
INTRODUCTION
Hepatitis C virus (HCV) is an important pathogen affecting approximately 130–150 million people worldwide [1, 2]. Chronic hepatitis C (CHC) patients have enhanced risk of cirrhosis and hepatocellular carcinoma [3, 4]. The emergence of direct-acting antivirals (DAAs) has revolutionized the treatment of HCV with shorter treatment durations, higher sustained virological response (SVR) rates, fewer adverse events (AEs) and fewer contraindications than those of traditional peginterferon and ribavirin (PegIFN/RBV, PR) treatment regimens [5–8].
With the wide application of DAAs, challenging issues regarding the efficacy and safety of new DAAs regimens have arisen, e.g., resistance-associated variants, drug-drug interactions (DDIs), HBV (hepatitis B virus) reactivation, hepatotoxicity and nephrotoxicity [9–20]. In October 2016, the United States Food and Drug Administration issued a black box warning regarding the risk for HBV activation with 9 DAAs, citing 24 cases that included 3 reports of acute liver failure (https://www.fda.gov/). The Institute for Safe Medicine Practices followed up with a review of Adverse Event Reporting System data covering a 12-month span. The review uncovered 524 cases of liver failure associated with DAAs and that 31.5% of the patients had died at the time of the review (http://www.ismp.org/default.asp). Traditional PR treatment regimens and first-generation protease inhibitors are considered nephrotoxic [21, 22]. Although all-oral DAAs regimens were well tolerated in clinical trials, recent real-world studies demonstrated some cases with nephrotoxicity that were treated with sofosbuvir (SOF)-containing regimens [18–20]. Some cases with hepatotoxicity and nephrotoxicity associated with DDIs were reported in CHC patients with concomitant diseases, HBV or HIV co-infections, and liver transplantations [11, 14, 16, 17].
Considering the increasing occurrence of cases with hepatotoxicity, nephrotoxicity, and DDIs, this study aimed to explore the changes of hepatic and renal function indices in CHC patients treated with DAAs.
RESULTS
Baseline characteristics and treatment efficacy
The main demographic, virological and clinical characteristics are described in Table 1. Of the 43 patients, 51.2% were more than 60 years old, with a mean age of 57.9 ± 15.7 years; 55.8% were male; 46.5% were PR treatment experienced; and 41.9% had cirrhosis. The mean values for estimated glomerular filtration rate (eGFR), serum creatinine (Scr) and uric acid (UA) were 86.7 ± 20.4 ml/min/1.73 m2, 83.9 ± 19.1 μmol/L, and 323.7 ± 86.2 μmol/L, respectively. Compared with non-cirrhotic patients, cirrhotic patients had higher PR treatment-experience rates (24% vs 77.8%, P = 0.001), mean liver stiffness measurement (LSM) scores (8.0 ± 3.7 vs 29.9 ± 14.6, P < 0.001), and aminotransferase (AST) levels (41.6 ± 24.2 vs 69.4 ± 34.4, P = 0.003) and lower platelet (PLT) counts (179.2 ± 61.5 vs 92.1 ± 31.7, P < 0.001). Other baseline characteristics did not differ significantly between non-cirrhotic patients and cirrhotic patients (Table 1). One patient discontinued the SOF/daclatasvir (DAC) treatment 8 w after the initiation of the treatment due to the development of renal area pain; all other patients completed the treatment and follow-up. A total of 97.7% (42/43) of the patients achieved SVR at 12 w post-treatment (SVR 12); one non-cirrhotic patient treated with SOF/ledipasvir (LDV) still had a detectable HCV RNA at the end of treatment.
Table 1: Baseline characteristics of enrolled patients
Characteristics |
All (n = 43) |
non-Cirrhotic (n1 = 25) |
Cirrhotic (n2 = 18) |
P(n1 vs n2) |
|---|---|---|---|---|
Age (mean) |
57.9 ± 15.7 |
54.9 ± 17.7 |
62.1 ± 11.8 |
NS |
Age (> 60 years) |
22 (51.2%) |
10 (40%) |
12 (66.7%) |
NS |
Male |
24 (55.8%) |
15 (60%) |
9 (50%) |
NS |
HCV RNA log10 (IU/ml) |
6.64 ± 0.87 |
6.81 ± 0.59 |
6.40 ± 1.13 |
NS |
PR (experienced) |
20 (46.5%) |
6 (24%) |
14 (77.8%) |
0.001 |
LSM (kPa) |
17.2 ± 14.6 |
8.0 ± 3.7 |
29.9 ± 14.6 |
< 0.001 |
ALT (IU/L) |
57.8 ± 38.1 |
54.0 ± 40.5 |
63.2 ± 35.0 |
NS |
AST (IU/L) |
53.2 ± 31.8 |
41.6 ± 24.2 |
69.4 ± 34.4 |
0.003 |
PLT (109/L) |
142.7 ± 66.8 |
179.2 ± 61.5 |
92.1 ± 31.7 |
< 0.001 |
eGFR(ml/min/1.73 m2) |
86.7 ± 20.4 |
88.4 ± 21.7 |
84.3 ± 18.7 |
NS |
Scr (μmol/L) |
83.9 ± 19.1 |
84.4 ± 20.4 |
83.2 ± 17.7 |
NS |
UA (μmol/L) |
323.7 ± 86.2 |
318.7 ± 83.9 |
330.7 ± 91.2 |
NS |
BUN (mmol/L) |
5.23 ± 1.46 |
4.97 ± 1.27 |
5.60 ± 1.67 |
NS |
NS: no significance.
Changes of hepatic function indices
The mean aminotransferase (ALT) and AST levels at the end of treatment and at 24 w post-treatment were significantly decreased compared with the baseline levels (ALT: 57.8 ± 38.1 vs 19.8 ± 14.2, P01 < 0.001; 57.8 ± 38.1 vs 17.3 ± 6.8, P02<0.001; AST: 53.2 ± 31.8 vs 24.4 ± 9.9, P01 < 0.001; 53.2 ± 31.8 vs 22.7 ± 6.9, P02 < 0.001) (Table 2), whereas one decompensated cirrhotic patient (LSM = 41.2 kPa, mild ascites) treated with SOF/LDV developed a liver injury at the end of treatment (ALT = 101 IU/L; AST = 72 IU/L). A 53-year-old female patient was hospitalized with a persistent low-grade fever, fatigue and sleepiness on January 22nd, 2016. The baseline ALT and AST levels were within the normal ranges and there was neither alcohol use nor concomitant medications during the SOF/LDV treatment. Silymarin capsules (MADAUS GmbH, Germany) were prescribed for two weeks (140 mg/bid), and ALT and AST levels were kept in normal ranges until 24 weeks post-treatment (Figure 1). Along with the recovery of the liver function, the PLT count at 24 w post-treatment was significantly increased compared with the PLT count at baseline (142.7 ± 66.8 vs 148.8 ± 67.4, P01 = 0.112; 142.7 ± 66.8 vs 155.7 ± 66.9, P02 < 0.01) (Table 2).
Table 2: Changes of hepatic and renal function indices among different time points
T0 |
T1 |
T2 |
P01 |
P02 |
PDAAs*Time |
|
|---|---|---|---|---|---|---|
ALT (IU/L) |
57.8 ± 38.1 |
19.8 ± 14.2 |
17.3 ± 6.8 |
< 0.001 |
< 0.001 |
NS |
AST (IU/L) |
53.2 ± 31.8 |
24.4 ± 9.9 |
22.7 ± 6.9 |
< 0.001 |
< 0.001 |
NS |
PLT (109/L) |
142.7 ± 66.8 |
148.8 ± 67.4 |
155.7 ± 66.9 |
NS |
0.003 |
NS |
eGFR(ml/min/1.73 m2) |
86.7 ± 20.4 |
80.5 ± 21.3 |
81.4 ± 18.6 |
0.005 |
0.013 |
NS |
Scr (μmol/L) |
83.9 ± 19.1 |
89.6 ± 21.1 |
87.9 ± 18.3 |
< 0.001 |
0.014 |
NS |
UA (μmol/L) |
323.7 ± 86.2 |
358.5 ± 93.2 |
349.3 ± 91.0 |
< 0.001 |
0.004 |
NS |
BUN (mmol/L) |
5.23 ± 1.46 |
5.29 ± 1.53 |
5.72 ± 1.81 |
NS |
0.017 |
NS |
T0: baseline; T1: end of treatment; T2: 24 w after the end of treatment. P01: significance of difference between T0 and T1; P02: significance of difference between T0 and T2; PDAAs*Time: interactive effects of DAAs regimens and time points on the changes of renal function indices. NS: no significance.
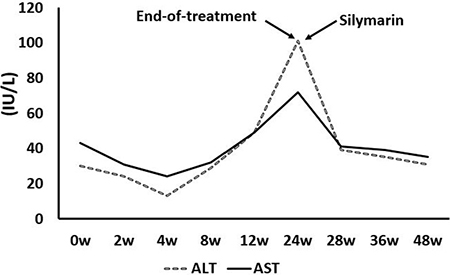
Figure 1: One decompensated cirrhotic patient with liver injury associated with treatment with DAAs.
Changes in renal function indices
At the end of treatment, the eGFR level was significantly decreased and the Scr and UA levels were significantly increased compared with baseline levels (eGFR: 86.7 ± 20.4 vs 80.5 ± 21.3, P01 = 0.005; Scr: 83.9 ± 19.1 vs 89.6 ± 21.1, P01 < 0.001; UA: 323.7 ± 86.2 vs 358.5 ± 93.2, P01 < 0.001), and no significant improvements were observed at 24 w post-treatment (eGFR: 86.7 ± 20.4 vs 81.4 ± 18.6, P02 = 0.013; Scr: 83.6 ± 17.9 vs 87.9 ± 18.3, P02 = 0.014; UA: 320.8 ± 76.3 vs 349.3 ± 91.0, P02 = 0.004). The blood urea nitrogen (BUN) level at the end of treatment showed no significant changes compared with the baseline level, while an increased BUN level was observed 24 w post-treatment (5.23 ± 1.46 vs 5.72 ± 1.81, P02 = 0.017) (Figure 2). The DAAs regimens and the time points had no interactive effects on the changes in renal function indices (PDAAs*Time > 0.05), which indicated that the SOF/DAC and SOF/LDV regimens had the same effects on the changes in renal function indices with main effects (Table 2).
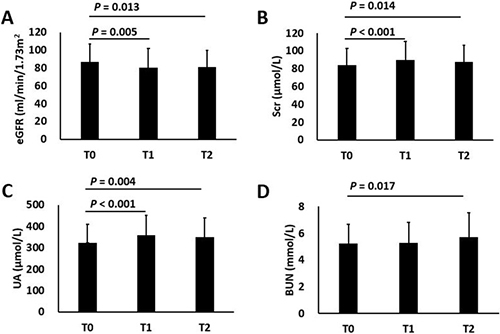
Figure 2: Changes in renal function indices among different observing points. (A) eGFR; (B) Scr; (C) UA; (D) BUN. T0: baseline; T1: end of treatment; T2: 24 w post-treatment. P01: statistical significance of the difference between T0 and T1; P02: statistical significance of the difference between T0 and T2.
Considering the difference in liver conditions and treatment durations, changes in renal function indices were compared between non-cirrhotic patients and cirrhotic patients (Table 3). At the end of treatment, non-cirrhotic patients and cirrhotic patients had decreased eGFR levels and increased Scr levels (non-cirrhotic: 88.4 ± 21.7 vs 81.9 ± 21.4, P01 = 0.046; 84.4 ± 20.4 vs 90.1 ± 22.0, P01 = 0.012; cirrhotic: 84.3 ± 18.7 vs 78.7 ± 21.5, P01 = 0.042; 83.2 ± 17.7 vs 88.9 ± 20.3, P01 = 0.013); at 24 w post-treatment, the eGFR and Scr levels were significantly improved in non-cirrhotic patients (eGFR: 88.4 ± 21.7 vs 83.8 ± 18.5, P02 = 0.142; Scr: 84.4 ± 20.4 vs 87.0 ± 16.9, P02 = 0.088), while no obvious improvements were observed in cirrhotic patients (eGFR: 84.3 ± 18.7 vs 78.1 ± 18.6, P02 = 0.002; Scr: 83.2 ± 17.7 vs 89.2 ± 20.6, P02 = 0.006) (Figure 3). The UA levels at the end of treatment and at 24 w post-treatment were significantly increased compared with baseline levels (non-cirrhotic: 318.7 ± 83.9 vs 355.2 ± 84.4, P01 = 0.001; 318.7 ± 83.9 vs 344.2 ± 92.2, P02 = 0.031; cirrhotic: 330.7 ± 91.2 vs 363.2 ± 106.6, P01 = 0.017; 330.7 ± 91.2 vs 356.5 ± 91.3, P02 = 0.04). The BUN levels in non-cirrhotic and cirrhotic patients had no significant changes across time points (Table 3).
Table 3: Changes of renal function indices in non-cirrhotic and cirrhotic patients
T0 |
T1 |
T2 |
P01 |
P02 |
||
|---|---|---|---|---|---|---|
non-Cirrhotic |
eGFR |
88.4 ± 21.7 |
81.9 ± 21.4 |
83.8 ± 18.5 |
0.046 |
NS |
(N = 25) |
Scr |
84.4 ± 20.4 |
90.1 ± 22.0 |
87.0 ± 16.9 |
0.012 |
NS |
UA |
318.7 ± 83.9 |
355.2 ± 84.4 |
344.2 ± 92.2 |
0.001 |
0.031 |
|
BUN |
4.97 ± 1.27 |
4.97 ± 1.19 |
5.38 ± 1.52 |
NS |
NS |
|
Cirrhotic |
eGFR |
84.3 ± 18.7 |
78.7 ± 21.5 |
78.1 ± 18.6 |
0.042 |
0.002 |
(N = 18) |
Scr |
83.2 ± 17.7 |
88.9 ± 20.3 |
89.2 ± 20.6 |
0.013 |
0.006 |
UA |
330.7 ± 91.2 |
363.2 ± 106.6 |
356.5 ± 91.3 |
0.017 |
0.04 |
|
BUN |
5.60 ± 1.67 |
5.73 ± 1.84 |
6.20 ± 2.11 |
NS |
NS |
T0: baseline; T1: end of treatment; T2: 24 w after the end of treatment. P01: significance of difference between T0 and T1; P02: significance of difference between T0 and T2. NS: no significance.
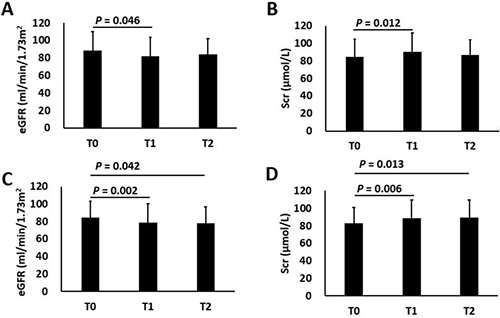
Figure 3: Changes of eGFR and Scr levels in non-cirrhotic and cirrhotic patients. Changes of eGFR (A) and Scr (B) levels in non-cirrhotic patients; Changes of eGFR (C) and Scr (D) levels in cirrhotic patients; T0: baseline; T1: end of treatment; T2: 24 w post-treatment. P01: statistical significance of the difference between T0 and T1; P02: statistical significance of the difference between T0 and T2.
Comorbidities and concomitant medications
A total of 62.7% (27/43) of the patients were found to have comorbidities; the main comorbidities were hypertension (32.6%), hyperlipidemia (16.3%), gastrointestinal diseases (14.0%), diabetes mellitus (11.6%), and thyroid dysfunction (11.6%). A total of 74.4% (32/43) of the patients used at least one concomitant medication; the main medications were antihypertensives (32.6%), antibiotics (23.3%), antipyretic analgesics (20.9%), statins (14.0%), antidiabetics (11.6%), gastro-kinetic agents (11.6%), proton pump inhibitors (9.3%), and hepatoprotectants (9.3%).
DISCUSSION
The availability and rapid development of DAAs has revolutionized the management of CHC and achieved a high SVR rate with a low incidence of AEs. Although DAAs are highly effective and well tolerated, some cases with hepatotoxicity and nephrotoxicity have been reported [14–20]. Thus, this study analyzed the efficacy of DAAs treatment and the effects on hepatic and renal function indices in CHC patients in clinical practice.
In this study, combined DAA therapy achieved a promising SVR rate (97.7%) that was not significantly different from the rates reported in previous studies [23–26]. However, the abnormal changes in renal function indices were unexpected. At the end of treatment, the eGFR level was significantly decreased and the Scr and UA levels were significantly increased; at 24 w post-treatment, non-cirrhotic patients showed improvements, whereas a persistent decrease in eGFR level and increases in Scr and UA levels were observed in cirrhotic patients (Table 2, Table 3). eGFR and Scr were important indices for assessing renal function, and an elevated UA level also predicted a rapid decline in kidney function [27].
Although the specific mechanisms were unknown, possible reasons for the abnormal changes in renal function indices in this study are as follows: (1) Potential DDIs caused by complicated concomitant medication use might be a major reason for the abnormal changes. Each DAA had its own metabolism and potential DDIs [28]; drug metabolic enzymes, such as cytochrome P450 (CYP450); drug transporters, such as P-glycoprotein (P-gp); and breast cancer resistance protein (BCRP) were the most common pathways leading to DDIs. Unlike in clinical trials, concomitant medications that had potential DDIs with DAAs are frequently prescribed to patients with chronic HCV infection in clinical practice [29, 30]. DAAs or concomitant medications could act as substrates, inhibitors and inducers of metabolic enzymes and transporters, leading to an elevated blood drug concentration [31, 32]. In this study, two combined DAAs regimens had the same effects on changes in renal function indices, and we speculated that the SOF use in the two regimens might account for the abnormal changes in renal function indices. SOF is intracellularly metabolized and forms the active metabolite GS-461203 and the inactive compound GS-331007, which is primarily renally excreted; moreover, SOF is a substrate of P-gp and BCRP and is 61–65% bound to plasma proteins [33]. DDIs among SOF, GS-331007 and concomitant medications could cause kidney injury due to increased blood drug concentration, especially when concomitant medications with potential hepatotoxicity and nephrotoxicity are prescribed. (2) High frequencies of comorbidities and concomitant medications in this elderly patients might also contribute to the abnormal changes in renal function indices. This was a relatively elderly cohort; the mean age was 57.9 ± 15.7 years, with 51.2% of the patients were more than 60 years old, and 41.9% of the patients had cirrhosis (Table 1); 62.7% of the patients were found to have comorbidities and 74.4% of the patients had at least one concomitant medication, including antihypertensives (32.6%), antibiotics (23.3%), antipyretic analgesics (20.9%), statins (14.0%), antidiabetics (11.6%), gastro-kinetic agents (11.6%), proton pump inhibitors (9.3%), or hepatoprotectants (9.3%). Recent studies also showed high frequencies of comorbidities and concomitant medications in elderly patients during treatment with DAAs, many of which had potential DDIs with DAAs [34–36]. (3) Cirrhotic patients had persistent abnormal changes in renal function indices. Cirrhotic patients received 24 weeks of combined DAA treatment, and prolonged treatment durations increased the risk of DDIs between DAAs and concomitant medications; the cirrhotic patients were older than the non-cirrhotic patients (Table 1), elderly patients had more concomitant medications, which represented high risks for DDIs [34, 35] and eGFR declined with aging by approximately 1 mL/min/1.73 m2 annually which could result in a decreased renal elimination capacity and increased blood drug concentration of DAAs or concomitant medications [27, 37]; studies using a single 400 mg dose of SOF in patients with renal impairment have shown a significant increase in serum levels of SOF and the metabolite GS331007 compared with levels in patients with normal renal function (eGFR > 80 ml/min/1.73 m2) [33]; cirrhotic patients in this cohorts had relatively lower eGFR levels than non-cirrhotic patients (Table 1), which might result in a decreased renal elimination capacity and the accumulation of SOF and its metabolite GS331007 or concomitant medications; these factors might have jointly contributed to the persistent elevation of Scr and UA levels in cirrhotic patients.
One decompensated cirrhotic patient treated with SOF/LDV was found to have elevated ALT and AST levels, and there were no other virus infections, alcohol use, or concomitant medications (Figure 1). Cirrhosis destroyed the structure and function of the liver, reduced the expression of drug metabolizing enzymes and thus reduced metabolizing capacity, which increased the blood concentration of the drugs metabolized by these enzymes [33, 38]; this might have led to liver injury in the patient with decompensated cirrhosis.
The abnormal changes observed in renal function indices associated with the SOF-containing regimens in this study should be taken as a note of caution. Clinical physicians should closely monitor hepatic and renal function in patients treated with SOF-containing regimens, especially in cirrhotic patients.
MATERIALS AND METHODS
Patients
Forty-three CHC patients who were treated with DAAs while hospitalized in Peking University First Hospital between January 2015 and January 2017 and met the following criteria were enrolled in this study: (1) infected with HCV GT 1b; (2) negative for hepatitis A virus immunoglobulin M (HAV IgM), hepatitis B surface antigen (HBsAg), hepatitis E virus IgM (HEV IgM), human immunodeficiency virus (HIV), Epstein-Barr virus (EBV), and cytomegalovirus (CMV); (3) no severe renal function impairment (eGFR < 30 ml/min/1.73 m2) and end-stage renal disease; (4) no severe heart disease; (5) no active drug use and no alcohol use; (6) no pregnancy; (7) DAAs treatment regimens prescribed according to the recommendation of the new guidelines [39–41]; and (8) clinical information is intact. A total of 31 patients were excluded, including 14 HCV GT2a infected patients, one HBV/HCV co-infected patient, one CMV/HCV co-infected patient, 3 patients with severe renal function damage, one patient treated with DAAs regimens who did not comply with the guidelines, and 11 patients with incomplete clinical information. Of the 43 patients, 18 were treated with SOF (400 mg/day) / DAC (60 mg/day) and 25 were treated with SOF (400 mg/day) / LDV (90 mg/day); non-cirrhotic patients were treated for 12 weeks and cirrhotic patients were treated for 24 weeks. All study participants provided informed written consent prior to enrollment in the study. Ethical approval was given by the Ethics Committee. The study was in compliance with the Helsinki Declaration.
Clinical data collection, HCV RNA quantitation, and genotyping
Hematological, biochemical, and urine tests were performed and recorded at 0 w, 2 w, 4 w, 8 w, 12 w, or 24 w during the DAA treatment, as well as at 4 w, 12 w, and 24 w post-treatment at a clinical laboratory. The virological endpoint was the achievement of SVR 12, and clinical indices at 24 w post-treatment were recorded as clinical endpoints. The ALT, AST and PLT count were used to assess liver function; eGFR, Scr, UA, and BUN were used to assess renal function.
LSMs were measured by transient elastography (Fibroscan, Echosens, Paris), and the presence of cirrhosis was determined by LSM ≥ 17.6 kPa [42–44]. The eGFR was calculated with the Modification of Diet in Renal Disease Study equation adjusted for the Chinese population: eGFR = 175 *(serum creatinine)−1.234 *age−0.179 *0.79 (if female) [45].
HCV RNA quantitation and genotyping were measured at the virus laboratory in the department of infectious disease. Serum HCV RNA quantitation was measured using a COBAS Taqman HCV Test kit (Roche Molecular Systems Inc., Pleasanton, CA, USA); a COBAS AmpliPrep instrument was used for automated specimen processing, and a COBAS Taqman analyzer was used for automated amplification and detection [46]. The detailed detection procedures were performed according to the manufacturer’s instructions. HCV genotypes were determined by restriction fragment length polymorphism (RFLP) analysis of the amplified 5′-noncoding genome region [47]. Detailed procedures were performed according to the following protocol: HCV RNA was extracted from 140 μL serum samples using a QIAamp viral RNA mini kit (Qiagen, Hilden, Germany); reverse transcription and polymerase chain reaction (PCR) amplification were conducted using BG1 (5′-CTGTGAGGAACTACTGTCTT-3′) and BG2 (5′-AACACTACTCGGCTAG CAGT-3′) as upstream and downstream primers for the first round reaction and BG3 (5′-TTCACGCAGAAAGCGTCTAG-3′) and BG4 (5′-GTTGATCCA AGAAAGGACCC-3′) as upstream and downstream primers for the second round reaction; the PCR products were purified using a QIAquick PCR Purification Kit (Qiagen, Hilden, Germany) and digested with Hae III at 37°C for 2 hours; and then, agarose gel electrophoresis was performed to analyze the RFLP of the digestion products.
Statistical analysis
Microsoft Excel (Microsoft, Redmond, Washington, USA) was used for data collection and analyses. Continuous variables were expressed as the means ± standard deviations and compared using Student’s t-test or Fisher’s exact test; categorical variables were expressed as absolute numbers and percentages and were compared using the Chi-square test. Repeated measures analysis of variance was used to provide comparisons between different time points and different groups and to calculate the interaction effects between regimens of DAAs and time points. Mauchly’s test of sphericity was used to judge whether there were relations among the repeatedly measured data. If any P < 0.05, the Greenhouse-Geisser corrected results were utilized; Bonferroni or Fisher’s Least Significant Difference tests (when Epsilon < 0.7, Bonferroni test) were used to examine pairwise comparisons of the repeatedly measured data at different measurement times. We conducted the statistical analyses using SPSS version 16.0. P < 0.05 was considered to indicate statistical significance.
Abbreviations
CHC, chronic hepatitis C; DAAs, directly acting antivirals; eGFR, estimated glomerular filtration rate; Scr, serum creatinine; UA, uric acid; HCV, hepatitis C virus; HBV, hepatitis C virus; SVR, sustained virological response; AEs, adverse events; PR, peginterferon and ribavirin; DDIs, drug-drug interactions; SOF, sofosbuvir; DAC, daclatavir; LDV, ledipasvir; LSM, liver stiffness measurement; RFLP, restriction fragment length polymorphism.
Authors’ contributions
Xiaoyuan Xu designed the research; Jianhong Chen performed the research, Jianhong Chen, Xiaxia Zhang, Hao Luo, Chihong Wu, Min Yu, Dan Liu, Hongli Xi, Yihang Zhou, and Yaoyu An contributed to data collection; Jianhong Chen analysed the data and wrote the paper.
ACKNOWLEDGMENTS AND FUNDING
Thanks for the financial support of the National Natural Science Foundation of China, NO. 81373056; Beijing Municipal Committee of Science and Technology, NO. D161100002716003; National Major Project for Infectious Diseases Control, NO. 2012ZX10002003-004-003.
CONFLICTS OF INTEREST
The authors declare that no conflicts of interest exists.
REFERENCES
1. Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013; 57:1333–42. doi: 10.1002/hep.26141.
2. Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol. 2014; 61:S45–57. doi: 10.1016/j.jhep.2014.07.027.
3. Tornesello ML, Buonaguro L, Izzo F, Buonaguro FM. Molecular alterations in hepatocellular carcinoma associated with hepatitis B and hepatitis C infections. Oncotarget. 2016; 7:25087–102. doi: 10.18632/oncotarget.7837.
4. Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol 2006; 45:529–38. doi: 10.1016/j.jhep.2006.05.013.
5. Everson GT, Sims KD, Rodriguez-Torres M, Hézode C, Lawitz E, Bourlière M, Loustaud-Ratti V, Rustgi V, Schwartz H, Tatum H, Marcellin P, Pol S, Thuluvath PJ, et al. Efficacy of an interferon- and ribavirin-free regimen of daclatasvir, asunaprevir, and BMS-791325 in treatment-naive patients with HCV genotype 1 infection. Gastroenterology. 2014; 146:420–9. doi: 10.1053/j.gastro.2013.10.057.
6. Pawlotsky JM. New Hepatitis C therapies: the toolbox, strategies, and challenges. Gastroenterology. 2014; 146:1176–92. doi: 10.1053/j.gastro.2014.03.003.
7. Asselah T. Daclatasvir plus sofosbuvir for HCV infection: an oral combination therapy with high antiviral efficacy. J Hepatol. 2014; 61:435–8. doi: 10.1016/j.jhep.
8. Lu MY, Huang CI, Hsieh MY, Hsieh TJ, Hsi E, Tsai PC, Tsai YS, Lin CC, Hsieh MH, Liang PC, Lin YH, Hou NJ, Yeh ML, et al. Dynamics of PBMC gene expression in hepatitis C virus genotype 1-infected patients during combined peginterferon/ribavirin therapy. Oncotarget. 2016; 7: 61325–35. doi: 10.18632/oncotarget.11348.
9. Sarrazin C. The importance of resistance to direct antiviral drugs in HCV infection in clinical practice. J Hepatol. 2016; 64:486–504. doi: 10.1016/j.jhep.2015.09.011.
10. Lontok E, Harrington P, Howe A, Kieffer T, Lennerstrand J, Lenz O, McPhee F, Mo H, Parkin N, Pilot-Matias T, Miller V. Hepatitis C virus drug resistance-associated substitutions: State of the art summary. Hepatology. 2015; 62:1623–32. doi: 10.1002/hep.27934.
11. Smolders EJ, Pape S, de Kanter CT, van den Berg AP, Drenth JP, Burger DM. Decreased tacrolimus plasma concentrations during HCV therapy: a drug-drug interaction or is there an alternative explanation? Int J Antimicrob Agents. 2017; 49:379–382. doi: 10.1016/j.ijantimicag.2016.12.004.
12. De Monte A, Courjon J, Anty R, Cua E, Naqvi A, Mondain V, Cottalorda J, Ollier L, Giordanengo V. Direct-acting antiviral treatment in adults infected with hepatitis C virus: Reactivation of hepatitis B virus coinfection as a further challenge. J Clin Virol. 2016; 78:27–30. doi: 10.1016/j.jcv.2016.02.026.
13. Belperio PS, Shahoumian TA, Mole LA, Backus LI. Evaluation of Hepatitis B Reactivation among 62,920 Veterans treated with Oral Hepatitis C Antivirals. Hepatology. 2017. doi: 10.1002/hep.29135.
14. Han H, Agarwal R, Martel-Laferriere V, Dieterich DT. Antiretroviral and anti-hepatitis C virus direct-acting antiviral-related hepatotoxicity. Clin Liver Dis. 2013; 17:657–70. doi: 10.1016/j.cld.2013.07.007.
15. Dyson JK, Hutchinson J, Harrison L, Rotimi O, Tiniakos D, Foster GR, Aldersley MA, McPherson S. Liver toxicity associated with sofosbuvir, an NS5A inhibitor and ribavirin use. J Hepatol. 2016; 64:234–8. doi: 10.1016/j.jhep.2015.07.041.
16. Marchan-Lopez A, Dominguez-Dominguez L, Kessler-Saiz P, Jarrin-Estupiñan ME. Liver failure in human immunodeficiency virus - Hepatitis C virus coinfection treated with sofosbuvir, ledipasvir and antiretroviral therapy. J Hepatol. 2016; 64:752–3. doi: 10.1016/j.jhep.2015.10.033.
17. Bunnell KL, Vibhakar S, Glowacki RC, Gallagher MA, Osei AM, Huhn G. Nephrotoxicity Associated with Concomitant Use of Ledipasvir-Sofosbuvir and Tenofovir in a Patient with Hepatitis C Virus and Human Immunodeficiency Virus Coinfection. Pharmacotherapy. 2016; 36:e148–53. doi: 10.1002/phar.1803.
18. Carrier P, Essig M, Debette-Gratien M, Sautereau D, Rousseau A, Marquet P, Jacques J, Loustaud-Ratti V. Anti-hepatitis C virus drugs and kidney. World J Hepatol. 2016; 8:1343–53. doi: 10.4254/wjh.v8.i32.1343.
19. Coilly A, Fougerou C, De Ledinghen V, Houssel-Debry P, Duvoux C, Di Martino V, Radenne S, Kamar N, D’Alteroche L, Leroy V, Canva V, Lebray P, Moreno C, et al. The association of sofosbuvir and daclatasvir for treating severe recurrence of HCV infection after liver transplantation: Results from a large french prospective multicentric ANRS CO23 CUPILT cohort. J Hepatol. 2015; 62:S236–7. doi: 10.1016/S0168-8278(15)30103-3.
20. Saxena V, Koraishy FM, Sise ME, Lim JK, Schmidt M, Chung RT, Liapakis A, Nelson DR, Fried MW, Terrault NA. Safety and efficacy of sofosbuvir-containing regimens in hepatitis C-infected patients with impaired renal function. Liver Int. 2016; 36:807–16. doi: 10.1111/liv.13102.
21. Mauss S, Hueppe D, Alshuth U. Renal impairment is frequent in chronic hepatitis C patients under triple therapy with telaprevir or boceprevir. Hepatology. 2014; 59:46–48. doi: 10.1002/hep.26602.
22. Loustaud-Ratti V, Rousseau A, Carrier P, Vong C, Chambaraud T, Jacques J, Debette-Gratien M, Sautereau D, Essig M. eGFR decrease during antiviral C therapy with first generation protease inhibitors: a clinical significance? Liver Int. 2015; 35:71–78. doi: 10.1111/liv.12631.
23. Ji D, Chen GF, Wang C, Wang YD, Shao Q, Li B, Zhao J, You SL, Hu JH, Liu JL, Niu XX, Chen J, Lu L, et al. Twelve-week ribavirin-free direct-acting antivirals for treatment-experienced Chinese with HCV genotype 1b infection including cirrhotic patients. Hepatol Int. 2016; 10:789–98. doi: 10.1007/s12072-016-9755-0.
24. Werner CR, Schwarz JM, Egetemeyr DP, Beck R, Malek NP, Lauer UM, Berg CP. Second-generation direct-acting-antiviral hepatitis C virus treatment: Efficacy, safety, and predictors of SVR12. World J Gastroenterol. 2016; 22:8050–59. doi: 10.3748/wjg.v22.i35.8050.
25. Jiménez-Pérez M, González-Grande R, España Contreras P, Pinazo Martínez I, de la Cruz Lombardo J, Olmedo Martín R. Treatment of chronic hepatitis C with direct-acting antivirals: The role of resistance. World J Gastroenterol. 2016; 22:6573–81. doi: 10.3748/wjg.v22.i29.6573.
26. Satsangi S, Mehta M, Duseja A, Taneja S, Dhiman RK, Chawla Y. Dual treatment with sofosbuvir plus ribavirin is as effective as triple therapy with pegylated interferon plus sofosbuvir plus ribavirin in predominant genotype 3 patients with chronic hepatitis C. J Gastroenterol Hepatol. 2016. doi: 10.1111/jgh.13595.
27. Kuwabara M, Bjornstad P, Hisatome I, Niwa K, Roncal-Jimenez CA, Andres-Hernando A, Jensen T, Milagres T, Sato Y, Garcia G, Ohno M, Lanaspa MA, Johnson RJ. Elevated Serum Uric Acid Level Predicts Rapid Decline in Kidney Function. Am J Nephrol. 2017; 45:330–37. doi: 10.1159/000464260.
28. Talavera Pons S, Boyer A, Lamblin G, Chennell P, Châtenet FT, Nicolas C, Sautou V, Abergel A. Managing drug-drug interactions with new direct-acting antiviral agents in chronic hepatitis C. Br J Clin Pharmacol. 2017; 83:269–93. doi: 10.1111/bcp.13095.
29. Lauffenburger JC, Mayer CL, Hawke RL, Brouwer KL, Fried MW, Farley JF. Medication use and medical comorbidity in patients with chronic hepatitis C from a US commercial claims database: high utilization of drugs with interaction potential. Eur J Gastroenterol Hepatol. 2014; 26:1073–82. doi: 10.1097/MEG.0000000000000152.
30. Maasoumy B, Port K, Calle Serrano B, Markova AA, Sollik L, Manns MP, Cornberg M, Wedemeyer H. The clinical significance of drug–drug interactions in the era of direct-acting anti-viral agents against chronic hepatitis C. Aliment Pharmacol Ther. 2013; 38:1365–72. doi: 10.1111/apt.12523.
31. Furihata T, Matsumoto S, Fu Z, Tsubota A, Sun Y, Matsumoto S, Kobayashi K, Chiba K. Different interaction profiles of direct-acting anti-hepatitisC virus agents with human organic anion transporting polypeptides. Antimicrob Agents Chemother. 2014; 58:4555–64. doi: 10.1128/AAC.02724-14.
32. Kiser JJ, Burton JR, Everson GT. Drug–drug interactions during antiviral therapy for chronic hepatitis C. Nat Rev Gastroenterol Hepatol. 2013; 10:596–606. doi: 10.1038/nrgastro.2013.106.
33. Smolders EJ, de Kanter CT, van Hoek B, Arends JE, Drenth JP, Burger DM. Pharmacokinetics, Efficacy, and Safety of Hepatitis C Virus Drugs in Patients with Liver and/or Renal Impairment. Drug Saf. 2016; 39:589–611. doi: 10.1007/s40264-016-0420-2.
34. Saab S, Park SH, Mizokami M, Omata M, Mangia A, Eggleton E, Zhu Y, Knox SJ, Pang P, Subramanian M, Kowdley K, Afdhal NH. Safety and efficacy of ledipasvir/sofosbuvir for the treatment of genotype 1 hepatitis C in subjects aged 65 years or older. Hepatology. 2016; 63:1112–9. doi: 10.1002/hep.28425.
35. Rodríguez-Osorio I, Cid P, Morano L, Castro Á, Suárez M, Delgado M, Margusino L, Meijide H, Pernas B, Tabernilla A, Pedreira JD, Mena Á, Poveda E. Real life experience with direct-acting antivirals agents against hepatitis C infection in elderly patients. J Clin Virol. 2017; 88:58–61. doi: 10.1016/j.jcv.2017.01.003.
36. Talavera Pons S, Boyer A, Lamblin G, Chennell P, Châtenet FT, Nicolas C, Sautou V, Abergel A. Managing drug-drug interactions with new direct-acting antiviral agents in chronic hepatitis C. Br J Clin Pharmacol. 2017; 83:269–93. doi: 10.1111/bcp.13095.
37. Sun H, Frassetto L, Benet LZ. Effects of renal failure on drug transport and metabolism. Pharmacol Ther. 2006; 109:1–11. doi: 10.1016/j.pharmthera. 2005.05.010.
38. Verbeeck R. Pharmacokinetics and dosage adjustment in patients with hepatic dysfunction. Eur J Clin Pharmacol. 2008; 64:1147–61. doi:10.1007/s00228-008-0553-z.
39. European Association for Study of Liver. EASL Recommendations on Treatment of Hepatitis C 2015. J Hepatol. 2015; 63:199–236. doi: 10.1016/j.jhep.2015.03.025.
40. AASLD/IDSA HCV Guidance Panel. Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology. 2015; 62:932–54. doi: 10.1002/hep.27950.
41. Chinese Society of Hepatology, Chinese Medical Association; Chinese Society of Infectious Diseases, Chinese Medical Association. The guideline of prevention and treatment for hepatitis C : a 2015 update. Chin J Hepatol. 2015; 23:906–23. doi: 10.3760/cma.j.issn.1007-3418.2015. 12.003.
42. Degos F, Perez P, Roche B, Mahmoudi A, Asselineau J, Voitot H, Bedossa P; FIBROSTIC study group. Diagnostic accuracy of FibroScan and comparison to liver fibrosis biomarkers in chronic viral hepatitis: a multicenter prospective study (the FIBROSTIC study). J Hepatol. 2010; 53:1013–21. doi: 10.1016/j.jhep.2010.05.035.
43. Ziol M, Handra-Luca A, Kettaneh A, Christidis C, Mal F, Kazemi F, de Lédinghen V, Marcellin P, Dhumeaux D, Trinchet JC, Beaugrand M. Noninvasive assessment of liver fibrosis by measurement of stiffness in patients with chronic hepatitis C. Hepatology. 2005; 41:48–54. doi: 10.1002/hep.20506.
44. Sterling RK, Lissen E, Clumeck N, Sola R, Correa MC, Montaner J, S Sulkowski M, Torriani FJ, Dieterich DT, Thomas DL, Messinger D, Nelson M; APRICOT Clinical Investigators. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006; 43:1317–25. doi: 10.1002/hep.21178.
45. Ma YC, Zuo L, Chen JH, Luo Q, Yu XQ, Li Y, Xu JS, Huang SM, Wang LN, Huang W, Wang M, Xu GB, Wang HY. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006; 17:2937–44. doi: 10.1681/ASN.2006040368.
46. Zhang R, Shao C, Huo N, Li M, Xu X. Association of IL28B Genotypes and Baseline Serum Interferon-γ-Inducible-Protein-10 Levels with Treatment Response in Hepatitis C Virus Patients in China. Gut Liver. 2016; 10:446–55. doi: 10.5009/gnl15162.
47. Bai L, Feng ZR, Lu HY, Li WG, Yu M, Xu XY. Prevalence of antinuclear and anti-liver-kidney-microsome type-1 antibodies in patients with chronic hepatitis C in China. Chin Med J (Engl). 2009; 122:5–9. doi: 10.3760/cma.j.issn.0366-6999.2009.01.002.