
Introduction
Glioblastomas are the most common brain malignancies, accounting for 15.1% of the total central nervous system tumors [1]. Glioblastomas are classified as either primary glioblastomas (pGBMs) or secondary glioblastomas (sGBMs), which develop from lower-grade gliomas [2]. The discovery that isocitrate dehydrogenase (IDH) mutations are more common in sGBMs was one of the most significant advancements in the understanding of gliomas [3, 4]. Patients with glioblastomas carrying IDH mutations or wildtype IDH, exhibited large differences in prognosis, age, and genetic alternations [5-9].
Mounting evidence suggests an important role for inflammation in tumor development [10, 11]. The development of gliomas, in particular, is closely associated with inflammation status and immune response [12, 13]. NLRs, PLRs, and LMRs are markers of host inflammation. A high NLR and PLR and low LMR are closely associated with a poor prognosis in solid malignancies, including gastrointestinal tumors, prostate cancer, and lung cancer [14-19]. While a low preoperative NLR closely correlates with lower glioma grade and better clinical outcome [20-22], there are no published data assessing the role of PLR or LMR in gliomas. Additionally, the role of the NLR in gliomas requires further study, due to the limited number of cases in previous studies [21, 22]. We therefore hypothesized that the inflammation status would likely vary according to the IDH mutation status, and could serve as a prognostic indicator. Herein, we investigated the prognostic value of NLRs, PLRs, and LMRs, in both pGBMs and sGBMs. The characteristics of NLRs, PLRs, and LMRs are also described here, taking into consideration IDH mutation status.
Results
Patient characteristics
We enrolled 166 patients with GBMs in the present study, including 70 females and 96 males. The age of the patients ranged from 18 to 80 years with an average of 52.1 ± 0.984 years. The frequency of IDH mutations was 9.9% (14/141) among pGBMs and 68% (17/25) among sGBM. The Karnofsky score (KPS), tumor location, surgical resection, and molecular markers are described in Table 1.
The median overall survival (OS) did not differ with respect to gender, tumor location, or tumor size (Table 1). Patients carrying IDH-1R132H mutations had better prognoses [median 17.17 months (95% CI 8.84 – 25.50) vs. 12.00 months (95% CI 9.34 – 14.66); p = 0.041]. Higher preoperative KPS, surgical resection, and full treatment with radiochemotherapy were also associated with better clinical outcomes (Table 1). Among patients meeting our inclusion criteria, these clinical characteristics varied within a reasonable range in previous reports [1, 2, 5, 8].
Table 1: Characteristics of the study population
Variables |
No. |
mOS (95% CI) months |
HR (95% CI) |
P |
Age |
||||
< 60 |
110 |
14.70 (11.83-17.58) |
1.48 (1.04-2.12) |
0.032 |
≥60 |
56 |
9.63 (7.96-11.30) |
||
Gender |
||||
female |
70 |
12.27 (7.30-17.24) |
1.16 (0.81-1.65) |
0.419 |
male |
96 |
12.80 (10.65-14.95) |
||
Preoperative KPS |
||||
≤70 |
82 |
10.67 (7.94-13.40) |
1.48 (1.04-2.09) |
0.028 |
>70 |
84 |
16.17 (12.81-19.53) |
||
Pathology |
||||
pGBM |
141 |
13.00 (10.42-15.58) |
1.37 (0.88-2.12) |
0.164 |
sGBM |
25 |
10.67 (5.82-15.52) |
||
Location |
||||
Frontal |
33 |
11.97 (8.86-15.08) |
1.04 (0.93-1.15) |
0.504 |
Temporal |
27 |
17.00 (10.14-23.87) |
||
Parietal |
12 |
10.96 (4.80-17.12) |
||
Other site |
19 |
8.37 (3.02-13.72) |
||
Mixed |
75 |
13.33 (9.45-17.21) |
||
Size |
||||
≤ 5 cm |
68 |
13.33 (7.86-18.80) |
0.95 (0.67-1.35) |
0.760 |
> 5 cm |
98 |
12.27 (10.34-14.20) |
||
Resection |
||||
GTR |
102 |
13.33 (10.50-16.26) |
1.47 (1.03-2.09) |
0.033 |
non-GTR |
64 |
9.40 (5.93-12.87) |
||
Standard treatment |
||||
yes |
114 |
14.87 (12.08-17.66) |
2.42 (1.67-3.50) |
0.000 |
no |
52 |
7.9 (4.44-11.36) |
||
IDH-1R132H |
||||
mutant |
31 |
17.17 (8.84-25.50) |
1.60 (1.01-2.52) |
0.043 |
wild-type |
135 |
12.00 (9.34-14.66) |
No association between NLR, PLR, or LMR and IDH mutations
We observed that NLR was elevated more frequently in pGBMs than sGBMs (p = 0.015). However, PLR did not differ between pGBMs and sGBMs (p=0.765), nor did LMR (p = 0.741, Table 2). No difference was found in NLR (p = 0.574), PLR (p = 0.966) or LMR (p = 0.564) with respect to IDH mutation status. We found no significant correlation between NLR or PLR and patients’ age, gender, KPS, tumor location or size, or molecular markers. (Data not shown)
Table 2: Correlation of inflammation markers with molecular markers
Inflammation marker |
Stratification |
Histopathology |
P |
IDH-1R132H |
P |
||
pGBM |
sGBM |
mutant |
wild-type |
||||
NLR |
≤ 4.0 |
114 |
25 |
0.015 |
27 |
112 |
0.574 |
> 4.0 |
27 |
0 |
4 |
23 |
|||
PLR |
≤ 175.0 |
109 |
20 |
0.765 |
24 |
105 |
0.966 |
> 175.0 |
32 |
5 |
7 |
30 |
|||
LMR |
≤ 3.7 |
46 |
9 |
0.741 |
12 |
43 |
0.464 |
> 3.7 |
95 |
16 |
19 |
92 |
|||
Analysis of NLR, PLR, and LMR in predicting outcomes
We found that NLR had no significant prognostic value for patients with glioblastomas [12.80 months (95% CI 10.40–15.20) vs. 6.03 months (95% CI 1.16–10.90); p=0.172, Figure 1a] and those in the pGBM group [13.30 months (95% CI 1.91–15.69) vs. 6.03 months (95% CI 1.16–10.90); p=0.104, Figure 1b]. However, patients who had a NLR ≤ 4.0 and were in the group carrying IDH-1R132H-wt had better prognoses [12.60 months (95% CI 10.22–14.98) vs. 5.50 months (95% CI 3.40–7.60); p=0.004, Figure 1c].
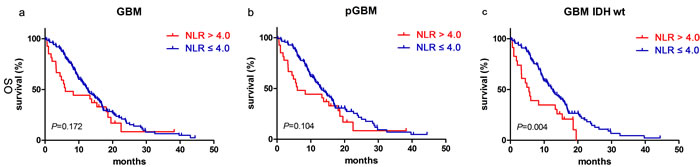
Figure 1: NLR predicted OS in glioblastomas. Kaplan-Meier method with log rank test for NLR in predicting OS for a. glioblastomas, b. pGBM and c. IDH wt GBM.
The median OS of 13.33 months (95% CI 11.25–15.41) for patients with PLR ≤ 175.0 was longer than the 7.00 months (95% CI 4.22–9.78) for patients with PLR > 175.0 (p=0.006, Figure 2a). PLR ≤ 175.0 was also associated with better clinical outcome in the pGBM group [14.27 months (95% CI 11.83–16.71) vs. 6.80 months (95% CI 3.57–10.03); p=0.014, Figure 2b] and the IDH-1R132H-wt group [13.00 months (95% CI 10.84–15.16) vs. 6.03 months (95% CI 3.38–7.68); p=0.002, Figure 2c].
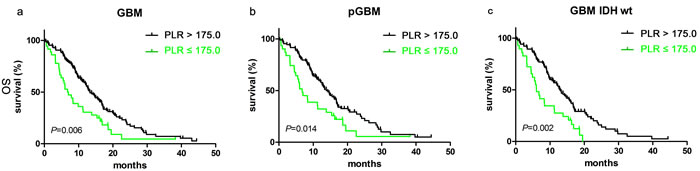
Figure 2: PLR predicted OS in glioblastomas. Kaplan-Meier method with log rank test for PLR in predicting OS for a. glioblastomas, b. pGBM and c. IDH wt GBM.
The median OS did not differ significantly between groups stratified based on LMR ≥ 3.7 [12.00 months (95% CI 9.94–14.06) vs. 12.60 months (95% CI 9.19–16.00); p=0.242, Figure 3a]. No significant prognostic value for LMR ≥ 3.7 was observed in patients with pGBM [13.83 months (95% CI 10.74–16.92) vs. 12.60 months (95% CI 8.82–16.39); p=0.567, Figure 3b], nor with IDH-1R132H-wt [12.00 months (95% CI 9.56–14.44) vs. 12.27 months (95% CI 9.07–15.47); p=0.181, Figure 3c].
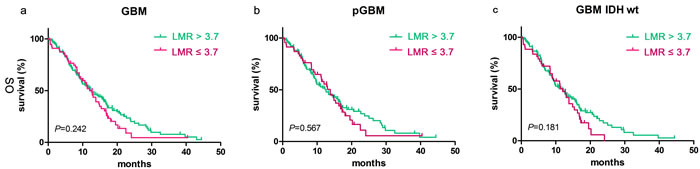
Figure 3: LMR didn’t predict OS in glioblastomas. Kaplan-Meier method with log rank test for LMR in predicting OS for a. glioblastomas, b. pGBM and c. IDH wt GBM.
Multivariate analysis indicated that age (p=0.022), extent of resection (p=0.034), full treatment (p=0.000) and IDH mutations (p=0.029) were independent prognostic factors after taking age, gender, KPS, extent of resection, full treatment, pathology and IDH mutations into account (Table 3). However, NLR, PLR, and LMR were strongly correlated with each other [(Spearman's rho coefficients of 0.631 (NLR vs PLR, p=0.000), -0.344 (NLR vs LMR, p=0.000) and -0.240 (PLR vs LMR, p=0.002)]. All three factors were analyzed in the multivariate analysis adjusted by the above 7 factors. Both NLR (HR=1.714, 95% CI 1.026-2.864, p=0.039) and PLR (HR=2.068, 95% CI 1.296-3.300, p=0.002) were indicated to be independent prognostic factors. However, we found that LMR had no independent prognostic value for OS (HR=0.733, 95% CI 0.481-1.119, p=0.150).
Table 3: Multivariate analysis of prognostic factors
Prognostic factors |
HR |
95% CI |
P value |
|
age |
1.636 |
1.073 |
2.495 |
0.022 |
gender |
0.988 |
0.664 |
1.471 |
0.953 |
Preoperative KPS |
1.250 |
0.837 |
1.866 |
0.276 |
Pathology |
1.362 |
0.687 |
2.701 |
0.376 |
Resection |
1.531 |
1.033 |
2.268 |
0.034 |
Standard treatment |
2.445 |
1.573 |
3.802 |
0.000 |
IDH-1R132H mutation |
1.993 |
1.074 |
3.698 |
0.029 |
Discussion
In the present study, we first assessed the prognostic value of NLR, PLR, and LMR in glioblastomas, taking into account IDH mutation status. NLR and PLR were independent prognostic biomarkers for patient outcomes and therefore confirm published data from glioblastomas [21-23] and other malignancies [14, 17, 24]. However, LMR was not predictive of OS in glioblastomas.
We found that reduced NLR was associated with improved OS in pGBM, though the significance was not as obvious as in previous studies [21-23]. This difference may be explained by differences among previous studies. While NLR was established as a prognostic marker for malignancies in some studies [14, 17], others failed to observe a significant prognostic value for NLR in breast cancer [25], gastric cancer [26], and prostate cancer [27]. It is likely that not all patients received the same treatment in each study. In our study, all patients underwent surgery. Among them, 61.44% (102/166) had a gross treatment resection, and 68.67% (114/166) received radiochemotherapy according to Stupp’s protocol. In other studies, the proportion of patients choosing each treatment strategy, which included biopsy, surgery, and radiochemotherapy, varied [21-23]. Additionally, the inclusion of IDH mutations was superior to histopathology alone for classifying glioblastomas [28]. We concluded that IDH-wt glioblastomas had better defined clinical outcomes than pGBM. Our multifactorial analysis first took IDH mutations as prognostic indicators, and NLR remained an independent prognostic biomarker. Interestingly, we observed that higher NLRs were more frequent in pGBM than sGBM. Zadora et al. reported that NLR values differed among glioma grades and were highest in glioblastomas [20]. Secondary glioblastoma originates from a lower-grade glioma. This likely explains why NLRs were low in sGBM. Furthermore, we also found that elevated PLR correlated closely with poor prognosis in our study, which is consistent with Han’s results [23]. The prognostic value of PLR was found not only in IDH-wt glioblastomas, but also in glioblastomas and pGBMs in our study.
The mechanism underlying the prognostic role of NLR/PLR remains unclear in glioblastomas. The blood-brain-barrier is frequently disrupted in glioblastomas, allowing circulating lymphocytes to cross [29]. Moreover, NLR was significantly related to high neutrophil and low CD3+ T-cell infiltration into glioblastomas [23]. Tumor-infiltrating lymphocytes (TILs), which are predominately regulatory T cells in the glioblastoma microenvironment, could suppress immune responses [30]. However, recent studies indicate that TILs are not sufficient to mediate the glioblastoma-related immune suppression [31-33]. PD-L1 (programmed death ligand 1) and CTLA-4 (Cytotoxic T-lymphocyte-associated protein 4) have been identified as alternatives for immunosuppression in glioblastomas [34, 35]. Additionally, PD-L1 proteins were detected in the microenvironment of glioblastomas or brain metastases [36-38]. These results suggest a more complicated immunosuppressive mechanism in glioblastomas, which is likely to involve both systemic and local microenvironmental inflammation. We therefore propose that a complete score system is needed to fully assess systemic inflammation status, involving an immunosuppressive biomarker in the microenvironment.
MATERIALS AND METHODS
Study population
This retrospective study was conducted to investigate the relationship between NLR/PLR and glioblastomas. The inclusion criteria were: (1) Surgical treatment in Sanbo Brain Hospital from 2009 to 2014, (2) the presence of histologically confirmed supratentorial glioblastomas, (3) operative blood test performed prior to corticosteroid treatment or no chemotherapy within the previous month, (4) available medical records indicating the patient’s age, gender, molecular pathology and follow-up data, and (5) provided informed consent before the investigation. Ultimately participating in the study were 166 patients, including 141 with pGBMs and 25 with sGBMs. The Stupp protocol was used for concurrent chemoradiotherapy followed by consolidation chemotherapy with temozolomide [39]. OS time was defined as the interval from surgery until death or the latest follow-up. All experiments using human tissues were approved by the Institutional Review Board of Sanbo Brain Hospital.
Immunohistochemistry
Immunohistochemistry was used for detection of IDH mutations. The procedures were performed as described previously [9] using primary antibodies against IDH1R132H (Dianova 1:100) . The cutoff values were 10% for IDH-1R132H mut.
Statistics
Data are presented as means ± SEM. SPSS 22.0 was used for all the other statistical analyses. The χ2 test was used to evaluate the correlations between NLR, PLR and LMR and the patients’ clinical characteristics. Survival curves were analyzed using the Kaplan-Meier method and the Breslow test. Values of p<0.05 (two-sided) were considered statistically significant.
ACKNOWLEDGMENTS
This work was supported by grants from National Key Technology Research and Development Program of the Ministry of Science and Technology of China (No.2014BAI04B01) and the National Youth Science Fund from China (No.81302200).
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
References
1. Ostrom QT, Gittleman H, Fulop J, Liu M, Blanda R, Kromer C, Wolinsky Y, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008-2012. Neuro Oncol. 2015; 17 Suppl 4: iv1-iv62. doi: 10.1093/neuonc/nov189.
2. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauer BW, Kleihues P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007; 114: 97-109. doi: 10.1007/s00401-007-0243-4.
3. Parsons DW, Jones S, Zhang X, Lin JC, Leary RJ, Angenendt P, Mankoo P, Carter H, Siu IM, Gallia GL, Olivi A, McLendon R, Rasheed BA, et al. An integrated genomic analysis of human glioblastoma multiforme. Science. 2008; 321: 1807-12. doi: 10.1126/science.1164382.
4. Yan H, Parsons DW, Jin G, McLendon R, Rasheed BA, Yuan W, Kos I, Batinic-Haberle I, Jones S, Riggins GJ, Friedman H, Friedman A, Reardon D, et al. IDH1 and IDH2 mutations in gliomas. N Engl J Med. 2009; 360: 765-73. doi: 10.1056/NEJMoa0808710.
5. Reuss DE, Mamatjan Y, Schrimpf D, Capper D, Hovestadt V, Kratz A, Sahm F, Koelsche C, Korshunov A, Olar A, Hartmann C, Reijneveld JC, Wesseling P, et al. IDH mutant diffuse and anaplastic astrocytomas have similar age at presentation and little difference in survival: a grading problem for WHO. Acta Neuropathol. 2015; 129: 867-73. doi: 10.1007/s00401-015-1438-8.
6. Reuss DE, Kratz A, Sahm F, Capper D, Schrimpf D, Koelsche C, Hovestadt V, Bewerunge-Hudler M, Jones DT, Schittenhelm J, Mittelbronn M, Rushing E, Simon M, et al. Adult IDH wild type astrocytomas biologically and clinically resolve into other tumor entities. Acta Neuropathol. 2015; 130: 407-17. doi: 10.1007/s00401-015-1454-8.
7. Yang P, Zhang W, Wang Y, Peng X, Chen B, Qiu X, Li G, Li S, Wu C, Yao K, Li W, Yan W, Li J, et al. IDH mutation and MGMT promoter methylation in glioblastoma: Results of a prospective registry. Oncotarget. 2015; 6:40896-906. doi: 10.18632/oncotarget.5683.
8. Ohgaki H, Kleihues P. The definition of primary and secondary glioblastoma. Clin Cancer Res. 2013; 19: 764-72. doi: 10.1158/1078-0432.CCR-12-3002.
9. Wang PF, Liu N, Song HW, Yao K, Jiang T, Li SW, Yan CX. IDH-1R132H mutation status in diffuse glioma patients: implications for classification. Oncotarget. 2016; 7:31393-400. doi: 10.18632/oncotarget.8918.
10. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010; 140: 883-99. doi: 10.1016/j.cell.2010.01.025.
11. Aggarwal BB, Vijayalekshmi RV, Sung B. Targeting inflammatory pathways for prevention and therapy of cancer: short-term friend, long-term foe. Clin Cancer Res. 2009; 15: 425-30. doi: 10.1158/1078-0432.CCR-08-0149.
12. Yeung YT, McDonald KL, Grewal T, Munoz L. Interleukins in glioblastoma pathophysiology: implications for therapy. Br J Pharmacol. 2013; 168: 591-606. doi: 10.1111/bph.12008.
13. Linos E, Raine T, Alonso A, Michaud D. Atopy and risk of brain tumors: a meta-analysis. J Natl Cancer Inst. 2007; 99: 1544-50. doi: 10.1093/jnci/djm170.
14. Templeton AJ, McNamara MG, Seruga B, Vera-Badillo FE, Aneja P, Ocana A, Leibowitz-Amit R, Sonpavde G, Knox JJ, Tran B, Tannock IF, Amir E. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014; 106: dju124. doi: 10.1093/jnci/dju124.
15. van Soest RJ, Templeton AJ, Vera-Badillo FE, Mercier F, Sonpavde G, Amir E, Tombal B, Rosenthal M, Eisenberger MA, Tannock IF, de Wit R. Neutrophil-to-lymphocyte ratio as a prognostic biomarker for men with metastatic castration-resistant prostate cancer receiving first-line chemotherapy: data from two randomized phase III trials. Ann Oncol. 2015; 26: 743-9. doi: 10.1093/annonc/mdu569.
16. You J, Zhu GQ, Xie L, Liu WY, Shi L, Wang OC, Huang ZH, Braddock M, Guo GL, Zheng MH. Preoperative platelet to lymphocyte ratio is a valuable prognostic biomarker in patients with colorectal cancer. Oncotarget. 2016; 7:25516-27. doi: 10.18632/oncotarget.8334.
17. Gu X, Gao X, Li X, Qi X, Ma M, Qin S, Yu H, Sun S, Zhou D, Wang W. Prognostic significance of neutrophil-to-lymphocyte ratio in prostate cancer: evidence from 16,266 patients. Sci Rep. 2016; 6: 22089. doi: 10.1038/srep22089.
18. Pinato DJ, Shiner RJ, Seckl MJ, Stebbing J, Sharma R, Mauri FA. Prognostic performance of inflammation-based prognostic indices in primary operable non-small cell lung cancer. Br J Cancer. 2014; 110: 1930-5. doi: 10.1038/bjc.2014.145.
19. Gu L, Ma X, Li H, Chen L, Xie Y, Zhao C, Luo G, Zhang X. Prognostic value of preoperative inflammatory response biomarkers in patients with sarcomatoid renal cell carcinoma and the establishment of a nomogram. Sci Rep. 2016; 6: 23846. doi: 10.1038/srep23846.
20. Zadora P, Dabrowski W, Czarko K, Smolen A, Kotlinska-Hasiec E, Wiorkowski K, Sikora A, Jarosz B, Kura K, Rola R, Trojanowski T. Preoperative neutrophil-lymphocyte count ratio helps predict the grade of glial tumor - a pilot study. Neurol Neurochir Pol. 2015; 49: 41-4. doi: 10.1016/j.pjnns.2014.12.006.
21. Bambury RM, Teo MY, Power DG, Yusuf A, Murray S, Battley JE, Drake C, O’Dea P, Bermingham N, Keohane C, Grossman SA, Moylan EJ, O’Reilly S. The association of pre-treatment neutrophil to lymphocyte ratio with overall survival in patients with glioblastoma multiforme. J Neurooncol. 2013; 114: 149-54. doi: 10.1007/s11060-013-1164-9.
22. Alexiou GA, Vartholomatos E, Voulgaris S. Prognostic value of neutrophil-to-lymphocyte ratio in patients with glioblastoma. J Neurooncol. 2013; 115: 521-2. doi: 10.1007/s11060-013-1240-1.
23. Han S, Liu Y, Li Q, Li Z, Hou H, Wu A. Pre-treatment neutrophil-to-lymphocyte ratio is associated with neutrophil and T-cell infiltration and predicts clinical outcome in patients with glioblastoma. BMC Cancer. 2015; 15: 617. doi: 10.1186/s12885-015-1629-7.
24. Gu X, Sun S, Gao XS, Xiong W, Qin S, Qi X, Ma M, Li X, Zhou D, Wang W, Yu H. Prognostic value of platelet to lymphocyte ratio in non-small cell lung cancer: evidence from 3,430 patients. Sci Rep. 2016; 6: 23893. doi: 10.1038/srep23893.
25. Leitch EF, Chakrabarti M, Crozier JE, McKee RF, Anderson JH, Horgan PG, McMillan DC. Comparison of the prognostic value of selected markers of the systemic inflammatory response in patients with colorectal cancer. Br J Cancer. 2007; 97: 1266-70. doi: 10.1038/sj.bjc.6604027.
26. Dutta S, Crumley AB, Fullarton GM, Horgan PG, McMillan DC. Comparison of the prognostic value of tumour and patient related factors in patients undergoing potentially curative resection of gastric cancer. Am J Surg. 2012; 204: 294-9. doi: 10.1016/j.amjsurg.2011.10.015.
27. Bahig H, Taussky D, Delouya G, Nadiri A, Gagnon-Jacques A, Bodson-Clermont P, Soulieres D. Neutrophil count is associated with survival in localized prostate cancer. BMC Cancer. 2015; 15: 594. doi: 10.1186/s12885-015-1599-9.
28. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol. 2016. doi: 10.1007/s00401-016-1545-1.
29. Muller C, Holtschmidt J, Auer M, Heitzer E, Lamszus K, Schulte A, Matschke J, Langer-Freitag S, Gasch C, Stoupiec M, Mauermann O, Peine S, Glatzel M, et al. Hematogenous dissemination of glioblastoma multiforme. Sci Transl Med. 2014; 6: 247ra101. doi: 10.1126/scitranslmed.3009095.
30. Wainwright DA, Sengupta S, Han Y, Lesniak MS. Thymus-derived rather than tumor-induced regulatory T cells predominate in brain tumors. Neuro Oncol. 2011; 13: 1308-23. doi: 10.1093/neuonc/nor134.
31. Thomas AA, Fisher JL, Rahme GJ, Hampton TH, Baron U, Olek S, Schwachula T, Rhodes CH, Gui J, Tafe LJ, Tsongalis GJ, Lefferts JA, Wishart H, et al. Regulatory T cells are not a strong predictor of survival for patients with glioblastoma. Neuro Oncol. 2015; 17: 801-9. doi: 10.1093/neuonc/nou363.
32. Han S, Zhang C, Li Q, Dong J, Liu Y, Huang Y, Jiang T, Wu A. Tumour-infiltrating CD4(+) and CD8(+) lymphocytes as predictors of clinical outcome in glioma. Br J Cancer. 2014; 110: 2560-8. doi: 10.1038/bjc.2014.162.
33. Yue Q, Zhang X, Ye HX, Wang Y, Du ZG, Yao Y, Mao Y. The prognostic value of Foxp3+ tumor-infiltrating lymphocytes in patients with glioblastoma. J Neurooncol. 2014; 116: 251-9. doi: 10.1007/s11060-013-1314-0.
34. Nduom EK, Weller M, Heimberger AB. Immunosuppressive mechanisms in glioblastoma. Neuro Oncol. 2015; 17 Suppl 7: vii9-vii14. doi: 10.1093/neuonc/nov151.
35. Wainwright DA, Chang AL, Dey M, Balyasnikova IV, Kim CK, Tobias A, Cheng Y, Kim JW, Qiao J, Zhang L, Han Y, Lesniak MS. Durable therapeutic efficacy utilizing combinatorial blockade against IDO, CTLA-4, and PD-L1 in mice with brain tumors. Clin Cancer Res. 2014; 20: 5290-301. doi: 10.1158/1078-0432.CCR-14-0514.
36. Zeng J, Zhang XK, Chen HD, Zhong ZH, Wu QL, Lin SX. Expression of programmed cell death-ligand 1 and its correlation with clinical outcomes in gliomas. Oncotarget. 2016; 7: 8944-55. doi: 10.18632/oncotarget.6884.
37. Vlahovic G, Fecci PE, Reardon D, Sampson JH. Programmed death ligand 1 (PD-L1) as an immunotherapy target in patients with glioblastoma. Neuro Oncol. 2015; 17: 1043-5. doi: 10.1093/neuonc/nov071.
38. Harter PN, Bernatz S, Scholz A, Zeiner PS, Zinke J, Kiyose M, Blasel S, Beschorner R, Senft C, Bender B, Ronellenfitsch MW, Wikman H, Glatzel M, et al. Distribution and prognostic relevance of tumor-infiltrating lymphocytes (TILs) and PD-1/PD-L1 immune checkpoints in human brain metastases. Oncotarget. 2015; 6: 40836-49. doi: 10.18632/oncotarget.5696.
39. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005; 352: 987-96. doi: 10.1056/NEJMoa043330.