Oncotarget (a primarily oncology-focused, peer-reviewed, open access journal) aims to maximize research impact through insightful peer-review; eliminate borders between specialties by linking different fields of oncology, cancer research and biomedical sciences; and foster application of basic and clinical science.
Its scope is unique. The term "oncotarget" encompasses all molecules, pathways, cellular functions, cell types, and even tissues that can be viewed as targets relevant to cancer as well as other diseases. The term was introduced in the inaugural Editorial,
Introducing Oncotarget.
As of January 1, 2022, Oncotarget has shifted to a continuous publishing model. Papers will now be published continuously within yearly volumes in their final and complete form and then quickly released to Pubmed.
Publication Alerts
Subscribe to receive alerts once a paper has been published by Oncotarget.
Received: August 10, 2010, Accepted: October 18, 2010, Published: October 19, 2010
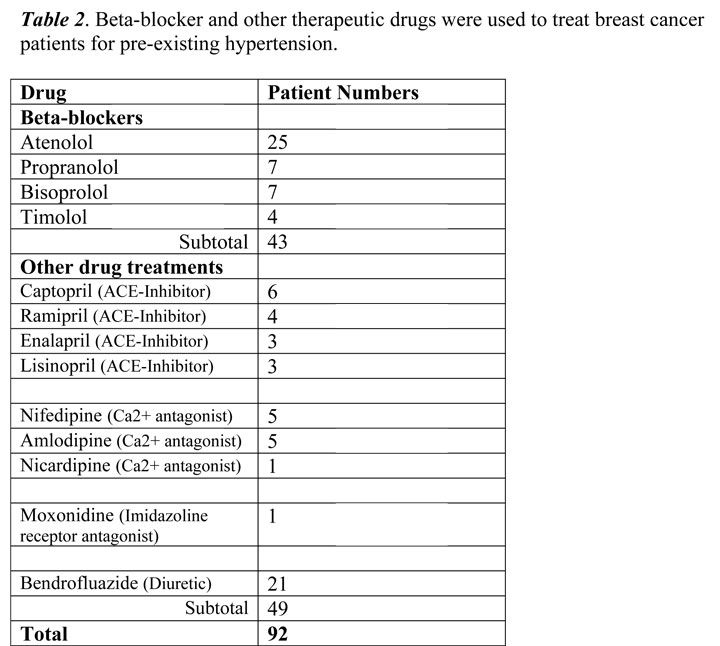
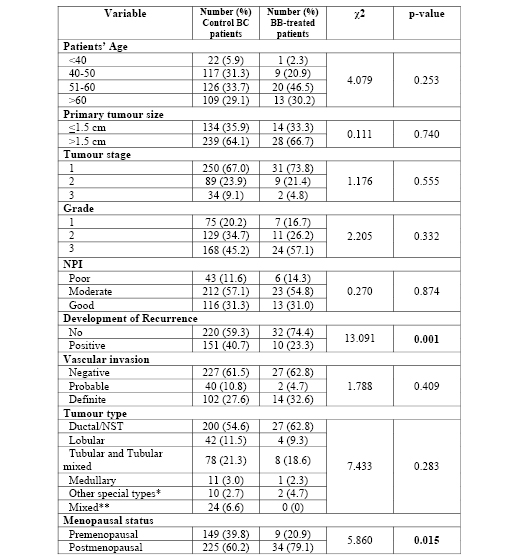
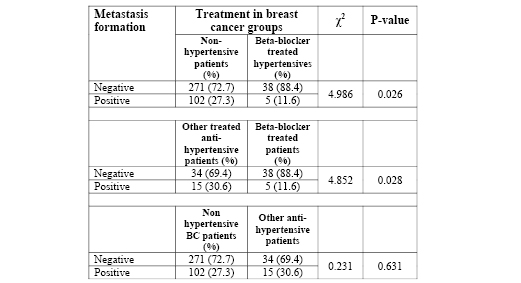
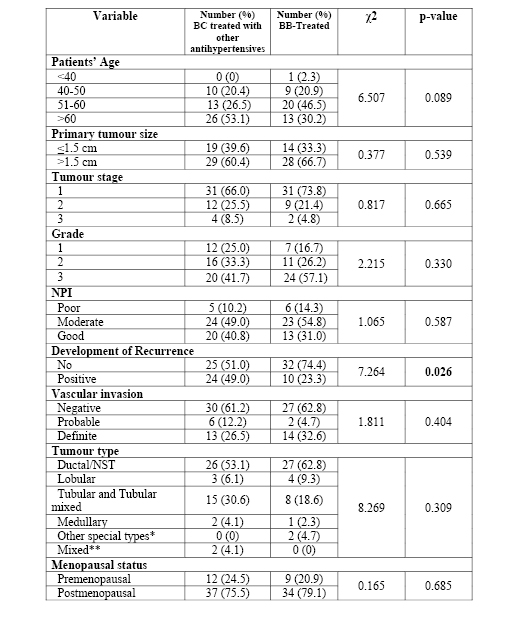
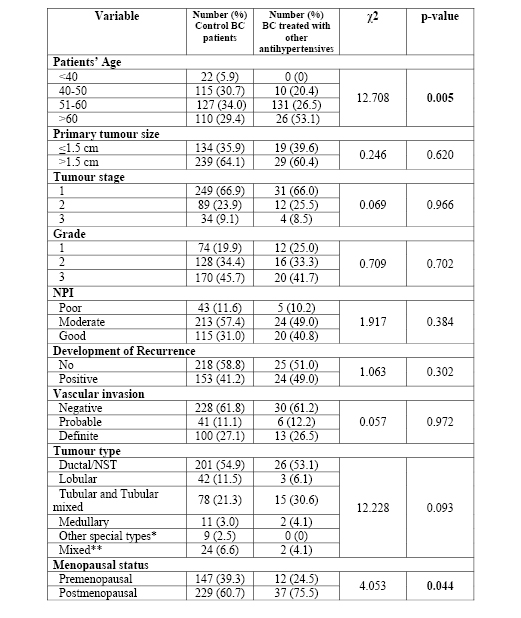
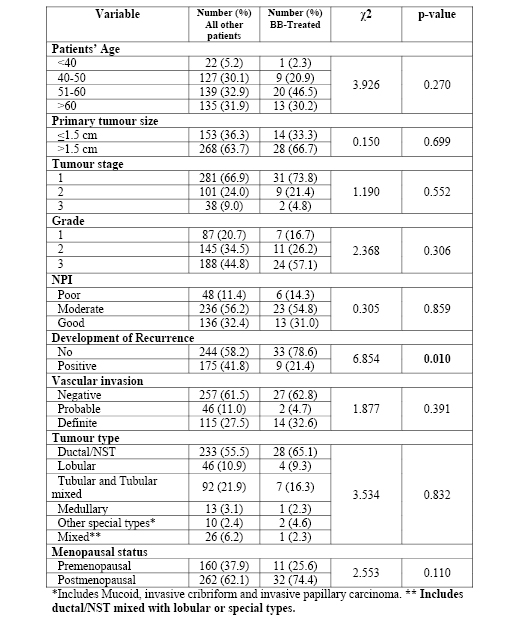
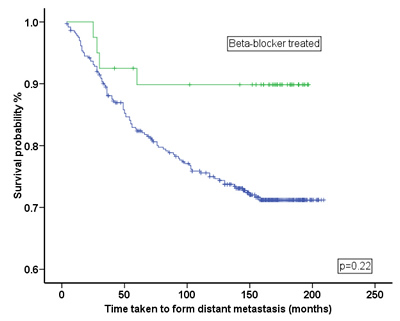
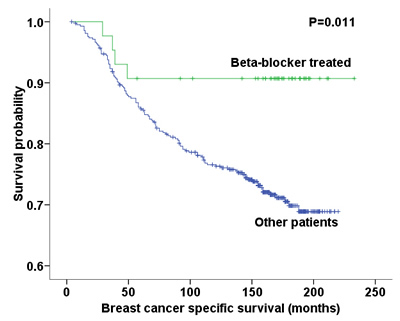
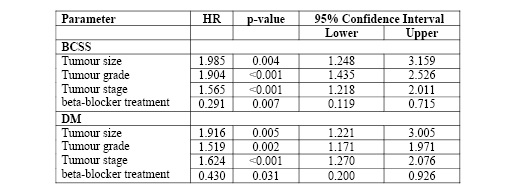
Laboratory models show that the beta-blocker, propranolol, can inhibit norepinephrine-induced breast cancer cell migration. We hypothesised that breast cancer patients receiving beta-blockers for hypertension would show reduced metastasis and improved clinical outcome. Three patient subgroups were identified from the medical records of 466 consecutive female patients (median age 57, range 28-71) with operable breast cancer and follow-up (>10 years). Two subgroups comprised 43 and 49 hypertensive patients treated with beta-blockers or other antihypertensives respectively, prior to cancer diagnosis. 374 patients formed a non-hypertensive control group. Metastasis development, disease free interval, tumour recurrence and hazards risk were statistically compared between groups. Kaplan-Meier plots were used to model survival and DM. Beta-blocker treated patients showed a significant reduction in metastasis development (p=0.026), tumour recurrence (p=0.001), and longer disease free interval (p=0.01). In addition, there was a 57% reduced risk of metastasis (Hazards ratio=0.430; 95% CI=0.200-0.926, p=0.031), and a 71% reduction in breast cancer mortality after 10 years (Hazards ratio=0.291; 95% CI=0.119-0.715, p=0.007). This proof-of-principle study showed beta-blocker therapy significantly reduces distant metastases, cancer recurrence, and cancer-specific mortality in breast cancer patients suggesting a novel role for beta-blocker therapy. A larger epidemiological study leading to randomised clinical trials is needed for breast and other cancer types including colon, prostate and ovary.
INTRODUCTION
Although an estimated 38,000 [1] patients are diagnosed with breast cancer in the US each year death rates are declining in part due to adjuvant therapies including the use of ER-antagonists and anti-HER2 (trastuzumab) therapy [2-4]. Nonetheless, approximately 30% of treated BC patients develop distant metastases [5] and these significantly account for 90% of breast cancer deaths [6]. Consequently, therapeutic strategies are needed that target metastasis [7, 8].
Metastasis formation involves migration of malignant cells from the primary tumour via lymphatic or blood vessel routes with the process being tightly regulated by exogenous cell signalling molecules, including ligands to G protein-coupled receptors (GPCRs) such as neurotransmitters and chemokines [9, 10]. In previous in vitro cell migration studies we have shown that the stress catecholamine hormone norepinephrine is a potent inducer of migratory activity in carcinoma cell lines of colon [11], prostate [12], ovarian cancer cells [13] and breast [14] tissue origin, and this finding has been confirmed in a mouse model [15