
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is responsible for around 6 percent of all deaths worldwide in 2012, and will be the third leading cause of death by 2020 [1, 2]. Although emerging different pharmacological treatments have significantly improved the lung function and exercise tolerance in mild or moderate COPD patients, few effective options are available for severe COPD [3]. Lung-volume-reduction surgery (LVRS), removing particularly damaged emphysema, allowing the relatively good lung to expand and work more efficiently, has been found to improve the quality of life and pulmonary functionfor patients with severe heterogeneous emphysema [4, 5]. However, due to the invasiveness and higher mortality associated with LVRS, it remains controversial to recommend patients for this surgery [5, 6].
Less invasive bronchoscopic lung volume reduction (BLVR) has achieved improvement in severe emphysema, including endobronchial coils, endobronchial valves, bronchial vapor ablation, lung sealants, and airway bypass [7, 8]. Recently, several randomized controlled trials (RCTs) have compared BLVR to medical therapy for advanced emphysema, and the results were encouraging, as confirmed in published meta-analyses [9-11]. However, previous meta-analyses pooled less RCTs and information, and more RCTs were published recently. Thus, to provide the latest and most convincing evidence, we aimed to identify and review RCTs which examined the roles and safety of BLVR in patients with emphysema.
RESULTS
Study characteristics
The study flow diagram, including the reasons for exclusion of studies, is shown in Figure 1. A total of 1802 records were retrieved from the database search, of which 385 studies were excluded for duplicates. We excluded 1369 studies based on abstracts, and the remaining 48 full-text articles were assessed for eligibility. Of these, 34 studies were excluded for the following: reviews (n=7), non-RCTs (n=25), and the same researches (n=2). Also, 1 RCT for bronchial vapor ablation, 1 RCT for lung sealants, and 1 RCT for airway bypass were omitted [12-14]. Finally, 3 RCTs for endobronchial coils and 8 RCTs for valves were included in the meta-analysis [15-25]. Of the 8 studies for valves, 6 studies used endobronchial valves (EBV (Zephyr)) [15, 17, 18, 20, 21, 24] and 2 studies used intrabronchial valves (IBV (Spiration)) [16, 22]. The characteristics and inclusion and exclusion criteria of the included trials were presented in Tables 1 and 2. The study by Valipour [17] included the data from 416 patients with advanced emphysema across Europe VENT trial by Herth [20] and USA VENT trial by Sciurba [24].
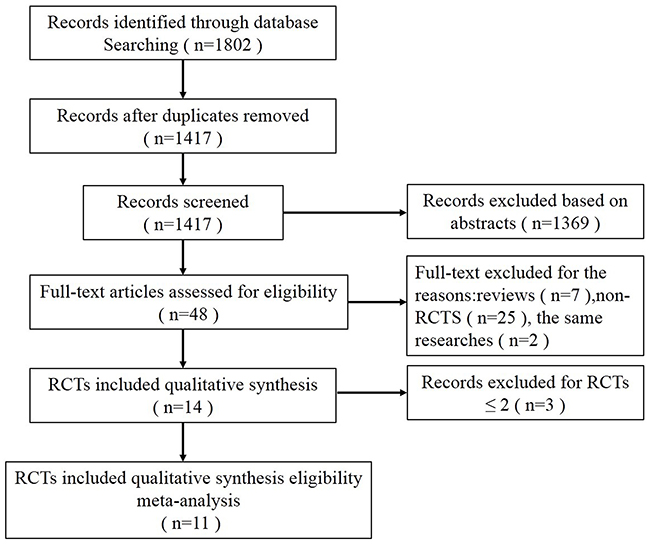
Figure 1: Flow diagram showing inclusion and exclusion of studies.
Table 1: Baseline demographics and disease characteristics of the included RCTs
Study |
Duration (months) |
Sample size |
Age (years), mean (SD) |
FEV1 (% predicted) mean (SD) |
6MWT (m) mean (SD) |
SGRQ (points) mean (SD) |
mMRC (points) mean (SD) |
Goals in MCID (from baseline) |
|---|---|---|---|---|---|---|---|---|
Sciurba 2010 |
3, 6, 12 |
EBV 220 |
EBV 65.3 (6.8) |
EBV 30.0 (8.0) |
EBV 333.9 (87.4 ) |
NR |
NR |
ΔFEV1 > 15% |
Ninane |
3 |
IBV 37 |
IBV 61.0 (7.0) |
IBV 35.0 (10.0) |
IBV 337.0 (106.0) |
IBV 61.0 (11.0) |
IBV 2.8 (0.7) |
ΔFEV1 (NR) |
Herth |
6, 12 |
EBV 111 |
EBV 59.7 (7.9) |
EBV 29.0 (8.0) |
EBV 341.0 (108.0) |
EBV 59.0 (13.0) |
NR |
ΔFEV1 ≥ 15% |
Shah |
3 |
Coils 23 |
Coils 62.0 (7.0) |
Coils 27.2 (8.0) |
Coils 293.7 (75.5) |
Coils 65.2 (8.7) |
Unclear |
ΔFEV1 ≥ 10% |
Valipour 2014 |
6 |
EBV 331 |
EBV 63.4 (7.7) |
EBV 30.0 (8.0) |
EBV 336.0 (95.0 ) |
EBV 54.4 (13.7) |
EBV 1.9 (1.0) |
ΔFEV1 ≥ 12% |
Wood |
6 |
IBV 142 |
IBV 64.7 (6.3) |
IBV 29.8 (7.5) |
IBV 314.1 (88.6) |
IBV 54.8 (15.5) |
IBV 2.7 (0.7) |
ΔFEV1 (NR) |
Davey |
3 |
EBV 25 |
EBV 62.3 (7.0) |
EBV 31.6 (10.2) |
EBV 342.0 (94.0) |
EBV 67.8 (13.2) |
EBV 4.0 (1.0) |
ΔFEV1 ≥ 15% |
Klooster 2015 |
6 |
EBV 34 |
EBV 58.0 (10.0) |
EBV 29.0 (7.0) |
EBV 372.0 (90.0) |
EBV 59.1 (13.7) |
EBV 2.7 (0.8) |
ΔFEV1 ≥ 10% |
Deslée |
6, 12 |
Coils 50 |
Coils 62.1 (8.3) |
Coils 25.7 (7.5) |
Coils 300.0 (112.0) |
Coils 60.8 (12.8) |
Unclear |
ΔFEV1 (NR) |
Sciurba |
12 |
Coils 158 |
Coils 63.4 (8.1) |
Coils 25.7 (6.3) |
Coils 312.0 (79.1) |
Coils 60.1 (12.8) |
Unclear |
ΔFEV1 ≥ 10% |
Valipour |
3 |
EBV 43 |
EBV 64.3 (6.3) |
EBV 28.4 (6.3) |
EBV 308.0 (91.0) |
EBV 63.2 (13.7) |
EBV 2.7 (0.8) |
ΔFEV1 ≥ 12% |
RCT = randomized controlled trial, Coils = endobronchial coils, EBV = endobronchial valves (Zephyr), IBV = intrabronchial valves (Spiration), MCID = minimal clinically important difference, FEV1 = forced expiratory volume in 1s, 6-min walk test (6MWT), SGRQ = St. George’s Respiratory Questionnaire, mMRC = modified Medical Research Council, NR = not reported.
Table 2: Inclusion and exclusion criteria
Study |
Major inclusion criteria |
Major exclusion criteria |
|---|---|---|
Sciurba 2010 |
Aged 40 to 75 years; Heterogeneous emphysema; 15 predicted < FEV1< 45% predicted; TLC >100% predicted; RV >150% predicted; PaCO2 < 50mm Hg and PaO2 >45mm Hg; 6MWT ≥140 m. |
DLCO < 20% predicted; Giant bulla or α1-antitrypsin deficiency; Thoracotomy, Excessive sputum; Severe pulmonary hypertension; Active infection. |
Ninane 2012 |
Aged 40 to 75 years; Predominantly upper lobe emphysema and severe dyspnea; FEV1 <45% predicted; TLC ≥100% predicted and RV ≥150% predicted; 6MWT ≥140 m. |
DLCO < 20% predicted; Giant bulla or α1-antitrypsin deficiency; Severe pulmonary hypertension; Requirement for > 6 L O2 to keep saturation ≥ 90% with exercise; Thoracotomy. |
Herth 2012 |
Similar to the study by Sciurba 2010. |
Similar to the study by Sciurba 2010. |
Shah 2013 |
Aged ≥35 years; Unilateral or bilateral emphysema; Homogeneous or heterogeneous emphysema; Post-bronchodilator FEV1 ≤ 45% predicted; TLC >100% predicted; mMRC dyspnoea score ≥2. |
Change in FEV1 > 20% post-bronchodilator; DLCO < 20% predicted; Active infection, uncontrolled pulmonary hypertension; 6MWT≤ 140 m; Significant bronchiectasis; Giant bullae; Thoracotomy; Taking ≥ 20 mg prednisone daily. |
Valipour 2014 |
Similar to the study by Sciurba 2010. |
Similar to the study by Sciurba 2010. |
Wood 2014 |
Aged 40 to 74 years; Predominantly upper lobe emphysema and severe dyspnea; FEV1 ≤ 45% predicted; TLC ≥ 100% predicted and RV ≥ 150% predicted; 6MWT ≥ 140 m. |
FEV1 and DLCO < 20% predicted; PCO2 > 50 mm Hg, PaO2 < 45 mm Hg; Two or more hospitalizations for COPD exacerbation or respiratory infections in the past year; Excessive sputum; Taking ≥ 15 mg prednisone daily; Giant bulla, α1-antitrypsin deficiency; Severe pulmonary hypertension; Requirement for > 6 L O2 to keep saturation ≥ 90% with exercise; Thoracotomy. |
Davey 2015 |
FEV1 ≤50% predicted; TLC ≥ 100% predicted and RV ≥ 150% predicted; 6MWT <450 m; mMRC dyspnoea score ≥3; Heterogeneous emphysema and intact adjacent interlobar fissures. |
Excessive sputum; Lower limits for lung function were not otherwise formally defined but patients were excluded if they were considered clinically to be too restricted or frail to undergo bronchoscopy or to tolerate a pneumothorax. |
Klooster 2015 |
Aged ≥ 35 years; Post-bronchodilator FEV1 ≤ 60% predicted, TLC ≥ 100% predicted and RV ≥ 150% predicted; mMRC dyspnoea score ≥ 1; Complete fissure between the target lobe and the adjacent lobe. |
Collateral ventilation in the target lobe and failure to achieve lobar occlusion with endobronchial valves. |
Deslée 2016 |
Bilateral emphysema; Post-bronchodilator FEV1 ≤ 50% predicted; TLC ≥ 100% predicted and RV ≥ 220% predicted; mMRC dyspnoea score ≥ 2. |
Post-bronchodilator FEV1 < 15% predicted; Post-bronchodilator change in FEV1 > 20%; Severe recurrent respiratory infections requiring more than 2 hospitalization stays in the past year; Severe pulmonary hypertension ; Unable to perform a 6MWT in room air; Giant bulla ; Homogeneous emphysema; Significant bronchiectasis; Thoracotomy. |
Sciurba 2016 |
Aged ≥35 years; Bilateral emphysema; post-bronchodilator FEV1 ≤ 45% predicted; TLC ≥ 100% predicted and RV ≥ 175% predicted; mMRC dyspnoea score ≥ 2. |
Severe homogeneous emphysema; Post-bronchodilator change in FEV1 >20%; DLCO <20% predicted; PaCO2 >55 mm Hg, PaO2 <45 mm Hg; Recurrent significant respiratory infections in the past year; Severe pulmonary hypertension; 6MWT≤ 140 m ; Significant bronchiectasis; Giant bulla or α1-antitrypsin deficiency ; Thoracotomy; Taking >20 mg prednisone daily. |
Valipour |
Aged ≥40 years; Homogeneous emphysema; 15 % predicted ≤ FEV1≤ 45 % predicted ;TLC > 100% predicted, RV ≥ 200% predicted; 6MWT > 150 m; Collateral ventilation negative target lobe |
Active pulmonary infection and more than 3 exacerbations with hospitalizations in the past year; Severe pulmonary hypertension ; α1-antitrypsin deficiency ; excessive sputum; PaCO2 > 55 mm Hg; Taking > 25mg Prednisolone daily; Giant bulla or α1-antitrypsin deficiency; Thoracotomy. |
FEV1 = forced expiratory volume in 1s, TLC = total lung capacity, RV = residual volume, 6MWT = 6-min walk test, DLCO = carbon monoxide diffusing capacity, mMRC= modified Medical Research Council.
Risk of bias
The assessment of risk of bias was summarized in Figure 2. Six RCTs were judged to be an unclear risk of selecting bias, and eight RCTs generated high risk of bias in performance bias. It is very difficult in implementing a sham procedure in blinding of patients and clinicians in BLVR and may have influenced outcomes.
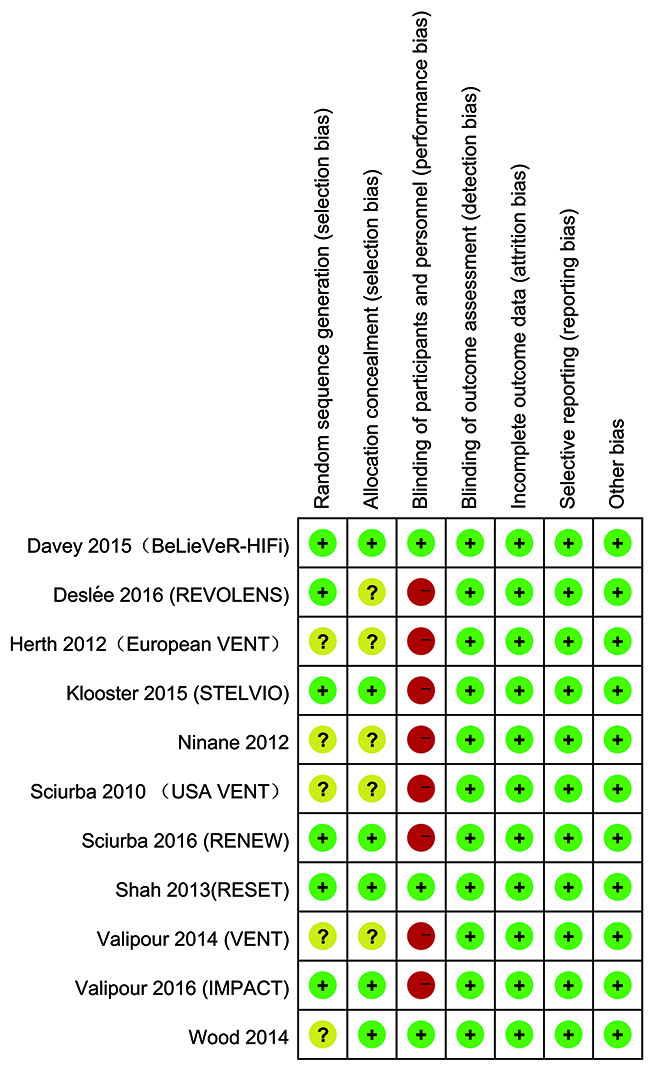
Figure 2: Risk of bias summary.
Primary outcomes: responder analysis
The most popular tools to assess lung function, exercise capacity and quality of life are forced expiratory volume in 1s (FEV1), 6-min walk test (6MWT) and St. George’s Respiratory Questionnaire (SGRQ), which were used in almost all included studies. The modified Medical Research Council (mMRC) dyspnea scale was also used to assess quality of life. In the present study, endobronchial coils achieved a clinically significant improvement in FEV1 (risk ratio (RR) = 2.37, 95% confidence interval (CI) = 1.61 – 3.48, p <0.0001, I2= 0%), in 6MWT (RR = 2.05, 95% CI = 1.18 –3.53, p = 0.01, I2 = 57%), and in SGRQ (RR = 2.32, 95% CI = 1.77 – 3.03, p < 0.00001, I2 = 0%), compared with control (Figures 3–5). Also, EBV treatment showed better response in minimal clinically important difference (MCID) for FEV1 (RR = 2.96, 95% CI = 1.49 – 5.87, p = 0.002, I2 = 58%), for 6MWT (RR = 2.90, 95% CI = 1.24 – 6.79, p = 0.01, I2 = 80%), for SGRQ (RR = 1.53, 95% CI = 1.22 – 1.92, p = 0.0002, I2 = 0%), as well as for mMRC (RR = 2.53, 95% CI = 1.71 – 3.76, p <0.00001, I2 = 0%) (Figures 3–6).
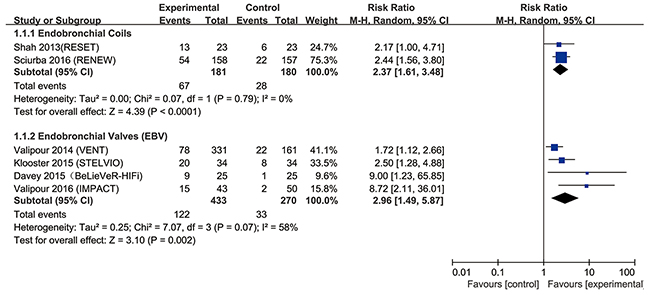
Figure 3: Effect of bronchoscopic lung volume reduction (BLVR) therapy on forced expiratory volume in 1s (FEV1) in patients with severe emphysema. The term “Events” refers to the number of patients who reached MCID, and “Total” refers to the number of total patients. Risk ratios for each trial are represented by the squares, and the horizontal line crossing the square represents the 95% confidence interval (CI). The diamonds represent the estimated overall effect based on the meta-analysis random effect of the trials.
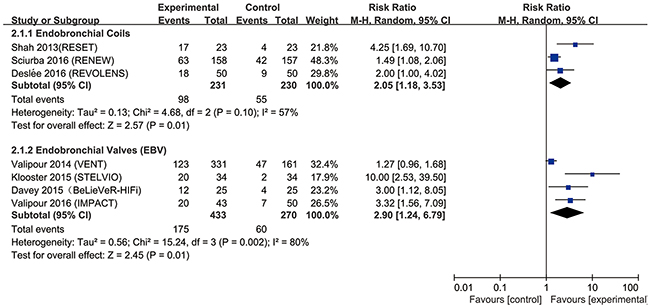
Figure 4: Effect of bronchoscopic lung volume reduction (BLVR) therapy on 6-min walk test (6MWT) in patients with severe emphysema. The term “Events” refers to the number of patients who reached MCID, and “Total” refers to the number of total patients. Risk ratios for each trial are represented by the squares, and the horizontal line crossing the square represents the 95% confidence interval (CI). The diamonds represent the estimated overall effect based on the meta-analysis random effect of the trials.
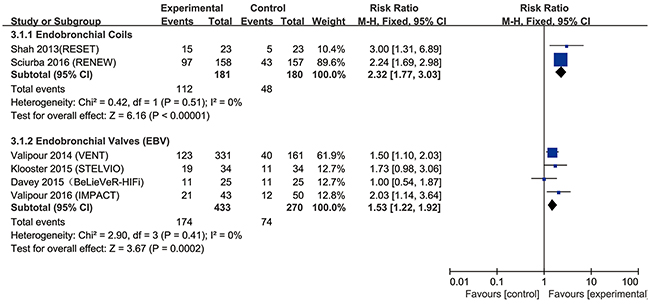
Figure 5: Effect of bronchoscopic lung volume reduction (BLVR) on St. George’s Respiratory Questionnaire (SGRQ) in patients with severe emphysema. The term “Events” refers to the number of patients who reached MCID, and “Total” refers to the number of total patients. Risk ratios for each trial are represented by the squares, and the horizontal line crossing the square represents the 95% confidence interval (CI). The diamonds represent the estimated overall effect based on the meta-analysis fixed effect of the trials.
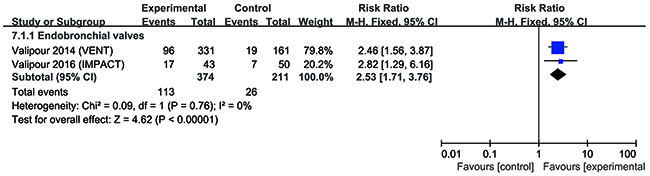
Figure 6: Effect of bronchoscopic lung volume reduction (BLVR) on modified Medical Research Council (mMRC) in patients with severe emphysema. The term “Events” refers to the number of patients who reached MCID, and “Total” refers to the number of total patients. Risk ratios for each trial are represented by the squares, and the horizontal line crossing the square represents the 95% confidence interval (CI). The diamonds represent the estimated overall effect based on the meta-analysis fixed effect of the trials.
Secondary outcomes: absolute change in FEV1, 6MWT, SGRQ and mMRC from baseline, and safety assessment
Data for the absolute change BLVR were available from 11 RCTs (Table 3). For the coils treatment, the pooled weighted mean differences (WMD) in ΔFEV1 was 7.31% (95% CI = 4.65 – 9.97, p < 0.00001, I2 = 0%), in Δ6MWT was 31.72m (95% CI = 4.95 – 58.49, p = 0.02, I2 = 71%), in ΔSGRQ was -9.16 points (95% CI =-11.64 – -6.68, p < 0.00001, I2 = 0%) and in mMRC was -0.36 point (95% CI = -0.69 – -0.03, p = 0.03, I 2 = 0%) changed from baseline, compared with conventional therapy. Similarly, EBV therapy was associated with significant improvement in ΔFEV1 (WMD = 11.44%, 95% CI = 6.11 – 16.77, p < 0.0001, I2 = 57%), in Δ6WMT (WMD = 33.86m, 95% CI = 11.54 – 56.19, p = 0.003, I2 = 76%), and in ΔSGRQ (WMD = -7.06 points, 95% CI = -10.71 – -3.41, p = 0.0001, I2 = 63%), in ΔmMRC (WMD = -0.35 point, 95% CI = -0.56 – -0.14, p = 0.0008, I2 = 30%). Of note, subgroup analysis showed that EBV treatment is more effective in patients with complete fissures. Furthermore, we compared the roles of coils treatment between heterogeneous and homogeneous emphysema, and no significant differences were detected. However, IBV group failed to show superior to conventional group.
Table 3: Meta-analysis of bronchoscopic lung volume reduction (BLVR) therapy for severe emphysema
Study group or subgroup |
Outcomes |
Heterogeneity |
Pooled results |
||
|---|---|---|---|---|---|
|
|
Ph |
I2 (%) |
Effect (95%CI) |
P value |
Coils group VS conventional group |
ΔFEV1 (%) |
0.38 |
0 |
WMD 7.31 (4.65 to 9.97) |
p < 0.00001 |
|
Δ6MWT (m) |
0.03 |
71 |
WMD 31.72 (4.95 to 58.49) |
p = 0.02 |
|
ΔSGRQ (points) |
0.86 |
0 |
WMD -9.16 (-11.64 to -6.68) |
p < 0.00001 |
|
ΔmMRC (points) |
0.48 |
0 |
WMD -0.36 (-0.69 to -0.03) |
p = 0.03 |
Coils group between heterogeneous and homogeneous emphysema |
ΔFEV1 (%) |
0.39 |
0 |
WMD 0.63 (-5.00 to 6.26) |
p = 0.83 |
|
Δ6MWT (m) |
0.83 |
0 |
WMD 4.78 (-15.11 to 24.68) |
p = 0.64 |
|
ΔSGRQ (points) |
0.93 |
0 |
WMD -1.25(-4.89 to 2.38) |
p = 0.50 |
|
ΔmMRC (points) |
None |
None |
None |
None |
EBV group VS conventional group |
ΔFEV1 (%) |
0.05 |
57 |
WMD 11.44 (6.11 to 16.77) |
p < 0.0001 |
|
Δ6MWT (m) |
0.003 |
76 |
WMD 33.86 (11.54 to 56.19) |
p = 0.003 |
|
ΔSGRQ (points) |
0.03 |
63 |
WMD -7.06 (-10.71 to -3.41) |
p = 0.0001 |
EBV group VS conventional group (complete tissue or low collateral ventilation) |
ΔmMRC (points) |
0.23 |
30 |
WMD -0.35 (-0.56 to -0.14) |
p = 0.0008 |
|
ΔFEV1 (%) |
0.97 |
0 |
WMD 17.50 (11.86 to 23.13) |
p < 0.00001 |
|
Δ6MWT (m) |
0.10 |
58 |
WMD 50.17 (25.04 to 75.29) |
p < 0.0001 |
|
ΔSGRQ (points) |
0.16 |
42 |
WMD -8.55 (-12.83 to -4.26) |
p < 0.0001 |
|
ΔmMRC (points) |
None |
None |
None |
None |
IBV group VS conventional group |
ΔFEV1 (%) |
None |
None |
None |
None |
|
Δ6MWT (m) |
0.48 |
0 |
WMD -18.77 (-35.27 to -2.28) |
p = 0.03 |
|
ΔSGRQ (points) |
0.24 |
28 |
WMD 2.30 (-1.50 to 6.11) |
p = 0.24 |
|
ΔmMRC (points) |
0.71 |
0 |
WMD -0.08 (-0.29 to 0.13) |
p = 0.47 |
Coils = endobronchial coils, EBV = endobronchial valves (Zephyr), IBV = intrabronchial valve (Spiration), WMD = weighted mean difference, FEV1 = forced expiratory volume in 1s, 6MWT = 6-min walk test, SGRQ = St. George’s Respiratory Questionnaire, mMRC = modified Medical Research Council, Ph = P values for heterogeneity of Q test, CI = confidence interval.
The usual severe adverse effects related were deaths, pneumonia, pneumothorax, hemoptysis, and COPD exacerbation required hospitalization. Table 4 suggested that the coils treatment did not show more significant adverse effect on deaths, COPD exacerbation with hospitalization, or hemoptysis, but had higher incidence of pneumonia or pneumothorax than conventional treatment.
Table 4: Meta-analysis of safety comparing bronchoscopic lung volume reduction (BLVR) with conventional therapy on the major complications
Study group |
Outcomes |
Heterogeneity |
Pooled results |
||
|---|---|---|---|---|---|
|
|
Ph |
I2 (%) |
Effect (95%CL) |
P value |
Coils group VS conventional group |
Deaths |
0.94 |
0 |
RR 1.27 (0.59 to 2.72) |
p = 0.54 |
|
COPD exacerbation with hospitalization |
0.95 |
0 |
RR 1.29 (0.81 to 2.05) |
p = 0.28 |
|
Pneumonia |
0.98 |
0 |
RR 4.42 (2.20 to 8.88) |
p < 0.00001 |
|
Pneumothorax |
0.54 |
0 |
RR 8.17 (2.22 to 30.03) |
p = 0.002 |
|
Hemoptysis |
0.61 |
0 |
RR 5.98 (0.73 to 49.25) |
p = 0.10 |
EBV group VS conventional group |
Deaths |
0.71 |
0 |
RR 1.56 (0.47 to 5.18) |
p = 0.47 |
|
COPD exacerbation with hospitalization |
0.53 |
0 |
RR 2.01 (1.19 to 3.40) |
p = 0.01 |
|
Pneumonia |
0.73 |
0 |
RR 2.17 (0.86 to 5.49) |
p = 0.10 |
|
Pneumothorax |
0.65 |
0 |
RR 9.65 (3.04 to 30.60) |
p = 0.0001 |
|
Hemoptysis |
0.43 |
0 |
RR 6.42 (1.21 to 34.01) |
p = 0.03 |
IBV group VS conventional group |
Deaths |
0.73 |
0 |
RR 4.78 (0.84 to 27.31) |
p = 0.08 |
Coils = endobronchial coils, EBV = endobronchial valves (Zephyr), IBV = intrabronchial valve (Spiration), Ph = P values for heterogeneity of Q test, CI = confidence interval, RR = risk ratio.
For EBV, we detected no between-group difference in deaths and pneumonia, compared with conventional treatment. However, pneumothorax, hemoptysis, or COPD exacerbation occurred more frequently in the EBV group. For IBV, there is no significant difference on deaths with conventional group.
DISCUSSION
COPD is a progressive disease characterised by the permanent hyperinflation and decreased elasticity of air spaces distal to the terminal bronchioles. BLVR consists of the steps of introducing a bronchoscope into the airway to a position close to the damaged lung and equilibrates air within the damaged section with atmospheric air, thus ultimately deflating the hyperinflation of target lung tissue. BLVR is of great importance in the treatment of severe emphysema, particularly for the patients who are unresponsive to medical therapy and do not meet the criteria for LVRS.
The major findings of this systematic review and meta-analysis can be summarized as follows: 1) Compared with conventional therapy, endobronchial coils or EBV treatment provided obvious clinical benefits, with significant improvement in exercise capacity, quality of life, and pulmonary function in patients with severe emphysema, while no significant improvement was detected in IBV treatment. In addition, the absolute change in mMRC, below the defined MCID, indicated that coils or EBV play a significant but moderate role in improving dyspnea. 2) Subgroup analysis regarding efficacy showed no difference between homogeneous and heterogeneous emphysema in coils group. 3) There was no difference in deaths in the coils group or EBV group VS the conventional care group, but other serious adverse events occurred more frequently in the coils or EBV group.
Differences between the previous and present meta-analyses should be noted. A meta-analysis by Iftikhar showed efficacy in BLVR group, while only pooled the mean change post-intervention [9]. After that, two meta-analyses regarding EBV concluded that EBV treatment was associated with superior efficacy compared with conventional treatments, but the conclusion was limited by only two RCTs included [10, 26]. Meanwhile, all of the above studies did not analyze the MCID, which indicates minimal clinical benefits. A more recent meta-analysis also showed the clinical benefits of coils or EBV treatment in patients with advanced emphysema, but the results were based on the mean change from baseline in treatment group, without the comparison with conventional treatment [11]. Furthermore, all the previous meta-analyses did not include new high-quality published data, and some pooled RCTs, observation, or case-report data together, probably threatening the authenticity of their findings.
The highlighted strength of our systematic review and meta-analysis were as follows: 1) the present study included new recently published data and all included studies were the randomized controlled trials, limiting the confounding by indication and selection bias. 2) The analysis focused on the comparative efficacy between the coils or valves treatment and conventional treatment. 3) We analyzed the efficacy of responder for MCID, and also the difference between heterogeneous and homogeneous emphysema in coils group, which were more comprehensive.
Endobronchial valves are placed to block air from entering selective pulmonary lobe that may improve lung function and exercise tolerance. Valves have two devices, EBV and IBV, the efficacy of which are different. In this analysis, compared with conventional treatment, EBV treatment provided, while IBV treatment failed to achieve, significant improvements in patients with severe emphysema. The current meta-analysis also revealed that EBV treatment led to clinically meaningful improvements in pulmonary function, quality of life, and exercise capacity. Nowadays, patients with complete fissures might be considered for treatment with EBV and our analysis also suggests that EBV could show better outcomes in patients with intact fissures. Some authors have suggested that a greater response to EBV treatment is associated with heterogeneous emphysema and EBV should be considered for patients with heterogeneous emphysema, but recently, IMPACT trial [15] demonstrated clinically meaningful benefits in selected patients with homogeneous emphysema without collateral ventilation. It should be noted that emphysema heterogeneity is quantified by visually scoring CT scans and there is no consensus for defining heterogeneity [27]. Further studies to investigate the effect of EBV treatment in homogeneous emphysema are still needed.
Two RCTs were included to compare intrabronchial valves with standard medical care. For the IBV, there was no significant difference in mortality with conventional care. However, IBV failed to show a direct effect on lung function and exercise capacity, which is associated with different approach of intrabronchial valves placement. Also, the two studies selected patients only with upper lobe predominant emphysema and did not aim at achieving lobar occlusion, which may affect the results. Although previous RCTs did not achieve meaningful results, the IBV treat remains a promising treatment for selected patients with low collateral ventilation and complete occlusion of a single lobe [16], and the other two RCTs (NCT01812447, NCT01812447) for heterogeneous emphysema are ongoing, which may alter the present results.
Shape-memory nitinol coils are bronchoscopically designated to induce parenchymal compression, enhance lung recoil, and thus improve ventilator function. Our data suggested that coils treatment showed clinically meaningful benefits and statistically absolute change in 6MWT, and SGRQ in patients with severe emphysema, compared with conventional therapy. However, FEV1 showed a statistically absolute improvement of 7.31%, below the defined MCID. The variance in the baseline level and ceiling effect may limit the response of the FEV1 measurement and the results needs to be interpreted with caution. Further subgroup analysis showed that there were no significant differences in absolute change of FEV1, 6MWT, and SGRQ between heterogeneous emphysema and homogeneous emphysema. Thus, the efficacy of coils treatment is independent of heterogeneous emphysema and could be applied in homogeneous emphysema. Of note, LVRS or EBV treatment for patients with homogenous emphysema is debatable, although good results were published [15, 28, 29]. So, coils treatment may be more suited to homogeneous emphysema.
Compare with conventional treatment, endobronchial coils or valves treatment did not increase the mortality rate. But coils was accompanied by higher rate of pneumonia, pneumothorax, and the increase in pneumothorax, hemoptysis, and COPD exacerbation were associated with the EBV. Most of serious complications occurred early and much less frequently afterwards, which could be cured by common therapy. Thus, due to the low morbidity rate and acceptable side effects, endobronchial coils or EBV treatment is more opted for severe emphysema than LVRS.
There was higher heterogeneity in outcomes especially in the EBV treatment. Sciurba et al. [24] have reported that emphysema heterogeneity and fissure completeness were associated with an enhanced response to EBV treatment. Different types emphysema included in EBV studies may cause high degree of heterogeneity. Other reasons for heterogeneity may be the variance in the measure and baseline characters, and high risk of bias in performance bias, and so on.
Unfortunately, bronchial vapor ablation, lung sealants and airway bypass had to be excluded for only 1 RCT included. The study by Come et al [14] showed that lung sealants were more efficacious in FEV1, 6WMT and SGRQ than conventional treatments, but accompanied with more adverse events that required hospitalization. Of note, early termination of this study, and subsequently the lower number of patients and short follow-up made the results less convincing. STEP-UP trial [13], comparing bronchial vapor ablation to standard medical treatments, selected patients with severe upper lobe-predominant emphysema. In this study, bronchial vapor ablation achieved clinically meaningful and statistically significant improvements in FEV1 and SGRQ at 6 months, with an acceptable safety profile. But, 6WMT could not be assessed for the lack of change in baseline numbers. EASE trial showed that airway bypass resulted in acute reduction in regional air trapping in patients with severe homogeneous emphysema, but failed to sustain long-term benefits. There was no significant between-group difference on adverse events.
There were also potential limitations that should be taken into consideration for this analysis. Firstly, the durations of follow-up in included trials were different and the results were varying, which may cause the fading of the effect or true differences. Meanwhile, the long-term data were scarce, and the assessments of most studies were limited to 12 months. Thus, the efficacy and safety of coils or valves on long-term lung function, exercise tolerance, and quality of life improvement are not certain. Moreover, some values were presented as MEAN (95% CI). We pooled theses values by converting mean (95% CI) to MEAN ± SD, and the follow-up term of some RCTs was variant, which might lead to high degree of heterogeneity and misleading conclusion. Thirdly, the random-effects modeling was used because of the significant heterogeneity in some analyses, which might affect the results of the present study.
Despite these limitations, this meta-analysis reinforced the results that endobronchial coils and EBV treatment were superior to conventional treatment in patients with severe emphysema, and did not increase deaths rate, but associated with some serious adverse effects. Further long-term follow up is needed to assess efficacy and safety on health outcomes.
MATERIALS AND METHODS
Search strategy
A comprehensive search was conducted including PubMed, Embase and the Cochrane Library. The following search strategies were used: “bronchoscopic lung volume reduction”, “BLVR”, “endobronchial coils”, “endobronchial coil”, “endobronchial valves”, “endobronchial valve”, “intrabronchial valves”, “intrabronchial valve”, “bronchial vapor ablation”, “vapor ablation”, “lung sealants”, “lung sealant”, or “airway bypass”. We reviewed the full-text articles designated for inclusion. In addition, we also manually searched the reference of the included studies and published reviews.
Study selection
As observational studies are highly liable to confound by indication and selection bias, we only included studies that were randomized controlled trial (published in English), comparing BLVR to medical therapy, and the population was emphysema patients. Included studies should report adverse effects, and any or all of the following outcomes: (1) FEV1; (2) 6MWT; (3) SGRQ; (4) SGRQ. Meta-analyses were carried out only when included RCTs ≥ 2 trials.
Assessment of risk of bias
Two authors independently assessed the risk of bias of RCTs based upon The Cochrane Collaboration tool [30]. The following domains were evaluated: selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias. Studies were independently assessed by two reviewers, and were divided into three categories: (1) low risk of bias; (2) unclear risk of bias; (3) high risk of bias, for one or more key domains.
Data extraction and statistical analysis
Data were extracted using a standard collection form. Information from each study including author names, year of publication, number of patients, intervention, control, outcomes, and adverse effect were extracted by two independent reviewers. If several studies reported the same patients, we chose the largest study to avoid the duplication. If some studies reported the results at different follow up time point, we chose the available data at the longest time point. Discrepancies were resolved through team consensus.
MCID is the smallest change in an outcome that a patient would benefit [31], and offers a threshold above which outcome is experienced as relevant by the patient, avoiding the problem of mere statistical significance. So, we took the proportion of patients who reached MCID as the primary outcome, and the MCID was determined as follows: ΔFEV1 ≥ 10% [32], Δ6MWT ≥ 26 meters [33], ΔSGRQ ≥ 4 points [34], and ΔmMRC ≥ 1 point [35]. Secondary outcome was an absolute change from baseline in FEV1, 6MWT, SGRQ and mMRC. Severe common adverse effects related were deaths, pneumonia, pneumothorax, hemoptysis, and COPD exacerbation required hospitalization.
Dichotomous outcomes data were compared by RR with 95% CI and WMD were also calculated for continuous outcomes. Heterogeneity was tested with the I2 statistic. I2 values of 50% ~ 75% or 75% ~ 100% were considered to have moderate or high heterogeneity, respectively. The fixed-effects modeling was used, but if heterogeneity was significant (I2 > 50%), the random-effects modeling was carried out [36]. All statistical analyses were performed by using RevMan version 5.3 (The Nordic Cochrane Center). P-values < 0.05 was considered statistically significant.
Abbreviations
BLVR = bronchoscopic lung volume reduction; RCT = randomized controlled trial; EBV = endobronchial valves; IBV = intrabronchial valves; MCID = minimal clinically important difference; FEV1 = forced expiratory volume in 1s; 6MWT = 6-min walk test; SGRQ = St. George’s Respiratory Questionnaire; COPD = chronic obstructive pulmonary disease; LVRS = lung-volume-reduction surgery; RR = risk ratio; CI = confidence interval; WMD = weighted mean differences; NR = not reported; Ph= p values for heterogeneity of Q test.
Author contributions
Z.C. and Y.W. takes responsibility for the integrity of this study; Z.C. and H.-H.S. designed and supervised the study; Y.W.,T.W.L. and F.X. contributed to the study design, data acquisition and interpretation; Z.C. and Y.W. drafted manuscript; J-S.Z., Z-Y.L., X-C.X., H-P.C., S-M.Y., Z.C., W.L., and H.-H.S. analyzed data and revised manuscript. All authors approved the final manuscript.
All authors are aware of and agree to the content of the paper and their being listed as an author. There are no potential conflicts of interest exist with any companies/organizations whose products or services may be discussed in this article.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
GRANT SUPPORT
This work was supported by the General Projects (81370142 and 81670031 to Z.H. Chen) from the National Natural Science Foundation of China, the Key Science-Technology Innovation Team of Zhejiang Province (2011R50016), and project from the National Clinical Research Center of China for Respiratory Disease.
REFERENCES
1. Pauwels R, Rabe K. Burden and clinical features of chronic obstructive. Lancet. 2004; 364:613-620.
2. Vestbo J, Hurd S, Agustí A, Jones P, Vogelmeier C, Anzueto A, Barnes P, Fabbri L, Martinez F, Nishimura M, Stockley R, Sin D, Rodriguez-Roisin R. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease GOLD executive summary. Am J Respir Crit Care Med. 2013; 187:347-365.
3. Kelly J, Bamsey O, Smith C, Lord V, Shrikrishna D, Jones P, Polkey M, Hopkinson N. Health status assessment in routine clinical practice: the chronic obstructive pulmonary disease assessment test score in outpatients. Respiration. 2012; 84:193-199.
4. Fishman A, Martinez F, Naunheim K, Piantadosi S, Wise R, Ries A, Weinmann G, Wood D; National Emphysema Treatment Trial Research Group. A randomized trial comparing lung-volume–reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003; 348:2058-2073.
5. van Agteren JE, Carson K, Tiong L, Smith B. Lung volume reduction surgery for diffuse emphysema. Cochrane Database Syst Rev. 2016; 10:CD001001. https://doi.org/10.1002/14651858.CD001001.pub3.).
6. Naunheim K, Wood D, Krasna M, DeCamp MJ, Ginsburg M, McKenna RJ, Criner G, Hoffman E, Sternberg A, Deschamps C; National Emphysema Treatment Trial Research Group. Predictors of operative mortality and cardiopulmonary morbidity in the National Emphysema Treatment Trial. J Thorac Cardiovasc Surg. 2006; 131:43-53.
7. Cohen E. Bronchoscopic treatment of end-stage chronic obstructive pulmonary disease. Curr Opin Anaesthesiol. 2014; 27:36-43.
8. Herth F, Gompelmann D, Ernst A, Eberhardt R. Endoscopic lung volume reduction. Respiration. 2010; 79:5-13.
9. Iftikhar I, McGuire F, Musani A. Efficacy of bronchoscopic lung volume reduction: a meta-analysis. Int J Chron Obstruct Pulmon Dis. 2014; 9:481-491.
10. Liu H, Xu M, Xie Y, Gao J, Ni S. Efficacy and safety of endobronchial valves for advanced emphysema: a meta analysis. J Thorac Dis. 2015; 7:320-328.
11. Kumar A, Dy R, Singh K, Jeffery MM. Early trends in bronchoscopic lung volume reduction: a systematic review and meta-analysis of efficacy parameters. Lung. 2016:1-10.
12. Shah P, Slebos D, Cardoso P, Cetti E, Voelker K, Levine B, Russell M, Goldin J, Brown M, Cooper J, Sybrecht G; EASE trial study group. Bronchoscopic lung-volume reduction with Exhale airway stents for emphysema (EASE trial): randomised, sham-controlled, multicentre trial. Lancet. 2011; 378:997-1005.
13. Herth F, Valipour A, Shah P, Eberhardt R, Grah C, Egan J, Ficker J, Wagner M, Witt C, Liebers U, Hopkins P, Gesierich W, Phillips M, et al. Segmental volume reduction using thermal vapour ablation in patients with severe emphysema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med. 2016; 4:185-193.
14. Come C, Kramer M, Dransfield M, Abu-Hijleh M, Berkowitz D, Bezzi M, Bhatt S, Boyd M, Cases E, Chen A, Cooper C, Flandes J, Gildea T, et al. A randomised trial of lung sealant versus medical therapy for advanced emphysema. Eur Respir J. 2015; 46:651-662.
15. Valipour A, Slebos D, Herth F, Darwiche K, Wagner M, Ficker J, Petermann C, Hubner R, Stanzel F, Eberhardt R; IMPACT Study Team. Endobronchial valve therapy in patients with homogeneous emphysema. Am J Respir Crit Care Med. 2016; 194:1073-1082.
16. Wood D, Nader D, Springmeyer S, Elstad M, Coxson H, Chan A, Rai N, Mularski R, Cooper C, Wise R, Jones P, Mehta A, Gonzalez X, et al. The IBV Valve trial: a multicenter, randomized, double-blind trial of endobronchial therapy for severe emphysema. J Bronchology Interv Pulmonol. 2014; 21:288-297.
17. Valipour A, Herth F, Burghuber O, Criner G, Vergnon J, Goldin J, Sciurba F, Ernst A; VENT Study Group. Target lobe volume reduction and COPD outcome measures after endobronchial valve therapy. Eur Respir J. 2014; 43:387-396.
18. Davey C, Zoumot Z, Jordan S, McNulty W, Carr D, Hind M, Hansell D, Rubens M, Banya W, Polkey M, Shah P, Hopkinson N. Bronchoscopic lung volume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR-HIFi study): a randomised controlled trial. Lancet. 2015; 386:1066-1073.
19. Deslée G, Mal H, Dutau H, Bourdin A, Vergnon J, Pison CK, Kessler R, Jounieaux V, Thiberville L, Leroy S, Marceau A, Laroumagne S, Mallet J, et al. Lung volume reduction coil treatment vs usual care in patients with severe emphysema: the REVOLENS randomized clinical trial. JAMA. 2016; 315:175-184.
20. Herth F, Noppen M, Valipour A, Leroy S, Vergnon J, Ficker J, Egan J, Gasparini S, Agusti C, Holmes-Higgin D, Ernst A; International VENT Study Group. Efficacy predictors of lung volume reduction with Zephyr valves in a European cohort. Eur Respir J. 2012; 39:1334-1342.
21. Klooster K, ten Hacken N, Hartman J, Kerstjens H, van Rikxoort E, Slebos D. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med. 2015; 373:2325-2335.
22. Ninane V, Geltner C, Bezzi M, Foccoli P, Gottlieb J, Welte T, Seijo L, Zulueta J, Munavvar M, Rosell A, Lopez M, Jones P, Coxson H, et al. Multicentre European study for the treatment of advanced emphysema with bronchial valves. Eur Respir J. 2012; 39:1319-1325.
23. Sciurba F, Criner G, Strange C, Shah P, Michaud G, Connolly T, Deslée G, Tillis W, Delage A, Marquette C, Krishna G, Kalhan R, Ferguson J, et al. Effect of endobronchial coils vs usual care on exercise tolerance in patients with severe emphysema: the RENEW Randomized Clinical Trial. JAMA. 2016; 315:2178-2189.
24. Sciurba F, Ernst A, Herth F, Strange C, Criner G, Marquette C, Kovitz K, Chiacchierini R, Goldin J, McLennan G; VENT Study Research Group. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010; 363:1233-1244.
25. Shah P, Zoumot Z, Singh S, Bicknell S, Ross E, Quiring J, Hopkinson N, Kemp S; RESET Trial Study Group. Endobronchial coils for the treatment of severe emphysema with hyperinflation (RESET): a randomised controlled trial. Lancet Respir Med. 2013 1:233-40; 1:233-240.
26. Choi M, Lee W, Lee M, Jeon K, Sheen S, Jheon S, Kim Y. Effectiveness of bronchoscopic lung volume reduction using unilateral endobronchial valve: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015; 10:703-710.
27. Valipour A, Shah PL, Gesierich W, Eberhardt R, Snell G, Strange C, Barry R, Gupta A, Henne E, Bandyopadhyay S, Raffy P, Yin Y, Tschirren J, Herth FJ. Patterns of emphysema heterogeneity. Respiration. 2015; 90:402-411.
28. Weder W, Tutic M, Lardinois D, Jungraithmayr W, Hillinger S, Russi E, Bloch K. Persistent benefit from lung volume reduction surgery in patients with homogeneous emphysema. Ann Thorac Surg. 2009; 87:229-237.
29. Shah P, Herth F, van GW, Deslee G, Slebos D. Lung volume reduction for emphysema. Lancet Respir Med. 2016; 4:e55.
30. Higgins J, Altman D, Gøtzsche P, Jüni P, Moher D, Oxman A, Savovic J, Schulz K, Weeks L, Sterne J; Cochrane Bias Methods Group and Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011; 343:d5928.
31. Jaeschke R, Singer J, Guyatt G. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989; 10:407-415.
32. Donohue JF. Minimal clinically important differences in COPD lung function. COPD. 2005; 2:111-124.
33. Puhan M, Chandra D, Mosenifar Z, Ries A, Make B, Hansel N, Wise R, Sciurba F; National Emphysema Treatment Trial (NETT) Research group. The minimal important difference of exercise tests in severe COPD. Eur Respir J. 2011; 37:784-790.
34. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2009; 2:75-79.
35. Cazzola M, MacNee W, Martinez FJ, Rabe KF, Franciosi LG, Barnes PJ, Brusasco V, Burge PS, Calverley PM, Celli BR, Jones PW, Mahler DA, Make B, et al. Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J. 2008; 31:416-469.
36. Higgins J, Thompson S, Deeks J, Altman D. Measuring inconsistency in meta-analyses. BMJ. 2003; 327:557-560.