
INTRODUCTION
Despite the decrease in its incidence and improvements in prognosis, gastric cancer remains the fifth most common malignancy and ranks third in terms of fatality among cancers worldwide, [1] with an especially high incidence in Eastern Asia. [2] Surgical resection is the only possible curative method for gastric cancer, especially for patients with early-stage disease, [3] but because of the high rate of postsurgical recurrence, patients with locally advanced tumors have a rather poor prognosis. [4].
Traditionally, gastric cancer outcomes are predicted on the basis of the TNM staging system, which involves tumor invasion depth, lymph node metastasis, and distant metastasis. However, other clinicopathological factors (e.g., tumor size and Lauren’s classification) that may be associated with prognosis are not considered in the TNM staging system. [5, 6] Further, there is an increasing need to develop more reliable biomarkers to refine the prediction of outcomes for gastric cancer patients. [7].
Previous studies have found a high rate of glucose uptake and lactate production in tumors. [8] According to the Warburg effect, cancer cells conduct anaerobic metabolism rather than aerobic metabolism to produce most of their energy, even under normoxic conditions. On the other hand, hypoxia, a characteristic feature of solid tumors, can facilitate the process of glycolysis as well as cancer proliferation. [9] Thus, in the process of converting glucose to lactate, which is regulated by the lactate dehydrogenase (LDH), cancer cells may protect themselves better from oxidative stress, avoid mitochondria pathway apoptosis, [10] and maintain a higher proliferation rate. Serum LDH (SLDH) levels are known to be an unfavorable prognosticator in many kinds of malignancies, as has been reported in patients with melanomas, [11] lymphoma, [12] myeloma, [13] gastrointestinal malignancies, [14–21] head and neck cancers, [22] lung cancer, [23] breast cancer, [24] renal cancer, [25] prostate cancer, [26] etc. However, only two of these studies are aimed at gastric cancer, and both include patients with advanced gastric cancer. [15, 21, 27] Therefore, studies regarding the prognostic value of SLDH in patients with resectable gastric cancer remain scarce, and preoperative SLDH might be identified as an inexpensive and accessible prognosticator for these patients.
In the present study, we investigated the prognostic significance of preoperative SLDH levels in patients with resected gastric cancer after D2 lymphadenectomy and incorporated these levels into nomograms for predicting the overall survival (OS) and disease-free survival (DFS) among these patients.
RESULTS
Patient characteristics
Table 1 summarizes the patient characteristics. The cohort consisted of 619 patients (409 men and 210 women) with Stage IB–IIIC gastric cancer, 111 (17.9%) of whom had tumors at the gastroesophageal junction. The mean patient age was 57.9 ± 11.7 years. All patients underwent D2 lymphadenectomy; 433 (69.8%) were found to have T3/4-stage disease, and 400 (64.7%) had LN metastasis. More than 15 lymph nodes (LNs) were retrieved from 478 (77.2%) patients and more than 25 LNs from 293 patients (47.3%). Further, 414 (66.8%) patients received adjuvant chemotherapy. The median follow-up time for survivors was 29.1 months (inter-quartile range, 20.7–37.9 months). During follow-up, 161 (26.0%) patients developed locoregional/distant recurrence and 102 (16.6%) died.
Table 1: Patients’ clinicopathologic characteristics
Clinicopathologic Characteristic |
Mean or No. of patients |
SD or % |
|---|---|---|
Age (years) |
57.9 |
11.7 |
≤ 60 |
339 |
54.8% |
> 60 |
280 |
45.2% |
Gender |
||
Male |
409 |
66.1% |
Female |
210 |
33.9% |
Preoperative SLDH (U/L) |
159.6 |
33.1 |
≤ 245 |
611 |
98.7% |
> 245 |
8 |
1.3% |
Tumor Size (cm) |
4.0 |
2.3 |
Tumor Location |
||
GEJ |
111 |
17.9% |
Non-GEJ |
508 |
82.1% |
Differentiation |
||
Moderate/high |
133 |
21.5% |
Poor/low |
486 |
78.5% |
Lauren’s Classification |
||
Diffuse |
303 |
48.9% |
Intestinal |
232 |
37.4% |
Mixed |
84 |
13.6% |
HER2 Status |
||
Negative |
553 |
89.4% |
Positive |
66 |
10.6% |
Lymphovascular Invasion |
||
Yes |
170 |
27.4% |
No |
449 |
72.6% |
Perineural Invasion |
||
Yes |
248 |
40.0% |
No |
371 |
60.0% |
pT |
||
T1 |
103 |
16.7% |
T2 |
83 |
13.4% |
T3 |
296 |
47.7% |
T4 |
137 |
22.1% |
MLN |
4.9 |
7.0 |
N0 |
219 |
35.3% |
N1 |
125 |
20.2% |
N2 |
117 |
18.9% |
N3 |
158 |
25.6% |
THN |
25.0 |
11.6 |
≤15 |
141 |
22.8% |
>15 |
185 |
29.9% |
>25 |
293 |
47.3% |
LNR |
0.2 |
0.2 |
Adjuvant Chemotherapy |
||
Yes |
414 |
66.8% |
No |
205 |
33.2% |
Abbreviations: SD, standard deviation; SLDH, serum lactate dehydrogenase; GEJ, gastroesophageal junction; pT, depth of invasion; MLN, metastatic lymph node; THN, total harvested lymph nodes; LNR, lymph node ratio.
Relationship between SLDH levels and clinicopathological factors in gastric carcinoma
The mean and median preoperative SLDH levels were 159.6 U/L and 157.2 U/L, respectively. High SLDH levels (>245 U/L) were noted in only 8 (1.3%) patients.
The correlation between SLDH level and other clinicopathologic factors is summarized in Tables 2 and 3. No significant differences were found in the SLDH levels depending on gender, tumor location, tumor size, tumor differentiation, Lauren’s classification, HER2 status, pathologic T stage (pT), N stage, lymphovascular invasion, perineural invasion, or receipt of adjuvant chemotherapy. A high SLDH level was found to be correlated with older age (r = 0.228, p < 0.01), but no correlation was found between SLDH level and tumor size, metastatic lymph nodes (MLN), total harvested lymph nodes (THN), or lymph node ratio (LNR).
Table 2: Correlation between SLDH levels and other continuous clinicopathological factors
Correlation |
r |
P* |
|---|---|---|
SLDH vs. age |
0.23 |
< 0.01 |
SLDH vs. tumor size |
−0.08 |
0.35 |
SLDH vs. MLN |
−0.02 |
0.63 |
SLDH vs. THN |
−0.01 |
0.87 |
SLDH vs. LNR |
−0.02 |
0.55 |
Abbreviations: SLDH, serum lactate dehydrogenase; MLN, metastatic lymph node; THN, total harvested lymph node; LNR, lymph node ratio; r, Spearman rank correlation coefficient.
*Measured using the Spearman rank correlation test.
Table 3: Correlation between SLDH levels and other categorical clinicopathological factors
Variable |
SLDH |
P |
|
|---|---|---|---|
mean ± SD |
median (IQR) |
||
Age (years) |
< 0.01a |
||
<60 |
154.4 ± 32.9 |
150.7 (131.9–172.2) |
|
≥60 |
165.9 ± 32.5 |
163.25 (142.1–187.6) |
|
Gender |
0.61a |
||
Male |
159.6 ± 34.4 |
156.2 (136.3–179.9) |
|
Female |
159.6 ± 30.7 |
159.05 (139.4–177.8) |
|
Tumor Location |
0.61a |
||
GEJ |
161.5 ± 29.7 |
158.4 (138.1–180.1) |
|
Non-GEJ |
159.4 ± 33.8 |
156.9 (137.6–178.9) |
|
Differentiation |
0.41a |
||
Moderate/high |
157.8 ± 30.7 |
153.2 (135.2–177.6) |
|
Poor/low |
159.4 ± 33.5 |
156.8 (137.5–178.9) |
|
Lauren’s Classification |
0.17b |
||
Diffuse |
157.6 ± 35.3 |
155.05 (134.4–178.7) |
|
Intestinal |
160.3 ± 30.6 |
157.7 (138.4–178.8) |
|
Mixed |
164.8 ± 32.2 |
161.95 (144.4–183.1) |
|
HER2 Status |
0.58b |
||
Negative |
157.8 ± 34.0 |
155.95 (136.0–178.8) |
|
Positive |
163.5 ±22.1 |
164.3 (148.1–180.6) |
|
Depth of invasion |
0.97a |
||
T1&T2 |
158.1 ± 29.6 |
158.2 (139.1–177.9) |
|
T3&T4 |
160.3 ± 34.6 |
156.5 (136.7–180.2) |
|
Nodal status |
0.60a |
||
Node-negative |
160.0 ± 31.2 |
159.25 (138.4–178.4) |
|
Node-positive |
159.5 ± 34.3 |
155.9 (136.6–179.4) |
|
Lymphovascular Invasion |
0.52a |
||
Yes |
159.8 ± 33.7 |
154.3 (136.5–180.6) |
|
No |
159.6 ± 33.1 |
158.2 (137.9–178.6) |
|
Perineural Invasion |
0.72a |
||
Yes |
160.5 ± 31.1 |
158.5 (137.7–180.6) |
|
No |
158.7 ± 34.3 |
156.5 (137.0–177.7) |
|
Adjuvant Chemotherapy |
0.62b |
||
Yes |
158.9 ± 34.4 |
157.2 (136.8–178.8) |
|
No |
159.0 ± 30.2 |
154.8 (136.1–177.9) |
|
Abbreviations: IQR, interquartile range; SLDH, serum lactate dehydrogenase; SD, standard deviation; GEJ: gastroesophageal junction; pT, depth of invasion; MLN, metastatic lymph node.
a Mann-Whitney U test;
b Kruskal-Wallis test
Survival analysis
The 3-year OS and 3-year DFS for the cohort were 80.2% and 70.0%, respectively. Univariate analysis showed that the SLDH level did not significantly affect OS or DFS when treated as continuous variable (OS: p = 0.087; DFS: p = 0.101) or categorical covariate divided according to the median value (log-rank: OS, p = 0.282; DFS, p = 0.189). However, in multivariate Cox regression models, the SLDH level was found to be an independent unfavorable prognostic factor for OS and DFS (OS: hazard ratio (HR) = 1.009, 95% confidence interval (CI) = 1.003–1.016, p < 0.01; DFS: HR = 1.008, 95% CI = 1.003–1.013, p < 0.01) (Tables 4 and 5). An HR of 1.009 for SLDH level as a continuous variable indicated a 50% increase in the risk of death with each 50 U/L increase in SLDH. A significant interaction was found between male gender and the SLDH level for predicting OS (p = 0.02), which indicated that the effect of SLDH level varied between the genders (Table 6); that is, high SLDH levels were associated with a greater risk of death and recurrence among male patients as compared to female patients (HR for OS: 1.012 vs. 1.000; HR for DFS: 1.009 vs. 1.006) (Tables 4 and 5), although the interaction between gender and SLDH levels was not apparent for prediction of DFS (p = 0.436).
Table 4: Multivariate cox regression model to predict OS
Multivariate analysis |
||||||
|---|---|---|---|---|---|---|
Variable |
All |
Male subgroup |
Female subgroup |
|||
HR (95% CI) |
P |
HR (95% CI) |
P |
HR (95% CI) |
P |
|
Gender |
||||||
Female |
1 |
|||||
Male |
12.416 |
0.026 |
||||
SLDH |
1.009 (1.003–1.016) |
0.007 |
1.012 |
0.001 |
1.000 (0.988–1.012) |
0.971 |
Tumor location |
||||||
GEJ |
1 |
|||||
Non-GEJ |
0.570 (0.363–0.895) |
0.015 |
0.527 (0.314–0.883) |
0.015 |
0.399 (0.166–0.961) |
0.041 |
pT |
||||||
T1&T2 |
1 |
< 0.001 |
1 |
0.002 |
1 |
0.001 |
T3 |
3.563 (1.591–7.978) |
0.002 |
3.514 (1.350–9.150) |
0.010 |
2.344 (0.641–8.576) |
0.198 |
T4 |
7.008 (3.045–16.131) |
< 0.001 |
5.942 (2.193–16.101) |
< 0.001 |
7.325 (2.001–26.816) |
0.003 |
LNR |
6.507 (3.321–12.746) |
< 0.001 |
6.854 (3.109–15.107) |
< 0.001 |
7.594 (2.275–25.351) |
0.001 |
Abbreviations: HR, hazard ratio; SLDH, serum lactate dehydrogenase; pT, depth of invasion; LNR, lymph node ratio; GEJ, gastroesophageal junction.
Bold P values have statistical significance (i.e., P < 0.05).
Table 5: Multivariate cox regression model to predict DFS
Variables |
Multivariate analysis |
|||||
|---|---|---|---|---|---|---|
All |
Male subgroup |
Female subgroup |
||||
HR (95% CI) |
P |
HR (95% CI) |
P |
HR (95% CI) |
P |
|
SLDH |
1.008 (1.003–1.013) |
0.002 |
1.009 (1.003–1.015) |
0.004 |
1.006 (0.997–1.016) |
0.199 |
Tumor location |
||||||
GEJ |
1 |
1 |
1 |
|||
Non-GEJ |
0.528 (0.374–0.747) |
<0.001 |
0.540 (0.356–0.819) |
0.004 |
0.418 (0.205–0.854) |
0.017 |
pT |
||||||
T1&T2 |
1 |
<0.001 |
1 |
<0.001 |
1 |
0.003 |
T3 |
2.621 (1.517–4.528) |
0.001 |
2.907 (1.463–5.777) |
0.002 |
2.035 (0.809–5.118) |
0.131 |
T4 |
4.462 (2.511–7.926) |
<0.001 |
4.430 (2.143–9.160) |
<0.001 |
4.298 (1.659–11.135) |
0.003 |
LNR |
9.738 (5.711–16.603) |
<0.001 |
10.054 (5.179–19.520) |
<0.001 |
9.715 (3.738–25.250) |
<0.001 |
Abbreviation: HR, hazard ratio; SLDH, serum lactate dehydrogenase; pT, depth of invasion; LNR, lymph node ratio; GEJ, gastroesophageal junction.
Bold P values have statistical significance (i.e., P < 0.05).
Table 6: Multivariate cox regression model including interaction effect between gender and sldh to predict OS
Multivariate analysis |
||
|---|---|---|
Variable |
HR (95% CI) |
P value |
Tumor location |
||
GEJ |
1 |
|
Non-GEJ |
0.518 (0.325–0.827) |
0.006 |
pT |
||
T1&T2 |
1 |
< 0.001 |
T3 |
3.581 (1.593–8.050) |
0.002 |
T4 |
7.043 (3.053–16.244) |
< 0.001 |
LNR |
6.621 (3.360–13.046) |
< 0.001 |
Gender* |
- |
0.026 |
SLDH* |
- |
0.001 |
Interaction effect* |
- |
0.016 |
SLDH by gender |
||
SLDH for female |
1.000 |
|
SLDH for male |
1.012 (1.005–1.019) |
0.001 |
Abbreviation: HR, hazard ratio; SLDH, serum lactate dehydrogenase; pT, depth of invasion; LNR, lymph node ratio; GEJ, gastroesophageal junction. * Hazard ratios for gender and SLDH are not shown because significant interaction has been proven between these two variables, indicating that the hazard ratios for SLDH differ according to gender. Accordingly, the hazard ratios for SLDH by gender are presented.
Predictive nomograms for OS and DFS
To develop an intuitive and quantitative method to better stratify patients with different prognoses, nomograms to predict 3-year OS and DFS were developed on the basis of the final models (Figure 1A and 2A). Through RCS examination, both SLDH levels and LNR were found to have a linear effect on the HRs for OS and DFS. The association between SLDH levels and OS differed by gender. For example, a male patient with a preoperative SLDH level of 150 U/L (43 points) and pT3-stage (26 points) gastric cancer of the gastroesophageal junction (15 points) and an LNR of 0.2 (8 points) had a total of 92 points, which yielded an estimated 3-year OS of 78%. If the same patient had an SLDH level of 250 U/L, the total score would increase to 120 points, which yielded an estimated 3-year OS of 43%. In contrast, the estimation would not change drastically according to the SLDH level in a female patient with the same clinicopathologic characteristics (the total score would decrease from 100 to 97 and the estimated 3-year OS would increase from 70% to 72%).
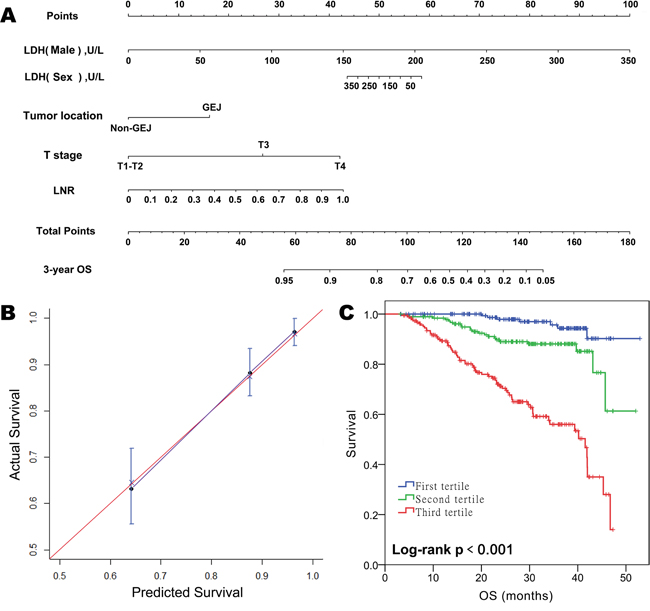
Figure 1: Prognostic nomogram for predicting overall survival (OS) in patients with resectable gastric cancer. A. Predictive nomogram for OS incorporating gender, SLDH levels, and the interaction effect between these two variables along with tumor location, T stage, and LNR. For the factor “SLDH”, the points assigned should be chosen based on whether the patient was male or female. B. Calibration plot for nomogram-predicted OS showing close correlation with the ideal 45-degree reference line. C. Kaplan-Meier curves demonstrating OS in patients grouped according to the tertiles of nomogram-predicted OS. Each group represents a distinct prognosis.
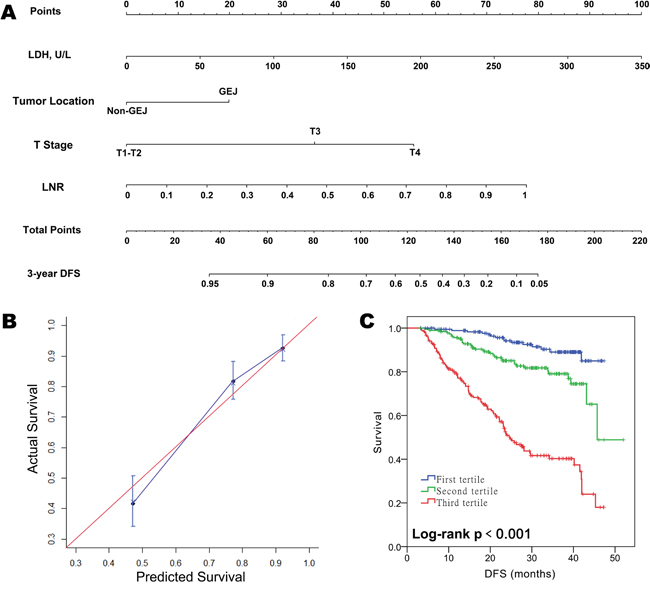
Figure 2: Prognostic nomogram for predicting disease-free survival (DFS) in patients with resectable gastric cancer. A. Predictive nomogram for DFS incorporating SLDH levels along with tumor location, T stage, and LNR. B. Calibration plot for nomogram-predicted DFS showing close correlation with the ideal 45-degree reference line. C. Kaplan-Meier curves demonstrating DFS in patients grouped according to the tertiles of nomogram-predicted DFS. Each group represents a distinct prognosis.
The unadjusted concordance indices (C-indices) for OS and DFS prediction were 0.79 and 0.77, respectively, and the corresponding bootstrap-corrected C-indices were 0.77 and 0.75, indicating minimal evidence of model overfit. The nomograms showed better predictive accuracies than the 7th American Joint Committee on Cancer (AJCC) TNM staging model (unadjusted C-index for OS and DFS: 0.74 and 0.73; p < 0.01 for both, Z test), and the model which incorporates tumor location, pT, LNR, but not SLDH (unadjusted C-index for OS and DFS: 0.77 and 0.75; p < 0.01 for both, Z test). The calibration plot showed excellent predictive accuracy for 3-year OS, as the prediction was similar to the ideal model (the 45-degree ideal reference line). The predictive accuracy for 3-year DFS was also good, with a less than 5% difference between the predicted and actual probabilities in each tertile (Figure 2B). By grouping the patients evenly into three subgroups according to the tertiles of nomogram-predicted OS or DFS, we found that each group had a distinct prognosis (Figure 2C). Collectively, the results showed that the nomograms were suitable for predicting OS and DFS.
DISCUSSION
In the present study, we observed that a high preoperative SLDH level was independently associated with low OS and DFS for patients who had undergone D2 lymphadenectomy, especially male patients. Further, nomograms incorporating SLDH with other clinicopathologic factors (tumor location, pT, and LNR) showed better discrimination than the 7th AJCC staging model and excellent calibration for OS and DFS prediction.
As an enzyme that participates in anaerobic metabolism, LDH may affect tumor malignancy via different mechanisms, including facilitating the proliferation, viability, and invasion capability of cancer cells, [8] and avoiding mitochondrial-mediated apoptosis. [10] In addition, several oncogenes, including HIF-1α and MYC, which are involved in upregulating genes responsible for glycolytic metabolism, angiogenesis, and cell survival, [21] were reported to be targeted by LDH. [28] Previous studies have shown that high SLDH levels are significantly associated with unfavorable prognosis in several gastrointestinal malignancies. [14–21] However, it is noteworthy that these studies were almost exclusively conducted on metastatic/non-resectable gastrointestinal tumor. To our knowledge, the prognostic role of SLDH in gastric cancer has been reported in only two studies [15, 21], and both included patients with advanced gastric cancer. The study by Zhao et al. [21] is the only previous study including patients with stage I–III gastric cancer, and it found that high preoperative SLDH levels were associated with poorer OS and DFS, consistent with our results. This previous study also found that patients with normal but relatively high SLDH levels had poorer outcomes compared with those with normal SLDH levels, which was again in line with the results of our study, in which only 8 (1.3%) patients had SLDH levels exceeding the upper limit of 245 U/L. Actually, we also divided the patients according to the median value of SLDH (157.2 U/L). As a result, normal but relatively high SLDH levels (> 157.2 U/L) were significantly associated with poorer OS (adjusted HR, 1.73; 95% CI, 1.16−2.57; p < 0.01) and DFS (adjusted HR, 1.74; 95% CI, 1.30−2.40; p < 0.01). However, Zhao et al. observed that high SLDH levels were correlated with advanced pT/pN stages but not age, while our study found that they were associated with age but not pT/pN. A reason for this could be the different distribution of clinicopathological factors between the study cohorts. For instance, the proportions of patients with stage I–II disease and those older than 60 years were higher in our cohort (51.4% and 46.8%, respectively) than those in Zhao et al.’s study (16.7% and 38.9%, respectively). In a study by Kostakis et al.,[29] the proportion of patients with stage I–II tumor was 47.5%, and SLDH levels were not found to be correlated with the T/N stage; the relationship between SLDH levels and age was not examined. Moreover, in the study by Zhao et al., [21] the proportions of patients with higher than normal LDH level were comparable among patients with Stage I−III tumor (2.4%−5.3%) but increased remarkably among patients with Stage IV tumor (14.0%). Yet, the authors did not assess the relationship between LDH and pT/pN solely among patients with Stage I−III gastric cancer. Future studies are needed to further demonstrate the relationship between LDH and locoregional cancer burden among patients with gastric cancer.
In the present study, high SLDH levels were associated with a significantly greater increase in the risk of death among male patients as compared to female patients, but the mechanisms underlying this interaction remain unclear. The male hormone androgen did not seem to be related, as older age (>60 years old) did not affect the influence of SLDH level on the risk of death or recurrence in male patients in this study (data not shown). Further, the SLDH level was found to be of prognostic value in patients with castration-resistant prostate cancer. [30, 31] Additional studies are needed to validate the prognostic role of SLDH levels in gastric cancer in male and female patients and to investigate the underlying mechanisms.
Prognostic nomograms are useful tools that allow intuitive individual risk evaluation. [32] A “point” prediction of patient prognosis is available in nomograms, and there is no need to categorize continuous variables—SLDH levels and LNR in the present study. To the best of our knowledge, ours is the first study to incorporate SLDH levels in nomograms predicting OS and DFS in gastric cancer patients who have undergone D2 lymphadenectomy. Our nomograms were more discriminative than the TNM staging. Their accuracies for prediction of OS and DFS were excellent, since nomogram-predicted survival probabilities were similar to actual survival probabilities. Kim et al. [34] constructed nomograms incorporating LNR along with patient age, gender, pT, and tumor site to predict OS and DFS and found that the nomograms had better discriminatory power than both the 7th AJCC staging system and the nomograms established by the Memorial Sloan Kettering Cancer Centre. [32] The nomograms constructed in the present study had an even higher discriminatory power than those of Kim et al. [34] (C-index for OS, 0.77 vs. 0.70; C-index for DFS, 0.75 vs. 0.71), possibly because they included preoperative SLDH levels.
The present study has some limitations. First, SLDH levels may be influenced by comorbidities, such as heart, lung, or liver diseases; hypothyroidism; and anemia, which were not controlled in our study. However, the patients in our study were all eligible for surgery and survived for over 90 days after the operation, which may indicate their relatively good overall health. Second, the median follow-up was 29.1 months (inter-quartile range, 20.7–37.9 months), because of which our data were not useful for long-term survival analysis. However, since the time span was narrow and recent (2011-2013), the treatment strategies were fairly standardized as all patients underwent D2 lymphadenectomy and most received S-1/capecitabine-based adjuvant chemotherapy (67%). Third, like in the previous nomograms [32–38], adjuvant therapy was not identified as a significant prognosticator in the current nomograms. Due to many missing data regarding the cycles of adjuvant chemotherapy and the small size, and the retrospective nature, it is not practical to select candidates for adjuvant chemotherapy using the nomograms in this study. Future studies are needed to demonstrate the use of the current nomograms for patient selection. Fourth, the nomograms were developed from a Chinese cohort, and external validation using datasets from other countries is required.
In conclusion, our study identified the preoperative SLDH level as an unfavorable prognosticator in patients with D2-resected gastric cancer. SLDH levels were incorporated into nomograms along with other clinicopathologic factors in order to refine OS and DFS prediction. The nomograms were bootstrap validated, and once they are externally validated, we believe that they could be useful tools for prognosis, follow-up, and treatment.
MATERIALS AND METHODS
Ethics statement
All patients provided written informed consent for their information to be stored in the hospital database and used. Study approval was obtained from independent ethics committees at the Cancer Center of Sun Yat-sen University. Further, this study was undertaken in accordance with the ethical standards of the World Medical Association Declaration of Helsinki.
Patient selection
Between December 2011 and July 2013, 847 gastric cancer patients who were diagnosed and underwent D2 lymphadenectomy at Cancer Center of Sun Yat-Sen University were identified. Patients included in the study had to meet the following criteria: (1) histologically confirmed IB–IIIC gastric adenocarcinoma; (2) histologically confirmed R0 resection; (3) follow-up data available. The exclusion criteria were as follows: (1) death within 90 days of surgery; (2) residual macroscopic or microscopic tumor, distant metastasis, or concurrent malignancies in other organs; (3) neoadjuvant chemo(radio)therapy or adjuvant radiotherapy. Finally, 619 patients remained in the study cohort.
Clinicopathological data collected for subsequent analysis included gender; age at diagnosis; preoperative SLDH level; tumor size; tumor location; degree of differentiation; Lauren’s classification; HER2 status; pT; MLN and THN; LNR; presence of lymphovascular invasion; and presence of perineural invasion. HER2 status was obtained from previous pathology reports from our center. Cases with an immunohistochemistry (IHC) score of 3 or an IHC score of 2 and a positive fluorescence in situ hybridization score were considered HER2 positive.
The clinical decision to administer postoperative chemotherapy was based on the disease stage, general health, and the patient’s preference. The chemotherapy regimens included single fluoropyrimidine regimens (S-1/capecitabine) and S-1/capecitabine-based combinations (S-1/capecitabine plus oxaliplatin/taxol/paclitaxel).
Statistical analysis
Analysis was performed using SPSS 19.0 and R 3.1.2 (http://www.r-project.org/) statistical packages. Categorical variables were reported as numbers (percentage), and continuous variables as means with standard deviations. The correlation between SLDH levels and other continuous variables was assessed using the Spearman correlation analysis, and the relationship between SLDH and categorized variables was evaluated using the t-test/Analysis of Variance or Mann-Whitney U test/Kruskal-Wallis test. OS was measured between the date of surgery until death from any cause, and DFS was defined as the time from surgery to recurrence or death. Kaplan-Meier analysis and univariate and multivariate Cox regression analyses were performed to assess the association between clinicopathological factors and OS/DFS.
Previous studies have demonstrated that LNR, which accounted for both the number of metastatic and examined nodes, can compensate for the stage migration effect on survival in gastric cancer surgery [39], and improve the predictive accuracy of survival as compared with pN or number of metastatic nodes [40]. Moreover, as the number of metastatic nodes and LNR was highly correlated with each other, it would cause multicollinearity if they were included simultaneously in the Cox regression model [41]. Therefore, we used LNR instead of pN or number of metastatic nodes for model development. Restricted cubic splines (RCS) were used to examine the proportional hazards assumption and linearity assumption for continuous variables [33, 42]. An appropriate transformation was selected when a continuous variable failed to satisfy the proportional hazards assumption or linearity assumption. For model development, we began with SLDH and all other accounted variables, with or without the first-order interaction terms between SLDH and other accounted variables. The final Cox models were obtained by using backward stepwise selection of the variables (keeping only those with P < 0.05). A nomogram to predict individual survival was constructed on the basis of the final Cox model. The comparative discriminative power of the nomogram and other staging systems was assessed using the C-index: [43] the higher the C-index, the more accurate was the prognostic prediction. [34] Nomogram calibration was assessed by reviewing the plot of nomogram-predicted survival probabilities versus the Kaplan-Meier-estimated probabilities. [44] Bootstraps with 1000 resamples were used to quantify any model overfit and calculate the Kaplan-Meier-estimates.
ACKNOWLEDGMENTS
We gratefully thank the staff members in the Department of Medical Oncology at Sun Yat-sen University Cancer Center for their suggestion and assistance.
CONFLICTS OF INTEREST
The authors have declared no conflicts of interest.
REFERENCES
1. Ferlay J SI, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No. 11. Lyon, France: International Agency for Research on Cancer. 2013. Available at: http://globocan.iarc.fr.
2. Chen W, Zheng R, Zeng H, Zhang S. The updated incidences and mortalities of major cancers in China, 2011. Chin J Cancer. 2015; 34: 53.
3. Dikken JL, van de Velde CJ, Coit DG, Shah MA, Verheij M, Cats A. Treatment of resectable gastric cancer. Therap Adv Gastroenterol. 2012; 5: 49-69.
4. Rivera F, Vega-Villegas ME, Lopez-Brea MF. Chemotherapy of advanced gastric cancer. Cancer Treat Rev. 2007; 33: 315-324.
5. Deng J, Zhang R, Pan Y, Ding X, Cai M, Liu Y, Liu H, Bao T, Jiao X, Hao X, Liang H. Tumor size as a recommendable variable for accuracy of the prognostic prediction of gastric cancer: a retrospective analysis of 1,521 patients. Ann Surg Oncol. 2015; 22: 565-572.
6. Qiu MZ, Cai MY, Zhang DS, Wang ZQ, Wang DS, Li YH, Xu RH. Clinicopathological characteristics and prognostic analysis of Lauren classification in gastric adenocarcinoma in China. J Transl Med. 2013; 11: 58. doi: 10.1186/1479-5876-11-58.
7. Wang X, Zhang H, He H, Shen Z, Tang Z, Xu J, Sun Y. Prognostic value of stromal cell-derived factor 1 expression in patients with gastric cancer after surgical resection. Cancer Sci. 2014; 105: 1447-1456.
8. Sun X, Sun Z, Zhu Z, Guan H, Zhang J, Zhang Y, Xu H, Sun M. Clinicopathological significance and prognostic value of lactate dehydrogenase A expression in gastric cancer patients. PLoS One. 2014; 9: e91068.
9. Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science. 2009; 324: 1029-1033.
10. Yao F, Zhao T, Zhong C, Zhu J, Zhao H. LDHA is necessary for the tumorigenicity of esophageal squamous cell carcinoma. Tumour Biol. 2013; 34: 25-31.
11. Garbe C, Peris K, Hauschild A, Saiag P, Middleton M, Spatz A, Grob JJ, Malvehy J, Newton-Bishop J, Stratigos A, Pehamberger H, Eggermont AM. Diagnosis and treatment of melanoma. European consensus-based interdisciplinary guideline--Update. 2012. Eur J Cancer. 2012; 48: 2375-2390.
12. Park JH, Yoon DH, Kim DY, Kim S, Seo S, Jeong Y, Lee SW, Park CS, Huh J, Suh C. The highest prognostic impact of LDH among International Prognostic Indices (IPIs): an explorative study of five IPI factors among patients with DLBCL in the era of rituximab. Ann Hematol. 2014; 93: 1755-1764.
13. Kiba T, Ito T, Nakashima T, Okikawa Y, Kido M, Kimura A, Kameda K, Miyamae F, Tanaka S, Atsumi M, Sumitani Y, Shitakubo Y, Niimi H. Bortezomib and dexamethasone for multiple myeloma: higher AST and LDH levels associated with a worse prognosis on overall survival. BMC Cancer. 2014; 14: 462. doi: 10.1186/1471-2407-14-462.
14. Tas F, Karabulut S, Ciftci R, Sen F, Sakar B, Disci R, Duranyildiz D. Serum levels of LDH, CEA, and CA19-9 have prognostic roles on survival in patients with metastatic pancreatic cancer receiving gemcitabine-based chemotherapy. Cancer Chemother Pharmacol. 2014; 73: 1163-1171.
15. Sougioultzis S, Syrios J, Xynos ID, Bovaretos N, Kosmas C, Sarantonis J, Dokou A, Tzivras D, Zografos G, Felekouras E, Papalambros E, Tsavaris N. Palliative gastrectomy and other factors affecting overall survival in stage IV gastric adenocarcinoma patients receiving chemotherapy: a retrospective analysis. Eur J Surg Oncol. 2011; 37: 312-318.
16. Chibaudel B, Bonnetain F, Tournigand C, Bengrine-Lefevre L, Teixeira L, Artru P, Desrame J, Larsen AK, Andre T, Louvet C, de Gramont A. Simplified prognostic model in patients with oxaliplatin-based or irinotecan-based first-line chemotherapy for metastatic colorectal cancer: a GERCOR study. Oncologist. 2011; 16: 1228-1238.
17. Haas M, Laubender RP, Stieber P, Holdenrieder S, Bruns CJ, Wilkowski R, Mansmann U, Heinemann V, Boeck S. Prognostic relevance of CA 19-9, CEA, CRP, and LDH kinetics in patients treated with palliative second-line therapy for advanced pancreatic cancer. Tumour Biol. 2010; 31: 351-357.
18. Scartozzi M, Giampieri R, Maccaroni E, Del Prete M, Faloppi L, Bianconi M, Galizia E, Loretelli C, Belvederesi L, Bittoni A, Cascinu S. Pre-treatment lactate dehydrogenase levels as predictor of efficacy of first-line bevacizumab-based therapy in metastatic colorectal cancer patients. Br J Cancer. 2012; 106: 799-804.
19. Haas M, Heinemann V, Kullmann F, Laubender RP, Klose C, Bruns CJ, Holdenrieder S, Modest DP, Schulz C, Boeck S. Prognostic value of CA 19-9, CEA, CRP, LDH and bilirubin levels in locally advanced and metastatic pancreatic cancer: results from a multicenter, pooled analysis of patients receiving palliative chemotherapy. J Cancer Res Clin Oncol. 2013; 139: 681-689.
20. Yin C, Jiang C, Liao F, Rong Y, Cai X, Guo G, Qiu H, Chen X, Zhang B, He W, Xia L. Initial LDH level can predict the survival benefit from bevacizumab in the first-line setting in Chinese patients with metastatic colorectal cancer. Onco Targets Ther. 2014; 7: 1415-1422. doi: 10.2147/OTT.S64559.
21. Zhao Z, Han F, Yang S, Hua L, Wu J, Zhan W. The clinicopathologic importance of serum lactic dehydrogenase in patients with gastric cancer. Dis Markers. 2014: 140913. doi: 10.1155/2014/140913.
22. Zhou GQ, Tang LL, Mao YP, Chen L, Li WF, Sun Y, Liu LZ, Li L, Lin AH, Ma J. Baseline serum lactate dehydrogenase levels for patients treated with intensity-modulated radiotherapy for nasopharyngeal carcinoma: a predictor of poor prognosis and subsequent liver metastasis. Int J Radiat Oncol Biol Phys. 2012; 82: e359-365.
23. Almasi CE, Drivsholm L, Pappot H, Hoyer-Hansen G, Christensen IJ. The liberated domain I of urokinase plasminogen activator receptor--a new tumour marker in small cell lung cancer. Apmis. 2013; 121: 189-196.
24. Liu X, Meng QH, Ye Y, Hildebrandt MA, Gu J, Wu X. Prognostic significance of pretreatment serum levels of albumin, LDH and total bilirubin in patients with non-metastatic breast cancer. Carcinogenesis. 2015; 36: 243-248.
25. Amato RJ, Flaherty A, Zhang Y, Ouyang F, Mohlere V. Clinical prognostic factors associated with outcome in patients with renal cell cancer with prior tyrosine kinase inhibitors or immunotherapy treated with everolimus. Urol Oncol. 2014; 32: 345-354.
26. Sonpavde G, Pond GR, Armstrong AJ, Clarke SJ, Vardy JL, Templeton AJ, Wang SL, Paolini J, Chen I, Chow-Maneval E, Lechuga M, Smith MR, Michaelson MD. Prognostic impact of the neutrophil-to-lymphocyte ratio in men with metastatic castration-resistant prostate cancer. Clin Genitourin Cancer. 2014; 12: 317-324.
27. Petrelli F, Cabiddu M, Coinu A, Borgonovo K, Ghilardi M, Lonati V, Barni S. Prognostic role of lactate dehydrogenase in solid tumors: A systematic review and meta-analysis of 76 studies. Acta Oncol. 2015; 54: 961-970.
28. Xie H, Hanai J-i, Ren J-G, Kats L, Burgess K, Bhargava P, Signoretti S, Billiard J, Duffy KJ, Grant A, Wang X, Lorkiewicz PK, Schatzman S et al. Targeting lactate dehydrogenase-A inhibits tumorigenesis and tumor progression in mouse models of lung cancer and impacts tumor initiating cells. Cell metabolism. 2014; 19: 795-809.
29. Kostakis ID, Vaiopoulos AG, Philippou A, Papavassiliou AG, Koutsilieris M, Kouraklis G. Preoperative serum lactate dehydrogenase levels in colorectal and gastric cancer: a hospital-based case-control study. Biomark Med. 2013; 7: 131-137.
30. Halabi S, Lin CY, Kelly WK, Fizazi KS, Moul JW, Kaplan EB, Morris MJ, Small EJ. Updated prognostic model for predicting overall survival in first-line chemotherapy for patients with metastatic castration-resistant prostate cancer. J Clin Oncol. 2014; 32: 671-677.
31. Templeton AJ, Pezaro C, Omlin A, McNamara MG, Leibowitz-Amit R, Vera-Badillo FE, Attard G, de Bono JS, Tannock IF, Amir E. Simple prognostic score for metastatic castration-resistant prostate cancer with incorporation of neutrophil-to-lymphocyte ratio. Cancer. 2014; 120: 3346-3352.
32. Kattan MW, Karpeh MS, Mazumdar M, Brennan MF. Postoperative nomogram for disease-specific survival after an R0 resection for gastric carcinoma. J Clin Oncol. 2003; 21: 3647-3650.
33. Han DS, Suh YS, Kong SH, Lee HJ, Choi Y, Aikou S, Sano T, Park BJ, Kim WH, Yang HK. Nomogram predicting long-term survival after d2 gastrectomy for gastric cancer. J Clin Oncol. 2012; 30: 3834-3840.
34. Hirabayashi S, Kosugi S, Isobe Y, Nashimoto A, Oda I, Hayashi K, Miyashiro I, Tsujitani S, Kodera Y, Seto Y, Furukawa H, Ono H, Tanabe S et al. Development and external validation of a nomogram for overall survival after curative resection in serosa-negative, locally advanced gastric cancer. Ann Oncol. 2014; 25: 1179-1184.
35. Kim Y, Spolverato G, Ejaz A, Squires MH, Poultsides G, Fields RC, Bloomston M, Weber SM, Votanopoulos K, Acher AW, Jin LX, Hawkins WG, Schmidt C et al. A nomogram to predict overall survival and disease-free survival after curative resection of gastric adenocarcinoma. Ann Surg Oncol. 2015; 22: 1828-1835.
36. Dikken JL, Baser RE, Gonen M, Kattan MW, Shah MA, Verheij M, van de Velde CJ, Brennan MF, Coit DG. Conditional probability of survival nomogram for 1-, 2-, and 3-year survivors after an R0 resection for gastric cancer. Ann Surg Oncol. 2013; 20: 1623-1630.
37. Song KY, Park YG, Jeon HM, Park CH. A nomogram for predicting individual survival of patients with gastric cancer who underwent radical surgery with extended lymph node dissection. Gastric Cancer. 2014; 17: 287-293.
38. Eom BW, Ryu KW, Nam BH, Park Y, Lee HJ, Kim MC, Cho GS, Kim CY, Ryu SW, Shin DW, Hyung WJ, Lee JH. Survival nomogram for curatively resected Korean gastric cancer patients: multicenter retrospective analysis with external validation. PLoS One. 2015; 10: e0119671.
39. Kong SH, Lee HJ, Ahn HS, Kim JW, Kim WH, Lee KU, Yang HK. Stage migration effect on survival in gastric cancer surgery with extended lymphadenectomy: the reappraisal of positive lymph node ratio as a proper N-staging. Ann Surg. 2012; 255: 50-58.
40. Wang W, Xu DZ, Li YF, Guan YX, Sun XW, Chen YB, Kesari R, Huang CY, Li W, Zhan YQ, Zhou ZW. Tumor-ratio-metastasis staging system as an alternative to the 7th edition UICC TNM system in gastric cancer after D2 resection--results of a single-institution study of 1343 Chinese patients. Ann Oncol. 2011; 22: 2049-2056.
41. Wang X, Wan F, Wang JJ. A common misuse of stepwise regression in studies of ratio of metastatic lymph nodes for gastric cancer. Ann Surg Oncol. 2008; 15: 1805-1806.
42. Hess KR. Assessing time by covariate interactions in proportional hazards regression models using cubic spline functions. Statistics in medicine. 1994; 13: 1045-1062.
43. Harrell FE, Jr., Califf RM, Pryor DB, Lee KL, Rosati RA. Evaluating the yield of medical tests. Jama. 1982; 247: 2543-2546.
44. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008; 26: 1364-1370.