
INTRODUCTION
Upper tract urothelial carcinoma (UTUC) is an uncommon but aggressive malignant disease that accounts for only 5% to 10% of all urothelial carcinomas [1]. The natural history and oncogenicity of UTUC appear to be rather different from that of urothelial carcinomas of the bladder. Around 50% of UTUCs are muscular invasive at diagnosis compared to only 15% of urothelial carcinomas of the bladder [2, 3]. Although radical nephroureterectomy (RNU) is the surgical standard for the treatment of patients with UTUC, the prognosis for patients who undergo RNU still remains poor. Currently, even after curative therapy, 5-year disease-specific survivals ranging between 50% and 80% have been reported [4, 5].
Pathological T stage, tumor grade, lymph node metastasis, distant metastasis, lymphovascular invasion (LVI) are well established pathological prognostic factors in patients with UTUC [1, 6–7]. Moreover, patient age and tumor multifocality are also independent predictors of patient survival [1, 8]. However, the potential prognostic preoperative factors are still limited in UTUC. Therefore, it is crucial to identify risk factors, which would allow for the assessment of individual risk profiles. The nutritional status of patients with cancer is an important parameter affecting survival outcomes [9, 10].
Pre-albumin, a visceral liver-synthesized protein, is a sensitive marker for determining the state of malnutrition and easily quantified in hospital laboratories. Study has shown that pre-albumin is a remarkable prognostic factor for treatment outcomes of esophagus [11], ovarian [12], and lung cancers [13, 14]. However, the prognostic value of plasma pre-albumin levels for urological cancer has not yet been reported.
Thus, this study was designed to clarify the potential prognostic value of preoperative pre-albumin and albumin level in a large number of patients who have undergone RNU for UTUC.
RESULTS
Clinical characteristics
Our final cohort included 279 men (65.6%) and 146 women (34.4%). Patients’ median age at surgery was 67.0 years (interquartile range (IQR), 58.0-75.0) (Table 1). Open RUN was performed in 281 patients (66.1%), while the remaining 144 patients (33.9%) underwent laparoscopic RUN, respectively. Pathological T stage was pTa-1 in 225 cases (52.9%), pT2 in 68 (16.0%), pT3 in 120 (28.2%) and pT4 in 12 (2.8%). Lymphadenectomy was done in 93 patients (21.8%) who presented with clinically enlarged lymph nodes. 86 patients received adjuvant chemotherapy (AC) in this study.
Table 1: Clinical and pathological characteristics of 425 UTUC patients stratified according to the presence of low pre-albumin level and hypoalbuminemia
Variables |
Pre-Albumin≥20mg/dl |
Pre-Albumin<20mg/dl |
P-value |
Albumin≥35g/L |
Albumin <35g/L |
P-value |
Age (years), median (IQR) |
67.0 (57.8-75.0) |
71.0 (60.0-77.0) |
0.040 |
67.0 (58.0-75.0) |
72.0 (61.0-77.0) |
0.231 |
Gender, n(%) |
0.090 |
1.000 |
||||
Male |
246(67.2) |
33(55.9) |
271(66.4) |
8(47.1) |
||
Female |
120(32.8) |
26(44.1) |
137(33.6) |
9(52.9) |
||
Hypertension |
0.702 |
0.488 |
||||
Yes |
121(33.1) |
21(35.6) |
135(33.1) |
7(41.2) |
||
No |
245(66.9) |
38(64.4) |
273(66.9) |
10(58.8) |
||
Diabetes mellitus |
0.049** |
0.012** |
||||
Yes |
41(11.2) |
12(20.3) |
47(11.5) |
6(35.3) |
||
No |
325(88.8) |
47(79.7) |
361(88.5) |
11(64.7) |
||
Location |
0.772 |
0.787 |
||||
Renal pelvic |
181(49.5) |
27(45.8) |
201(49.3) |
7(41.2) |
||
Ureteral |
118(32.2) |
19(32.2) |
131(32.1) |
6(35.3) |
||
Multifocal |
67(18.3) |
13(22.0) |
76(18.6) |
4(23.5) |
||
T stage |
0.021** |
0.137 |
||||
Ta-1 |
202(55.2) |
23(39.0) |
219(53.7) |
6(35.3) |
||
T2-4 |
164(44.8) |
36(61.0) |
189(46.3) |
11(64.7) |
||
Lymph node dissection |
0.033** |
0.381 |
||||
N0 |
62(16.9) |
7(11.9) |
67(16.4) |
2(11.8) |
||
N1-3 |
16(4.4) |
8(13.6) |
22(5.4) |
2(11.8) |
||
Nx |
288(78.7) |
44(74.6) |
319(78.2) |
13(76.5) |
||
WHO Grade |
0.150 |
0.154 |
||||
Low |
128(35.0) |
15(25.4) |
140(34.3) |
3(17.6) |
||
High |
238(65.0) |
44(74.6) |
268(65.7) |
14(82.4) |
||
LVI |
0.024** |
0.806 |
||||
Yes |
51(13.9) |
15(25.4) |
63(15.4) |
3(17.6) |
||
No |
315(86.1) |
44(74.6) |
345(84.6) |
14(82.4) |
||
Adjuvant Chemotherapy |
0.472 |
0.758 |
||||
No |
294(80.3) |
45(76.3) |
326(79.9) |
13(76.5) |
||
Yes |
72(19.7) |
14(23.7) |
82(20.1) |
4(23.5) |
Abbreviations: UTUC= Upper tract urothelial carcinoma; LVI= lymphovascular invasion.
Association with clinical and pathologic characteristics
The median preoperative pre-albumin, albumin was 27.2 mg/dL(IQR, 22.5-31.3) and 41.8 g/L (IQR, 39.6-44.1). Lower pre-albumin was significantly associated with older age, higher tumor stage (muscle invasive vs nonmuscle invasive), higher rate of diabetes, regional lymph node metastasis and LVI (all p<0.05**, Table 1), but not gender, tumor location and tumor grade. On the other hand, hypoalbuminemia was only significantly associated with diabetes (p<0.05**, Table 1).
Association with prognosis of UTUC
At a median follow-up period of 38.5 months (IQR, 23.0-62.0), low pre-albumin level was associated significantly with poor prognosis. In particular, the patients with preoperative low pre-albumin level had a significantly reduced rate of survival than those without low pre-albumin level with regard to CSS and OS (log-rank test, all P=0.001). The 5-year CSS rate was 54.9% in patients with low pre-albumin level and 75.5% in patients with normal pre-albumin level (Figure 1). Meanwhile the 5-year OS rate was 47.6% in patients with low pre-albumin level vs 68.8% in patients with normal pre-albumin level (Figure 2). Tables 2 and 3 show the results of the stepwise Cox survival analyses for predicting the CSS and OS, respectively. Multivariable analysis showed that low pre-albumin level (HR, 1.85;P=0.013) was an independent predictor of CSS, along with age greater than 65 (HR, 2.49; P<0.001), tumor multifocality (HR, 1.81; P=0.017), pT stage(HR, 3.08; P<0.001), grade(HR, 2.28; P=0.004), LVI(HR, 1.77;P=0.012), but hypoalbuminemia was not. As to OS, multivariable analysis also demonstrated that low pre-albumin level (HR, 1.73;P=0.015) was an independent predictor, along with age greater than 65 (HR, 3.03; P<0.001), tumor multifocality (HR, 1.85; P=0.007), pT stage (HR, 2.35; P<0.001), pN stage(HR, 1.94; P=0.029), grade(HR, 1.88; P=0.007), LVI(HR, 1.56;P=0.032), but hypoalbuminemia was not. The model with variables plus pre-albumin had higher c-index than the model with variables alone in CSS (0.775 vs. 0.771) and OS (0.765 vs. 0.760) in all patients.
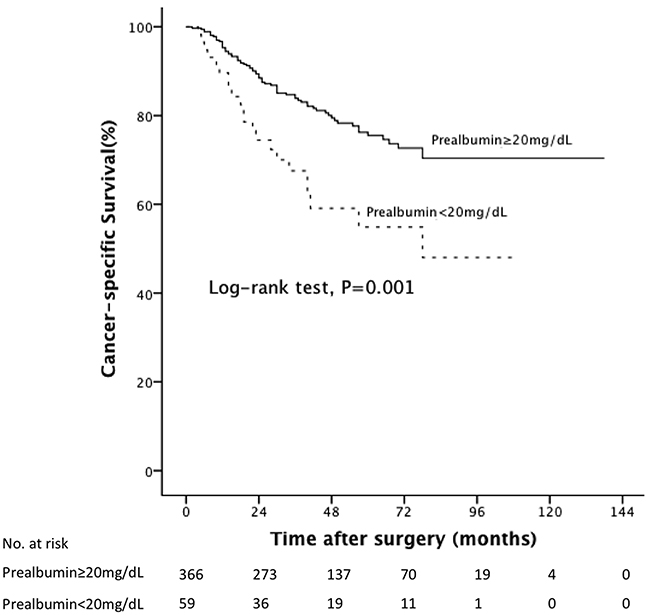
Figure 1: Kaplan-Meier curves predicting CSS by preoperative pre-albumin.
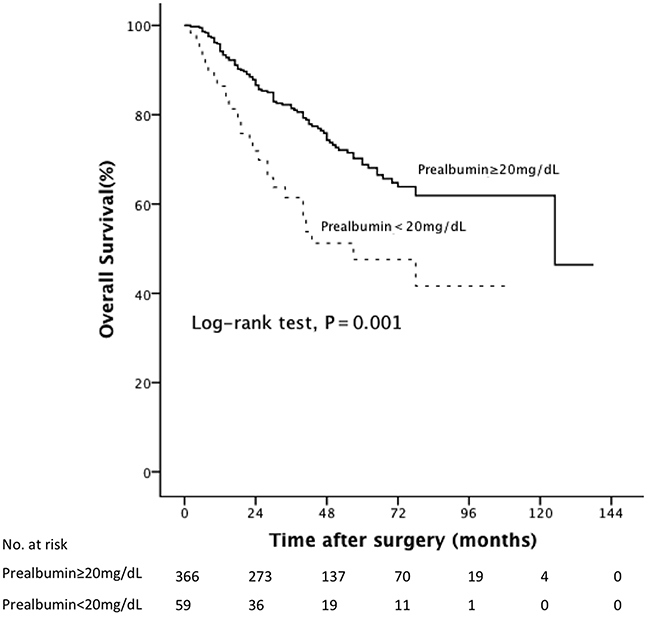
Figure 2: Kaplan-Meier curves predicting OS by preoperative pre-albumin.
Table 2: Univariable and multivariable Cox regression models to predict CSS in 425 patients treated with radical nephroureterectomy for UTUC
Variables |
Univariable Analysis |
Multvariable Analysis |
||
|---|---|---|---|---|
HR(95%CI) |
P-value |
HR(95%CI) |
P-value |
|
Age greater than 65 |
2.41(1.52-3.83) |
<0.001 |
2.49(1.56-3.97) |
<0.001 |
Gender(Female vs. Male) |
1.05(0.69-1.60) |
0.828 |
||
Hypertension(yes vs. no) |
1.17(0.77-1.78) |
0.468 |
||
Diabetes mellitus (yes vs. no) |
2.01(1.20-3.37) |
0.008 |
- |
- |
Multifocality(yes vs no) |
1.83(1.12-2.97) |
0.015 |
1.81(1.11-2.96) |
0.017 |
pTNM stage: |
||||
T(2-4vs a-1) |
4.36(2.70-7.02) |
<0.001 |
3.08(1.88-5.07) |
<0.001 |
N1-3 vs pNx/0 |
3.47(1.84-6.54) |
<0.001 |
- |
- |
Grade (High vs Low) |
3.48(2.03-5.96) |
<0.001 |
2.28(1.30-4.02) |
0.004 |
LVI(yes vs no) |
2.79(1.81-4.30) |
<0.001 |
1.77(1.13-2.76) |
0.012 |
Adjuvant Chemotherapy (yes vs no) |
1.64(1.03-2.61) |
0.037 |
- |
- |
pre-Albumin(<20mg/dL vs≥20mg/dL) |
2.18(1.35-3.51) |
0.001 |
1.85(1.14-3.00) |
0.013 |
Albumin(<35g/L vs≥35g/L ) |
2.51(1.22-5.18) |
0.013 |
- |
- |
Abbreviations: HR= hazard ratio; CI=confidence interval; UTUC= Upper tract urothelial carcinoma; LVI= lymphovascular invasion.
Table 3: Univariable and multivariable Cox regression models to predict OS in 425 patients treated with radical nephroureterectomy for UTUC
Variables |
Univariable Analysis |
Multvariable Analysis |
||
|---|---|---|---|---|
HR(95%CI) |
P-value |
HR(95%CI) |
P-value |
|
Age greater than 65 |
2.90(1.89-4.46) |
<0.001 |
3.03(1.97-4.68) |
<0.001 |
Gender(Female vs. Male) |
0.95(0.65-1.39) |
0.796 |
||
Hypertension(yes vs. no) |
1.11(0.76-1.61) |
0.600 |
||
Diabetes mellitus (yes vs. no) |
2.19(1.40-3.44) |
0.001 |
- |
- |
Multifocality(yes vs no) |
1.71(1.10-2.65) |
0.017 |
1.85(1.18-2.90) |
0.007 |
pTNM stage: |
||||
T(2-4vs a,1) |
3.25(2.20-4.82) |
<0.001 |
2.35(1.56-3.56) |
<0.001 |
N1-3 vs pNx/0 |
3.59(2.05-6.30) |
<0.001 |
1.94(1.07-3.53) |
0.029 |
Grade (High vs Low) |
2.65(1.71-4.10) |
<0.001 |
1.88(1.19-2.99) |
0.007 |
LVI(yes vs no) |
2.38(1.60-3.53) |
<0.001 |
1.56(1.04-2.35) |
0.032 |
Adjuvant Chemotherapy (yes vs no) |
1.28(0.82-1.98) |
0.280 |
||
Pre-Albumin(<20mg/dL vs≥20mg/dL) |
2.08(1.36-3.20) |
0.001 |
1.73(1.12-2.70) |
0.015 |
Albumin(<35g/L vs≥35g/L ) |
1.96(0.96-4.01) |
0.066 |
||
Abbreviations: HR= hazard ratio; CI=confidence interval; UTUC= Upper tract urothelial carcinoma; LVI= lymphovascular invasion.
DISCUSSION
In the present study, we investigated pre-albumin level, albumin level and other standard prognostic factors in 425 patients undergoing RNU for localized UTUC. Multivariate analysis showed that in addition to other well-established prognostic factors, preoperative pre-albumin level was an independent predictor of CSS and OS, but not hypoalbuminemia. To the best of our knowledge, this study was the first to investigate the prognostic impact of pre-albumin level in patients of urological cancer. Our study also showed that age greater than 65, tumor multifocality, pT stage, pN stage, grade, LVI were associated with survival outcomes, which is consistent with previous study [1].
Cancer-related malnutrition has a high incidence [15–17], and in patients with cancer, an impaired nutritional state has a negative impact on treatment outcomes, length of stay in hospital, prognosis and survival [9, 18]. It is well accepted that nutrition is an important determinant of immune responses and that malnutrition impairs the immune system, suppresses immune functions [19–22]. Furthermore, protein energy malnutrition is common in patients undergoing surgery and is associated with significant immunodeficiency, especially in the cell-mediated mechanisms, which is known to play a crucial role in the host defenses against infection or cancer [23].
Few studies have been conducted to determine the influence of perioperative nutritional status in the prognosis of UTUC patients [10, 24]. Kang et al. demonstrated that preoperative underweight (BMI<21.6 kg/m2) could significantly increase the rate of cancer-specific motility and overall mortality in UTUC patiets after RUN [24]. Ku et al. reported that preoperative hypoalbuminemia (albumin<3.5 g/dL) is an independent prognostic factor of CSS and OS in UTUC patients [10].
Pre-albumin is a visceral liver-synthesized protein, which is sensitive to determining malnutrition. Its biological half-life is approximately 2.5 days and is not altered by stress or acute inflammation [25]. Albumin has a half-life of 20 days and, as such, cannot be a suitable sensitive indicator of nutritional insufficiency [26]. So we hypothesize that the pre-albumin level may be a better indicator than albumin level for determining nutritional status and prognosis of UTUC. In our study, we found that in localized UTUC, the rate of low pre-albumin level (59/425,13.9%) was much higher than that of hypoalbuminemia (17/425, 4.0%). Also in the present series of patients with UTUC, those who had low pre-albumin level were more likely to have diabetes, higher T stage, N stage and lymphovascular invasion comparing with those with normal pre-albumin level. Meanwhile, hypoalbuminemia was only associated with diabetes in UTUC patients. These differences between patients with and without low pre-albumin level in terms of tumor characteristics may partly explain why the patients with low pre-albumin level in our cohort had more aggressive disease. In our multivariable analysis, low pre-albumin level was an independent predictor in UTUC patients but not hypoalbuminemia. The patients with low pre-albumin level had a 1.85-fold higher risk of dying of UTUC compared with those without low pre-albumin level.
Despite recent progress in the identification of genetic and molecular alterations in UTUC has been made [27], the most widely used routine prognostic assessment of UTUC currently still relies on traditional clinicopathological prognostic variables [28, 29]. The predictive accuracy of prognostic model might be improved by these biomarkers, but the high costs of analysis, the time-consuming preparation, and the lack of evidence together prevent them into clinical practice. In our study, we showed that adding pre-albumin was able to raise the predictive accuracy in this cohort of UTUC patients regarding to CSS and OS. The base model with traditional variables plus pre-albumin had higher c-index than the base model alone in CSS (0.775 vs. 0.771) and OS (0.765 vs. 0.760) in our cohort of patients. Because of the poor patient prognosis in UTUC, detailed understanding of individual risk factor associated with patients’ prognosis will impart benefits for outcome prediction and individual patient treatment choices, such as neoadjuvant chemotherapy and lymph node dissection. Thus we believe that the present results may add additional prognostic information to accurate assessment of individual risk profiles even before the surgery.
Limitations of this study include that the retrospective nature of the data collection and study completed at a single high-volume center. Additionally, we did not compare the pre-albumin with other nutritional tools.
MATERIALS AND METHODS
Patients
After institutional review board approval, the medical records from January 2003 to June 2013 archived at Renji Hospital were reviewed. During this period, 520 consecutive patients with nonmetastatic UTUC (Ta-4N0/+M0) underwent RNU at the department of urology at our institution. After excluding patients lost to follow-up within 3 months, patients without data on preoperative pre-albumin and albumin levels, patients with an active infection, patients with concomitant carcinoma invading bladder muscle and patients who underwent cisplatin-based neoadjuvant chemotherapy, there were 425 remaining patients who were included in the analyses.
Dissection of regional lymph nodes was performed in patients with lymph nodes enlarged in preoperative imaging. Pathological T stages were uniformly adjusted according to the 2009 TNM classification system [30] and tumor grade was assessed according to Tumor grading was assessed according to the 1998 WHO consensus classification [31]. We defined multifocal tumors as follows: the synchronous presence of two or more pathologically confirmed tumors in any location within the upper urinary tract [8]. Plasma pre-albumin and albumin levels were routinely measured 1 to 3 day before surgical intervention as a routine preoperative examination. Pre-albumin level was accessed by turbidimetric immuno-assay (Hitachi, Tokyo, Japan). The cutoff points to stratify pre-albumin and albumin were using pre-albumin <20 mg/dl to identify low pre-albumin, albumin <35 g/L to identify hypoalbuminemia [32]. AC would be offered as an option to patients with muscle invasive disease, lymph node positive disease, or pT1 disease with LVI, high grade disease or tumor multifocality after surgery. The patient would make a decision after the benefits and side effects of postoperative AC were explained by the treating urologist and oncologist together. The chemotherapy patients were administered 1000 mg/m2 gemcitabine on day 1, and 8 and 70 mg/m2 cisplatin on day 2 for the GC regimen. Cisplatin was replaced by carboplatin if the glomerular filtration rate was less than 40 ml/minute/1.73 m2. Four to 6 cycles of chemotherapy were planned according to patient status.
Patients were assessed by urine cytology and cystoscopy 3 months and every 6 months for 3 years after RNU and every 12 months thereafter. Computed tomography and/or magnetic resonance imaging were also performed every 6 months for 3 years and annually thereafter. CSS was defined as the time in months from the date of surgery to cancer related death. OS was defined as the time in months from the date of surgery to patient death from any cause.
The statistical software SPSS, v21.0 (IBM Corp., Armonk, NY, USA) was applied to all the analyses in this study. As to the clinicopathological outcomes according to the pre-albumin and albumin, for continuous variables, the Student t test was used for the variables reported as median (interquartile range (IQR)), for categorical variables, the chi-square and continuity corrected chi-square tests were used. The survival distributions were estimated by the Kaplan-Meier method and compared by a log-rank test. Univariable Cox proportional hazards models were used to address the relative impact of categorically coded low pre-albumin level, hypoalbuminemia, and other clinical and pathologic variables on CSS and OS. To prevent against overfitting by decreasing the number of variables, we selected only variables that were significant in univariable Cox models for the stepwise Cox regression analysis. Hazard ratio (HR) and 95% confidence interval (CI) were computed. The Harrell concordance index with variables only or combined pre-albumin data were used to evaluate the prognostic accuracy. All p values reported are two-sided, and p<0.05 was considered statistically significant.
ACKNOWLEDGMENTS AND GRANT SUPPORT
The design and conduct of the project was supported in part by Award Number 81402084, 81472378, 81672513 from National Natural Science Foundation of China, Award Number 2013SY027 from the Shanghai Municipal Commission of Health and Family Planning and Award Number PYXJS16-008 from the Incubating Program for Clinical Research and Innovation of Renji Hospital.
CONFLICTS OF INTEREST
The authors declare that they have no potential conflict of interest relevant to this article.
REFERENCES
1. Rouprêt M, Babjuk M, Compérat E, Zigeuner R, Sylvester RJ, Burger M, Cowan NC, Böhle A, Van Rhijn BW, Kaasinen E, Palou J, Shariat SF. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Cell Carcinoma: 2015 Update. Eur Urol. 2015; 68:868-879.
2. Catto JW, Yates DR, Rehman I, Azzouzi AR, Patterson J, Sibony M, Cussenot O, Hamdy FC. Behavior of urothelial carcinoma with respect to anatomical location. J Urol. 2007; 177: 1715-1720.
3. Green DA, Rink M, Xylinas E, Matin SF, Stenzl A, Roupret M, Karakiewicz PI, Scherr DS, Shariat SF. Urothelial carcinoma of the bladder and the upper tract: disparate twins. J Urol. 2013;189: 1214-1221.
4. Fairey AS, Kassouf W, Estey E, Tanguay S, Rendon R, Bell D, Izawa J, Chin J, Kapoor A, Matsumoto E, Black P, So A, Lattouf JB, et al. Comparison of oncological outcomes for open and laparoscopic radical nephroureterectomy: results from the Canadian Upper Tract Collaboration. BJU Int. 2013; 112:791-797.
5. Dalpiaz O, Pichler M, Mannweiler S, Martín Hernández JM, Stojakovic T, Pummer K, Zigeuner R, Hutterer GC. Validation of the pretreatment derived neutrophil-lymphocyte ratio as a prognostic factor in a European cohort of patients with upper tract urothelial carcinoma. Br J Cancer. 2014; 110:2531-2536.
6. Yates DR, Hupertan V, Colin P, Ouzzane A, Descazeaud A, Long JA, Pignot G, Crouzet S, Rozet F, Neuzillet Y, Soulie M, Bodin T, Valeri A, et al. French collaborative national database on UUT-UC. Cancer-specific survival after radical nephroureterectomy for upper urinary tract urothelial carcinoma: proposal and multi-institutional validation of a post-operative nomogram. Br J Cancer. 2012; 106:1083-1088.
7. Ku JH, Byun SS, Jeong H, Kwak C, Kim HH, Lee SE. Lymphovascular invasion as a prognostic factor in the upper urinary tract urothelial carcinoma: a systematic review and meta-analysis. Eur J Cancer. 2013; 49:2665-2680.
8. Chromecki TF, Cha EK, Fajkovic H, Margulis V, Novara G, Scherr DS, Lotan Y, Raman JD, Kassouf W, Bensalah K, Weizer A, Kikuchi E, Roscigno M, et al. The impact of tumor multifocality on outcomes in patients treated with radical nephroureterectomy. Eur Urol. 2012; 61:245-253.
9. Morgan TM, Tang D, Stratton KL, Barocas DA, Anderson CB, Gregg JR, Chang SS, Cookson MS, Herrell SD, Smith JA Jr, Clark PE. Preoperative nutritional status is an important predictor of survival in patients undergoing surgery for renal cell carcinoma. Eur Urol. 2011; 59:923-928.
10. Ku JH, Kim M, Choi WS, Kwak C, Kim HH. Preoperative serum albumin as a prognostic factor in patients with upper urinary tract urothelial carcinoma. Int Braz J Urol. 2014; 40:753-762.
11. Kelly P, Paulin F, Lamont D, Baker L, Clearly S, Exon D, Thompson A. Pre-treatment plasma proteomic markers associated with survival in oesophageal cancer. Br J Cancer. 2012; 106: 955-961.
12. Mählck CG, Grankvist K. Plasma prealbumin in women with epithelial ovarian carcinoma. Gynecol Obstet Invest. 1994; 37:135-140.
13. Alifano M, Mansuet-Lupo A, Lococo F, Roche N, Bobbio A, Canny E, Schussler O, Dermine H, Régnard JF, Burroni B, Goc J, Biton J, Ouakrim H, et al. Systemic inflammation, nutritional status and tumor immune microenvironment determine outcome of resected non-small cell lung cancer. PLoS One. 2014; 9:e106914.
14. Kawai H, Ota H. Low perioperative serum prealbumin predicts early recurrence after curative pulmonary resection for non-small-cell lung cancer. World J Surg. 2012; 36:2853-2857.
15. Bauer J, Capra S, Ferguson M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur J Clin Nutr. 2002; 56:779-785.
16. Daudt HM, Cosby C, Dennis DL, Payeur N, Nurullah R. Nutritional and psychosocial status of colorectal cancer patients referred to an outpatient oncology clinic. Support Care Cancer, 2011; 20: 1417-1423.
17. Leithold C, Jordan K, Jahn F, Behlendorf T, Schaffrath J, Müller-Tidow C, Rüssel J. Diagnostic work-up for the detection of malnutrition in hospitalized cancer patients. J Community Support Oncol. 2016; 14: 155-161.
18. Esfahani A, Ghoreishi Z, Abedi Miran M, Sanaat Z, Ostadrahimi A, Eivazi Ziaei J, Ghayour Nahand M, Asghari Jafarabadi M, Sorusheh Y, Esmaili H. Nutritional assessment of patients with acute leukemia during induction chemotherapy: association with hospital outcomes. Leuk Lymphoma. 2014; 55:1743-1750.
19. Chandra RK, Kumari S. Nutrition and immunity: an overview. J Nutr. 1994; 124:1433S-1435S.
20. Lesourd B. Protein undernutrition as the major cause of decreased immune function in the elderly: clinical and functional implications. Nutr Rev. 1995; 53:S86-S94.
21. Walrand S, Moreau K, Caldefie F, Tridon A, Chassagne J, Portefaix G, Cynober L, Beaufrère B, Vasson MP, Boirie Y. Specific and non-specific immune responses to fasting and refeeding differ in healthy young adult and elderly persons. Am J Clin Nutr. 2001; 74:670-678.
22. Marcos A, Nova E, Montero A. Changes in the immune system are conditioned by nutrition. Eur J Clin Nutr. 2003; 57:S66-S69.
23. Chandra RK. Nutrition and the immune system: an introduction. Am J Clin Nutr. 1997; 66:460S-463S.
24. Kang HW, Jung HD, Ha YS, Kim TH, Kwon TG, Byun SS, Yun SJ, Kim WJ, Choi Y. Preoperative Underweight Patients with Upper Tract Urothelial Carcinoma Survive Less after Radical Nephroureterectomy. J Korean Med. 2015; 30:1483-1489.
25. Myron Johnson A, Merlini G, Sheldon J, Ichihara K; Scientific Division Committee on Plasma Proteins (C-PP), International Federation of Clinical Chemistry and Laboratory Medicine (IFCC). Clinical indications for plasma protein assays: transthyretin (prealbumin) in inflammation and malnutrition. Clin Chem Lab Med. 2007; 45:419-426.
26. Gregg JR, Cookson MS, Phillips S, Salem S, Chang SS, Clark PE, Davis R, Stimson CJ Jr, Aghazadeh M, Smith JA Jr, Barocas DA. Effect of preoperative nutritional deficiency on mortality after radical cystectomy for bladder cancer. J Urol. 2011;185:90-96.
27. Li Q, Bagrodia A, Cha EK, Coleman JA. Prognostic Genetic Signatures in Upper Tract Urothelial Carcinoma. Curr Urol Rep. 2016; 17:12.
28. Jeldres C, Sun M, Lughezzani G, Isbarn H, Shariat SF, Widmer H, Graefen M, Montorsi F, Perrotte P, Karakiewicz PI. Highly predictive survival nomogram after upper urinary tract urothelial carcinoma. Cancer. 2010; 116: 3774-3784.
29. Rouprêt M, Hupertan V, Seisen T, Colin P, Xylinas E, Yates DR, Fajkovic H, Lotan Y, Raman JD, Zigeuner R, Remzi M, Bolenz C, Novara G, et al. Prediction of cancer specific survival after radical nephroureterectomy for upper tract urothelial carcinoma: development of an optimized postoperative nomogram using decision curve analysis. J Urol. 2013; 189:1662-1669.
30. Sobin LH, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumors. 7th ed. NJ: Wiley-Blackwell 2009.
31. Epstein JI, Amin MB, Reuter VR, Mostofi FK. The World Health Organization/International Society of Urological Pathology consensus classification of urothelial (transitional cell) neoplasms of the urinary bladder. Bladder Consensus Conference Committee. Am J Surg Pathol. 1998; 22: 1435-1448.
32. Grass F, Bertrand PC, Schäfer M, Ballabeni P, Cerantola Y, Demartines N, Hübner M. Compliance with preoperative oral nutritional supplements in patients at nutritional risk--only a question of will? Eur J Clin Nutr. 2015; 69:525-529.