
INTRODUCTION
Lung cancer is the most frequent cause of cancer-related death worldwide, with non-small cell lung cancer (NSCLC) being the most common type [1, 2]. Improved understanding of genetic alteration in lung cancer has led to the development of many onco-targeted drugs and significant achievements [3–5].
Activating mutations of epidermal growth factor receptor (EGFR) are identified in about 20% of lung adenocarcinomas in Western countries [6] and 40%–60% of lung adenocarcinomas in East Asia [7–9]. These mutations, which mainly consist of EGFR exon 19 deletion (~50%) and exon 21 L858R mutation (~40%), are highly responsive to EGFR–tyrosine kinase inhibitors (EGFR–TKIs), such as gefitinib and erlotinib [4, 10, 11]. However, for stage III patients with EGFR mutations who received radical surgery, the adjuvant therapy that provides better results remains unclear.
As a unique pathological morphology, the micropapillary pattern (MPP) has drawn increasing attention in recent years. The micropapillary structure, which has been described as highly invasive and metastatic, is predictive of poor prognosis. Meanwhile, the suitability of the result for EGFR mutation remains unclear, and the prognostic value of MPP remains inconclusive in advanced-stage lung adenocarcinoma.
In the present study, we retrospectively investigated the clinicopathologic characteristics and prognosis of patients with activating EGFR exon mutations in a large cohort of patients with lung adenocarcinoma. We found that patients with exon 19 and the MPP pathological type had longer overall survival (OS), compared with those harboring exon 21 mutation or the non-MPP pathological type; in addition, patients with exon 19 mutation exhibited a better response to EGFR–TKIs, compared with patients with exon 21 mutation.
RESULTS
A total of 1,801 patients with lung adenocarcinoma diagnosed from January 2011 to December 2014 were screened for EGFR mutation status. Among these patients, 678 (37.6%) harbored mutations in EGFR; of this number, 636 (93.8% of 678) cases with classic activating mutations (exon 19 or exon 21 mutations) and 42 (6.2% of 678) cases with rare mutations (exon 18 or exon 20 mutations) were detected.
Of the 636 patients with activating mutations of EGFR exon, 168 were tumor-node-metastasis (TNM) stage III cases who received radical surgery. These patients had a median follow-up duration of 30 months (range: 4–61 months). Of the 168 cases, 79 (47.02%) were carrying EGFR exon 19 mutations, 65 (38.7%) were over 60 years old, and 109 (64.9%) were never-smokers. The predominant pathological subtype included 89 (53.0%) cases with MPP (Figure 1). No significant differences were found between the patients carrying EGFR exon 19 mutation and those with EGFR exon 21 mutation with respect to gender, age, smoking history, Karnofsky Performance Status (KPS) score, TNM stage, and pathological types (Table 1).
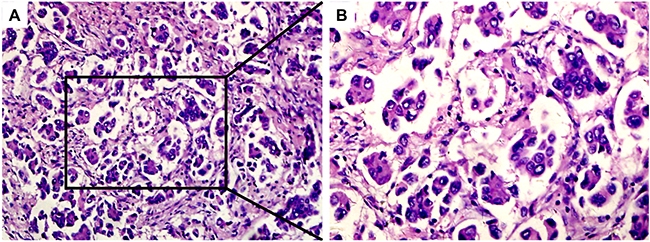
Figure 1: Hematoxylin–eosin staining of MPP-positive specimens. MPP-predominant specimen (A, ×100 magnification; B, ×200 magnification).
Table 1: Comparison of clinical characteristics between NSCLCs harboring EGFR exon 19 and EGFR exon 21 mutation
Characteristics |
Total |
Exon 19 |
Exon 21 |
P |
|---|---|---|---|---|
N. of patients |
168 |
79 |
89 |
|
Age, years |
||||
≤60 |
103 |
49 |
54 |
0.858 |
>60 |
65 |
30 |
35 |
|
Sex |
||||
Male |
57 |
26 |
31 |
0.793 |
Famale |
111 |
53 |
58 |
|
Smoking status |
||||
Ever |
59 |
26 |
33 |
0.572 |
Never |
109 |
53 |
56 |
|
KPS score |
||||
>80 |
113 |
48 |
65 |
0.091 |
≤80 |
55 |
31 |
24 |
|
TNM stage |
||||
IIIA |
154 |
74 |
80 |
0.376 |
IIIB |
14 |
5 |
9 |
|
Pathological type |
||||
MPP |
99 |
49 |
50 |
0.737 |
Non-MPP |
62 |
29 |
33 |
|
Unknown |
7 |
1 |
6 |
|
First-line treatment |
||||
TKI |
31 |
18 |
13 |
0.167 |
Non-TKI |
131 |
58 |
73 |
|
Unknown |
6 |
3 |
3 |
|
First-line treatment |
||||
Thoracic RT |
21 |
11 |
10 |
0.568 |
Non-Thoracic RT |
140 |
64 |
76 |
|
Unknown |
7 |
4 |
3 |
|
TKI |
||||
Yes |
58 |
32 |
26 |
0.124 |
No |
110 |
47 |
63 |
|
Thoracic RT |
||||
Yes |
30 |
13 |
17 |
0.655 |
No |
138 |
66 |
72 |
Among all 168 patients with EGFR mutations, EGFR status (p=0.023), KPS score (p<0.001), and pathological type (p<0.001) were significantly associated with OS; KPS score (p<0.001) and first-line treatment (p=0.032) were significantly correlated with worse progression-free survival (PFS). In multivariate analysis incorporating EGFR status, KPS score, and pathological type, EGFR status (hazard ratio=1.681, 95% confidence interval: 1.075–2.629, p=0.023), KPS score (hazard ratio=0.053, 95% confidence interval: 0.018–0.157, p<0.001), and pathological type (hazard ratio=0.357, 95% confidence interval: 0.148–0.860, p=0.022) were the independent predictors for OS. In multivariate analysis incorporating KPS score and first-line treatment, KPS score (hazard ratio=0.148, 95% confidence interval: 0.087–0.253, p<0.001), and first-line treatment (hazard ratio=0.442, 95% confidence interval: 0.210–0.931, p=0.032) were the independent predictors for PFS (Figure 2, Tables 2 and 3).
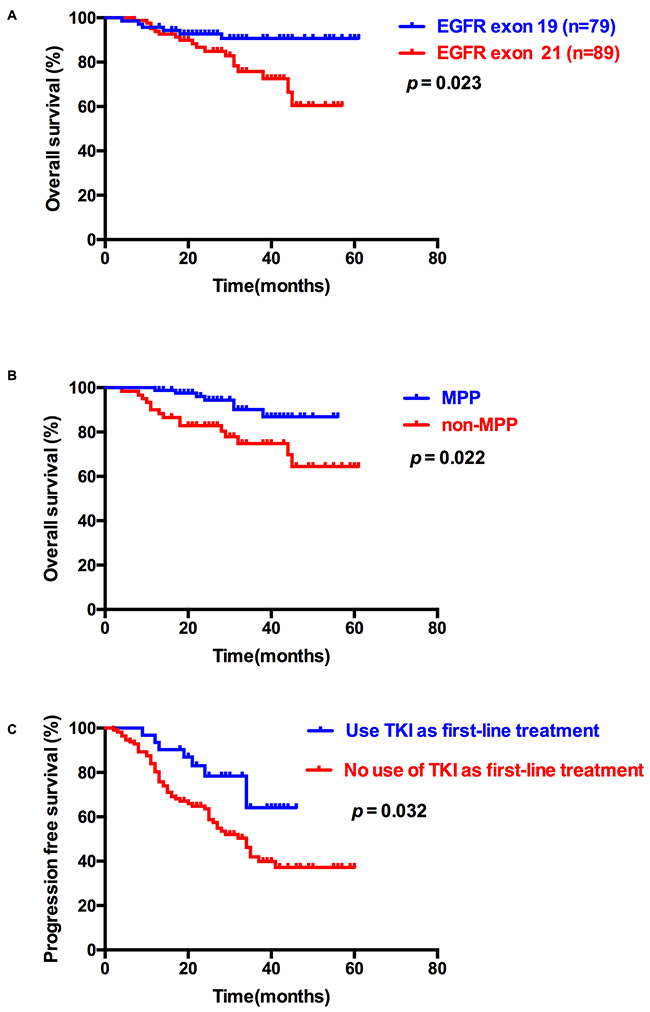
Figure 2: Overall survival (OS) and progression-free survival (PFS) of patients with classic EGFR mutations. (A) Kaplan–Meier survival curves for OS analyses between EGFR exon 19 and 21 mutations. (B) Kaplan–Meier survival curves for OS analyses between MPP and non-MPP. (C) Kaplan–Meier survival curves for PFS analyses between TKI and non-TKI as first-line treatment.
Table 2: Overall survival analysis of the whole 168 patients
Univariate analysis |
Multivariate analysis |
|||
|---|---|---|---|---|
P |
HR(95% CI) |
P |
HR(95% CI) |
|
EGFR |
||||
Exon 19 |
0.046 |
1.00 |
0.023 |
1.00 |
Exon 21 |
1.562(1.009-2.417) |
1.681(1.075-2.629) | ||
Age |
||||
≤60 |
0.966 |
1.00 |
||
>60 |
1.018(0.456-2.272) |
|||
Sex |
||||
Male |
0.782 |
1.00 |
||
Famale |
0.888(0.383-2.059) |
|||
Smoking status |
||||
Never |
0.381 |
1.00 |
||
Ever |
1.431(0.642-3.190) |
|||
KPS score |
||||
≤80 |
<0.001 |
1.00 |
<0.001 |
1.00 |
>80 |
0.044(0.015-0.128) |
0.053(0.018-0.157) | ||
TNM stage |
||||
IIIA |
0.834 |
1.00 |
||
IIIB |
0.857(0.202-3.638) |
|||
Pathological type |
||||
Non-MPP |
0.025 |
1.00 |
0.022 |
1.00 |
MPP |
0.372(0.157-0.881) |
0.357(0.148-0.860) | ||
TKI |
||||
Yes |
0.847 |
1.00 |
||
No |
1.082(0.486-2.411) |
|||
Thoratic RT |
||||
Yes |
0.068 |
1.00 |
||
No |
0.399(0.149-1.069) |
|||
Abbreviations: OS: overall survival; HR: hazard radio; MPP: micropapillary pattern; RT: radiotherapy; TKI: Tyrosine Kinase Inhibitor.
Table 3: Progression free survival analysis of the whole 168 patients
Univariate analysis |
Multivariate analysis |
|||
|---|---|---|---|---|
P |
HR(95% CI) |
P |
HR(95% CI) |
|
EGFR |
||||
Exon 19 |
0.531 |
1.00 |
||
Exon 21 |
1.082(0.845-1.386) |
|||
Age |
||||
≤60 |
0.393 |
1.00 |
||
>60 |
1.252(0.747-2.099) |
|||
Sex |
||||
Male |
0.969 |
1.00 |
||
Famale |
0.990(0.583-1.679) |
|||
Smoking status |
||||
Ever |
0.762 |
1.00 |
||
Never |
0.921(0.543-1.564) |
|||
KPS score |
||||
>80 |
<0.001 |
1.00 |
<0.001 |
1.00 |
≤80 |
0.147(0.087-0.249) |
0.148(0.087-0.253) | ||
TNM stage |
||||
IIIA |
0.194 |
1.00 |
||
IIIB |
0.464(0.145-1.479) |
|||
Pathological type |
||||
MPP |
0.477 |
1.00 |
||
Non-MPP |
0.831(0.498-1.386) |
|||
First-line treatment |
||||
Non-TKI |
0.021 |
1.00 |
0. 032 |
1.00 |
TKI |
0.418(0.199-0.848) |
0.442(0.210-0.931) | ||
First-line treatment |
||||
RT |
0.759 |
1.00 |
||
Non-RT |
0.884(0.403-1.940) |
|||
Abbreviations: PFS: progression free survival; HR: hazard radio; MPP: micropapillary pattern; RT: radiotherapy; TKI: Tyrosine Kinase Inhibitor.
The results demonstrated that the patients carrying exon 19 mutation had a better OS than those carrying exon 21 mutation; thus, we divided the patients into 2 subgroups: patients with EGFR exon 19 mutation and patients with EGFR exon 21 mutation. For patients with EGFR exon 19 mutation, treatment (thoracic radiotherapy or not, p=0.045), and pathological type (p=0.016) were significantly associated with OS; KPS score (p<0.001) and first-line treatment (TKI or not, p=0.008) were significantly associated with PFS. In multivariate analysis incorporating treatment (thoracic radiotherapy or not) and pathological type, pathological type (hazard ratio=0.073, 95% confidence interval: 0.009–0.611, p=0.016) was the independent predictors of OS. In multivariate analysis incorporating KPS score and first-line treatment (TKI or not), KPS score (hazard ratio=0.120, 95% confidence interval: 0.047–0.307, p<0.001) and first-line treatment (TKI or not, hazard ratio=0.109, 95% confidence interval: 0.014-0.828, p=0.032) were the independent predictors of OS (Tables 4 and 5). For patients with EGFR exon 21 mutation, KPS score (p<0.001) and treatment (TKI or not, p=0.025) were significantly associated with OS, and KPS score (p<0.001) was significantly associated with PFS. In multivariate analysis incorporating KPS score and treatment (TKI or not), KPS score (hazard ratio=0.067, 95% confidence interval: 0.022–0.207, p<0.001) was the independent predictor of OS (Figure 3 and Supplementary Figure 1, Tables 4 and 5).
Table 4: Overall survival analysis of patients with exon 19 mutation and exon 21 mutation seperately
EGFR exon 19 |
EGFR exon 21 |
|||||||
|---|---|---|---|---|---|---|---|---|
Univariate analysis |
Multivariate analysis |
Univariate analysis |
Multivariate analysis |
|||||
P |
HR(95% CI) |
P |
HR(95% CI) |
P |
HR(95% CI) |
P |
HR(95% CI) |
|
Age |
||||||||
≤60 |
0.635 |
1.00 |
0.528 |
1.00 |
||||
>60 |
1.437 (0.321-6.420) |
0.733 (0.279-1.925) |
||||||
Sex |
||||||||
Male |
0.496 |
1.00 |
0.966 |
1.00 |
||||
Famale |
0.594 (0.133-2.658) |
0.997 (0.354-2.810) |
||||||
Smoking status |
||||||||
Never |
0.503 |
1.00 |
0.556 |
1.00 |
||||
Ever |
1.669 (0.373-7.459) |
1.332 (0.513-3.454) |
||||||
KPS score |
||||||||
≤80 |
0.181 |
1.00 |
<0.001 |
1.00 |
<0.001 |
1.00 | ||
>80 |
0.002 (0.000-17.332) |
0.062 (0.020-0.190) |
0.067 (0.022-0.207) | |||||
TNM stage |
||||||||
IIIA |
0.655 |
1.00 |
0.783 |
1.00 |
||||
IIIB |
0.045 (0-36089) |
0.813 (0.186-3.545) |
||||||
Pathological type |
||||||||
Non-MPP |
0.032 |
1.00 |
0.016 |
1.00 |
0.371 |
1.00 |
||
MPP |
0.099 (0.012-0.822) |
0.073 (0.009-0.611) |
0.634 (0.234-1.720) |
|||||
TKI |
||||||||
Yes |
0.123 |
1.00 |
0.025 |
1.00 |
0.103 |
1.00 | ||
No |
0.189 (0.023-1.573) |
3.032 (1.146-8.022) |
2.265 (0.847-6.056) | |||||
RT |
||||||||
Yes |
0.045 |
1.00 |
0.059 |
1.00 |
0.357 |
1.00 |
||
No |
0.216 (0.048-0.969) |
0.128 (0.015-1.081) |
0.497 (0.112-2.202) |
|||||
Abbreviations: OS: overall survival; HR: hazard radio; MPP: micropapillary pattern; RT: radiotherapy; TKI: Tyrosine Kinase Inhibitor.
Table 5: Progression free survival analysis of patients with exon 19 mutation and exon 21 mutation seperately
EGFR exon 19 |
EGFR exon 21 |
|||||||
|---|---|---|---|---|---|---|---|---|
Univariate analysis |
Multivariate analysis |
Univariate analysis |
Multivariate analysis |
|||||
P |
HR(95% CI) |
P |
HR(95% CI) |
P |
HR(95% CI) |
P |
HR(95% CI) |
|
Age |
||||||||
≤60 |
0.722 |
1.00 |
0.130 |
1.00 |
||||
>60 |
1.152 (0.529-2.508) |
0.584 (0.292-1.172) |
||||||
Sex |
||||||||
Male |
0.959 |
1.00 |
0.935 |
1.00 |
||||
Famale |
0.980 (0.452-2.126) |
0.970 (0.466-2.019) |
||||||
Smoking status |
||||||||
Ever |
0.731 |
1.00 |
0.467 |
1.00 |
||||
Never |
1.145 (0.528-2.484) |
0.762 (0.367-1.584) |
||||||
KPS score |
||||||||
>80 |
<0.001 |
1.00 |
<0.001 |
1.00 |
<0.001 |
1.00 |
||
≤80 |
0.082 (0.032-0.211) |
0.120 (0.047-0.307) |
0.208 (0.106-0.410) |
|||||
TNM stage |
||||||||
IIIA |
0.651 |
1.00 |
0.201 |
1.00 |
||||
IIIB |
0.629 (0.084-4.711) |
0.394 (0.095-1.643) |
||||||
Pathological type |
||||||||
Non-MPP |
0.324 |
1.00 |
0.979 |
1.00 |
||||
MPP |
0.682 (0.319-1.459) |
0.991 (0.492-1.991) |
||||||
First-line treatment |
||||||||
Non-TKI |
0.008 |
1.00 |
0.032 |
1.00 |
0.603 |
1.00 |
||
TKI |
0.067 (0.009-0.492) |
0.109 (0.014-0.828) |
1.246 (0.544-2.854) |
|||||
First-line treatment |
||||||||
RT |
0.585 |
1.00 |
0.889 |
1.00 |
||||
Non-RT |
0.716 (0.216-2.377) |
1.077 (0.380-3.053) |
||||||
Abbreviations: PFS: progression free survival; HR: hazard radio; MPP: micropapillary pattern; RT: radiotherapy; TKI: Tyrosine Kinase Inhibitor.
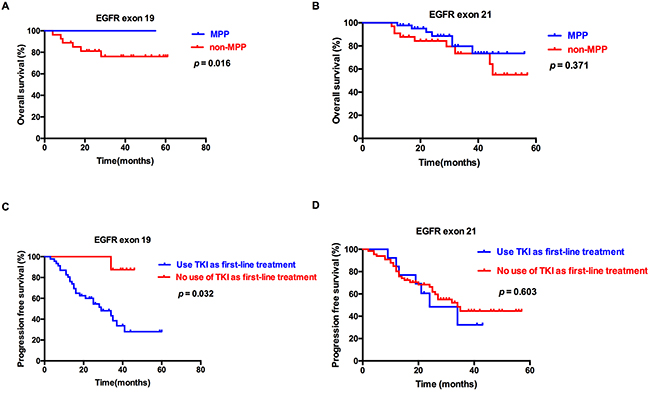
Figure 3: Overall survival (OS) and progression-free survival (PFS) of patients with EGFR exon 19 and 21mutations. Kaplan–Meier survival curves for OS between MPP and non-MPP for patients with EGFR exon 19 (A) and EGFR exon 21 (B) mutations. Kaplan–Meier survival curves for PFS between TKI and non-TKI as first-line treatment for patients with EGFR exon 19 (C) and EGFR exon 21 (D) mutations.
We then separated the 168 patients into 4 subgroups: patients with EGFR exon 19 mutation and showing MPP in pathological type, patients with EGFR exon 19 mutation and showing non-MPP in pathological type, patients with EGFR exon 21 mutation and MPP in pathological type, and patients with EGFR exon 21 mutation and non-MPP in pathological type. Notably, patients with EGFR exon 19 mutation and MPP in pathological type had the longest OS (53.72 months), whereas patients with EGFR exon 21 mutation and non-MPP in pathological type had the shortest OS (44.9 months, p=0.033, Table 6 and Figure 4). This result demonstrated that lung adenocarcinoma with EGFR exon 19 mutation and MPP in pathological type may be good prognostic factors for OS.
Table 6: Overall survival analysis of four subgroups
Group |
OS (months) |
SD |
95% CI |
|---|---|---|---|
EGFR exon 19 + MPP |
53.72 |
1.26 |
51.24-56.20 |
EGFR exon 19 + non-MPP |
49.85 |
4.02 |
41.96-57.73 |
EGFR exon 21 + MPP |
48.50 |
2.50 |
43.60-53.40 |
EGFR exon 21 + non-MPP |
44.90 |
3.29 |
38.45-51.36 |
Abbreviations: MPP: micropapillary pattern.
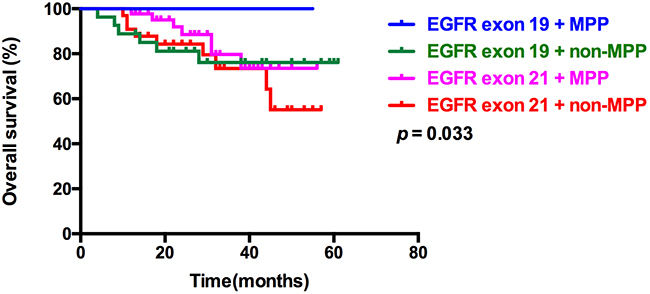
Figure 4: Kaplan–Meier survival curves for OS among 4 subgroups, based on EGFR mutation types and pathological types. Kaplan–Meier survival curves for OS among 4 subgroups: EGFR exon 19 mutation and MPP, EGFR exon 19 mutation and non-MPP, EGFR exon 21 mutation and MPP, and EGFR exon 21 mutation and non-MPP.
DISCUSSION
In our study, survival analysis results indicated significant differences in OS between EGFR exon 19 mutation and EGFR exon 21 mutation. Comparison of the Kaplan–Meier curves suggested that the OS of patients with exon 19 mutation was longer than those with exon 21 mutation. However, no significant differences in PFS were indicated between patients with exon 19 mutation and those with exon 21 mutation. Our results indicated that exon 19 mutation may be an indicator of good prognosis compared with exon 21 mutation, which is similar to previous reports [12]. Further investigations are required to address these differences.
As a unique pathological morphology, lung adenocarcinoma with a micropapillary pattern (MPPAC) has drawn increased attention from researchers in recent years. The cells of MPPAC are small, cube-shaped, budding with clustered growth, and lack fibrovascular development. Researchers have discovered that the structure appears in various tumors, such as breast cancer [13], bladder cancer [14], colorectal cancer [15], and ovarian cancer [16]. According to published studies, MPPAC most commonly occur in males and nonsmokers and is associated with lymphatic invasion, pleural invasion, and lymph node metastases [13, 17].
MPP has been verified to be an unfavorable prognostic marker in early-stage lung adenocarcinoma egardless of cohorts [18–21]. However, the role of MPP with regard to prognosis remains inconclusive in advanced-stage lung adenocarcinoma. Zhang et al. have reported that MPA (5% of MPP) had statistically worse recurrence-free survival, compared with nonmicropapillary-predominant adenocarcinoma with MPP observed in 5% of stage I patients; a similar correlation was not found in stage II–III patients [22]. Campos-Parra et al. have indicated that high-grade adenocarcinoma (micropapillary-, papillary-, and solid-predominant) is associated with better survival, compared with intermediate-grade adenocarcinoma (lepidic- and acinar-predominant) in advanced adenocarcinoma (stages IIIB and IV); the median PFS and OS were 6.4 vs. 5.5 months (p= 0.009) and 25 vs. 16.8 months (p= 0.023), respectively. For this result, they considered that a better response to chemotherapy probably contributed to this phenomenon [23]. Subsequently, Clay et al. have shown that MPP is not a predictor of unfavorable survival in stage III–IV [24]. By contrast, Warth A et al. have indicated that the presentation of MPP is a predictor of unfavorable outcome in not only early-stage adenocarcinoma but late-stage adenocarcinoma as well [25].
Previous studies have investigated the prognostic value of lung adenocarcinoma with an MPP, compared with those without such a pattern, or micropapillary-predominant lung adenocarcinoma compared with other histologic subtypes. However, as far as we were concerned, this study represents the first comparison study between MPP-positive adenocarcinoma and MPP-negative adenocarcinoma in EGFR exon 19 and 21 mutations of TNM stage III lung adenocarcinoma with regard to clinicopathologic characteristics and prognosis.
In the current study, we included patients with stage III lung adenocarcinoma who received radical surgery harboring EGFR exon 19 or 21. Notably, MPP was a good prognosis predictor for patients with EGFR exon 19 mutation, which varies from the results previous reported. We further divided the patients into 4 subgroups according to EGFR mutation types and pathological types; patients with exon 19 mutation and MPP had the longest OS, while those with exon 21 mutation and MPP negative had the worst OS. The differences may be attributed to better response to and better PFS from chemotherapy (61.76% vs. 37.5%) and TKIs (86.67% vs. 75%); this finding is similar to the results in a previous study in which patients with MPP harboring EGFR mutations had better survival when they received TKI treatment, compared with those with either no treatment [22].
The current study includes several limitations. First, the finding that patients with MPP pathological type had a significantly worse OS than those without MPP pathological type was based on a small number of patients and thus needs to be validated in a larger study. Second, we used cDNA-PCR sequencing as the experimental method to identify mutations; results might change if more sensitive methods are used.
In conclusion, our data analyzed risk factors of TNM stage III lung adenocarcinoma with EGFR mutations in exon 19 or 21 after radical surgery. Our results demonstrated that patients with exon 19 mutation had a better OS and were more sensitive to EGFR–TKI than those with exon 21 mutation. For patients with exon 19 mutation, the MPP pathological type may indicate good prognosis. These results may be useful in the treatment of patients with classic EGFR exon mutations.
MATERIALS AND METHODS
Patients and samples
From January 2011 to December 2014, we consecutively collected lung tumors resected in the Department of Pulmonary Surgery at Tianjin Medical University in Tianjin, China. Inclusion criteria for this study were as follows: (1) Patients underwent complete resection, and (2) Specimens were pathologically confirmed as lung adenocarcinomas with sufficient tissue for comprehensive mutational analyses. Pathologic slides were reviewed by 3 certified pathologists (Yan Qingna, Li Qi, and Sun Leina) to classify histologic subtypes of lung adenocarcinomas according to the International Association for the Study of Lung Cancer/The American Thoracic Society/The European Respiratory Society (IASLC/ATS/ERS) multidisciplinary classification system. The following clinicopathologic parameters for each patient were also collected: gender, age at diagnosis, smoking history, systemic treatment, pathological type, and TNM stage in line with the seventh edition of the lung cancer staging system. The PFS and OS of patients diagnosed from January 2011 to December 2014 were recorded based on a follow-up clinic visit or a telephone call.
Mutational analysis
After frozen tumor specimens were dissected in TRIzol reagent (Invitrogen, Carlsbad, CA, USA), DNA and RNA were extracted per standard protocol, and the RNA was reverse-transcribed into cDNA with the use of the PrimeScript RT Reagent Kit (TaKaRa, Dalian, China). EGFR (exons 18–21) were routinely amplified by PCR using cDNA. Direct dideoxynucleotide sequencing was then performed to analyze the amplified products. The EGFR (exons 18–21)-amplified products obtained by PCR using DNA for sequencing were used to confirm the uncommon EGFR mutations.
Statistical analysis
Pearson’s χ2 test was used to investigate the correlations between 2 categorical variables. PFS and OS distribution was analyzed using the Kaplan–Meier method, and log-rank tests were employed for comparison of PFS or OS between 2 categories in univariate analysis. Multivariate survival analysis was conducted using Cox proportional hazards regression to identify independent prognostic factors. Data were statistically analyzed using SPSS 21.0 (Abbott Laboratories, North Chicago, IL, USA). Statistical significance was set at p < 0.05.
Ethics statement
This study was approved by the institutional review board at Tianjin Medical University. Written informed consent was obtained from each patient to allow their biological samples to be genetically analyzed. The experimental protocol of this study was performed strictly in accordance with the guidelines.
Abbreviations
NSCLC: non-small cell lung cancer; TNM: tumor-node-metastasis; MPPAC: adenocarcinoma with micropapillary pattern; MPP: micropapillary pattern; TKI: tyrosine kinase inhibitors; EGFR: Epidermal growth factor receptor; OS: overall survival; PFS: progression free survival; IASLC/ATS/ERS: International Association for the Study of Lung Cancer, the American Thoracic Society, and the European Respiratory Society.
Authors’ contributions
Zhang Tian and Wang Jing designed this study, performed experiments and wrote the main manuscript. Su Yanjun performed some of the surgical operations. Yan Qingna, Li Qi and Sun leina reviewed the pathologic slides and collected the pathologic data. Chen Xi, Wang Yuwen and Er Puchun collected the clinical data, tumor samples and performed experiments. Pang Singsong and Wang Ping designed and directed the overall project. All authors reviewed the manuscript.
ACKNOWLEDGMENTS
We thank for the funding support from the National Natural Science Foundation of China (81372518 to Wang Ping) and Key Technology R&D Program (13ZCZCSY20300 to Hao Xishan). We also appreciate the language support by Rheez C.S. (University of Maryland, US).
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FUNDING
This work was funded by the National Natural Science Foundation of China (81372518) and Key Technology R&D Program (13ZCZCSY20300).
REFERENCES
1. Parkin DM. Global cancer statistics in the year 2000. The Lancet Oncology. 2001; 2:533-543.
2. Spiro SG, Silvestri GA. One hundred years of lung cancer. American journal of respiratory and critical care medicine. 2005; 172:523-529.
3. Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat SM, Supko JG, Haluska FG, Louis DN, Christiani DC, Settleman J, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. The New England journal of medicine. 2004; 350:2129-2139.
4. Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, Naoki K, Sasaki H, Fujii Y, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science (New York, NY). 2004; 304:1497-1500.
5. Kwak EL, Bang YJ, Camidge DR, Shaw AT, Solomon B, Maki RG, Ou SH, Dezube BJ, Janne PA, Costa DB, Varella-Garcia M, Kim WH, Lynch TJ, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. The New England journal of medicine. 2010; 363:1693-1703.
6. Dogan S, Shen R, Ang DC, Johnson ML, D’Angelo SP, Paik PK, Brzostowski EB, Riely GJ, Kris MG, Zakowski MF, Ladanyi M. Molecular epidemiology of EGFR and KRAS mutations in 3,026 lung adenocarcinomas: higher susceptibility of women to smoking-related KRAS-mutant cancers. Clin Cancer Res. 2012; 18:6169-6177.
7. Sun Y, Ren Y, Fang Z, Li C, Fang R, Gao B, Han X, Tian W, Pao W, Chen H, Ji H. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. Journal of clinical oncology. 2010; 28:4616-4620.
8. Wu JY, Yu CJ, Chang YC, Yang CH, Shih JY, Yang PC. Effectiveness of tyrosine kinase inhibitors on “uncommon” epidermal growth factor receptor mutations of unknown clinical significance in non-small cell lung cancer. Clin Cancer Res. 2011; 17:3812-3821.
9. Wu YL, Lee JS, Thongprasert S, Yu CJ, Zhang L, Ladrera G, Srimuninnimit V, Sriuranpong V, Sandoval-Tan J, Zhu Y, Liao M, Zhou C, Pan H, et al. Intercalated combination of chemotherapy and erlotinib for patients with advanced stage non-small-cell lung cancer (FASTACT-2): a randomised, double-blind trial. The Lancet Oncology. 2013; 14:777-786.
10. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, Nishiwaki Y, Ohe Y, Yang JJ, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. The New England journal of medicine. 2009; 361:947-957.
11. Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I, Fujita Y, Okinaga S, Hirano H, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. The New England journal of medicine. 2010; 362:2380-2388.
12. Kuan FC, Kuo LT, Chen MC, Yang CT, Shi CS, Teng D, Lee KD. Overall survival benefits of first-line EGFR tyrosine kinase inhibitors in EGFR-mutated non-small-cell lung cancers: a systematic review and meta-analysis. British journal of cancer. 2015; 113:1519-1528.
13. Li G, Yang S, Yao J, Wang Z, Yao G, Liu M, Ye C. Invasive micropapillary carcinoma of the breast had poor clinical characteristics but showed no difference in prognosis compared with invasive ductal carcinoma. World journal of surgical oncology. 2016; 14:207.
14. Goodman AL, Osunkoya AO. Human Epidermal Growth Factor Receptor 2 Expression in Micropapillary Urothelial Carcinoma of the Bladder: An Analysis of 27 Cases. Human pathology. 2016.
15. Miyaoka Y, Fujiwara A, Kotani S, Tsukano K, Ogawa S, Yamanouchi S, Kusunoki R, Fujishiro H, Kohge N, Yamamoto T, Amano Y. Primary micropapillary carcinoma of the colon with submucosal invasion: A case report. Endoscopy international open. 2016; 4:E744-747.
16. Hacker KE, Uppal S, Johnston C. Principles of Treatment for Borderline, Micropapillary Serous, and Low-Grade Ovarian Cancer. Journal of the National Comprehensive Cancer Network. 2016; 14:1175-1182.
17. Zhao Y, Wang R, Shen X, Pan Y, Cheng C, Li Y, Shen L, Zhang Y, Li H, Zheng D, Ye T, Zheng S, Sun Y, et al. Minor Components of Micropapillary and Solid Subtypes in Lung Adenocarcinoma are Predictors of Lymph Node Metastasis and Poor Prognosis. Annals of surgical oncology. 2016; 23:2099-2105.
18. Sumiyoshi S, Yoshizawa A, Sonobe M, Kobayashi M, Fujimoto M, Tsuruyama T, Date H, Haga H. Pulmonary adenocarcinomas with micropapillary component significantly correlate with recurrence, but can be well controlled with EGFR tyrosine kinase inhibitors in the early stages. Lung cancer (Amsterdam, Netherlands). 2013; 81:53-59.
19. Sica G, Yoshizawa A, Sima CS, Azzoli CG, Downey RJ, Rusch VW, Travis WD, Moreira AL. A grading system of lung adenocarcinomas based on histologic pattern is predictive of disease recurrence in stage I tumors. The American journal of surgical pathology. 2010; 34:1155-1162.
20. Zhang Y, Sun Y, Xiang J, Zhang Y, Hu H, Chen H. A clinicopathologic prediction model for postoperative recurrence in stage Ia non-small cell lung cancer. The Journal of thoracic and cardiovascular surgery. 2014; 148:1193-1199.
21. Sun Y, Yu X, Shi X, Hong W, Zhao J, Shi L. Correlation of survival and EGFR mutation with predominant histologic subtype according to the new lung adenocarcinoma classification in stage IB patients. World journal of surgical oncology. 2014; 12:148.
22. Zhang Y, Wang R, Cai D, Li Y, Pan Y, Hu H, Wang L, Li H, Ye T, Luo X, Zhang Y, Li B, Shen L, et al. A comprehensive investigation of molecular features and prognosis of lung adenocarcinoma with micropapillary component. Journal of thoracic oncology. 2014; 9:1772-1778.
23. Campos-Parra AD, Aviles A, Contreras-Reyes S, Rojas-Marin CE, Sanchez-Reyes R, Borbolla-Escoboza RJ, Arrieta O. Relevance of the novel IASLC/ATS/ERS classification of lung adenocarcinoma in advanced disease. The European respiratory journal. 2014; 43:1439-1447.
24. Clay TD, Do H, Sundararajan V, Moore MM, Conron M, Wright GM, McLachlan SA, Dobrovic A, Russell PA. The clinical relevance of pathologic subtypes in metastatic lung adenocarcinoma. Journal of thoracic oncology. 2014; 9:654-663.
25. Warth A, Muley T, Meister M, Stenzinger A, Thomas M, Schirmacher P, Schnabel PA, Budczies J, Hoffmann H, Weichert W. The novel histologic International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification system of lung adenocarcinoma is a stage-independent predictor of survival. Journal of clinical oncology. 2012; 30:1438-1446.