
INTRODUCTION
Alcohol-induced osteonecrosis of the femoral head (ONFH) is a degenerative lesion of joints and a partial blood circulation disorder of the femoral head. It has several complex causes that are common to non-traumatic ONFH and results in further osteocyte ischemia, necrosis, bone trabecula fracture, and complete collapse of the femoral head [1]. It causes a destructive femoral head collapse in approximately 80% of patients without treatment [2, 3]. Because drinking has become a global health concern, the World Health Organization (WHO) has identified high alcohol consumption as one of the most important pathogenic factors of alcohol-induced ONFH (http://www.who.int/entity/substanceabuse/publications/globalalcoholreport/msbgsrwpr.pdf), and the incidence of this disease is rising worldwide. For example, the overall number of osteonecrosis cases in China has almost reached 7 million and 100,000 to 200,000 new patients are diagnosed each year [4], approximately one-third of whom have alcohol-induced ONFH. This multifactorial disease is the result of several complicated interactions among environmental, lifestyle, metabolic and genetic factors [5–7]. The widely known pathologic mechanisms of alcohol-induced ONFH are dyslipidemia, osteoporosis, intraosseous hypertension, gene-associated mechanisms, and the abnormal differentiation of osteoblasts/osteoclasts from bone marrow mesenchymal stem cells (BMSCs), and most of the mechanisms are related to the pathologic process of dyslipidemia. So, more investigation of the pathologic mechanisms of alcohol-induced ONFH from different perspectives is needed. Genetic research offers insight into the occurrence, treatment and development of alcohol-induced ONFH, and genetic variations are identified as a normal biological phenomenon that influences immunoreaction and protein transcription and even determine individual susceptibilities of some pathological diseases of the joints [8–10]. Although many people drink, only some of them experience alcohol-induced ONFH, illustrating that individual susceptibilities might cause different incidences of this disease among different populations. Single-nucleotide polymorphisms (SNPs) have been widely researched because of their variations in a single base pair in the DNA sequence. On the basis of previous studies, we found the polymorphisms of several genes, including ApoA1, ApoB, SREBF1 and TLR4 were associated with the risk of alcohol-induced ONFH [4, 11–13].
Matrix metalloproteinases (MMPs) are a family of proteases that could be involved in the degradation of osseous tissue and other extracellular matrices in the human body. Among the more than 20 types of MMP genes, MMP-3 and MMP-8 are the most influential. MMP-3 encodes an enzyme that degrades fibronectin, laminin, collagens III, IV, IX, and X, and cartilage proteoglycans [14]. MMP-8 is involved in the breakdown of the extracellular matrix in embryonic development, reproduction, and tissue remodeling [15]. Previous studies show that several types of MMPs are abnormally expressed in different orthopedic diseases. MMP-1 and MMP-3 are overexpressed in the synoviocytes and chondrocytes of osteoarthritis patients. MMP-2 and MMP-9 are overexpressed in the serum and synovia of osteoarthritis patients [16]. Collectively, the dynamic equilibrium of MMPs and their natural inhibitors, tissue inhibitors of metalloproteinases (TIMPs), can significantly influence bone metabolism in the human body [17]. However, no studies have explored the relation between MMP-3 and MMP-8 in the MMP/TIMP pathway and alcohol-induced ONFH. Our case-control study investigated whether MMP-3 and MMP-8 have a potential association with alcohol-induced ONFH among a population of Chinese males at a genetic level.
RESULTS
We performed a case-control study that selected 695 individuals, including 299 alcohol-induced ONFH patients (mean age: 43.24 ± 13.07) and 396 healthy control subjects (mean age: 47.62 ± 10.28). All the individuals are males (Table 1). We researched eight SNPs (rs639752, rs650108, rs520540, rs646910, rs602128, rs679620, rs678815, and rs522616) on gene MMP-3 and five SNPs (rs3740938, rs2012390, rs1940475, rs11225394, and rs11225395) on gene MMP-8. The basic SNP information of all the individuals in our study, including the minor allele frequency (MAF), odds ratios (ORs), 95% confidence intervals (95% CIs), position, band, alleles, and the P-values of alleles evaluated by χ2 test, are shown in Table 2. All 13 SNPs are in accord with the Hardy-Weinberg equilibrium (HWE) (P > 0.05). The minor allele G of rs650108 on MMP-3 was significantly associated with 0.78-fold decreased alcohol-induced ONFH risk (OR = 0.78, 95% CI = 0.63-0.97, P = 0.026). All the primers utilized for genotyping in this study are listed in Table 7 , and the statistical power of the SNPs in our study are listed in the Table 8.
Table 1: Characteristics of the male individuals in controls and alcohol-induced ONFH
Group |
N |
Mean |
Std. Deviation |
Mean±SD |
P-value |
|
Age |
Case |
299 |
43.24 |
13.07 |
43.24±13.07 |
P < 0.001* |
Control |
396 |
47.62 |
10.28 |
47.62±10.28 |
*P values was calculated by Welch’s t-tests
Table 2: Basic SNP information summary of all the male individuals in our study
Gene |
SNP ID |
Position |
Band |
Alleles Aa/B |
MAF |
Role |
HWE-P |
OR(95%CI) |
Pb value |
|
Case |
Control |
|||||||||
MMP-3 |
rs639752 |
102707339 |
11q22.3 |
C/A |
0.31 |
0.36 |
Intron |
0.27 |
0.82(0.65-1.02) |
0.079 |
MMP-3 |
rs650108 |
102708787 |
11q22.3 |
G/A |
0.39 |
0.45 |
Intron |
0.54 |
0.78(0.63-0.97) |
0.026* |
MMP-3 |
rs520540 |
102709425 |
11q22.3 |
A/G |
0.31 |
0.36 |
Coding exon |
0.27 |
0.82(0.65-1.02) |
0.079 |
MMP-3 |
rs646910 |
102709522 |
11q22.3 |
A/T |
0.08 |
0.09 |
Intron (boundary) |
0.76 |
0.83(0.57-1.23) |
0.354 |
MMP-3 |
rs602128 |
102713465 |
11q22.3 |
A/G |
0.31 |
0.36 |
Coding exon |
0.51 |
0.83(0.66-1.04) |
0.104 |
MMP-3 |
rs679620 |
102713620 |
11q22.3 |
T/C |
0.31 |
0.36 |
Coding exon |
0.44 |
0.81(0.65-1.02) |
0.074 |
MMP-3 |
rs678815 |
102713777 |
11q22.3 |
G/C |
0.31 |
0.36 |
Intron |
0.33 |
0.81(0.65-1.02) |
0.075 |
MMP-3 |
rs522616 |
102715048 |
11q22.3 |
C/T |
0.39 |
0.34 |
Promoter |
1.00 |
1.24(1.00-1.55) |
0.054 |
MMP-8 |
rs3740938 |
102587062 |
11q22.3 |
A/G |
0.23 |
0.26 |
Coding exon |
0.70 |
0.83(0.64-1.06) |
0.134 |
MMP-8 |
rs2012390 |
102590777 |
11q22.3 |
G/A |
0.26 |
0.3 |
Intron |
0.48 |
0.79(0.63-1.01) |
0.058 |
MMP-8 |
rs1940475 |
102593248 |
11q22.3 |
T/C |
0.36 |
0.39 |
Coding exon |
1.00 |
0.90(0.73-1.13) |
0.371 |
MMP-8 |
rs11225394 |
102595413 |
11q22.3 |
T/C |
0.11 |
0.08 |
Intron (boundary) |
1.00 |
1.42(0.98-2.05) |
0.059 |
MMP-8 |
rs11225395 |
102596480 |
11q22.3 |
A/G |
0.35 |
0.38 |
Promoter |
1.00 |
0.90(0.72-1.12) |
0.336 |
SNP, single nucleotide polymorphism; MAF, minor allele frequency; HWE, Hardy-Weinberg equilibrium; ORs, odds ratios; CI, confidence interval;
a Minor allele
b P were adjusted by gender and age, * P < 0.05, statistical significance
We developed a hypothesis that compared each minor allele with the corresponding wild-type allele. Every minor allele on an SNP was one risk factor, and we built five different genetic models and used unconditional logistic regression to assess the relation between SNPs and alcohol-induced ONFH risk. The results are shown in Table 3 . We found that rs650108 on MMP-3 was related to a decreased risk of alcohol-induced ONFH in the dominant model (OR = 0.69, 95% CI = 0.50-0.95, P = 0.023) and the log-additive model (OR = 0.78, 95% CI = 0.63-0.97, P = 0.025). We also found that rs11225394 on MMP-8 was related to an increased alcohol-induced ONFH risk in the codominant model (OR = 1.59, 95% CI = 1.08-2.36, P = 0.021), the dominant model (OR = 1.54, 95% CI = 1.04-2.27, P = 0.030), and the over-dominant model (OR = 1.60, 95% C I = 1.08-2.38, P = 0.018).
Table 3: Analysis of the association between SNPs and alcohol-induced ONFH risk in males (based on logistical tests)
SNP ID |
Model |
Genotype |
Group=control |
Group=Alcohol |
OR (95% CI) |
P-value |
AIC |
BIC |
rs650108 (MMP-3) |
Codominant |
A/A |
116 (29.4%) |
112 (37.6%) |
1 |
0.064 |
947.6 |
961.2 |
A/G |
202 (51.1%) |
139 (46.6%) |
0.71 (0.51-1.00) |
|||||
G/G |
77 (19.5%) |
47 (15.8%) |
0.63 (0.40-0.99) |
|||||
Dominant |
A/A |
116 (29.4%) |
112 (37.6%) |
1 |
0.023* |
945.9 |
955 |
|
A/G-G/G |
279 (70.6%) |
186 (62.4%) |
0.69 (0.50-0.95) |
|||||
Recessive |
A/A-A/G |
318 (80.5%) |
251 (84.2%) |
1 |
0.200 |
949.5 |
958.5 |
|
G/G |
77 (19.5%) |
47 (15.8%) |
0.77 (0.52-1.15) |
|||||
Overdominant |
A/A-G/G |
193 (48.9%) |
159 (53.4%) |
1 |
0.240 |
949.7 |
958.8 |
|
A/G |
202 (51.1%) |
139 (46.6%) |
0.84 (0.62-1.13) |
|||||
Log-additive |
--- |
--- |
--- |
0.78 (0.63-0.97) |
0.025* |
946.1 |
955.2 |
|
rs11225394 (MMP-8) |
Codominant |
C/C |
327 (84.7%) |
234 (78.3%) |
1 |
0.021* |
936.8 |
950.4 |
T/C |
57 (14.8%) |
65 (21.7%) |
1.59 (1.08-2.36) |
|||||
T/T |
2 (0.5%) |
0 (0%) |
0.00 (0.00-NA) |
|||||
Dominant |
C/C |
327 (84.7%) |
234 (78.3%) |
1 |
0.030* |
937.8 |
946.9 |
|
T/C-T/T |
59 (15.3%) |
65 (21.7%) |
1.54 (1.04-2.27) |
|||||
Recessive |
C/C-T/C |
384 (99.5%) |
299 (100%) |
1 |
0.130 |
940.2 |
949.3 |
|
T/T |
2 (0.5%) |
0 (0%) |
0.00 (0.00-NA) |
|||||
Overdominant |
C/C-T/T |
329 (85.2%) |
234 (78.3%) |
1 |
0.018* |
937 |
946 |
|
T/C |
57 (14.8%) |
65 (21.7%) |
1.60 (1.08-2.38) |
|||||
Log-additive |
--- |
--- |
--- |
1.46 (1.00-2.13) |
0.052 |
938.8 |
947.8 |
SNP, single nucleotide polymorphism; ORs, odds ratios; CI, confidence interval; AIC, Akaike’s Information criterion; BIC, Bayesian Information criterion.
P value was calculated with logistic analysis. * P < 0.05, statistical significance.
Furthermore, we found that the results were still superior after adjusting for age, and we also found another SNP (rs2012390) on MMP-8 that was significant but not superior. After adjusting for age, we found, as shown in Table 4, that rs650108 on MMP-3 was associated with a decreased alcohol-induced ONFH risk in the dominant model (OR = 0.68, 95% CI = 0.49-0.95, P = 0.022) and the log-additive model (OR = 0.78, 95% CI = 0.63-0.98, P = 0.030), and rs11225394 on MMP-8 was associated with an increased risk of alcohol-induced ONFH in the codominant model (OR = 1.72, 95% CI = 1.15-2.58, P = 0.010), the dominant model (OR = 1.67, 95% CI = 1.12-2.48, P = 0.012), the over-dominant model (OR = 1.73, 95% CI = 1.16-2.59, P = 0.007), and the log-additive model (OR = 1.57, 95% CI = 1.07-2.32, P = 0.022). Additionally, we found that rs2012390 on MMP-8 was significant and associated with a decreased alcohol-induced ONFH risk in the dominant model (OR=0.72, 95% CI = 0.53-0.97, P = 0.032) and the log-additive model (OR = 0.77, 95% CI = 0.60-0.98, P = 0.035).
Table 4: Analysis of the association between SNPs and alcohol-induced ONFH risk in males (adjusted for age)
SNP ID |
Model |
Genotype |
Group=control |
Group=Alcohol |
OR (95% CI) |
P-value |
AIC |
BIC |
rs650108 (MMP-3) |
Codominant |
A/A |
116 (29.4%) |
112 (37.6%) |
1 |
0.066 |
925.6 |
943.7 |
A/G |
202 (51.1%) |
139 (46.6%) |
0.70 (0.49-0.98) |
|||||
G/G |
77 (19.5%) |
47 (15.8%) |
0.64 (0.41-1.01) |
|||||
Dominant |
A/A |
116 (29.4%) |
112 (37.6%) |
1 |
0.022* |
923.7 |
937.3 |
|
A/G-G/G |
279 (70.6%) |
186 (62.4%) |
0.68 (0.49-0.95) |
|||||
Recessive |
A/A-A/G |
318 (80.5%) |
251 (84.2%) |
1 |
0.270 |
927.8 |
941.4 |
|
G/G |
77 (19.5%) |
47 (15.8%) |
0.80 (0.53-1.19) |
|||||
Overdominant |
A/A-G/G |
193 (48.9%) |
159 (53.4%) |
1 |
0.190 |
927.2 |
940.9 |
|
A/G |
202 (51.1%) |
139 (46.6%) |
0.81 (0.60-1.11) |
|||||
Log-additive |
--- |
--- |
--- |
0.78 (0.63-0.98) |
0.030* |
924.3 |
937.9 |
|
rs2012390 (MMP-8) |
Codominant |
A/A |
189 (47.7%) |
165 (55.4%) |
1 |
0.095 |
928.2 |
946.4 |
A/G |
174 (43.9%) |
113 (37.9%) |
0.73 (0.53-1.00) |
|||||
G/G |
33 (8.3%) |
20 (6.7%) |
0.65 (0.36-1.19) |
|||||
Dominant |
A/A |
189 (47.7%) |
165 (55.4%) |
1 |
0.032* |
926.4 |
940 |
|
A/G-G/G |
207 (52.3%) |
133 (44.6%) |
0.72 (0.53-0.97) |
|||||
Recessive |
A/A-A/G |
363 (91.7%) |
278 (93.3%) |
1 |
0.330 |
930 |
943.6 |
|
G/G |
33 (8.3%) |
20 (6.7%) |
0.75 (0.42-1.35) |
|||||
Overdominant |
A/A-G/G |
222 (56.1%) |
185 (62.1%) |
1 |
0.100 |
928.2 |
941.9 |
|
A/G |
174 (43.9%) |
113 (37.9%) |
0.77 (0.56-1.05) |
|||||
Log-additive |
--- |
--- |
--- |
0.77 (0.60-0.98) |
0.035* |
926.5 |
940.1 |
|
rs11225394 (MMP-8) |
Codominant |
C/C |
327 (84.7%) |
234 (78.3%) |
1 |
0.001* |
914.9 |
933 |
T/C |
57 (14.8%) |
65 (21.7%) |
1.72 (1.15-2.58) |
|||||
T/T |
2 (0.5%) |
0 (0%) |
0.00 (0.00-NA) |
|||||
Dominant |
C/C |
327 (84.7%) |
234 (78.3%) |
1 |
0.012* |
915.8 |
929.4 |
|
T/C-T/T |
59 (15.3%) |
65 (21.7%) |
1.67 (1.12-2.48) |
|||||
Recessive |
C/C-T/C |
384 (99.5%) |
299 (100%) |
1 |
0.140 |
920 |
933.5 |
|
T/T |
2 (0.5%) |
0 (0%) |
0.00 (0.00-NA) |
|||||
Overdominant |
C/C-T/T |
329 (85.2%) |
234 (78.3%) |
1 |
0.007* |
914.8 |
928.4 |
|
T/C |
57 (14.8%) |
65 (21.7%) |
1.73 (1.16-2.59) |
|||||
Log-additive |
--- |
--- |
--- |
1.57 (1.07-2.32) |
0.022* |
916.9 |
930.5 |
ORs, odds ratios; CI, confidence interval; AIC, Akaike’s Information criterion; BIC, Bayesian Information criterion.
P value was adjusted by age and gender; * P < 0.05, statistical significance.
Our study used polymorphism detection to analyze the pairwise linkage disequilibrium (LD) of MMP-3 and MMP-8. The parameters r2 and D′ were used to analyze the LD pattern, and the results are shown in Figure 1 and Table 5 . We observed one block in MMP-3, including eight SNPs: rs639752, rs650108, rs520540, rs646910, rs602128, rs679620, rs678815, and rs522616. We used χ2 and logistic tests to analyze the haplotype (Table 5). The CGATATGT sequence was found to be associated with a significantly decreased alcohol-induced ONFH risk after adjustment for age (OR = 0.75, 95% CI = 0.57-0.97, P = 0.029). Additionally, we did not find any association between alcohol-induced ONFH and MMP-8 after analyzing the pairwise LD, the results are shown in Table 6 and Figure 2.
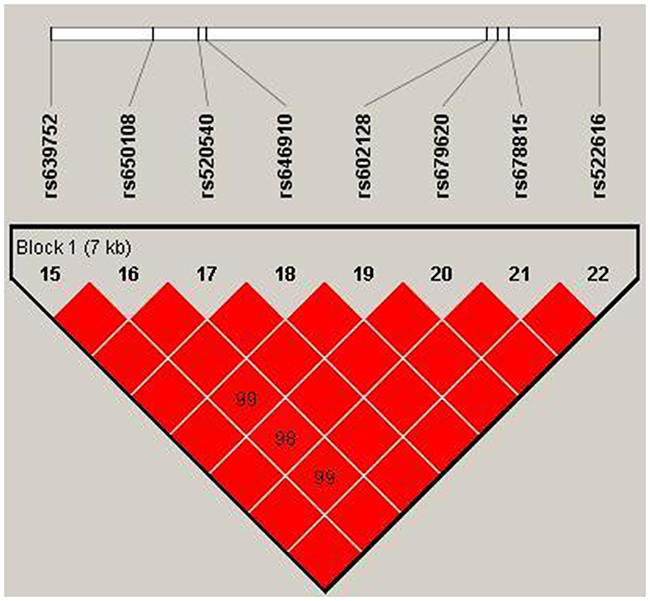
Figure 1: We used the parameters r2 and D′ to analyze the linkage disequilibrium (LD) of the SNPs on MMP-3. Significant LD is indicated by bright red standard colors.
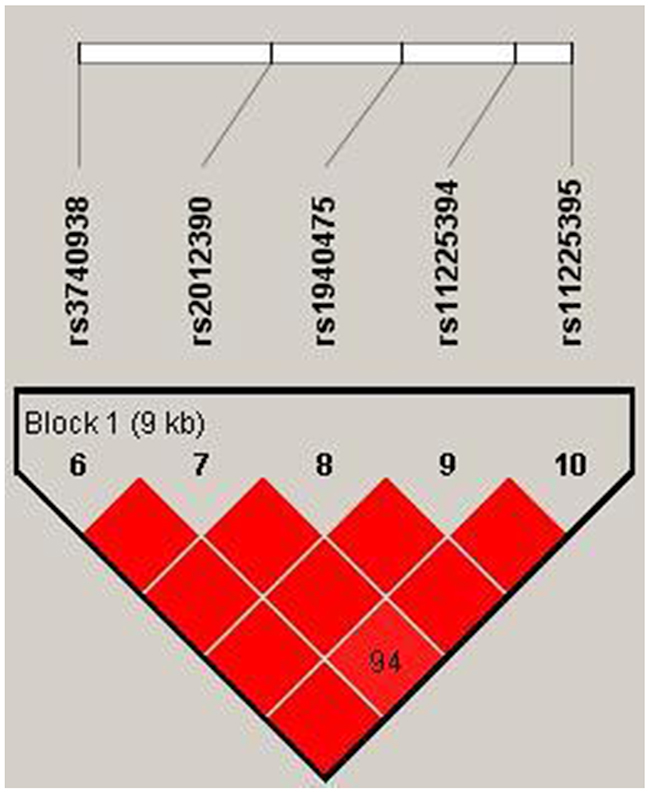
Figure 2: We used the parameters r2 and D′’ to analyze the linkage disequilibrium (LD) of the SNPs on MMP-8. Significant LD is indicated by bright red standard colors.
Table 5: Haplotype association with response (n=695, adjusted by age).
rs639752 |
rs650108 |
rs520540 |
rs646910 |
rs602128 |
rs679620 |
rs678815 |
rs522616 |
Freq |
OR (95% CI) |
P-value |
|
1 |
A |
A |
G |
T |
G |
C |
C |
C |
0.3655 |
1 |
--- |
2 |
C |
G |
A |
T |
A |
T |
G |
T |
0.3367 |
0.75 (0.57 - 0.97) |
0.029* |
3 |
A |
A |
G |
T |
G |
C |
C |
T |
0.2079 |
0.88 (0.65 - 1.18) |
0.380 |
4 |
A |
G |
G |
A |
G |
C |
C |
T |
0.0849 |
0.75 (0.50 - 1.14) |
0.190 |
rare |
* |
* |
* |
* |
* |
* |
* |
* |
0.005 |
0.47 (0.08 - 2.75) |
0.400 |
Global haplotype association P-value: 0.19
rs639752, rs650108, rs520540, rs646910, rs602128, rs679620, rs678815 and rs522616 are on gene MMP-3
ORs, odds ratios; CI, confidence interval;
* P < 0.05, statistical significance.
Table 6: Haplotype association with response (n=695, adjusted by age).
rs3740938 |
rs2012390 |
rs1940475 |
rs11225394 |
rs11225395 |
Freq |
OR (95% CI) |
P-value |
|
1 |
G |
A |
C |
C |
G |
0.6226 |
1 |
--- |
2 |
A |
G |
T |
C |
A |
0.2457 |
0.81 (0.62 - 1.05) |
0.12 |
3 |
G |
A |
T |
T |
A |
0.0928 |
1.37 (0.93 - 2.03) |
0.11 |
4 |
G |
G |
T |
C |
A |
0.0267 |
0.55 (0.26 - 1.13) |
0.11 |
5 |
G |
G |
T |
C |
G |
0.0108 |
1.02 (0.35 - 2.97) |
0.97 |
Global haplotype association p-value: 0.021
Table 7: All the information of the primers in this case-control study
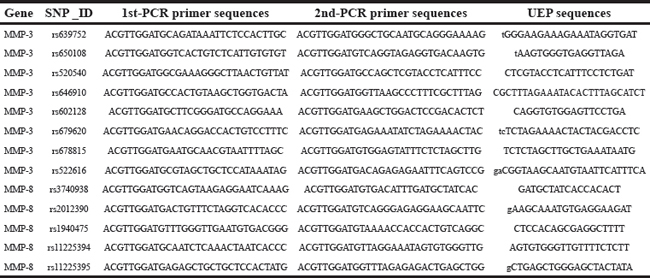
Table 8: All the statistical power of the SNPs in this study
SNP_ID |
Gene(s) |
case _n1 |
control _n2 |
case _A |
control _A |
case _p1 |
contol _p2 |
p |
zβ |
power |
rs639752 |
MMP3 |
598 |
792 |
186 |
186 |
0.311037 |
0.234848 |
0.267626 |
1.206173 |
0.886124538 |
rs650108 |
MMP3 |
596 |
790 |
233 |
233 |
0.39094 |
0.294937 |
0.336219 |
1.777753 |
0.962277821 |
rs520540 |
MMP3 |
598 |
792 |
186 |
186 |
0.311037 |
0.234848 |
0.267626 |
1.206173 |
0.886124538 |
rs646910 |
MMP3 |
598 |
792 |
46 |
46 |
0.076923 |
0.058081 |
0.066187 |
-0.55131 |
0.290709864 |
rs602128 |
MMP3 |
596 |
782 |
187 |
187 |
0.313758 |
0.23913 |
0.271408 |
1.117555 |
0.868121497 |
rs679620 |
MMP3 |
598 |
792 |
187 |
187 |
0.312709 |
0.236111 |
0.269065 |
1.217832 |
0.88835615 |
rs678815 |
MMP3 |
592 |
790 |
185 |
185 |
0.3125 |
0.234177 |
0.267728 |
1.282388 |
0.900146697 |
rs522616 |
MMP3 |
598 |
790 |
236 |
236 |
0.394649 |
0.298734 |
0.340058 |
1.768172 |
0.961483907 |
rs3740938 |
MMP8 |
598 |
790 |
135 |
135 |
0.225753 |
0.170886 |
0.194524 |
0.590001 |
0.722404948 |
rs2012390 |
MMP8 |
596 |
792 |
153 |
153 |
0.256711 |
0.193182 |
0.220461 |
0.85629 |
0.804081313 |
rs1940475 |
MMP8 |
598 |
792 |
217 |
217 |
0.362876 |
0.27399 |
0.31223 |
1.571273 |
0.941940363 |
rs11225394 |
MMP8 |
598 |
772 |
65 |
65 |
0.108696 |
0.084197 |
0.094891 |
-0.41971 |
0.337347429 |
rs11225395 |
MMP8 |
598 |
792 |
210 |
210 |
0.351171 |
0.265152 |
0.302158 |
1.488018 |
0.931626918 |
DISCUSSION
Excessive and chronic alcohol consumption are the most important causes of alcohol-induced ONFH. The association between several polymorphisms and alcohol-induced ONFH has been reported [4, 11, 13, 18]]. However, each polymorphism only contributes to a small relative risk of alcohol-induced ONFH, and more comprehensive genetic polymorphisms are needed to enrich the genetic information on this disease. Our study is the first to investigate the association between the MMP-3 and MMP-8 polymorphisms and alcohol-induced ONFH. We researched 13 SNPs on MMP-3 and MMP-8, and found two protective SNPs, rs650108 (10556C>T) on MMP-3 and rs2012390 (9909C>T), on MMP-8 and one high-risk SNP, rs11225394 (5273G>A), on MMP-8 associated with alcohol-induced ONFH risk.
The destruction and repair of bone tissue depend on bone resorption and bone formation. They are the basis of bone metabolism. MMPs are a group of endopeptidases that contain zinc finger motifs, which have the function of degrading all the components of extracellular matrix. A study by Grässel et al [19] reported that the expression and activity of MMP-2 and MMP-9 increase the impaired bone matrix repair capacity, restoring the balance between bone resorption and de novo bone formation in ONFH. So MMP-3 and MMP-8, might be like MMP-2 and MMP-9 and are associated with ONFH.
MMP-3 and MMP-8 localize to chromosome 11q22.3. MMP-3 encodes an enzyme that degrades fibronectin, laminin, collagens III, IV, IX, and X, and cartilage proteoglycans. The expression of MMP-3 involves in the degradation of bone matrix in bone resorption [14]. A previous study demonstrated that 6A/6A polymorphism of MMP-3 is associated with the degradation of collagen, resulting in extracellular matrix degradation, ultimately leading to cartilage and bone loss [20], and this pathway is one of the major pathological mechanismsmechanism in ONFH. Our research found that rs650108 (10556C>T) of MMP-3 decreases the risk of alcohol-induced ONFH. We speculated that the polymorphism of MMP-3 might be involvedinvolve in the prevention pathway of extracellular matrix degradation and decreasing cartilage and bone loss in ONFH. MMP-8 encodes interstitial collagenases that promote bone tissue degradation. The expression of MMP-8 involves in the breakdown of extracellular matrix in bony tissue development, reproduction, and tissue remodeling, including disease processes such as arthritis and metastasis [15]. Our research found that rs2012390 (9909C>T) on MMP-8 decreases ONFH risk and rs11225394 (5273G>A) on MMP-8 increases ONFH risk. The polymorphisms of MMP-8 might influence the breakdown pathway of the extracellular matrix in bony tissue development, reproduction, and tissue remodeling, and is a risk or preventionprevent factor in ONFH. Previous studies have determined that MMP-3 and MMP-8 are key factors in the pathological process of orthopedic diseases [16, 21, 22]. For example, MMP-1 and MMP-3 encode the key enzyme for bone surface collagen formation. The expression of MMP-1 and MMP-3 promote bone resorption to accelerate sclerotin repair [23]. In osteoarthritis patients, MMP-3 promotes the degradation of bone matrix and stimulates bone tissue repair [16]. We speculated that the SNPs rs650108 (10556C>T) on MMP-3 and rs2012390 (9909C>T) on MMP-8 might decrease alcohol-induced ONFH risk by regulating the breakdown of the extracellular matrix (ECM) and finally result in regulating bone tissue repair.; We also found rs11225394 (5273G>A) on MMP-8increases alcohol-induced ONFH risk. Thethe role of MMP-3 is supposedly related to the breakdown of the ECM, resulting in the loss of tissue integrity [24].Additionally, MMP-3 is a factor in the formation of bone tissue and in the formation of osteoclasts, osteoblasts, osteoid and pro-osteoclasts [25]. Osteoclasts are differentiated from pro-osteoclasts, and the dynamic equilibrium of the osteoblast/osteoclast ratio is the major part of the maintenance of bone resorption, bony remodeling, and bone metabolism. We found that the genetic polymorphisms of MMP-3, rs650108 (10556C>T), decrease ONFH risk.We speculated that thethe polymorphism of MMP-3 might on the one hand regulate the breakdown of the ECM and on the other hand influence the formation of osteoblasts and osteoclasts and influence bone metabolism, resulting in decreased alcohol-induced ONFH risk. MMP-8 is mainly produced by neutrophils and is also expressed by extensive cells, including chondrocytes [26] and synovial fibroblasts [27]. MMP-8 is a key factor in the pathogenesis of several inflammatory conditions because is encodes a potent collagenolytic enzyme [28]. The action of MMP-8 in the inflammatory process depends on the stimulus in different situations, and MMP-8 might have a promoting or protective function in arthritis pathogenesis [29, 30]. A previous investigation indicated that the polymorphism of MMP-8 influencesinfluence the development of the inflammatory reaction itself [31]. A lack of MMP-8 causes the aggravation of arthritis through promotion of inflammation by IL-1β and PTX3, inducing the maturation and activation of osteoclasts or enhancement of the inflammatory infiltrate by PROKR2 and IL-1β [32]. So, we speculated that the polymorphisms of MMP-8 mightmight influence the development of the inflammatory reaction process in the femoral head, and might be involvedand involve in the regulation of the inflammatory response in the bone joint tissue, resulting in an influence on the risk of alcohol-induced ONFH. Additionally, rs650108 (10556C>T) is a sensitive SNP in MMP-3 that has been found to have an association with the risk of primary sclerosing cholangitis [33], breast cancer [34], and rotator cuff repair [35]. The mutation of rs650108 in these diseases are a key factor in inflammatory or fibrogenic response, and the pathogenic development of alcohol-induced ONFH is closely tied to the fibrogenic response of bone resorption and remodeling of bone tissue. Thus, we speculated that the mutation of rs650108 on MMP-3 may influence the process of bone resorption and remodeling that is associated with the fibrogenic response in alcohol-induced ONFH. MoreoverMoreover, we found the expression of a different genotype in a different SNP on the same gene might have a different influence in the same disease.
Furthermore, our study is the first to explore the association between alcohol-induced ONFH and MMP-3 and MMP-8 polymorphism. Further explorations with larger samples and individuals from different areas are needed to confirm our conclusion.
MATERIALS AND METHODS
Ethics committee statement
Our present study strictly observed the principles of the Declaration on Helsinki of the World Medical Association and was approved by the Ethics Committee of Zhengzhou Traditional Chinese Medicine Traumatology Hospital. Informed consent forms were signed by all the individuals and they were all notified for our case-control study.
Research subjects
Our case-control study consecutively recruited a total of 695 male individuals (299 alcohol-induced ONFH patients and 396 healthy control subjects) from September 2014 to January 2016 in Zhengzhou Traditional Chinese Medicine Traumatology Hospital. All the participants were selected randomly without age restriction and were genetically unrelated ethnic Han Chinese males.
Medical diagnostic criteria of alcohol-induced ONFH is based on clinical manifestations such as pain and activity limitation of hip and sick-side lower limb muscle atrophy. Further diagnosis depends on magnetic resonance imaging (MRI) analysis and examination of changes on X-ray, such as high density shadows of the femoral head, hip joint narrowness and bumpiness, or joint surface rupture. All the selected patients were given thorough physical examinations.
When we selected the participants for the case group, the exclusion criteria were refusal to participate in this study, liver disease or dyslipidemia caused by drugs, not satisfying alcohol-induced ONFH medical diagnostic criteria or the presence of traumatic osteonecrosis or other hip diseases, requirement of steroids for replacement therapy in serious primary disease, and overuse of steroids or a chronic metabolic disorder of the heart, kidney, or liver.
When we selected the control group, all the individuals were healthy. We collected the epidemiological information by using a standardized questionnaire and collected clinical information from medical records and pathological reports.
SNP sites selection
A total of 13 single nucleotide polymorphisms (SNPs), including eight SNPs on the gene MMP-3 and five on the gene MMP-8, were selected for our study. Most of the 13 SNPs had not been reported in the past. However, several SNPs were related to some other disease, such as frozen shoulder [36], breast cancer [34], carpal tunnel syndrome [37], rheumatoid arthritis (RA) [38], or osteoarthritis (OA) [39]. The selection of SNPs depended on their location, allele frequencies, and disease relevance determined by use of the Hapmap public databases (dbSNP; http://www.ncbi.nlm.nih.gov/SNP/, HAPMAP; http://www.Hapmap.org/index.html.en). The minor allele frequency (MAF) is higher than 5% in the HapMap Chinese Han Beijing (CHB) population.
Genotyping
We extracted genomic DNA from whole blood samples by using a purification kit (GoldMag, China), and then stored the extract at a temperature of −20° C. We measured the DNA concentration by spectrometry (DU530 UV/VIS spectrophotometer, Beckman Instruments, Fullerton, CA, USA). Per the manufacturer’s instructions, we performed the genotyping by using the Sequenom MassARRAY® RS1000 system. The amplification and extension of primers were completed by application of Sequenom MassARRAY® Assay Design 3.0 software [40]. We also utilized Sequenom Typer 4.0 software to analyze and manage our data [40, 41].
Statistical analysis
We utilized SPSS17.0 statistical software (SPSS, Chicago, IL) and Microsoft Excel to calculate the statistical analyses of our study. P ≤ 0.05 indicates statistical significance and all the P-values are two-sided. The SNP genotype frequencies in our case and control groups were performed by χ2 tests. We used the Hardy-Weinberg equilibrium (HWE) to check the genotype frequency of the individuals in the control group. To make sure the results of our study are credible and to assess the relation between SNPs and alcohol-induced ONFH risk, unconditional logistic regression analysis with adjustment for age was used to examined constructed 95% confidence intervals (95% CIs) and odds ratios (ORs) [42], and the adjustment for age was done for the dominant, recessive, codominant and log-additive models. In addition, we used Haploview 4.2 to test the linkage disequilibrium structure.
Limitations
Our study had some limitations. First, patients were only enrolled in one hospital, which may increase the false-positive rate by avoiding the selection bias. This bias was not meaningful because the genetic frequencies and the difference in the distribution of demographic segmentation had been dissolved into nothingness. Second, because the number of alcohol-induced ONFH patients was not large, the sample size of our case-control study was not large. If we increase the sample size, some negative results might change to positive results that could make our conclusion more powerful and meaningful. The population was not stratified by the amount of alcohol consumption, and we did not confirm that this locus was significant for drinkers. Third, we did not evaluate the heterogeneity of alcohol consumption and the comorbidities, but in a previous study, evaluation of heterogeneity in drinking behaviors contributed to progress in elucidating the pathogenesis of alcohol-induced ONFH [43].
CONCLUSION
We investigated 13 SNPs to explore the relation of polymorphisms of the genes MMP-3 and MMP-8 to alcohol-induced ONFH risk in Chinese males. We found that genetic polymorphisms of rs650108 (10556C>T) in MMP-3 and rs2012390 (9909C>T) in MMP-8 decreased alcohol-induced ONFH, and rs11225394 (5273G>A) on MMP-8 with polymorphism significantly increased the risk of alcohol-induced ONFH. The mutation of the three SNPs might promote the degradation of bone matrix and influence the breakdown of extracellular matrix, the formation of osteoclasts and osteoblasts, or the activation of the inflammatory response to regulate the osteoblast/osteoclast ratio, bony tissue development, reproduction, and tissue remodeling, and then lead to the repair of bone tissue in the femoral head, and that associated with alcohol-induced ONFH risk.
ACKNOWLEDGMENTS
This study was supported by the National Natural Science Foundation of China (Grant No.81160228, No.81260284 and NO.81660378). We are grateful to all the participants in our study, this study could not succeed without them. We would also like to thank the clinicians and hospital staff who contributed to the data collection for this study.
CONFLICTs OF INTEREST
The authors have no conflicts of interest to report.
Author contributions
Jianzhong Wang, Guoqiang Wang and Tianbo Jin conceived and designed this experiment. Junyu Chen completed the experiments and wrote of the manuscript. Xiyang Zhang and Wanlin Liu proofread the manuscript. Yongchang Guo analyzed the data. Jieli Du, Yong Zhu, Yuju Cao and Jian Li gathered the samples. The final manuscript was read and approved by all authors.
REFERENCES
1. Pavelka K. Osteonecrosis. Bailliere's best practice & research Clinical rheumatology. 2000; 14:399-414.
2. Mont MA, Marulanda GA, Jones LC, Saleh KJ, Gordon N, Hungerford DS and Steinberg ME. Systematic analysis of classification systems for osteonecrosis of the femoral head. The Journal of bone and joint surgery American volume. 2006; 88 Suppl 3:16-26.
3. Mont MA, Jones LC and Hungerford DS. Nontraumatic osteonecrosis of the femoral head: ten years later. The Journal of bone and joint surgery American volume. 2006; 88:1117-1132.
4. Yin JM, Liu Z, Zhao SC, Guo YJ and Liu ZT. Relationship between the Apolipoprotein AI, B gene polymorphism and the risk of non-traumatic osteonecrosis. Lipids in health and disease. 2014; 13:149.
5. Zaidi M, Sun L, Robinson LJ, Tourkova IL, Liu L, Wang Y, Zhu LL, Liu X, Li J, Peng Y, Yang G, Shi X, Levine A, et al. ACTH protects against glucocorticoid-induced osteonecrosis of bone. Proceedings of the National Academy of Sciences of the United States of America. 2010; 107:8782-8787.
6. Wang Y, Li Y, Mao K, Li J, Cui Q and Wang GJ. Alcohol-induced adipogenesis in bone and marrow: a possible mechanism for osteonecrosis. Clinical orthopaedics and related research. 2003; :213-224.
7. Chang JD, Hur M, Lee SS, Yoo JH and Lee KM. Genetic background of nontraumatic osteonecrosis of the femoral head in the Korean population. Clinical orthopaedics and related research. 2008; 466:1041-1046.
8. Zhou X, Yishake M, Li J, Jiang L, Wu L, Liu R and Xu N. Genetic susceptibility to prosthetic joint infection following total joint arthroplasty: A systematic review. Gene. 2015; 563:76-82.
9. Omar HS, Shaker OG, Nassar YH, Marzouk SA and ElMarzouky MS. The association between RANKL and Osteoprotegerin gene polymorphisms with breast cancer. Molecular and cellular biochemistry. 2015; 403:219-229.
10. Hadjigeorgiou G, Dardiotis E, Dardioti M, Karantanas A, Dimitroulias A and Malizos K. Genetic association studies in osteonecrosis of the femoral head: mini review of the literature. Skeletal radiology. 2008; 37:1-7.
11. Okazaki S, Nishitani Y, Nagoya S, Kaya M, Yamashita T and Matsumoto H. Femoral head osteonecrosis can be caused by disruption of the systemic immune response via the toll-like receptor 4 signalling pathway. Rheumatology. 2009; 48:227-232.
12. Lee HJ, Choi SJ, Hong JM, Lee WK, Baek JI, Kim SY, Park EK, Kim SY, Kim TH and Kim UK. Association of a polymorphism in the intron 7 of the SREBF1 gene with osteonecrosis of the femoral head in Koreans. Annals of human genetics. 2009; 73:34-41.
13. Wang Y, Cao Y, Li Y, Guo Y, Wang Q, Yang M, Zhang N, Jin T and Wang J. Genetic association of the ApoB and ApoA1 gene polymorphisms with the risk for alcohol-induced osteonecrosis of femoral head. International journal of clinical and experimental pathology. 2015; 8:11332-11339.
14. Feng Z, He G, Chen Z, Wu Z and Li J. Lack of association of matrix metalloproteinase-3 gene polymorphism with susceptibility to rheumatoid arthritis: a meta-analysis. BMC musculoskeletal disorders. 2014; 15:376.
15. Sathyamoorthy T, Sandhu G, Tezera LB, Thomas R, Singhania A, Woelk CH, Dimitrov BD, Agranoff D, Evans CA, Friedland JS and Elkington PT. Gender-dependent differences in plasma matrix metalloproteinase-8 elevated in pulmonary tuberculosis. PloS one. 2015; 10:e0117605.
16. Ho LJ, Lin LC, Hung LF, Wang SJ, Lee CH, Chang DM, Lai JH and Tai TY. Retinoic acid blocks pro-inflammatory cytokine-induced matrix metalloproteinase production by down-regulating JNK-AP-1 signaling in human chondrocytes. Biochemical pharmacology. 2005; 70:200-208.
17. Geoffroy V, Marty-Morieux C, Le Goupil N, Clement-Lacroix P, Terraz C, Frain M, Roux S, Rossert J and de Vernejoul MC. In vivo inhibition of osteoblastic metalloproteinases leads to increased trabecular bone mass. Journal of bone and mineral research. 2004; 19:811-822.
18. Kim TH, Baek JI, Hong JM, Choi SJ, Lee HJ, Cho HJ, Park EK, Kim UK and Kim SY. Significant association of SREBP-2 genetic polymorphisms with avascular necrosis in the Korean population. BMC medical genetics. 2008; 9:94.
19. Grassel S, Beckmann J, Rath B, Vogel M, Grifka J and Tingart M. Expression profile of matrix metalloproteinase-2 and -9 and their endogenous tissue inhibitors in osteonecrotic femoral heads. International journal of molecular medicine. 2010; 26:127-133.
20. Williams RO, Feldmann M and Maini RN. Cartilage destruction and bone erosion in arthritis: the role of tumour necrosis factor alpha. Annals of the rheumatic diseases. 2000; 59 Suppl 1:i75-80.
21. Rubin C, Sun YQ, Hadjiargyrou M and McLeod K. Increased expression of matrix metalloproteinase-1 in osteocytes precedes bone resorption as stimulated by disuse: evidence for autoregulation of the cell's mechanical environment? Journal of orthopaedic research. 1999; 17:354-361.
22. Ben David D, Reznick AZ, Srouji S and Livne E. Exposure to pro-inflammatory cytokines upregulates MMP-9 synthesis by mesenchymal stem cells-derived osteoprogenitors. Histochemistry and cell biology. 2008; 129:589-597.
23. Karsdal MA, Andersen TA, Bonewald L and Christiansen C. Matrix metalloproteinases (MMPs) safeguard osteoblasts from apoptosis during transdifferentiation into osteocytes: MT1-MMP maintains osteocyte viability. DNA and cell biology. 2004; 23:155-165.
24. Wielockx B, Lannoy K, Shapiro SD, Itoh T, Itohara S, Vandekerckhove J and Libert C. Inhibition of matrix metalloproteinases blocks lethal hepatitis and apoptosis induced by tumor necrosis factor and allows safe antitumor therapy. Nature medicine. 2001; 7:1202-1208.
25. Adiguzel M, Horozoglu C, Kilicoglu O, Ozger H, Acar L and Ergen A. MMP-3 gene polymorphisms and Osteosarcoma. Indian journal of experimental biology. 2016; 54:175-179.
26. Cole AA, Chubinskaya S, Schumacher B, Huch K, Szabo G, Yao J, Mikecz K, Hasty KA and Kuettner KE. Chondrocyte matrix metalloproteinase-8. Human articular chondrocytes express neutrophil collagenase. The Journal of biological chemistry. 1996; 271:11023-11026.
27. Hanemaaijer R, Sorsa T, Konttinen YT, Ding Y, Sutinen M, Visser H, van Hinsbergh VW, Helaakoski T, Kainulainen T, Ronka H, Tschesche H and Salo T. Matrix metalloproteinase-8 is expressed in rheumatoid synovial fibroblasts and endothelial cells. Regulation by tumor necrosis factor-alpha and doxycycline. The Journal of biological chemistry. 1997; 272:31504-31509.
28. Van Lint P, Wielockx B, Puimege L, Noel A, Lopez-Otin C and Libert C. Resistance of collagenase-2 (matrix metalloproteinase-8)-deficient mice to TNF-induced lethal hepatitis. Journal of immunology. 2005; 175:7642-7649.
29. Itoh T, Matsuda H, Tanioka M, Kuwabara K, Itohara S and Suzuki R. The role of matrix metalloproteinase-2 and matrix metalloproteinase-9 in antibody-induced arthritis. Journal of immunology. 2002; 169:2643-2647.
30. Close DR. Matrix metalloproteinase inhibitors in rheumatic diseases. Annals of the rheumatic diseases. 2001; 60 Suppl 3:iii62-67.
31. Balbin M, Fueyo A, Tester AM, Pendas AM, Pitiot AS, Astudillo A, Overall CM, Shapiro SD and Lopez-Otin C. Loss of collagenase-2 confers increased skin tumor susceptibility to male mice. Nature genetics. 2003; 35:252-257.
32. Garcia S, Forteza J, Lopez-Otin C, Gomez-Reino JJ, Gonzalez A and Conde C. Matrix metalloproteinase-8 deficiency increases joint inflammation and bone erosion in the K/BxN serum-transfer arthritis model. Arthritis research & therapy. 2010; 12:R224.
33. Juran BD, Atkinson EJ, Schlicht EM, Larson JJ, Ellinghaus D, Franke A and Lazaridis KN. Genetic polymorphisms of matrix metalloproteinase 3 in primary sclerosing cholangitis. Liver international. 2011; 31:785-791.
34. Slattery ML, John E, Torres-Mejia G, Stern M, Lundgreen A, Hines L, Giuliano A, Baumgartner K, Herrick J and Wolff RK. Matrix metalloproteinase genes are associated with breast cancer risk and survival: the Breast Cancer Health Disparities Study. PloS one. 2013; 8:e63165.
35. Ling Y, Peng C, Liu C, Zhang N and Yue S. Gene polymorphism of IL-6 and MMP-3 decreases passive range of motion after rotator cuff repair. International journal of clinical and experimental pathology. 2015; 8:5709-5714.
36. Xu Q, Gai PY, Lv HL, Li GR and Liu XY. Association of MMP3 genotype with susceptibility to frozen shoulder: a case-control study in a Chinese Han population. Genetics and molecular research. 2016; 15(1).
37. Burger MC, De Wet H and Collins M. Matrix metalloproteinase genes on chromosome 11q22 and risk of carpal tunnel syndrome. Rheumatology international. 2016; 36:413-419.
38. Ma MJ, Liu HC, Qu XQ and Wang JL. Matrix metalloproteinase-3 gene polymorphism and its mRNA expression in rheumatoid arthritis. Genetics and molecular research. 2015; 14:15652-15659.
39. Shi J, Zhang C, Yi Z and Lan C. Explore the variation of MMP3, JNK, p38 MAPKs, and autophagy at the early stage of osteoarthritis. IUBMB life. 2016; 68:293-302.
40. Gabriel S, Ziaugra L and Tabbaa D. SNP genotyping using the Sequenom MassARRAY iPLEX platform. Current protocols in human genetics / editorial board, Jonathan L Haines [et al]. 2009; Chapter 2:Unit 2 12.
41. Thomas RK, Baker AC, Debiasi RM, Winckler W, Laframboise T, Lin WM, Wang M, Feng W, Zander T, MacConaill L, Lee JC, Nicoletti R, Hatton C, et al. High-throughput oncogene mutation profiling in human cancer. Nature genetics. 2007; 39:347-351.
42. Bland JM and Altman DG. Statistics notes. The odds ratio. Bmj. 2000; 320:1468.
43. Okazaki S, Nagoya S, Tateda K, Katada R, Mizuo K, Watanabe S, Yamashita T and Matsumoto H. Experimental rat model for alcohol-induced osteonecrosis of the femoral head. International journal of experimental pathology. 2013; 94:312-319.