
INTRODUCTION
Androgen steroids play a key role in prostate cancer growth and development making the androgen-deprivation the principal therapeutic approach in the different stages of disease. However, hormone therapies lead to a transitory decrease in testosterone and dihydrotestosterone synthesis. Prostate cancer, especially in advanced disease, can only benefit temporarily from these treatments progressing to a castration-resistant prostate cancer (CRPC) status [1]. Despite this resistance to hormonal drugs, androgen signaling remains persistent, therefore targeting the androgen receptor pathway still continues to be a good therapeutic challenge for these patients [2]. Enzalutamide is a next generation anti-androgen with a great affinity for androgen receptor (AR) [3]. The results of two randomized phase 3 trials on enzalutamide versus placebo in patients with CRPC before docetaxel treatment (Prevail study) and after docetaxel (Affirm trial), respectively, showed its efficacy in increasing progression-free survival (PFS) and overall survival (OS) [4, 5]. More recently, in two randomized phase 2 studies (Terrain study and Strive trial) enzalutamide significantly reduced risk of progression or death compared with bicalutamide in patients with asymptomatic or mildly symptomatic CRPC [6, 7]. These promising results lead to the increasing use of enzalutamide. Therefore it becomes essential to better understand the mechanisms of drug resistance to select patients who will really experience a treatment benefit in terms of PFS and OS.
AR axis is one of the most important actors in acquiring resistance to androgen targeting therapies. It has been shown that studying specific AR-related alterations could represent an optimal chance for finding predictive markers [8]. Circulating cell free DNA (cfDNA) is a promising, non-invasive source of molecular biomarkers and constitutes a “liquid biopsy” providing a genomic landscape of the cancer at the time of sample taking [9]. For this reason, many efforts have been made for studying aberrations, such as copy number alterations or specific mutations of AR in cfDNA, also thanks to the advancement in next generation sequencing technologies [10, 11]. In recent studies, a significant association has been reported between AR copy number (CN) in cfDNA and the clinical outcome of metastatic CRPC patients treated with abiraterone [8, 12]. We here aimed to test the association between AR CN in cfDNA and resistance to enzalutamide in a cohort of 59 CRPC patients treated with enzalutamide after docetaxel.
RESULTS
AR copy number gain in CRPC
Fifty-nine patients with metastatic CRPC were treated with enzalutamide between August 2012 and November 2015 and serum samples were collected at starting of treatment. Serum DNA was extracted and was tested for AR CN. Median DNA concentration was 4.5 ng/μl (range: 2–23.7 ng/μl). AR gene was gained in 21 (36%) patients. Approach sensitivity was previously tested [12]. Clinical characteristics are reported in Table 1. Higher median baseline PSA, alkaline phosphatase and lactate dehydrogenase levels were significantly associated with AR CN gain (p = 0.007, p = 0.003, p = 0.0009, respectively). Nine out of 28 (32%) patients previously treated with abiraterone had AR gain. This frequency of AR gain was similar to the prevalence in patients who had not received abiraterone (39%) (p = 0.602), therefore the probability to find AR gain in patients with or without previous abiraterone treatment was the same (Table 1). The frequency of AR gain was similar in patients with response duration to androgen deprivation therapy less than 18 months (52%) vs. those with a response longer than 18 months (38%, p = n.s.).
Table 1: Patient characteristics
Characteristics |
No. cases (%) |
AR |
p-value |
|
|---|---|---|---|---|
N |
A |
|||
No (%) |
No (%) |
|||
Total |
59 (100) |
38 (100) |
21 (100) |
- |
Median age, y [range] |
75 [43–91] |
75 [43–91] |
74 [66–87] |
0.715 |
Gleason Score |
|
|
|
|
6–7 |
20 (34) |
14 (37) |
6 (28) |
0.806 |
8–9 |
30 (51) |
20 (53) |
10 (48) |
|
Unknown |
9 (15) |
4 (10) |
5 (24) |
|
ECOG PS |
|
|
|
|
0–1 |
56 (95) |
36 (95) |
20 (95) |
0.934 |
2 |
3 (5) |
2 (5) |
1 (5) |
|
Visceral metastases |
|
|
|
|
No |
51 (86) |
32 (84) |
19 (90) |
0.504 |
Yes |
8 (14) |
6 (16) |
2 (10) |
|
No. of previous chemotherapeutic lines |
|
|
|
|
1 |
21 (36) |
15 (39) |
6 (29) |
0.406 |
2 or more |
38 (64) |
23 (61) |
15 (71) |
|
Previous abiraterone treatment |
|
|
|
|
No |
31 (52) |
19 (50) |
12 (57) |
0.602 |
Yes |
28 (48) |
19 (50) |
9 (43) |
|
Median baseline PSA level, ng/mL [range] |
68.2 [0.6–4351] |
40.5 [0.6–4351] |
182.0 [19.8–1443] |
0.007 |
Median baseline ALP level, mU/mL [range] |
125 [32–6000] |
100 [32–313] |
416 [73–6000] |
0.003 |
Median baseline LDH level, mU/mL [range] |
204 [122–1808] |
194 [122–459] |
272 [144–1808] |
0.0009 |
AR, androgen receptor; N, normal; A, amplified; ECOG, Eastern Cooperative Oncology Group; PS, performance status; PSA, prostate-specific antigen, ALP, alkaline phosphatase; LDH, lactate dehydrogenase.
Association with PSA decline and clinical outcome
A PSA decline ≥ 50% was reported in 18 of the 59 (31%) patients, 4 of 21 (19%) with AR gene gain and 14 of 38 (37%) without AR gene gain (p = 0.260). A PSA decline ≥ 90% was reported in 5 of the 59 (8%) patients, all cases without AR gene gain.
At the time of the analysis, 54 of the 59 patients had progressive disease (PD) and 39 patients had died. Median PFS and OS for the overall population were 3.5 months (95% CI: 2.7–4.4) and 9.4 months (95% CI: 7.8–14.1), respectively. The median PFS of patients with AR gene gain was 2.4 months (95% CI: 1.9–3.2) vs. 4.0 months (95% CI: 3.0–6.5) of those with no CN variation (p = 0.0004) (Figure 1). The median OS of patients with AR gene gain was 6.1 months (95% CI: 3.4-8.6) compared to 14.1 months (95% CI: 8.2–20.5) for individuals with one copy of the gene (p = 0.0003) (Figure 2). Supplementary Figures S1 and S2 show the PFS and OS curves, respectively, made for AR gain vs. non-gain in patients without abiraterone and AR gain vs. non-gain with previous abiraterone.
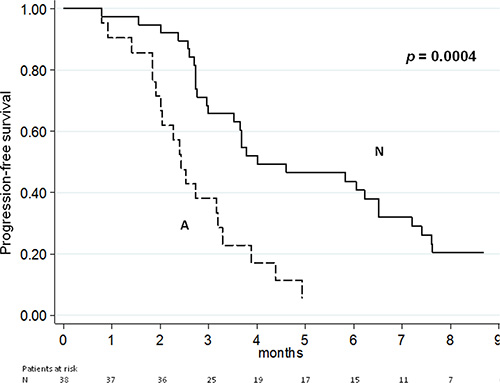
Figure 1: Progression free-survival according to AR CN.
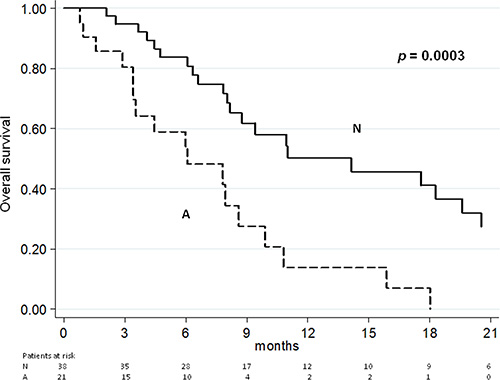
Figure 2: Overall survival according to AR CN.
Raw hazard ratios for PFS and OS are summarized in Table 2. Univariate analysis showed a significant association for PFS and OS with patients previously treated or not with abiraterone, PSA decline and AR CN (Table 2). At multivariate analysis, the only factors which maintained the association with PFS and OS were PSA decline ≥ 50% (p = 0.008 and p = 0.009, respectively) and AR CN (p = 0.002 and p = 0.001, respectively). We also analyzed the sensitivity and specificity of AR CN in PFS and OS (Supplementary Table S1).
Table 2: Univariate analysis for progression-free survival and for overall survival
Progression-free survival |
Overall survival |
||||
|---|---|---|---|---|---|
Raw HR (95%CI) |
p |
Raw HR (95%CI) |
p |
||
Visceral metastases |
yes vs. no |
1.57 (0.72−3.41) |
0.257 |
2.44 (1.11−5.37) |
0.027 |
No. of previous chemo lines |
≥ 2 vs. 1 |
1.67 (0.94−2.99) |
0.081 |
2.24 (1.09−4.63) |
0.029 |
Previous abiraterone |
yes vs. no |
1.97 (1.13−3.46) |
0.017 |
2.41 (1.21−4.78) |
0.012 |
PSA decline ≥ 50% |
no vs. yes |
3.23 (1.71−6.10) |
0.0003 |
3.52 (1.59−7.79) |
0.002 |
AR CN variation |
A vs. N |
2.79 (1.55−5.02) |
0.0006 |
3.23 (1.64−6.35) |
0.0007 |
PSA, prostate-specific antigen; AR, androgen receptor; CN, copy number; A, amplified; N, normal.
DISCUSSION
Analysis of cfDNA is a promising and minimally invasive approach for characterizing the tumor genome in CRPC patients [13, 14]. In this paper, we performed AR copy number analysis on cfDNA in CRPC patients treated with enzalutamide after docetaxel. The distribution of median baseline PSA, alkaline phosphatase and lactate dehydrogenase levels were significantly higher in patients with AR CN gain, even if a cause-effect relationship cannot be established. Detection of AR gain in pretreatment cfDNA was significantly associated with treatment resistance and with shorter PFS and OS.
This study highlighted AR gain as an independent biomarker from univariate and multivariate analyses for PFS and for OS. Moreover the multivariate analysis demonstrated PSA decline ≥ 50% could be a predictor of higher PFS and OS. The lack of association between AR CN gene and PSA response rate could have an explanation in possible changes of tumor biology during enzalutamide that were not present before treatment (e.g. neuroendocrine differentiation), even if a bias due to the small sample size needs to be considered [15, 16].
Currently, the sequential treatment is a hot topic of CRPC because of increasingly availability of survival-prolonging agents arising the importance of patient selection to improve CRPC management. We here selected a cohort of patients who had all received docetaxel and, in 48% of cases, also abiraterone. As expected, we therefore observed a shorter PFS and OS and lower response rate than reported in the chemotherapy-naïve setting. Our study supported the use of AR gain to select patients for enzalutamide but requires repeating in cohorts of patients with different clinical history to confirm that the association with outcome is maintained. Interestingly, prior use of abiraterone was no associated with a higher prevalence of AR gain, in keeping with our previous study that reported no significant change in AR status in sequential samples to progression [8].
To allow analysis of all our patients treated in early access program, we used serum samples. Due to concerns with increased leukocyte DNA release, we have more recently collected plasma for cfDNA studies. Increased levels of normal DNA could reduce our ability to detect AR CN gain clones and thus, reduce the difference we observed between AR gain and normal cancers. Overall, our observation may therefore be shown to be even more significant in future studies.
The only univariate analysis for PFS and OS showed a significant inverse association with prior abiraterone treatment. This confirms the limited antitumor activity of enzalutamide following abiraterone in metastatic CRPC patients irrespective of prior docetaxel use [17]. However, abiraterone before enzalutamide treatment and the number of previous chemotherapeutic lines did not influence the frequency of AR CN variation at baseline. These evidences confirmed the lack of changes in AR status during hormonal treatment identified in circulating tumor DNA from 44 CRPC patients treated with abiraterone [8].
In addition, among clinical features of prostate cancer, the presence of visceral metastases has been evaluated in this paper: no correlation with AR CN frequency was observed. Conversely, the univariate analysis revealed that the presence of visceral metastases had a significant negative effect only on OS as well as we have shown in our previous work of 256 CRPC patients treated with abiraterone after docetaxel [18].
The small sample size, the retrospective nature of the analysis and the absence of an independent validation set represented the main limitations of our study. Consequently, our results should be considered preliminary and hypothesis-generating. It can be hypothesized that enzalutamide-resistant patients with AR CN gain may benefit in terms of survival from chemotherapy and from other therapies that do not target AR signaling. Previously, several studies have already demonstrated that AR CN gain together with somatic point mutations were correlated with worse clinical outcome in CRPC patients [8, 10, 12, 19].
Identifying clinical and molecular factors predictive of response to enzalutamide remains a high priority for future research. Recently, Antonarakys et al. [20] have demonstrated that a splice variant of AR, ARV7, found in circulating tumor cells, was strongly associated with a poor outcome in patients treated with abiraterone or enzalutamide. We believe that also the evaluation of AR CN variation could have a similar important impact in guiding clinical decision in CRPC patients.
In conclusion, AR CN variation seems to be a biomarker potentially valid from an analytical point of view and pave the way for a further clinical validation in prospective studies on larger number of patients.
MATERIALS AND METHODS
Patient cohort
Patients with metastatic CRPC without neuroendocrine differentiation in the primary tumor after at least one chemotherapeutic treatment including docetaxel and treated with enzalutamide were included in this retrospective evaluation in a cohort of patients collected prospectively to study. Additional selection criteria included Eastern Cooperative Oncology Group (ECOG) performance status ≤ 2; adequate cardiac, hepatic, renal and bone marrow function; serum potassium level ≥ 3.5 mmol/L; and ongoing androgen deprivation therapy with serum testosterone < 50 ng/dL. The protocol was approved by the Institutional Review Board. Written informed consent was obtained from all patients.
Treatment consisted of enzalutamide 160 mg daily, that was given continuously until evidence of PD or unacceptable toxicity. Baseline serum PSA levels were typically measured in the week before starting enzalutamide treatment. All recorded PSA test and scan results were collected for these patients: PSA was usually evaluated every 4 weeks for serologic response and imaging investigations as clinically indicated. The Prostate Cancer Working Group 2 (PCWG2) criteria were used to define response and progression [21]. However, in clinical practice deterioration, in clinical conditions and/or radiologic progression according to local radiologist evaluation were also criteria sufficient to establish PD and discontinuation of enzalutamide treatment.
CN analysis
Serum DNA was extracted with QIAamp DNA Mini Kit (Qiagen, Milan, Italy). DNA was quantified by spectrophotometric evaluation (NanoDrop® ND-1000, Celbio, Milan, Italy). CN analyses were performed by a duplex TaqMan real-time PCR assay (Applied Biosystems, Foster City, CA, USA) for AR gene and 2 different reference genes: RNaseP (TaqMan Copy Number Reference Assay) and AGO1 (ID: Hs02320401). Samples analysis was performed as previously described [12]. For AR, the cutoff values were > 1.5 for amplification. Data were also analyzed by Digital PCR QuantStudio® 3D System. We performed an absolute quantification of target and reference gene for each sample.
Statistical analysis
PFS was defined as the time between the first day of enzalutamide therapy and the date of PD or death. Patients without PD at database closure were censored at the final follow up. OS was defined as the time between the first day of enzalutamide and the date of death from any cause or censored at the date of the last follow-up visit.
The association between CN gain and clinical outcome was evaluated by the Kaplan-Meier method and log-rank test. A Cox regression model was used to estimate hazard ratios (HR) and 95% confidence intervals (CI) for PFS and OS. The multivariable Cox models included all factors that were significantly associated in the univariate models. All P-values were two-sided and a P < 0.05 was considered statistically significant. Statistical analyses were performed with SAS 9.3 software (SAS Institute, Cary, NC).
ACKNOWLEDGMENTS
The authors thank Sara Pignatta, Chiara Molinari, and Pietro Fici for editing the manuscript.
CONFLICTS OF INTEREST
The authors declared no conflicts of interest.
GRANT SUPPORT
This was an institution-funded study.
REFERENCES
1. Attard G, Parker C, Eeles RA, Schroder F, Tomlins SA, Tannock I, Drake CG, de Bono JS. Prostate cancer. Lancet. 2016; 387:70–82.
2. Zhang TY, Agarwal N, Sonpavde G, DiLorenzo G, Bellmunt J, Vogelzang NJ. Management of castrate resistant prostate cancer-recent advances and optimal sequence of treatments. Curr Urol Rep. 2013; 14:174–183.
3. Tran C, Ouk S, Clegg NJ, Chen Y, Watson PA, Arora V, Wongvipat J, Smith-Jones PM, Yoo D, Kwon A, Wasielewska T, Welsbie D, Chen CD, et al. Development of a second-generation antiandrogen for treatment of advanced prostate cancer. Science. 2009; 324:787–790.
4. Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, Iversen P, Bhattacharya S, Carles J, Chowdhury S, Davis ID, de Bono JS, Evans CP, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014; 371:424–433.
5. Scher HI, Fizazi K, Saad F, Taplin ME, Sternberg CN, Miller K, de Wit R, Mulders P, Chi KN, Shore ND, Armstrong AJ, Flaig TW, Flechon A, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012; 367:1187–1197.
6. Shore ND, Chowdhury S, Villers A, Klotz L, Siemens DR, Phung D, van Os S, Hasabou N, Wang F, Bhattacharya S, Heidenreich A. Efficacy and safety of enzalutamide versus bicalutamide for patients with metastatic prostate cancer (TERRAIN): a randomised, double-blind, phase 2 study. Lancet Oncol. 2016; 17:153–163.
7. Penson DF, Armstrong AJ, Concepcion R, Agarwal N, Olsson C, Karsh L, Dunshee C, Wang F, Wu K, Krivoshik A, Phung, Higano CS. Enzalutamide Versus Bicalutamide in Castration-Resistant Prostate Cancer: The STRIVE Trial. J Clin Oncol. 2016 Jan 25; [Epub ahead of print].
8. Romanel A, Tandefelt DG, Conteduca V, Jayaram A, Casiraghi N, Wetterskog D, Salvi S, Amadori D, Zafeiriou Z, Rescigno P, Bianchini D, Gurioli G, Casadio V, et al. Plasma AR and abiraterone-resistant prostate cancer. Sci Transl Med. 2015; 7:312re10.
9. Diaz LA, Jr, Bardelli A. Liquid biopsies: genotyping circulating tumor DNA. J Clin Oncol. 2014; 32:579–586.
10. Azad AA, Volik SV, Wyatt AW, Haegert A, Le Bihan S, Bell RH, Anderson SA, McConeghy B, Shukin R, Bazov J, Youngren J, Paris P, Thomas G, et al. Androgen Receptor Gene Aberrations in Circulating Cell-Free DNA: Biomarkers of Therapeutic Resistance in Castration-Resistant Prostate Cancer. Clin Cancer Res. 2015; 21:2315–2324.
11. Frenel JS, Carreira S, Goodall J, Roda D, Perez-Lopez R, Tunariu N, Riisnaes R, Miranda S, Figueiredo I, Nava-Rodrigues D, Smith A, Leux C, Garcia-Murillas I, et al. Serial Next-Generation Sequencing of Circulating Cell-Free DNA Evaluating Tumor Clone Response To Molecularly Targeted Drug Administration. Clin Cancer Res. 2015; 21:4586–4596.
12. Salvi S, Casadio V, Conteduca V, Burgio SL, Menna C, Bianchi E, Rossi L, Carretta E, Masini C, Amadori D, Calistri D, Attard G, De Giorgi U. Circulating cell-free AR and CYP17A1 copy number variations may associate with outcome of metastatic castration-resistant prostate cancer patients treated with abiraterone. Br J Cancer. 2015; 112:1717–1724.
13. Murtaza M, Dawson SJ, Tsui DW, Gale D, Forshew T, Piskorz AM, Parkinson C, Chin SF, Kingsbury Z, Wong AS, Marass F, Humphray S, Hadfield J, et al. Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature. 2013; 497:108–112.
14. Crowley E, Di Nicolantonio F, Loupakis F, Bardelli A. Liquid biopsy: monitoring cancer-genetics in the blood. Nat Rev Clin Oncol. 2013; 10:472–484.
15. Conteduca V, Aieta M, Amadori D, De Giorgi U. Neuroendocrine differentiation in prostate cancer: current and emerging therapy strategies. Crit Rev Oncol Hematol. 2014; 92:11–24.
16. Conteduca V, Burgio SL, Menna C, Carretta E, Rossi L, Bianchi E, Masini C, Amadori D, De Giorgi U. Chromogranin A is a potential prognostic marker in prostate cancer patients treated with enzalutamide. The Prostate. 2014; 74:1691–1696.
17. Azad AA, Eigl BJ, Murray RN, Kollmannsberger C, Chi KN. Efficacy of enzalutamide following abiraterone acetate in chemotherapy-naive metastatic castration-resistant prostate cancer patients. Eur Urol. 2015; 67:3–29.
18. Conteduca V, Caffo O, Fratino L, Lo Re G, Basso U, D’Angelo A, Donini M, Verderame F, Ratta R, Procopio G, Campadelli E, Massari F, Gasparro D, et al. Impact of visceral metastases on outcome to abiraterone after docetaxel in castration-resistant prostate cancer patients. Future Oncol. 2015; 11:2881–2891.
19. Carreira S, Romanel A, Goodall J, Grist E, Ferraldeschi R, Miranda S, Prandi D, Lorente D, Frenel JS, Pezaro C, Omlin A, Rodrigues DN, Flohr P, et al. Tumor clone dynamics in lethal prostate cancer. Sci Transl Med. 2014; 6:254ra125.
20. Antonarakis ES, Lu C, Wang H, Luber B, Nakazawa M, Roeser JC, Chen Y, Mohammad TA, Chen Y, Fedor HL, Lotan TL, Zheng Q, De Marzo AM, et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N Engl J Med. 2014; 371:1028–1038.
21. Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, Eisenberger MA, Higano C, Bubley GJ, Dreicer R, Petrylak D, Kantoff P, Basch E, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008; 26:1148–1159.