
INTRODUCTION
Numerous epidemiological studies have indicated that tobacco smoking is the most crucial risk factor for chronic obstructive pulmonary disease (COPD) [1–6]. A considerably high prevalence of smoking has been reported among patients with COPD (approximately 54%–77% in patients with mild COPD and 38%–51% in patients with severe COPD) [7–10]. A 25-year follow-up study based on general population data from the Danish Death Register reported that 92% of patients who died from COPD had a regular smoking habit at the beginning of follow up, regardless of the timing of smoking cessation [2].
Smoking is associated with increased colon cancer incidence and mortality. A meta-analysis of 106 observational studies reported that the risk of colon cancer was higher among cigarette smokers than among those who never smoked [relative risk =1.18, 95% confidence interval (CI) = 1.11, 1.25] [11]. In addition, cigarette smoking is a risk factor for essentially all colonic polyps. Regarding adenomatous polyps, the risk is particularly high for advanced adenomas (i.e., large adenomas and those with dysplastic features) [12]. Moreover, smoking is a major risk factor for serrated polyps of the colon, including those that are hyperplastic and adenomatous [13–16]. In addition, smoking may increase the risk of colon cancer in patients with Lynch syndrome (i.e., hereditary nonpolyposis colorectal cancer) [17]. Therefore, most COPD patients with smoking habits may have a relatively increased risk of colon cancer compared with the general population.
Our previous observational study reported that statin use may reduce the overall risk of cancer and those of specific cancers [18]. The possible mechanisms underlying the decreased risk of cancer with statin use include the inhibition of downstream products of the mevalonate pathway [19–22], activation of tumor-specific apoptosis [23], and inhibition of the proteasome pathway [24]. Observational studies have suggested that statins have a protective effect against several cancers including colon cancer; however, the overall data are conflicting [25–29]. A modest reduction in the incidence of colon cancer, as a secondary endpoint, was observed in two large-scale clinical trials evaluating the benefits of pravastatin and simvastatin in coronary artery disease [30, 31].
The present study is the first to evaluate the incidence of colon cancer in patients with COPD and identify the statin type that most favorably reduces colon cancer risk in these patients.
RESULTS
The COPD cohort comprised 43,802 patients: 10,086 (23%) used statins, whereas 33,716 (77%) did not (Table 1). The total follow-up duration was 194,933.6 and 80,239.4 person-years for statin users and nonusers, respectively (Table 2). The prevalence of preexisting medical comorbidities, namely diabetes (P < 0.001), hypertension (P < 0.001), and dyslipidemia (P < 0.001), and CCI (P < 0.001) was higher in the statin users than in the statin nonusers. In addition, significant differences were observed in the distribution of age; monthly income; urbanization level; and nonstatin lipid-lowering drug, aspirin, ACEI, and metformin use between statin and statin nonusers (Table 1). A higher proportion of statin nonusers used nonstatin lipid-lowering drugs, metformin, ACEI, and aspirin at ≥28 cDDDs, whereas most statin users used these drugs at <28 cDDDs. A higher proportion of statin users had a monthly income of NT$21,000–NT$33,300 or ≥NT$33,301 and resided in urban areas. Moreover, a larger proportion of statin users were women and elderly patients. Table 2 presents the colon cancer risk among the statin users and nonusers. After adjustment for age, sex, CCI, diabetes, hypertension, dyslipidemia, urbanization level, and monthly income in the PS analysis, we analyzed the colon cancer risk. Compared with the statin nonusers, the adjusted HRs (aHRs) of colon cancer decreased in the statin users (aHRs = 0.52, 95% CI = 0.44, 0.62). The stratified analysis revealed that the aHRs remained significantly decreased in the statin users, particularly in those aged 40–64 and ≥75 years, regardless of sex. Compared with the statin nonusers, the aHRs of colon cancer decreased in the statin users aged 40–64, 65–74, and ≥75 years (aHRs = 0.47, 0.54, and 0.48, respectively). After sex stratification, the aHR of colon cancer was lower in the statin users than in the statin nonusers (women: aHR = 0.55, 95% CI = 0.42, 0.72; men: aHR = 0.49, 95% CI = 0.39, 0.63). The effect of the reduced colon cancer risk was more predominant in the male statin users with COPD.
Table 1: Characteristic of the sample population
Whole cohort |
Patients with statin use (≥28 cDDD ; n=10086) |
Patients without statin use (<28 cDDD ; n=33716) |
Pa |
||||
|---|---|---|---|---|---|---|---|
n |
% |
n |
% |
n |
% |
||
Age, years (Mean ± SD) |
62.92 (13.18) |
61.55 (10.97) |
63.33 (13.74) |
<0.001 |
|||
40-54 |
14458 |
33.01 |
3180 |
31.53 |
11278 |
33.45 |
<0.001 |
55-64 |
9644 |
22.02 |
2899 |
28.74 |
6745 |
20.01 |
|
65-74 |
10455 |
23.87 |
2777 |
27.53 |
7678 |
22.77 |
|
≥75 |
9245 |
21.11 |
1230 |
12.20 |
8015 |
23.77 |
|
Gender |
|||||||
Female |
19715 |
45.01 |
5150 |
51.06 |
14565 |
43.20 |
<0.001 |
Male |
24087 |
54.99 |
4936 |
48.94 |
19151 |
56.80 |
|
CCI Index+ |
|||||||
0 |
11279 |
25.75 |
2586 |
25.64 |
8693 |
25.78 |
<0.001 |
1 |
12597 |
28.76 |
3014 |
29.88 |
9583 |
28.42 |
|
2 |
9075 |
20.72 |
2195 |
21.76 |
6880 |
20.41 |
|
≥3 |
10851 |
24.77 |
2291 |
22.71 |
8560 |
25.39 |
|
Diabetes |
|||||||
No |
33491 |
76.46 |
6819 |
67.61 |
26672 |
79.11 |
<0.001 |
Yes |
10311 |
23.54 |
3267 |
32.39 |
7044 |
20.89 |
|
Hypertension |
|||||||
No |
22067 |
50.38 |
4158 |
41.23 |
17909 |
53.12 |
<0.001 |
Yes |
21735 |
49.62 |
5928 |
58.77 |
15807 |
46.88 |
|
Dyslipidemia |
|||||||
No |
31731 |
72.44 |
5785 |
57.36 |
25946 |
76.95 |
<0.001 |
Yes |
12071 |
27.56 |
4301 |
42.64 |
7770 |
23.05 |
|
Nonstatin lipid-lowering drugs |
|||||||
<28 cDDDs |
39267 |
89.65 |
7212 |
71.51 |
32055 |
95.07 |
<0.001 |
28-365 cDDDs |
3186 |
7.27 |
1923 |
19.07 |
1263 |
3.75 |
|
>365 cDDDs |
1349 |
3.08 |
951 |
9.43 |
398 |
1.18 |
|
Metformin |
|||||||
<28 cDDDs |
35961 |
82.10 |
6286 |
62.32 |
29675 |
88.01 |
<0.001 |
28-365 cDDDs |
2684 |
6.13 |
964 |
9.56 |
1720 |
5.10 |
|
>365 cDDDs |
5157 |
11.77 |
2836 |
28.12 |
2321 |
6.88 |
|
ACEI |
|||||||
<28 cDDDs |
23928 |
54.63 |
3066 |
30.40 |
20862 |
61.88 |
<0.001 |
28-365 cDDDs |
7925 |
18.09 |
1928 |
19.12 |
5997 |
17.79 |
|
>365 cDDDs |
11949 |
27.28 |
5092 |
50.49 |
6857 |
20.34 |
|
Aspirin |
|||||||
<28 cDDDs |
28319 |
64.65 |
4161 |
41.26 |
24158 |
71.65 |
<0.001 |
28-365 cDDDs |
7385 |
16.86 |
2296 |
22.76 |
5089 |
15.09 |
|
>365 cDDDs |
8098 |
18.49 |
3629 |
35.98 |
4469 |
13.25 |
|
Level of Urbanization |
|||||||
Urban |
30539 |
69.72 |
7208 |
71.47 |
23331 |
69.20 |
<0.001 |
Suburban |
8914 |
20.35 |
1920 |
19.04 |
6994 |
20.74 |
|
Rural |
4349 |
9.93 |
958 |
9.50 |
3391 |
10.06 |
|
Monthly income (NT$) |
|||||||
0 |
3464 |
7.91 |
795 |
7.88 |
2669 |
7.92 |
<0.001 |
1-21000 |
15001 |
34.25 |
3067 |
30.41 |
11934 |
35.40 |
|
21000-33300 |
12904 |
29.46 |
3165 |
31.38 |
9739 |
28.89 |
|
≥33301 |
12433 |
28.38 |
3059 |
30.33 |
9374 |
27.80 |
|
a Comparison between statins use and statin nonusers
+CCI Index: Charlson Comorbidity Index
Table 2: Risk of colon cancer among statin and non-statin in study cohort
All Group |
Patients without statin use |
Patients with statin use |
Adjusted HR† |
||||
|---|---|---|---|---|---|---|---|
No. of |
Incidence rate |
No. of |
Incidence rate |
||||
Whole cohort |
|||||||
Colon Cancer |
783 |
401.7 |
(373.5, 429.8) |
163 |
203.1 |
(172.0, 234.3) |
0.52(0.44, 0.62)*** |
Age, 40-64a |
|||||||
Colon Cancer |
304 |
261.6 |
(232.2, 291.0) |
73 |
144.6 |
(111.4, 177.8) |
0.47(0.36, 0.62)*** |
Age, 65-74b |
|||||||
Colon Cancer |
261 |
585.0 |
(514.1, 656.0) |
66 |
303.1 |
(229.9, 376.2) |
0.54(0.41, 0.72)*** |
Age, ≥75c |
|||||||
Colon Cancer |
218 |
639.4 |
(554.6, 724.3) |
24 |
300.6 |
(180.3, 420.8) |
0.48(0.31, 0.74)*** |
Femaled |
|||||||
Colon Cancer |
277 |
317.0 |
(279.6, 354.3) |
78 |
186.5 |
(145.1, 227.9) |
0.55(0.42, 0.72)*** |
Malee |
|||||||
Colon Cancer |
506 |
470.5 |
(429.5, 511.5) |
85 |
221.3 |
(174.2, 268.3) |
0.49(0.39, 0.63)*** |
aTotal follow-up 116228.5 person-year for patients without statin use and 50476.0 for patients with statin use.
bTotal follow-up 44612.9 person-year for patients without statin use and 21778.3 for patients with statin use.
cTotal follow-up 34092.2 person-year for patients without statin use and 7985.1 for patients with statin use.
dTotal follow-up 87389.9 person-year for patients without statin use and 41828.7 for patients with statin use.
eTotal follow-up 107543.7 person-year for patients without statin use and 38410.7 for patients with statin use.
C.I.: confidence interval
HR: hazard ratio
†Main model is adjusted for age, sex, Charlson comorbidity index, diabetes, hypertension, dyslipidemia, level of urbanization, Monthly income in propensity score.
Statins dose-dependently reduced the colon cancer risk in the different cDDD subgroups, and the main model was adjusted for age, sex, CCI, diabetes, hypertension, dyslipidemia, urbanization level, and monthly income in the PS analysis (Table 3). Lipophilic statins included simvastatin, lovastatin, atorvastatin, and fluvastatin. Hydrophilic statins included pravastatin and rosuvastatin. Both lipophilic and hydrophilic statins reduced the colon cancer risk in the patients with COPD in a dose-dependent manner (P for trend < 0.001; Table 3). When the patients with COPD had 91–365 or >365 cDDDs of statins, the hydrophilic statins exerted a larger preventive effect on the reduction in colon cancer risk. Regarding individual statin users, lovastatin, pravastatin, and fluvastatin nonsignificantly reduced the colon cancer risk. Compared with the statin nonusers, the aHRs of colon cancer decreased in individual statin users (rosuvastatin, simvastatin, and atorvastatin: aHRs = 0.28, 0.64, and 0.65, respectively). Our results revealed that different statin types had different efficacies in reducing colon cancer in the patients with COPD.
Table 3: Incidence rate and adjusted HRs of colon cancer associated with statin use during the follow-up period in COPD patients
Variable |
No. of patients |
No. of person-years |
No. of patients with |
Incidence rate |
Adjusted HR (95%C.I.) |
P for |
|
Total statin use |
|||||||
Nonuser (<28 cDDDs) |
33716 |
194933.6 |
783 |
401.7 |
(373.5, 429.8) |
1.00 |
<0.001 |
User (≥28 cDDDs) |
10086 |
80239.4 |
163 |
203.1 |
(172.0, 234.3) |
0.52(0.44, 0.62)*** |
|
28-90 cDDDs |
2346 |
17095.6 |
49 |
286.6 |
(206.4, 366.9) |
0.72(0.54, 0.96)* |
|
91-365 cDDDs |
3215 |
24193.1 |
59 |
243.9 |
(181.6, 306.1) |
0.62(0.47, 0.80)*** |
|
>365 cDDDs |
4525 |
38950.7 |
55 |
141.2 |
(103.9, 178.5) |
0.36(0.27, 0.47)*** |
|
Lipophilia statin use† |
|||||||
Nonuser (<28 cDDDs) |
35008 |
204288.0 |
799 |
391.1 |
(364.0, 418.2) |
1.00 |
<0.001 |
User (≥28 cDDDs) |
8794 |
70885.0 |
147 |
207.4 |
(173.9, 240.9) |
0.64(0.53, 0.77)*** |
|
28-90 cDDDs |
2296 |
17069.8 |
42 |
246.0 |
(171.6, 320.5) |
0.69(0.50, 0.94)* |
|
91-365 cDDDs |
3012 |
23258.7 |
59 |
253.7 |
(188.9, 318.4) |
0.77(0.58, 1.01) |
|
>365 cDDDs |
3486 |
30556.4 |
46 |
150.5 |
(107.0, 194.0) |
0.50(0.36, 0.67)*** |
|
Hydrophilia statin use† |
|||||||
Nonuser (>28 cDDDs) |
39878 |
242812.7 |
902 |
371.5 |
(347.2, 395.7) |
1.00 |
<0.001 |
User (≥28 cDDDs) |
3924 |
32360.4 |
44 |
136.0 |
(95.8, 176.1) |
0.48(0.35, 0.66)*** |
|
28-90 cDDDs |
1122 |
8876.1 |
19 |
214.1 |
(117.8, 310.3) |
0.72(0.45, 1.13) |
|
91-365 cDDDs |
1531 |
12432.2 |
14 |
112.6 |
(53.6, 171.6) |
0.41(0.24, 0.69)*** |
|
>365 cDDDs |
1271 |
11052.0 |
11 |
99.5 |
(40.7, 158.3) |
0.36(0.20, 0.66)*** |
|
Individual statin use |
|||||||
Simvastatin |
3418 |
28625.0 |
48 |
167.7 |
(120.2, 215.1) |
0.64(0.47, 0.87)** |
|
Lovastatin |
2109 |
18281.5 |
47 |
257.1 |
(183.6, 330.6) |
1.02(0.75, 1.38) |
|
Atorvastatin |
5484 |
44678.1 |
84 |
188.0 |
(147.8, 228.2) |
0.65(0.52, 0.83)*** |
|
Fluvastatin |
1510 |
12855.7 |
29 |
225.6 |
(143.5, 307.7) |
0.93(0.63, 1.35) |
|
Pravastatin |
1501 |
12654.5 |
27 |
213.4 |
(132.9, 293.8) |
0.89(0.60, 1.32) |
|
Rosuvastatin |
2741 |
22641.7 |
18 |
79.5 |
(42.8, 116.2) |
0.28(0.17, 0.45)*** |
|
Main model is adjusted for age, sex, Charlson comorbidity index, diabetes, hypertension, dyslipidemia, level of urbanization, Monthly income in propensity score.
†Lipophilia statins include simvastatin, lovastatin, atorvastatin, and fluvastatin. Hydrophilia statins include pravastatin and rosuvastatin.
‡The HRs of individual statin users (≥ 28 cDDDs) were compared with Total statin of nonusers (<28 cDDDs).
In the sensitivity analysis, adjustments were made to estimate the association of age; sex; CCI; diabetes; hypertension; dyslipidemia; urbanization level; monthly income; and nonstatin lipid-lowering drug, metformin, ACEI, and aspirin use with the incidence of colon cancer in different models. Table 4 shows that the effects of statins remained significant in the subgroups of various covariates in the main model adjusted for PSs. Statins dose-dependently reduced the colon cancer risk in all subgroups and in the main model with additional covariates (nonstatin lipid-lowering drugs, metformin, ACEI, and aspirin use). All aHRs indicated that statins significantly and dose-dependently reduced the colon cancer risk in all subgroups, regardless of age, sex, comorbidity, or drug use (P < 0.001). Thus, our data revealed that statins exert a chemopreventive effect against colon cancer dose-dependently.
Table 4: Sensitivity analysis of adjusted HRs of statin in risk reduction of colon cancer
Statin use |
P for trend |
||||
<28 cDDDs |
28-90 cDDDs |
91-365 cDDDs |
>365 cDDDs |
||
Adjusted HR |
Adjusted HR |
Adjusted HR |
Adjusted HR |
||
Main model† |
1.00 |
0.72(0.54, 0.96)* |
0.62(0.47, 0.80)*** |
0.36(0.27, 0.47)*** |
<0.001 |
Additional covariates‡ |
|||||
Main model + Nonstatin |
1.00 |
0.73(0.54, 0.97)* |
0.63(0.48, 0.82)*** |
0.37(0.28, 0.49)*** |
<0.001 |
Main model + Metformin |
1.00 |
0.72(0.54, 0.96)* |
0.63(0.48, 0.82)*** |
0.39(0.29, 0.51)*** |
<0.001 |
Main model + ACEI |
1.00 |
0.73(0.55, 0.98)* |
0.66(0.50, 0.86)** |
0.42(0.31, 0.56)*** |
<0.001 |
Main model + Aspirin |
1.00 |
0.72(0.54, 0.97)* |
0.64(0.49, 0.84)** |
0.39(0.29, 0.52)*** |
<0.001 |
Subgroup effects |
|||||
Age, years |
|||||
40-64 |
1.00 |
0.59(0.37, 0.95)* |
0.58(0.38, 0.87)** |
0.36(0.25, 0.54)*** |
<0.001 |
65-74 |
1.00 |
0.86(0.55, 1.35) |
0.64(0.42, 0.98)* |
0.35(0.22, 0.55)*** |
<0.001 |
≥75 |
1.00 |
0.80(0.42, 1.50) |
0.54(0.28, 1.06) |
0.24(0.10, 0.58)** |
<0.001 |
Sex |
|||||
Female |
1.00 |
0.73(0.47, 1.14) |
0.67(0.46, 1.00) |
0.40(0.27, 0.59)*** |
<0.001 |
Male |
1.00 |
0.73(0.50, 1.07) |
0.57(0.40, 0.83)** |
0.32(0.22, 0.48)*** |
<0.001 |
CCI Index+ |
|||||
0 |
1.00 |
0.46(0.23, 0.93)* |
0.46(0.26, 0.83)* |
0.35(0.21, 0.59)*** |
<0.001 |
1 |
1.00 |
0.74(0.44, 1.24) |
0.57(0.34, 0.94)* |
0.45(0.28, 0.71)*** |
<0.001 |
2 |
1.00 |
0.70(0.39, 1.27) |
0.57(0.32, 1.01) |
0.36(0.20, 0.63)*** |
<0.001 |
≥3 |
1.00 |
0.99(0.57, 1.71) |
0.83(0.51, 1.36) |
0.16(0.06, 0.39)*** |
<0.001 |
Diabetes |
|||||
No |
1.00 |
0.67(0.48, 0.95)* |
0.59(0.43, 0.82)** |
0.34(0.23, 0.48)*** |
<0.001 |
Yes |
1.00 |
0.84(0.49, 1.43) |
0.62(0.39, 0.98)* |
0.36(0.23, 0.56)*** |
<0.001 |
Dyslipidemia |
|||||
No |
1.00 |
0.68(0.47, 0.98)* |
0.52(0.36, 0.75)*** |
0.35(0.24, 0.51)*** |
<0.001 |
Yes |
1.00 |
0.77(0.48, 1.26) |
0.73(0.49, 1.09) |
0.35(0.23, 0.54)*** |
<0.001 |
Hypertension |
|||||
No |
1.00 |
0.86(0.57, 1.29) |
0.44(0.26, 0.73)** |
0.38(0.24, 0.62)*** |
<0.001 |
Yes |
1.00 |
0.62(0.41, 0.93)* |
0.69(0.50, 0.94)* |
0.33(0.23, 0.46)*** |
<0.001 |
NonStatin |
|||||
<28 cDDDs |
1.00 |
0.77(0.56, 1.05) |
0.63(0.46, 0.86)** |
0.34(0.24, 0.48)*** |
<0.001 |
28-365 cDDDs |
1.00 |
0.48(0.19, 1.22) |
0.69(0.37, 1.29) |
0.47(0.26, 0.83)* |
0.013 |
>365 cDDDs |
1.00 |
1.17(0.30, 4.54) |
0.47(0.12, 1.83) |
0.31(0.10, 0.99)* |
0.028 |
Metformin |
|||||
<28 cDDDs |
1.00 |
0.68(0.48, 0.95)* |
0.63(0.46, 0.87)** |
0.31(0.21, 0.47)*** |
<0.001 |
28-365 cDDDs |
1.00 |
0.86(0.40, 1.85) |
0.55(0.24, 1.22) |
0.34(0.13, 0.86)* |
0.010 |
>365 cDDDs |
1.00 |
1.07(0.45, 2.55) |
0.90(0.47, 1.75) |
0.68(0.40, 1.15) |
0.150 |
ACEI |
|||||
<28 cDDDs |
1.00 |
0.75(0.49, 1.15) |
0.56(0.35, 0.90)* |
0.27(0.13, 0.53)*** |
<0.001 |
28-365 cDDDs |
1.00 |
0.91(0.54, 1.53) |
0.67(0.38, 1.18) |
0.72(0.42, 1.24) |
0.102 |
>365 cDDDs |
1.00 |
0.77(0.42, 1.43) |
1.01(0.67, 1.54) |
0.51(0.34, 0.76)*** |
0.003 |
Aspirin |
|||||
<28 cDDDs |
1.00 |
0.77(0.52, 1.14) |
0.59(0.38, 0.89)* |
0.45(0.29, 0.69)*** |
<0.001 |
28-365 cDDDs |
1.00 |
0.75(0.44, 1.27) |
0.69(0.41, 1.17) |
0.52(0.30, 0.92)* |
0.010 |
>365 cDDDs |
1.00 |
0.79(0.38, 1.64) |
0.90(0.55, 1.46) |
0.38(0.23, 0.63)*** |
<0.001 |
* : p<0.05 ** : p<0.01 *** : p<0.001
HR: hazard ratio
+CCI Index: Charlson Comorbidity Index
†Main model is adjusted for age, sex, Charlson comorbidity index, diabetes, hypertension, dyslipidemia, level of urbanization, Monthly income in propensity score.
‡The models were adjusted for covariates in the main model as well as each additional listed covariate.
DISCUSSION
COPD is characterized by both airway and systemic inflammation [36]. Epidemiological studies have reported that an increase in the levels of systemic inflammatory markers, mainly C-reactive protein (CRP), interleukin 6 (IL-6), and fibrinogen, predicts poor outcomes in COPD, higher propensity to infective exacerbations, and higher mortality [37–39]. COPD significantly enhances this inflammatory disposition by acting as a recurring proinflammatory stimulus to the pulmonary and immune systems. An increase in systemic inflammation in patients with COPD has been linked to progressive loss of lung function [40–46] and several cancer types [46–48]. The strongest association of chronic inflammation with malignant diseases is in colon carcinogenesis arising in individuals with inflammatory bowel disease [49]. Mucosal inflammation may be an independent risk factor for colon cancer [50]. The connection between inflammation and tumorigenesis is well-established and has been reported in genetic, pharmacological, and epidemiological studies in the last decade [51–54]. Moreover, inflammation is likely involved in other forms of sporadic and heritable colon cancer [52]. Furthermore, >90% of patients with COPD are habitual smokers [2, 55], and smoking is associated with an increased incidence of colon cancer [11]. Smoking is also a risk factor for essentially all colonic polyp types [12, 13]. Therefore, patients with severe COPD may have a high colon cancer risk. Furthermore, inclusion of patients without COPD may reveal the different colon cancer preventive effects of statins [56]. The Global Initiative for Chronic Obstructive Lung Disease guidelines recommend that a fixed combination of inhaled corticosteroids or long-acting b2 agonists should be considered for patients with group C or D COPD, who are highly symptomatic or have a high risk of complications [57]. Here, the presence of a baseline pneumonia event and frequent baseline and recent AE were used as surrogates to control for COPD severity. Because our study included only those COPD patients with more than two instances of AEs or any AE requiring hospitalization within the 12 months between enrollment and the index date, the enrolled patients likely represented those who essentially required inhaled corticosteroid therapy [57, 58]. The development of a safe and effective chemopreventive strategy is warranted for patients with severe COPD in order to reduce the risk of colon cancer.
The beneficial effects of statins are not completely understood. Studies have reported that statins reduce inflammation and baseline inflammatory marker levels, cause thrombogenicity, and reverse endothelial dysfunction [59–61]. Randomized studies have reported that statins reduce levels of inflammatory markers such as CRP and IL-6 [62, 63]. However, the mechanisms by which statins interfere in the inflammatory response remain unclear. A possible mechanism is the impairment of inflammatory cell adhesion through the inhibition of the beta-2 integrin leukocyte function antigen-1 [64, 65]. Other potentially contributing factors include decreased lipidation of intracellular proteins, expression of major histocompatibility complex class II molecules on antigen-presenting cells in response to interferons, and subsequent activation of T lymphocytes [65, 66]. A statin-induced decrease in CRP levels may be partly mediated by the decreased monocyte expression of proinflammatory cytokines that stimulate the release of acute phase proteins [67]. This may be the mechanism by which statins reduce the colon cancer risk in patients with COPD and high systemic inflammation [36].
Colon cancer is the most common malignancy in Taiwan [68]. Age is a major risk factor for sporadic colon cancer. Large bowel cancer is uncommon in people younger than 40 years; thus, we included only those patients who were aged ≥40 years and we observed a larger chemopreventive effect against colon cancer in patients with COPD aged 40–64 and ≥75 years (Table 2). This finding indicates that statins exert a chemopreventive effect in middle-aged and elderly patients with COPD. After sex stratification, the aHR was lower in the statin users than in the statin nonusers (women: aHR = 0.55, 95% CI = 0.42, 0.72; men: aHR = 0.49, 95% CI = 0.39, 0.63). Moreover, in our study, the effect of colon cancer risk reduction was predominant in the male statin users with COPD. This finding is consistent with that of another study that reported primary prevention of coronary heart disease through statin therapy in women; this risk reduction was weakly significant (HR = 0.89; 95% CI = 0.79, 1.00; P = 0.05) [69]. However, the reasons for the differences in the effects have not been clarified thus far.
In our study, statins dose-dependently reduced the colon cancer risk in different cDDD subgroups, and the main model was adjusted for age, sex, CCI, diabetes, hypertension, dyslipidemia, urbanization level, and monthly income in the PS analysis (Table 3). Both lipophilic and hydrophilic statins reduced the colon cancer risk in the patients with COPD in a dose-dependent manner (P for trend < 0.001; Table 3). In those who used statins at a 91–365 or >365 cDDDs, the hydrophilic statins exerted a larger preventive effect in the reduction of the colon cancer risk. Regarding the various statin types, lovastatin, pravastatin, and fluvastatin nonsignificantly reduced the colon cancer risk in the patients with COPD. Compared with the statin nonusers, the aHRs of colon cancer decreased in the individual statin users (aHRs = 0.28, 0.64, and 0.65 for rosuvastatin, simvastatin, and atorvastatin, respectively). Therefore, our results indicate that different statin types have different efficacies in reducing colon cancer risk in patients with COPD. The efficacy of statins in reducing this risk is compatible with the lipid-lowering potency of different statins. Rosuvastatin, atorvastatin, and simvastatin cause the highest percentage change in low-density lipoprotein cholesterol [70–72] and have the largest chemopreventive effect against colon cancer in patients with COPD. The efficacy of individual statins in reducing inflammation and baseline inflammatory marker levels, causing thrombogenicity, and reversing endothelial dysfunction are also distinct [73–75]. This is the first study to evaluate which statin type has the largest chemopreventive effect in reducing colon cancer risk in patients with COPD. Our study results can facilitate the appropriate selection of more favorable statins in future clinical studies.
In vitro and in vivo data suggest that angiotensin II is involved in promoting cancer development and that ACEI use and reduced colon cancer cell growth are associated [76, 77]. Metformin use significantly reduces the incidence of pancreatic, liver, breast, and colon cancers [78]. Regular use of aspirin and other nonsteroidal anti-inflammatory drugs decreases the risk of adenomatous polyps and colorectal cancer [79, 80]. Nonstatin lipid-lowering drugs and statins differ regarding their mechanisms of action and lipid-lowering degrees and types. Therefore, we used a sensitivity analysis to include possible unmeasured confounding factors to distinguish the independent anticolon cancer effects of statins. In the present study, a higher proportion of statin nonusers used nonstatin lipid-lowering drugs, metformin, ACEI, and aspirin at ≥28 cDDDs, whereas most statin users used these drugs at <28 cDDDs. Furthermore, moderate-to-high (28–365 cDDDs or >365 cDDD) use of aspirin, metformin, and ACEI masked the chemopreventive effect of statins in reducing the colon cancer risk (Table 4). In our sensitivity analysis, the aHRs of statins in reducing the colon cancer risk of patients with COPD were significant when the statin dose was increased to >365 cDDDs. These outcomes may explain the independent chemopreventive effects of aspirin, metformin, ACEI, nonstatin lipid-lowering drugs, and statins [81, 82]. This is the first study to report that statins exert a dose-dependent chemopreventive effect against colon cancer in patients with COPD.
Our study has some potential limitations. We could not eliminate the bias of additional risk factors related to COPD and colon cancer such as personal or family history of sporadic colon cancer, obesity, alcohol use, excessive processed meat consumption, physical activity, and smoking status. Therefore, a large-scale randomized trial with a suitable regimen in selected patients should compare standard approaches to obtain this crucial information. However, methodological concerns may obscure the precise association between these factors and colon cancer risk. In addition, a low socioeconomic status is associated with an increased risk of colon cancer [83]. In our study, we used the PS analysis to match age, sex, CCI, diabetes, hypertension, dyslipidemia, urbanization level, and monthly income between groups. Urbanization level and monthly income are nonvalidated alternatives to lifestyle and environmental factors. Moreover, the diagnoses of colon cancer and all other comorbid conditions depended completely on the ICD-9-CM codes. Nevertheless, the National Health Insurance Administration randomly reviews medical records and interviews patients to validate diagnoses. The hospitals with outlier diagnoses and practices may be audited and subsequently heavily penalized if malpractice or discrepancies are discovered. Another limitation is that information on several unmeasured confounders, such as body mass index, smoking, alcohol intake, and other over-the-counter drug use (associated with colon cancer), is unavailable in the NHIRD. However, considering the magnitude and significance of the observed effects, these limitations have unlikely compromised the final results. Finally, our study is not a prospective randomized blinded study; hence, a cause–effect relationship could not be established. The findings of this study suggest that statins dose-dependently exert a significant chemopreventive effect against colon cancer in patients with COPD. Additional randomized studies are required to verify these findings.
PATIENTS AND METHODS
The National Health Insurance program, implemented in 1995, currently provides comprehensive health insurance coverage to >98% of the 23 million residents of Taiwan. We used data from the National Health Insurance Research Database (NHIRD), in which the distributions of age, sex, and health care costs does not differ significantly from those in the general population. Data in the NHIRD that could identify patients or care providers, including medical institutions and physicians, are encrypted before being forwarded to the National Health Research Institutes for database construction and are further encrypted before being released to researchers. Theoretically, querying the data alone to identify people at any level by using this database is impractical [18].
From the NHIRD, all patients who received a COPD diagnosis at health care facilities in Taiwan (n = 116,017) between January 1, 2001, and December 31, 2012 were identified according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes 491, 492, 496, and A-code A325. Among the patients who fulfilled the selection criteria of COPD, those with two episodes of acute exacerbation (AE) within 1 year or one episode of AE requiring hospitalization were identified, with the first AE date defined as the enrollment date. AE was defined as emergency department visits or admissions with ICD-9-CM codes 491, 492, 496, and A-code A325 plus prescription of systemic corticosteroids. We excluded all patients without a subsequent outpatient visit, emergency department visit, or inpatient hospitalization for COPD within 12 months of the first presentation (n = 48,212) because they were considered to not have COPD (Figure 1). The index date was noted as 365 days after the enrollment date. The baseline frequency of AE was calculated during the 1-year period from the enrollment to the index date [32]. In addition, we excluded 15,436 patients who were aged <40 years (n = 52,369), had a history of any inpatient or outpatient diagnosis related to cancer before the enrollment date (n = 5,353), or had any statin prescription within 6 months before the enrollment date (n = 3,214). Finally, we included 43,802 patients with COPD in the study cohort and followed them for an 11-year period. Of the 43,802 patients with COPD, 10,086 used statins and 33,716 did not.
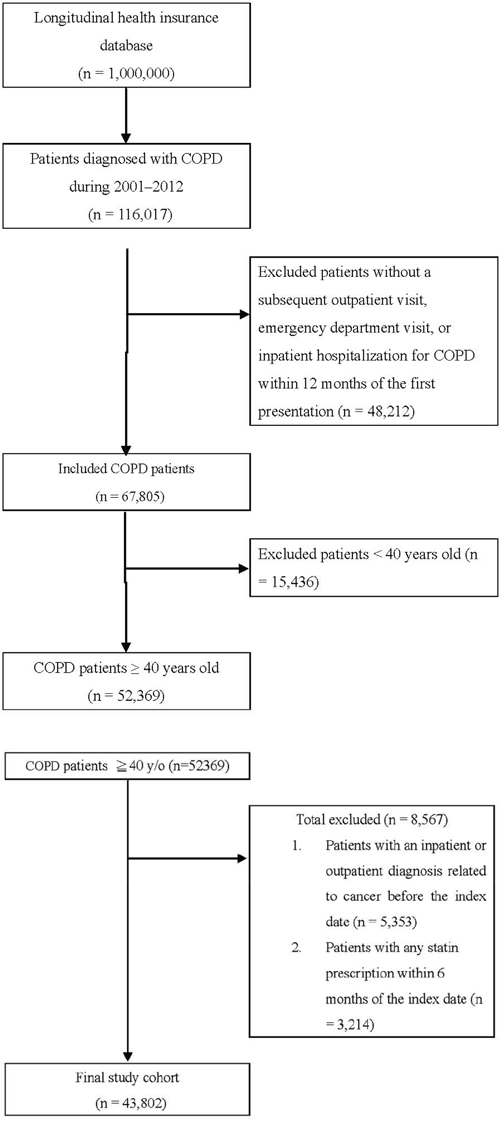
Figure 1: Patient selection flowchart.
Each patient was followed to assess the colon cancer risk and protective factors. We evaluated the demographic characteristics of age and sex; comorbidities of diabetes, hypertension, and dyslipidemia; Charlson comorbidity index (CCI); urbanization level; monthly income; and nonstatin lipid-lowering drug, metformin, aspirin, and angiotensin-converting enzyme inhibitor (ACEI) use (Supplementary Table S1). The date of COPD diagnosis was considered the index date of statin use. This study aimed to evaluate the preventive effects of statin use in patients with COPD and a high colon cancer risk. The primary endpoint was colon cancer risk, and the secondary endpoints were the benefits of different doses and types of statins used in patients with COPD. The defined daily dose (DDD), as defined by the World Health Organization, is a measure of the prescribed drug amount. DDD is the assumed average maintenance dose per day of a drug consumed for its main indication in adults [18]. Because the duration of the prescription refill card is 3 months, we categorized the DDD (entire duration of observation for each patient) of statins into four groups in each cohort [<28, 28–90, 91–365, and >365 cumulative DDDs (cDDDs)] to examine the dose–response relationship. Patients who received statins at <28 cDDDs were defined as statin nonusers (Tables 2–4) [33]. Furthermore, we categorized statins used into individual statin groups in each cohort to examine the preventive effect of different statin types (Table 3).
A propensity score (PS) was derived using a logistic regression model to estimate the effect of statins by accounting for covariates predicted during the intervention (statins). All potential confounders (Supplementary Table S1) were included in the list of regressors (C statistic: 0.678). This method is used in observational studies to reduce selection bias [34]. The covariates in the main model were adjusted for the PSs of age (40–54, 55–64, and ≥75 years), sex, CCI, diabetes, hypertension, dyslipidemia, urbanization level, and monthly income (0, NT$1–NT$21,000, NT$21,000–NT$33,300, and ≥NT$33,301; Table 2). The endpoint was the incidence of colon cancer (ICD-9-CM codes 153.0–153.9) among the statin and statin nonusers with a subsequent outpatient visit, emergency department visit, or inpatient hospitalization for colon cancer within 12 months; patients who did not receive statins served as the reference arm. The cumulative incidence of colon cancer in the patients with COPD with or without statin use was estimated using the Kaplan–Meier method.
A time-dependent Cox proportional hazard model was used to calculate the hazard ratios (HRs) of colon cancer among the statin users and nonusers. In the multivariate analysis, the HRs were adjusted for age, sex, CCI, diabetes, hypertension, dyslipidemia, urbanization level, and monthly income. A stratified analysis was conducted to evaluate the effect of statin use on age and sex (Table 2). All analyses were conducted using SAS software (version 9.3; SAS, Cary, NC, USA); two-tailed P < 0.05 was considered significant. In sensitivity analyses, external adjustments clarify the effects of drugs and other covariates in epidemiological database studies [35]. Hence, in the sensitivity analysis conducted in the present study, adjustments were made to estimate the association of age and sex; diabetes, dyslipidemia, hypertension, CCI, and anxiety disorder; and nonstatin lipid-lowering drug, metformin, aspirin, and ACEI use with the incidence of colon cancer in different models. The models stratified by the use of different drugs were adjusted for covariates in the main model and each additional covariate (Table 4).
CONCLUSIONS
Statins dose-dependently exert a significant chemopreventive effect against colon cancer in patients with COPD, with rosuvastatin, atorvastatin, and simvastatin exerting the largest chemopreventive effects.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Van Durme YM, Verhamme KM, Stijnen T, van Rooij FJ, Van Pottelberge GR, Hofman A, Joos GF, Stricker BH, Brusselle GG. Prevalence, incidence, and lifetime risk for the development of COPD in the elderly: the Rotterdam study. Chest. 2009; 135:368-377.
2. Lokke A, Lange P, Scharling H, Fabricius P, Vestbo J. Developing COPD: a 25 year follow up study of the general population. Thorax. 2006; 61:935-939.
3. Tager IB, Speizer FE. Risk estimates for chronic bronchitis in smokers: a study of male-female differences. The American review of respiratory disease. 1976; 113:619-625.
4. Xu X, Weiss ST, Rijcken B, Schouten JP. Smoking, changes in smoking habits, and rate of decline in FEV1: new insight into gender differences. The European respiratory journal. 1994; 7:1056-1061.
5. Forey BA, Thornton AJ, Lee PN. Systematic review with meta-analysis of the epidemiological evidence relating smoking to COPD, chronic bronchitis and emphysema. BMC pulmonary medicine. 2011; 11:36.
6. Berndt A, Leme AS, Shapiro SD. Emerging genetics of COPD. EMBO molecular medicine. 2012; 4:1144-1155.
7. Wedzicha JA, Calverley PM, Seemungal TA, Hagan G, Ansari Z, Stockley RA. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. American journal of respiratory and critical care medicine. 2008; 177:19-26.
8. Vestbo J, Sorensen T, Lange P, Brix A, Torre P, Viskum K. Long-term effect of inhaled budesonide in mild and moderate chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 1999; 353:1819-1823.
9. Watson L, Vonk JM, Lofdahl CG, Pride NB, Pauwels RA, Laitinen LA, Schouten JP, Postma DS. Predictors of lung function and its decline in mild to moderate COPD in association with gender: results from the Euroscop study. Respiratory medicine. 2006; 100:746-753.
10. Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, Yates JC, Vestbo J. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. The New England journal of medicine. 2007; 356:775-789.
11. Botteri E, Iodice S, Bagnardi V, Raimondi S, Lowenfels AB, Maisonneuve P. Smoking and colorectal cancer: a meta-analysis. JAMA. 2008; 300:2765-2778.
12. Botteri E, Iodice S, Raimondi S, Maisonneuve P, Lowenfels AB. Cigarette smoking and adenomatous polyps: a meta-analysis. Gastroenterology. 2008; 134:388-395.
13. Wallace K, Grau MV, Ahnen D, Snover DC, Robertson DJ, Mahnke D, Gui J, Barry EL, Summers RW, McKeown-Eyssen G, Haile RW, Baron JA. The association of lifestyle and dietary factors with the risk for serrated polyps of the colorectum. Cancer epidemiology, biomarkers & prevention. 2009; 18:2310-2317.
14. Buchanan DD, Sweet K, Drini M, Jenkins MA, Win AK, English DR, Walsh MD, Clendenning M, McKeone DM, Walters RJ, Roberts A, Pearson SA, Pavluk E, Hopper JL, Gattas MR, Goldblatt J, et al. Risk factors for colorectal cancer in patients with multiple serrated polyps: a cross-sectional case series from genetics clinics. PloS one. 2010; 5:e11636.
15. Kim KM, Lee EJ, Ha S, Kang SY, Jang KT, Park CK, Kim JY, Kim YH, Chang DK, Odze RD. Molecular features of colorectal hyperplastic polyps and sessile serrated adenoma/polyps from Korea. The American journal of surgical pathology. 2011; 35:1274-1286.
16. Figueiredo JC, Crockett SD, Snover DC, Morris CB, McKeown-Eyssen G, Sandler RS, Ahnen DJ, Robertson DJ, Burke CA, Bresalier RS, Church JM, Church TR, Baron JA. Smoking-associated risks of conventional adenomas and serrated polyps in the colorectum. Cancer causes & control. 2015; 26:377-386.
17. Pande M, Lynch PM, Hopper JL, Jenkins MA, Gallinger S, Haile RW, LeMarchand L, Lindor NM, Campbell PT, Newcomb PA, Potter JD, Baron JA, Frazier ML, Amos CI. Smoking and colorectal cancer in Lynch syndrome: results from the Colon Cancer Family Registry and the University of Texas M.D. Anderson Cancer Center. Clinical cancer research. 2010; 16:1331-1339.
18. Chen CI, Kuan CF, Fang YA, Liu SH, Liu JC, Wu LL, Chang CJ, Yang HC, Hwang J, Miser JS, Wu SY. Cancer risk in HBV patients with statin and metformin use: a population-based cohort study. Medicine (Baltimore). 2015; 94:e462.
19. Chan KK, Oza AM, Siu LL. The statins as anticancer agents. Clinical cancer research. 2003; 9:10-19.
20. Danesh FR, Sadeghi MM, Amro N, Philips C, Zeng L, Lin S, Sahai A, Kanwar YS. 3-Hydroxy-3-methylglutaryl CoA reductase inhibitors prevent high glucose-induced proliferation of mesangial cells via modulation of Rho GTPase/ p21 signaling pathway: Implications for diabetic nephropathy. Proceedings of the National Academy of Sciences of the United States of America. 2002; 99:8301-8305.
21. Blanco-Colio LM, Munoz-Garcia B, Martin-Ventura JL, Lorz C, Diaz C, Hernandez G, Egido J. 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors decrease Fas ligand expression and cytotoxicity in activated human T lymphocytes. Circulation. 2003; 108:1506-1513.
22. Takemoto M, Liao JK. Pleiotropic effects of 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibitors. Arteriosclerosis, thrombosis, and vascular biology. 2001; 21:1712-1719.
23. Wong WW, Dimitroulakos J, Minden MD, Penn LZ. HMG-CoA reductase inhibitors and the malignant cell: the statin family of drugs as triggers of tumor-specific apoptosis. Leukemia. 2002; 16:508-519.
24. Rao S, Porter DC, Chen X, Herliczek T, Lowe M, Keyomarsi K. Lovastatin-mediated G1 arrest is through inhibition of the proteasome, independent of hydroxymethyl glutaryl-CoA reductase. Proceedings of the National Academy of Sciences of the United States of America. 1999; 96:7797-7802.
25. Poynter JN, Gruber SB, Higgins PD, Almog R, Bonner JD, Rennert HS, Low M, Greenson JK, Rennert G. Statins and the risk of colorectal cancer. The New England journal of medicine. 2005; 352:2184-2192.
26. Kaye JA, Jick H. Statin use and cancer risk in the General Practice Research Database. British journal of cancer. 2004; 90:635-637.
27. Coogan PF, Smith J, Rosenberg L. Statin use and risk of colorectal cancer. Journal of the National Cancer Institute. 2007; 99:32-40.
28. Singh H, Mahmud SM, Turner D, Xue L, Demers AA, Bernstein CN. Long-term use of statins and risk of colorectal cancer: a population-based study. The American journal of gastroenterology. 2009; 104:3015-3023.
29. Cao C, Wu Y, Xu Z, Lv D, Zhang C, Lai T, Li W, Shen H. The effect of statins on chronic obstructive pulmonary disease exacerbation and mortality: a systematic review and meta-analysis of observational research. Scientific reports. 2015; 5:16461.
30. Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, Brown L, Warnica JW, Arnold JM, Wun CC, Davis BR, Braunwald E. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. The New England journal of medicine. 1996; 335:1001-1009.
31. Pedersen TR, Berg K, Cook TJ, Faergeman O, Haghfelt T, Kjekshus J, Miettinen T, Musliner TA, Olsson AG, Pyorala K, Thorgeirsson G, Tobert JA, Wedel H, Wilhelmsen L. Safety and tolerability of cholesterol lowering with simvastatin during 5 years in the Scandinavian Simvastatin Survival Study. Archives of internal medicine. 1996; 156:2085-2092.
32. Lee MC, Lee CH, Chien SC, Chang JH, She HL, Wang JY, Yu MC. Inhaled Corticosteroids Increase the Risk of Pneumonia in Patients With Chronic Obstructive Pulmonary Disease: A Nationwide Cohort Study. Medicine (Baltimore). 2015; 94:e1723.
33. Singh S, Singh PP. Statins for prevention of hepatocellular cancer: one step closer? Hepatology. 2014; 59:724-726.
34. D’Agostino RB, Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Statistics in medicine. 1998; 17:2265-2281.
35. Schneeweiss S. Sensitivity analysis and external adjustment for unmeasured confounders in epidemiologic database studies of therapeutics. Pharmacoepidemiology and drug safety. 2006; 15:291-303.
36. Sin DD, Paul Man SF. Cooling the fire within: inhaled corticosteroids and cardiovascular mortality in COPD. Chest. 2006; 130:629-631.
37. Sin DD, Man SF. Interleukin-6: a red herring or a real catch in COPD? Chest. 2008; 133:4-6.
38. Cazzola M, Page CP, Calzetta L, Matera MG. Emerging anti-inflammatory strategies for COPD. The European respiratory journal. 2012; 40:724-741.
39. Ahmad T, Mabalirajan U, Sharma A, Aich J, Makhija L, Ghosh B, Agrawal A. Simvastatin improves epithelial dysfunction and airway hyperresponsiveness: from asymmetric dimethyl-arginine to asthma. American journal of respiratory cell and molecular biology. 2011; 44:531-539.
40. Sin DD, Man SF. Why are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary disease. Circulation. 2003; 107:1514-1519.
41. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. The European respiratory journal. 2009; 33:1165-1185.
42. Barr RG. The epidemiology of vascular dysfunction relating to chronic obstructive pulmonary disease and emphysema. Proceedings of the American Thoracic Society. 2011; 8:522-527.
43. Walter RE, Wilk JB, Larson MG, Vasan RS, Keaney JF, Jr., Lipinska I, O’Connor GT, Benjamin EJ. Systemic inflammation and COPD: the Framingham Heart Study. Chest. 2008; 133:19-25.
44. Fabbri LM, Beghe B, Agusti A. Cardiovascular mechanisms of death in severe COPD exacerbation: time to think and act beyond guidelines. Thorax. 2011; 66:745-747.
45. Chang SS, Vaz Fragoso CA, Van Ness PH, Fried LP, Tinetti ME. Association between combined interleukin-6 and C-reactive protein levels and pulmonary function in older women: results from the Women’s Health and Aging Studies I and II. Journal of the American Geriatrics Society. 2011; 59:113-119.
46. Siemes C, Visser LE, Coebergh JW, Splinter TA, Witteman JC, Uitterlinden AG, Hofman A, Pols HA, Stricker BH. C-reactive protein levels, variation in the C-reactive protein gene, and cancer risk: the Rotterdam Study. Journal of clinical oncology. 2006; 24:5216-5222.
47. Cho WC, Kwan CK, Yau S, So PP, Poon PC, Au JS. The role of inflammation in the pathogenesis of lung cancer. Expert opinion on therapeutic targets. 2011; 15:1127-1137.
48. Chaturvedi AK, Caporaso NE, Katki HA, Wong HL, Chatterjee N, Pine SR, Chanock SJ, Goedert JJ, Engels EA. C-reactive protein and risk of lung cancer. Journal of clinical oncology. 2010; 28:2719-2726.
49. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002; 420:860-867.
50. Heuschen UA, Hinz U, Allemeyer EH, Stern J, Lucas M, Autschbach F, Herfarth C, Heuschen G. Backwash ileitis is strongly associated with colorectal carcinoma in ulcerative colitis. Gastroenterology. 2001; 120:841-847.
51. Ericsson AC, Myles M, Davis W, Ma L, Lewis M, Maggio-Price L, Franklin C. Noninvasive detection of inflammation-associated colon cancer in a mouse model. Neoplasia. 2010; 12:1054-1065.
52. Terzic J, Grivennikov S, Karin E, Karin M. Inflammation and colon cancer. Gastroenterology. 2010; 138:2101-2114 e2105.
53. Beatty PL, Narayanan S, Gariepy J, Ranganathan S, Finn OJ. Vaccine against MUC1 antigen expressed in inflammatory bowel disease and cancer lessens colonic inflammation and prevents progression to colitis-associated colon cancer. Cancer prevention research. 2010; 3:438-446.
54. Vetrano S, Borroni EM, Sarukhan A, Savino B, Bonecchi R, Correale C, Arena V, Fantini M, Roncalli M, Malesci A, Mantovani A, Locati M, Danese S. The lymphatic system controls intestinal inflammation and inflammation-associated Colon Cancer through the chemokine decoy receptor D6. Gut. 2010; 59:197-206.
55. She J, Yang P, Wang Y, Qin X, Fan J, Gao G, Luo G, Ma K, Li B, Li C, Wang X, Song Y, Bai C. Chinese water-pipe smoking and the risk of COPD. Chest. 2014; 146:924-931.
56. Cheng MH, Chiu HF, Ho SC, Tsai SS, Wu TN, Yang CY. Statin use and the risk of colorectal cancer: a population-based case-control study. World journal of gastroenterology. 2011; 17:5197-5202.
57. Vestbo J, Hurd SS, Agusti AG, Jones PW, Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ, Nishimura M, Stockley RA, Sin DD, Rodriguez-Roisin R. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. American journal of respiratory and critical care medicine. 2013; 187:347-365.
58. Gershon AS, Campitelli MA, Croxford R, Stanbrook MB, To T, Upshur R, Stephenson AL, Stukel TA. Combination long-acting beta-agonists and inhaled corticosteroids compared with long-acting beta-agonists alone in older adults with chronic obstructive pulmonary disease. JAMA. 2014; 312:1114-1121.
59. Albert MA, Danielson E, Rifai N, Ridker PM. Effect of statin therapy on C-reactive protein levels: the pravastatin inflammation/CRP evaluation (PRINCE): a randomized trial and cohort study. JAMA. 2001; 286:64-70.
60. Ridker PM, Rifai N, Pfeffer MA, Sacks FM, Moye LA, Goldman S, Flaker GC, Braunwald E. Inflammation, pravastatin, and the risk of coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events (CARE) Investigators. Circulation. 1998; 98:839-844.
61. Jialal I, Stein D, Balis D, Grundy SM, Adams-Huet B, Devaraj S. Effect of hydroxymethyl glutaryl coenzyme a reductase inhibitor therapy on high sensitive C-reactive protein levels. Circulation. 2001; 103:1933-1935.
62. Panichi V, Paoletti S, Mantuano E, Manca-Rizza G, Filippi C, Santi S, Taccola D, Donadio C, Tramonti G, Innocenti M, Casto G, Consani C, Sbragia G, Franzoni F, Galetta F, Panicucci E, et al. In vivo and in vitro effects of simvastatin on inflammatory markers in pre-dialysis patients. Nephrology, dialysis, transplantation. 2006; 21:337-344.
63. McCarty MF. Reduction of serum C-reactive protein by statin therapy may reflect decreased isoprenylation of Rac-1, a mediator of the IL-6 signal transduction pathway. Medical hypotheses. 2003; 60:634-639.
64. Weitz-Schmidt G, Welzenbach K, Brinkmann V, Kamata T, Kallen J, Bruns C, Cottens S, Takada Y, Hommel U. Statins selectively inhibit leukocyte function antigen-1 by binding to a novel regulatory integrin site. Nature medicine. 2001; 7:687-692.
65. Frenette PS. Locking a leukocyte integrin with statins. The New England journal of medicine. 2001; 345:1419-1421.
66. Kwak B, Mulhaupt F, Myit S, Mach F. Statins as a newly recognized type of immunomodulator. Nature medicine. 2000; 6:1399-1402.
67. Ferro D, Parrotto S, Basili S, Alessandri C, Violi F. Simvastatin inhibits the monocyte expression of proinflammatory cytokines in patients with hypercholesterolemia. Journal of the American College of Cardiology. 2000; 36:427-431.
68. Health Promotion Administration MoHaW. (2011). Taiwan Cancer Registry report, 2011 edition. (Health Promotion Administration, Ministry of Health and Welfare).
69. Petretta M, Costanzo P, Perrone-Filardi P, Chiariello M. Impact of gender in primary prevention of coronary heart disease with statin therapy: a meta-analysis. International journal of cardiology. 2010; 138:25-31.
70. Jones PH, Davidson MH, Stein EA, Bays HE, McKenney JM, Miller E, Cain VA, Blasetto JW. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* Trial). The American journal of cardiology. 2003; 92:152-160.
71. Rosenson RS. Rosuvastatin: a new inhibitor of HMG-coA reductase for the treatment of dyslipidemia. Expert review of cardiovascular therapy. 2003; 1:495-505.
72. Brown AS, Bakker-Arkema RG, Yellen L, Henley RW, Jr., Guthrie R, Campbell CF, Koren M, Woo W, McLain R, Black DM. Treating patients with documented atherosclerosis to National Cholesterol Education Program-recommended low-density-lipoprotein cholesterol goals with atorvastatin, fluvastatin, lovastatin and simvastatin. Journal of the American College of Cardiology. 1998; 32:665-672.
73. Tsan YT, Lee CH, Wang JD, Chen PC. Statins and the risk of hepatocellular carcinoma in patients with hepatitis B virus infection. Journal of clinical oncology. 2012; 30:623-630.
74. Tsan YT, Lee CH, Ho WC, Lin MH, Wang JD, Chen PC. Statins and the risk of hepatocellular carcinoma in patients with hepatitis C virus infection. Journal of clinical oncology. 2013; 31:1514-1521.
75. Karp I, Behlouli H, Lelorier J, Pilote L. Statins and cancer risk. The American journal of medicine. 2008; 121:302-309.
76. Kedika R, Patel M, Pena Sahdala HN, Mahgoub A, Cipher D, Siddiqui AA. Long-term use of angiotensin converting enzyme inhibitors is associated with decreased incidence of advanced adenomatous colon polyps. Journal of clinical gastroenterology. 2011; 45:e12-16.
77. Makar GA, Holmes JH, Yang YX. Angiotensin-converting enzyme inhibitor therapy and colorectal cancer risk. Journal of the National Cancer Institute. 2014; 106:djt374.
78. Decensi A, Puntoni M, Goodwin P, Cazzaniga M, Gennari A, Bonanni B, Gandini S. Metformin and cancer risk in diabetic patients: a systematic review and meta-analysis. Cancer prevention research. 2010; 3:1451-1461.
79. Flossmann E, Rothwell PM. Effect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studies. Lancet. 2007; 369:1603-1613.
80. Jacobs EJ, Thun MJ, Bain EB, Rodriguez C, Henley SJ, Calle EE. A large cohort study of long-term daily use of adult-strength aspirin and cancer incidence. Journal of the National Cancer Institute. 2007; 99:608-615.
81. Gronich N, Rennert G. Beyond aspirin-cancer prevention with statins, metformin and bisphosphonates. Nature reviews Clinical oncology. 2013; 10:625-642.
82. Janne PA, Mayer RJ. Chemoprevention of colorectal cancer. The New England journal of medicine. 2000; 342:1960-1968.
83. Doubeni CA, Laiyemo AO, Major JM, Schootman M, Lian M, Park Y, Graubard BI, Hollenbeck AR, Sinha R. Socioeconomic status and the risk of colorectal cancer: an analysis of more than a half million adults in the National Institutes of Health-AARP Diet and Health Study. Cancer. 2012; 118:3636-3644.