
INTRODUCTION
Paclitaxel is a chemotherapeutic agent that acts as a microtubule stabilizer to inhibit cell division, which ultimately leads to cell death [1]. Paclitaxel has a wide antineoplastic spectrum and it is broadly used for the treatment of lung, ovarian, breast, head and neck, bladder, and other epithelial cancers [2]. The clinical use of paclitaxel is limited by its poor aqueous solubility. Therefore, it is usually formulated as an emulsion for intravenous (IV) delivery using 50% polyoxyethylated castor oil (Cremophor EL) and 50% ethanol as the solvent [3]. However, thisemulsion can lead to infusion-related hypersensitivity reactions (HSRs) [4]. The incidences of allergic and serious allergic reactions associated with paclitaxel administration are 0.7-7.7%. Some of these allergic reactions can be fatal [5, 6]. Therefore, effective premedications are usually administered to decrease the rate of allergic reactions and avoid the occurrence of severe allergic reactions due to paclitaxel treatment [7]. The standard premedication consists of dexamethasone, cimetidine, and diphenhydramine. Dexamethasone is orally administered 12 and 6 h before paclitaxel administration, whereas cimetidine and diphenhydramine are intravenously administered 30 min before paclitaxel administration [8]. Dexamethasone plays a pivotal role in preventing allergic reactions; however, it has also been associated with a number of adverse reactions. In addition, dexamethasone must be taken 12 and 6 h before chemotherapy. Therefore, forgetting to take one or both dexamethasone doses may be unsafe for patients. In view of this, experimental premedication with an IV dose of dexamethasone 30 min prior to paclitaxel administration has been implemented clinically. However, the results of the systematic reviews on the therapeutic effects of these different regimens are unclear [9].
In this report, we analysed the effects of two common administration routes of dexamethasone premedication on the prevention of paclitaxel-induced HSRs. We also evaluated the effectiveness of each route to provide an evidence-based reference for physicians.
RESULTS
Selected studies
Of the studies initially identified, we excluded reports that did not meet the inclusion criteria after first screening the study titles and abstracts. Six studies [9–14] were ultimately included in the meta-analysis. Figure 1 illustrates how the six selected studies were obtained from the literature search.
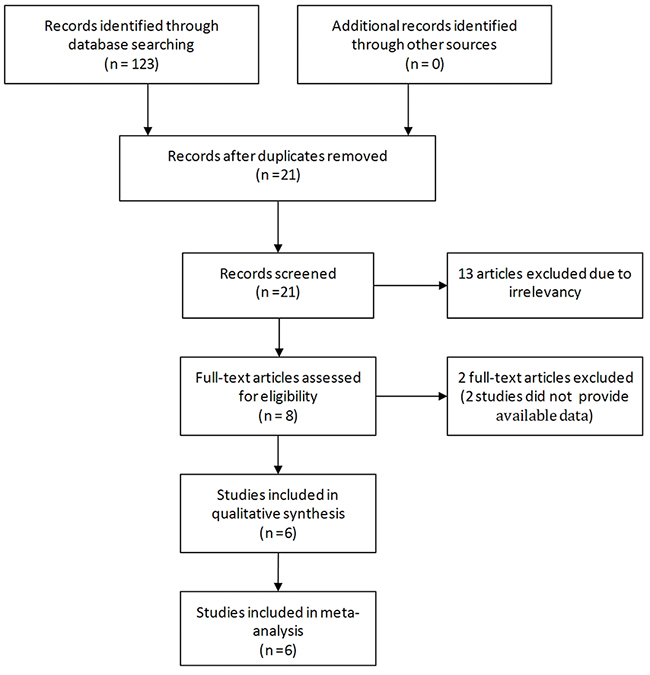
Figure 1: Flow diagram of the study selection process.
Study characteristics and quality assessment
The six selected studies were published between 1996 and 2013, and including two in Canada [9], two in China [12, 13], one in Sweden [11] and one in Italy [10]. The sample sizes of the included studies ranged from 137 to 483 patients, comprising a total of 1347 included patients. The main characteristics of the studies are listed in Table 1. Five of the six inclusion studies were retrospective studies, with the sixth study published by P Rosenberg classified as a randomized controlled trial [11], but none of these studies described the random allocation method in detail or specified if there was blinding or allocation concealment. In addition, three of the studies only recorded the incidences of allergic (Common Terminology Criteria for Adverse Events version 3.0, grades 1 to 2) and severe allergic reactions (Common Terminology Criteria for Adverse Events version 3.0, grade 3) and were therefore missing a detailed description of the final indicator [14]. Table 1 shows the Newcastle–Ottawa scores and the modified Jadad scale for the quality assessment of the non-randomized studies and randomized studies.
Table 1: Summary of the characteristics of the studies included in the meta-analysis
Study |
First author |
Publication year |
PO-D |
IV-D |
Quality score |
||||
|---|---|---|---|---|---|---|---|---|---|
SAA |
AA |
Total |
SAA |
AA |
Total |
||||
1 |
Gennari A |
1996 |
1 |
7 |
90 |
1 |
3 |
47 |
6 |
2 |
Kwon JS |
2002 |
1 |
8 |
107 |
8 |
19 |
110 |
8 |
3 |
Hua XM |
2004 |
8 |
24 |
212 |
12 |
34 |
271 |
5 |
4 |
P Rosenberg |
2002 |
5 |
29 |
106 |
5 |
29 |
99 |
4 |
5 |
Chen Y |
2013 |
0 |
3 |
77 |
0 |
1 |
80 |
5 |
6 |
Sean M |
2013 |
0 |
5 |
93 |
3 |
8 |
55 |
7 |
Abbreviations: AA, allergic reaction; IV-D, intravenous dexamethasone; PO-D, oral dexamethasone; SAA, serious allergic reaction
Main results of meta-analysis
Comparison of the HSR rates from the PO-D and IV-D treatments
The six studies included 1347 patients; of these, 94 (14.20%) patients in the IV-D group and 76 (11.09%) patients in the PO-D group experienced an HSR to paclitaxel (Figure 2A). We used a fixed effects model to analyse the results owing to the moderate inconsistency between the two groups of study results (χ2 = 6.81, P = 0.23, I2 = 27%). The combined OR (95% CI) was 0.76 (0.55-1.06), which indicates no statistically significant association between the PO-D and IV-D treatments. In a further investigation, subgroup analyses were performed. When stratified by “study type,” the “retrospective studies” group yielded an OR of 0.71, and the 95% CI was 0.47–1.05 (Figure 2B). In the subgroup analysis by “country,” the “non-Chinese studies” group yielded an OR of 0.65 with a 95% CI of 0.43–1.00 (Figure 2C).
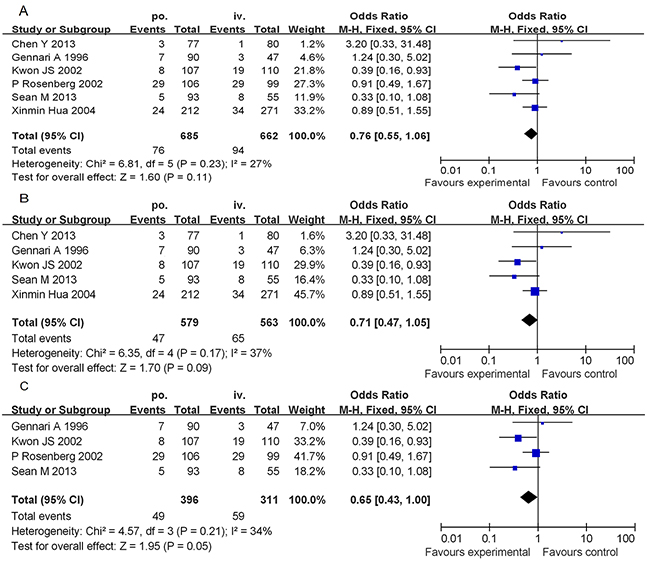
Figure 2: Forest plots of the meta-analysis of the allergic reactions in patients administered PO-D regimen compared with reactions in patients administered the IV-D regimen. Notes: A. overall studies; B. subgroup analyses (excluding the randomized controlled trial); C. subgroup analyses (excluding the People’s Republic of China). Abbreviations: IV-D, intravenous dexamethasone; CI, confidence interval; PO-D, oral dexamethasone.
Comparison of the severe HSR rates from the PO-D and IV-D treatments
The rates of severe HSRs from pretreatment with PO-D versus pretreatment with IV-D were 2.47% (15/608) versus 4.98% (29/582), respectively, (Figure 3A). We used a fixed effects model to analyse the results owing to the moderate inconsistency between the two groups of study results (χ2 = 5.23, P = 0.26, I2 = 23%). The combined OR (95% CI) was 0.53 (0.28-0.99), which indicates a statistically significant association between the PO-D and IV-D treatments. In the subgroup analysis by study type and country, the combined ORs were 0.45 (95% CI: 0.22–0.92, P = 0.03) for the retrospective studies (Figure 3B) and 0.36 (95% CI: 0.15–0.85, P = 0.02) for the non-Chinese studies (Figure 3C). According to Figure 3, the number of severe HSRs from PO-D premedication accounted for 36-53% of those from IV-D premedication. This indicates that the incidence of severe HSRs due to PO-D premedication is significantly lower than that from premedication with IV-D in preventing paclitaxel-induced HSRs.
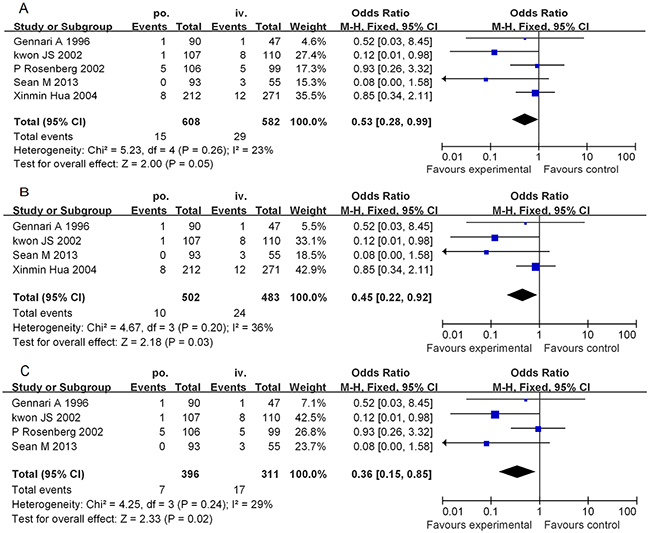
Figure 3: Forest plots of the meta-analysis of the severe allergic reactions in patients administered the PO-D regimen compared with in patients administered the IV-D regimen. Notes: A. overall studies; B. subgroup analyses (excluding the randomized controlled trial); C. subgroup analyses (excluding the People’s Republic of China). Abbreviations: IV-D, intravenous dexamethasone; CI, confidence interval; PO-D, oral dexamethasone.
Publication bias
Regarding publication bias, there was an obvious asymmetry of the funnel plot (Figure 4), which suggests that there was some level of publication bias. However, because the number of included studies was only six, the funnel plots may not be significant. Egger’s test revealed that publication bias was not significant in both overall HSR (P = 0.073) and severe HSR (P = 0.195) analysis.
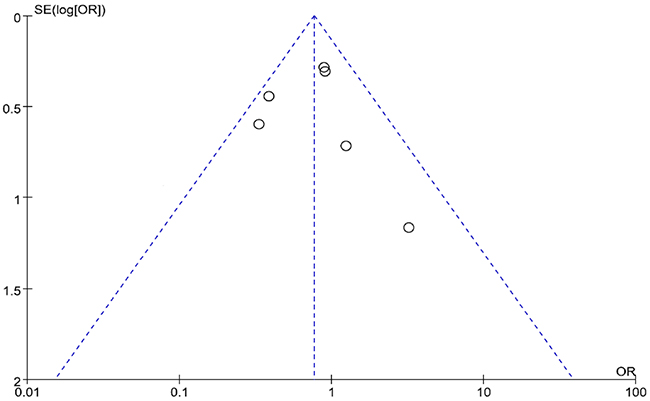
Figure 4: Funnel plots of the six selected studies.
DISCUSSION
Paclitaxel is a natural diterpenoid extracted from the stem bark of Taxus brevifolia and has been a research focus for decades due to its unique therapeutic effects and excellent anticancer activities [1–3]. By promoting tubulin assembly and stabilizing microtubules, paclitaxel can inhibit mitosis and result in the apoptosis of tumour cells [15–16]. Due to paclitaxel’s lack of aqueous solubility, the drug is usually solubilized in polyoxyethylated castor oil (Cremophor EL) [17]; however, this can cause HSRs because Cremophor EL induces the release of histamine. Paclitaxel-induced HSRs are consistent with type I HSRs, which are caused by immunoglobulin E-mediated release of histamine and leukotrienes from mast cells [18–21]. It has been reported that severe HSRs are characterized by chest pain, dyspnoea, bronchospasm, urticaria, abdominal cramping, and hypertension [22], all of which can be life threatening at times. In addition, if severe HSRs occur, paclitaxel treatment is discontinued, which is disadvantageous for patients; thus, prophylactic treatments have been used. Dexamethasone is a long-acting synthetic glucocorticoid with a biological half-life of approximately 48 h. Dexamethasone exerts its effects by diminishing cytokine production by tumours [23], increasing the expression level of tumour necrosis factor [24], and decreasing the expression levels of interleukin 1 beta [25] and vascular endothelial growth factor [26, 27]. Dexamethasone can alleviate myelosuppression and enhance the antitumour effects based on this activity. Thus, it is an essential drug that is widely administered with chemotherapeutic agents to alleviate the toxic side effects of chemotherapy [27–29].
For patients treated with paclitaxel, the US Food and Drug Administration has approved premedication with oral dexamethasone (20 mg, administered 12 and 6 h before paclitaxel administration), oral or IV diphenhydramine (25-50 mg), and an H2 antagonist. Diphenhydramine and the H2 antagonist are commonly administered 30-60 min prior to paclitaxel infusion. However, it has been reported that patients are noncompliant with and inconvenienced by the abovementioned oral dosing schedules. In addition, overuse of the premedication regimen can critically desensitize cells against chemotherapy and induce HSRs [30]. Some studies [16, 31] have shown that pretreatment with dexamethasone can inhibit the therapeutic efficacy of paclitaxel. The inhibitory effect of a 20 mg/kg dose of paclitaxel on the growth of breast and ovarian xenograft tumours was found to be reduced by approximately 20-25% when animals were pretreated with 1 mg/kg dexamethasone [16]. This observation prompted investigations into developing more convenient but equally safe alternative dexamethasone regimens. Premedication with IV-D (administered 30 min before paclitaxel infusion) precludes the oral intake of dexamethasone on the night before and on the morning of paclitaxel treatment. This can improve patient compliance and, to a certain degree, the patient’s quality of life.
The data obtained from the meta-analysis indicates that the incidence of HSRs and severe HSRs due to PO-D premedication was lower than that due to IV-D premedication. Therefore, we suggest that the PO-D regimen should be the preferred regimen to minimize paclitaxel infusion-related HSRs. However, prophylaxis with IV-D (10-20 mg, administered 30 min before paclitaxel administration) may be necessary in the following conditions: (i) if the patient is noncompliant, (ii) if the patient forgot to take either or both oral doses of the premedication, and (iii) if higher doses of PO-D are required, which can induce some adverse reactions. The latter is especially important for patients with diabetes or osteoporosis. Paclitaxel-related HSRs occurring after IV-D administration should be immediately and appropriately managed by using the following techniques: (i) stopping the paclitaxel infusion but continuing to administer IV normal saline at 200 cc/h to maintain and stabilize blood pressure; (ii) administering oxygen at 2-4 L/min via nasal cannula to maintain oxygenation; (iii) administering an IV push of 125 mg methylprednisolone to counteract respiratory distress; (iv) administering an IV push of 50 mg diphenhydramine to counteract respiratory distress and inflammation; (v) continuously monitoring blood pressure, pulse, and oxygen saturation; and (vi) immediately notifying the physician for further orders and initiating a code if either airway patency is not maintained or cardiopulmonary arrest occurs [32]. Beyond these recovery methods, we should reevaluate additional research that is available regarding paclitaxel infusion-associated HSRs because the solvent and dosage formulations are increasingly changing.
O’Cathail SM et al [9] reported on the management of paclitaxel-induced HSRs. The authors compared the incidence of HSRs resulting from administration of the conventional prophylactic regimen of two oral doses of corticosteroids with the incidence from administering a single IV dose of a corticosteroid, which was similar to our meta-analysis. In that study, only two previous reports, both of which were English articles, were reviewed in addition to their own experience on the subject. The authors observed a statistically significant difference between the frequencies of HSRs from the two different regimens. However, only a few severe HSRs were observed in the studies, and a meta-analysis of severe HSRs was not performed. In this study, we analysed six independent studies, including two Chinese articles, obtained from searches of English and Chinese databases.
The data obtained from our meta-analysis indicate that premedication with either PO-D or IV-D can prevent HSRs and severe HSRs due to paclitaxel administration. However, compared with the standard regimen of administering PO-D at 12 and 6 h before paclitaxel infusion, administering IV-D 30 min before paclitaxel infusion is associated with a higher rate of HSRs. The differences in the rates of severe HSRs between the two administration routes were found to be statistically significant (P = 0.05). In the subgroup analyses according to study type and country, similar outcomes were observed between the two dexamethasone premedication protocols. This suggests that PO-D protocols are the better premedication option.
Our meta-analysis had several limitations. First, because only six studies met our inclusion criteria, publication bias could not be completely excluded based on the low power of the funnel plot asymmetry and Egger’s test. Second, the number of included patients was small, and the lower quality of the non-randomized and randomized studies could make the conclusion less convincing. Third, one study [12] used a different study protocol as well as different doses of dexamethasone, which could have caused significant heterogeneity in the data; however, the heterogeneity from our data analysis was not significant. Therefore, large-scale and well-designed randomized controlled studies are needed to verify these results.
In summary, our meta-analysis shows there was no significant difference between PO-D and IV-D administration in preventing HSRs. The PO-D protocol could significantly decrease the risk of severe HSRs induced by paclitaxel compared to IV-D administration. More randomized controlled trials with larger sample sizes should be conducted to confirm these findings.
MATERIALS AND METHODS
Search strategy
We performed a systematic literature search in PubMed, China National Knowledge Infrastructure, and Web of Science databases using the following keywords: “paclitaxel,” “dexamethasone,” “allergic reactions,” and “hypersensitivity reactions.” We then assessed the reference lists of the selected articles for studies that compared the effects of premedication with oral and IV dexamethasone on preventing paclitaxel-induced allergic reactions. We selected randomized and non-randomized trials provided they were well designed.
Inclusion criteria
Published studies were selected for analysis based on the following criteria: (i) use of human subjects, (ii) study design (controlled clinical study comparing the effects of two administration routes of dexamethasone on preventing paclitaxel-induced allergic reactions), and (iii) dose of dexamethasone. We selected studies in which oral dexamethasone (PO-D; 10-20 mg, given 12 and 6 h before paclitaxel administration) and IV dexamethasone (IV-D; 10-20 mg, given 30 min before paclitaxel administration) were assigned to the control and experimental groups, respectively.
Exclusion criteria
The exclusion criteria were as follows: (i) original studies that did not compare the effects of two administration routes of dexamethasone on preventing paclitaxel-induced allergic reactions and (ii) original studies that did not meet criterion (i) but in which different doses of dexamethasone were administered to the experimental and control groups.
Study selection and data extraction
Two reviewers independently screened the titles and abstracts of all identified articles and excluded studies that clearly did not meet the criteria. A second screening was based on a full text review. Information collected from these publications included the following: first author’s name, publication year, study design, sample size, and quality evaluation. Next, we extracted all data using a standardized data extraction form. Differences were resolved through discussions with a third independent expert.
Quality evaluation
To determine the validity of the selected studies, a modified Jadad scale was used to assess the quality of the included randomized studies [33]. High quality studies have scores of 4-8, whereas low quality studies have scores of 0-3. For non-randomized studies, the Newcastle-Ottawa Quality Assessment Scale was used [34]. Each study was graded as either low quality (0-5) or high quality (6-9).
Statistical analysis
All statistical meta-analyses were conducted using RevMan 5.2 software, which was provided by Cochrane (London, UK). Heterogeneity among the studies was evaluated using the X2 test. An alpha level of 5% was used to designate statistical significance. We used a fixed effects model to analyse results when there was no significant heterogeneity (P > 0.05, I2 ≤ 50%). On the other hand, a random effects model was used when there was significant heterogeneity (P < 0.05, I2 ≤ 50%) but no clinical differences. Pooled odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for the categorical outcomes using the Mantel-Haenszel fixed effects model because there was no evidence of significant heterogeneity for the outcomes.
CONFLICTS OF INTEREST
The authors report no conflicts of interest in this work.
REFERENCES
1. Loong HH, Chan AC, Wong AC. Evolving evidence of the efficacy and safety of nab-paclitaxel in the treatment of cancers with squamous histologies. J Cancer. 2016; 7:268–75. doi: 10.7150/jca.12986.
2. Barbuti AM, Chen ZS. Paclitaxel through the ages of anticancer therapy: exploring its role in chemoresistance and radiation therapy. Cancers (Basel). 2015; 7:2360–71. doi: 10.3390/cancers7040897.
3. van Zuylen L, Karlsson MO, Verweij J, Brouwer E, de Bruijn P, Nooter K, Stoter G, Sparreboom A. Pharmacokinetic modeling of paclitaxel encapsulation in Cremophor EL micelles. Cancer Chemother Pharmacol. 2001; 47:309–18. doi: 10.1007/s002800000215.
4. Szebeni J, Muggia FM, Alving CR. Complement activation by Cremophor EL as a possible contributor to hypersensitivity to paclitaxel: an in vitro study. J Natl Cancer Inst. 1998; 90:300–06. doi: 10.1093/jnci/90.4.300.
5. Kwon JS, Elit L, Finn M, Hirte H, Mazurka J, Moens F, Trim K. A comparison of two prophylactic regimens for hypersensitivity reactions to paclitaxel. Gynecol Oncol. 2002; 84:420–25. doi: 10.1006/gyno.2001.6546.
6. Berger MJ, Vargo C, Vincent M, Shaver K, Phillips G, Layman R, Macrae E, Mrozek E, Ramaswamy B, Wesolowski R, Shapiro CL, Lustberg MB. Stopping paclitaxel premedication after two doses in patients not experiencing a previous infusion hypersensitivity reaction. Support Care Cancer. 2015; 23:2019–24. doi: 10.1007/s00520-014-2556-x.
7. Wiernik PH, Schwartz EL, Strauman JJ, Dutcher JP, Lipton RB, Paietta E. Phase I clinical and pharmacokinetic study of taxol. Cancer Res. 1987; 47:2486–93.
8. Kintzel PE. Prophylaxis for paclitaxel hypersensitivity reactions. Ann Pharmacother. 2001; 35:1114–17. doi: 10.1345/aph.10287.
9. O’Cathail SM, Shaboodien R, Mahmoud S, Carty K, O’Sullivan P, Blagden S, Gabra H, Whear S, Kwon JS, Agarwal R. Intravenous versus oral dexamethasone premedication in preventing Paclitaxel infusion hypersensitivity reactions in gynecological malignancies. Int J Gynecol Cancer. 2013; 23:1318–25. doi: 10.1097/IGC.0b013e31829f1799.
10. Gennari A, Salvadori B, Tognoni A, Conte PF. Rapid intravenous premedication with dexamethasone prevents hypersensitivity reactions to paclitaxel. Ann Oncol. 1996; 7:978–79. doi: 10.1093/oxfordjournals.annonc.a010806.
11. Rosenberg P, Andersson H, Boman K, Ridderheim M, Sorbe B, Puistola U, Parö G. Randomized trial of single agent paclitaxel given weekly versus every three weeks and with peroral versus intravenous steroid premedication to patients with ovarian cancer previously treated with platinum. Acta Oncol. 2002; 41:418–24. doi: 10.1080/028418602320404998.
12. Hua XM, Liu FL, Ren XW, Duan GX, Li ZJ, Zhang CJ, Yang YJ, Zhang GX. A study of steroid premedication for hypersensitivity reaction and reinfusion in taxane family regimen. J Pract Oncol. 2004; 18:38–40.
13. Chen Y, Qi HX. A comparison of two premedication protocols for hypersensitivity reactions to paclitaxel. J Chifeng Univ. 2013; 29:108–09.
14. Common Terminology Criteria for Adverse Events v 4.3. National Cancer Institute, http://evs.nci.nih.gov/ftp1/CTCAE (2010, accessed December 2010).
15. Wen G, Qu XX, Wang D, Chen XX, Tian XC, Gao F, Zhou XL. Recent advances in design, synthesis and bioactivity of paclitaxel-mimics. Fitoterapia. 2016; 110:26–37. doi: 10.1016/j.fitote.2016.02.010.
16. Sui M, Chen F, Chen Z, Fan W. Glucocorticoids interfere with therapeutic efficacy of paclitaxel against human breast and ovarian xenograft tumors. Int J Cancer. 2006; 119:712–17. doi: 10.1002/ijc.21743.
17. Zhang Q, Huang XE, Gao LL. A clinical study on the premedication of paclitaxel liposome in the treatment of solid tumors. Biomed Pharmacother. 2009; 63:603–07. doi: 10.1016/j.biopha.2008.10.001.
18. Markman M, Kennedy A, Webster K, Peterson G, Kulp B, Belinson J. An effective and more convenient drug regimen for prophylaxis against paclitaxel-associated hypersensitivity reactions. J Cancer Res Clin Oncol. 1999; 125:427–29. doi: 10.1007/s004320050297.
19. Köppler H, Heymanns J, Weide R. Dose reduction of steroid premedication for paclitaxel: no increase of hypersensitivity reactions. Onkologie. 2001; 24:283–85.
20. Schwartz JR. Dexamethasone premedication for prophylaxis of taxane toxicities: can the doses be reduced when paclitaxel or docetaxel are given weekly? J Oncol Pharm Pract. 2012; 18:250–56. doi: 10.1177/1078155211409473.
21. Prieto García A, Pineda de la Losa F. Immunoglobulin E-mediated severe anaphylaxis to paclitaxel. J Investig Allergol Clin Immunol. 2010; 20:170–71.
22. Raisch DW, Campbell W, Garg V, Qureshi ZP, Bookstaver PB, Norris LB, Bennett CL. Description of anaphylactic reactions to paclitaxel and docetaxel reported to the FDA, with a focus on the role of premedication. Expert Opin Drug Saf. 2011; 10:521–28. doi: 10.1517/14740338.2011.582865.
23. Rutz HP. Effects of corticosteroid use on treatment of solid tumours. Lancet. 2002; 360:1969–70. doi: 10.1016/S0140-6736(02)11922-2.
24. Mahesh R, Perumal RV, Pandi PV. Cancer chemotherapy-induced nausea and vomiting: role of mediators, development of drugs and treatment methods. Pharmazie. 2005; 60:83–96.
25. Castro-Caldas M, Mendes AF, Carvalho AP, Duarte CB, Lopes MC. Dexamethasone prevents interleukin-1beta-induced nuclear factor-kappaB activation by upregulating IkappaB-alpha synthesis, in lymphoblastic cells. Mediators Inflamm. 2003; 12:37–46. doi: 10.1080/0962935031000096953.
26. Wang H, Li M, Rinehart JJ, Zhang R. Pretreatment with dexamethasone increases antitumor activity of carboplatin and gemcitabine in mice bearing human cancer xenografts: in vivo activity, pharmacokinetics, and clinical implications for cancer chemotherapy. Clin Cancer Res. 2004; 10:1633–44. doi: 10.1158/1078-0432.CCR-0829-3.
27. Wang H, Wang Y, Rayburn ER, Hill DL, Rinehart JJ, Zhang R. Dexamethasone as a chemosensitizer for breast cancer chemotherapy: potentiation of the antitumor activity of adriamycin, modulation of cytokine expression, and pharmacokinetics. Int J Oncol. 2007; 30:947–53.
28. Wershil BK, Furuta GT, Lavigne JA, Choudhury AR, Wang ZS, Galli SJ. Dexamethasone and cyclosporin A suppress mast cell-leukocyte cytokine cascades by multiple mechanisms. Int Arch Allergy Immunol. 1995; 107:323–24. doi: 10.1159/000237015.
29. Sau S, Banerjee R. Cationic lipid-conjugated dexamethasone as a selective antitumor agent. Eur J Med Chem. 2014; 83:433–47. doi: 10.1016/j.ejmech.2014.06.051.
30. Figueredo E, Cuesta-Herranz JI, De Las Heras M, Lluch-Bernal M, Umpierrez A, Sastre J. Anaphylaxis to dexamethasone. Allergy. 1997; 52:877. doi: 10.1111/j.1398-9995.1997.tb02166.x.
31. Wu W, Pew T, Zou M, Pang D, Conzen SD. Glucocorticoid receptor-induced MAPK phosphatase-1 (MPK-1) expression inhibits paclitaxel-associated MAPK activation and contributes to breast cancer cell survival. J Biol Chem. 2005; 280:4117–24. doi: 10.1074/jbc.M411200200.
32. Myers JS. Hypersensitivity reaction to paclitaxel: nursing interventions. Clin J Oncol Nurs. 2000; 4:161–63.
33. Griffin D, Parsons N, Shaw E, Kulikov Y, Hutchinson C, Thorogood M, Lamb SE, and UK Heel Fracture Trial Investigators. Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. BMJ. 2014; 349:g4483. doi: 10.1136/bmj.g4483.
34. Wells GA, Shea B. O’connellD, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses. Available: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.