

INTRODUCTION
TROP2 (also known as TACSTD2) is a transmembrane glycoprotein that has high expression in many cancers and is associated with patient survival [1–11]. Emerging evidence suggests that TROP2 is a promising molecular target for the treatment of various malignancies [11]. Several ongoing clinical trials for TROP2-targeting therapies are showing signs of efficacy [11]. TROP2 has been used as a target of antibody-drug conjugate (ADC) therapy [11]. Sacituzumab govitecan (IMMU-132) is an anti-TROP2 ADC [11–18] that contains SN-38, the active metabolite of irinotecan. Without severe side effects, IMMU-132 has been effective against triple-negative breast cancer [19], metastatic small cell lung carcinoma (SCLC) [14], and metastatic non-SCLC (NSCLC) resistant to anti-PD-1/PD-L1 therapy [15].
Lung carcinoma represents a group of histologically and molecularly heterogeneous diseases [20–28]. The major subtypes include adenocarcinoma, squamous cell carcinoma (SqCC), and high-grade neuroendocrine tumor (HGNET), which consists of SCLC and large cell neuroendocrine carcinoma (LCNEC). Even within the same subtype, tumors display heterogeneous characteristics. For example, alterations in cancer driver genes differ between lung adenocarcinomas (e.g., EGFR, KRAS, ALK, RET, and ROS1) [27]. Little is known about the role of TROP2 in lung cancer [1–3, 11, 14, 15]. Because TROP2 is a promising molecular target for the treatment of lung cancer, we examined the association of TROP2 expression with clinicopathological and molecular features as well as with prognosis of various lung cancer subtypes, including 270 consecutive cases of adenocarcinoma, 201 cases of SqCC, and 115 cases of HGNET (74 cases of SCLC and 41 cases of LCNEC).
RESULTS
TROP2 expression in lung cancer
We defined high TROP2 expression as intensity 1 with ≥50% expression or intensity 2 with ≥10% expression in tumor membranous staining, as mentioned in Materials and Methods section and presented in Figure 1. High TROP2 expression was observed in 172 (64%) adenocarcinomas, 150 (75%) SqCCs, and 21 (18%) HGNETs using immunohistochemistry. Table 1 shows the clinicopathological and molecular characteristics of each lung cancer subtype according to the TROP2 expression level (no/low vs. high). In adenocarcinoma, high TROP2 expression was associated with the male gender (P = 0.0018), larger tumor size (>30 mm) (P = 0.016), higher pathological-stage (p-stage) (II–IV) (P = 0.012), and less tumor differentiation (moderate to poor) (P = 0.045). In SqCC, high TROP2 expression was associated with a higher rate of well tumor differentiation (P = 0.040). In HGNET, high TROP2 expression was associated with the LCNEC subtype (P = 0.0013). Of the 115 cases of HGNETs, only 22 cases of SCLC underwent neoadjuvant chemotherapy, and high TROP2 expression was not associated with the status of neoadjuvant chemotherapy in SCLC (P = 0.67). In HGNET, the Ki-67 index (< 60% vs. ≥ 60%) was not associated with TROP2 expression (no/low vs. high expression) (P = 0.61).
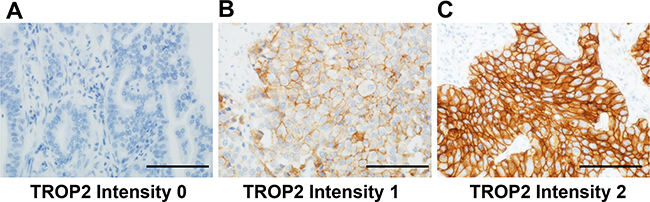
Figure 1: Immunohistochemical evaluation of membranous TROP2 expression in tumor cells from patients with lung adenocarcinoma. (A) TROP2 intensity 0 (negative), (B) TROP2 intensity 1 (weak to moderate), and (C) TROP2 intensity 2 (strong). Figure 1A shows a TROP2 immunohistochemical image of well- to moderately-differentiated adenocarcinoma, whereas Figure 1B and 1C show those of poorly-differentiated adenocarcinoma. Scale bar = 200 µm.
Table 1: Clinicopathological and molecular characteristics of lung cancer according to TROP2 expression in tumor cells
Variables |
Adenocarcinoma |
SqCC |
HGNET |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
N of samples (%) |
TROP2 expression |
N of samples (%) |
TROP2 expression |
N of samples (%) |
TROP2 expression |
|||||||
No/low (n=98) (36%) |
High (n=172) (64%) |
P-values |
No/low (n=51) (25%) |
High (n=150) (75%) |
P-values |
No/low (n=94) (82%) |
High (n=21) (18%) |
P-values |
||||
Age (years) |
0.24 |
0.39 |
0.78 |
|||||||||
< 60 |
96 (36%) |
33 (34%) |
63 (37%) |
21 (10%) |
7 (14%) |
14 (9.3%) |
28 (24%) |
24 (26%) |
4 (19%) |
|||
≥ 60 |
174 (64%) |
65 (66%) |
109 (60%) |
180 (90%) |
44 (86%) |
136 (91%) |
87 (76%) |
70 (74%) |
17 (81%) |
|||
Gender |
0.0018 |
0.84 |
0.76 |
|||||||||
Male |
144 (53%) |
40 (41%) |
104 (60%) |
175 (87%) |
44 (86%) |
131 (87%) |
93 (81%) |
75 (80%) |
18 (86%) |
|||
Female |
126 (47%) |
58 (59%) |
68 (40%) |
26 (13%) |
7 (14%) |
19 (13%) |
22 (19%) |
19 (20%) |
3 (14%) |
|||
Smoking status |
0.17 |
0.45 |
1.00 |
|||||||||
Never smoker |
112 (41%) |
46 (47%) |
66 (38%) |
2 (1.0%) |
1 (2.0%) |
1 (0.7%) |
3 (2.6%) |
3 (3.2%) |
0 (0%) |
|||
Ever smoker |
158 (59%) |
52 (53%) |
52 (53%) |
198 (99%) |
50 (98%) |
148 (99%) |
112 (97%) |
91 (97%) |
21 (100%) |
|||
Smoking Index (SI) |
0.36 |
1.00 |
1.00 |
|||||||||
SI < 400 |
150 (56%) |
58 (59%) |
92 (53%) |
13 (6.5%) |
3 (5.9%) |
10 (6.7%) |
18 (16%) |
15 (16%) |
3 (14%) |
|||
SI ≥ 400 |
120 (44%) |
40 (41%) |
80 (47%) |
187 (94%) |
48 (94%) |
139 (93%) |
97 (84%) |
79 (84%) |
18 (86%) |
|||
Tumor size |
0.016 |
0.79 |
0.20 |
|||||||||
≤ 30 mm |
150 (56%) |
64 (65%) |
86 (50%) |
82 (41%) |
20 (39%) |
62 (41%) |
69 (60%) |
59 (63%) |
10 (48%) |
|||
> 30 mm |
119 (44%) |
34 (35%) |
85 (50%) |
119 (59%) |
31 (61%) |
88 (59%) |
46 (40%) |
35 (37%) |
11 (52%) |
|||
p-stage |
0.012 |
0.67 |
0.39 |
|||||||||
I |
152 (56%) |
65 (66%) |
87 (51%) |
117 (58%) |
31 (61%) |
86 (57%) |
53 (47%) |
45 (48%) |
8 (38%) |
|||
II–IV |
118 (44%) |
33 (34%) |
85 (49%) |
84 (42%) |
20 (39%) |
64 (43%) |
61 (54%) |
48 (52%) |
13 (62%) |
|||
Tumor differentiation |
0.045 |
0.040 |
||||||||||
Well |
113 (42%) |
49 (50%) |
64 (37%) |
17 (8.6%) |
1 (2.0%) |
16 (11%) |
||||||
Moderate to poor |
156 (58%) |
49 (50%) |
107 (63%) |
180 (91%) |
49 (98%) |
131 (91%) |
||||||
SCLC or LCNEC |
0.0013 |
|||||||||||
SCLC |
74 (64%) |
67 (71%) |
7 (33%) |
|||||||||
LCNEC |
41 (36%) |
27 (29%) |
14 (67%) |
|||||||||
EGFR status |
0.26 |
|||||||||||
Wild type |
98 (51%) |
32 (46%) |
66 (54%) |
|||||||||
Mutant |
94 (49%) |
38 (54%) |
56 (46%) |
|||||||||
KRAS status |
0.89 |
|||||||||||
Wild type |
168 (88%) |
61 (88%) |
107 (88%) |
|||||||||
Mutant |
23 (12%) |
8 (12%) |
15 (12%) |
|||||||||
ALK rearrangement |
0.75 |
|||||||||||
Negative |
260 (96%) |
95 (97%) |
165 (96%) |
|||||||||
Positive |
10 (3.7%) |
3 (3.1%) |
7 (4.1) |
|||||||||
Neoadjuvant chemotherapy |
0.072 |
|||||||||||
No |
270 (100%) |
98 (100%) |
172 (100%) |
201 (100%) |
51 (100%) |
150 (100%) |
93 (81%) |
73 (78%) |
20 (95%) |
|||
Yes |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
22 (19%) |
21 (22%) |
1 (4.8%) |
|||
Adjuvant chemotherapy |
NA |
NA |
0.16 |
|||||||||
No |
NA |
NA |
NA |
NA |
NA |
NA |
50 (43%) |
38 (40%) |
12 (57%) |
|||
Yes |
NA |
NA |
NA |
NA |
NA |
NA |
65 (57%) |
56 (60%) |
9 (43%) |
|||
Ki-67 index |
0.61 |
|||||||||||
< 60% |
55 (48%) |
46 (49%) |
9 (43%) |
|||||||||
≥ 60% |
60 (52%) |
48 (51%) |
12 (57%) |
|||||||||
The percentages indicate the proportion of cases with a specific clinical, pathological, or molecular feature within each category.
Abbreviations: HGNET, high-grade neuroendocrine tumor; LCNEC, large cell neuroendocrine carcinoma; p-stage, pathological stage; SCLC, small cell lung carcinoma; SI, smoking index = (number of cigarettes per day) × (duration in years); SqCC, squamous cell carcinoma.
TROP2 expression and lung cancer mortality
Out of the 270 patients with adenocarcinoma, there were 149 deaths, including 109 lung cancer-specific deaths, during a median follow-up period of 13.0 years (IQR: 9.1–15.5 years) for the censored cases. High TROP2 expression was associated with shorter lung cancer-specific (log-rank, P = 0.025; Figure 2A) and overall survival (log-rank, P = 0.023; Figure 2B). A univariable Cox regression analysis revealed that high TROP2 expression was associated with shorter lung cancer-specific (univariable hazard ratio [HR] = 1.60, 95% confidence interval [CI] = 1.07–2.44, P = 0.022) and overall survival (univariable HR = 1.49, 95% CI = 1.06–2.13, P = 0.021). In a multivariable analysis, however, the association was not significant for both lung cancer-specific (P = 0.26) and overall survival (P = 0.21) (Table 2). Next, we analyzed the association of other covariates with patient mortality using univariable and multivariable Cox regression analyses. The results showed that p-stage (P < 0.0001), tumor differentiation grade (P = 0.0013), and age (P = 0.043) were confounding factors for TROP2 expression in lung cancer-specific survival (Supplementary Table 1).
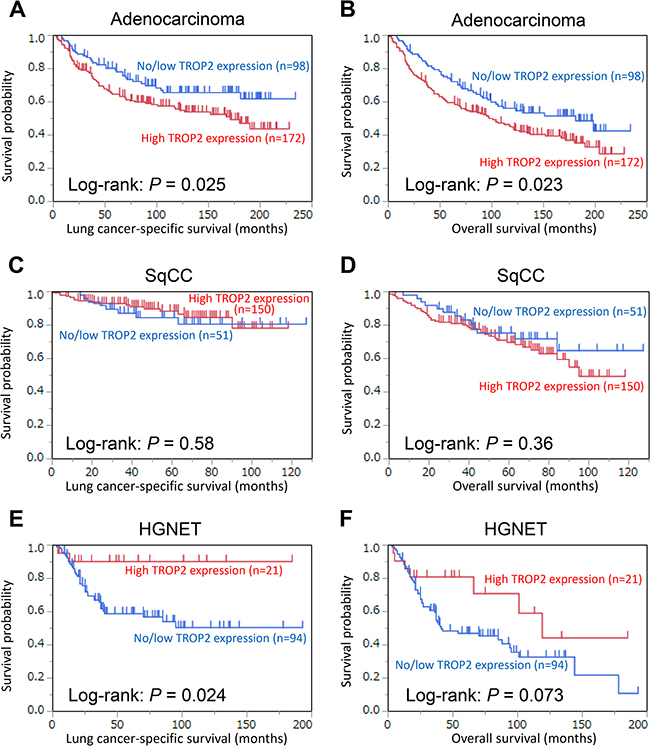
Figure 2: Kaplan–Meier curves for lung cancer-specific (A, C, and E) and overall survival (B, D, and F) according to TROP2 expression levels in tumor cells (no/low vs. high). (A and B) adenocarcinoma, (C and D) squamous cell carcinoma (SqCC), and (E and F) high-grade neuroendocrine tumor (HGNET).
Table 2: TROP2 expression and patient mortalitya in lung cancer
Lung cancer-specific mortality |
Overall mortality |
||||||||||
Univariable analysis |
Multivariable analysisb |
Univariable analysis |
Multivariable analysisb |
||||||||
N of cases |
N of events |
HR (95% CI) |
P-values |
HR (95% CI) |
P-values |
N of events |
HR (95% CI) |
P-values |
HR (95% CI) |
P-values |
|
Adenocarcinoma |
0.022 |
0.26 |
0.021 |
0.21 |
|||||||
No/low TROP2 expression |
98 |
32 |
1 (referent) |
1 (referent) |
46 |
1 (referent) |
1 (referent) |
||||
High TROP2 expression |
172 |
77 |
1.60 (1.07-2.44) |
1.27 (0.84-1.96) |
103 |
1.49 (1.06 -2.13) |
1.25 (0.88-1.80) |
||||
SqCC |
0.59 |
0.56 |
0.35 |
0.35 |
|||||||
No/low TROP2 expression |
51 |
8 |
1 (referent) |
1 (referent) |
13 |
1 (referent) |
1 (referent) |
||||
High TROP2 expression |
150 |
17 |
0.79 (0.35-1.94) |
0.78 (0.35-1.91) |
46 |
1.34 (0.74-2.58) |
1.33 (0.74-2.57) |
||||
HGNET |
0.0096 |
0.0003 |
0.057 |
0.0015 |
|||||||
No/low TROP2 expression |
94 |
38 |
1 (referent) |
1 (referent) |
55 |
1 (referent) |
1 (referent) |
||||
High TROP2 expression |
21 |
2 |
0.23 (0.037-0.74) |
0.13 (0.020-0.44) |
7 |
0.50 (0.21-1.02) |
0.30 (0.12-0.65) |
||||
aCox proportional hazards regression models were used to calculate HR and 95% CI.
bFor adenocarcinoma, the multivariable model initially included age (< 60 years vs. ≥ 60 years), gender (male vs. female), smoking status (ever smoker vs. never smoker), tumor differentiation grade (well vs. moderate-poor), pathological stage (p-stage) (I vs. II–IV), EGFR status (wild type vs. mutant), KRAS status (wild type vs. mutant), and ALK rearrangement status (negative vs. positive). For SqCC, the multivariable model initially included age (< 60 years vs. ≥ 60 years), gender (male vs. female), smoking history (smoking index ≥ 400 vs. < 400), tumor differentiation grade (well vs. moderate-poor), and p-stage (I vs. II–IV). For HGNET, the multivariable model initially included age (< 60 years vs. ≥ 60 years), gender (male vs. female), smoking history (smoking index ≥ 400 vs. < 400), p-stage (I vs. II–IV), histology (SCLC vs. LCNEC), neoadjuvant chemotherapy (yes vs. no), and adjuvant chemotherapy (yes vs. no).
We created missing categories for any missing variables. A backward stepwise elimination with a threshold of P = 0.05 was performed to determine the variables for the final model.
Abbreviations: CI, confidence interval; HGNET, high-grade neuroendocrine tumor; HR, hazard ratio; p-stage, pathological stage; LCNEC, large cell neuroendocrine carcinoma; SCLC, small cell lung carcinoma; SqCC, squamous cell carcinoma.
Out of the 201 patients with SqCC, there were 59 deaths, including 25 lung cancer-specific deaths, during a median follow-up period of 5.0 years (3.1–6.3 years) for the censored cases. High TROP2 expression was not associated with lung cancer-specific (log-rank, P = 0.58; Figure 2C) or overall survival (log-rank, P = 0.36; Figure 2D). A Cox regression analysis revealed that high TROP2 expression was not associated with lung cancer-specific (univariable analysis, P = 0.59 and multivariable analysis, P = 0.56) or overall survival (univariable analysis, P = 0.35 and multivariable analysis, P = 0.35) (Table 2).
Out of the 115 patients with HGNET, there were 62 deaths, including 40 lung cancer-specific deaths, during a median follow-up period of 5.8 years (3.1–8.2 years) for the censored cases. High TROP2 expression was associated with longer lung cancer-specific (log-rank, P = 0.024; Figure 2E) and overall survival (log-rank, P = 0.073; Figure 2F). A univariable Cox regression analysis revealed that high TROP2 expression was associated with longer lung cancer-specific (univariable HR = 0.23, 95% CI = 0.037–0.74, P = 0.0096) and overall survival (univariable HR = 0.50, 95% CI = 0.21–1.02, P = 0.057). A multivariable analysis also showed that high TROP2 expression was associated with longer lung cancer-specific (multivariable HR = 0.13, 95% CI = 0.020–0.44, P = 0.0003) and overall survival (multivariable HR = 0.30, 95% CI = 0.12–0.65, P = 0.0015) (Table 2).
The association of other covariates with patient mortality for adenocarcinoma, SqCC, and HGNET using univariable and multivariable Cox regression analyses is also provided in Supplementary Table 1.
DISCUSSION
We examined the association of TROP2 expression in tumors with clinicopathological/molecular features and with prognosis of various lung cancer subtypes, including adenocarcinoma, SqCC, and HGNET (SCLC and LCNEC). The association of high TROP2 expression with prognosis varied based on the lung cancer subtype. In adenocarcinoma, high TROP2 expression was associated with higher patient mortality. In SqCC, high TROP2 expression was not associated with mortality. In HGNET, high TROP2 expression was unexpectedly associated with lower patient mortality. This study suggests a differential role for TROP2 in different lung cancer subtypes.
Little is known about the association of TROP2 expression with clinicopathological/molecular features and prognosis in lung cancer subtypes. Kobayashi et al. reported that TROP2 overexpression was associated with higher overall mortality in 130 patients with small-sized (< 2cm) lung adenocarcinoma (P = 0.056) [1]. Li et al. showed an association of high TROP2 expression with poor prognosis (P = 0.046) in 68 cases of adenocarcinoma and demonstrated that TROP2 overexpression enhanced cell proliferation, migration, and invasion in the lung adenocarcinoma cell line A549 [3]. In contrast, Pak et al. reported that TROP2 overexpression resulted in a better overall survival in 100 patients with lung adenocarcinoma (P = 0.02) and showed a tendency toward better overall survival in 64 patients with SqCC (P = 0.49) [2]. To the best of our knowledge, our study is the first to examine the prognostic association of TROP2 expression in HGNET (SCLC and LCNEC). In addition, our study used the largest sample sizes of lung adenocarcinoma and SqCC to examine TROP2 expression. We demonstrated that high TROP2 expression was related to differential prognoses based on the lung cancer subtype. High TROP2 expression was associated with higher mortality in lung adenocarcinoma, was not associated with mortality in SqCC, and was associated with lower mortality in HGNET. Similarly, PD-L1 positivity was associated with higher mortality in lung adenocarcinoma [29–31], whereas PD-L1 positivity was related to lower mortality in SCLC [32, 33]. Thus, PD-L1 and TROP2 appear to play different roles depending on the lung cancer subtype. Of interest, high TROP2 expression was significantly more frequent in LCNEC than in SCLC. Emerging evidence suggests that LCNEC is a biologically heterogeneous group, containing SCLC-phenotype/NSCLC-phenotype [34] and YAP1-negative group/YAP1-positive group[35]. There may be an association of high TROP2 expression in LCNEC with SCLC-phenotype/NSCLC-phenotype or YAP1 expression. Because the Ki-67 index was not substantially different according to the TROP2 expression level (no/low vs. high) in HGNET, the other mechanisms except for proliferation, including SCLC-phenotype/NSCLC-phenotype or YAP1 expression, might explain the differential clinicopathological differences according to the TROP2 expression level in HGNET. The use of different downstream signaling pathways may explain the divergent associations of TROP2 expression with prognosis for adenocarcinoma and SqCC [36]. Further studies are required to elucidate the mechanisms accounting for differential clinicopathological associations according to tumor histological subtypes.
We also determined the prevalence of high TROP2 expression and its association with clinicopathological/molecular features in different lung cancer subtypes. A high proportion of patients with adenocarcinoma (64%) and SqCC (75%) showed high TROP2 expression, suggesting that therapies targeting TROP2 may be effective. However, a low proportion of high TROP2 expression was observed in HGNET tumors (18%), suggesting that the probability of good clinical response of HGNET to this type of therapy may be low, although that of TROP2-expressing HGNET may be high. In adenocarcinoma, high TROP2 expression was associated with the male gender, larger tumor size, advanced stage, and less tumor differentiation but not with genetic alterations in EGFR, KRAS, or ALK. In HGNET, 34% (14/41) of LCNEC and 9.5% (7/74) of SCLC tumors showed high TROP2 expression. This information must be useful for the development of therapies targeting TROP2.
A growing body of evidence suggests that TROP2 is a promising molecular target for the treatment of various malignancies [11]. IMMU-132 is an anti-TROP2 ADC that has been shown to be effective against various cancers without severe side effects in various cancers [11–18], including metastatic SCLC [14] and NSCLC resistant to anti-PD-1/PD-L1 therapy [15]. Because little data are available on TROP2 expression in lung cancer, our data are valuable for establishing the utility of TROP2-targeting therapies.
Our study had limitations that need to be stated. First, there is no standardized method for the immunohistochemical assessment of TROP2 expression in tumors, which may influence the reproducibility of the results. We evaluated membranous TROP2 expression in cancer cells because this assessment is required to predict the efficacy of molecular-targeted therapies for lung cancer. However, some studies evaluated both membranous and cytoplasmic TROP2 expression, which could yield conflicting results as to the association of TROP2 expression with clinicopathological/prognostic features. In our study, two pathologists conducted a blinded and independent assessment of TROP2 expression with a good interobserver agreement. Second, we used tissue microarrays to evaluate TROP2 expression in tumors. Intratumoral heterogeneity is a characteristic of lung cancer; thus, tumors with heterogeneous TROP2 expression can affect the results. We speculate that this potential misclassification of tumors based on TROP2 expression would be randomly dispersed; therefore, null results would have been yielded. Nonetheless, we have shown statistically significant results. In addition, an experienced pulmonary pathologist (KI) chose each core site with a relatively large diameter (2 mm) based on the most histologically representative region of the tumor to minimize the chance of this potential misclassification affecting the results. Third, the difference of follow-up periods among the three subtypes might be a potential confounder of our results. Nonetheless, we monitored survivors for the median (interquartile range) of 13.0 years (9.1–15.5 years) in adenocarcinoma, 5.0 years (3.1–6.3 years) in SqCC, and 5.8 years (3.1–8.2 years) in HGNET. Therefore, less time between surgery and death in SqCC and HGNET did not appear to affect our results substantially. Fourth, the total number of patients, especially those with HGNET (N = 115), was not sufficient, and the statistical power was therefore limited. Fifth, our database was retrospectively created. Finally, we only enrolled Japanese patients at a single cancer hospital. Therefore, additional studies in other patient populations are needed.
In conclusion, we demonstrated that the prognostic association of high TROP2 expression differed according to lung cancer subtypes. Although high TROP2 expression was associated with higher mortality in lung adenocarcinoma, it was associated with lower mortality in HGNET, and was not associated with mortality in SqCC. We also determined the prevalence of high TROP2 expression and its association with clinicopathological/molecular features in these lung cancer subtypes. This information is beneficial for determining the utility of TROP2-targeting therapy. Additional large-scale studies are required to confirm our findings.
MATERIALS AND METHODS
Study population
We examined 270 consecutive cases of lung adenocarcinoma, 201 cases of SqCC, and 115 cases of HGNET (74 SCLC cases and 41 LCNEC cases) to assess the TROP2 expression in tumors and survival. Lung adenocarcinoma, SqCC, and HGNET were surgically resected between April 1995 and January 2002, between April 2005 and February 2014, and between July 1990 and November 2014, respectively, at The Cancer Institute Hospital, Japanese Foundation for Cancer Research (JFCR) in Tokyo, Japan. Patients were observed until death or December 1, 2015. For the assessment of smoking history, we used a smoking index (SI) calculated by multiplying the “number of cigarettes per day” by “duration in years.” This study was approved by the institutional review board of JFCR, and informed consent was obtained from all patients included in this study.
Pathological evaluation
Pathological diagnoses were made by experienced expert pulmonary pathologists (KI and YI), essentially based on the 2015 WHO classification of lung tumors [37]. Tumor differentiation grades were defined according to the Japanese Lung Cancer Society criteria [38, 39]. All patients were pathologically staged according to the 7th edition of the AJCC-TNM staging system [40].
Immunohistochemistry for TROP2 and Ki-67
Membranous TROP2 expression of tumor cells was evaluated by an immunohistochemical analysis of tissue microarrays. Using the archived surgical specimens used for initial pathological diagnoses of primary lung cancers, we constructed tissue microarrays as previously described [41]. Briefly, we punched points of the donor paraffin blocks using a 2 mm-diameter coring needle and transferred the tissue to the array in the recipient block using a manual tissue arrayer (KIN-1; Azumaya, Tokyo, Japan). For each tumor, an experienced pulmonary pathologist (KI) selected one site exhibiting the most representative histology for that tumor [42].
Sections with a thickness of 4 μm were immunostained for TROP2 with an anti-TROP2 mouse monoclonal antibody (clone: 1E5-1E2, Daiichi Sankyo Co., Ltd., Tokyo, Japan; diluted 1:400) using the Leica Bond III automated system (Leica Biosystems Melbourne Pty Ltd., Australia). This monoclonal antibody recognizes an epitope in the extracellular domain (Mer1-Thr274) of human TROP2. The sections were incubated at pH 6 for 10 min at 100°C. TROP2 expression on the membranes of tumor cells was interpreted by an experienced pulmonary pathologist (KI) in a blinded manner. The intensity of TROP2 membranous staining in tumor cells was defined as 0 (absent), 1 (weak to moderate), or 2 (strong) (Figure 1). We calculated the percentage of tumor cells at each TROP2 intensity level. For the statistical analyses, we categorized the specimens into two groups based on the staining intensity and percentage of positive cells: no/low TROP2 expression (Intensity 1 < 50% and Intensity 2 < 10%) and high TROP2 expression (Intensity 1 ≥ 50% or Intensity 2 ≥ 10%). A random sample set of 127 cases of lung adenocarcinoma, all 201 cases of SqCC, and all 115 cases of HGNET were blindly examined by a second pathologist (YY). There were high concordances between the two observers, as evidenced by a kappa of 0.66 (95% CI = 0.53–0.79; P < 0.0001) for adenocarcinoma, 0.60 (95% CI = 0.47–0.73;P < 0.0001) for SqCC, and 0.63 (95% CI = 0.45–0.81; P < 0.0001) for HGNET. In addition, to assess intratumoral heterogeneity of TROP2 expression, we immunostained TROP2 using whole sections from 20, 15, and 12 cases of adenocarcinoma, SqCC, and HGNET (6 SCLCs and 6 LCNECs), respectively and did not observe substantial intratumoral heterogeneity in any cases in terms of tumor TROP2 expression.
For HGNET, we also conducted immunostaining for Ki-67 (MIB-1, Dako, Glostrup, Denmark; diluted 1:200) using the Leica Bond III automated system (Leica Biosystems Melbourne Pty Ltd.). The tumor Ki-67 index was calculated by an experienced pulmonary pathologist (KI) in a blinded manner. For the statistical analysis, we categorized the specimens into two groups by the Ki-67 index of 60%, which is a median of all HGNET cases (< 60% vs. ≥ 60%). All 115 cases of HGNET were blindly examined by a second pathologist (YY) with a high concordance between the two observers, as evidenced by a kappa of 0.66 (95% CI = 0.53–0.79; P < 0.0001).
For negative and positive controls, we used a cell array (provided by Daiichi Sankyo Co., Ltd., Tokyo, Japan). This cell array consisted of cell line Calu-6 (ATCC, Manassas, VA, USA) showing very low (below the detection limit) TROP2 expression and N-87 (ATCC) showing high TROP2 expression. Immunohistochemistry was performed using Calu-6 as a specific negative control and N-87 as a positive control. Sections processed with replacement of primary antibody by Dako REAL™ Antibody Diluent (Dako, Glostrup, Denmark) were also used as a non-specific negative control.
Detection of EGFR and KRAS mutations and ALK fusion
Tumor specimens were snap-frozen in liquid nitrogen typically within 20 min after surgical resection and stored at −80°C until use. DNA was extracted using a standard proteinase K digestion and phenol-chloroform extraction. For analysis of the EGFR mutation, we examined four exons (exons 18–21) that code for the tyrosine kinase domain of the EGFR gene. For exons 18 (G719X), 20 (S768I and T790M), and 21 (L858R and L861Q), the TaqManTM SNP Genotyping Assay kit (Applied Biosystems, Foster City, CA, USA) was used according to the manufacturer’s instructions. For exon 19 deletion and exon 20 insertion, a fragment analysis was conducted, as previously described [43]. For the analysis of KRAS mutation, we performed direct sequencing assays for codons 12, 13, and 61, as previously described [43].
For detection of ALK fusion, we performed immunohistochemistry using an anti-ALK mouse monoclonal antibody (clone: 5A4, Leica Biosystems Newcastle Ltd., UK; diluted 1:50) and the Leica Bond III automated system (Leica Biosystems Melbourne Pty Ltd). The sections were incubated at pH 9 for 30 min at 100°C. In the ALK-positive tumors, ALK fusions were confirmed by fluorescence in situ hybridization, as previously described [27].
Statistical analysis
All statistical analyses were conducted using the JMP statistical software package 12 (SAS Institute Inc., Cary, NC, USA) and Excel 2013 software (Microsoft, Redmond, WA, USA). All P-values were two-sided. The statistical significance level was set to P = 0.05.
To investigate the association of TROP2 expression with clinicopathological and molecular features in lung cancer, we used the chi-square or Fisher’s exact test as appropriate.
The Kaplan–Meier method and log-rank test were used for survival analyses. For the analysis of lung cancer-specific mortality, deaths as a result of other causes were censored. We also used univariable and multivariable Cox proportional hazards regression models to calculate HR for mortality according to the TROP2 expression level. For adenocarcinoma, the multivariable model initially included age (< 60 years vs. ≥ 60 years), gender (male vs. female), smoking status (ever smoker vs. never smoker), tumor differentiation grade (well vs. moderate-poor), p-stage (I vs. II–IV),EGFR status (wild type vs. mutant),KRAS status (wild type vs. mutant), and ALK rearrangement status (negative vs. positive). For SqCC, the multivariable model initially included age (< 60 years vs. ≥ 60 years), gender (male vs. female), smoking history (smoking index ≥ 400 vs. < 400), tumor differentiation grade (well vs. moderate-poor), and p-stage (I vs. II–IV). For HGNET, the multivariable model initially included age (< 60 years vs. ≥ 60 years), gender (male vs. female), smoking history (smoking index ≥ 400 vs. < 400), p-stage (I vs. II–IV), histology (SCLC vs. LCNEC), neoadjuvant chemotherapy (yes vs. no), and adjuvant chemotherapy (yes vs. no). We created missing categories for any missing variable, if applicable. A backward stepwise elimination was performed using a P = 0.05 threshold to select variables for the final model. The proportionality of hazards assumption in each subtype was confirmed using the graphs of the log(-log[survival probability]) vs. log of survival time to visually assess if the lines were approximately parallel.
Abbreviations
ADC, antibody-drug conjugate; CI, confidence interval; HGNET, high-grade neuroendocrine tumor; HR, hazard ratio; IQR, interquartile range; LCNEC, large cell neuroendocrine carcinoma; NSCLC, non-small cell lung carcinoma; p-stage, pathological stage; SCLC, small cell lung carcinoma; SI, smoking index; SqCC, squamous cell carcinoma.
Author contributions
K.I., Y.Y., T.S., and Y.I. conceptualized the study and contributed to the development of the study design and methodology. K.I., Y.Y., M.K., H.Ni., R.S., S.S., H.Na., K.N., S.O., and Y.I. were responsible for the collection of tumor tissue, and acquisition of clinical and tumor tissue data, including histopathological and immunohistochemical characteristics. K.I. and Y.I. performed data analysis. All authors contributed to the interpretation of the findings. K.I. drafted the initial manuscript. All authors contributed revisions and read and approved the final draft. K.I. and Y.I. are responsible for the overall content as guarantors.
ACKNOWLEDGMENTS
The authors thank Mr. Motoyoshi Iwakoshi, Ms. Miyuki Kogure, and Ms. Tomoyo Kakita for their technical assistance and Ms. Yuki Takano, Ms. Chikako Yoshida, and Ms. Yuka Toyama for their secretarial expertise.
CONFLICTS OF INTEREST
Y.Y. and T.S. are employees of Daiichi Sankyo Co., Ltd., Tokyo, Japan. Y.I. received research grants from Daiichi Sankyo Co., Ltd., Chugai Pharmaceutical Co. Ltd., and Sony Corp. Y.I. is also a consultant for Fujirebio Inc. All other authors declare no conflict of interest.
GRANT SUPPORT
This study was supported financially by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology, Japan, including JSPS KAKENHI Grant Numbers JP16K08679 (K.I.), JP26430149 (H.Ni.), and JP15H04714 (Y.I.); the Ministry of Health, Labour and Welfare, Japan; the Ministry of the Environment, Japan; the Smoking Research Foundation; and the research grant from Daiichi Sankyo Co., Ltd.
REFERENCES
1. Kobayashi H, Minami Y, Anami Y, Kondou Y, Iijima T, Kano J, Morishita Y, Tsuta K, Hayashi S, Noguchi M. Expression of the GA733 gene family and its relationship to prognosis in pulmonary adenocarcinoma. Virchows Arch. 2010; 457:69-76.
2. Pak MG, Shin DH, Lee CH, Lee MK. Significance of EpCAM and TROP2 expression in non-small cell lung cancer. World J Surg Oncol. 2012; 10:53.
3. Li Z, Jiang X, Zhang W. TROP2 overexpression promotes proliferation and invasion of lung adenocarcinoma cells. Biochem Biophys Res Commun. 2016; 470:197-204.
4. Liu T, Liu Y, Bao X, Tian J, Liu Y, Yang X. Overexpression of TROP2 predicts poor prognosis of patients with cervical cancer and promotes the proliferation and invasion of cervical cancer cells by regulating ERK signaling pathway. PLoS One. 2013; 8:e75864.
5. Cardillo TM, Govindan SV, Sharkey RM, Trisal P, Arrojo R, Liu D, Rossi EA, Chang CH, Goldenberg DM. Sacituzumab Govitecan (IMMU-132), an Anti-Trop-2/SN-38 Antibody-Drug Conjugate: Characterization and Efficacy in Pancreatic, Gastric, and Other Cancers. Bioconjug Chem. 2015; 26:919-931.
6. Trerotola M, Ganguly KK, Fazli L, Fedele C, Lu H, Dutta A, Liu Q, De Angelis T, Riddell LW, Riobo NA, Gleave ME, Zoubeidi A, Pestell RG, et al. Trop-2 is up-regulated in invasive prostate cancer and displaces FAK from focal contacts. Oncotarget. 2015; 6:14318–28. doi: 10.18632/oncotarget.3960.
7. Mao Y, Wang X, Zheng F, Wang C, Tang Q, Tang X, Xu N, Zhang H, Zhang D, Xiong L, Liang J, Zhu J. The tumor-inhibitory effectiveness of a novel anti-Trop2 Fab conjugate in pancreatic cancer. Oncotarget. 2016; 7:24810–23. doi: 10.18632/oncotarget.8529.
8. Xie J, Mølck C, Paquet-Fifield S, Butler L, Sloan E, Ventura S, Hollande F, Australian Prostate Cancer Bioresource. High expression of TROP2 characterizes different cell subpopulations in androgen-sensitive and androgen-independent prostate cancer cells. Oncotarget. 2016; 7:44492–504. doi: 10.18632/oncotarget.9876.
9. Xu N, Zhang Z, Zhu J, Xu L, Li Y, Duan L, Mao Y, Li H. Overexpression of trophoblast cell surface antigen 2 as an independent marker for a poor prognosis and as a potential therapeutic target in epithelial ovarian carcinoma. Int J Exp Pathol. 2016; 97:150-158.
10. Zhao W, Zhu H, Zhang S, Yong H, Wang W, Zhou Y, Wang B, Wen J, Qiu Z, Ding G, Feng Z, Zhu J. Trop2 is overexpressed in gastric cancer and predicts poor prognosis. Oncotarget. 2016; 7:6136–45. doi: 10.18632/oncotarget.6733.
11. Shvartsur A, Bonavida B. Trop2 and its overexpression in cancers: regulation and clinical/therapeutic implications. Genes Cancer. 2015; 6:84–105. doi: 10.18632/genesandcancer.40.
12. Strop P, Tran TT, Dorywalska M, Delaria K, Dushin R, Wong OK, Ho WH, Zhou D, Wu A, Kraynov E, Aschenbrenner L, Han B, O’Donnell CJ, et al. Abstract 2640: RN927C, a potent site-specific Trop-2 antibody-drug-conjugate (ADC) for treatment of solid tumors. Cancer Research. 2014; 74:2640.
13. Goldenberg DM, Cardillo TM, Govindan SV, Rossi EA, Sharkey RM. Trop-2 is a novel target for solid cancer therapy with sacituzumab govitecan (IMMU-132), an antibody-drug conjugate (ADC). Oncotarget. 2015; 6:22496–512. doi: 10.18632/oncotarget.4318.
14. Starodub A, Camidge DR, Scheff RJ, Thomas SS, Guarino MJ, Masters GA, Kalinsky K, Gandhi L, Bardia A, Messersmith WA, Ocean AJ, Maliakal PP, Sharkey RM, et al. Trop-2 as a therapeutic target for the antibody-drug conjugate (ADC), sacituzumab govitecan (IMMU-132), in patients (pts) with previously treated metastatic small-cell lung cancer (mSCLC). J Clin Oncol. 2016; 34: abst 8559.
15. Camidge DR, Heist RS, Masters GA, Scheff RJ, Starodub A, Messersmith WA, Bardia A, Ocean AJ, Horn L, Berlin J, Maliakal PP, Sharkey RM, Wilhelm F, et al. Therapy of metastatic, non-small cell lung cancer (mNSCLC) with the anti-Trop-2-SN-38 antibody-drug conjugate (ADC), sacituzumab govitecan (IMMU-132). J Clin Oncol. 2016; 34: abst 9011.
16. Sharkey RM, McBride WJ, Cardillo TM, Govindan SV, Wang Y, Rossi EA, Chang CH, Goldenberg DM. Enhanced Delivery of SN-38 to Human Tumor Xenografts with an Anti-Trop-2-SN-38 Antibody Conjugate (Sacituzumab Govitecan). Clin Cancer Res. 2015; 21:5131-5138.
17. Chang CH, Wang Y, Zalath M, Liu D, Cardillo TM, Goldenberg DM. Combining ABCG2 Inhibitors with IMMU-132, an Anti-Trop-2 Antibody Conjugate of SN-38, Overcomes Resistance to SN-38 in Breast and Gastric Cancers. Mol Cancer Ther. 2016; 15:1910-1919.
18. Strop P, Tran TT, Dorywalska M, Delaria K, Dushin R, Wong OK, Ho WH, Zhou D, Wu A, Kraynov E, Aschenbrenner L, Han B, O’Donnell CJ, et al. RN927C, a site-specific Trop-2 antibody-drug-conjugate (ADC) with enhanced stability, is highly efficacious in preclinical solid tumor models. Mol Cancer Ther. 2016; 15:2698-2708.
19. Bardia A, Diamond JR, Mayer IA, Starodub AN, Moroose RL, Isakoff SJ, Ocean AJ, Guarino MJ, Berlin JD, Messersmith WA, Thomas SS, O’Shaughnessy JA, Kalinsky K, et al. Safety and efficacy of anti-Trop-2 antibody drug conjugate, sacituzumab govitecan (IMMU-132), in heavily pretreated patients with TNBC. Cancer Research. 2016; 76: abst PD3-06.
20. Rikova K, Guo A, Zeng Q, Possemato A, Yu J, Haack H, Nardone J, Lee K, Reeves C, Li Y, Hu Y, Tan Z, Stokes M, et al. Global survey of phosphotyrosine signaling identifies oncogenic kinases in lung cancer. Cell. 2007; 131:1190-1203.
21. Govindan R, Ding L, Griffith M, Subramanian J, Dees ND, Kanchi KL, Maher CA, Fulton R, Fulton L, Wallis J, Chen K, Walker J, McDonald S, et al. Genomic landscape of non-small cell lung cancer in smokers and never-smokers. Cell. 2012; 150:1121-1134.
22. Imielinski M, Berger AH, Hammerman PS, Hernandez B, Pugh TJ, Hodis E, Cho J, Suh J, Capelletti M, Sivachenko A, Sougnez C, Auclair D, Lawrence MS, et al. Mapping the hallmarks of lung adenocarcinoma with massively parallel sequencing. Cell. 2012; 150:1107-1120.
23. The Cancer Genome Atlas Research Network. Comprehensive genomic characterization of squamous cell lung cancers. Nature. 2012; 489:519-525.
24. The Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature. 2014; 511:543-550.
25. George J, Lim JS, Jang SJ, Cun Y, Ozretic L, Kong G, Leenders F, Lu X, Fernandez-Cuesta L, Bosco G, Muller C, Dahmen I, Jahchan NS, et al. Comprehensive genomic profiles of small cell lung cancer. Nature. 2015; 524:47-53.
26. Huang P, Cheng CL, Chang YH, Liu CH, Hsu YC, Chen JS, Chang GC, Ho BC, Su KY, Chen HY, Yu SL. Molecular gene signature and prognosis of non-small cell lung cancer. Oncotarget. 2016; 7:51898–907. doi: 10.18632/oncotarget.10622.
27. Takeuchi K, Soda M, Togashi Y, Suzuki R, Sakata S, Hatano S, Asaka R, Hamanaka W, Ninomiya H, Uehara H, Lim Choi Y, Satoh Y, Okumura S, et al. RET, ROS1 and ALK fusions in lung cancer. Nat Med. 2012; 18:378-381.
28. Inamura K, Ishikawa Y. MicroRNA In Lung Cancer: Novel Biomarkers and Potential Tools for Treatment. J Clin Med. 2016; 5:36.
29. Tang Y, Fang W, Zhang Y, Hong S, Kang S, Yan Y, Chen N, Zhan J, He X, Qin T, Li G, Tang W, Peng P, Zhang L. The association between PD-L1 and EGFR status and the prognostic value of PD-L1 in advanced non-small cell lung cancer patients treated with EGFR-TKIs. Oncotarget. 2015; 6:14209–19. doi: 10.18632/oncotarget.3694.
30. Mao Y, Li W, Chen K, Xie Y, Liu Q, Yao M, Duan W, Zhou X, Liang R, Tao M. B7-H1 and B7-H3 are independent predictors of poor prognosis in patients with non-small cell lung cancer. Oncotarget. 2015; 6:3452–61. doi: 10.18632/oncotarget.3097.
31. Inamura K, Yokouchi Y, Sakakibara R, Kobayashi M, Subat S, Ninomiya H, Nagano H, Nomura K, Okumura S, Ishikawa Y. Relationship of tumor PD-L1 expression with EGFR wild-type status and poor prognosis in lung adenocarcinoma. Jpn J Clin Oncol. 2016; 46:935-941.
32. Ishii H, Azuma K, Kawahara A, Yamada K, Imamura Y, Tokito T, Kinoshita T, Kage M, Hoshino T. Significance of programmed cell death-ligand 1 expression and its association with survival in patients with small cell lung cancer. J Thorac Oncol. 2015; 10:426-430.
33. Miao L, Lu Y, Xu Y, Zhang G, Huang Z, Gong L, Fan Y. PD-L1 and c-MET expression and survival in patients with small cell lung cancer. Oncotarget. 2016 June 1. doi: 10.18632/oncotarget.9765 [Epub Ahead of Print].
34. Rekhtman N, Pietanza MC, Hellmann MD, Naidoo J, Arora A, Won H, Halpenny DF, Wang H, Tian SK, Litvak AM, Paik PK, Drilon AE, Socci N, et al. Next-Generation Sequencing of Pulmonary Large Cell Neuroendocrine Carcinoma Reveals Small Cell Carcinoma-like and Non-Small Cell Carcinoma-like Subsets. Clin Cancer Res. 2016; 22:3618-3629.
35. Ito T, Matsubara D, Tanaka I, Makiya K, Tanei ZI, Kumagai Y, Shiu SJ, Nakaoka HJ, Ishikawa S, Isagawa T, Morikawa T, Shinozaki-Ushiku A, Goto Y, et al. Loss of YAP1 defines neuroendocrine differentiation of lung tumors. Cancer Sci. 2016; 107:1527-1538.
36. Stjernstrom A, Karlsson C, Fernandez OJ, Soderkvist P, Karlsson MG, Thunell LK. Alterations of INPP4B, PIK3CA and pAkt of the PI3K pathway are associated with squamous cell carcinoma of the lung. Cancer Med. 2014; 3:337-348.
37. Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. (2015). WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th ed. (Lyon: IARC Press).
38. Japan Lung Cancer Society. (1999). General Rules for Clinical and Pathologic Record of Lung Cancer [in Japanese], 5th ed. (Tokyo: Kanahara).
39. Inamura K, Satoh Y, Okumura S, Nakagawa K, Tsuchiya E, Fukayama M, Ishikawa Y. Pulmonary adenocarcinomas with enteric differentiation: histologic and immunohistochemical characteristics compared with metastatic colorectal cancers and usual pulmonary adenocarcinomas. Am J Surg Pathol. 2005; 29:660-665.
40. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. (2010). AJCC cancer staging manual. (New York: Springer).
41. Hiramatsu M, Ninomiya H, Inamura K, Nomura K, Takeuchi K, Satoh Y, Okumura S, Nakagawa K, Yamori T, Matsuura M, Morikawa T, Ishikawa Y. Activation status of receptor tyrosine kinase downstream pathways in primary lung adenocarcinoma with reference of KRAS and EGFR mutations. Lung Cancer. 2010; 70:94-102.
42. Inamura K, Yokouchi Y, Kobayashi M, Sakakibara R, Ninomiya H, Subat S, Nagano H, Nomura K, Okumura S, Shibutani T, Ishikawa Y. Tumor B7-H3 (CD276) expression and smoking history in relation to lung adenocarcinoma prognosis. Lung Cancer. 2017; 103:44-51.
43. Inamura K, Togashi Y, Nomura K, Ninomiya H, Hiramatsu M, Okui M, Satoh Y, Okumura S, Nakagawa K, Tsuchiya E, Ishikawa Y. Up-regulation of PTEN at the transcriptional level is an adverse prognostic factor in female lung adenocarcinomas. Lung Cancer. 2007; 57:201-206.