
INTRODUCTION
Hip fracture is a fracture of the upper part of the femur, and has high incidence in the elderly [1]. Hip fractures in aged people leads to high mortality, high risk of postoperative complication, and impaired quality of life [2–5]. The mortality is increased from 8.4% to 36% in the first postoperative year [6].
The risk factors for mortality following hip fracture surgery was demonstrated in some studies [7], we hope to reveal the clinically relevant biomarkers to evaluate prognosis and complication events. It has been reported that serum albumin level and lymphocyte count served as an independent prognostic factor in hip fracture patients [8]. The prognostic nutritional index (PNI) is calculated by the serum albumin concentration and the peripheral blood lymphocyte count [9]. Albumin is an indicator of nutritional status which is correlated with post-operative complications [10]. The PNI can be used to assess the immunological and nutritional status of surgery patients [11], and estimated according to the following formula: 10 × serum albumin (g/dL) + 0.05 total lymphocyte count (/mm3) [12]. C-reactive protein (CRP) is an inflammatory marker which is closely related to the infections and outcomes in orthopaedics [13]. And PNI is associated with cancer mortality and has a prognostic value [14].
The correlation of CRP/PNI ratio and mortality after hip fracture surgery, especially in elderly population remains unknown. This study is aim to evaluate the predictive value of CRP/PNI ratio in elderly patients after orthopedic surgery, and compare it with clinical variables.
RESULTS
We estimated the CRP/PNI ratio in 80 patients, 35 (43.75%) of whom were men and 45 (56.25%) were women. The results are presented in Figure 1 and summarized in Table 1; the mean CRP and PNI were 11.3 ± 9.6 mg/L and 41.3 ± 11.0, respectively. An inverse correlation was found between CRP and PNI with a correlation coefficient of -0.761 which was shown in Figure 1 (P =0.016). The relationships between the CRP/PNI ratio and clinical characteristics were shown in Table 1. Based on the receiver operating characteristics (ROC) analyses, the best cut-off value of CRP/PNI ratio was 0.10. Then, patients were divided into two groups: patients with CRP/PNI ratio ≤0.10 and patients with CRP/PNI ratio >0.10. There were 42 (52.5%) patients with CRP/PNI ratio ≤0.10 and 38 (47.5%) patients with CRP/PNI ratio >0.10. CRP/PNI ratio is correlated significantly with CRP (P <0.001), leukocytosis (P =0.003), lymphocyte counts (P <0.001), hypoalbuminemia (P =0.001), PNI (P <0.001) and survival (P <0.001), but no relationships were found between CRP/PNI ratio and other factors such as comorbidity, platelet count and anemia.
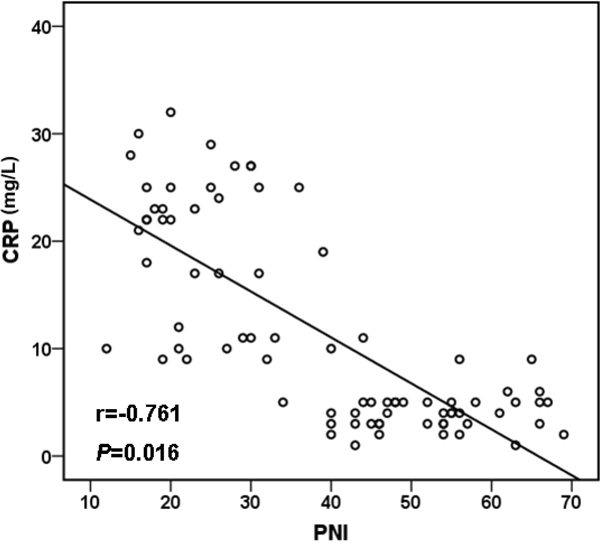
Figure 1: Pearson correlation. A signifcant negative correlation between CRP and PNI (r=-0.761, P =0.016). CRP: C-reactive protein; PNI: prognostic nutritional index.
Table 1: The CRP/PNI ratio and clinicopathological parameters
|
Case(n) |
CRP/PNI ratio |
p Value |
|
|---|---|---|---|---|
≤ 0.10 |
> 0.10 |
|||
Age (years) |
86±5 |
85±7 |
87±3 |
0.192 |
Men |
35 |
18 |
17 |
0.301 |
Weight (kg) |
62 (49–78) |
61 (45–74) |
63 (55–78) |
0.762 |
Length of stay (day) |
7 (5–14) |
6 (5–10) |
9 (6–14) |
0.162 |
Duration of surgery (min) |
140 (111–170) |
140 (111–170) |
140 (111–170) |
0.912 |
Comorbidity |
|
|
|
|
Diabetes mellitus |
34 |
17 |
17 |
0.684 |
Cardiovascular disease |
24 |
13 |
11 |
0.726 |
Hypertension |
63 |
32 |
31 |
0.710 |
Renal disefficiency |
21 |
12 |
9 |
0.691 |
CRP, mg/L |
|
|
|
|
<10 |
43 |
39 |
4 |
0.000* |
≥10 |
36 |
2 |
34 |
|
Platelet count,/mm3 |
|
|
|
|
<214 |
43 |
18 |
25 |
0.067 |
≥214 |
37 |
24 |
13 |
|
Leukocytosis |
|
|
|
|
Yes |
26 |
9 |
17 |
0.033* |
No |
54 |
33 |
21 |
|
Anemia |
|
|
|
|
Yes |
42 |
25 |
17 |
0.262 |
No |
38 |
17 |
21 |
|
Lymphocyte counts,/mm3 |
|
|
|
|
<1673 |
43 |
31 |
12 |
0.000* |
≥1673 |
37 |
11 |
26 |
|
Hypoalbuminemia |
|
|
|
|
Yes |
28 |
26 |
2 |
0.001* |
No |
52 |
16 |
36 |
|
PNI |
|
|
|
|
<44 |
39 |
1 |
38 |
0.000* |
≥44 |
41 |
41 |
0 |
|
Survival status |
|
|
|
|
Dead |
41 |
3 |
38 |
0.000* |
Alive |
39 |
39 |
0 |
|
CRP: C-reactive protein; PNI: prognostic nutritional index; * P<0.05 is considered significant.
Concerning survival, only 3 of 42 (7.1 %) patients in the CRP/PNI ratio ≤0.10 group died versus 38 of 38 (100.0 %) in the CRP/PNI ratio >0.10 group (Table 2). The survival was significantly influenced by only CRP (P <0.001), lymphocyte counts (P =0.013), hypoalbuminemia (P =0.002), PNI (P <0.001) and CRP/PNI ratio (P <0.001), while all variables were compared separately to survival status (Table 2). In univariate analysis, the Kaplan–Meier survival curves showed to no significant relationship between platelet count, leukocytosis, anemia and survival. The Kaplan–Meier survival curves of low CRP/PNI ratio versus high CRP/PNI ratio showed a highly significant separation (P <0.001, Figure 2C). Furthermore, patients with high CRP (P <0.001, Figure 2A) or low PNI (P <0.001, Figure 2B) were also related to the poor 1-year survival, respectively. When a multivariate Cox proportional hazard model was constructed (including age, duration of surgery, weight, length of stay, sex, CRP, PNI, platelet count, leukocytosis, anemia, lymphocyte counts, hypoalbuminemia and CRP/PNI ratio), the CRP/PNI ratio was the strongest independent predictor of survival (Table 3).
Table 2: Survival status and clinicopathological parameters in 80 specimens
|
Case(n) |
Survival status |
p Value |
|
|---|---|---|---|---|
Dead=41 |
Alive=39 |
|||
Age (years) |
86±5 |
87±5 |
85±4 |
0.059 |
Men |
35 |
19 |
16 |
0.142 |
Weight (kg) |
62 (49–78) |
60 (49–72) |
63 (50–78) |
0.699 |
Length of stay (day) |
7 (5–14) |
8 (6–14) |
7 (5–12) |
0.734 |
Duration of surgery (min) |
140 (111–177) |
146 (112–177) |
139 (111–168) |
0.209 |
Comorbidity |
|
|
|
|
Diabetes mellitus |
34 |
20 |
14 |
0.550 |
Cardiovascular disease |
24 |
13 |
11 |
0.673 |
Hypertension |
63 |
33 |
30 |
0.897 |
Renal disefficiency |
21 |
11 |
10 |
0.803 |
CRP, mg/L |
|
|
|
|
<10 |
43 |
7 |
36 |
0.000* |
≥10 |
36 |
34 |
2 |
|
Platelet count,/mm3 |
|
|
|
|
<214 |
43 |
26 |
17 |
0.116 |
≥214 |
37 |
15 |
22 |
|
Leukocytosis |
|
|
|
|
Yes |
26 |
17 |
9 |
0.098 |
No |
54 |
24 |
30 |
|
Anemia |
|
|
|
|
Yes |
42 |
18 |
24 |
0.125 |
No |
38 |
23 |
15 |
|
Lymphocyte counts,/mm3 |
|
|
|
|
<1673 |
43 |
13 |
30 |
0.013* |
≥1673 |
37 |
28 |
9 |
|
Hypoalbuminemia |
|
|
|
|
Yes |
28 |
26 |
2 |
0.002* |
No |
52 |
15 |
37 |
|
PNI |
|
|
|
|
<44 |
39 |
39 |
0 |
0.000* |
≥44 |
42 |
2 |
30 |
|
CRP/PNI |
|
|
|
|
≤ 0.10 |
42 |
3 |
39 |
0.000* |
> 0.10 |
38 |
38 |
0 |
|
CRP: C-reactive protein; PNI: prognostic nutritional index; * P<0.05 is considered significant.
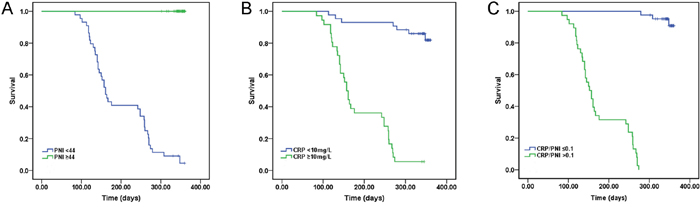
Figure 2: Kaplan-Meier survival curves stratifed by CPR, PNI and CRP/PNI ratio. (A and B) Patients with elevated CRP (P <0.001) or decreased PNI (P <0.001) were associated with decreased 1-year survival, respectively. (C) Patients with CRP/PNI ratio ≤0.10 had a better 1-year survival than patients with CRP/PNI ratio >0.10 (P <0.001). CRP: C-reactive protein; PNI: prognostic nutritional index.
Table 3: Contribution of various potential prognostic factors to survival by Cox regression analysis in 80 specimens
|
Hazard ratio |
95 % CI |
P |
|---|---|---|---|
Age(years) |
1.5 |
0.775~2.430 |
0.158 |
Duration of surgery (min) |
0.7 |
0.341~3.776 |
0.342 |
Weight (kg) |
1.8 |
0.656~3.167 |
0.782 |
Length of stay (day) |
0.2 |
0.096~2.034 |
0.053 |
Sex |
1.9 |
0.127~3.907 |
0.102 |
CRP, mg/L |
3.3 |
1.337~8.737 |
0.054 |
PNI |
0.2 |
0.028~0.650 |
0.067 |
Platelet count,/mm3 |
2.0 |
0.672~6.101 |
0.210 |
Leukocytosis |
0.9 |
0.313~2.860 |
0.922 |
Anemia |
1. 3 |
0.432~3.811 |
0.653 |
Lymphocyte counts,/mm3 |
2.1 |
1.093~6.107 |
0.059 |
Hypoalbuminemia |
1.4 |
0.897~3.357 |
0.072 |
CRP/PNI |
8.1 |
1.806~36.216 |
0.006* |
CRP: C-reactive protein; PNI: prognostic nutritional index; CI: confidence interval; statistical analyses were performed by the log-rank test; * P<0.05 is considered significant.
The areas under the curve (AUC) was 0.998 for CRP/PNI ratio (95% CI: 0.000-1.000, P <0.001), 0.928 (95% CI: 0.861-0.990, P <0.001) for CRP and 0.953 (95% CI: 0.002-0.996, P <0.001) for PNI. Our results indicated that the CRP/PNI ratio was superior to the CRP or PNI (Figure 3) for the older patients after hip fracture surgery.
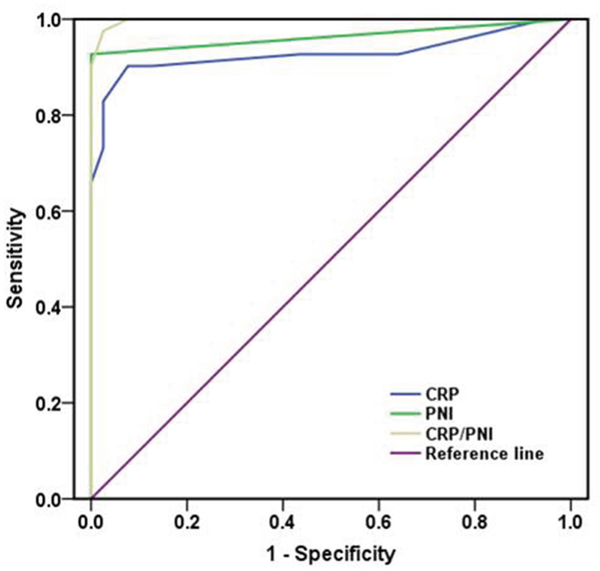
Figure 3: Comparison of the AUC for ROC curves. The AUC of the CRP/PNI ratio was higher than other CRP or PNI, indicating that the CRP/PNI ratio was superior to the CRP or PNI for prognosis. CRP: C-reactive protein; PNI: prognostic nutritional index; AUC: area under curve; ROC: receiver operating characteristics.
DISCUSSION
Because of the poor prognosis of acute surgery in elderly patients, biomarkers in clinical management of these patients are important. In our study, CRP/PNI ratio was used as an independent prognostic factor for elderly patients after orthopedic surgery. And this is the first study which examined the prognostic value of CRP/PNI ratio for elderly patients after orthopedic surgery.
Infection or traumas has a strong relationship with inflammation. Previous data have shown that CRP is a sensitive and non-specific inflammatory marker of human infection or traumas [15]. CRP is proved to be very useful in diagnosis and functioned as a monitor of infections in orthopaedics [13]. A retrospective analysis conducted by Kim et al. [15] revealed that preoperative CRP was an independent risk factor for 1-year mortality after hip fracture surgery in the elderly. In our current research, these patients with low CRP levels (≤10.0 mg/L) had better survival than those with CRP >10.0 mg/L (83.7% vs. 5.6%, P <0.001). Regrettably, in the multivariate analyses, there was no evidence to prove that CRP was an independent prognostic factor (P =0.054).
The PNI was designed to assess the immunologic and nutritional aspects of surgical patients [16], and calculated by the serum albumin concentration and the lymphocyte count in the peripheral blood [17]. Hypoalbuminemia served as a potential preoperative predictor of outcomes [18]. Lu et al. showed that a lower serum albumin level and total lymphocyte count were important risk factors to predict the one-year mortality of elderly patients with fracture [19]. However, few studies focused on PNI in elderly patients after hip fracture surgery. In our data, PNI was not an independent prognostic factor (P =0.067).
As CRP and PNI are affected by various conditions, the CRP/PNI ratio could therefore reduce the potential bias. The prognostic value of CRP/PNI ratio is better than CRP or PNI in elderly patients after hip fracture surgery. In this study, the CRP/PNI ratio has been investigated to assess the outcomes of the elderly patients after hip fracture surgery. Patients with low CRP/PNI ratio had a longer median survival time than those with high CRP/PNI ratio (88.6% vs. 0%, P <0.001). CRP/PNI ratio has been demonstrated as an important predictive factor of 1-year survival by multivariate analyses (P=0.006). The CRP/PNI ratio had not been investigated before in hip fracture surgery patients before, especially in elderly patients. This is the first time to elucidate that CRP/PNI ratio is a predictor of hip fracture surgery in elderly patients.
In our Cox regression model, multivariate analyses revealed that the CRP/PNI ratio was an independent prognostic factor. Our data showed that the AUC was higher in CRP/PNI ratio than CRP (0.928) or PNI (0.963) by ROC analyses. High levels of CRP/PNI ratio could help us to avoid adverse consequences. Patients will benefit from the CRP/PNI ratio, especially in the elderly patients.
Nevertheless, several limitations should be paid attention in this study. Firstly, this study is a retrospective and single-institution study. Secondly, the number of patients was not adequate (n =80). Thence, larger prospective studies need to be carried out to confirm these preliminary results.
In summary, current data indicate that CRP/PNI ratio is correlated with 1-year survival in elderly patients after hip fracture surgery. Based on these results, we believe that CRP/PNI ratio is a novel and useful predictive factor in elderly patients after hip fracture surgery.
MATERIALS AND METHODS
Patients
The data of 80 elderly patients after hip fracture surgery in Shanghai Pudong Hospital between 2015 and 2016 were collected in our study. The 70 years of age or older patients were included, and the patients were excluded if CRP, platelet count, leukocyte count, lymphocyte counts, hemoglobin and albumin measurements were lacking. Ethical approval was obtained for the study protocols and informed consents were obtained from each patient.
Data collection
We collected clinical data including age, sex, weight, length of stay, duration of surgery, comorbidity, biological data and survival time. The patients had been tested for serum CRP, platelet count, leukocyte count, lymphocyte counts, hemoglobin and albumin before surgery. At the same time, we carefully reviewed the associated comorbidities of these patients. The biological data were measured by automatic laser nephelometry (BN 100 analyzer, Germany). The normal values of CRP, platelet count, leukocyte count, lymphocyte counts, hemoglobin and albumin were 0–10 mg/L, 125–350 ×109/L, 3.5–9.5×109/L, 1.1–3.2 ×109/L, 110–175 ×109/L, 35–50 g/L, respectively.
Follow-up and endpoint
The mean follow-up period for these patients was 8.7 months (range: 3–12 months). All patients were followed up by phone monthly. The endpoint was mortality within one year.
Statistical analysis
All statistical analyses were used the SPSS version 22.0 statistical software. The association between CRP and PNI were studied using the Spearman rank correlation test Survival analysis. For analysis of survival data, Kaplan-Meier curves were constructed, and the log-rank test was used for analysis. Univariate and multivariate analyses were performed using Cox’s proportional hazards model. Differenceswere considered statistically significant when P value was less than 0.05.
ACKNOWLEDGMENTS
This study was funded by the Outstanding Leaders Training Program of Pudong Health Bureau of Shanghai (grant PWR12013-01), the Program for Outstanding Academic Leader of Shanghai, and the Program for Medical Key Department of Shanghai (Grant ZK 2015B17).
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
1. Heiberg KE, Bruun-Olsen V, Bergland A. The effects of habitual functional training on physical functioning in patients after hip fracture: the protocol of the HIPFRAC study. BMC Geriatr. 2017; 17: 23.
2. Katsoulis M, Benetou V, Karapetyan T, Feskanich D, Grodstein F, Pettersson-Kymmer U, Eriksson S, Wilsgaard T, Jorgensen L, Ahmed LA, Schottker B, Brenner H, Bellavia A, et al. Excess mortality after hip fracture in elderly persons from Europe and the USA: the CHANCES project. J Intern Med. 2017; 281: 300-10.
3. Mundi S, Pindiprolu B, Simunovic N, Bhandari M. Similar mortality rates in hip fracture patients over the past 31 years. Acta Orthop. 2014; 85: 54-9.
4. Huddleston JM, Whitford KJ. Medical care of elderly patients with hip fractures. Mayo Clin Proc. 2001; 76: 295-8.
5. Tarride JE, Burke N, Leslie WD, Morin SN, Adachi JD, Papaioannou A, Bessette L, Brown JP, Pericleous L, Muratov S, Hopkins RB. Loss of health related quality of life following low-trauma fractures in the elderly. BMC Geriatr. 2016; 16: 84.
6. Abrahamsen B, Van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009; 20: 1633-50.
7. Folbert EC, Hegeman JH, Gierveld R, Van Netten JJ, Velde DV, Ten Duis HJ, Slaets JP. Complications during hospitalization and risk factors in elderly patients with hip fracture following integrated orthogeriatric treatment. Arch Orthop Trauma Surg. 2017; 137: 507-15.
8. Symeonidis PD, Clark D. Assessment of malnutrition in hip fracture patients: effects on surgical delay, hospital stay and mortality. Acta Orthop Belg. 2006; 72: 420-7.
9. Nozoe T, Ninomiya M, Maeda T, Matsukuma A, Nakashima H, Ezaki T. Prognostic nutritional index: a tool to predict the biological aggressiveness of gastric carcinoma. Surg Today. 2010; 40: 440-3.
10. Adogwa O, Martin JR, Huang K, Verla T, Fatemi P, Thompson P, Cheng J, Kuchibhatla M, Lad SP, Bagley CA, Gottfried ON. Preoperative serum albumin level as a predictor of postoperative complication after spine fusion. Spine (Phila Pa 1976). 2014; 39: 1513-9.
11. Han-Geurts IJ, Hop WC, Tran TC, Tilanus HW. Nutritional status as a risk factor in esophageal surgery. Dig Surg. 2006; 23: 159-63.
12. Hu Q, Wang G, Ren J, Ren H, Li G, Wu X, Gu G, Li R, Guo K, Deng Y, Li Y, Hong Z, Wu L, Li J. Preoperative prognostic nutritional index predicts postoperative surgical site infections in gastrointestinal fistula patients undergoing bowel resections. Medicine (Baltimore). 2016; 95: e4084.
13. Neumaier M, Braun KF, Sandmann G, Siebenlist S. C-reactive protein in orthopaedic surgery. Acta Chir Orthop Traumatol Cech. 2015; 82: 327-31.
14. Miao Y, Li S, Yan Q, Li B, Feng Y. Prognostic significance of preoperative prognostic nutritional index in epithelial ovarian cancer patients treated with platinum-based chemotherapy. Oncol Res Treat. 2016; 39: 712-9.
15. Kim BG, Lee YK, Park HP, Sohn HM, Oh AY, Jeon YT, Koo KH. C-reactive protein is an independent predictor for 1-year mortality in elderly patients undergoing hip fracture surgery: a retrospective analysis. Medicine (Baltimore). 2016; 95: e5152.
16. Buzby GP, Mullen JL, Matthews DC, Hobbs CL, Rosato EF. Prognostic nutritional index in gastrointestinal surgery. Am J Surg. 1980; 139: 160-7.
17. Onodera T, Goseki N, Kosaki G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi. 1984; 85: 1001-5.
18. Kamath AF, Nelson CL, Elkassabany N, Guo Z, Liu J. Low albumin is a risk factor for complications after revision total knee arthroplasty. J Knee Surg. 2017; 30: 269-75.
19. Lu J, Chen YY, Zhang L, Li YG, Wang C. Laboratory nutritional parameters predict one-year mortality in elderly patients with intertrochanteric fracture. Asia Pac J Clin Nutr. 2016; 25: 457-63.