
INTRODUCTION
TP53 is the most frequent gene involved in human cancers and has been widely evaluated in urothelial carcinoma (UC). The spectrum of TP53 mutations can be used as prognostic molecular biomarkers for various cancers [1–3]. Abnormal p53 protein translated by the mutant gene has a longer half-life than the wild-type protein, resulting in cellular accumulation of abnormal p53 [4]. Based on this characteristic, immunohistochemical (IHC) staining for p53 has been widely utilized as a surrogate marker for the mutant TP53 gene [5]. A meta-analysis reviewed 7 small UTUC series and concluded that p53 overexpression as determined by IHC staining could be a biomarker for predicting poor disease outcomes [6].
Recently, A > T transversions in the TP53 gene of UTUC tumors have been documented as being associated with aristolochic acid (AA) exposure [7]. We have previously shown that AA-induced UTUC, defined by A:T to T:A transversion in tumors and aristolactam-DNA adducts in the renal cortex, has characteristic outcomes, including likely contralateral upper urinary tract recurrence [8]. In addition, TP53 gene mutation patterns were shown to be associated with different prognoses in other cancers, such as colorectal [9] and breast cancers [10]. Together with the above evidence, TP53 mutation pattern may be correlated with disease outcomes and recurrence patterns of UTUC.
However, studies that describe the predictive value of TP53 mutations and patterns in the prognosis of UTUCs have not been reported until now. Herein, we analyzed TP53 mutation patterns in UTUC and evaluated the association between patterns of mutations and recurrences. In addition, the association of p53 overexpression and TP53 mutation pattern was also evaluated.
RESULTS
Patient demographics and clinical features (Table 1)
Table 1: Demographics of the patients stratified by TP53 mutation patterns
TP53 mutation pattern |
Mutations with A > T (AT group) |
Mutations other than A > T (NAT group) |
Wild type (WT group) |
p value |
|---|---|---|---|---|
Patient number (n) |
55 |
42 |
68 |
|
Median age (range) |
63.5 (30–87) |
67.9 (5–88) |
66.4 (42–90) |
0.168 |
Gender |
|
|
|
0.001 |
Male |
20 (36%) |
20 (48%) |
48 (71%) |
|
Female |
35 (64%) |
22 (52%) |
20 (29%) |
|
Smoking history |
|
|
|
0.055 |
Yes |
6 (11%) |
11 (26%) |
19 (28%) |
|
No |
49 (89%) |
31 (74%) |
49 (72%) |
|
Heavy smokinga |
|
|
|
0.009 |
Yes |
3 (5%) |
8 (19%) |
18 (26%) |
|
No |
52 (95%) |
34 (81%) |
50 (74%) |
|
CKD stage |
|
|
|
0.361 |
Normal |
16 (29%) |
16 (38%) |
26 (38%) |
|
3 |
21 (38%) |
15 (36%) |
29 (43%) |
|
4 |
3 (5%) |
4 (10%) |
6 (9%) |
|
5 |
15 (27%) |
7 (17%) |
7 (10%) |
|
ESRD |
|
|
|
0.124 |
Yes |
13 (24%) |
6 (14%) |
7 (10%) |
|
No |
42 (76%) |
36 (86%) |
61 (90%) |
|
DM |
|
|
|
0.07 |
Yes |
11 (20%) |
6 (15%) |
22 (33%) |
|
No |
44 (80%) |
35 (85%) |
45 (67%) |
|
Hypertension |
|
|
|
0.15 |
Yes |
18 (33%) |
21 (51%) |
31 (46%) |
|
No |
37 (67%) |
20 (49%) |
36 (54%) |
|
AL-DNA adduct |
|
|
<0.001 |
|
Yes |
47 (89%) |
22 (54%) |
35 (51%) |
|
No |
6 (11%) |
19 (46%) |
33 (49%) |
|
Tumor location |
|
|
|
|
Renal pelvis |
36 (65%) |
22 (52%) |
50 (74%) |
0.077 |
Upper ureter |
15 (27%) |
8 (19%) |
10 (15%) |
0.219 |
Lower ureter |
17 (31%) |
20 (48%) |
22 (32%) |
0.176 |
Synchronous bladder tumor |
14 (25%) |
9 (21%) |
18 (26%) |
0.831 |
Multiple tumor location |
18 (33%) |
11 (26%) |
22 (32%) |
0.745 |
Grade |
|
|
|
0.046 |
High |
45 (82%) |
31 (74%) |
42 (62%) |
|
Low |
10 (18%) |
11 (26%) |
26 (38%) |
|
Stage |
|
|
|
0.16 |
Ta-1NoMo |
25 (44%) |
19 (45%) |
40 (59%) |
|
T2-4NoMo |
25 (45%) |
22 (52%) |
25 (37%) |
|
nodal or metastatic |
6 (11%) |
1 (2%) |
3 (4%) |
|
p53 IHC staining |
|
|
|
0.011 |
Negative |
15 (38%) |
10 (29%) |
28 (54%) |
|
< = 50% |
13 (33%) |
12 (34%) |
20 (38%) |
|
> 50% |
12 (30%) |
13 (37%) |
4 (8%) |
|
Missing |
15 |
7 |
16 |
|
Follow-up (months, range) |
55 (4–208) |
61 (4–157) |
57 (4–169) |
0.605 |
CKD = chronic kidney disease; ESRD = end-stage renal disease; DM = diabetes mellitus; AL-DNA = aristolactam-DNA; IHC = immunohistochemical.
aheavy smoking was defined as more than 20 pack-years.
In this cohort, 55 (33.3%), 42 (25.5%), and 68 (41.2%) patients were classified as AT group (TP53 mutation with A:T to T:A SBS), NAT group (TP53 mutation with only other than A:T to T:A SBS), and WT group (wild-type TP53), respectively. The distribution of TP53 mutation patterns was shown in Figure 1 according to patient groups. Eight (14.5%) patients in AT group had both A:T to T:A SBS and non-A:T to T:A SBS. There were more females in AT group than in NAT group or WT group. A total of 35 (64%) AT group patients were female; In contrast, 71% of WT group patients were males. Only 36 (21.8%) patients in this cohort had a history of smoking, and the smoking rate was insignificantly lower in AT group than WT group (p = 0.055). WT group (26%) had more smoking histories of ≥ 20 pack-years than AT group (5%) (p = 0.009). In addition, TP53 mutation rate was higher in the patients without smoking histories (72%) than those with smoking histories (47%) (Table S1). In the patients with TP53 mutations, A:T to T:A transversion was more frequently noted in non-smokers, but mutation only other than A:T to T:A transversion was more identified in smokers. End-stage renal disease (ESRD) was more common in AT group (24%) than in NAT group and WT group combined (12%) (p = 0.0495). Diabetes mellitus was more frequently noted in WT group (33%) than the other two groups combined (18%) (p = 0.026). The median follow-up duration from the date of nephroureterectomies was 59 months (from 4 to 208 months) without significant difference among groups.
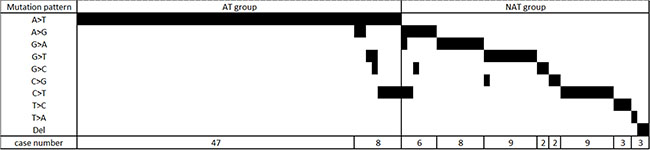
Figure 1: The distribution of TP53 mutation pattern in AT group and NAT group patients. AT group refers to those with A:T > T:A transversion in TP53 gene. NAT group refers to the patients have TP53 mutations, but no A:T > T:A transversion.
Tumor characteristics (Table 1)
An increased number of high-grade tumors were observed in AT group (89%) compared to NAT group (74%) or WT group (62%). AT group had more nodal or metastatic diseases (11%) upon diagnosis of UTUC than NAT group (2%) or WT group (4%), although the rate was not statistically significant. Upon the UTUC diagnosis, 51 (31%) of all patients had tumors at ≥ 2 locations, including renal pelvis, upper ureter, lower ureter, and bladder. Multiple tumor locations and synchronous bladder tumor rates in the three groups were similar.
Association among TP53 mutation patterns, types and p53 immunohistochemical staining (Tables 1 and 2)
Table 2: Association between TP53 mutation type, pattern and p53 immunohistochemical staining
|
Mutation type |
|
|||
|---|---|---|---|---|---|
|
Missense |
Nonsense |
Silent |
Wild type |
|
p53 IHC staining |
|
|
|
|
|
> 50% |
23 (79%) |
0 |
2 (7%) |
4 (14%) |
|
< = 50% |
11 (24%) |
7 (16%) |
7 (16%) |
20 (44%) |
|
Negative |
8 (15%) |
12 (23%) |
5 (9%) |
28 (53%) |
|
TP53 mutation pattern |
|
|
|
|
|
Mutations with A > T |
18 (45%) |
10 (25%) |
12 (30%) |
0 |
|
Mutations other than A > T |
24 (69%) |
9 (26%) |
2 (6%) |
0 |
|
Wild type |
0 |
0 |
0 |
52 (100%) |
|
IHC = immunohistochemical.
Positively-stained cells were more frequently observed in AT group and NAT group than WT group (62%, 71%, and 46%, respectively). Only 8% of WT group tumors had more than 50% of p53 IHC staining (30% in AT group and 27% in NAT group). Accordingly, TP53 mutations were associated with higher percentage of p53 IHC staining in tumors. However, no significant difference of p53 IHC staining result was noted between AT group and NAT group.
A significant association was identified among TP53 mutation types and p53 IHC staining (Table 2). Tumors with more than 50% of p53 IHC staining had a higher proportion (79%) of missense mutations than did those with < = 50% and negative results of IHC staining (24% and 15%, respectively; p < 0.001). Missense mutations were most frequently identified in UTUC tumors of AT (45%) and NAT (69%) groups.
Bladder tumor recurrence
Of all patients, 82 (49.7%) had bladder recurrences during a median follow-up of 59 months (range: 4 to 208 months). Forty-four (26.7%) with previous or synchronous bladder tumors (n = 41) or prophylactic cystectomy (n = 3) were excluded from bladder recurrence analysis. Thirty-nine (32.2%) of the remaining patients (n = 121) had newly diagnosed bladder cancer recurrences. The median time to bladder recurrence was only 7 months (range: 3 to 65) after nephroureterectomy. Compared to AT group and WT group, patients in NAT group had shorter bladder recurrence-free survival duration (log-rank test, p = 0.037 and 0.005, respectively) (Figure 2A). In univariable analysis of Cox proportional hazard model (Table 3), diabetes and TP53 mutation pattern were the only two significant prognosticators of bladder recurrence. Lower ureteral tumor location was a statistically insignificant factor for bladder recurrence (p = 0.065). Multivariable analysis of the full model (model 1) revealed that diabetes and TP53 mutations other than A:T to T:A transversions (NAT group) were associated with more bladder recurrences. In the model filled with interested variables and clinically important prognosticators, including gender, tumor grade, stage, and lower ureteral tumors, TP53 mutations other than A:T to T:A transversions still presented as an independent variable predicting a higher risk (HR: 8.4 and 3.7, p < 0.001 and = 0.01, respectively) of bladder recurrence compared with wild-type TP53 and TP53 mutations with A:T to T:A transversions.
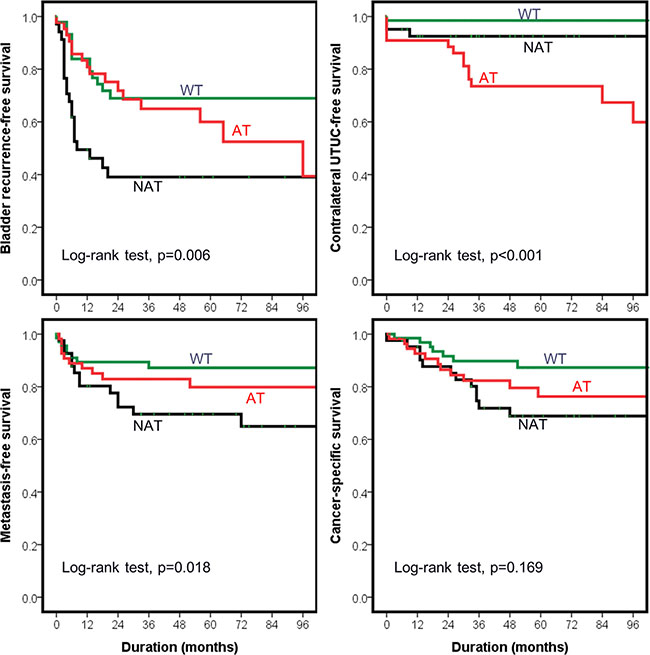
Figure 2: Outcomes of upper urinary tract urothelial carcinoma (UTUC) patients stratified by mutational status of TP53. AT group refers to those with A:T > T:A transversion in TP53 gene. NAT group refers to the patients have TP53 mutations, but no A:T > T:A transversion. WT group represents those without TP53 mutation.
Table 3: The Cox proportional hazard model of bladder recurrence in UTUC patients
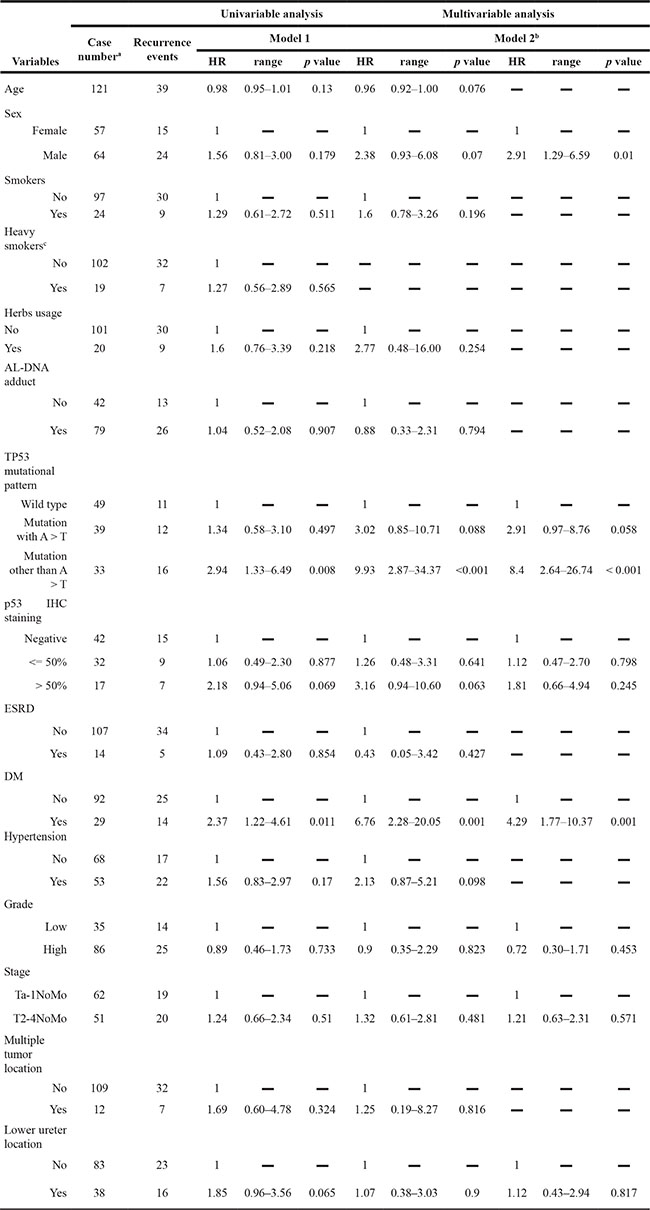
UTUC = upper urinary tract urothelial carcinoma; AL-DNA = aristolactam-DNA; IHC = immunohistochemical; ESRD = end-stage renal disease; DM = diabetes mellitus.
aThe patients with synchronous or previous bladder cancers or receiving radical cystectomies were excluded from this study.
bModel 2 includes variables with p < 0.05 in the univariable analysis, and classical prognostic factors.
cHeavy smoking was defined as more than 20 pack-years.
A total of 57% of the patients with previous or synchronous bladder cancer had TP53 mutations, whereas 72% of those with bladder recurrence after nephroureterectomies had TP53 mutations. In addition, mutation other than A:T to T:A transversion was more frequently noted in the UTUC patients with bladder recurrence after nephroureterectomies compared to those with previous or synchronous bladder cancer history (Table S2).
Metachronous contralateral UTUC recurrence
In this cohort, previous, synchronous or metachronous bilateral UTUC diseases were identified in 18 patients, of whom 14 (78%) from AT group, 3 (17%) from NAT group, and 1 (6%) from WT group. Nine patients in AT group and 1 patient in NAT group had contralateral UTUC occurrences after nephroureterectomy. None of the WT group patients had metachronous contralateral UTUC. In the patients with synchronous or previous contralateral UTUC (N = 8), 5 and 2 were AT and NAT groups, respectively. Only one patient had no mutation in TP53 gene. Excluding those with previous and synchronous UTUC diseases, we identified AT group had a shorter contralateral UTUC-free survival duration than the other two groups (log-rank test, both p < 0.001) (Figure 2B). Univariable analysis revealed herbs usage, aristolactam-DNA adducts, TP53 mutation with A:T to T:A transversions, and diabetes increased risk of metachronous contralateral UTUC recurrence. Multivariable analysis can’t be performed due to the limited number of events.
Metastasis
Of patients with non-metastatic diseases before nephroureterectomy (n = 155), metastases occurred in 7 (14.3%), 12 (29.3%), and 5 (7.7%) patients in AT, NAT and WT groups, respectively. Median duration between metastasis and nephroureterectomy was 8.5 months. NAT group patients had a shorter metastasis-free survival than the other two groups (Figure 2C). Tumor stage, grade, p53 IHC staining and TP53 mutation patterns were statistically significant prognosticators of metastases. After stratifying for tumor grade and stage, NAT group predicted earlier metastasis compared to AT and WT groups combined in the multivariable model (HR = 2.50, 95% CI. 1.12–5.58, p = 0.026).
Survival outcomes
A total of 44 patients died during a median follow-up of 59 months. Older age, advanced tumor grade and stage predicted shorter overall survival duration in univariable and multivariable analyses. Cancer-specific deaths were noted in 30 UTUC patients, and only tumor grade and stage were prognosticators. Patients in NAT group had an insignificantly increased risk of cancer-specific death compared to WT group (HR = 2.41, 95% CI. 0.93–6.21, p = 0.07). No difference in survival outcomes was noted between AT and NAT groups (Figure 2D).
DISCUSSION
By stratifying UTUC patients according to TP53 mutation patterns, we observed that patients with an A:T to T:A transversion in the TP53 gene had a higher risk of contralateral upper urinary tract recurrence, and those with non- A:T to T:A transversion mutations had more bladder tumor recurrences and metastases than the other two groups. These findings demonstrate that TP53 mutation pattern is a useful biomarker for predicting patient outcomes. Therefore, the TP53 mutation pattern should be considered important information for clinicians in improving follow-up protocols for UTUC patients.
Previous studies discovered that p53 protein overexpression in UTUC [6, 11] was associated with recurrence- and progression-free survival duration. However, these studies used IHC staining to determine p53 expression levels. Based on the principle of this assay, positive IHC results do not recognize null mutations, such as deletions, insertions, nonsense and splicing site mutations. Approximately 30% of somatic TP53 mutations are not identified by IHC assay, suggesting that IHC is not sufficient for detection of TP53 mutations [12]. Hashimoto et al. reported that null mutations predicted outcomes better than the IHC assay [13]. Besides, positive IHC results from early tumor lesions should be interpreted carefully because local responses to inflammatory microenvironments can cause accumulation of wild-type p53 in tumors [14]. Hence, DNA sequencing remains the gold standard for identifying TP53 mutations. That is why our present study investigates patients according to TP53 sequencing results.
TP53 mutation patterns were significantly associated with patient demographics. Tumors in smokers had fewer A:T to T:A transversions, but had more non- A:T to T:A transversion mutations. As that in lung cancer study, a G:T transversion at codon 157 in TP53 is frequent in smokers [15, 16]. On the other hand, only 1 out of 11 patients with an A:T to T:A transversion had ever smoked in our cohort. Patients who had been exposed to herbs had a higher frequency of A:T to T:A transversions, which is the signature mutation of AA [7]. Furthermore, the A:T to T:A transversion was associated with poor renal function given that AA induces renal tubular damage [17]. In our cohort, TP53 mutations with an A:T to T:A transversion were more frequent in female UTUC patients than males, which may be partially due the fact that more Taiwanese women tend to take herbs containing AA than men [18]. Whether gender or carcinogens contributed to differences in TP53 mutation patterns should be further investigated.
Based on the results combining aristolactam-DNA adducts in renal cortical tissue and A:T to T:A transversions in the TP53 gene, patients with AA-induced UTUC had more high-grade and high-stage tumors than non-AA UTUC patients [8]. This extended cohort revealed that patients with TP53 mutations had more unfavorable tumor characteristics than those without TP53 mutations. A:T to T:A transversion pattern was associated with the worst initial tumor presentations, such as high grade and nodal or metastatic disease, in this cohort. As the signature mutation of AA, A:T to T:A transversion suggests that AA is responsible for carcinogenesis in these cases of UTUC. Patients with this signature mutation were considered as having bilateral, either synchronous or metachronous, UTUC [8].
UTUCs with TP53 non- A:T to T:A transversions have more and earlier bladder recurrences than those without TP53 mutations or A:T to T:A transversions. Using IHC staining, previous studies revealed that p53 overexpression in tumors had conflicting disease-free survival results in UTUC patients [6]. In fact, p53 protein overexpression could be caused by different TP53 mutation patterns. As shown in this study, UTUC patients with an A:T to T:A transversion did not have poorer outcomes of bladder recurrences or metastases than those without TP53 mutations. However, non- A:T to T:A transversion mutations in the TP53 gene did predict poorer outcomes. Hence, the precise stratification of TP53 mutations would help predict patient outcomes.
In contrast to other tumor suppressor genes which are changed by truncating mutations, most of TP53 gene mutations are missense substitutions (75%) [19] that are resulted from SBS clustering within DNA-binding domain of protein. Furthermore, the most frequent mutants have been revealed to have ability to cooperate with oncogenes for cellular transformation [20]. Our UTUC patients with TP53 mutations other than A:T to T:A transversion had higher proportion of missense mutations (69%) than those with A > T transversion (45%) and no mutation (0%) (Table 2). Tumors with TP53 mutations were supposed to be more invasive than those without mutations.
UTUC patients were under risks of bladder recurrence and contralateral recurrence after nephroureterectomy. Pathological characteristics and tumor location might help identify patients who are at risk. In this study, TP53 mutation pattern further stratified those at risk of bladder recurrence or contralateral upper tract recurrence and facilitated decisions regarding individualized follow-up protocols. Importantly, tumor DNA sequencing is not complex, although predictive values should not be overlooked.
Compared with the current published UTUC series with results of bladder outcome, most of clinicopathological characters, such as tumor stages, multi-focality, tumor location, bladder recurrence rate excluding patients with previous bladder cancer histories were similar to our series (Table 4) [21, 22]. Therefore, the findings of our study could be further extended to other population.
Table 4: Comparison of clinicopathological presentation of western UTUC series and our series
Series |
Countries |
Case number |
Ta-1 proportion |
High grade |
Multifocality |
Renal pelvis location |
Bladder recurrence* |
|---|---|---|---|---|---|---|---|
Zigeuner et al.22 |
Austria |
191 |
51.3% |
50.5% |
33.0% |
64.4% |
32.0% |
Novara et al.21 |
Italy |
231 |
46.3% |
(G3) 48.5% |
39.0% |
64.9% |
35.6% |
Our large cohort25 |
Taiwan |
538 |
46.6% |
57.2% |
21.0% |
68.0% |
30.4% |
Current study |
Taiwan |
165 |
50.9% |
71.5% |
30.9% |
65.5% |
32.2% |