
INTRODUCTION
Autoimmune diseases (ADs) are some complex disorders includes a substantial portion of pathobiology, the potential inheritance and induced environment, efficacy of the common therapies and co-occurrence among diseases. ADs accounted for 4-5% of the population and had always become difficult issues [1]. More recently, genome-wide association study (GWAS) and the sequencing approaches had been widely used to discover low-frequency disease risk alleles, and thousands susceptibility locis might predispose to multiple ADs. An expected observation for risk variants are shared across diseases. Colocalized genetic effects had enlighted a common pathway to interfere with pathobiology underlying defect immune functions [2, 3]. Several genes are associated in multiple ADs and are included in the shared network [3, 4].
The studied variant rs1801274 in FCGR2A had been reported and it was associated with the susceptibility to multiple autoimmune diseases, including systemic lupus erythematosus (SLE), Kawasaki disease (KD), diabetes mellitus type 1 (T1D), autoimmune thyroid disease (ATD), ulcerative colitis (UC), Crohn’s disease (CD), rheumatoid arthritis (RA) [5-11], etc. However, the inadequate statistical data, ethnic differences or publication bias resulting in the controversial and inconclusive in different case-control studies. Here, we performed a meta-analysis to evaluate between FCGR2A rs1801274 polymorphisms and the susceptibility to multiple ADs.
RESULTS
Studies included in the meta-analysis
A total of 43 relevant studies with the FCGR2A rs1801274 polymorphism and autoimmune diseases were identified through PubMed and Web of Science search, and 17 articles included KD [6, 16-21], UC [9, 10, 22, 23], CD [7, 10, 22, 24], ATD [8], RA [7, 25], T1D [7] and SLE [26, 27] met the inclusion criteria for analysis. And 8 articles included multiple case-control studies in different autoimmune diseases or different populations. Overall, 30 eligible case-control comparisons including 16760 ADs and 30585 controls were enrolled in the meta-analysis. The ethnicities encompassed in qualified studies were stratified into Caucasian, non-Caucasian European, African-American, and Asian populations. The characteristics of the selected studies were summarized in (Supplementary Table S1)
The results revealed significant association between FCGR2A rs1801274 A-allele and KD (OR = 1.409, 95% CI: 1.320-1.505, P < 0.001) and UC (OR = 1.237, 95% CI: 0.968-1.581, P < 0.001). In KD, significant association were observed in the population of Caucasian (OR = 1.466, 95% CI: 1.276-1.685, P < 0.001) and Asia population(OR = 1.395, 95% CI: 1.285-1.515, P < 0.001). For UC, significant association was found in Asia population (OR = 1.480, 95% CI: 1.356-1.615, P < 0.001) (Table 1).
The summary of meta-analysis for the FCGR2A rs1801274 polymorphism with autoimmune diseases was shown in Table 2. The results were showed no significant association between FCGR2A rs1801274 with susceptibility to these all phenotypes in overall populations. Additionally, sub-group analysis were also performed in the study. In Asian population, increased risk of ADs in the allelic (OR = 1.378, 95% CI: 1.287-1.475, P = 0.000), homozygous (OR = 1.866, 95% CI: 1.631-2.135, P = 0.001), dominant (OR = 1.667, 95% CI: 1.462-1.901, P = 0.000) and recessive (OR = 1.434, 95% CI: 1.319-1.559, P = 0.000) were found . In African-American population, decreased risk of AD was detected in the allelic (OR = 0.882, 95% CI: 0.800-0.972, P = 0.011), homozygous (OR = 0.777, 95% CI: 0.638-0.947, P = 0.013), dominant (OR = 0.850, 95% CI: 0.733-0.986, P = 0.032) and recessive (OR = 0.840, 95% CI: 0.707-0.999, P = 0.048). However, no significant association was found when all the contrasts were performed in Caucasian and non-Caucasian Europe populations.
Table 1: Meta-analysis of the FCGR2A rs1801274 polymorphism in autoimmune diseases.
Diseases |
Comparison |
Population |
Sample size |
Study number |
Test of association (A vs G) |
Model |
Test of heterogeneity |
||||
OR (95% CI) |
Z |
P Value |
Q |
P Value |
I2 (%) |
||||||
KD |
A vs G |
Overall |
17865 |
10 |
1.409(1.320-1.505) |
10.23 |
<0.001 |
R |
9.53 |
0.39 |
5.6 |
Caucasian |
6754 |
2 |
1.466(1.276-1.685) |
5.39 |
<0.001 |
R |
0.10 |
0.751 |
0 |
||
Asian |
11111 |
8 |
1.395(1.285-1.515) |
7.93 |
<0.001 |
R |
9.05 |
0.249 |
22.6 |
||
UC |
A vs G |
Overall |
9752 |
7 |
1.237(0.968-1.581) |
3.50 |
<0.001 |
R |
34.91 |
0 |
82.8 |
Caucasian |
3238 |
5 |
1.059(0.959-1.169) |
1.13 |
0.257 |
NA |
0 |
NA |
NA |
||
Asian |
5655 |
1 |
1.480(1.356-1.615) |
8.80 |
<0.001 |
F |
2.80 |
0.592 |
0 |
||
Non-Caucasian Europe |
859 |
1 |
0.969(0.801-1.171) |
0.33 |
0.742 |
NA |
0 |
NA |
NA |
||
CD |
A vs G |
Overall |
8136 |
6 |
0.832(0.592-1.168) |
1.06 |
0.288 |
R |
119.99 |
0 |
95.8 |
Caucasian |
5578 |
3 |
0.709(0.363-1.382) |
1.01 |
0.312 |
R |
115.24 |
0 |
98.3 |
||
Non-Caucasian Europe |
1324 |
2 |
0.937(0.804-1.093) |
0.83 |
0.407 |
F |
0.10 |
0.747 |
0 |
||
Asian |
1234 |
1 |
1.043(0.867-1.253) |
0.44 |
0.657 |
NA |
0.00 |
NA |
NA |
||
RA |
A vs G |
Overall |
2278 |
3 |
1.008(0.493-2.061) |
0.02 |
0.983 |
R |
50.43 |
0 |
96.0 |
Caucasian |
1856 |
2 |
0.875(0.340-2.252) |
0.28 |
0.782 |
R |
37.42 |
0 |
97.3 |
||
Asian |
422 |
1 |
1.358(0.965-1.909) |
1.76 |
0.079 |
NA |
0 |
NA |
NA |
||
SLE |
A vs G |
Overall |
4366 |
2 |
0.941(0.864-1.025) |
1.39 |
0.165 |
R |
7.53 |
0.06 |
86.7 |
AA vs GG |
Overall |
4366 |
2 |
0.886(0.743-1.057) |
1.34 |
0.179 |
R |
8.28 |
0.004 |
87.9 |
|
AA + AG vs GG |
Overall |
4366 |
2 |
0.914(0.797-1.049) |
1.28 |
0.200 |
R |
6.55 |
0.01 |
84.7 |
|
AG + GG vs AA |
Overall |
4366 |
2 |
1.072(0.932-1.234) |
0.97 |
0.330 |
R |
4.22 |
0.04 |
76.3 |
|
KD, Kawasaki disease; UC, Ulcerative colitis; CD, Crohn’s disease; RA, rheumatoid arthritis; SLE, Systemic lupus erythematosus; HWE, Hardy–Weinberg equilibrium; OR, odds ratio; CI, confidence interval; F, fixed-effects model; R, random-effects model; NA, not applicable.
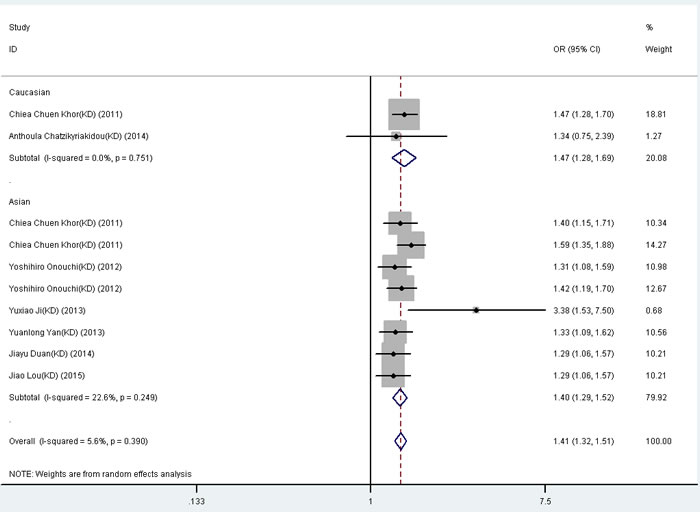
Figure 1: Forest plot for the meta-analysis of association between FCGR2A rs1801274 polymorphism and kawasaki disease (KD) stratified by the ethnicity of study population. ORs and 95% CIs for the outcomes of the allelic comparison in the overall population (P < 0.001, OR = 1.41, 95% CI = 1.32-1.51) and Caucasians (P < 0.001, OR = 1.47, 95% CI = 1.28-1.69).
Test of heterogeneity
As shown in Table 1, the P value for the distribution of genotype for HWE in the control groups was calculated. Only one study in control population was not consistent with HWE. However, when studies were omitted individually from the meta-analysis to evaluate possible individual influences, heterogeneity disappear in CD and RA.
Then we pooled results according to the ethnicity of study populations. Heterogeneity was found for the FCGR2A rs1801274 A-allele and CD in Caucasian population. The study with the highest OR were then excluded, and the heterogeneity disappeared but the result remained none significant (OR = 1.067, 95% CI: 0.995-1.143, P = 0.258).
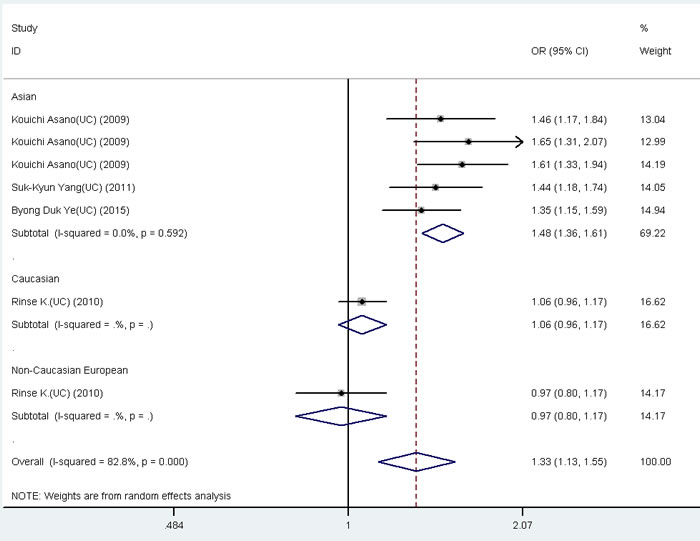
Figure 2: Forest plot for the meta-analysis of association between FCGR2A rs1801274 polymorphism and ulcerative colitis (UC). ORs and 95% CIs for the outcomes of the allelic comparison in the overall population (P < 0.001, OR = 1.33, 95% CI = 1.13-1.55) and Asian (P < 0.001, OR = 1.48, 95% CI = 1.36-1.61).
Publication bias
Publication bias analysis on KD, UC, CD and overall phenotypes were performed . but not on RA, SLE, ATD and T1D due to small numbers of these studies. No obvious asymmetry evidence was detected according to the shapes of the funnel plots (data not shown).
No evidence of publication bias by the method of Egger’s test and Begg’s tests (Table 2) were found. However, there was evidence of heterogeneity in this study. Assessment of potential sources of heterogeneity, by both stratified and meta-regression analyses, found that sample size, ethnicity, publication year or disease phenotype was unable to explain the variance. The results suggested that these potential factors were probably not the major sources of heterogeneity (data not shown).
Table 2: Meta-analysis of the association between the FCGR2A rs1801274 polymorphism and multiple autoimmune diseases.
Comparison |
Population |
No. of studies |
Test of association (A vs G) |
Model |
Test of heterogeneity |
Publication bias |
||||
OR (95% CI) |
Z |
P Value |
P Value |
I2 (%) |
Begg |
Egger |
||||
A vs G |
Overall |
30 |
1.119(0.984-1.272) |
1.71 |
0.086 |
R |
0 |
94.2 |
0.363 |
0.148 |
Caucasian |
10 |
0.843(0.653-1.088) |
1.31 |
0.189 |
R |
0 |
96.9 |
0.592 |
0.542 |
|
Asian |
16 |
1.378(1.287-1.475) |
9.23 |
0 |
R |
0.034 |
43.3 |
0.471 |
0.132 |
|
Non-Caucasian Europe |
3 |
0.949(0.843-1.070) |
0.85 |
0.395 |
F |
0.916 |
0 |
1 |
0.581 |
|
African-American |
1 |
0.882(0.800-0.972) |
2.53 |
0.011 |
NA |
NA |
NA |
NA |
NA |
|
AA vs GG |
Overall |
30 |
1.237(0.968-1.581) |
1.70 |
0.090 |
R |
0 |
92.0 |
0.232 |
0.068 |
Caucasian |
10 |
0.745(0.466-1.192) |
1.23 |
0.220 |
R |
0 |
96.2 |
0.592 |
0.579 |
|
Asian |
16 |
1.866(1.631-2.135) |
9.08 |
0 |
F |
0.751 |
0 |
0.322 |
0.071 |
|
Non-Caucasian Europe |
3 |
0.901(0.71-1.145) |
0.85 |
0.396 |
F |
0.917 |
0 |
1 |
0.585 |
|
African-American |
1 |
0.777(0.638-0.947) |
2.50 |
0.013 |
NA |
NA |
NA |
NA |
NA |
|
AA + AG vs GG |
Overall |
30 |
1.186(0.998-1.409) |
1.94 |
0.052 |
R |
0 |
87.1 |
0.148 |
0.036 |
Caucasian |
10 |
0.839(0.613-1.148) |
1.10 |
0.272 |
R |
0 |
93.8 |
0.858 |
0.640 |
|
Asian |
16 |
1.667(1.462-1.901) |
7.64 |
0.000 |
F |
0.97 |
0 |
0.126 |
0.118 |
|
Non-Caucasian Europe |
3 |
0.933(0.764-1.139) |
0.68 |
0.497 |
F |
0.946 |
0 |
1 |
0.602 |
|
African-American |
1 |
0.850(0.733-0.986) |
2.15 |
0.032 |
NA |
NA |
NA |
NA |
NA |
|
AG + GG vs AA |
Overall |
30 |
1.115(0.949-1.311) |
1.32 |
0.186 |
R |
0.000 |
92.6 |
0.532 |
0.649 |
Caucasian |
10 |
0.780(0.552-1.102) |
1.41 |
0.159 |
R |
0.000 |
95.9 |
0.858 |
0.535 |
|
Asian |
16 |
1.434(1.319-1.559) |
8.45 |
0.000 |
R |
0.032 |
43.7 |
0.589 |
0.257 |
|
Non-Caucasian Europe |
3 |
0.933(0.7721.129) |
0.71 |
0.478 |
F |
0.941 |
0 |
1 |
0.563 |
|
African-American |
1 |
0.840(0.707-0.999) |
1.97 |
0.048 |
NA |
NA |
NA |
NA |
NA |
|
HWE, Hardy–Weinberg equilibrium; OR, odds ratio; CI, confidence interval; F, fixed-effects model; R, random-effects model; NA, not applicable.
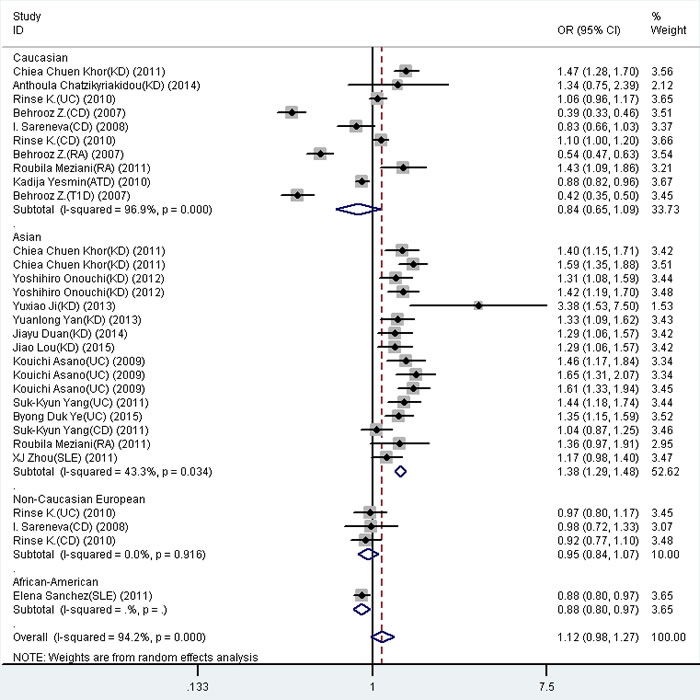
Figure 3: Forest plot for the meta-analysis of association between FCGR2A rs1801274 polymorphism and autoimmune diseases stratified by the ethnicity. ORs and 95% CIs for the outcomes of the allelic comparison in the overall population (P = 0.086, OR = 1.12, 95% CI = 0.98-1.27) and Asian (P < 0.001, OR = 1.38, 95% CI = 1.29-1.48).
DISCUSSION
ADs invokeed a wide spectrum of signs and symptoms, genetic analysis revealed multiple genes underlying distinct autoimmune conditions, which provided direct evidence that might have common immunopathologic mechanism.
FCGR2A gene was located on chromosome 1q23, which consists of 7 exons spanning approximately 18.58 kb of genomic DNA. It encodes a member of a family of Fc γ receptors for immunoglobulin G. FCGR2A protein played an essential role in the protection against foreign antigens by removing antigen-antibody complexes in the circulation, and transduces activating signals into cells via immune receptor when ligated with immune complexes [28]. This stimulatory receptor was expressed by most leukocytes, including monocytes, dendritic cells, macrophages, natural killer cells, platelets and endothelial cells, and a subpopulation of T-cells. Upon binding of antibodies or autoantibodies, FCGR2A and FCGR3A activate immune cell functions, including phagocytosis, and the release of inflammatory mediators, were therefore linked to the pathogenic consequences which triggered by autoantibodies or immune complexes in multiple immune-mediated diseases [29].
The associated polymorphism FCGR2A rs1801274 was a missense variant leading to an amino-acid substitution of histidine by arginine at position 131 (H131R). The variant H131R was reported to interact differently with immunoglobulin G subclasses, and associated with the susceptibility to multiple autoimmune diseases. Specifically, the substitution of FCGR2A rs1801274 affected the Fc region of IgG receptor and determined the affinity of FCGR2A for IgG subclasses. This variant was capable of binding to and mediating phagocytosis with IgG2, potentially leading to altered immune response to infectious agents and activation of B cells and overproduction of cytokines [30].
However, owing to low prevalence or the inadequate statistical power, the discrepancy of the results was always achieved among different studies. Meta-analysis was a method of increasing the effective sample size through the pooling of datas from individual studies, thus enhancing the statistical power of the analysis for the estimation of genetic effect [31].
The results of the meta-analysis revealed significant association between the FCGR2A rs1801274 polymorphism and autoimmune diseases including KD and UC, indicating a protecting effect to KD and predisposing to UC, FCGR2A rs1801274 polymorphism might have no effect on CD or RA. However, the exact biological mechanism that the FCGR2A gene polymorphisms influence susceptibility to ADs remains unclear.
The significant association between FCGR2A rs1801274 polymorphism susceptibility to ADs in the overall population was failed to detect. Sub-population analysis revealed association between different genotypes and Asia population. The AD risk increased significantly in Asia populations using allelic, homozygous, recessive and dominant genetic models. Further studies including larger sample size, well-designed case-control studies in different ethnic populations will be needed to unravel their exact roles in the pathogenesis of multiple ADs.
Several limitations of the present meta-analysis should be showed. First, for several autoimmune diseases, the number of studies is small, and this might cause insufficient power to detect slight association. Second, significant heterogeneity between-study was found in some comparisons. Third, the majority of the included studies were conducted in population of Caucasian and Asia, thus further studies in other ethnic populations were required. Fourth, the present meta-analysis was based on uncorrected estimates. A more precise analysis could be performed if the potential confounding factors including sex, age, environmental factors and other lifestyle factors were available. Thus, the results of the meta-analysis should be interpreted with caution.
In summary, the meta-analysis demonstrated that the FCGR2A rs1801274 polymorphism was associated with the susceptibility to multiple autoimmune diseases including KD and UC. It also provided evidence that the FCGR2A rs1801274 polymorphism may be associated with susceptibility to multiple ADs in Asia population. The FCGR2A rs1801274 polymorphism in multiple autoimmune diseases provides further evidence supporting the concept of common gene underlying multiple autoimmune diseases. Further studies including larger sample size, well-designed case-control studies in different ethnic populations will be needed to unravel their exact roles in the pathogenesis of multiple ADs.
MATERIALS and methods
A comprehensive search examining the association between the FCGR2A rs1801274 polymorphism with autoimmune diseases were conducted. by searching the following Medical Subject Heading (MeSH) terms and/or text words: ‘‘Fc fragment of IgG, low-affinity IIa, receptor’’, ‘‘FCGR2A’’, ‘‘polymorphism’’, ‘‘autoimmune diseases’’, and ‘‘autoimmunity’’ in PubMed and Web of Science literature base for the period up to 2015-12-01, and relevant articles were identified for further literature filtering. A study was included if the following criteria were satisfied (1) case-control genetic association study published before June 2015; (2) genotype frequencies in the cases group and controls group were both available for estimating an odds ratios (OR) and their 95% confidence interval (CI). The exclusion criteria included: (1) studies that contained overlapping data with other literatures; (2) studies which the genotype or allele frequency could not be obtained; (3) data came from case-reports, reviews or abstracts; (4) control group did not confirm to Hardy-Weinberg equilibrium (HWE).
The following information from each study were extracted: first author’s name, publication year, country, ethnicity, genotype-methods, the number of cases and controls and allele frequencies of the FCGR2A rs1801274 polymorphism. Data extraction was performed independently by two authors, and disagreements were solved by discussion.
Statistical analysis for the meta-analysis was conducted by Stata version 10.0 (Stata Corporation, College Station, TX). This meta-analysis examined the contrast of G versus A (allelic contrast), GG versus AA (homozygote contrast), G/G+G/A versus AA (dominant models), G/G versus A/A+G/A (recessive models). The heterogeneity between studies was evaluated by Cochrane’s Q-statistic as well as I2-statistic which was used to quantify the effect of heterogeneity (I2 = 100% (Q-df)/Q) [12]. Subgroup analysis stratified by ethnicity were also performed in this meta-analysis. Meta-regression analysis was undertaken to explore potential sources of heterogeneity across studies when statistical heterogeneity was detected.
The funnel plot was used to assess potential publication bias [13]. Egger’s test and Begg’s tests were performed to evaluate potential publication bias of the literatures [14, 15]. The significance of the intercept was calculated by the t-test suggested by Egger, P value less than 0.05 was considered significant publication bias.
CONFLICTS OF INTEREST
The authors declare there are no conflicts of interests.
REFERENCES
1. Vyse TJ , Todd JA. Genetic analysis of autoimmune disease. Cell. 1996;85:311-8.
2. Tait KF, Marshall T, Berman J, Carr-Smith J, Rowe B, Todd JA, Bain SC, Barnett AH, Gough SC. Clustering of autoimmune disease in parents of siblings from the Type 1 diabetes Warren repository. Diabet Med. 2004;21:358-62.
3. Lettre G , Rioux JD. Autoimmune diseases: insights from genome-wide association studies. Hum Mol Genet. 2008;17:R116-21.
4. Hunt KA, Zhernakova A, Turner G, Heap GA, Franke L, Bruinenberg M, Romanos J, Dinesen LC, Ryan AW, Panesar D, Gwilliam R, Takeuchi F, McLaren WM et al. Newly identified genetic risk variants for celiac disease related to the immune response. Nat Genet. 2008;40:395-402.
5. Harley JB, Alarcon-Riquelme ME, Criswell LA, Jacob CO, Kimberly RP, Moser KL, Tsao BP, Vyse TJ, Langefeld CD, Nath SK, Guthridge JM, Cobb BL, Mirel DB et al. Genome-wide association scan in women with systemic lupus erythematosus identifies susceptibility variants in ITGAM, PXK, KIAA1542 and other loci. Nat Genet. 2008;40:204-10.
6. Khor CC, Davila S, Breunis WB, Lee YC, Shimizu C, Wright VJ, Yeung RS, Tan DE, Sim KS, Wang JJ, Wong TY, Pang J, Mitchell P et al. Genome-wide association study identifies FCGR2A as a susceptibility locus for Kawasaki disease. Nat Genet. 2011;43:1241-6.
7. Alizadeh BZ, Valdigem G, Coenen MJ, Zhernakova A, Franke B, Monsuur A, van Riel PL, Barrera P, Radstake TR, Roep BO, Wijmenga C, Koeleman BP. Association analysis of functional variants of the FcgRIIa and FcgRIIIa genes with type 1 diabetes, celiac disease and rheumatoid arthritis. Hum Mol Genet. 2007;16:2552-9.
8. Yesmin K, Hargreaves C, Newby PR, Brand OJ, Heward JM, Franklyn JA, Gough SC, Simmonds MJ. Association of FcGRIIa with Graves’ disease: a potential role for dysregulated autoantibody clearance in disease onset/progression. Clin Endocrinol. (Oxf) 2010;73:119-25.
9. Asano K, Matsushita T, Umeno J, Hosono N, Takahashi A, Kawaguchi T, Matsumoto T, Matsui T, Kakuta Y, Kinouchi Y, Shimosegawa T, Hosokawa M, Arimura Y et al. A genome-wide association study identifies three new susceptibility loci for ulcerative colitis in the Japanese population. Nat Genet. 2009;41:1325-9.
10. Weersma RK, Crusius JB, Roberts RL, Koeleman BP, Palomino-Morales R, Wolfkamp S, Hollis-Moffatt JE, Festen EA, Meisneris S, Heijmans R, Noble CL, Gearry RB, Barclay ML et al. Association of FcgR2a, but not FcgR3a, with inflammatory bowel diseases across three Caucasian populations. Inflamm Bowel Dis. 2010;16:2080-9.
11. Hughes LB, Criswell LA, Beasley TM, Edberg JC, Kimberly RP, Moreland LW, Seldin MF, Bridges SL. Genetic risk factors for infection in patients with early rheumatoid arthritis. Genes Immun. 2004;5:641-7.
12. Higgins JP , Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539-58.
13. Sterne JA, Egger M, Smith GD. Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ. 2001;323:101-5.
14. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629-34.
15. Begg CB , Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088-101.
16. Onouchi Y, Ozaki K, Burns JC, Shimizu C, Terai M, Hamada H, Honda T, Suzuki H, Suenaga T, Takeuchi T, Yoshikawa N, Suzuki Y, Yasukawa K et al. A genome-wide association study identifies three new risk loci for Kawasaki disease. Nat Genet. 2012;44:517-21.
17. Ji Y, Zhang H , Lin S. Single nucleotide polymorphism of FCGR2A gene in Han Chinese children with Kawasaki disease. Chinese Journal of Contemporary Pediatrics. 2013:196-200.
18. Duan J, Lou J, Zhang Q, Ke J, Qi Y, Shen N, Zhu B, Zhong R, Wang Z, Liu L, Wu J, Wang W, Gong F et al. A genetic variant rs1801274 in FCGR2A as a potential risk marker for Kawasaki disease: a case-control study and meta-analysis. PLoS One. 2014;9:e103329.
19. Yan Y, Ma Y, Liu Y, Hu H, Shen Y, Zhang S, Tao D, Wu Q, Peng Q, Yang Y. Combined analysis of genome-wide-linked susceptibility loci to Kawasaki disease in Han Chinese. Hum Genet. 2013;132:669-80.
20. Chatzikyriakidou A, Aidinidou L, Giannopoulos A, Papadopoulou-Legbelou K, Kalinderi K, Fidani L. Absence of association of FCGR2A gene polymorphism rs1801274 with Kawasaki disease in Greek patients. Cardiol Young. 2015;25:681-3.
21. Lou J, Zhong R, Shen N, Lu X, Ke J, Duan J, Qi Y, Wang Y, Zhang Q, Wang W, Gong F, Miao X. Systematic confirmation study of GWAS-identified genetic variants for Kawasaki disease in a Chinese population. Sci Rep. 2015;5:8194.
22. Yang SK, Jung Y, Kim H, Hong M, Ye BD, Song K. Association of FCGR2A, JAK2 or HNF4A variants with ulcerative colitis in Koreans. Dig Liver Dis. 2011;43:856-61.
23. Ye BD, Choi H, Hong M, Yun WJ, Low HQ, Haritunians T, Kim KJ, Park SH, Lee I, Bang SY, Kim TH, Shin HD, Kang D et al. Identification of Ten Additional Susceptibility Loci for Ulcerative Colitis Through Immunochip Analysis in Koreans. Inflamm Bowel Dis. 2016;22:13-9.
24. Sareneva I, Koskinen LL, Korponay-Szabo IR, Kaukinen K, Kurppa K, Ziberna F, Vatta S, Not T, Ventura A, Adany R, Pocsai Z, Szeles G, Maki M et al. Linkage and association study of FcgammaR polymorphisms in celiac disease. Tissue Antigens. 2009;73:54-8.
25. Meziani R, Yamada R, Takahashi M, Ohigashi K, Morinobu A, Terao C, Hiratani H, Ohmura K, Yamaguchi M, Nomura T, Vasilescu A, Kokubo M, Renault V et al. A trans-ethnic genetic study of rheumatoid arthritis identified FCGR2A as a candidate common risk factor in Japanese and European populations. Mod Rheumatol. 2012;22:52-8.
26. Zhou XJ, Lv JC, Qin LX, Yang HZ, Yu F, Zhao MH, Zhang H. Is FCGR2A a susceptibility gene to systemic lupus erythematosus in Chinese? Lupus. 2011;20:1198-202.
27. Sanchez E, Comeau ME, Freedman BI, Kelly JA, Kaufman KM, Langefeld CD, Brown EE, Alarcon GS, Kimberly RP, Edberg JC, Ramsey-Goldman R, Petri M, Reveille JD et al. Identification of novel genetic susceptibility loci in African American lupus patients in a candidate gene association study. Arthritis Rheum. 2011;63:3493-501.
28. Nimmerjahn F, Ravetch JV. Fcgamma receptors as regulators of immune responses. Nat Rev Immunol. 2008;8:34-47.
29. Falcini F, Trapani S, Turchini S, Farsi A, Ermini M, Keser G, Khamashta MA, Hughes GR. Immunological findings in Kawasaki disease: an evaluation in a cohort of Italian children. Clin Exp Rheumatol. 1997;15:685-9.
30. Hosgood HD, 3rd, MP Purdue, SS Wang, T Zheng, LM Morton, Q Lan, I Menashe, Y Zhang, JR Cerhan, A Grulich, W Cozen, M Yeager, TR Holford et al. A pooled analysis of three studies evaluating genetic variation in innate immunity genes and non-Hodgkin lymphoma risk. Br J Haematol. 2011;152:721-6.
31. Cen H, Wang W, Leng RX, Wang TY, Pan HF, Fan YG, Wang B, Ye DQ. Association of IFIH1 rs1990760 polymorphism with susceptibility to autoimmune diseases: a meta-analysis. Autoimmunity. 2013;46:455-62.