
INTRODUCTION
Transarterial chemoembolization (TACE) is a well-recommended treatment for unresectable intermediate stage hepatocellular carcinoma (HCC) patients [1–3]. Unfortunately, the efficacy of conventional TACE (cTACE) in liver metastases is not satisfactory, and this might be due to the embolic material used. Lipiodol is the most common material used, and plays an important role in any cTACE procedure. It can be mixed with chemotherapeutic drugs, acting like a carrier, to enable the concentration and retention of the chemotherapeutic agent into the tumor.
HepaSphere microspheres (Merit Medical Systems, Inc., South Jordan, UT, USA) are soft, with a high conformability, and can be loaded with doxorubicin. They have been used for number of years, but have just recently been introduced in China. These small, nonabsorbable, doxorubicin-loaded microspheres can be more distally embolized, releasing the chemotherapeutic agent in a controlled and prolonged manner into the tumor, with lower systemic toxicity. Initial clinical results have been published, and show a good tumor response and safety profile [4–6]. Thus far, there have been no studies in the clinical literature about the use of HepaSphere microspheres in liver cancer in China. The aim of this study was to present the clinical efficacy and safety of HepaSphere microspheres in liver cancer management in China.
RESULTS
The technical success was 100%, with a total of 44 HepaSphere procedures being performed in the 30 patients. There were 16 patients with HCCs and 14 patients with liver metastases, with the following primary tumor sites: colorectal, bile duct, neuroendocrine, gallbladder, pancreatic, lung, and gastric. The overall median follow-up period was six months, ranging from three to 15 months.
The tumor response was evaluated using CT/MRI according to the mRECIST criteria [7]. Following the HepaSphere microsphere treatment, two patients (6.7%) had complete responses (CR) (Figure 1), 17 (56.7%) had partial responses (PR) (Figure 2), seven (23.3%) had stable disease (SD), and four (13.3%) had progressive disease (PD). The total objective response was 63.3%, and the disease control rate was 86.7%. The pre-TACE and post-TACE tumor indicator details are given in Table 1, and many of the tumor markers had decreased one month postembolization.
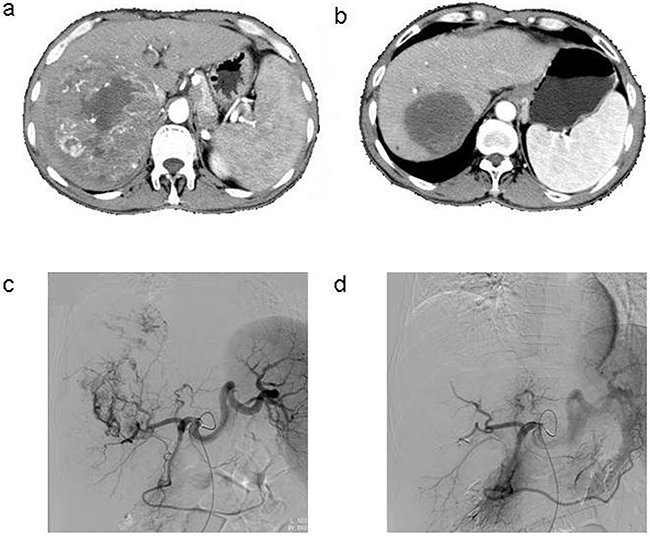
Figure 1: a. Contrast-enhanced CT scan done before the procedure in the patient with HCC, b. Enhanced CT showed complete tumor necrosis 6 months after three TACE sessions, c. Common artery angiography of the patient with HCC during 1st TACE, selective catheterisation of the pathologic branch of right hepatic artery supplying the tumor, d. After chemoembolization angiography with 1st TACE.
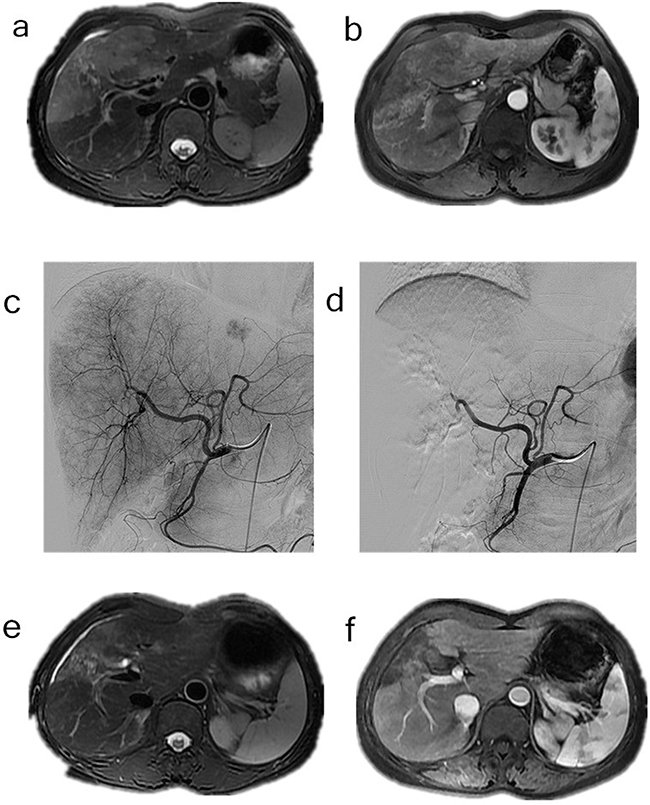
Figure 2: a-b. Contrast-enhanced MRI and CT scan done before the procedure in the patient with cholangiocarcinoma, c. Common hepatic artery angiography of the patient with cholangiocarcinoma, d. After chemoembolization angiography with extraction of pathologic vascularization, e-f. Gadolinium contrast MRI control 6 months after TACE, extraction of the vascularization of the tumor.
Table 1: The details of tumor indicators pre-TACE and post-TACE
Patient number |
Type of tumor |
Type of tumor marker |
Pre-TACE |
1m Post-TACE |
|---|---|---|---|---|
1 |
HCC |
AFP |
6373.3 |
2332.1 |
2 |
HCC |
AFP |
204.1 |
3.5 |
3 |
metastatic gallbladder tumor |
CA199 |
12000 |
12000 |
4 |
mCRC |
CEA |
15.4 |
4.3 |
5 |
mCRC |
CEA |
133.1 |
72.6 |
6 |
HCC |
AFP |
4031.9 |
15.2 |
7 |
HCC |
AFP |
2532.3 |
471.2 |
8 |
metastatic neuroendocrine tumor |
CA199 |
67.1 |
50.9 |
9 |
metastatic cholangiocarcinoma |
CA199 |
12000 |
230.1 |
10 |
metastatic lung tumor |
CA199 |
13.4 |
12.5 |
11 |
mCRC |
CEA |
50.5 |
33.1 |
12 |
metastatic gastric cancer |
CA199 |
7.2 |
4.1 |
13 |
HCC |
AFP |
62.8 |
30.5 |
14 |
HCC |
AFP |
193.5 |
39.9 |
15 |
HCC |
AFP |
1.3 |
0.9 |
16 |
HCC |
AFP |
339.9 |
133 |
17 |
HCC |
AFP |
7.8 |
4.9 |
18 |
HCC |
AFP |
6.7 |
5.6 |
19 |
HCC |
AFP |
908.3 |
81.3 |
20 |
metastatic cholangiocarcinoma |
CA199 |
40.9 |
23.1 |
21 |
metastatic pancreatic carcinoma |
CA199 |
1113.8 |
58.1 |
22 |
HCC |
AFP |
2.7 |
5.8 |
23 |
HCC |
AFP |
3 |
2.6 |
24 |
HCC |
AFP |
26 |
15.3 |
25 |
metastatic gallbladder tumor |
CA199 |
6.3 |
11.9 |
26 |
metastatic neuroendocrine tumor |
CA199 |
3.3 |
2.9 |
27 |
metastatic neuroendocrine tumor |
CA199 |
3 |
3.4 |
28 |
metastatic pancreatic carcinoma |
CA199 |
153.6 |
8.6 |
29 |
HCC |
AFP |
91.9 |
59.3 |
30 |
HCC |
AFP |
2.3 |
1.6 |
Grade 2 toxicities (NCI-CTC) occurred in 43.3% (n=13), and grade 3 toxicities occurred in 26.7% (n=8) of all of the courses in terms of the liver function post-TACE (Table 2). No reversible leukopenia or thrombocytopenia occurred in any of the patients; however, mild fevers (grade 1, n=11) and abdominal pain (grade 3, n=7) were observed in some of the cases. Three of the patients had moderate abdominal pain and were treated with pethidine hydrochloride. Overall, none of the patients had any severe complications, such as bile duct infections, liver abscesses, abdominal bleeding, tumor ruptures, gastrointestinal bleeding, marrow suppression, or myocardiotoxicity.
Table 2: Change of liver function for patients with pre-TACE and post-TACE
Liver function |
Pre-TACE |
3d Post-TACE (P)* |
1m Post-TACE (P)# |
|---|---|---|---|
ALB (g/L) |
41.7±3.54 |
36.9±5.82 (0.12) |
39.9±4.68 (0.22) |
ALT (U/L) |
30.8±11.6 |
88.1±52.9 (0.001) |
33.8±10.2 (0.17) |
AST (U/L) |
37.3±15.3 |
122.1±72.5 (0.002) |
41.2±15.3 (0.19) |
TB (μmol/L) |
12.8±4.52 |
18.3±7.65 (0.001) |
13.2±6.22 (0.17) |
*3d Post-TACE vs Pre-TACE, #1m Post-TACE vs Pre-TACE
DISCUSSION
HCC is the fifth most common form of cancer, and the third leading cause of cancer-related death worldwide. Approximately 50% of the world HCC incidence is found in China, where it is the second leading cause of cancer-related death [8]. While resection is the first-line curative treatment for liver cancer, the majority of patients are not candidates for resection; therefore, TACE is the mainstay of treatment for unresectable intermediate stage HCC patients. TACE has been clinically proven to prolong overall survival, while showing potential benefits for a patient’s quality of life.
Embolic material plays an important role in a TACE procedure. The cTACE technique requires the transarterial infusion of lipiodol and a chemotherapeutic agent, such as doxorubicin or cisplatin, into the hepatic artery, which can be followed by the embolic material. However, there are two major drawbacks to this technique: (1) incomplete lipiodol deposition in the tumor, leading to a poorer tumor response [9], and (2) most chemotherapeutic agents are hydrophilic, while lipiodol is not. This mixture would be transient, allowing for a quick release of the chemotherapeutic drug into the systemic circulation, leading to an increase in adverse events and a decrease in the local regional response. In liver cancer management, the slow release of a chemotherapeutic drug and prolonged exposure in the tumor, while lowering the systemic response, would result in a better response. Therefore, a new microsphere was developed to accommodate the need for a better embolic material with drug-eluting ability. There are two kinds of drug-eluting microspheres: HepaSphere and DC Bead [6, 10]. These microspheres could carry doxorubicin to the tumor and increase the intratumoral concentration.
When compared with lipiodol, which is commonly used in cTACE, HepaSphere microspheres have a superior safety profile and could carry a larger amount of the chemotherapeutic drug that can be released in a slow and controlled manner. The doxorubicin is released by the microspheres for a period of one month after the embolization [11]. This could provide more consistent results and facilitate the standardization of the TACE procedure.
Since the drug-eluting TACE procedure does not require the use of lipiodol, the evaluation of the tumor is not hindered by lipiodol retention, and it can be performed properly using Modified Response Evaluation Criteria In Solid Tumors (mRECIST) criteria [7]. With regard to the size of the embolic material, there is no recommendation, and it should be based on the vascularity, vessel size, and tumor anatomy. Some studies using drug-eluting embolic materials have shown that smaller calibers of microspheres are attractive, because they can achieve more distal embolization [12–15]. Only diameters <300 μm penetrate deep into the tumor microvasculature, according to the study by Lee et al. [16]. Distal embolization is desirable to avoid hypoxia-induced neoangiogenesis [17–19]. In our study, the HepaSphere microspheres were 50-100 μm in the dry state, and this was the smallest size available, since the 30-60 μm HepaSphere microspheres have not yet been introduced in China. The size the 50-100 μm HepaSphere microsphere in vivo is 200-400 μm after loading with doxorubicin; therefore, it is slightly larger than the DC Bead microsphere, which is 100-300 μm [11].
Several previous studies have shown good tumor responses in HepaSphere HCC treatment. In one study conducted by Malagari et al. in 2014 [6], the objective response was 68.9% and the one year survival was 100%, with a median follow-up period of 15.6 months. For advanced unresectable HCC, Kirchhoff et al. used degradable starch microspheres and iodized oil for embolization, and the response rates were: PD 9%, SD 55%, PR 36%, and CR 0% [20]. The overall one, two, and three-year survival rates were 75%, 59%, and 41%, respectively, and the median survival was 26 months.
Sorafenib is recommended for advanced stage HCC treatment. In a Phase II trial of sorafenib conducted by Pawlik, combined with concurrent transarterial chemoembolization and drug-eluting beads for HCC treatment, the results showed a good disease control rate of 95%. This suggests that combining cTACE and sorafenib could lead to better disease control with an acceptable complication rate [21]. Most liver metastases are hypovascular in nature, and the cTACE treatment response remains unsatisfactory, with possible complication development, like infection. In the study by Jarzabek et al., doxorubicin loaded HepaSphere microspheres were used as the liver metastasis treatment. The objective response rate was 26.7%, and the disease control rate was 60.1%, indicating that HepaSphere microspheres are a potential treatment for liver metastases [5]. These patients showed liver metastases from colorectal, cholangiocarcinoma, gastrinoma, gallbladder, pancreatic, gastrointestinal stromal, lung, kidney, breast, and larynx primary tumors. Another study conducted by Huppert et al. using irinotecan loaded HepaSphere microspheres in metastatic colorectal cancer (mCRC) showed the HepaSphere microspheres to be safe and effective in mCRC treatment [22]. The preliminary results from our study also showed a promising result with the use of HepaSphere microspheres in liver cancer treatment. The total objective response rate was 63.3%, and the disease control rate was 86.7%, which seemed to be superior or comparable with the results of the studies in which drug-eluting devices of 100-300 μm were used [13, 23].
Overall, drug-eluting TACE using HepaSphere microspheres is safe and well tolerated. The liver enzymes were slightly increased after embolization in all of the patients, but returned to normal 3-4 days later, a pattern that was also observed in other drug-eluting embolic studies [13, 15, 24-26]. This happened frequently in the cTACE procedures. More than 90% of those patients that underwent cTACE treatment exhibited postembolization syndrome (PES). However, only some of the patients treated with HepaSphere microspheres showed mild PES, and the severity was much lesser than those undergoing cTACE. Based on previous studies of drug-eluting TACE with DC Bead microspheres, complications occurred in 4.2%-11.4% of the cases, including gastric ulcers, liver failure, and cholecystitis. The treatment-related mortality was 0%-3.7%, mainly due to tumor rupture, liver failure, liver abscess, and cholecystitis [24, 25]. None of our patients treated with HepaSphere microspheres showed these complications.
The limitations of our study were that it was a single center study with a small patient number and a short follow-up period, with diverse patient characteristics and tumor backgrounds. Further investigations are required to evaluate the long term efficacy in a larger cohort or a randomized control trial. Despite these limitations, the use of HepaSphere microspheres in liver cancer management may be a safe, well-tolerated, and effective treatment modality, which has been shown to have a good objective response and disease control rate in both hypervascular and hypovascular tumors.
MATERIALS AND METHODS
Patients
Thirty patients from the First Affiliated Hospital at the Zhejiang University School of Medicine in Zhejiang, China, from February 2014 to September 2015, were included in our study. There were 18 males, 12 females, and the median age was 53.5 years old. All of the patients were treated with doxorubicin-loaded HepaSphere microspheres. Each of the HCC patients was diagnosed clinically and pathologically [27], and all of the patients with liver metastasis had a biopsy-confirmed pathological diagnosis. Based on the tumor vascularity and pathology, 16 of the patients were classified as having hypervascular tumors (all had HCC). Fourteen of the patients had hypovascular tumors: three had metastatic colorectal cancer (mCRC), two had metastatic gallbladder tumors, three had metastatic neuroendocrine tumors, two had metastatic cholangiocarcinoma, two had metastatic pancreatic carcinoma, one had a metastatic lung tumor, and one had metastatic gastric cancer.
Letters of consent were obtained from all of the patients, and the experimental protocols were approved by the local ethics committee (The Medical Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine, Zhejiang, China). The procedure was carried out in accordance with the approved guidelines, and informed consent was obtained from all of the subjects. All of the data was anonymized and de-identified prior to the analysis.
Patient eligibility
Inclusion criteria
A patient was included in this study if they: (1) had an unresectable HCC or liver metastasis, were not a candidate for locoregional tumor ablation, were refractory or intolerant of systemic chemotherapy, or had recurrent HCC; (2) were Child-Pugh status A or B, or Eastern Cooperative Oncology Group (ECOG) 0 to 2; and (3) did not have a tumor thrombosis in the main portal vein.
Exclusion criteria
A patient was excluded if they: (1) were Child-Pugh status C, (2) had uncorrectable impaired clotting, (3) had a tumor thrombosis in the main portal vein or portal hypertension, (4) had an infectious disease (e.g. liver abscess), (5) had a life expectancy of less than 3 months, or (6) had an aneurysm in the hepatic artery or portal vein.
Doxorubicin loading and TACE procedure
HepaSphere microspheres are loadable microspheres with a dry caliber of 50-100 μm, which expands to 200-400 μm after doxorubicin loading. The drug loading method was conducted as suggested by the manufacturer. The doxorubicin solution was prepared by adding 4 ml of normal saline into each 10 mg vial of doxorubicin powder, creating a concentration of 2.5 mg/ml. Five 20 ml vials of doxorubicin were prepared for each patient. Next, 10 ml of the doxorubicin solution was added into a 50-100 μm HepaSphere vial, mixed gently 5-10 times, and allowed to sit for 10 minutes. After 10 minutes, the remaining doxorubicin solution was loaded into the HepaSphere vial and allowed to stand for 60 minutes. An hour later, all of the supernatant was extracted, and 20 ml of nonionic contrast medium was added into a syringe containing the doxorubicin-loaded HepaSphere microspheres, and mixed gently until homogeneity was reached.
Procedure
The interventional procedure was done by the experienced interventional radiologists at our hospital. Hepatic angiography was performed to identify the feeding artery and collaterals. In the case of a hypovascular tumor, angiography at the superior mesenteric artery, inferior mesenteric artery, and left gastric artery had to be conducted.
The TACE procedures followed the classical steps, and were performed superselectively in the tumor-feeding arteries. After the identification of the feeding arteries, a microcatheter was advanced as distally as possible. Then, the HepaSphere microspheres were injected slowly, at a rate of 1 ml/min, until stasis was observed. The angiography was repeated to ensure the devascularization of the feeding arteries had occurred. In those cases in which a tumor stain was observed, the HepaSphere microspheres were injected until the tumor stain disappeared. Normally, one vial of HepaSphere was required, with a maximum dose of two vials. Embosphere microspheres (Merit Medical Systems, Inc., South Jordan, UT, USA) were injected into the feeding arteries when the tumor stain was still observed after two HepaSphere vials were used.
Postembolization patient management
The routine postembolization medication included the following: 100 mg of tramadol was only used in case of pain, 40 mg of esomeprazole was given intravenously every 12 h, 5 mg of ondansetron was given intravenously every 12 h, and 1500 mg cefuroxime sodium was given intravenously every 12 h for 3 days after embolization. Intravenous drops of 80 mg of a glycyrrhizin compound were given daily, with 1000 mg of ademetionine to protect the liver function. Finally, 200 mg of celecoxib was used if the temperature was higher than 38.5°C.
Follow-up
CT/MRI images were assessed one month after the procedure using the modified Response Evaluation Criteria in Solid Tumors (mRECIST) [7]. Laboratory analyses, including 3-day liver function tests for each patient, were also performed. During the procedure and follow-up, any adverse events were collected according to the National Cancer Institute Common Toxicity Criteria (NCI-CTC) ver. 4.0.
Data analysis
The data processing and analyses were performed using SPSS 19.0 (Chicago, IL, USA). Chi-squared and t-tests were used when appropriate, and statistical significance was defined as a P value <0.05.
ACKNOWLEDGMENTS
Jun-Hui Sun, Guan-Hui Zhou, Yue-Lin Zhang, Chun-Hui Nie, Tan-Yang Zhou, Tong-Yin Zhu carried out the research and drafted the manuscript. Wei-Lin Wang and Shu-Sen Zheng revised the manuscript. Jing Ai, Wei-Lin Wang and Shu-Sen Zheng kindly offered valuable suggestions about the experiment design. Jun-Hui Sun, Guan-Hui Zhou, Yue-Lin Zhang designed the experiments, analyzed the results and revised the manuscript. All authors reviewed the manuscript.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
GRANT SUPPORT
This study was supported by the National Clinical Key Subject Construction Project (General Surgery), the National Natural Science Foundation of China (No. 81371658), Zhejiang Provincial Natural Science Foundation of China (No. LQ14H120001), Medical Health Fund of Zhejiang Province (No.2013KYB097), and the Basic Health Appropriate Technology for the Transformation of Major Projects during the 12th Five-Year Plan Period of Zhejiang Province (Grant No.2013T301-15)
REFERENCES
1. Bruix J and Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011; 53:1020-1022.
2. Benson ABR, Abrams TA, Ben-Josef E, Bloomston PM, Botha JF, Clary BM, Covey A, Curley SA, D’Angelica MI, Davila R, Ensminger WD, Gibbs JF, Laheru D, Malafa MP, Marrero J, Meranze SG, et al. NCCN clinical practice guidelines in oncology: hepatobiliary cancers. J Natl Compr Canc Netw. 2009; 7:350-391.
3. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012; 56:908-943.
4. Huppert P, Wenzel T and Wietholtz H. Transcatheter arterial chemoembolization (TACE) of colorectal cancer liver metastases by irinotecan-eluting microspheres in a salvage patient population. Cardiovasc Intervent Radiol. 2014; 37:154-164.
5. Jarzabek M, Jargiello T, Wolski A, Poluha P and Szczerbo-Trojanowska M. Drug-eluting microspheres transarterial chemoembolization (DEM TACE) in patients with liver metastases. Pilot study. Pol J Radiol. 2011; 76:26-32.
6. Malagari K, Pomoni M, Moschouris H, Kelekis A, Charokopakis A, Bouma E, Spyridopoulos T, Chatziioannou A, Sotirchos V, Karampelas T, Tamvakopoulos C, Filippiadis D, Karagiannis E, Marinis A, Koskinas J and Kelekis DA. Chemoembolization of hepatocellular carcinoma with HepaSphere 30-60 mum. Safety and efficacy study. Cardiovasc Intervent Radiol. 2014; 37:165-175.
7. Lencioni R and Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010; 30:52-60.
8. Jemal A, Bray F, Center MM, Ferlay J, Ward E and Forman D. Global cancer statistics. CA Cancer J Clin. 2011; 61:69-90.
9. Chen CS, Li FK, Guo CY, Xiao JC, Hu HT, Cheng HT, Zheng L, Zong DW, Ma JL, Jiang L and Li HL. Tumor vascularity and lipiodol deposition as early radiological markers for predicting risk of disease progression in patients with unresectable hepatocellular carcinoma after transarterial chemoembolization. Oncotarget. 2016; 7:7241-7252. doi: 10.18632/oncotarget.6892.
10. Song MJ, Chun HJ, Song DS, Kim HY, Yoo SH, Park CH, Bae SH, Choi JY, Chang UI, Yang JM, Lee HG and Yoon SK. Comparative study between doxorubicin-eluting beads and conventional transarterial chemoembolization for treatment of hepatocellular carcinoma. J Hepatol. 2012; 57:1244-1250.
11. Dinca H, Pelage J, Baylatry M, Ghegediban S, Pascale F and Manfait M. Why do small size doxorubicin-eluting microspheres induce more tissue necrosis than larger ones? A comparative study in healthy pig liver (oral communication 2206-2). CIRSE Annual meeting, Lisbon. 2012.
12. Varela M, Real MI, Burrel M, Forner A, Sala M, Brunet M, Ayuso C, Castells L, Montana X, Llovet JM and Bruix J. Chemoembolization of hepatocellular carcinoma with drug eluting beads: efficacy and doxorubicin pharmacokinetics. J Hepatol. 2007; 46:474-481.
13. Malagari K, Chatzimichael K, Alexopoulou E, Kelekis A, Hall B, Dourakis S, Delis S, Gouliamos A and Kelekis D. Transarterial chemoembolization of unresectable hepatocellular carcinoma with drug eluting beads: results of an open-label study of 62 patients. Cardiovasc Intervent Radiol. 2008; 31:269-280.
14. Akinwande OK, Philips P, Duras P, Pluntke S, Scoggins C and Martin RC. Small Versus Large-Sized Drug-Eluting Beads (DEBIRI) for the Treatment of Hepatic Colorectal Metastases: A Propensity Score Matching Analysis. Cardiovasc Intervent Radiol. 2014.
15. Malagari K, Pomoni M, Kelekis A, Pomoni A, Dourakis S, Spyridopoulos T, Moschouris H, Emmanouil E, Rizos S and Kelekis D. Prospective randomized comparison of chemoembolization with doxorubicin-eluting beads and bland embolization with BeadBlock for hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2010; 33:541-551.
16. Lee KH, Liapi E, Vossen JA, Buijs M, Ventura VP, Georgiades C, Hong K, Kamel I, Torbenson MS and Geschwind JF. Distribution of iron oxide-containing Embosphere particles after transcatheter arterial embolization in an animal model of liver cancer: evaluation with MR imaging and implication for therapy. J Vasc Interv Radiol. 2008; 19:1490-1496.
17. Xiang Z, Zeng Z, Tang Z, Fan J, Sun H, Wu W and Tan Y. Increased expression of vascular endothelial growth factor-C and nuclear CXCR4 in hepatocellular carcinoma is correlated with lymph node metastasis and poor outcome. Cancer J. 2009; 15:519-525.
18. Wang B, Xu H, Gao ZQ, Ning HF, Sun YQ and Cao GW. Increased expression of vascular endothelial growth factor in hepatocellular carcinoma after transcatheter arterial chemoembolization. Acta Radiol. 2008; 49:523-529.
19. Miura H, Miyazaki T, Kuroda M, Oka T, Machinami R, Kodama T, Shibuya M, Makuuchi M, Yazaki Y and Ohnishi S. Increased expression of vascular endothelial growth factor in human hepatocellular carcinoma. J Hepatol. 1997; 27:854-861.
20. Kirchhoff TD, Bleck JS, Dettmer A, Chavan A, Rosenthal H, Merkesdal S, Frericks B, Zender L, Malek NP, Greten TF, Kubicka S, Manns MP and Galanski M. Transarterial chemoembolization using degradable starch microspheres and iodized oil in the treatment of advanced hepatocellular carcinoma: evaluation of tumor response, toxicity, and survival. Hepatobiliary Pancreat Dis Int. 2007; 6:259-266.
21. Pawlik TM, Reyes DK, Cosgrove D, Kamel IR, Bhagat N and Geschwind JF. Phase II trial of sorafenib combined with concurrent transarterial chemoembolization with drug-eluting beads for hepatocellular carcinoma. J Clin Oncol. 2011; 29:3960-3967.
22. Lencioni R, Aliberti C, de Baere T, Garcia-Monaco R, Narayanan G, O’Grady E, Rilling WS, Walker D and Martin RC. Transarterial treatment of colorectal cancer liver metastases with irinotecan-loaded drug-eluting beads: technical recommendations. J Vasc Interv Radiol. 2014; 25:365-369.
23. Lammer J, Malagari K, Vogl T, Pilleul F, Denys A, Watkinson A, Pitton M, Sergent G, Pfammatter T, Terraz S, Benhamou Y, Avajon Y, Gruenberger T, Pomoni M, Langenberger H, Schuchmann M, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent Radiol. 2010; 33:41-52.
24. Malagari K, Pomoni M, Spyridopoulos TN, Moschouris H, Kelekis A, Dourakis S, Alexopoulou E, Koskinas J, Angelopoulos M, Kornezos J, Pomoni A, Tandeles S, Marinis A, Rizos S and Kelekis D. Safety profile of sequential transcatheter chemoembolization with DC Bead: results of 237 hepatocellular carcinoma (HCC) patients. Cardiovasc Intervent Radiol. 2011; 34:774-785.
25. Burrel M, Reig M, Forner A, Barrufet M, Lope CRd, Tremosini S, Ayuso C, Llovet JM, Real MI and Bruix J. Survival of patients with hepatocellular carcinoma treated by transarterial chemoembolisation (TACE) using Drug Eluting Beads. Implications for clinical practice and trial design. Journal of Hepatology. 2012; 56:1330-1335.
26. Reyes DK, Vossen JA, Kamel IR, Azad NS, Wahlin TA, Torbenson MS, Choti MA and Geschwind JF. Single-center phase II trial of transarterial chemoembolization with drug-eluting beads for patients with unresectable hepatocellular carcinoma: initial experience in the United States. Cancer J. 2009; 15:526-532.
27. Bruix J and Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005; 42:1208-1236.