
INTRODUCTION
Oral squamous cell carcinoma (OSCC) is the most common malignancy of the head and neck worldwide and, in some Asian countries such as India and Taiwan, may accounting for more than 10% of all malignancies [1, 2]. Prior studies have shown evidences that the susceptibility to OSCC of an individual is strongly mediated by some carcinogen-exposure behaviors, such as betel nut [3, 4]. Traditionally, the mainstay treatment for OSCC includes excision of the primary tumor, with or without dissection of the neck lymph nodes. For patients with advanced diseases or pathologic risk factors, adjuvant radiotherapy and/or chemotherapy are also parts of the standard treatments [5]. Despite ongoing advances in the surgical techniques and adjuvant therapies, the 5-year overall survival rate remains unfavorable in a considerable portion of OSCC patients because invasion of the neighboring tissues and metastasis to the neck lymph nodes are common [6, 7]. Therefore, identifying new biomarkers that can predict the risk of OSCC progression, especially local invasion and lymph node metastasis, is mandatory to improve the treatment of this deadly disease.
For cancers to invade and metastasize, tumor cells must degrade the extracellular matrix (ECM) and gain access to blood vessels and lymphatics [8]. Matrix metalloproteinases (MMPs) are zinc-dependent endopeptidases that can degrade the components of the ECM and basement membranes, and increased expression of these enzymes is detected in almost all human cancers and has been associated with the aggressiveness in various neoplasms [8–11]. MMP-11, also known as stromelysin-3, is closely related with tissue remodeling during involution, embryogenesis, and wound healing in normal physiologic conditions [12]. Like many other members of MMPs, increased expression of MMP-11 has been observed in most invasive human carcinomas, including lung, breast, colorectal and ovarian carcinomas, and high levels of its mRNA was reportedly associated with aggressive phenotypes and poor clinical outcome [13–15].
The clinical significance of MMP-11 expression has been demonstrated previously by immunohistochemical studies on tumor specimens of OSCC patients. Soni et al found that, in tobacco-associated OSCC, expression of MMP-11 was significantly associated with the involvement of neck lymph node [16]. The data, however, failed to demonstrate the clinical significance of MMP-11 expression in OSCC tissues which are closely related to the consumption of betel nut. To address this issue, and also to determine whether measurement of MMP-11 expression could possibly serve as a prognostic indicator for OSCC, we conducted an immunohistochemical analysis to investigate the relationships between the expression of MMP-11 and clinicopathologic parameters in 279 patients with OSCC. Moreover, in established human oral cancer cell lines, we further evaluated the migration capability in MMP-11 overexpressed OSCC cell lines and the underlying mechanisms.
RESULTS
Patient characteristics
The demographic and clinicopathological data of this study subjects were shown in Table 1. A total of 279 patients (264 men, 15 women) with OSCC were included in the current investigation. The patients were aged 31 to 90 years (mean age=55.80 ± 11.15 years). The tumors located over the following sites: buccal mucosa (n=109), tongue (n=93), gingiva (n=34), palate (n=16) and floor of the mouth (n=14). As to TNM staging of the OSCC, 53 (19.0 %) were at stage I, 56 (20.1 %) were at stage II, 35 (12.5 %) were at stage III, and 135 (48.4 %) were at stage IV. Grade of tumor cell differentiation included 42 (15.1%) well differentiation and 237 (84.9%) moderate or poor differentiation.
Table 1: Distributions of demographical characteristics in 279 patients with oral cancer
Characteristics |
Total (%) |
|---|---|
Total number of patients |
279 |
Age (year) |
|
Mean ± SD |
55.80 ± 11.15 |
Gender |
|
Male |
264 (94.6%) |
Female |
15 (5.4%) |
Cancer location |
|
Buccal mucosa |
109 (39.1 %) |
Tongue |
93 (33.3 %) |
Gingiva |
34 (12.2 %) |
Palate |
16 (5.7 %) |
Floor of Mouth |
14 (5.0 %) |
Others |
13 (4.7 %) |
Clinical stage |
|
I |
53 (19.0%) |
II |
56 (20.1%) |
III |
35 (12.5%) |
IV |
135 (48.4%) |
T classification |
|
T1 |
70 (25.1%) |
T2 |
88 (31.5%) |
T3 |
23 (8.2%) |
T4 |
98 (35.1%) |
N classification |
|
N0 |
176 (63.1%) |
N1 |
36 (12.9%) |
N2 |
63 (22.6%) |
N3 |
4 (1.4%) |
M classifications |
|
M0 |
276 (98.9%) |
M1 |
3 (1.1%) |
Grade |
|
Well |
42 (15.1%) |
moderate, poor |
237 (84.9%) |
Association of expression of MMP-11 and clinicopathological characteristics in OSCC
According to the expression level in the OSCC tissues (Figure 1), we divided MMP-11 immunohistological stains into two groups: weak and strong. Weak expression of MMP-11 was present in 161 out of 279 patients (57.7 %), while strong expression in 118 patients (42.3 %). Statistical analysis revealed no significant differences between MMP-11 expression and age, gender, cancer location, clinical stage, tumor classification and distant metastasis. Patients with strong MMP-11 expression, however, were associated with higher incidence of lymph node metastasis (p=0.034) and worse grade of tumor differentiation (p=0.009) (Table 2).
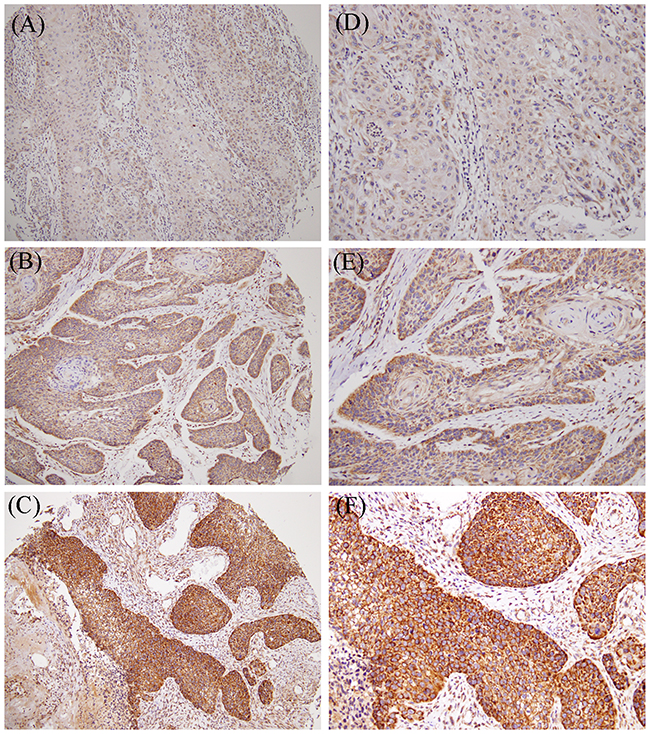
Figure 1: MMP-11 expression in primary oral cancer. Tissue microarrays of primary oral squamous cell carcinomas (OSCCs) were immunohistochemically analyzed for MMP-11. (A and D) no detectable MMP-11 (0). (B and E) weak expression levels (1+). (C and F) strong expression levels (2+). (A-C) low-power field (100x); (D-F) high-power field (200x).
Table 2: Patient characteristics regarding MMP-11 expression
Characteristics |
No. of patients (%) |
||
|---|---|---|---|
MMP-11 (weak) |
MMP-11 (strong) |
p value |
|
Total number of patients |
161 (57.7) |
118 (42.3) |
|
Age (year) |
|||
<55 |
84 (52.2) |
56 (47.5) |
0.436 |
≥55 |
77 (47.8) |
62 (52.5) |
|
Gender |
|||
Male |
155 (96.3) |
109 (92.4) |
0.154 |
Female |
6 (3.7) |
9 (7.6) |
|
Cancer location |
|||
Buccal mucosa |
71 (44.1) |
38 (32.2) |
0.164 |
Tongue |
52 (32.3) |
41 (34.7) |
|
Gingiva |
18 (11.2) |
16 (13.6) |
|
Others |
20 (12.4) |
23 (19.5) |
|
Clinical stage |
|||
I+II |
64 (39.8) |
45 (38.1) |
0.785 |
III+IV |
97 (60.2) |
71 (61.9) |
|
T classification |
|||
T1+T2 |
88 (54.7) |
70 (59.3) |
0.437 |
T3+T4 |
73 (45.3) |
48 (40.7) |
|
N classification |
|||
N0 |
110 (68.3) |
66 (55.9) |
0.034* |
N1+2+3 |
51 (31.7) |
52 (44.1) |
|
M classification |
|||
M0 |
159 (98.8) |
117 (99.2) |
0.752 |
M1 |
2 (1.2) |
1 (0.8) |
|
Grade |
|||
Well |
32 (19.9) |
10 (8.5) |
0.009* |
moderate, poor |
129 (80.1) |
108 (91.5) |
|
* p value < 0.05 as statistically significant.
Survival analyses of MMP-11 and clinicopathological parameters
Univariate analysis using Cox proportional hazards regression model showed that advanced clinical stage (p< 0.001), large tumor size (p=0.002), positive lymph node metastasis (p< 0.001), worse grade of differentiation (p=0.027) and strong expression of MMP-11 (p=0.010) were correlated with a poor overall survival of patients with OSCC (Table 3). However, no significant association was found between age, gender and survival rate (Table 3). If analyzed with multivariate analysis using Cox regression model, the results showed that T status (p=0.024), N status (p< 0.001) and MMP-11 expression (p=0.043) were correlated with a poor overall survival of patients with OSCC, while there was no such association for clinical stage and differentiation grade with the prognosis of OSCC patients (Table 4).
Table 3: Univariate survival analyses of MMP-11 and clinicopathological parameters among patients with OSCC using the Cox proportional hazard regression model
All cases (N=279) |
Hazard ratio (95% CI) |
p value |
|---|---|---|
Age (<55 versus ≥55) |
0.987 (0.615–1.585) |
0.958 |
Gender (Male versus Female) |
1.504 (0.530–4.268) |
0.443 |
Clinical stage (stage I + II versus stage III + IV) |
2.929 (1.780–4.818) |
< 0.001* |
T status (T1 + T2 versus T3 + T4) |
2.185 (1.337–3.569) |
0.002* |
N status (N0 versus N1 + N2 + N3) |
4.136 (2.398–7.133) |
< 0.001* |
Grade (Well versus moderate, poor) |
2.122 (1.088–4.141) |
0.027* |
MMP-11 (weak versus strong) |
1.902 (1.166–3.100) |
0.010* |
* p value < 0.05 as statistically significant.
Table 4: Multivariate survival analyses of MMP-11 and clinicopathological parameters among patients with OSCC using the Cox regression model
All cases (N=279) |
Hazard ratio (95% CI) |
p value |
|---|---|---|
Clinical stage (stage I + II versus stage III + IV) |
0.601 (0.202–1.788) |
0.360 |
T status (T1 + T2 versus T3 + T4) |
2.878 (1.150–7.204) |
0.024* |
N status (N0 versus N1 + N2 + N3) |
4.655 (1.973–10.984) |
< 0.001* |
Grade (Well versus moderate, poor) |
1.662 (0.813–3.397) |
0.164 |
MMP-11 (weak versus strong) |
1.726 (1.017–2.930) |
0.043* |
* p value < 0.05 as statistically significant.
A Kaplan-Meier analysis was also performed to evaluate the association between the expression of MMP-11 and overall survival. The analysis showed that OSCC patients with strong expression of MMP-11 had a significantly lower survival rate (p=0.010) (Figure 2). The median survival in weak expression of MMP-11 was 79.2 months, whereas that in strong expression of MMP-11 was 48 months.
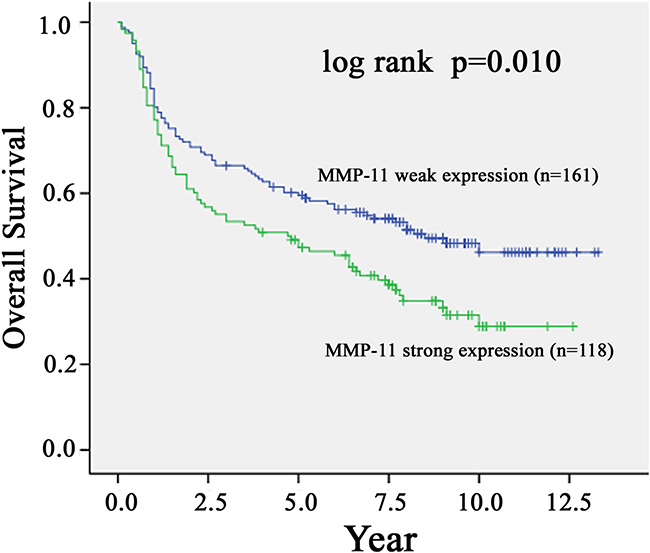
Figure 2: Kaplan-Meier survival curve showing the relation between MMP-11 expression in primary tumors and survival in 279 oral squamous cell carcinoma (OSCC) patients. The overall survival of OSCC patients with positive MMP-11 staining was significantly lower than that of OSCC patients with negative MMP-11 staining (p<0.05, log-rank test).
MMP-11 promoted the cell migration of OSCC cell lines
Since we found that expression of MMP-11 was significantly correlated with the presence of lymph node metastasis, the effects of the MMP-11-overexpression on the OSCC cell line were investigated by in vitro wound-closure assay, Boyden chamber cell invasion and migration assay. The MMP-11 expression of TW2.6 cells transfected with pcDNA3.0-MMP-11 was confirmed by western blot and RT-PCR (Figure 3A). We next evaluated the effect of MMP-11 overexpression on TW2.6 cell migration. Using an in vitro wound-closure assay, Boyden chamber cell migration assay and invasion assay, it was shown that MMP-11 overexpression significantly increased the migration capability of TW2.6 cells (Figure 3B-3D).
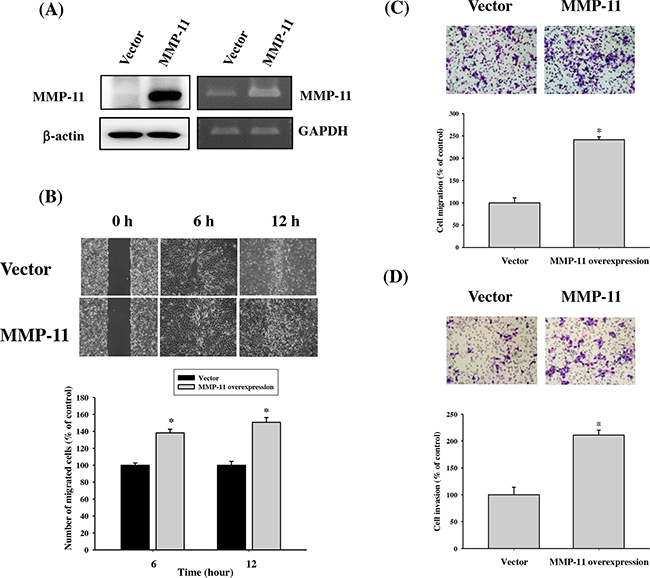
Figure 3: The relationships between MMP-11 expression and cell migration in TW2.6 OSCC cell lines. (A) The MMP-11 expression of TW2.6 cells transfected with pcDNA3.0-MMP-11 was examined by western blot and RT-PCR. (B-D) Detection of cell migratory abilities by transfection with MMP-11 overexpression vector in TW2.6 cell. Migratory abilities of pcDNA3.0 and pcDNA3.0-MMP-11 cells were evaluated using (B) wound healing assay. The (C) migratory and (D) invasive abilities of pcDNA3.0 and pcDNA3.0-MMP-11 cells were evaluated using Boyden chamber migration and Matrigel invasion assays. Differences are presented as the mean of triplicate experiments compared with control cells. *p < 0.05 compared with control cells.
Effects of MMP-11 expression on regulation of focal adhesion kinase/Src kinase (FAK/Src) and MAP-Kinase signalling pathway
The focal adhesion kinase/Src kinase (FAK/Src) and Mitogen-activated protein kinases (MAPK) pathway is known to play a role in cancer metastasis [17–21]. To elucidate the involvement of FAK/Src and MAPK signaling in MMP-11 overexpression TW2.6 cell, western blot analysis was performed. The results revealed phosphorylation of FAK and Src were significantly increased in the MMP-11-overexpressed TW2.6 OSCC cells compared with those in their parental, whereas it had no effect on ERK1/2, JNK1/2 and p38 phosphorylation (Figures 4A-4B). Moreover, pretreatment with FAK inhibitor (FAKI-14) or Src inhibitor (PPI) reversed the MMP-11 overexpression-induced migration in OSCC cells (Figure 4C and 4D). These results indicate that MMP-11 increases OSCC migration may through the FAK/Src signaling pathway. To further support this conclusion, we also examined the expression of MMP-11, FAK and Src in HNSCC tissue by using the The Cancer Genome Atlas (TCGA) Database. The results showed that the relative MMP-11 levels were positively correlated with the expression of FAK (Spearman rank correlation coefficient r =0.2935, p<0.0001) and Src (Spearman rank correlation coefficient r =0.1817, p<0.0001) mRNAs in HNSCC (Figures 4E-4F).
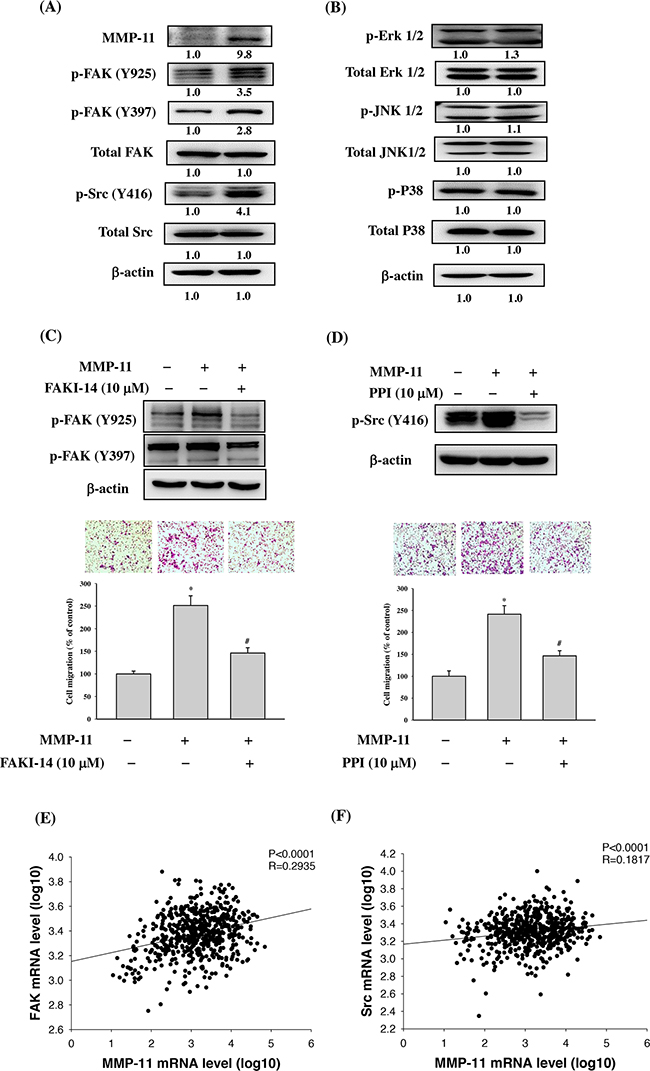
Figure 4: FAK/Src signaling pathway is involved in MMP-11-promoted cell migration. (A) TW2.6 cells transfected with pcDNA3.0 and pcDNA3.0-MMP-11 overexpression vector for 24 h and the total cell lysates were then subjected to western blot to analyze the phosphorylation of (A) FAK and Src (B) Erk 1/2, JNK1/2 and p38 as described in the Materials and Methods section. (C) TW2.6 cells were treated with a FAK inhibitor (FAKI-14; 10μM) for 24h. FAK phosphorylation was examined by western blot and cell migration was examined by Boyden chamber migration. (D) TW2.6 cells were treated with a Src inhibitor (PPI; 10μM) for 24h. Src phosphorylation was examined by western blot and cell migration was examined by Boyden chamber migration. Data are expressed as the mean ± SEM *p < 0.05 compared with control; #p < 0.05 compared with the pcDNA3.0-MMP-11 overexpression vector group. (E-F) The correlations among mRNA levels of MMP-11 and FAK as well as Src in head and neck squamous cell carcinoma from The Cancer Genome Atlas (TCGA) Data Portal. (E) A significant correlation was found between MMP-11 and FAK (Spearman rank correlation coefficient r =0.2935, p<0.0001). (F) A significant correlation was found between MMP-11 and Src (Spearman rank correlation coefficient r =0.1817, p<0.0001).
DISCUSSION
Tobacco use and alcohol consumption are well-known carcinogen-exposure behaviors and risk factors for most head and neck cancers, especially OSCC [22]. Betel nut chewing, a very common social behavior in Taiwan, is another well-established etiological factor in the tumorigenesis of OSCC [3, 23]. For these patients, oral tumors develop most frequently on the tongue and the buccal mucosa, where most contact and irritation by the betel nut occur [24]. The high prevalence of OSCC, ongoing increase of betel nut chewing, and grave outcomes for advanced OSCC, have become an important healthcare issue in Taiwan. In the current study, we examined the correlation between clinicopathological characteristics and MMP-11 expression in OSCC patients, most of them had the behaviors of tobacco use and/or betel nut chewing. Our data showed that a strong expression of MMP-11 was associated with increased lymph node metastasis and poor survival in these patients.
Most members of MMPs have been implicated in the tumorigenesis of various human malignancies. For head and neck cancers, MMP-1, MMP-2, MMP-9 and membrane type-1 MMP were constantly observed overexpressed in the tumor tissues and were considered associated with the development and progression of cancer [10, 25–29]. Expression of MMP-11 in the head and neck cancers, on the other hand, was scarcely investigated in the literature. Soni et al performed immunohistochemical analysis of MMP-11 expression in tumor specimens of 177 OSCC patients and found positive expression in 70% of these samples [16]. Their data also demonstrated that MMP-11 positivity was correlated with metastasis of neck lymph node, although survival analysis failed to reveal association with the expression of MMP-11. Another study of serial paraffin sections, which included 220 OSCC and 90 precancerous lesions, discovered that concomitant expression of MMP-11 and proangiogenic factors was an indicator for progression from precancerous stage to flank malignancy [22]. Of note, study subjects of the abovementioned researches were mainly tobacco and/or alcohol-associated OSCC, while our study enrolled betel nut-associated OSCC as well in Taiwan. Unlike the results of Soni’s study, our data showed that strong expression of MMP-11 was correlated with a poor overall survival of OSCC patients, suggesting a relatively important role of MMP-11 in the aggressiveness of OSCC in Taiwan.
The FAK and Src activation is capable of modulating cell migration and invasion [18, 19, 30]. Our previous study revealed that FAK phosphorylation was involved in caffeic acid phenethyl ester-inhibited oral cancer cell metastasis [21] and WISP1-induced OSCC angiogenesis [31]. Other studies have also reported that FAK/Src pathway was associated the OSCC cell migration [32, 33]. Moreover, Pal et al. shows that thrombospondin-1 promotes migration of oral cancer cells and stimulates the expression of MMP-11 partly through the integrin signaling [34]. Therefore, we utilized a western blot to characterize the phosphorylation of FAK and Src in the MMP-11-overexpressed TW2.6 OSCC cells and showed that phosphorylation of FAK and Src was significantly increased. These data suggested that FAK/Src signaling is involved in MMP-11-mediated cell metastasis in OSCC. However, limitations do exist in our investigation and should be addressed. The present study was the lacking of in vivo animal study, which could provide additional support to our findings and will be included in our future work.
In summary, by using immunohistochemical analysis, we observed that strong expression of MMP-11 in OSCC tissues was associated with an increased incidence of lymph node metastasis. In addition, strong MMP-11 expression was significantly related to poor overall survival in patients with OSCC. The results suggest that MMP-11 is a potential biomarker for prognostic indicator in patients with OSCC.
MATERIALS AND METHODS
Patients and tissue microarrays
We constructed formalin-fixed, paraffin-embedded tissue microarrays composed of 279 OSCC tissue cores as previously described [35]. Diagnosis of OSCC was based on histological examination of hematoxylin and eosin-stained tissue sections. Approval from the Institutional Review Board of Chung-Shan Medical University Hospital and Changhua Christian Hospital was obtained prior to this study.
Immunohistochemical (IHC) analysis
Paraffin-embedded OSCC tissue sections (4 μm) of the paraffin slice on coated slides were washed with xylene to remove the paraffin as previously described [36]. After incubation with an anti-MMP-11 (1:100 dilution; Santa Cruz Biotechnology, Santa Cruz, CA) antibody for 60 min at room temperature, slides were thoroughly washed three times with PBS. The conventional streptavidin peroxidase method (LSAB Kit K675; DAKO, Copenhagen, Denmark) was performed for signal development. The intensity of staining was respectively scored −, 1+, and 2+ for weak (− or 1+) and strong staining (2+). All immunohistochemical staining cases were examined by two pathologists and a final agreement was obtained for each score at a discussion microscope.
Cell culture and full-length MMP-11 plasmid DNA transfection
TW2.6 cells, derived from a buccal cancer patient who chewed Betel quid [37], were cultured in Dulbecco’s modified Eagle’s medium supplemented with an equal volume of a nutrient mixture, F-12 Ham’s medium (Life Technologies, Grand Island, NY, USA). All cell cultures were maintained at 37 °C in a humidified atmosphere of 5% CO2. The pcDNA3.0-MMP-11 expression vector and pcDNA3.0 control vector were transiently transfected into TW2.6 cells using Lipofectamine 2000 (Invitrogen, Carlsbad, CA, USA). The MMP-11-overexpressing TW2.6 cells were established and the MMP-11 expression levels shown by these cells were confirmed using western blot and RT-PCR analysis.
In vitro wound closure
TW2.6 cells (5 × 104 cells/well) were plated in 6 cm petri dishes for 24 h and wounds were produced by manually scratching with a 200 μL pipette tip as described previously [7]. Images were recorded at indicated times after treatment using a phase-contrast microscope (×100).
Cell migration and invasion assays
After a treatment with the MMP-11 overexpression for 24 h, TW2.6 cells were harvested and seeded to Boyden chamber (Neuro Probe, Cabin John, MD, USA) at 104 cell/well in serum free medium and then incubated for 24 h at 37°C. The invaded cells were fixed with 100% methanol and stained with 5% Giemsa. Cell numbers were counted under a light microscope as previously described [38]. To determine cell Invasion, the cells were seeded into the Boyden chamber on membrane filters that were coated with Matrigel [39].
Western blot analysis
Cellular lysates were prepared by suspending 2x106/10cm dish in 200μL of RIPA buffer containing protease inhibitors cocktail. Cell lysates were subjected to a centrifugation of 10,000 rpm for 10 min at 4°C, and the insoluble pellet was discarded. The 20 μg samples of cell lysates was separated by SDS-PAGE on 10% polyacrylamide gels and transferred onto a nitrocellulose membrane using the Mini-Protean Tetra Electrophoresis System as described previously [18]. The blot was subsequently incubated with 5% non-fat milk in Tris-buffered saline (20 mM Tris, 137 mM NaCl, pH 7.6) for 1 h to block non-specific binding and then overnight with polyclonal antibodies against MMP-11 (Santa Cruz, CA, USA) and β-actin (Novus Biologicals, Co, USA). Blots were then incubated with a horseradish peroxidase anti-rabbit IgG for 1 h. Afterwards, signal was detected by using enhanced chemiluminescence (ECL) commercial kit (Amersham Biosciences, Piscataway, NJ, USA).
Reverse transcriptase–polymerase chain reaction (RT-PCR)
Total RNA was isolated using Total RNA mini kit (Qiagen, Valencia, CA, USA) and reverse transcribe into cDNA using High Capacity cDNA Reverse Transcription kit (Applied Biosystems, Foster City, CA, USA) as previously described [40]. The sequences of the primers were: F-5’-CAGGTGGCAGCCCATGAATT3’and R-5’- GTACTGAGCACCTTGGAAGA-3’ for MMP-11, and F-5’-CGGAGTCAACGGATTTGGTCGTAT-3’ and R-5’-AGCCTTCTCCATGGTTGGTGAAGAC-3’ for GAPDH. The reaction mix was first denatured at 95°C for 5 min. The PCR condition for MMP-11 were 94°C for 1 min, 64°C for 1 min, 72°C for 2 min for 30 cycles; for GAPDH were 94°C for 1 min, 65°C for 1 min, 72°C for 2 min for 18 cycles, followed by 72°C for 10 min.
Statistical analysis
Correlations of MMP-11 with clinicopathologic parameters of OSCC were examined by Pearson’s χ2 test or Fisher exact test. Cumulative survival was analyzed by the Kaplan-Meier method. Univariate analysis was analyzed by the Cox proportional hazards regression model and multivariable analysis using a Cox regression model (SPSS, Version 17.0; SPSS, Inc, Chicago, IL, USA). Difference between control and treated groups were calculated by Student’s t-test and p < 0.05 was considered as statistically significant.
ACKNOWLEDGMENTS
This study was supported by a research grant from National Science Council, Taiwan (NSC 101-2314-B-040-019) and Chung Shan Medical University Hospital, Taiwan (CSH-2016-C-007).
CONFLICTS OF INTEREST
The authors declare that no conflicts of interest exist.
REFERENCES
1. Petersen PE. Oral cancer prevention and control--the approach of the World Health Organization. Oral Oncol. 2009; 45: 454-460.
2. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013; 63: 11-30.
3. Lai KC, Lee TC. Genetic damage in cultured human keratinocytes stressed by long-term exposure to areca nut extracts. Mutat Res. 2006; 599: 66-75.
4. Yeh CM, Lin CW, Yang JS, Yang WE, Su SC, Yang SF. Melatonin inhibits TPA-induced oral cancer cell migration by suppressing matrix metalloproteinase-9 activation through the histone acetylation. Oncotarget. 2016; 7: 21952-21967. doi: 10.18632/oncotarget.8009.
5. Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefebvre JL, Greiner RH, Giralt J, Maingon P, Rolland F, Bolla M, Cognetti F, Bourhis J, Kirkpatrick A, van Glabbeke M. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004; 350: 1945-1952.
6. Zini A, Czerninski R, Sgan-Cohen HD. Oral cancer over four decades: epidemiology, trends, histology, and survival by anatomical sites. J Oral Pathol Med. 2010; 39: 299-305.
7. Lin CW, Yang WE, Lee WJ, Hua KT, Hsieh FK, Hsiao M, Chen CC, Chow JM, Chen MK, Yang SF, Chien MH. Lipocalin 2 prevents oral cancer metastasis through carbonic anhydrase IX inhibition and is associated with favourable prognosis. Carcinogenesis. 2016; 37: 712-722.
8. Su SC, Hsieh MJ, Yang WE, Chung WH, Reiter RJ, Yang SF. Cancer metastasis: Mechanisms of inhibition by melatonin. J Pineal Res. 2017; 62. doi: 10.1111/jpi.12370.
9. Shuman Moss LA, Jensen-Taubman S, Stetler-Stevenson WG. Matrix metalloproteinases: changing roles in tumor progression and metastasis. Am J Pathol. 2012; 181: 1895-1899.
10. Chien MH, Lin CW, Cheng CW, Wen YC, Yang SF. Matrix metalloproteinase-2 as a target for head and neck cancer therapy. Expert Opin Ther Targets. 2013; 17: 203-216.
11. Su SC, Lin CW, Yang WE, Fan WL, Yang SF. The urokinase-type plasminogen activator (uPA) system as a biomarker and therapeutic target in human malignancies. Expert Opin Ther Targets. 2016; 20: 551-566.
12. Fiorentino M, Fu L, Shi YB. Mutational analysis of the cleavage of the cancer-associated laminin receptor by stromelysin-3 reveals the contribution of flanking sequences to site recognition and cleavage efficiency. Int J Mol Med. 2009; 23: 389-397.
13. Rouyer N, Wolf C, Chenard MP, Rio MC, Chambon P, Bellocq JP, Basset P. Stromelysin-3 gene expression in human cancer: an overview. Invasion Metastasis. 1994; 14: 269-275.
14. Anderson IC, Sugarbaker DJ, Ganju RK, Tsarwhas DG, Richards WG, Sunday M, Kobzik L, Shipp MA. Stromelysin-3 is overexpressed by stromal elements in primary non-small cell lung cancers and regulated by retinoic acid in pulmonary fibroblasts. Cancer Res. 1995; 55: 4120-4126.
15. Porte H, Chastre E, Prevot S, Nordlinger B, Empereur S, Basset P, Chambon P, Gespach C. Neoplastic progression of human colorectal cancer is associated with overexpression of the stromelysin-3 and BM-40/SPARC genes. Int J Cancer. 1995; 64: 70-75.
16. Soni S, Mathur M, Shukla NK, Deo SV, Ralhan R. Stromelysin-3 expression is an early event in human oral tumorigenesis. Int J Cancer. 2003; 107: 309-316.
17. Yang M, Huang CZ. Mitogen-activated protein kinase signaling pathway and invasion and metastasis of gastric cancer. World J Gastroenterol. 2015; 21: 11673-11679.
18. Lee BY, Timpson P, Horvath LG, Daly RJ. FAK signaling in human cancer as a target for therapeutics. Pharmacol Ther. 2015; 146: 132-149.
19. Cheng HL, Lin CW, Yang JS, Hsieh MJ, Yang SF, Lu KH. Zoledronate blocks geranylgeranylation not farnesylation to suppress human osteosarcoma U2OS cells metastasis by EMT via Rho A activation and FAK-inhibited JNK and p38 pathways. Oncotarget. 2016; 7: 9742-9758. doi: 10.18632/oncotarget.7138.
20. Huang YW, Chuang CY, Hsieh YS, Chen PN, Yang SF, Shih Hsuan L, Chen YY, Lin CW, Chang YC. Rubus idaeus extract suppresses migration and invasion of human oral cancer by inhibiting MMP-2 through modulation of the Erk1/2 signaling pathway. Environ Toxicol. 2016; 32:1037-1046. doi: 10.1002/tox.22302.
21. Peng CY, Yang HW, Chu YH, Chang YC, Hsieh MJ, Chou MY, Yeh KT, Lin YM, Yang SF, Lin CW. Caffeic Acid phenethyl ester inhibits oral cancer cell metastasis by regulating matrix metalloproteinase-2 and the mitogen-activated protein kinase pathway. Evid Based Complement Alternat Med. 2012; 2012: 732578.
22. Gillison ML. Current topics in the epidemiology of oral cavity and oropharyngeal cancers. Head Neck. 2007; 29: 779-792.
23. Chen YJ, Chang JT, Liao CT, Wang HM, Yen TC, Chiu CC, Lu YC, Li HF, Cheng AJ. Head and neck cancer in the betel quid chewing area: recent advances in molecular carcinogenesis. Cancer Sci. 2008; 99: 1507-1514.
24. Li-Ting C, Chung-Ho C, Yi-Hsin Y, Pei-Shan H. The development and validation of oral cancer staging using administrative health data. BMC Cancer. 2014; 14: 380.
25. Rosenthal EL, Matrisian LM. Matrix metalloproteases in head and neck cancer. Head Neck. 2006; 28: 639-648.
26. Lin CW, Chen PN, Chen MK, Yang WE, Tang CH, Yang SF, Hsieh YS. Kaempferol reduces matrix metalloproteinase-2 expression by down-regulating ERK1/2 and the activator protein-1 signaling pathways in oral cancer cells. PLoS One. 2013; 8: e80883.
27. Yang JS, Lin CW, Su SC, Yang SF. Pharmacodynamic considerations in the use of matrix metalloproteinase inhibitors in cancer treatment. Expert Opin Drug Metab Toxicol. 2016; 12: 191-200.
28. Yang SF, Chen MK, Hsieh YS, Yang JS, Zavras AI, Hsieh YH, Su SC, Kao TY, Chen PN, Chu SC. Antimetastatic effects of Terminalia catappa L. on oral cancer via a down-regulation of metastasis-associated proteases. Food Chem Toxicol. 2010; 48: 1052-1058.
29. Yang SF, Yang WE, Kuo WH, Chang HR, Chu SC, Hsieh YS. Antimetastatic potentials of flavones on oral cancer cell via an inhibition of matrix-degrading proteases. Arch Oral Biol. 2008; 53: 287-294.
30. Hsin CH, Wu BC, Chuang CY, Yang SF, Hsieh YH, Ho HY, Lin HP, Chen MK, Lin CW. Selaginella tamariscina extract suppresses TPA-induced invasion and metastasis through inhibition of MMP-9 in human nasopharyngeal carcinoma HONE-1 cells. BMC Complement Altern Med. 2013; 13: 234.
31. Chuang JY, Chen PC, Tsao CW, Chang AC, Lein MY, Lin CC, Wang SW, Lin CW, Tang CH. WISP-1 a novel angiogenic regulator of the CCN family promotes oral squamous cell carcinoma angiogenesis through VEGF-A expression. Oncotarget. 2015; 6: 4239-4252. doi: 10.18632/oncotarget.2978.
32. Huang WC, Chan SH, Jang TH, Chang JW, Ko YC, Yen TC, Chiang SL, Chiang WF, Shieh TY, Liao CT, Juang JL, Wang HC, Cheng AJ, et al. miRNA-491-5p and GIT1 serve as modulators and biomarkers for oral squamous cell carcinoma invasion and metastasis. Cancer Res. 2014; 74: 751-764.
33. Min A, Zhu C, Wang J, Peng S, Shuai C, Gao S, Tang Z, Su T. Focal adhesion kinase knockdown in carcinoma-associated fibroblasts inhibits oral squamous cell carcinoma metastasis via downregulating MCP-1/CCL2 expression. J Biochem Mol Toxicol. 2015; 29: 70-76.
34. Pal SK, Nguyen CT, Morita KI, Miki Y, Kayamori K, Yamaguchi A, Sakamoto K. THBS1 is induced by TGFB1 in the cancer stroma and promotes invasion of oral squamous cell carcinoma. J Oral Pathol Med. 2016; 45: 730-739.
35. Chien MH, Ying TH, Hsieh YH, Lin CH, Shih CH, Wei LH, Yang SF. Tumor-associated carbonic anhydrase XII is linked to the growth of primary oral squamous cell carcinoma and its poor prognosis. Oral Oncol. 2012; 48: 417-423.
36. Yang WE, Ho CC, Yang SF, Lin SH, Yeh KT, Lin CW, Chen MK. Cathepsin B Expression and the Correlation with Clinical Aspects of Oral Squamous Cell Carcinoma. PLoS One. 2016; 11: e0152165.
37. Kok SH, Hong CY, Lin SK, Lee JJ, Chiang CP, Kuo MY. Establishment and characterization of a tumorigenic cell line from areca quid and tobacco smoke-associated buccal carcinoma. Oral Oncol. 2007; 43: 639-647.
38. Cheng HL, Hsieh MJ, Yang JS, Lin CW, Lue KH, Lu KH, Yang SF. Nobiletin inhibits human osteosarcoma cells metastasis by blocking ERK and JNK-mediated MMPs expression. Oncotarget. 2016; 7: 35208-35223. doi: 10.18632/oncotarget.9106.
39. Lin CW, Chou YE, Chiou HL, Chen MK, Yang WE, Hsieh MJ, Yang SF. Pterostilbene suppresses oral cancer cell invasion by inhibiting MMP-2 expression. Expert Opin Ther Targets. 2014; 18: 1109-1120.
40. Ho HY, Lin CW, Chien MH, Reiter RJ, Su SC, Hsieh YH, Yang SF. Melatonin suppresses TPA-induced metastasis by downregulating matrix metalloproteinase-9 expression through JNK/SP-1 signaling in nasopharyngeal carcinoma. J Pineal Res. 2016; 61: 479-492.