
INTRODUCTION
Gastric cancer is an important cancer type occurring in the upper digestive tract, and presents with high morbidity and mortality in China [1]. The extensive heterogeneity of this malignancy complicates the precise assessment of tumor aggressiveness and prognosis, complicating implementation of effective therapeutic strategies [2]. Thus, it is important to investigate the molecular mechanisms involved in the transformation and progression of gastric cancer. Additionally, there is a need to identify prognostic predictors and novel biomarkers that could predict certain patients benefitting from the targeted therapies.
Tissue factor (TF), a 47-kDa trans-membrane glycoprotein, is a cellular receptor for coagulation factor VII (FVII), activating a clotting cascade involved in many physio-pathological processes [3, 4]. It has been demonstrated that TF could be constitutively expressed by various extra-vascular cells and cancer cells [5]. TF could influence protease-activated receptor-dependent tumor cell behavior and regulate integrin function, leading to the intratumoral angiogenesis both in vitro and in vivo [6]. Our previous study demonstrated that the higher expression of TF in human esophageal cancer tissues significantly associated with tumor invasion and intratumoral angiogenesis, suggesting a positive role of TF in cancer progression [3]. Aberrant TF expression could be induced by a majority of oncogenic events, such as activation of K-Ras or epidermal growth factor receptor (EGFR), inactivation of p53 tumor suppressor, and loss of phosphatase and tensin homolog (PTEN) [7–9].
Besides its transmembrane form, TF also exhibits alternatively spliced transcripts. In 2003, Bogdanov et al. reported a novel alternatively-spliced human TF (asTF) in which exon 5 is deleted (as shown in Figure 1) [10]. The full-length TF (flTF) has six exons, and the asTF lacks exon 5, leading to a truncation of the transmembrane domain and a soluble form of TF [10]. Although lacking pro-coagulant activity, asTF could promote primary growth of human pancreatic cancer cells in vivo and augment tumor-associated angiogenesis [11, 12]. In this study, the transcripts of the two TF isoforms, flTF and asTF, in human gastric cancer tissues were assessed. These two transcripts in gastric cancer tissues and adjacent normal tissues were determined by real-time PCR. The correlation between the mRNA expression levels of TF isoforms and patient’s clinicopathological features was also analyzed.
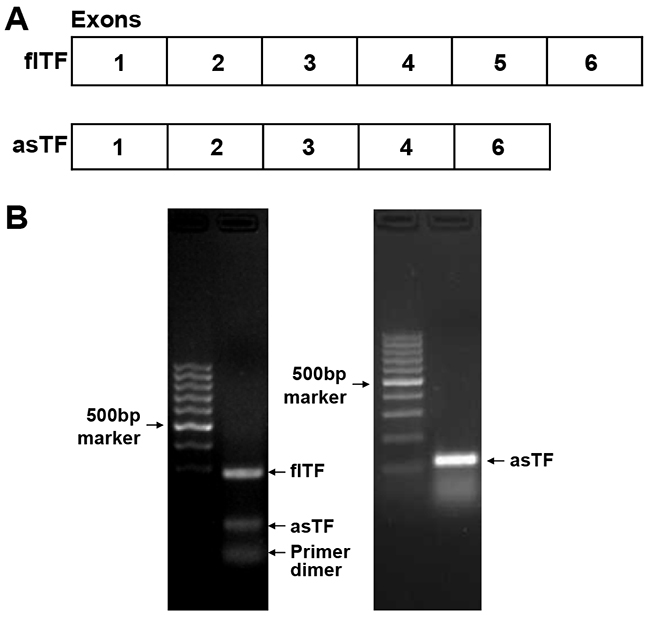
Figure 1: The structure of flTF and asTF. (A) The exons of flTF and asTF. (B) The electrophoresis analysis of the PCR products of flTF and asTF. Left panel, the primers for flTF as well as asTF adopted from the reference. Right panel, the primers designed by ourselves which were used in the real-time PCR assay.
RESULTS
mRNA expression levels of flTF and asTF in human gastric cancer tissues and adjacent normal tissues
The relative mRNA expression level of flTF in human gastric cancer tissues [7.45 (0.34~33.68)] was significantly higher than in normal control tissues [3.00 (1.36~5.02)] (Figure 2A, P=0.035). In addition, the relative mRNA expression level of asTF in human gastric cancer tissues [0.88 (0.07~26.00)] was also found significantly higher than in normal control tissues [0.33 (0.03~0.97)] (Figure 2B, P=0.006). To determine the association of flTF and asTF expression in gastric cancer, we further sub-grouped the 52 patients into flTFLow group (n=23), flTFHigh group (n=29), asTFLow group (n=31), or asTFHigh group (n=20) based on the selected and relative cut-off levels for flTF and asTF (5.02 and 0.97, respectively).
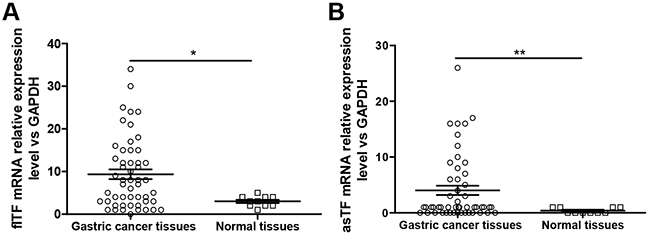
Figure 2: The mRNA expression levels of flTF and asTF in human gastric tissues. (A) The mRNA expression level of flTF in gastric cancer tissues was significantly higher than that in normal gastric tissues. (B) The mRNA expression level of asTF in gastric cancer tissues was significantly higher than that in normal gastric tissues.
Relationship between clinical pathological variables and mRNA relative expression levels of flTF and asTF in gastric cancer tissues
In this study, the mRNA expression level of flTF was not associated with any patients’ clinical parameters (Table 1). The mRNA expression level of asTF in gastric cancer tissues was significantly associated with patients’ age (P=0.018), while it was not correlated with any other clinical parameters of the patients (Table 1).
Table 1: Correlation between patients’ clinical parameters and the mRNA expression levels of flTF and asTF in human gastric cancer tissues
Clinical parameters |
Cases |
flTF expression level |
χ2 |
P-value |
Cases |
asTF expression level |
χ2 |
P-value |
||
|---|---|---|---|---|---|---|---|---|---|---|
High (n, %) |
Low (n, %) |
High (n, %) |
Low (n, %) |
|||||||
Gender |
||||||||||
Male |
34 |
18(52.9) |
16(47.1) |
0.318 |
0.573 |
34 |
15(44.1) |
19(55.9) |
1.028 |
0.311 |
Female |
18 |
11(61.1) |
7(38.9) |
17 |
5(29.4) |
12(70.6) |
||||
Age (years) |
||||||||||
≤60 |
19 |
13(68.4) |
6(31.6) |
1.943 |
0.163 |
18 |
11(61.1) |
7(38.9) |
5.595 |
0.018 |
>60 |
33 |
16(48.5) |
17(51.5) |
33 |
9(27.3) |
24(72.7) |
||||
Tumor stage |
||||||||||
T2 |
3 |
2(66.7) |
1(33.3) |
2.484 |
0.289 |
3 |
1(33.3) |
2(66.7) |
1.106 |
0.575 |
T3 |
7 |
2(28.6) |
5(71.4) |
7 |
4(57.1) |
3(42.9) |
||||
T4 |
42 |
25(59.5) |
17(40.5) |
41 |
15(36.6) |
26(63.4) |
||||
Nodal stage |
||||||||||
N0 |
3 |
2(66.7) |
1(33.3) |
1.44 |
0.696 |
2 |
1(50.0) |
1(50.0) |
0.952 |
0.813 |
N1 |
8 |
3(37.5) |
5(62.5) |
8 |
2(25.0) |
6(75.0) |
||||
N2 |
18 |
11(61.1) |
7(38.9) |
18 |
7(38.9) |
11(61.1) |
||||
N3 |
23 |
13(56.5) |
10(43.5) |
23 |
10(43.5) |
13(56.5) |
||||
Distant metastasis |
||||||||||
No |
45 |
25(55.6) |
20(44.4) |
0.006 |
0.937 |
44 |
17(38.6) |
27(61.4) |
0.045 |
0.832 |
Yes |
7 |
4(57.1) |
3(42.9) |
7 |
3(42.9) |
4(57.1) |
||||
TNM stage |
||||||||||
I |
1 |
1(100.0) |
0(0.0) |
2.092 |
0.553 |
1 |
0(0.0) |
1(100.0) |
0.686 |
0.876 |
II |
6 |
2(33.3) |
4(66.7) |
5 |
2(40.0) |
3(60.0) |
||||
III |
38 |
22(57.9) |
16(42.1) |
38 |
15(39.5) |
23(60.5) |
||||
IV |
7 |
4(57.1) |
3(42.9) |
7 |
3(42.9) |
4(57.1) |
||||
Tumor size (cm) |
||||||||||
≤5 |
18 |
10(55.6) |
8(44.4) |
0.029 |
0.864 |
18 |
6(33.3) |
12(66.7) |
0.213 |
0.644 |
>5 |
31 |
18(58.1) |
13(41.9) |
30 |
12(40.0) |
18(60.0) |
||||
Invasion to the whole layer |
||||||||||
No |
10 |
4(40.0) |
6(60.0) |
1.248 |
0.264 |
10 |
5(50.0) |
5(50.0) |
0.607 |
0.436 |
Yes |
42 |
25(59.5) |
17(40.5) |
41 |
15(36.6) |
26(63.4) |
||||
Histological type |
||||||||||
Well-differentiated |
28 |
12(42.9) |
16(57.1) |
3.808 |
0.051 |
28 |
7(25.0) |
21(75.0) |
2.316 |
0.128 |
Poor-differentiated |
18 |
13(72.2) |
5(27.8) |
17 |
8(47.1) |
9(52.9) |
||||
Chemo-sensitivity |
||||||||||
Insensitive |
19 |
12(63.2) |
7(36.8) |
0.012 |
0.912 |
18 |
6(33.3) |
12(66.7) |
0.121 |
0.728 |
Sensitive |
26 |
16(61.5) |
10(38.5) |
26 |
10(38.5) |
16(61.5) |
||||
Values in bold signify P < 0.05.
Prognostic values of mRNA expression levels of flTF and asTF in gastric cancer tissues
To determine whether flTF and asTF are prognostic factors in gastric cancer, we further carried out survival analyses based on the sub-groups stratified by low/high flTF and asTF expression. As shown in Table 2, we found that the patient’s age (P=0.014), tumor size (P=0.009), and flTF expression level (P=0.018) was significantly associated with post-operative survival. COX model analyses showed that tumor size (P=0.009), distant metastasis (P=0.008), and flTF expression level (P=0.048) could be independent risk factors. The expression level of asTF was also significantly associated with patient’s post-operative survival (Table 3, P=0.038). COX model analyses showed that histo-pathological type (P=0.012), tumor size (P=0.002), tumor differentiation (P=0.041), distant metastasis (P=0.005), and asTF expression level (P=0.002) were independent risk factors of gastric cancer. Also, as shown in Figure 3, we also found that the overall survival rate of the patients with both low flTF and asTF was significantly better than those with flTF and asTF either high group (Figure 3C, P=0.033). The overall survival rate of the patients with flTF and asTF both high was significantly poorer than other patients (Figure 3D, P=0.0003). The overall survival rate of the patients with flTF and asTF either high group was significantly better than those with flTF and asTF both high group (Figure 3E, P=0.012). We also found there was a significant difference among the three subgroups, namely the patients with flTF and asTF both low, the patients with flTF and asTF either high, and the patients with flTF and asTF both high (Figure 3F, P=0.001).
Table 2: Cox model analysis of flTF mRNA expression level in predicting gastric patients’ prognoses
Clinical parameters |
Univariate |
Multivariate |
||||
|---|---|---|---|---|---|---|
HR |
95% CI |
P-value |
HR |
95% CI |
P-value |
|
Gender |
||||||
Male / Female |
0.76 |
0.31~1.84 |
0.543 |
1.36 |
0.27~6.74 |
0.707 |
Age (year) |
||||||
50-60/<50 |
0.37 |
0.11~1.23 |
0.104 |
2.63 |
0.32~21.45 |
0.366 |
≥60/<50 |
0.26 |
0.09~0.76 |
0.014* |
2.13 |
0.19-24.28 |
0.543 |
Histo-pathological type |
||||||
Ulcer / Invasive |
0.54 |
0.21~1.40 |
0.204 |
1.34 |
0.25~7.19 |
0.733 |
Others / Invasive |
0.72 |
0.22~2.37 |
0.594 |
6.80 |
0.71~65.52 |
0.097 |
Tumor size |
||||||
≥5cm/<5cm |
7.03 |
1.62~30.54 |
0.009* |
13.98 |
1.95~100.34 |
0.009* |
Depth of invasion |
||||||
Whole layer / Non-whole layer |
1.88 |
0.62~5.72 |
0.268 |
0.87 |
0.12~6.10 |
0.885 |
Nodal metastasis |
||||||
Yes / No |
1.49 |
0.35~6.38 |
0.595 |
4.05 |
0.47~34.71 |
0.202 |
Differentiation |
||||||
Poor / Well |
2.33 |
0.91~5.94 |
0.077 |
3.38 |
0.92~12.44 |
0.067 |
Distant metastasis |
||||||
Yes / No |
3.04 |
0.97~9.52 |
0.056 |
16.57 |
2.10~130.48 |
0.008* |
flTF mRNA expression level |
||||||
High / Low |
3.19 |
1.22~8.35 |
0.018* |
6.03 |
1.02~35.71 |
0.048* |
Values in bold signify P < 0.05.
Table 3: Cox model analysis of asTF mRNA expression level in predicting gastric patients’ prognoses
Clinical parameters |
Univariate |
Multivariate |
||||
|---|---|---|---|---|---|---|
HR |
95% CI |
P-value |
HR |
95% CI |
P-value |
|
Gender |
||||||
Male / Female |
0.76 |
0.31~1.84 |
0.543 |
0.52 |
0.07~4.13 |
0.534 |
Age (year) |
||||||
50-60/<50 |
0.37 |
0.11~1.23 |
0.104 |
7.45 |
0.52~106.87 |
0.140 |
≥60/<50 |
0.26 |
0.09~0.76 |
0.014* |
2.63 |
0.25~27.44 |
0.419 |
Histo-pathological type |
||||||
Ulcer / Invasive |
0.54 |
0.21~1.40 |
0.204 |
1.98 |
0.39~10.19 |
0.414 |
Others / Invasive |
0.72 |
0.22~2.37 |
0.594 |
25.91 |
2.02~331.81 |
0.012* |
Tumor size |
||||||
≥5cm/<5cm |
7.03 |
1.62~30.54 |
0.009* |
28.56 |
3.50~233.00 |
0.002 * |
Depth of invasion |
||||||
Whole layer / Non-whole layer |
1.88 |
0.62~5.72 |
0.268 |
3.10 |
0.581~16.54 |
0.185 |
Nodal metastasis |
||||||
Yes / No |
1.49 |
0.35~6.38 |
0.595 |
4.12 |
0.40~42.48 |
0.235 |
Differentiation |
||||||
Poor / Well |
2.33 |
0.91~5.94 |
0.077 |
4.78 |
1.07~21.33 |
0.041* |
Distant metastasis |
||||||
Yes / No |
3.04 |
0.97~9.52 |
0.056 |
17.40 |
2.37~127.85 |
0.005* |
asTF mRNA expression level |
||||||
High / Low |
2.50 |
1.05~5.95 |
0.038* |
10.74 |
2.32~49.59 |
0.002* |
Values in bold signify P < 0.05.
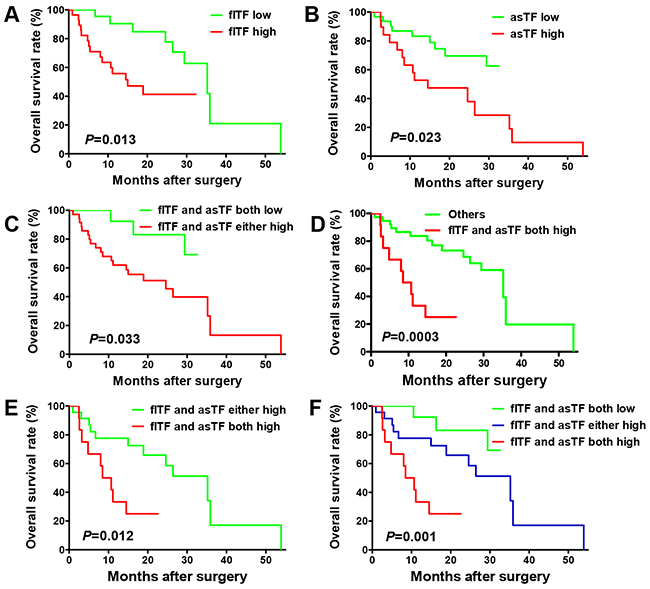
Figure 3: Prognostic value of flTF and asTF levels in human gastric cancer tissues. (A) The overall survival rate of the patients with low flTF was significantly better than those with high flTF. (B) The overall survival rate of the patients with low asTF was significantly better than those with high asTF. (C) The overall survival rate of the patients with both low flTF and asTF was significantly better than those with flTF and asTF either high group. (D) The overall survival rate of the patients with flTF and asTF both high was significantly poorer than other patients. (E) The overall survival rate of the patients with flTF and asTF either high group was significantly better than those with flTF and asTF both high group. (F) There was a significant difference among the three subgroups, namely the patients with flTF and asTF both low, the patients with flTF and asTF either high, and the patients with flTF and asTF both high.
DISCUSSION
TF is an initiation factor regulating extrinsic coagulation and multiple physiological and pathological processes such as tumor angiogenesis, wound healing, intracellular signaling, and tumor metastasis [4]. It has been demonstrated that high TF expression could be found in many different tumor cells, such as pancreatic carcinoma, lung carcinoma, and colorectal carcinoma, as well as in vascular endothelial cell and interstitial macrophages of tumor tissues [13]. In addition, abnormal expression of TF is associated with cell growth, tumor invasiveness and metastasis, prognosis, and multi-drug resistance [14].
The open reading frame of human TF gene encodes 6 exons, with flTF containing all 6 exons. In 2003, a study by Bogdanov reported an alternatively spliced tissue factor (asTF) transcript in myeloid leukemia HL-60 cell through by selectively removing exon 5 [10]. In contrast to the flTF, asTF lacks a trans-membrane domain and contain unique amino acid sequence [10]. It has been demonstrated that asTF does not play a significant role during coagulation due to the truncation of the extracellular domain encoded by exon 5, but contributes to tumor-associated angiogenesis and cancer growth [11, 15–17]. A previous study suggested a paradigm for the role of flTF by interacting with FVIIa to affect angiogenesis through its cytoplasmic domain and PAR-2 activation [13]. However, unlike flTF, asTF does not affect angiogenesis via PAR-dependent pathways but relies on integrin ligation [18]. Currently, the role of flTF and asTF levels in human cancers remains elusive. Rollin et al. [19] demonstrated that the transcript level of asTF was an independent prognostic marker in NSCLC. Our data showed that both flTF and asTF were over-expressed on gastric cancer tissues, and their expression significantly associated with prognosis. We also analyzed the correlation between both flTF and asTF expression in gastric cancer and patients’ clinico-pathological characteristics such as gender, age, histologic grade, TNM stage, pathologic type. Except age, we found that flTF and asTF did not significantly associate with any clinical patient parameters.
Pre-mRNA splicing is an essential, ubiquitous, and precisely regulated process that occurs following gene transcription and before mRNA translation [20]. Alternative splicing can generate a variety of different transcripts from a single gene. Alternative splicing represents an important molecular mechanism of gene regulation in a series of physiological processes, including developmental programming, disease, and even cancer [21]. Many tumor-associated splice variants have clear diagnostic value and may serve as potential drug targets [22]. Thus, understanding the process of aberrant splicing and the detailed characterization of the splice variants may improve our understanding of malignant transformation targeting TF involved in gastric cancer progression and metastasis.
In this study, we established a set of self-designed asTF primers and TaqMan probe to detect asTF transcripts (Table 4). Our self-designed asTF forward primer is located at the junction of exon 4 and exon 6 of TF. As demonstrated in the previous literature [23], the asTF forward and reverse primers were located at the exon 4 and exon 6, respectively, and the asTF TaqMan probe was located at the junction of exon 4 and exon 6 of TF. According to this method, the pair of primers of asTF can amplify a special fragment of asTF, while it can also amplify the fragment of flTF containing exon 5. This suggests a primer competition leading to a decrease of the amplification efficiency of this pair of primers. Herein, we selected the gastric cancer tissues, used the asTF primers and TaqMan probes designed by ourselves as well as adopted from the literature respectively, for the real-time PCR assay. The PCR products were then determined in the 2% agarose electrophoresis (as shown in Figure 1), indicating an optimal system for our self-designed primers and TaqMan probe to detect asTF transcripts.
Table 4: Sequences of primers and probes
Genes |
Sequences (5’→3’) |
|---|---|
flTF (ref. [14]) |
|
Forward primer |
TGATGTGGATAAAGGAGAAAACTACTG |
Reverse primer |
CTACCGGGCTGTCTGTACTCTTC |
Probe |
FAM-TTCAAGCAGTGATTCCCTCCCGAACA-TAMRA |
asTF (ref. [14]) |
|
Forward primer |
GGGATGTTTTTGGCAAGGACTTA |
Reverse primer |
CCAGGATGATGACAAGGATGATG |
Probe |
FAM-AATCTTCAAGTTCAGGAAAGAAATATTCTACATCATTGGA-TAMRA |
asTF(self-designed) |
|
Forward primer |
ATCTTCAAGTTCAGGAAAGAAATATTCTAC |
Reverse primer |
GCTCTGCCCCACTCCTGCC |
Probe |
FAM-TTGGAGCTGTGGTATTTGTGGTCATCATC-TAMRA |
β-actin |
|
Forward primer |
GGAAGGTGAAGGTCGGAGTC |
Reverse primer |
CGTTCTCAGCCTTGACGGT |
Probe |
FAM-TTTGGTCGTATTGGGCGCCTG-TANRA |
In the present study, the multi-factor COX model was used to analyze the prognostic value of flTF and asTF expression in gastric cancer patients. The COX model included the age, gender, stage, histological grade, TNM stage, pathologic type, and flTF/asTF mRNA expression level. Our study showed that both flTF and asTF mRNA expression levels could be used as independent prognostic factors, supporting the notion that flTF and asTF levels in gastric cancer have important prognosis values.
MATERIALS AND METHODS
Patients and tissue samples
Gastric cancer tissues were collected from 52 patients who underwent surgical resection between January 2001 and April 2015 at our hospital (34 men and 18 women; median age at diagnosis, 58 years). No patients received pre-operative chemotherapy or radiotherapy. All gastric cancer tissues were confirmed as gastric adenocarcinoma by hematoxylin and eosin (H&E) staining after surgical resection, and cancer stages were assigned according to criteria established by the American Joint Committee on Cancer [24]. Moreover, 10 cases of adjacent normal tissues were analyzed as control samples. Detailed patient clinical parameters are shown in Table 1. The study protocol was approved by the ethics committee of the hospital.
RNA isolation and reverse transcription
Total RNA in gastric tissues was extracted by using a total RNA purification kit (Biocolor BioScience and Technology Company, Shanghai, China) following the manufacturer’s protocol. The quality of the RNA samples was determined by absorbance measurements at 260/280 nm. Two μg of total RNA was reverse transcribed to cDNA using the first strand cDNA synthetic kit (Fermantas, Vilnius, Lithuania) according to the manufacturer’s instructions. cDNA standards were amplified by conventional PCR and the PCR product was purified by agarose-gel electrophoresis. DNA standards were extracted using the EZ-10 spin column DNA gel extraction kit (Sangon Biological Engineer Technology and Services Limited Corporation, Shanghai, China).
Real-time PCR
All real-time PCR reactions were performed in the ABI 7500 (Applied Biosystem, USA) using a final volume of 20μl. Reactions were performed with 10μl of 2x TaqMan® Universal PCR Master Mix PCR buffer, 2μl of 5μM forward primer, 2μl of 5μM reverse primer, 2μl of 2.5μM TaqMan probe, 2μl template cDNA, and 2μl ddH2O. The primers and TaqMan probes used to identify flTF were adapted from Szotowki et al. [23]. The primers and TaqMan probes of asTF and the reference gene GAPDH were designed according to the National Center for Biotechnology Information (NCBI) database by using the Primer Primier 5.0 software (Palo Alto, CA, USA). The forward primer of asTF was located at the junction of exon 4 and exon 6, which is different from the design of the reference [23]. The sequences of all primers and TaqMan probes used in the present study were listed in Table 4. The cycling conditions for flTF and asTF were as follows: pre-denaturation at 50ºC for 2 min, initial denaturation at 95ºC for 10 min, followed by 40 cycles at 95ºC for 15 sec and 60ºC for 1 min, collecting the fluorescence signal at 60ºC. The data were normalized to GAPDH, and relative expression was calculated by the 2-ΔΔCT method.
Statistical analyses
Statistical analyses were performed using the GraphPad Prism 4.0 software package (GraphPad Software, Inc., San Diego, USA). Paired Student’s t-test, Wilcoxon signed rank test, or the log rank survival analysis were used where appropriate. A p-value of <0.05 was determined as statistically significant.
ACKNOWLEDGMENTS
This work was supported by grants from the National Natural Science Foundation of China (No. 81301960, 81302585, 31428005, 31570877 and 31570908), the Key R&D Project of Science and Technology Department of Jiangsu Province (BE2015633), Changzhou High-Level Medical Talents Training Project (No. 2016CZBJ001).
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016; 66:115-132.
2. Jiang J, Zhu Y, Wu C, Shen Y, Wei W, Chen L, Zheng X, Sun J, Lu B, Zhang X. Tumor expression of B7-H4 predicts poor survival of patients suffering from gastric cancer. Cancer Immunol Immunother. 2010; 59:1707-1714.
3. Chen L, Luo G, Tan Y, Wei J, Wu C, Zheng L, Zhang X, Xu N. Immunolocalisation of tissue factor in esophageal cancer is correlated with intratumoral angiogenesis and prognosis of the patient. Acta Histochem. 2010; 112:233-239.
4. Eisenreich A, Bolbrinker J, Leppert U. Tissue Factor: A Conventional or Alternative Target in Cancer Therapy. Clin Chem. 2016; 62:563-70.
5. Callander NS, Varki N, Rao LV. Immunohistochemical identification of tissue factor in solid tumors. Cancer. 1992; 70:1194-1201.
6. van den Berg YW, Osanto S, Reitsma PH, Versteeg HH. The relationship between tissue factor and cancer progression: insights from bench and bedside. Blood. 2012; 119:924-932.
7. Yu JL, May L, Lhotak V, Shahrzad S, Shirasawa S, Weitz JI, Coomber BL, Mackman N, Rak JW. Oncogenic events regulate tissue factor expression in colorectal cancer cells: implications for tumor progression and angiogenesis. Blood. 2005; 105:1734-1741.
8. Milsom CC, Yu JL, Mackman N, Micallef J, Anderson GM, Guha A, Rak JW. Tissue factor regulation by epidermal growth factor receptor and epithelial-to-mesenchymal transitions: effect on tumor initiation and angiogenesis. Cancer Res. 2008; 68:10068-10076.
9. Rong Y, Belozerov VE, Tucker-Burden C, Chen G, Durden DL, Olson JJ, Van Meir EG, Mackman N, Brat DJ. Epidermal growth factor receptor and PTEN modulate tissue factor expression in glioblastoma through JunD/activator protein-1 transcriptional activity. Cancer Res. 2009; 69:2540-2549.
10. Bogdanov VY, Balasubramanian V, Hathcock J, Vele O, Lieb M, Nemerson Y. Alternatively spliced human tissue factor: a circulating, soluble, thrombogenic protein. Nat Med. 2003; 9:458-462.
11. Signaevsky M, Hobbs J, Doll J, Liu N, Soff GA. Role of alternatively spliced tissue factor in pancreatic cancer growth and angiogenesis. Semin Thromb Hemost. 2008; 34:161-169.
12. Unruh D, Unlu B, Lewis CS, Qi X, Chu Z, Sturm R, Keil R, Ahmad SA, Sovershaev T, Adam M, Van Dreden P, Woodhams BJ, Ramchandani D, et al. Antibody-based targeting of alternatively spliced tissue factor: a new approach to impede the primary growth and spread of pancreatic ductal adenocarcinoma. Oncotarget. 2016;7:25264-75. doi: 10.18632/oncotarget.7955.
13. Kasthuri RS, Taubman MB, Mackman N. Role of tissue factor in cancer. J Clin Oncol. 2009; 27:4834-4838.
14. Liu Y, Jiang P, Capkova K, Xue D, Ye L, Sinha SC, Mackman N, Janda KD, Liu C. Tissue factor-activated coagulation cascade in the tumor microenvironment is critical for tumor progression and an effective target for therapy. Cancer Res. 2011; 71:6492-6502.
15. Censarek P, Bobbe A, Grandoch M, Schror K, Weber AA. Alternatively spliced human tissue factor (asHTF) is not pro-coagulant. Thromb Haemost. 2007; 97:11-14.
16. Boing AN, Hau CM, Sturk A, Nieuwland R. Human alternatively spliced tissue factor is not secreted and does not trigger coagulation. J Thromb Haemost. 2009; 7:1423-1426.
17. Kocaturk B, Tieken C, Vreeken D, Unlu B, Engels CC, de Kruijf EM, Kuppen PJ, Reitsma PH, Bogdanov VY, Versteeg HH. Alternatively spliced tissue factor synergizes with the estrogen receptor pathway in promoting breast cancer progression. J Thromb Haemost. 2015; 13:1683-1693.
18. van den Berg YW, van den Hengel LG, Myers HR, Ayachi O, Jordanova E, Ruf W, Spek CA, Reitsma PH, Bogdanov VY, Versteeg HH. Alternatively spliced tissue factor induces angiogenesis through integrin ligation. Proc Natl Acad Sci U S A. 2009; 106:19497-19502.
19. Rollin J, Regina S, Gruel Y. Tumour expression of alternatively spliced tissue factor is a prognostic marker in non-small cell lung cancer. J Thromb Haemost. 2010; 8:607-610.
20. Venables JP. Aberrant and alternative splicing in cancer. Cancer Res. 2004; 64:7647-7654.
21. Korner M, Miller LJ. Alternative splicing of pre-mRNA in cancer: focus on G protein-coupled peptide hormone receptors. Am J Pathol. 2009; 175:461-472.
22. Brinkman BM. Splice variants as cancer biomarkers. Clin Biochem. 2004; 37:584-594.
23. Szotowski B, Goldin-Lang P, Antoniak S, Bogdanov VY, Pathirana D, Pauschinger M, Dorner A, Kuehl U, Coupland S, Nemerson Y, Hummel M, Poller W, Hetzer R, et al. Alterations in myocardial tissue factor expression and cellular localization in dilated cardiomyopathy. J Am Coll Cardiol. 2005; 45:1081-1089.
24. Strong VE, D’Amico TA, Kleinberg L, Ajani J. Impact of the 7th Edition AJCC staging classification on the NCCN clinical practice guidelines in oncology for gastric and esophageal cancers. J Natl Compr Canc Netw. 2013;11:60-6.