
INTRODUCTION
Rheumatoid arthritis (RA) is an autoimmune inflammatory disease, which is characterized by chronic destructive inflammation in synovial joints. To date, the etiology of RA is poorly understood, but it is believed that complex genetic and environmental factors play important roles in the pathogenesis of RA [1]. Previous studies have suggested that genetic factors may be account for approximately 50–65% of the risk of RA [2]. Human leukocyte antigen (HLA) alleles are well recognized to be implicated in the pathogenesis of RA [3]. However, family studies indicated that HLA alleles contribute to about 30% of genetic susceptibility and that non-HLA loci are also related to RA [2, 4].
Tumor necrosis factor alpha inducible protein 3 (TNFAIP3), a deubiquitinating protein, is reported to play a pivotal role in T cell activation and inflammatory signaling [5]. It can deregulate NF-κB-dependent gene expression via deubiquitinating specific NF-κB signaling molecules [6]. Genome-wide association studies (GWASs) have identified TNFAIP3 gene as a common genetic risk factor for RA [7, 8]. A host of studies [7, 9–21] investigated the associations between TNFAIP3 gene rs10499194, rs13207033 polymorphisms and RA susceptibility, but with conflicting findings. However, these studies were conflicting and inconclusive due to clinical heterogeneity, different ethnic populations, and small sample sizes. In order to precisely elucidate the genetic roles for TNFAIP3 gene polymorphisms (rs10499194, rs13207033) in the development of RA, we performed a comprehensive meta-analysis of identified studies to clarify the possible association between TNFAIP3 gene rs10499194, rs13207033 polymorphisms and RA risk.
RESULTS
Characteristics of the included studies
We yielded a total of 251 citations after initial search. 77 citations were removed because of duplicates, and 141 citations were excluded after screening the titles and abstracts. 33 citations were selected for further full text review. 19 citations were excluded due to the following reasons: 9 investigated other polymorphisms; 4 citations did not provide detailed genotyping data; 2 were about juvenile idiopathic arthritis; 3 were reviews; and 1 was not case-control study. We finally identified 14 eligible citations [7, 9–21] including 17 studies (23,918 cases and 33,486 controls) in this meta-analysis. Selection for eligible studies included in this meta-analysis was presented in Figure 1. 6 studies with 11,166 cases and 11,231 controls examined rs13207033 polymorphism; 13 studies including 15,341 cases and 24,535 controls investigated rs10499194 polymorphism. The characteristics of included studies are summarized in Table 1. The Newcastle-Ottawa Scale (NOS) scores of all included studies ranged from 5 to 7 stars, suggesting that these studies were of high methodological quality.
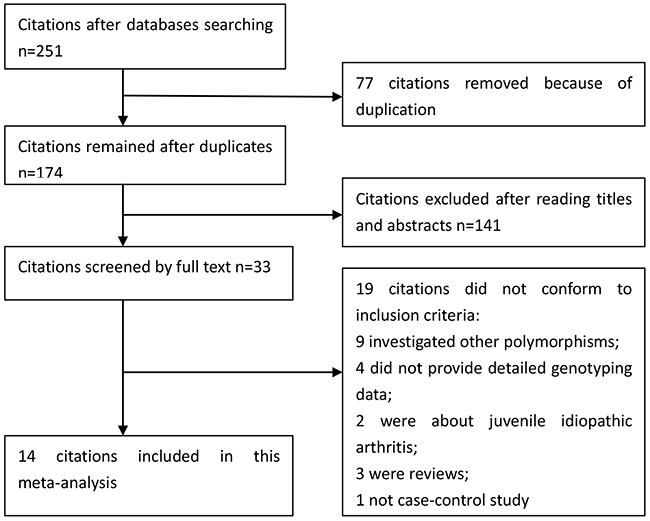
Figure 1: Selection for eligible publications included in this meta-analysis.
Table 1: Characteristics of included studies
Author and year |
Country |
Ethnicity |
Case |
Control |
HWE |
NOS |
||||
rs10499194 |
CC |
CT |
TT |
CC |
CT |
TT |
||||
Hegab_2016 |
Egypt |
Caucasian |
319 |
71 |
3 |
344 |
52 |
2 |
0.982 |
6 |
Zhang_2014 |
China |
Asian |
1156 |
12 |
4 |
1215 |
63 |
2 |
0.218 |
6 |
Hughes_2010 |
USA |
African-American |
374 |
164 |
18 |
558 |
213 |
20 |
0.951 |
7 |
Shimane_2010 |
Japan |
Asian |
2944 |
450 |
17 |
2049 |
243 |
7 |
0.943 |
6 |
Han_2009 |
Korea |
Asian |
1199 |
113 |
2 |
936 |
66 |
1 |
0.883 |
5 |
Coenen_2009 |
Dutch |
Caucasian |
790 |
499 |
79 |
972 |
614 |
97 |
0.998 |
7 |
Stark_2009 |
Slovakia |
Caucasian |
281 |
200 |
37 |
149 |
116 |
37 |
0.058 |
6 |
Perdigones_2009 |
Spain |
Caucasian |
305 |
275 |
46 |
306 |
287 |
70 |
0.824 |
6 |
Raychaudhuri_2008 |
Mixed |
Caucasian |
1353 |
1522 |
428 |
4636 |
5929 |
1895 |
0.993 |
7 |
Plenge_2007 |
USA |
Caucasian |
229 |
145 |
23 |
195 |
167 |
36 |
0.977 |
6 |
Plenge_2007 |
Sweden |
Caucasian |
560 |
280 |
35 |
519 |
276 |
37 |
0.968 |
6 |
Plenge_2007 |
North America |
Caucasian |
317 |
190 |
28 |
496 |
426 |
91 |
0.973 |
6 |
Plenge_2007 |
North America |
Caucasian |
491 |
327 |
55 |
673 |
604 |
136 |
0.977 |
6 |
rs13207033 |
GG |
GA |
AA |
GG |
GA |
AA |
||||
Zhang_2014 |
China |
Asian |
1040 |
232 |
8 |
1048 |
216 |
16 |
0.203 |
7 |
Han_2009 |
Korea |
Asian |
987 |
295 |
27 |
773 |
208 |
19 |
0.257 |
5 |
Maxwell_2012 |
UK |
Caucasian |
149 |
106 |
13 |
129 |
116 |
16 |
0.129 |
6 |
Orozco_2009 |
UK |
Caucasian |
2067 |
1403 |
224 |
1563 |
1237 |
229 |
0.464 |
7 |
Dieguez-Gonzalez_2009 |
Spain |
Caucasian |
825 |
684 |
142 |
800 |
676 |
143 |
0.991 |
6 |
Plant_2010 |
Mixed |
Caucasian |
1614 |
1148 |
202 |
2214 |
1555 |
273 |
0.999 |
6 |
HWE, Hardy–Weinberg equilibrium; NOS, Newcastle-Ottawa Scale
Meta-analysis of TNFAIP3 gene rs10499194, rs13207033 polymorphisms
In the overall analysis, we detected significant association (Table 2) between TNFAIP3 gene rs10499194, rs13207033 polymorphisms with decreased RA risk (rs10499194, TT vs. CT+CC: OR, 0.80; 95% CI, 0.74–0.88, P < 0.001, Figure 2; rs13207033, GA vs. GG: OR, 0.88; 95% CI, 0.79–0.99, P = 0.034, Figure 3). Stratification analyses were conducted according to ethnicity (Table 3). Our data indicated that rs10499194 polymorphism was also significantly associated with a decreased risk of RA among Caucasian populations (TT vs. CT+CC: OR, 0.79; 95% CI, 0.72–0.86, P < 0.001, Figure 4), but not among Asian and African-American populations. We also found rs13207033 polymorphism was weakly associated with a decreased risk of RA among Caucasian populations (GA vs. GG: OR, 0.88; 95% CI, 0.79–1.00, P = 0.044). All included studies conform to Hardy–Weinberg equilibrium (HWE), indicating control subjects were representative of the general population.
Table 2: Meta-analysis of association between TNFAIP3 rs10499194, rs13207033 polymorphisms and RA risk
Comparison |
OR(95%CI) |
P-value |
P for heterogeneity |
I2 (%) |
Model |
rs10499194 |
|||||
T vs. C |
0.91(0.81,1.02) |
0.097 |
<0.001 |
85.0 |
Random |
CT+TT vs. CC |
0.90(0.78,1.03) |
0.131 |
<0.001 |
84.9 |
Random |
TT vs. CT+CC |
0.80(0.74,0.88) |
<0.001 |
0.115 |
33.4 |
Fixed |
CT vs. CC |
0.92(0.80,1.06) |
0.239 |
<0.001 |
82.7 |
Random |
TT vs. CC |
0.75(0.62,0.90) |
0.002 |
0.026 |
48.4 |
Random |
rs13207033 |
|||||
A vs. G |
0.96(0.89,1.04) |
0.349 |
0.023 |
61.8 |
Random |
GA+AA vs. GG |
0.96(0.87,1.06) |
0.446 |
0.025 |
61.1 |
Random |
AA vs. GA+GG |
0.90(0.81,1.01) |
0.080 |
0.305 |
16.9 |
Fixed |
GA vs. GG |
0.88(0.79,0.99) |
0.034 |
0.146 |
39.0 |
Fixed |
AA vs. GG |
0.97(0.89,1.07) |
0.556 |
0.062 |
52.4 |
Random |
*Bold values are statistically significant (P < 0.05).
Table 3: Summary of the subgroup analyses in this meta-analysis
Comparison |
Category |
Category |
Studies |
OR (95% CI) |
P-value |
rs10499194 |
|||||
T vs. C |
Ethnicity |
Asian |
3 |
0.86(0.45,1.63) |
0.638 |
Caucasian |
9 |
0.86(0.78,0.94) |
0.001 |
||
African–American |
1 |
1.15(0.94,1.41) |
0.173 |
||
CT+TT vs. CC |
Ethnicity |
Asian |
3 |
0.81(0.40,1.65) |
0.561 |
Caucasian |
9 |
0.85(0.76,0.95) |
0.005 |
||
African–American |
1 |
1.17(0.92,1.47) |
0.200 |
||
TT vs. CT+CC |
Ethnicity |
Asian |
3 |
1.72(0.82,3.62) |
0.153 |
Caucasian |
9 |
0.79(0.72,0.86) |
<0.001 |
||
African–American |
1 |
1.29(0.68,2.46) |
0.440 |
||
CT vs. CC |
Ethnicity |
Asian |
3 |
0.75(0.35,1.61) |
0.467 |
Caucasian |
9 |
0.88(0.80,0.98) |
0.020 |
||
African–American |
1 |
1.15(0.90,1.46) |
0.262 |
||
TT vs. CC |
Ethnicity |
Asian |
3 |
1.75(0.83,3.68) |
0.141 |
Caucasian |
9 |
0.69(0.58,0.82) |
<0.001 |
||
African–American |
1 |
1.34(0.70,2.57) |
0.374 |
||
rs13207033 |
|||||
A vs. G |
Ethnicity |
Asian |
2 |
1.05(0.92,1.19) |
0.451 |
Caucasian |
4 |
0.93(0.85,1.03) |
0.170 |
||
GA+AA vs. GG |
Ethnicity |
Asian |
2 |
1.08(0.94,1.24) |
0.296 |
Caucasian |
4 |
0.92(0.82,1.04) |
0.174 |
||
AA vs. GA+GG |
Ethnicity |
Asian |
2 |
0.83(0.52,1.34) |
0.454 |
Caucasian |
4 |
0.91(0.81,1.02) |
0.105 |
||
GA vs. GG |
Ethnicity |
Asian |
2 |
0.85(0.53,1.37) |
0.505 |
Caucasian |
4 |
0.88(0.79,1.00) |
0.044 |
||
AA vs. GG |
Ethnicity |
Asian |
2 |
1.10(0.95,1.27) |
0.207 |
Caucasian |
4 |
0.93(0.84,1.03) |
0.187 |
||
*Bold values are statistically significant (P < 0.05)
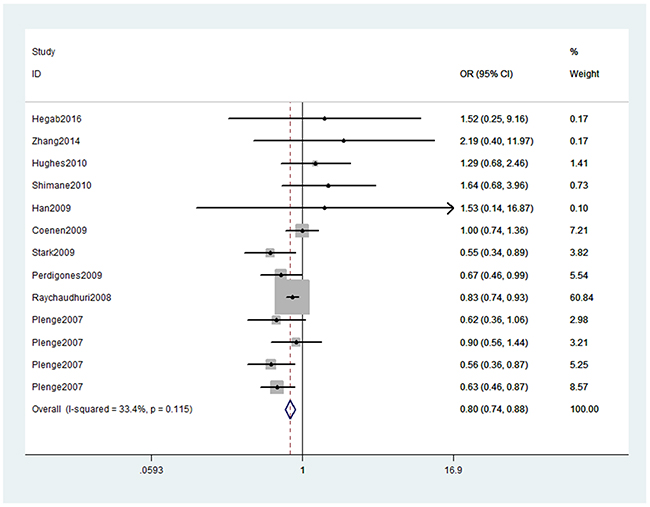
Figure 2: Forest plot shows odds ratio for the associations between rs10499194 polymorphism and RA risk (TT vs. CT+CC).
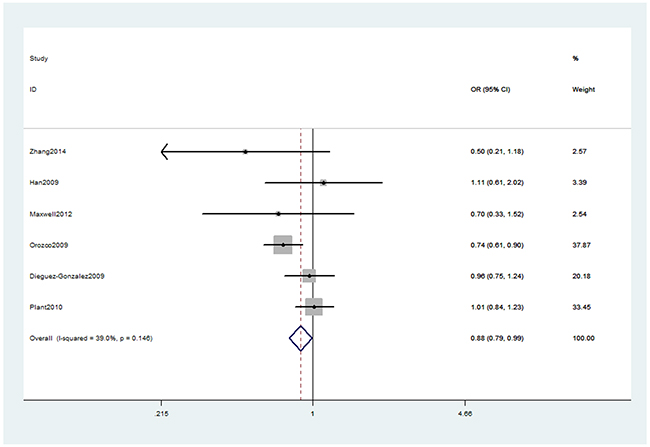
Figure 3: Forest plot shows odds ratio for the associations between rs13207033 polymorphism and RA risk (GA vs. GG).
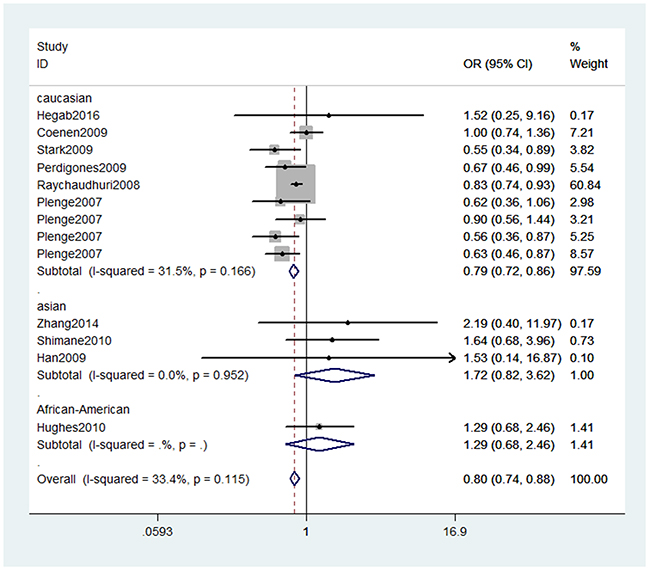
Figure 4: Stratification analyses of ethnicity between rs10499194 polymorphism and RA risk (TT vs. CT+CC).
We assessed sensitivity by omitting each study once at a time in every genetic model for rs10499194 and rs13207033 polymorphisms. The pooled ORs for the effects of these two single nucleotide polymorphisms (SNPs) (rs10499194, TT vs. CT+CC: Figure 5) on the risk for RA risk indicated that our data were stable and trustworthy. Both Egger’s and Begg’s tests (rs10499194: TT vs. CT+CC, Figure 6) were used to evaluated the publication bias of this meta-analysis. Our data revealed that there was no obvious publication bias for rs10499194 and rs13207033 polymorphisms (data not shown).
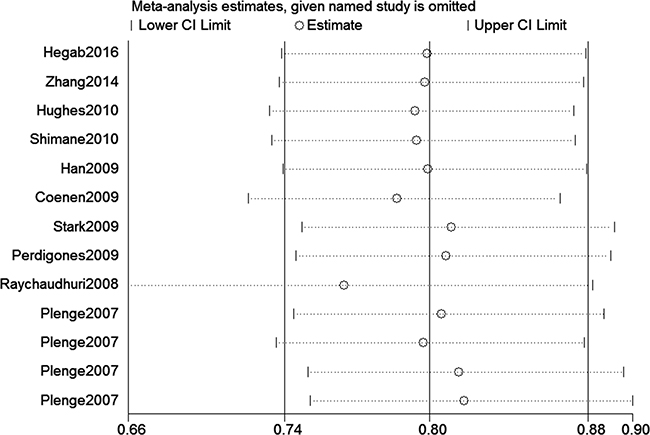
Figure 5: Sensitivity analyses between the rs10499194 polymorphism and RA risk (TT vs. CT+CC).
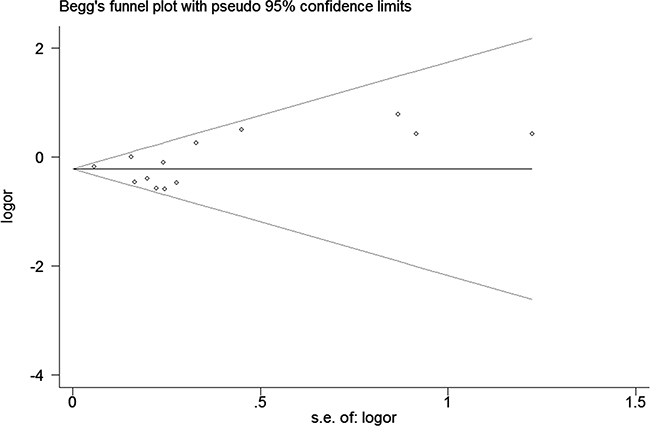
Figure 6: Begg’s tests between rs10499194 polymorphism and RA risk (TT vs. CT+CC).
DISCUSSION
In this current meta-analysis, we found that TNFAIP3 gene rs10499194, rs13207033 polymorphisms were associated with the decreased risk of RA. Stratification analyses of ethnicity indicated that rs10499194 and rs13207033 polymorphisms decreased the risk of RA among Caucasians, but not among Asians.
Studies have demonstrated that NF-κB-dependent gene expression is significantly associated with the development of RA [21]. TNFAIP3 is an inhibitor of the NF-κB signaling pathway and it is indispensable in the development of RA [22]. Defects in TNFAIP3 expression are associated with development of RA [23]. Matmati et al. indicated that TNFAIP3 deficiency in myeloid cells triggers erosive polyarthritis resembling RA [24]. They revealed a pivotal and cell-specific function for TNFAIP3 in the pathogenesis of RA [24]. Recently, a number of [7, 9–21] studies explored the associations between TNFAIP3 gene polymorphisms (rs10499194, rs13207033) and RA risk. However, these studies obtained inconsistent results. The limitations of these studies including clinical heterogeneity, different ethnic populations, inadequate statistical power, and small sample sizes may contribute to the disaccord. Therefore, to obtain reliable conclusions, it is indispensable to conduct a comprehensive meta-analysis to demonstrate the associations between TNFAIP3 gene rs10499194, rs13207033 polymorphisms and RA susceptibility. Our data indicated that TNFAIP3 gene rs10499194 and rs13207033 polymorphisms decreased the risk of RA.
Previously, Lee et al. also performed a meta-analysis to investigate TNFAIP3 gene rs10499194 polymorphism with RA susceptibility [25]. They indicated that rs10499194 polymorphism was not associated with RA susceptibility [25]. Stratification analyses of ethnicity in their meta-analysis [25] suggested that rs10499194 polymorphism was weakly associated with an increased risk of RA among Asian populations, while no association was observed among Caucasian populations. However, our meta-analysis found that rs10499194 polymorphism was significantly associated with a decreased risk of RA among Caucasian populations, but not among Asian populations, indicating that diversity inheritance of different ethnicities. The reasons why the decreased risk of RA among Asians is not obvious are still unclear. The clinical heterogeneity, different ethnicities and small sample sizes may explain it. We think previous meta-analysis [25] conducted by Lee et al. had several limitations. First, Lee et al. did not include two studies [7, 16] which actually conformed to the inclusion criteria. Second, they identified a Spanish study [10] by Dieguez-Gonzalez et al., but we did not find the genotype numbers of rs10499194 polymorphism. Three, previous research indicated that searching one or two databases was insufficient for meta-analysis of case-control studies [26]. Lee et al. conducted a literature search only in the database of MEDLINE, but omitting Embase and other databases. Consequently, the reliability of their conclusions should be interpreted with caution. Due to these above limitations of previous meta-analysis, we re-conducted this meta-analysis. We believe our meta-analysis has some strength over previous meta-analysis for the following reasons. One, we identified 13 studies [7, 9, 11–13, 16, 18–21], including 15,341 cases and 24,535 controls with regard to rs10499194 polymorphism and the sample size of this meta-analysis was large enough. Two, sensitivity analysis indicated that our data about rs10499194 polymorphism were trustworthy and robust. Three, the power analysis indicated that our study had a power of 99.9% to detect the effect of rs10499194 polymorphism on RA susceptibility, assuming an OR of 0.80.
Regarding TNFAIP3 gene rs13207033 polymorphism, six studies explored the association between this SNP and RA risk. A study from UK [15] found rs13207033 polymorphism was significantly associated with a decreased risk of RA, but the remaining five studies [10, 11, 14, 17, 21] did not replicate the association. Therefore, we conducted the meta-analysis to demonstrate this SNP with RA risk. To our knowledge, this is the first meta-analysis to address the association between this SNP and RA risk. A weak association was obtained about rs13207033 polymorphism in our study. Stratification analyses by ethnicity also found a weak association between rs13207033 polymorphism and Caucasian RA risk.
Several potential limitations should be addressed in this meta-analysis. First, due to limited data, we could not perform further stratification analyses of other potential factors, such as anti-citrullinated peptide antibody (ACPA) and rheumatoid factor (RF). Second, our results were based on unadjusted estimates for confounding factors, which might have affected the final conclusions. Third, we could not assess potential gene-gene and gene-environment interactions because of the lack of relevant data. Fourth, the heterogeneity of this meta-analysis was high in some genetic models. Fifth, the conclusions about rs10499194 polymorphism among Asians should be interpreted with caution due to limited sample size.
In conclusion, this meta-analysis indicates that TNFAIP3 gene rs10499194, rs13207033 polymorphisms are associated with the decreased risk of RA, especially among Caucasians. Further studies are necessary to validate whether TNFAIP3 gene rs10499194, rs13207033 polymorphisms contribute to RA susceptibility in other ethnic groups.
MATERIALS AND METHODS
Literature search and criteria of inclusion
We systematically searched the PubMed, Embase, and China Knowledge Resource Integrated Database to identify studies through July 26, 2016. The following search terms were used: “tumor necrosis factor alpha inducible protein 3,” ‘‘TNFAIP3,’’ ‘‘A20,’’ ‘‘Rheumatoid Arthritis,’’ ‘‘RA,’’ ‘‘polymorphism,’’ ‘‘SNP’’ and ‘‘polymorphisms’’. No restrictions were placed on the search. Additional initially omitted studies (such as reference lists of identified studies) have been identified by hand screening. The identified studies conformed to the following criteria: (1) studies that evaluated the association between RA risk and TNFAIP3 gene rs10499194 or rs13207033 polymorphism, (2) studied on human beings, (3) study provided sufficient data to calculate the odds ratios (ORs) and 95% confidence intervals (CIs), and P value, and (4) case-control study.
Data extraction and quality assessment
Relevant information was carefully extracted from all eligible studies. The extracted information from all eligible studies including: name of first author, publication year, country of origin, ethnicity, and genotype numbers of cases and controls. Two reviewers independently performed the extraction of data and assessed the study quality based on the NOS [27]. All disagreements were discussed and resolved with consensus.
Statistical analysis
All statistical analyses were performed using the Stata 11.0 software (StataCorp, College Station, TX, USA). ORs and 95%CIs were used to assess the strength of associations between TNFAIP3 gene rs10499194, rs13207033 polymorphisms and RA risk. Stratification analysis was carried out by ethnicity. P < 0.05 was considered statistically significant. When a Q test indicated P < 0.1 or I2 > 50% indicated heterogeneity across studies, a random-effect model was used. Otherwise, the fixed-effects model was applied [28]. Pooled ORs were calculated for allele model, dominant model, recessive model, homozygous model, and heterozygous model. We performed sensitivity analyses by omitting each study in turn to determine the effect on the test of heterogeneity and evaluated the stability of the overall results. We assessed the departure from the HWE in the controls using Pearson’s χ2 test. Potential publication bias was assessed by Begger’s and Egger’s linear regression test [29]; P < 0.05 was considered to indicate statistically significant. The power of this meta-analysis was calculated with a significant value of 0.05 [30].
Abbreviations
RA, rheumatoid arthritis; TNFAIP3, tumor necrosis factor alpha inducible protein 3; HLA, Human leukocyte antigen; CI, confidence interval; OR, odds ratio; NOS, Newcastle-Ottawa Scale; HWE, Hardy–Weinberg equilibrium; SNP, single nucleotide polymorphism
ACKNOWLEDGMENTS
This study was supported by National Natural Science Foundation of China, No. 81371927.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
REFERENCES
1. Smolen JS, Aletaha D and McInnes IB. Rheumatoid arthritis. Lancet. 2016.
2. MacGregor AJ, Snieder H, Rigby AS, Koskenvuo M, Kaprio J, Aho K and Silman AJ. Characterizing the quantitative genetic contribution to rheumatoid arthritis using data from twins. Arthritis and rheumatism. 2000; 43:30-37.
3. Kurko J, Besenyei T, Laki J, Glant TT, Mikecz K and Szekanecz Z. Genetics of rheumatoid arthritis - a comprehensive review. Clinical reviews in allergy & immunology. 2013; 45:170-179.
4. Klareskog L, Catrina AI and Paget S. Rheumatoid arthritis. Lancet. 2009; 373:659-672.
5. Elsby LM, Orozco G, Denton J, Worthington J, Ray DW and Donn RP. Functional evaluation of TNFAIP3 (A20) in rheumatoid arthritis. Clinical and experimental rheumatology. 2010; 28:708-714.
6. Wertz IE, O’Rourke KM, Zhou H, Eby M, Aravind L, Seshagiri S, Wu P, Wiesmann C, Baker R, Boone DL, Ma A, Koonin EV and Dixit VM. De-ubiquitination and ubiquitin ligase domains of A20 downregulate NF-kappaB signalling. Nature. 2004; 430:694-699.
7. Plenge RM, Cotsapas C, Davies L, Price AL, de Bakker PI, Maller J, Pe’er I, Burtt NP, Blumenstiel B, DeFelice M, Parkin M, Barry R, Winslow W, Healy C, Graham RR, Neale BM, et al. Two independent alleles at 6q23 associated with risk of rheumatoid arthritis. Nature genetics. 2007; 39:1477-1482.
8. Thomson W, Barton A, Ke X, Eyre S, Hinks A, Bowes J, Donn R, Symmons D, Hider S, Bruce IN, Wellcome Trust Case Control C, Wilson AG, Marinou I, Morgan A, Emery P, Consortium Y, et al. Rheumatoid arthritis association at 6q23. Nature genetics. 2007; 39:1431-1433.
9. Coenen MJ, Trynka G, Heskamp S, Franke B, van Diemen CC, Smolonska J, van Leeuwen M, Brouwer E, Boezen MH, Postma DS, Platteel M, Zanen P, Lammers JW, Groen HJ, Mali WP, Mulder CJ, et al. Common and different genetic background for rheumatoid arthritis and coeliac disease. Human molecular genetics. 2009; 18:4195-4203.
10. Dieguez-Gonzalez R, Calaza M, Perez-Pampin E, Balsa A, Blanco FJ, Canete JD, Caliz R, Carreno L, de la Serna AR, Fernandez-Gutierrez B, Ortiz AM, Herrero-Beaumont G, Pablos JL, Narvaez J, Navarro F, Marenco JL, et al. Analysis of TNFAIP3, a feedback inhibitor of nuclear factor-kappaB and the neighbor intergenic 6q23 region in rheumatoid arthritis susceptibility. Arthritis research & therapy. 2009; 11:R42.
11. Han TU, Bang SY, Kang C and Bae SC. TRAF1 polymorphisms associated with rheumatoid arthritis susceptibility in Asians and in Caucasians. Arthritis and rheumatism. 2009; 60:2577-2584.
12. Hegab MM, Abdelwahab AF, El-Sayed Yousef AM, Salem MN, El-Baz W, Abdelrhman S, Elshabacy F, Alhefny A, Abouraya W, Ibrahim SM and Ragab G. CD28 and PTPN22 are associated with susceptibility to rheumatoid arthritis in Egyptians. Human immunology. 2016; 77:522-526.
13. Hughes LB, Reynolds RJ, Brown EE, Kelley JM, Thomson B, Conn DL, Jonas BL, Westfall AO, Padilla MA, Callahan LF, Smith EA, Brasington RD, Edberg JC, Kimberly RP, Moreland LW, Plenge RM, et al. Most common single-nucleotide polymorphisms associated with rheumatoid arthritis in persons of European ancestry confer risk of rheumatoid arthritis in African Americans. Arthritis and rheumatism. 2010; 62:3547-3553.
14. Maxwell JR, Gowers IR, Kuet KP, Barton A, Worthington J and Wilson AG. Expression of the autoimmunity associated TNFAIP3 is increased in rheumatoid arthritis but does not differ according to genotype at 6q23. Rheumatology. 2012; 51:1514-1515.
15. Orozco G, Hinks A, Eyre S, Ke X, Gibbons LJ, Bowes J, Flynn E, Martin P, Wellcome Trust Case Control C, consortium Y, Wilson AG, Bax DE, Morgan AW, Emery P, Steer S, Hocking L, et al. Combined effects of three independent SNPs greatly increase the risk estimate for RA at 6q23. Human molecular genetics. 2009; 18:2693-2699.
16. Perdigones N, Lamas JR, Vigo AG, de la Concha EG, Jover JA, Urcelay E, Gutierrez BF and Martinez A. 6q23 polymorphisms in rheumatoid arthritis Spanish patients. Rheumatology. 2009; 48:618-621.
17. Plant D, Flynn E, Mbarek H, Dieude P, Cornelis F, Arlestig L, Dahlqvist SR, Goulielmos G, Boumpas DT, Sidiropoulos P, Johansen JS, Ornbjerg LM, Hetland ML, Klareskog L, Filer A, Buckley CD, et al. Investigation of potential non-HLA rheumatoid arthritis susceptibility loci in a European cohort increases the evidence for nine markers. Annals of the rheumatic diseases. 2010; 69:1548-1553.
18. Raychaudhuri S, Remmers EF, Lee AT, Hackett R, Guiducci C, Burtt NP, Gianniny L, Korman BD, Padyukov L, Kurreeman FA, Chang M, Catanese JJ, Ding B, Wong S, van der Helm-van Mil AH, Neale BM, et al. Common variants at CD40 and other loci confer risk of rheumatoid arthritis. Nature genetics. 2008; 40:1216-1223.
19. Shimane K, Kochi Y, Horita T, Ikari K, Amano H, Hirakata M, Okamoto A, Yamada R, Myouzen K, Suzuki A, Kubo M, Atsumi T, Koike T, Takasaki Y, Momohara S, Yamanaka H, et al. The association of a nonsynonymous single-nucleotide polymorphism in TNFAIP3 with systemic lupus erythematosus and rheumatoid arthritis in the Japanese population. Arthritis and rheumatism. 2010; 62:574-579.
20. Stark K, Rovensky J, Blazickova S, Grosse-Wilde H, Ferencik S, Hengstenberg C and Straub RH. Association of common polymorphisms in known susceptibility genes with rheumatoid arthritis in a Slovak population using osteoarthritis patients as controls. Arthritis research & therapy. 2009; 11:R70.
21. Zhang X, Li W, Zhang X, Zhao L, Zhang X, Jiang L, Guo Y, Zhang J, Liang Z and Wang X. Single nucleotide polymorphisms in TNFAIP3 were associated with the risks of rheumatoid arthritis in northern Chinese Han population. BMC medical genetics. 2014; 15:56.
22. Lee EG, Boone DL, Chai S, Libby SL, Chien M, Lodolce JP and Ma A. Failure to regulate TNF-induced NF-kappaB and cell death responses in A20-deficient mice. Science. 2000; 289:2350-2354.
23. Vereecke L, Beyaert R and van Loo G. The ubiquitin-editing enzyme A20 (TNFAIP3) is a central regulator of immunopathology. Trends in immunology. 2009; 30:383-391.
24. Matmati M, Jacques P, Maelfait J, Verheugen E, Kool M, Sze M, Geboes L, Louagie E, Mc Guire C, Vereecke L, Chu Y, Boon L, Staelens S, Matthys P, Lambrecht BN, Schmidt-Supprian M, et al. A20 (TNFAIP3) deficiency in myeloid cells triggers erosive polyarthritis resembling rheumatoid arthritis. Nature genetics. 2011; 43:908-912.
25. Lee YH, Bae SC, Choi SJ, Ji JD and Song GG. Associations between TNFAIP3 gene polymorphisms and rheumatoid arthritis: a meta-analysis. Inflammation research. 2012; 61:635-641.
26. Lemeshow AR, Blum RE, Berlin JA, Stoto MA and Colditz GA. Searching one or two databases was insufficient for meta-analysis of observational studies. Journal of clinical epidemiology. 2005; 58:867-873.
27. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. European journal of epidemiology. 2010; 25:603-605.
28. Higgins JP and Thompson SG. Quantifying heterogeneity in a meta-analysis. Statistics in medicine. 2002; 21:1539-1558.
29. Peters JL, Sutton AJ, Jones DR, Abrams KR and Rushton L. Comparison of two methods to detect publication bias in meta-analysis. Jama. 2006; 295:676-680.
30. Hedges LV and Pigott TD. The power of statistical tests in meta-analysis. Psychological methods. 2001; 6:203-217.