyneuropathy. In the 16 patients who were reported to receive lumber puncture, 15 patients (93.8%) had elevated cerebrospinal fluid protein levels. Increasing cerebrospinal fluid opening pressure was observed in 4 patients (25.0%). Abnormal white cell count was not observed in any patient. In addition, oligoclonal bands were positive in 3 patients (15.0%).
Twenty-six patients (92.9%) had organomegaly, in which 14 patients (50.0%) had hepatomegaly, 21 (75.0%) had splenomegaly, and 17 patients (60.7%) had lymphadenopathy. Seven patients (25.0%) had both hepatosplenomegaly and lymphadenopathy. Eleven of these patients underwent lymph node biopsy, four patients (36.4%) of them had normal manifestation and 7 patients (63.6%) had Castleman’s disease.
Skin manifestations were observed in 26 patients (92.9%). Hyperpigmentation was the most common manifestation occurring in 23 patients (82.1%), which was followed by skin thickening (8, 28.6%) and hypertrichosis (3, 10.7%). Raynaud’s phenomenon occurred in 3 patients (10.7%). In our study, twenty-three patients (82.1%) had at least one recognized endocrinopathy, with thyroid dysfunction (17, 60.7%) as the most common abnormality. Among the patients with thyroid dysfunction, 14 patients (82.3%) needed replacement treatment with high TSH and low serum thyroxine, 2 patients (11.8%) presented with subclinical hypothyroidism while one patient (5.9%) had hyperthyroidism. Hypogonadism (14, 50.0%) was also a common endocrinopathy in patients of POEMS complicated with ischemic stroke. However, only three patients (10.7%) had impaired glucose metabolism.
The evidence of monoclonal plasma proliferative disorder was found in 25 patients (89.3%). The types of monoclonal protein in these patients consisted of IgA-λ (10, 40.0%), IgG-λ (8, 32.0%), λ-light chain alone (2, 8.0%), IgA-κ (1, 4.0%), and IgG-κ (1, 4.0%). The type of monoclonal protein was not reported in 3 patients. Bone marrow aspiration and biopsy were undertaken in a half of patients (50%). Only one patient had >10% plasma cell.
A variety of patterns of extravascular volume overload was reported in 24 patients (85.7%). Peripheral edema (18, 64.3%) was the most common manifestation in our cases, but pleural effusion (12, 42.9%), pericardial effusion (12, 42.9%) and ascites (9, 32.1%) were also common. In addition, polyserositis was observed in 10 patients (35.7%). Osteosclerotic lesions was documented in 12 patients (42.9%). Papilledema was observed in 7 patients (25%). Eight patients suffered from weight loss and three patients had pulmonary hypertension.
LABORATORY FEATURES
Thrombocytosis was a very common manifestation in POEMS patients with ischemic stroke. It was found in 17 patients (60.7%). The abnormal platelet count varied from 329×109/L to 1000×109/L. Polycythemia (5, 17.8%) was more common than anemia (2, 7.1%). Hyperfibrinogenemia was documented in 6 patients (18.5%) while elevated CRP levels in 9 patients (33.3%), elevated ESR in 8 patients (28.3%), hypoalbuminemia in 3 patients (10.7%), renal impairment in 3 patients (10.7%), hyperglobulinemia in 3 patients (10.7%), proteinuria in 3 patients (10.7%) and hyperlipidemia in 2 patients (7.1%). In the five patients who performed the measure of the serum VEGF level, all of them had elevated serum VEGF level. In addition, hyperhomocysteinemia was observed in 2 patients (7.1%). Only two patients had autoantibody abnormality, all of them were antinuclear antibody.
ISCHEMIC STROKE FEATURES
Eleven patients (39.3%) experienced more than one event of ischemic stroke. The highest frequency of ischemic attack was more than 4-5 times per day. In our study cohort, multiple ischemic lesions (20, 71.5%) were much more common than single ischemic lesion (8, 28.5%). Evaluation of cerebral arteries was performed by magnetic resonance angiography (9, 36.0%), digital subtraction angiography (7, 25.0%), ultrasonograph (7, 25.0%) and CT angiography (2, 8.0%) in 25 patients. Nineteen patients (76.0%) were found with cerebral vasculopathy while 12 patients (48.0%) had more than one artery involved. It was noteworthy that mismatch between the infarct area and recognized vasculopathy was observed in 8 patients (28.6%). In addition, extracerebral vasculopathy was found in 9 patients (32.1%).
TREATMENT AND OUTCOME
Data of treatment was available in 25 patients (88.9%) of all the patients. Among them, five patients underwent POEMS therapy with melphalan-based chemotherapy, five patients with prednisone or dexamethasone alone, three patients with chemotherapy and autologous stem cell transplantation, two patients with lenalidomide and dexamethasone, one patient with thalidomide and dexamethasone, one patient with cyclophosphamide, one patient with prednisone and percutaneous radiotherapy. Eight patients underwent subsequent treatment due to the poor response to the initial treatment. Data of stroke therapy was available in 22 patients. Among them, 13 patients were treated with single antiplatelet drug (11 cases with aspirin, 1 case with a sequential treatments of aspirin and clopidogrel, 1 case without detail in the report), 2 patients with aspirin and clopidogrel, 2 patients with antiplatelet and anticoagulation therapy (2 cases with aspirin and oral anticoagulation, 1 case with clopidogrel and phenprocoumon) , 2 patients with anticoagulation therapy, 1 patient with a sequential treatment of defibrase, ozagrel and aspirin, 1 patient with aspirin and bypass surgery. Ischemic events were documented in 8 patients even when they were undergoing all the therapy for ischemic stroke, but in 3 cases of them, ischemic attack stopped after the combined treatment for ischemic stroke and POEMS syndrome. Survival data was available in 18 patients with a longest follow-up time of 2 years, ten patients died in total. The comparison of the baseline characteristics of patients with and without fatal outcome was showed in Table 4. Due to the rare occurrence of ischemic stroke in patients with POEMS syndrome, the sample size was too small to establish any meaningful difference of clinical features between patients with and without fatal outcome. Patients with fatal outcome were older, and more likely to have multiple cerebral vasculopathies, extracerebral pathology, hepatomegaly, hepatosplenomegaly, papilledema, polyendocrinopathy, and extravascular volume overload. Moreover, very few patients in survived group had extracerebral pathology, hepatomegaly hepatosplenomegaly, papilledema, pericardial effusion, ascites and polyserositis.
Table 4: Comparison of clinical features in the patients with and without fatal outcome
Characteristics |
Death (N= 10) |
Survived (N= 8) |
Age ( median, years) |
52 |
46 |
Male |
6 (60.0%) |
5 (62.5%) |
Multiple ischemic lesions |
8 (80.0%) |
6 (75%) |
Cerebral vasculopathy |
6 (66.7%) |
4 (57.1%) |
Multiple cerebral vasculopathies |
5 (55.6%) |
2 (28.6%) |
Recurrent stroke |
4 (40.0%) |
3 (37.5%) |
Extracerebral pathology |
5 (50.0%) |
1 (12.5%) |
Polyneuropathy |
10 (100%) |
8 (100%) |
Elevated CSF protein |
6 (60.0%) |
4 (50.0%) |
Organomegaly |
10 (100%) |
7 (87.5%) |
Hepatomegaly |
7 (70.0%) |
1 (12.5%) |
Splenomegaly |
8 (80.0%) |
5 (62.5%) |
Lymphadenopathy |
6 (60.0%) |
4 (50.0%) |
Hepatosplenomegaly |
6 (60.0%) |
1 (12.5%) |
Endocrinopathy |
9 (90.0%) |
5 (62.5%) |
Thyroid dysfunction |
6 (60.0%) |
4 (50.0%) |
Polyendocrinopathy |
6 (60.0%) |
3 (37.5%) |
Skin changes |
9 (90.0%) |
6 (75.0%) |
Papilledema |
6 (60.0%) |
0 (0%) |
Extravascular volume overload |
10 (100%) |
5 (62.5%) |
Peripheral edema |
9 (90.0%) |
3 (37.5%) |
Pleural effusion |
6 (60.0%) |
2 (25.0%) |
Pericardial effusion |
6 (60.0%) |
1 (12.5%) |
Ascites |
5 (50.0%) |
0 (0%) |
Polyserositis |
6 (60.0%) |
0 (0%) |
Sclerotic bone lesions |
7 (70.0%) |
4 (50.0%) |
Thrombocytosis |
9 (90.0%) |
6 (75.0%) |
Hyperfibrinogenemia |
1 (10.0%) |
0 (0%) |
Values are given as number (percent), unless otherwise indicated. The percentages for subcategories are demonstrated as the percentage of patients with the abnormality among those patients who finished the test.
DISCUSSION
POEMS syndrome is a rare multi-systemic paraneoplastic disease resulting from an underlying clonal plasma cell disorder, which is characterized by the acronym: polyneuropathy, organomegaly, endocrinopathy, mono-clonal plasma cell disorder, and skin changes [2]. It’s also well known to be associated with a myriad of clinical presentations including Castleman’s disease, sclerotic bone lesions, pulmonary manifestations, clubbing, weight loss, thrombocytosis, polycythemia, extravascular volume overload and elevated VEGF levels [1]. The pathophysiologic correlates between the myriad of symptoms and the underlying disease have not yet been fully understood, but the correlation has been postulated that cytokines or proangiogenic factors play a pivotal role as mediators [7-9, 17]. Due to its complicated manifestations and atypical initial presentations of POEMS syndrome, misdiagnosis is very common and extensive [18], which is sometimes a major challenge for physicians. Besides the manifestations commonly seen in this syndrome, arterial or venous thrombosis is attracting increasing attention as a less-recognized feature which is suggested to be a predictor of poor prognosis [8, 10, 11, 14]. So far, several cases of ischemic stroke in patients with POEMS syndrome have been reported in the literature [8, 10, 12-15, 19-39].
Our patient was a 65-year-old female. She presented polyneuropathy, monoclonal protein, splenomegaly, lymphadenopathy, hypothyroidism, extravascular volume overload (peripheral edema, pericardial effusion, pleural effusion and ascites) and skin changes. She also showed Castleman disease, papilledema, elevated serum VEGF and weight loss. According to the diagnosis criteria recommended by Dispenzieri [1], this patient fulfilled two mandatory major criteria, two other major criteria and six minor criteria. The diagnosis was established after excluding other differential diagnoses. In spite of the absence of traditional and modifiable atherosclerosis risk factors such as diabetes, hypertension, hypercholesteremia or smoking, our patient still developed multiple cerebral infarctions under an adequate secondary stroke prevention therapy including aspirin and atorvastatin. Images of CT angiography showed a diffuse stenosis in the large vessels from the origin of left ICA to the M1 segment of the left MCA which is not likely the result of atherosclerosis but a result of POEMS syndrome. The etiological detection for ischemic stroke (complete blood count, coagulation markers, blood chemistry, serum tumor marks, antiphospholipid antibody, autoimmune antibodies and screen for vasculitis) was unremarkable except for anemia, thrombocytosis, hyperhomocysteinemia and hyperfibrinogenemia. It’s noteworthy that thrombocytosis and bone marrow plasmacytosis lead to an increased risk of ischemic stroke in Dupont’s study [12]. Thrombocytosis is a well recognized etiologic factor of arterial thrombosis with proposed mechanisms including increased blood viscosity and pre-thromboticstate [10, 40]. However, in our study, there are 11 patients (39.3%) with normal platelet counts. Meanwhile, the incidence of thrombocytosis in our cohort consist of POEMS patients with ischemic stroke is very similar to the two large series studies of POEMS performed by Dispenzieri [41] and Li [18] respectively. Most patients in our study just presented mild or moderate thrombocytosis. Only one patient had a platelet count more than 1000×109/L. In contrast, most studies agreed that platelet count apparently did not correlate with the risk of thrombosis in patients with essential thrombocythemia except the patients with the basis of age above 60 years, cardiovascular risk factors, thrombosis history and the presence of JAK-2 mutation [42, 43]. Even a very high platelet count is associated with a high risk of bleeding but not thrombosis [43]. Also, it is very rare that myeloproliferative and plasma cell proliferation develop in the same patient. It’s postulated that abnormal cytokine hyperproduction such as interleukin-6 (IL-6) and interleukin-1 (IL-1) may be responsible for the muti-systematic manifestations including thrombocytosis and Castleman’s disease [44]. In addition, the recurrence of ischemic stroke was observed in 8 patients even under sufficient oral antiplatelet therapy, which indicated a complex association between POEMS syndrome and ischemic stroke.
Recently, fibrinogen is emerging as an independent risk factor for cardiovascular diseases and peripheral vascular diseases. However, still few studies are available to regard the role of fibrinogen in the pathogenesis of ischemic stroke. Previous studies have shown conflicting results as to whether fibrinogen is a predictor for risk of ischemic stroke [45, 46]. Kang and colleagues found all of their three cases had elevated fibrinogen levels [21]. The phenomenon was also observed in a patient with a large area of cerebral infarction and Castleman’s disease reported by Huang et al [23]. They suggested IL-6 inducing hyperfibrinogenemia might act a pivotal part as a trigger of procoagulatory in the development of stroke in patients with POEMS syndrome [15, 21, 23, 34]. Fibrinogen is a predictor of wide-spread inflammation process and also frequently elevated before the cerebrovascular events in the patients without a history of POEMS, because cytokines such as IL-1, IL-6 and tumor necrosis factor which were demonstrated to be elevated in patients with POEMS syndrome, can also be produced by atherosclerosis macrophages [47, 48, 49]. Moreover, hyperfibrinogenemia is not observed in all patients with elevated cytokine levels. In addition, there were only six patients (21.2%) had elevated fibrinogen levels in our review. From the standpoint of available evidence, the hypothesis of the pivotal role of fibrinogen in the etiologic link between the two disorders is less plausible.
On the other hand, hyperhomocysteinemia was observed in our case and two patients (7.1%) in our review, which may be a critical but often-neglected component of POEMS. Numerous studies have demonstrated that hyperhomocysteinemia is a strong and independent risk factor for ischemic stroke [49, 50]. It is now well recognized that vitamin B12 supplement therapy can reduce homocysteine levels, which will lead to a reduced risk of ischemic stroke [50]. Recently, vitamin B12 deficiency unresponsive to replacement therapy has been recognized as a less common manifestation of POEMS [3, 4]. Although our patient received a sufficient treatment of oral mecobalamin 500ug three times a day, we still detected a low vitamin B12 value and hyperhomocysteinemia without the presence of intrinsic factor antibodies. The pathophysiological mechanisms under vitamin B12 deficiency and hyperhomocysteinemia in POEMS syndrome worth exploring. This phenomenon may be caused by the abnormal uptake in gastric mucosa which may suffer from microangiopathy and vasopermeability induced by VEGF.
Vessel endothelial cell is an important target of cytokines and M protein [8, 10, 17, 51, 52]. It’s noteworthy that large artery occlusive disease in our study is much more common than that reported in stroke registry studies [53, 54, 55]. However, the frequencies of stroke risk factors such as diabetes mellitus, hypertension and atrial fibrillation occurred in our study are similar to or even lower than those in stroke registries [54, 55]. In accordance with previous literature, the preponderance of multiple cerebral vessel lesions and coexistence of extracerebral vessel disease in patients of POEMS without stroke risk factors are also more common than those reported in stroke registries [13-14, 22-24, 27-28, 38]. This phenomenon may suggest that POEMS syndrome has a predisposition towards large-vessel vasculopathy which could only be confirmed by biopsy. To the best of our knowledge, pathologically confirmed cerebral vasculopathy has not been reported yet. Conventional angiographic findings of cerebral vasculopathy are nonspecific and can’t reliably distinguish vasculopathy from atherosclerosis [56]. Magnetic resonance vessel-wall imaging is the most promising technique for differentiating between vasculopathy and atherosclerotic disease [56]. Our patient showed a thickening and enhancement of the vessel wall of the left ICA, indicative of vasculitis. In the previous studies, a noninflammatory vasculopathy, which is speculated to be the pathogeny of stroke according to the benign cerebrospinal fluid manifestation in patients [12, 28], might be due to proangiogenic factors including VEGF. However, the hypothesis is challenged in the absence of pathological evidence [12, 28]. There is growing evidence that endothelial dysfunction plays an important role in the pathogenesis of POEMS syndrome. Moreover, pathologically confirmed vasculitis involving small-sized and medium-sized muscular artery are reported to be directly associated with POEMS syndrome [57, 58]. In addition, larger-sized vessels are also suspected to be affected in POEMS syndrome [8, 10, 22, 59]. Co-existing quasi-moyamoya disease and POEMS syndrome were observed in a patient with sudden-onset intracranial hemorrhage [60]. Progressive intracranial large-vessel vasculopathy has been reported as the initial presenting manifestation of POEMS [28].
The precise pathophysiological mechanism of the development of cerebral vasculopathy remains unknown. An correlation with cerebral vasculopathy and Castleman’s disease in patients with POEMS syndrome was reported in several studies. Castleman’s disease is one of the major criteria for the diagnosis of POEMS syndrome [1]. An association with Castleman’s disease was reported in nearly half of patients with POEMS syndrome. However, the pathogenesis of Castleman’s disease remains unclear. A complex cytokine and chemokine network, including VEGF, IL-6, and IL-1, may play an important role in the development of Castleman’s disease [61]. Also, the network may induce a systemic inflammatory condition which may lead to cerebral vasculopathy and ischemic stroke [62]. Ischemic stroke is the most common manifestation of cerebrovascular involvements of Castleman’s disease. Seven patients were found with Castleman’s disease and ischemic stroke in our study. In the five patients who had undergone an evaluation of cerebral vessels, all of them were found with cerebral vascopathy. It indicated that there was a strong association between cerebral vasculopathy and Castleman’s disease. Hori et al. [38] described a patient with Castleman’s disease and POEMS syndrome who presented hypertrophic cranial pachymeningitis and bilateral internal carotid artery occlusion due to suspected vasculitis. Rössler and colleague [22] reported a patient with Castleman’s disease and POEMS syndrome who presented recurrent ischemic stroke secondary to clinical diagnosed cerebral vasculitis. Garcia et al. [13] described two patients with diffuse stenosis of the intracranial arteries, being suggestive of a non-atherosclerotic cerebral vasculopathy. They hypothesized that cerebral vascopathy might be caused by the overproduction of cytokines, such as VEGF, IL-6, and IL-1. Elevating serum levels of IL-6 is very common in patients with Castleman’s disease [61], and it’s well known as a key factor of the systemic inflammatory and a predictor of poor outcome of ischemic stroke [62]. IL-6 may play a pivotal role in the etiologic link between Castleman’s disease and the occurrence of cerebral vascopathy and ischemic stroke.
Recently, the overproduction of VEGF has been proved to contribute to most of the clinical manifestations and correlate with the disease activity and response to therapy [5, 6]. Meanwhile, VEGF is also suggested to be the key factor of vessel walls damage in POEMS syndrome. VEGF is a potent multifunctional cytokine that potently induces angiogenesis, microvascular hyperpermeability and inflammation on vascular endothelial cells [63, 64]. Elevated serum or plasma VEGF, as one of the major diagnostic criteria of POEMS syndrome, induces plasma exudation and the migration of inflammatory cells into vascular inflammatory lesions via upregulating the expression of procoagulative properties, endothelial adhesion molecules and leukocyte chemokine, which in turns initiate and aggravate endothelial damage [65]. Angiogenesis within the adventitia of vessel walls induced by VEGF, which also plays an important role in the pathogenic of chronic inflammation of vessel walls [7, 8, 64]. The histopathological findings of high VEGF expression on arterial smooth muscle cells may result from the high level of VEGF. On the other hand, the elevated VEGF may be produced not only by VEGF secreted from plasma cells and platelets but also by VEGF exudation from inflamed organs including vessels [63]. In this context, VEGF is suggested to be an important mediator in the development of multiple vasculopathy lesions, and this hypothesis is strengthened by the phenomenon that increased VEGF has been observed in many vasculitic disorders include Takayasu’s arteritis and Behcet’s disease [66].
POEMS syndrome is considered as a chronic disease with a good long-term outcome. Recent data demonstrated that 5-year and 10-years survival rate was 84% and 77%, respectively [67]. It’s documented that only age more than 50 years, pulmonary hypertension, pleural effusion and an eGFR less than 30 ml/min/1.73 m2 were independently associated with overall survival [67]. In contrast, we observed fatal outcome in POEMS patients complicated with ischemic stroke. Ten of the eighteen patients who had follow-up data died within two years after stroke events. Even most of them had already received sufficient therapies for ischemic stroke and POEMS syndrome [10, 14, 15, 24, 26, 28]. It suggested that ischemic stroke was a poor outcome predictor in patients with POEMS syndrome. But until now, there is a lack of evidence and standard of the appropriate treatment for the patients who suffer from POEMS syndrome and ischemic stroke simultaneously. The recommended treatments for POEMS syndrome include autologous stem cell transplantation, radiotherapy and melphalan-based chemotherapy [1]. It is worth noting that recurrent ischemic stroke events were interrupted after chemotherapy or corticosteroids therapy in several patients [12, 25, 27]. Immunomodulatory drugs including thalidomide and lenalidomide represent a new treatment option for the patients with POEMS syndrome, not only because of their excellent suppression of monoclonal plasma cell proliferation, but also because of the modulation of VEGF secretion and upregulated cytokines suppressed by these drugs [1, 5, 6, 68]. Meanwhile, VEGF inhibition is currently studied in cardiovascular disease [69] and has also shown neuroprotective effects on cerebral ischemia and reperfusion injury [70]. They have been considered for cerebrovascular disease. Single antiplatelet therapy including aspirin and clopidogrel, as a recommendation of AHA/ASA guideline for stroke secondary prevention [54], showed no effect on stopping ischemic recurrence in many reports [13, 15, 20, 21, 24, 29]. Meanwhile, recurrent events were observed under heparinization or oral anticoagulation [15, 20, 22]. So more aggressive therapy is required. Dual antiplatelet therapy with clopidogrel and aspirin may be a potential treatment, which was reported in some studies [24, 29]. Even though there is an increased incidence of hemorrhage using combination therapy with clopidogrel and aspirin, the risk of ischemic events is markedly reduced in predisposed patients with no response to initial antithrombotic therapy treatment or with established atherothrombotic disease. Despite these advances, the management of POEMS syndrome remains a major challenge, especially in the patients complicated with ischemic stroke.
LIMITATIONS
Ischemic stroke is a less common manifestation of a rare disease-POEMS syndrome. As a result of the lack of understanding of the association between ischemic stroke and POEMS syndrome, many cases have been misdiagnosed. There have been just a few reports on this disease and most of them are case reports. Also, details were not provided in some of the cases, including vascular imaging data, recurrent event data and survival data. The extremely rare occurrence of ischemic stroke in patients with POEMS syndrome and a comprehensive analysis of literature primarily based on cases reports present challenges in establishing any firm conclusions on pathogenesis, management and prognosis. Further research focusing on larger cohort may help in better characterizing and treating this rare complication of POEMS syndrome.
CONCLUSION
To the best of our knowledge, the present case of POEMS syndrome is the first to describe to be associated with cerebral vasculitis confirmed by magnetic resonance vessel-wall imaging technique. The underlying cerebral vasculopathy, leading to the occurrence of ischemic stroke, may be induced by the overproduction of cytokines and systemic inflammation due to POEMS syndrome. Magnetic resonance vessel-wall imaging technique, which is the most promising noninvasive technique for differentiating cerebral vasculopathy from atherosclerotic disease, may contribute to an early diagnosis and treatment for patients with POEMS syndrome. Our literature analysis has revealed that ischemic stroke is a poor outcome predictor in patients with POEMS syndrome. A preponderance of multiple cerebral vessel lesions and low survival rate were observed. VEGF may play a critical role in the pathogenesis of POEMS syndrome. It’s also an important mediator in the development of cerebral vasculopathy. Carefully studying ischemic stroke in patients with POEMS syndrome might help to improve the survival rate and the prognosis.
Authors’ contributions
Fang-wang Fu was the chief physician for this patient and collected the data of this patient. Fang-wang Fu and Jie Rao performed the literature search, extracted and analyzed the data, and wrote the manuscript; Yuan-yuan Zheng, Hui-lin Wang and Jian-guang Yang collected the clinic data and searched published literature. Guo-qing Zheng conceived and designed the study, critically reviewed and revised the manuscript; All authors have read and approved the final submission.
CONSENT
Written informed consent was obtained from the patient before and after all procedures.
CONFLICTS OF INTEREST
The authors declare that they have no conflict of interests regarding the publication of this paper.
REFERENCES
1. Dispenzieri A. POEMS syndrome: update on diagnosis, risk-stratification, and management. Am J Hematol. 2015; 90:951-962.
2. Bardwick PA, Zvaifler NJ, Gill GN, Newman D, Greenway GD, Resnick DL. Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature. Medicine (Baltimore). 1980; 59:311-322.
3. Lewerenz J, Gocht A, Hoeger PH, von den Driesch P, Eckert B, Lamszus K, Stuerenburg HJ, Methner A. Multiple vascular abnormalities and a paradoxical combination of vitamin B12 deficiency and thrombocytosis in a case with POEMS syndrome. J Neurol. 2003; 250:1488-1491.
4. Haider S, Ahmad N, Anaissie EJ, Abdel Karim N. Atypical B12 deficiency with nonresolving paraesthesia. Case Rep Oncol Med. 2013; 2013:823-842.
5. Misawa S, Sato Y, Katayama K, Hanaoka H, Sawai S, Beppu M, Nomura F, Shibuya K, Sekiguchi Y, Iwai Y, Watanabe K, Amino H, Ohwada C, et al. Vascular endothelial growth factor as a predictive marker for POEMS syndrome treatment response: retrospective cohort study. BMJ Open. 2015; 5:e009157.
6. Misawa S, Sato Y, Katayama K, Nagashima K, Aoyagi R, Sekiguchi Y, Sobue G, Koike H, Yabe I, Sasaki H, Watanabe O, Takashima H, Nishizawa M, et al. Safety and efficacy of thalidomide in patients with POEMS syndrome: a multicentre, randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2016; 15:1129-1137.
7. Hashiguchi T, Arimura K, Matsumuro K, Otsuka R, Watanabe O, Jonosono M, Maruyama Y, Maruyama I, Osame M. Highly concentrated vascular endothelial growth factor in platelets in Crow-Fukase syndrome. Muscle Nerve. 2000; 23:1051-1056.
8. Soubrier M, Guillon R, Dubost JJ, Serre AF, Ristori JM, Boyer L, Sauvezie B. Arterial obliteration in POEMS syndrome: possible role of vascular endothelial growth factor. J Rheumatol. 1998; 25:813-815.
9. D’Souza A, Hayman SR, Buadi F, Mauermann M, Lacy MQ, Gertz MA, Kyle RA, Kumar S, Greipp PR, Lust JA, Russell SJ, Zeldenrust S, Dingli D, et al. The utility of plasma vascular endothelial growth factor levels in the diagnosis and follow-up of patients with POEMS syndrome. Blood. 2011; 118:4663-4665.
10. Lesprit P, Authier FJ, Gherardi R, Belec L, Paris D, Melliere D, Schaeffer A, Godeau B. Acute arterial obliteration: a new feature of the POEMS syndrome? Medicine (Baltimore). 1996; 75:226-232.
11. Witoonpanich R, Phankhian S, Jootar S, Poonyathalang A, Worapongpaiboon S, Phudhichareonrat S, Chanplakorn N. POEMS syndrome with venous sinus thrombosis and visual failure: a case report. J Med Assoc Thai. 2005; 88:690-694.
12. Dupont SA, Dispenzieri A, Mauermann ML, Rabinstein AA, Brown RD Jr. Cerebral infarction in POEMS syndrome: incidence, risk factors, and imaging characteristics. Neurology. 2009; 73:1308-1312.
13. Garcia T, Dafer R, Hocker S, Schneck M, Barton K, Biller J. Recurrent strokes in two patients with POEMS syndrome and Castleman’s disease. J Stroke Cerebrovasc Dis. 2007; 16:278-284.
14. Lee MR, Choi HJ, Lee EB, Baek HJ. POEMS syndrome complicated by extensive arterial thromboses. Clin Rheumatol. 2007; 26:1989-1992.
15. Akyol A, Nazliel B, Batur Caglayan HZ, Oner Y, Sucak GT. Recurrent Transient Ischemic Attacks in a Patient with POEMS Syndrome. Case Rep Neurol Med. 2014; 2014:158471.
16. Rajan R, Wilson V, Das B, Singh P, Ahluwalia J, Mehta S, Lal V. Stroke and POEMS syndrome: More than a chance association. Neurol India. 2016; 64:1318-1319.
17. Soubrier M, Dubost JJ, Serre AF, Ristori JM, Sauvezie B, Cathebras P, Piette JC, Chapman A, Authier FJ, Gherardi RK. Growth factors in POEMS syndrome: evidence for a marked increase in circulating vascular endothelial growth factor. Arthritis Rheum. 1997; 40:786-787.
18. Li J, Zhou DB, Huang Z, Jiao L, Duan MH, Zhang W, Zhao YQ, Shen T. Clinical characteristics and long-term outcome of patients with POEMS syndrome in China. Ann Hematol. 2011; 90:819-826.
19. Forster A, Muri R. Recurrent cerebrovascular insult—manifestation of POEMS syndrome? Schweiz Med Wochenschr. 1998; 128:1059-1064.
20. Erro ME, Lacruz F, Aymerich N, Ayuso T, Soriano G, Gallego J, Villanueva JA. Acute carotid obliteration: a new vascular manifestation in POEMS syndrome. Eur J Neurol. 2003; 10:383-384.
21. Kang K, Chu K, Kim DE, Jeong SW, Lee JW, Roh JK. POEMS syndrome associated with ischemic stroke. Arch Neurol. 2003; 60:745-749.
22. Rossler M, Kiessling B, Klotz JM, Langohr HD. Recurrent cerebral ischemias due to cerebral vasculitis within the framework of incomplete POEMS syndrome with Castleman disease. Nervenarzt. 2004; 75:790-794.
23. Huang J, Wang L, Zhou W, Jin J. Hyaline vascular Castleman disease associated with POEMS syndrome and cerebral infarction. Ann Hematol. 2007; 86:59-61.
24. Sommer B, Schaumberg J. Therapeutic challenges in a patient with POEMS syndrome and recurrent stroke: presentation of a case and review of the literature. Acta Neurol Belg. 2012; 112:9-13.
25. Dacci P, Lessi F, Dalla Bella E, Morbin M, Briani C, Lauria G. Ischemic stroke as clinical onset of POEMS syndrome. J Neurol. 2013; 260:3178-3181.
26. Yu H, Yao F, Li Y, Li J, Cui QC. Castleman disease variant of POEMS syndrome complicated with multiple cerebral infarction: a rare case report and review of literature. Int J Clin Exp Pathol. 2015; 8:13578-13583.
27. Han TT, Zheng S, Chen ZA, Liu W, Hu YM. Young patient with arterial thrombosis and skin changes as the onset manifestations: POEMS syndrome. Oncotarget. 2016; 7:74410-74414. doi: 10.18632/oncotarget.12570.
28. Yaghi S, Elkind MS. Paraneoplastic Progressive Vasculopathy as the Presenting Manifestation of Polyneuropathy, Organomegaly, Endocrinopathy or Edema, M-Spike, and Skin Manifestations: A Case Report. J Stroke Cerebrovasc Dis. 2016; 25:e103-107.
29. Wang Z, Xiong L, Zu H. Recurrent Stroke as the Clinical Onset of POEMS Syndrome. J Clin Neurol. 2017; 13:199-200.
30. Wang HY, Li W, Zhao Z, Jiang L. POEMS syndrome with cerebral infarction: a case report. J Apop and Nerv Dis. 2006; 23:431.
31. Du ZG, Wang Y. Cerebral infarction in a patient with Crow-Fukase syndrome. J Fourth Mil Med Univ. 2008; 29:832.
32. Zheng HF. Cerebral infarction in a patient with POEMS syndrome. J Med Theor and Prac. 2008; 21:533-535.
33. Shi X, Zhu Y, Zhuang Q, Luo M, Lu Y, Fei X, Wang L, Yu X, Ba R. POEMS syndrome complicated with cerebral infarction: a case report. Jiangsu Med J. 2010; 36:615-616.
34. Jing J, Zhao Z, Ren X, Zhang H. Cerebral infarction in patients with POEMS syndrome: a case report and literature review. J Chin Prac Nerv Dis. 2011; 14:46-47.
35. Li X, Ren Y, Ren S. Bilateral cerebral infarction in a patient with POEMS syndrome. J Chin Diffic and Compl Cas. 2015; 14:971-972.
36. Sun LX, Lu H, Wu X, Ma G, Zhang J. Peripheral neuropathy, M protein, multiple abnormalities in the cerebral cortex. Clin Focus. 2015; 30:1309-1312.
37. Liu XX, Pang Q, Zhang G, Chen L, Hu H, Sun L. Cerebral infarction and POEMS syndrome: a case report and literature review. J Apop and Nerv Dis. 2016; 33:848-849.
38. Hori T, Tsuboi Y, Okubo R, Hirooka M, Yamada T. Crow-Fukase syndrome associated with Castleman disease showing hypertrophic cranial pachymeningitis and bilateral internal carotid artery occlusion. Rinsho Shinkeigaku. 1999; 39:456-460.
39. Zhan SQ, Jia JP, Wang ML. Acute Cerebral Infarction in POEMS Syndrome. Chinese Journal of Medical Imaging Technology. 2002;18:30-31.
40. Zenone T, Bastion Y, Salles G, Rieux C, Morel D, Felman P, Espinouse D, Bryon PA, Coiffier B. POEMS syndrome, arterial thrombosis and thrombocythaemia. J Intern Med. 1996; 240: 107-9.
41. Dispenzieri A, Kyle RA, Lacy MQ, Rajkumar SV, Therneau TM, Larson DR, Greipp PR, Witzig TE, Basu R, Suarez GA, Fonseca R, Lust JA, Gertz MA. POEMS syndrome: definitions and long-term outcome. Blood. 2003; 101:496-506.
42. Barbui T, Finazzi G, Carobbio A, Thiele J, Passamonti F, Rumi E, Ruggeri M, Rodeghiero F, Randi ML, Bertozzi I, Gisslinger H, Buxhofer-Ausch V, De Stefano V, et al. Development and validation of an International Prognostic Score of thrombosis in World Health Organization-essential thrombocythemia (IPSET-thrombosis). Blood. 2012; 120:5128-5133.
43. Carobbio A, Finazzi G, Antonioli E, Guglielmelli P, Vannucchi AM, Delaini F, Guerini V, Ruggeri M, Rodeghiero F, Rambaldi A, Barbui T. Thrombocytosis and leukocytosis interaction in vascular complications of essential thrombocythemia. Blood. 2008; 112:3135-3137.
44. Gherardi RK, Authier FJ, Belec L. Pro-inflammatory cytokines: a pathogenic key of POEMS syndrome. Rev Neurol (Paris). 1996; 152:409-412.
45. Moons KG, Bots ML, Salonen JT, Elwood PC, Freire de Concalves A, Nikitin Y, Sivenius J, Inzitari D, Benetou V, Tuomilehto J, Koudstaal PJ, Grobbee DE. Prediction of stroke in the general population in Europe (EUROSTROKE): Is there a role for fibrinogen and electrocardiography? J Epidemiol Community Health. 2002; 56:i30-36.
46. Chuang SY, Bai CH, Chen WH, Lien LM, Pan WH. Fibrinogen independently predicts the development of ischemic stroke in a Taiwanese population: CVDFACTS study. Stroke. 2009; 40:1578-1584.
47. Margaglione M, Grandone E, Mancini FP, Di Minno G. Genetic Modulation of Plasma Fibrinogen Concentrations: Possible Importance of Interleukin-6. J Thromb Thrombolysis. 1996; 3:51-56.
48. Di Napoli M, Arakelyan A. POEMS syndrome, fibrinogen, and ischemic stroke: a critical point of view. Arch Neurol. 2004; 61:155.
49. Di Napoli M, Papa F, Villa Pini Stroke Data Bank I. Inflammation, hemostatic markers, and antithrombotic agents in relation to long-term risk of new cardiovascular events in first-ever ischemic stroke patients. Stroke. 2002; 33:1763-1771.
50. Saposnik G, Ray JG, Sheridan P, McQueen M, Lonn E, Heart Outcomes Prevention Evaluation I. Homocysteine-lowering therapy and stroke risk, severity, and disability: additional findings from the HOPE 2 trial. Stroke. 2009; 40:1365-1372.
51. Seitz M, Reichenbach S, Bonel HM, Adler S, Wermelinger F, Villiger PM. Rapid induction of remission in large vessel vasculitis by IL-6 blockade. A case series. Swiss Med Wkly. 2011; 141:w13156.
52. Flatley EM, Segal GM, Batiuk TD, Bennett WM, Houghton DC, Troxell ML. Glomerular endothelial vesicles in a renal allograft: an unusual pattern of immunoglobulin deposition in a patient with biclonal gammopathy of unknown significance. Am J Surg Pathol. 2015; 39:864-869.
53. Gorelick PB, Wong KS, Bae HJ, Pandey DK. Large artery intracranial occlusive disease: a large worldwide burden but a relatively neglected frontier. Stroke. 2008; 39:2396-2399.
54. Kernan WN, Ovbiagele B, Black HR, Bravata DM, Chimowitz MI, Ezekowitz MD, Fang MC, Fisher M, Furie KL, Heck DV, Johnston SC, Kasner SE, Kittner SJ, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014; 45:2160-2236.
55. Cole JW. Large Artery Atherosclerotic Occlusive Disease. Continuum (Minneap Minn). 2017; 23:133-157.
56. Kuker W, Gaertner S, Nagele T, Dopfer C, Schoning M, Fiehler J, Rothwell PM, Herrlinger U. Vessel wall contrast enhancement: a diagnostic sign of cerebral vasculitis. Cerebrovasc Dis. 2008; 26:23-29.
57. Shibata M, Yamada T, Tanahashi N, Koto A, Kuramochi S, Fukushima S, Fukuuchi Y. POEMS syndrome with necrotizing vasculitis: a novel feature of vascular abnormalities. Neurology. 2000; 54:772-773.
58. Fukatsu A, Tamai H, Nishikawa K, Matsukawa W, Yoshida F, Matsuo S, Takeda A, Kodera K, Morozumi K, Ito Y, Miyakawa K, Toriyama T, Kawahara H, et al. The kidney disease of Crow-Fukase (POEMS) syndrome: a clinico-pathological study of four cases. Clin Nephrol. 1991; 36:76-82.
59. Lee J, Huprikar S, Jenkins SG. Are patients with POEMS syndrome at increased risk of Salmonella aortitis? Int J Infect Dis. 2009; 13:e97-99.
60. Yamaguchi I, Satomi J, Yamamoto N, Yoshioka S, Tada Y, Yagi K, Kanematsu Y, Nagahiro S. Coexistence of Quasi-moyamoya Disease and POEMS Syndrome in a Patient with Intracranial Hemorrhage: A Case Report and Literature Review. NMC Case Report Journal. 2017; 4:5-9.
61. El-Osta HE, Kurzrock R. Castleman’s disease: from basic mechanisms to molecular therapeutics. Oncologist. 2011; 16:497-511.
62. Bustamante A, Sobrino T, Giralt D, Garcia-Berrocoso T, Llombart V, Ugarriza I, Espadaler M, Rodriguez N, Sudlow C, Castellanos M, Smith CJ, Rodriguez-Yanez M, Waje-Andreassen U, et al. Prognostic value of blood interleukin-6 in the prediction of functional outcome after stroke: a systematic review and meta-analysis. J Neuroimmunol. 2014; 274:215-224.
63. Grutzkau A, Kruger-Krasagakes S, Baumeister H, Schwarz C, Kogel H, Welker P, Lippert U, Henz BM, Moller A. Synthesis, storage, and release of vascular endothelial growth factor/vascular permeability factor (VEGF/VPF) by human mast cells: implications for the biological significance of VEGF206. Mol Biol Cell. 1998; 9:875-884.
64. Keyt BA, Berleau LT, Nguyen HV, Chen H, Heinsohn H, Vandlen R, Ferrara N. The carboxyl-terminal domain (111-165) of vascular endothelial growth factor is critical for its mitogenic potency. J Biol Chem. 1996; 271:7788-7795.
65. Kim I, Moon SO, Kim SH, Kim HJ, Koh YS, Koh GY. Vascular endothelial growth factor expression of intercellular adhesion molecule 1 (ICAM-1), vascular cell adhesion molecule 1 (VCAM-1), and E-selectin through nuclear factor-kappa B activation in endothelial cells. J Biol Chem. 2001; 276:7614-7620.
66. Ozturk MA, Unverdi S, Oktar SO, Bukan N, Gulbahar O, Ureten K, Goker B, Haznedaroglu S, Sungur G, Ciftci TU, Onat AM. Vascular endothelial growth factor and carotid intima-media thickness in patients with Behcet’s disease. Clin Rheumatol. 2008; 27:961-966.
67. Wang C, Huang XF, Cai QQ, Cao XX, Duan MH, Cai H, Zhou DB, Li J. Prognostic study for overall survival in patients with newly diagnosed POEMS syndrome. Leukemia. 2017; 31:100-106.
68. Wu KL, Chen HW, Lin SH, Chen JS. Intractable ascites, changes in serum vascular endothelial growth factor levels and thalidomide treatment in POEMS syndrome. Am J Med Sci. 2014; 347:510-512.
69. Orea-Tejeda A, Arrieta-Rodriguez O, Castillo-Martinez L, Rodriguez-Reyna T, Asensio-Lafuente E, Granados-Arriola J, Dorantes-Garcia J. Effects of thalidomide treatment in heart failure patients. Cardiology. 2007; 108:237-242.
70. Palencia G, Medrano JA, Ortiz-Plata A, Farfan DJ, Sotelo J, Sanchez A, Trejo-Solis C. Anti-apoptotic, anti-oxidant, and anti-inflammatory effects of thalidomide on cerebral ischemia/reperfusion injury in rats. J Neurol Sci. 2015; 351:78-87.