
INTRODUCTION
Hepatocellular carcinoma (HCC) is one of the most common causes of cancer-related death [1–3]. Currently, the most widely accepted therapeutic algorithm is derived from BCLC staging system [4–5], in which the mainstay treatment options for HCC include liver transplantation (LT), surgical resection, radiofrequency ablation (RFA), percutaneous ethanol injection (PEI), transarterial embolization (TAE) or chemoembolization (TACE), and sorafenib. Several novel therapeutic modalities have been also explored, such as percutaneous acetic acid injection (PAI), three-dimensional conformal radiation therapy (3D-CRT), argon-helium cryotherapy system (AHCS), traditional Chinese medicine (TCMs), cytokine-induced killer (CIK) cell therapy, and portal vein embolization (PVE), etc. It remains unclear about whether or such novel therapeutic modalities could be applied to the clinical practice. Meta-analysis can provide the highest level of evidence for our clinical decisions by combining all scattered data [6–7]. Herein, we systematically reviewed the major findings from all meta-analyses regarding the treatment of HCC and attempted to propose the evidence-based recommendations and uncertainties.
RESULTS
Overall, 2039 papers were identified. Among them, 153 meta-analysis papers were finally included [8–160] (Figure 1). The number of relevant papers was gradually increased over years (Supplementary Figure S1). The characteristics of these included papers were shown in Table 1. Their major findings were summarized according to the treatment modalities (Tables 2–5 and Supplementary Tables S1–S8).
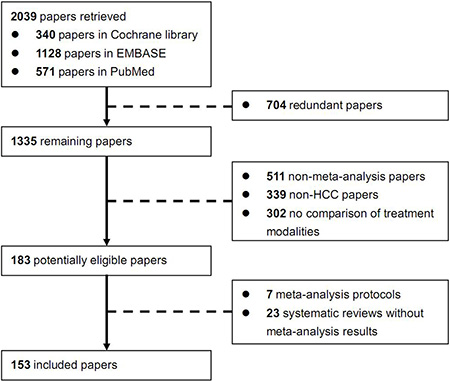
Figure 1: Flowchart of study inclusion.
Table 1: Study characteristics: An overview of included studies
First author |
Journal (Year) |
Country |
Type of participants |
No. included studies/pts. |
Comparisons |
Type of studies |
|
|---|---|---|---|---|---|---|---|
RCT |
Non-RCT |
||||||
Al Hasan |
Liver Transpl (2014) |
Saudi Arabia |
Unselected HCC |
7/1388 |
Living donor LT vs deceased donor LT |
0 |
7 |
Bouza |
BMC Gastroenterol (2009) |
Spain |
Early, small HCC |
6/787 |
RFA vs PEI |
6 |
0 |
Breitenstein |
Br J Surg (2009) |
Switzerland |
Unselected HCC |
7/620 |
Interferon after resection or ablation |
7 |
0 |
Cai |
HPB (2013) |
China |
HCC ≤ 5 cm |
5/NA |
RFA vs surgical resection |
NA |
NA |
Camma |
Radiology (2002) |
Italy |
Unresectable HCC |
18/2466 |
TACE vs non-active treatment; different transarterial modalities of therapy (TACE, TCE, TAE) |
5; 13 |
0 |
Cao |
Ultrasound Med Biol (2011) |
China |
Unselected HCC |
9/736 |
TACE plus HIFU vs TACE alone |
0 |
9 |
Chen |
Dig Dis Sci (2011) |
China |
Unselected HCC |
9/1503 |
Anatomic vs nonanatomic resection |
0 |
9 |
Chen |
Zhonghua Wai Ke Za Zhi (2008) |
China |
HCC ≤ 5 cm, number of lesions ≤ 3 |
6/697 |
RFA vs surgical resection |
1 |
5 |
Chen |
Chinese-German Journal of Clinical Oncology (2013) |
China |
Unresectable HCC |
9/870 |
CIK cell + TACE |
9 |
0 |
Cheng |
J Cancer Res Clin Oncol (2014) |
China |
Resectable HCC |
10/909 |
Preoperative TACE vs control; postoperative TACE vs control |
4; 6 |
0; 0 |
Cheung |
Evid Based Complement Alternat Med (2013) |
China |
Unresectable HCC |
67/5211 |
TACE + Chinese medicines vs TACE alone |
67 |
0 |
Cho |
Hepatology (2009) |
Korea |
Unselected HCC |
4/652 |
RFA vs PEI |
4 |
0 |
Cho |
Expert Opin Investig Drugs (2009) |
China |
HCC patients receiving TACE |
30/2428 |
TACE + Chinese herbal therapy vs TACE alone |
30 |
0 |
Chu |
Asian J Surg (2010) |
China |
Post-operative HCC |
5/206 |
Vitamin analogues (vitamin A and K2) after hepatic resection or local ablative therapy |
5 |
0 |
Cinco |
Hepatology International (2011) |
Philippines |
Advanced HCC |
2/828 |
Sorafenib vs placebo |
9 |
0 |
Cucchetti |
Ann Surg Oncol (2012) |
Italy |
Unselected HCC |
18/9036 |
Anatomic vs nonanatomic resection |
0 |
18 |
Cucchetti |
J Hepatol (2013) |
Italy |
Early HCC ≤ 5 cm |
17/8420 |
RFA vs surgical resection |
NA |
NA |
Dhir |
HPB (2012) |
USA |
Early HCC within Milan Criteria |
10/1763 |
LT vs resection |
0 |
10 |
Dong |
World J Gastroenterol (2014) |
China |
Unselected HCC |
22/NA |
Surgical resection vs nonsurgical-resection ablation therapies; RFA vs PEI; RFA vs RFA+TACE |
2; 5; 0 |
10; 0; 5 |
Duan |
World J Surg Oncol (2013) |
China |
Unselected HCC |
12/8612 |
RFA vs surgical resection |
2 |
12 |
Duffy |
Hepatology (2013) |
USA |
Unselected HCC |
6/2464 |
Antiangiogenic agents vs placebo |
6 |
21 |
Estanislao |
J Gastroenterol Hepatol (2009) |
Philippine |
Advanced HCC |
NA/NA |
Octreotide vs no octreotide |
NA |
NA |
Fancellu |
J Surg Res (2011) |
Italy |
Resectable HCC |
9/590 |
Minimally-invasive vs open hepatectomy |
0 |
9 |
Feng |
J Cancer Res Clin Oncol (2014) |
China |
Small HCC (1 lesion < 6.5 cm; no more than 3 lesions < 4.5 cm) |
23/15482 |
RFA vs surgical resection |
3 |
20 |
Flores |
J Gastroenterol Hepatol (2009) |
Philippines |
Post-operative HCC |
2/236 |
Adjuvant immunotherapy in combination with surgical resection |
2 |
0 |
Fu |
Hepato-gastroenterology (2014) |
China |
Small HCC (single < 6.5 cm, or ≤ 3 lesions, ≤ 4.5 cm) |
5/776 |
RFA vs surgical resection |
5 |
0 |
Fu |
J Cancer Res Clin Oncol (2014) |
China |
Unselected HCC |
9/900 |
TACE + sorafenib vs TACE alone |
5 |
4 |
Fu |
J Cancer Res Ther (2014) |
China |
Unresectable HCC |
9/608 |
Kanglaite injection plus hepatic arterial intervention vs hepatic arterial intervention alone |
0 |
9 |
Furtado |
Ann Surg Oncol (2014) |
Australia |
Unselected HCC |
5/334 |
Surgery + Adjuvant I(131) lipiodol vs surgery alone |
2 |
3 |
Gao |
Hepato-gastroenterology (2013) |
China |
Unresectable HCC |
7/693 |
DEB-TACE vs conventional TACE |
0 |
7 |
Germani |
J Hepatol (2010) |
UK |
Unselected HCC |
8/1035 |
RFA vs PEI; Percutaneous acetic acid injection vs PEI |
5; 2 |
0; 0 |
Geschwind |
Am J Clin Oncol (2003) |
USA |
Unselected HCC |
4/268 |
Therapeutic embolization vs supportive care alone |
4 |
0 |
Gong |
Nucl Med Commun (2014) |
China |
Unselected HCC |
6/466 |
Adjuvant therapy with intra-arterial iodine-131-labeled lipiodol ((131)I-lipiodol) to hepatic resection |
2 |
8 |
Grant |
Clin Transplant (2013) |
Canada |
Unselected HCC |
16/2202 |
Living donor LT vs deceased donor LT |
0 |
16 |
Gu |
J Cancer Res Clin Oncol (2014) |
China |
Unselected HCC |
18/2120 |
TACE + local ablative therapy vs monotherapy |
7 |
11 |
Guo |
J Cancer Res Clin Oncol (2009) |
China |
Advanced HCC |
6/352 |
Octreotide vs placebo or best supportive care |
6 |
0 |
Han |
Journal of Interventional Radiology (China) (2013) |
China |
Unselected HCC |
8/698 |
RFA + TACE vs TACE |
0 |
8 |
Han |
PLoS One (2014) |
China |
Unresectable HCC |
5/454 |
DEB-TACE vs conventional TACE |
3 |
2 |
Hoshida |
Hepatology (2000) |
Japan |
Non-advanced HCC |
17/NA |
Surgical resection vs PEI; Surgical resection vs LT |
0; 0 |
5; 12 |
Hu |
HPB (2013) |
China |
Unselected HCC |
18/NA |
RFA vs surgical resection |
4 |
14 |
Huang |
Hepato-gastroenterology (2013) |
China |
Unselected HCC |
4/433 |
RFA vs cryosurgery ablation |
0 |
4 |
Huang |
J Gastroenterol Hepatol (2014) |
China |
Unresectable HCC |
7/700 |
DEB-TACE vs conventional TACE |
2 |
5 |
Huang |
J Viral Hepat (2013) |
China Taiwan |
Unselected HCC |
22/3156 |
Adjuvant interferon therapy after curative treatment |
10 |
13 |
Huang |
Zhonghua Nei Ke Za Zhi (2008) |
China |
Early HCC within Milan Criteria |
6/862 |
RFA vs other therapeutic methods |
6 |
0 |
Ji |
Med Sci Monit (2011) |
China |
Advanced HCC |
9/759 |
Octreotide vs placebo or no treatment |
9 |
0 |
Jiang |
Tumour Biol (2014) |
China |
Unselected HCC |
19/1728 |
RFA + TACE vs RFA alone |
8 |
11 |
Jiang |
World J Surg Oncol (2013) |
China |
Unselected HCC |
10/1029 |
Adjuvant interferon therapy after treatment with surgical resection or TACE |
8 |
2 |
Kong |
Tumour Biol (2014) |
China |
Unselected HCC |
19/1728 |
RFA + TACE vs RFA alone |
8 |
11 |
Lan |
Journal of Gastroenterology and Hepatology Research (Hong Kong) (2013) |
China |
Unselected HCC |
10/701 |
Lamivudine treatment vs no antiviral therapy after liver resection or RFA |
0 |
10 |
Leng |
ANZ J Surg (2014) |
China |
HCC patients with PVTT |
5/600 |
TACE vs control treatment |
2 |
3 |
Li |
World J Gastroenterol (2012) |
China |
Unselected HCC |
11/1013 |
Primary LT vs salvage LT |
0 |
11 |
Li |
Hepatol Res (2012) |
China |
Unselected HCC |
10/627 |
Laparoscopic vs open liver resection |
0 |
10 |
Li |
Hepato-gastroenterology (2011) |
China |
Unselected HCC |
4/776 |
Anatomic vs nonanatomic resection |
0 |
4 |
Li |
J Gastroenterol Hepatol (2012) |
China |
Unselected HCC |
6/877 |
RFA vs surgical resection |
2 |
4 |
Li |
Chinese Journal of Evidence-Based Medicine (2012) |
China |
Intermediate-advanced stage |
17/907 |
TACE + thermotherapy vs TACE alone |
17 |
0 |
Li |
Chinese Journal of Evidence-Based Medicine (2013) |
China |
Intermediate-advanced stage |
16/1467 |
TACE + argon-helium cryotherapy system (AHCS) vs TACE alone; TACE + argon-helium cryotherapy system vs AHCS |
15; 7 |
0 |
Li |
Chinese Journal of Cancer Prevention and Treatment (2013) |
China |
Unselected HCC |
8/818 |
Adjuvant IFN vs without IFN after curative treatment |
8 |
0 |
Li |
Clin Res Hepatol Gastroenterol (2014) |
China |
Unresectable HCC |
11/936 |
CIK+TACE+RFA vs TACE+RFA; CIK+TACE vs TACE |
6 |
5 |
Liang |
Liver Transpl (2012) |
China |
Unselected HCC |
7/1310 |
Living donor LT vs deceased donor LT |
0 |
7 |
Liang |
Liver Transpl (2012) |
China |
Unselected HCC |
5/2950 |
Sirolimus-based immunosuppression (SRL) after LT vs SRL-free |
0 |
5 |
Liao |
PLoS One (2013) |
China |
Unselected HCC |
28/2497 |
TACE+PEI vs TACE; TACE+RT vs TACE; TACE+ three-dimensional conformal radiation therapy (3D-CRT) vs TACE; TACE+RFA vs TACE; TACE+HIFU vs TACE |
4; 3; 1; 1; 1 |
5; 4; 5; 0; 4 |
Liu |
World J Gastroenterol (2010) |
China |
Unselected HCC |
10/1522 |
RFA vs surgical resection |
0 |
10 |
Liu |
Surg Laparosc Endosc Percutan Tech (2010) |
China |
Unselected HCC |
8/1188 |
RFA vs surgical resection |
8 |
0 |
Liu |
Tumour Biol (2014) |
China |
Unselected HCC |
7/571 |
RFA + TACE vs RFA alone |
7 |
0 |
Liu |
PLoS One (2014) |
China |
Unresectable HCC |
17/676 |
TACE + sorafenib vs monotherapy |
3 |
14 |
Llovet |
Hepatology (2003) |
Spain |
Unresectable HCC |
14/1443 |
TACE vs control treatment; Tamoxifen vs control treatment |
7; 7 |
0; 0 |
Lu |
Eur J Gastroenterol Hepatol (2013) |
China |
Unselected HCC |
7/574 |
RFA + TACE vs RFA alone |
7 |
0 |
Ma |
Experimental Hematology and Oncology (2012) |
China |
Unresectable HCC |
13/1212 |
CIK cell therapy vs non-CIK therapy |
13 |
0 |
Ma |
Chinese Journal of Cancer Prevention and Treatment (2011) |
China |
Post-operative HCC |
4/423 |
Hepatic resection or RFA alone vs surgery + adoptive immunotherapy |
4 |
0 |
Marelli |
Cardiovasc Intervent Radiol (2007) |
UK |
Unselected HCC |
12/NA |
TACE vs control treatment; TACE vs TAE alone |
9; 3 |
0 |
Mathurin |
Aliment Pharmacol Ther (2003) |
France |
Post-operative HCC |
21/NA |
Adjuvant therapy after curative liver resection |
10 |
11 |
Meng |
Radiother Oncol (2009) |
China |
Unselected HCC |
17/1476 |
TACE + radiotherapy vs TACE alone |
5 |
12 |
Meng |
Hepatology International (2011) |
China |
Post-operative HCC |
4/209 |
Vitamin K2 vs placebo after curative treatment |
4 |
0 |
Meng |
J Altern Complement Med (2008) |
China |
Unresectable HCC |
37/2653 |
TACE + Traditional Chinese Medicine vs TACE alone |
NA |
NA |
Meng |
Explore (NY) (2011) |
China |
Unresectable HCC |
12/1008 |
TACE + Traditional Chinese Medicine vs TACE alone |
11 |
0 |
Menon |
Aliment Pharmacol Ther (2013) |
UK |
Unselected HCC |
5/474 |
Sirolimus-based immunosuppression (SRL) after LT vs SRL-free |
0 |
5 |
Miao |
World J Gastroenterol (2010) |
China |
Unselected HCC |
16/1224 |
Adjuvant antiviral therapy after curative therapy |
5 |
8 |
Miyake |
J Viral Hepat (2010) |
Japan |
Unselected HCC |
5/355 |
Interferon-alpha after curative therapy |
3 |
2 |
Moriguchi |
Hepatology (2006) |
Japan |
Unselected HCC |
4/604 |
Tumor ablation plus interferon therapy |
4 |
0 |
Ni |
J Cancer Res Clin Oncol (2013) |
China |
Unselected HCC |
10/21494 |
RFA/PEI (PAT) vs surgical resection |
6 |
4 |
Ni |
World J Gastroenterol (2013) |
China |
Unselected HCC |
8/598 |
RFA + TACE vs RFA alone |
8 |
0 |
Ni |
J Cancer Res Clin Oncol (2013) |
China |
Unselected HCC |
6/376 |
RFA + TACE vs RFA or TACE alone |
6 |
0 |
Nowak |
Cochrane Database Syst Rev (2004); Cancer (2005) |
Australia |
Unresectable HCC |
10/1709 |
Tamoxifen vs placebo/no intervention |
10 |
0 |
Oliveri |
Cochrane Database Syst Rev (2011) |
Denmark |
Unresectable HCC |
9/645 |
TACE or TAE vs placebo, sham, or no intervention |
9 |
0 |
Ono |
Cancer (2001) |
Japan |
Post-operative HCC |
3/108 |
Adjuvant chemotherapy after resection |
3 |
0 |
Orlando |
Am J Gastroenterol (2009) |
Italy |
Small HCC |
5/701 |
RFA vs PEI |
5 |
0 |
Pang |
Chinese Journal of Evidence-Based Medicine (2010) |
China |
Unselected HCC |
7/309 |
Laparoscopic vs conventional open hepatectomy |
0 |
7 |
Parks |
HPB (Oxford) (2014) |
USA |
Unselected HCC |
15/1002 |
Laparoscopic vs open liver resection |
0 |
15 |
Proneth |
Ann Surg Oncol (2014) |
Germany |
Unselected HCC |
9/1572 |
LT vs resection |
0 |
7 |
Qi |
J Clin Gastroenterol (2014) |
China |
Early-stage HCC |
3/559 |
RFA vs surgical resection |
3 |
0 |
Rahman |
J Gastrointest Surg (2012) |
USA |
Unselected HCC |
9/2279 |
LT vs resection |
0 |
9 |
Riaz |
BMC Gastroenterol (2012) |
Pakistan |
Post-operative HCC |
5/754 |
Vitamin K2 or its analogues vs placebo or No vitamin K |
5 |
0 |
Schoppmeyer |
Cochrane Database Syst Rev (2009) |
Germany |
Early HCC |
3/261 |
PEI vs percutaneous acetic acid injection; PEI vs surgery |
2; 1 |
0; 0 |
Shen |
J Gastroenterol Hepatol (2013) |
China |
Small HCC < 3 cm |
4/766 |
RFA vs PEI |
4 |
0 |
Shen |
J Clin Gastroenterol (2013) |
China |
Unresectable HCC |
5/1462 |
Sorafenib vs placebo |
5 |
0 |
Shen |
J Hepatol (2010) |
China Taiwan |
Unselected HCC |
13/1180 |
Adjuvant interferon therapy after curative therapy |
9 |
4 |
Shu |
Integr Cancer Ther (2005) |
USA |
Unresectable HCC |
26/2079 |
Chinese herbal medicine + chemotherapy vs chemotherapy alone |
24 |
2 |
Singal |
Aliment Pharmacol Ther (2010) |
USA |
Unselected HCC |
10/645 |
Interferon after resection or ablation |
5 |
5 |
Sun |
World Chinese Journal of Digestology (2011) |
China |
Small HCC |
11/2965 |
RFA vs surgical resection |
2 |
9 |
Sun |
PLoS One (2014) |
China |
Unselected HCC |
13/6350 |
Nucleot(s)ide analogues vs placebo or no treatment after curative treatment |
1 |
12 |
Sun |
Afr J Tradit Complement Altern Med (2012) |
China |
Unresectable HCC |
10/726 |
TACE + Compound Kushen Injection vs TACE alone |
0 |
10 |
Tang |
Hepato-gastroenterology (2012) |
China |
Unselected HCC |
5/799 |
Hepatectomy with a margin aiming at 2 cm vs a margin aiming at 1 cm |
1 |
4 |
Tang |
Hepato-gastroenterology (2013) |
China |
Resectable HCC |
12/1829 |
Anatomic vs nonanatomic resection |
0 |
12 |
Twaij |
World J Gastroenterol (2014) |
United Kingdom |
Unselected HCC |
4/420 |
Laparoscopic vs open liver resection |
0 |
4 |
Wang |
Hepato-gastroenterology (2011) |
China |
Unselected HCC |
3/257 |
Preoperative TACE vs control |
3 |
0 |
Wang |
PLoS One (2014) |
China |
Early HCC |
28/11873 |
RFA vs surgical resection |
3 |
25 |
Wang N |
Med Oncol (2011) |
China |
Unselected HCC |
7/623 |
TACE + PEI vs TACE alone |
7 |
0 |
Wang W |
Liver Int (2010) |
China |
Unselected HCC |
10/595 |
TACE + percutaneous ablation therapy (RFA or PEI) vs TACE or percutaneous ablation therapy alone |
10 |
0 |
Wang |
Asian Pac J Cancer Prev (2013) |
China |
Unselected HCC |
4/1382 |
Sorafenib with or without chemotherapy vs placebo with or without chemotherapy |
4 |
0 |
Wang |
Can J Gastroenterol (2012) |
China |
Unresectable HCC |
4/210 |
Prophylactic antibiotic treatment vs no prophylactic antibiotic treatment after transarterial therapy |
3 |
1 |
Wang |
Can J Gastroenterol (2013) |
China |
Post-operative HCC |
27/2614 |
Different adjuvant therapy after potentially curative treatment |
27 |
0 |
Weis |
Cochrane Database Syst Rev (2013) |
Germany |
Unselected HCC |
11/NA |
RFA vs surgical resection; RFA vs PEI or RFA vs acetic acid injection; RFA vs microwave ablation; RFA vs laser ablation |
3; 6; 1; 1 |
0; 0; 0; 0 |
Wong |
Aliment Pharmacol Ther (2011) |
China |
Unselected HCC |
9/551 |
Antiviral treatment vs no anti-viral treatment |
0 |
9 |
Wu |
J Exp Clin Cancer Res (2009) |
China |
Unresectable HCC |
45/3236 |
Traditional Chinese Medicines vs other treatment |
45 |
0 |
Wu |
J Cancer Res Ther (2014) |
China |
Unresectable HCC |
9/659 |
TACE + Cinobufacini vs TACE only |
0 |
9 |
Xie |
Tumour Biol (2014) |
China |
Advanced HCC |
5/582 |
TACE vs TAE |
5 |
0 |
Xie |
J Cancer Res Clin Oncol (2012) |
China |
Unresectable HCC |
13/1840 |
TACE vs microsphere embolization |
7 |
6 |
Xie |
PLoS One (2012) |
China |
Post-operative HCC |
6/494 |
Adoptive immunotherapy vs non-immunotherapy after surgery |
6 |
0 |
Xiong |
World J Gastroenterol (2012) |
China |
Unselected HCC |
9/550 |
Laparoscopic vs open liver resection |
0 |
15 |
Xu |
Journal of Xi’an Jiaotong University (Medical Sciences) (2012) |
China |
Unselected HCC |
9/2145 |
LT vs resection |
0 |
9 |
Xu |
Hepatobiliary Pancreat Dis Int (2014) |
China |
Unselected HCC |
17/4238 |
LT vs resection |
0 |
17 |
Xu |
World J Surg Oncol (2012) |
China |
Early HCC |
13/2535 |
RFA vs surgical resection |
2 |
11 |
Xu |
Eur J Med Res (2014) |
China |
Small HCC < 5 cm |
6/983 |
RFA vs PEI |
6 |
0 |
Xu |
Hepatol Res (2014) |
China |
Unselected HCC |
9/1565 |
Adjuvant interferon therapy after surgical treatment |
5 |
4 |
Xue |
BMC Gastroenterol (2013) |
China |
Advanced HCC with PVTT |
8/1601 |
TACE vs conservative treatment |
0 |
8 |
Yan |
Dig Dis Sci (2012); Dig Dis Sci (2013) |
China |
Unselected HCC |
19/1728 |
RFA + TACE vs RFA alone |
8 |
11 |
Yang |
Mol Biol Rep (2014) |
China |
Unresectable HCC |
6/1181 |
TACE + sorafenib vs TACE alone |
3 |
3 |
Yao |
Chinese Journal of Evidence-Based Medicine (2013) |
China |
Unselected HCC |
13/701 |
Laparoscopic vs open hepatectomy |
0 |
13 |
Ye |
Asian Pac J Cancer Prev (2012) |
China |
Unselected HCC |
11/1576 |
Anatomic vs nonanatomic resection |
0 |
11 |
Yin |
Ann Surg Oncol (2013) |
China |
Unselected HCC |
15/1238 |
Laparoscopic vs open hepatectomy |
0 |
15 |
Yu |
Chinese-German Journal of Clinical Oncology (2013) |
China |
Unselected HCC |
7/1347 |
Preoperative TACE vs control |
0 |
7 |
Zhang |
PLoS One (2014) |
China |
Unresectable/advanced HCC |
6/1254 |
TACE + sorafenib vs TACE alone |
2 |
4 |
Zhang |
Anticancer Drugs (2010) |
China |
Advanced HCC |
3/924 |
Sorafenib-based therapy with other agent-based therapy |
3 |
0 |
Zhang |
Hepatobiliary Pancreat Dis Int (2012) |
China |
Advanced HCC |
6/1164 |
Sorafenib vs placebo |
3 |
3 |
Zhang |
Molecular and Clinical Oncology (2014) |
China |
Unselected HCC |
14/1385 |
Adjuvant interferon after curative surgery or ablation therapy |
9 |
5 |
Zhang |
Int J Cancer (2009) |
China |
Post-surgical or ablative HCC |
6/600 |
IFN-alpha with placebo or no treatment after tumor resection or ablation |
6 |
0 |
Zhao |
Journal of Interventional Radiology (China) (2013) |
China |
Unselected HCC |
21/2339 |
RFA + TACE vs RFA or TACE alone |
21 |
0 |
Zhao |
Zhonghua Wai Ke Za Zhi (2008) |
China |
Unselected HCC |
9/494 |
Preoperative portal vein embolization (PVE) vs no PVE for extended hepatectomy |
0 |
9 |
Zheng |
Transplantation (2014) |
China |
Unselected HCC |
62/10170 |
LT vs resection |
0 |
62 |
Zheng |
Int J Cancer (2014) |
China |
Unselected HCC |
48/4747 |
Hepatectomy + adjuvant chemotherapy vs hepatectomy alone |
13 |
35 |
Zhong |
Hepatol Res (2010) |
China |
UICC TNM stage 3A HCC |
6/659 |
Postoperative adjuvant TACE |
6 |
0 |
Zhong |
World Chinese Journal of Digestology (2012); PLoS One (2013) |
China |
Post-operative HCC |
6/930 |
Curative treatments alone vs curative treatments + oral vitamin K2 analogs |
6 |
0 |
Zhong |
Molecular and Clinical Oncology (2014) |
China |
Post-operative HCC |
3/286 |
Adjuvant conventional oral systemic chemotherapy after curative hepatic resection |
3 |
0 |
Zhou |
Dig Dis Sci (2011) |
China |
Unselected HCC |
10/494 |
Laparoscopic vs open resection |
0 |
10 |
Zhou |
Langenbecks Arch Surg (2011) |
China |
Unselected HCC |
16/2917 |
Anatomic vs nonanatomic resection |
0 |
16 |
Zhou |
BMC Gastroenterol (2013) |
China |
Unselected HCC |
21/3210 |
Preoperative TACE vs no preoperative TACE |
4 |
17 |
Zhou |
Zhonghua Wai Ke Za Zhi (2011) |
China |
Small HCC (Milan criteria) |
4/539 |
RFA vs surgical resection |
4 |
0 |
Zhou |
BMC Gastroenterol (2010) |
China |
Small HCC (Yao’s criteria) |
10/1411 |
RFA vs surgical resection |
1 |
9 |
Zhou |
World J Surg (2014) |
China |
Unselected HCC |
20/8204 |
Antiviral therapy after curative resection |
1 |
19 |
Zhu |
Transplant Proc (2013) |
China |
Unselected HCC |
14/1508 |
Primary LT vs salvage LT |
0 |
14 |
Zhuang |
PLoS One (2013) |
China |
Unselected HCC |
13/1344 |
Interferon after curative therapy |
13 |
0 |
Zhuang |
Zhonghua Gan Zang Bing Za Zhi (2012) |
China |
Unselected HCC |
8/857 |
Interferon after curative therapy |
8 |
0 |
Zou |
Acta Academiae Medicinae Sinicae (2011) |
China |
Advanced HCC |
2/828 |
Sorafenib vs placebo |
2 |
0 |
Table 2: Findings of meta-analyses: An overview of included studies regarding LT
First author |
Journal (Year) |
Comparisons |
OS |
DFS, RFS, TTP, PFS |
Recurrence, time to recurrence |
Other endpoints |
Major comments |
|---|---|---|---|---|---|---|---|
Living donor LT (LDLT) versus deceased donor LT (DDLT) |
|||||||
Al Hasan |
Liver Transpl (2014) |
LDLT vs DDLT |
OS: 1-, 3-, 5-year: statistically similar. |
DFS: 1-, 3-, 5-year: statistically similar. |
Recurrence: 1-, 3-year: statistically similar. 5-year: favor DDLT. |
NA. |
OS and DFS are comparable, but long-term recurrence is higher in LDLT. |
Grant |
Clin Transplant (2013) |
LDLT vs DDLT |
OS: statistically similar. |
DFS: favor DDLT. |
NA. |
NA. |
LDLT has lower DFS than DDLT. |
Liang |
Liver Transpl (2012) |
LDLT vs DDLT |
OS: 1-, 3-, 5-year: statistically similar. |
RFS: 1-, 3-, 5-year: statistically similar. |
Recurrence: statistically similar. |
NA. |
LDLT is an acceptable option especially for patients within Milan criteria. |
Primary LT versus salvage LT |
|||||||
Li |
World J Gastroenterol (2012) |
Primary LT vs salvage LT |
OS: 1-, 3-, 5-year: statistically similar. |
DFS: 1-, 3-, 5-year: statistically similar. |
NA. |
NA. |
OS and DFS were not significantly different. |
Zhu |
Transplant Proc (2013) |
Primary LT vs salvage LT |
OS: 1-, 3-, 5-year: statistically similar. |
DFS: 1-, 3-year: statistically similar. 5-year: favor primary LT. |
NA. |
Operative time: longer in salvage LT. Intraoperative blood loss: increased in salvage LT. Number of transfused units of packed red blood cells: larger in salvage LT. Length of hospital stay and ICU stay: statistically similar. Peri-operative mortality: statistically similar. |
Salvage LT achieves the same short- and long-term outcomes as primary LT. |
Sirolimus-based immunosuppression (SRL) after LT |
|||||||
Liang |
Liver Transpl (2012) |
SRL after LT vs SRL-free |
OS: 1-, 3-, 5-year: favor SRL. |
DFS: 1-year: favor SRL. |
Recurrence: 1-year: favor SRL. |
Major SRL-related post-transplant complications: statistically similar. |
SRL is safe and prolongs survival and decrease tumor recurrence. |
Menon |
Aliment Pharmacol Ther (2013) |
SRL after LT vs SRL-free |
Overall mortality: favor SRL. |
RFS: better in SRL (no statistical comparison). Recurrence-related mortality: low in SRL. |
Recurrence: favor SRL. |
NA. |
SRL has lower recurrence rate, lower overall mortality and longer RFS and OS. |
LT versus surgical resection |
|||||||
Dhir |
HPB (2012) |
LT vs resection |
OS: 5-year: early HCC: favor LT. early HCC with well compensated cirrhosis: favor LT. early HCC using ITT strategy: statistically similar. early HCC with well compensated cirrhosis using ITT strategy: favor LT. |
NA. |
NA. |
NA. |
LT has favorable survival advantage in some settings. |
Hoshida |
Hepatology (2000) |
Surgical resection vs PEI and LT (including LT vs surgical resection) |
OS: Surgical resection vs LT: 3-year: statistically similar. |
DFS: Surgical resection vs LT: 3-year: favor LT. |
NA. |
NA. |
LT improved 3-year DFS for HCC patients. |
Proneth |
Ann Surg Oncol (2014) |
LT vs resection |
OS: 5-year: statistically similar. |
NA. |
NA. |
NA. |
LR is a good alternative to LT in patients with resectable HCC in whom both seem feasible. |
Rahman |
J Gastrointest Surg (2012) |
LT vs resection |
OS: 1-year: all studies: favor resection. non-ITT analysis: statistically similar. ITT analysis: favor resection. 5-year: all studies: statistically similar. non-ITT analysis: statistically similar. ITT analysis: favor LT. 10-year: all studies: favor LT. non-ITT analysis: favor LT. ITT analysis: favor LT. |
DFS: 1-year: all studies: statistically similar. non-ITT analysis: statistically similar. ITT analysis: statistically similar. 5-year survival: all studies: favor LT. non-ITT analysis: favor LT. ITT analysis: favor LT. 10-year: all studies: favor LT. non-ITT analysis: favor LT. ITT analysis: statistically similar. |
NA. |
NA. |
LT results in increased DFS and OS. |
Xu |
Journal of Xi’an Jiaotong University (2012) |
LT vs resection |
OS: 1-year: statistically similar. 3-, 5-year survival: favor LT. |
DFS: 5-year: favor LT. |
Recurrence: favor LT. |
NA. |
Both treatments were effective. But LT has a better prognosis than resection. |
Xu |
Hepatobiliary Pancreat Dis Int (2014) |
LT vs resection |
OS: 1-, 3-year: statistically similar. 5-year survival: favor LT. |
DFS: 1-, 3-, 5-year: favor LT. |
NA. |
Surgery-related morbidity: higher in LT. Surgery-related mortality: higher in LT. |
Long-term survival and tumor-free survival are higher in LT than in resection. |
Zheng |
Transplantation (2014) |
LT vs resection |
OS: 1-year: statistically similar. 3-, 5-year: favor LT. |
DFS: 1-, 3-, 5-year: favor LT. |
Recurrence: favor LT. |
NA. |
LT provides increased survival and lower recurrence rates than resection. |
Table 3: Findings of meta-analyses: An overview of included studies regarding surgical resection

Table 4: Findings of meta-analyses: An overview of included studies regarding ablation therapy

Table 5: Findings of meta-analyses: An overview of included studies regarding TACE

LT
Living donor LT (LDLT) versus deceased donor LT (DDLT)
Three meta-analyses compared the outcomes of LDLT versus DDLT [8, 41, 67]. All of them demonstrated that the OS was statistically similar between the two groups [8, 41, 67]. Two of them showed that the 1-, 3-, and 5-year DFS were statistically similar between the two groups [8, 67], but another one favored DDLT in term of DFS [41]. One of them found that the recurrence was statistically similar between the two groups [67]; by comparison, another one favored LDLT in term of 5-year recurrence, but not 1- or 3-year recurrence [8].
Only non-RCT studies, rather than RCTs, were included in the three meta-analyses.
The meta-analysis by Grant had a larger number of included studies than those by Al Hasan and Liang (16 versus 7 and 7) (Supplementary Table S9). Notably, there was an overlap of included studies between the two meta-analyses by Liang and Grant. All studies which were included in the meta-analysis by Liang were also covered by the meta-analysis by Grant. The meta-analysis by Al Hasan did not show the included studies.
Given its superiority in the quantity of non-RCT studies, the results of the meta-analysis by Grant might be more reliable. In details, LDLT has lower DFS than DDLT.
Primary versus salvage LT
Two meta-analyses compared the outcomes of primary versus salvage LT [59, 157]. Both of them demonstrated that the OS and 1- and 3-year DFS were statistically similar between the two groups [59, 157]. One of them favored primary LT in term of 5-year DFS [157]; by comparison, another one showed that the 5-year DFS was statistically similar between the two groups [59]. In addition, salvage LT had significantly longer operative time, increased intra-operative blood loss, and larger number of transfused units of packed red blood cells than primary LT [157]. But the length of hospital and ICU stay was statistically similar between the two groups [157].
Only non-RCT studies, rather than RCTs, were included in the two meta-analyses.
The meta-analysis by Zhu had a larger number of included studies than that by Li (14 versus 11) (Supplementary Table S10). Notably, there was an overlap of included studies between them. All studies which were included in the meta-analysis by Li were also included in the meta-analysis by Zhu.
Given its superiority in the quantity of non-RCT studies, the results of the meta-analysis by Zhu might be more reliable. In details, salvage LT achieves the same short- and long-term survival as primary LT. However, primary LT was significantly superior to salvage LT in terms of operative time, blood loss, and blood transfusion.
Sirolimus-based immunosuppression after LT
Two meta-analyses compared the outcomes of sirolimus-based immunosuppression versus no sirolimus after LT [66, 83]. Both of them favored the use of sirolimus after LT in terms of OS, DFS/RFS, and recurrence [66, 83].
Only non-RCT studies, rather than RCTs, were included in the two meta-analyses.
Both of them had a similar number of included studies (5 versus 5) (Supplementary Table S11). But not all included studies were the same between them.
The results were completely consistent between the two meta-analyses. In details, the use of sirolimus after LT should be favored.
LT versus surgical resection
Seven meta-analyses compared the outcomes of LT versus surgical resection [25, 46, 96, 98, 129, 131, 146]. There were 4, 4, 6, and 1 meta-analyses to compare the 1-, 3-, 5-, and 10-year survival, respectively. As for the 1-year survival, three of them demonstrated that the survival was statistically similar between the two groups [129, 131, 146], but another one favored surgical resection [98]. As for the 3-year survival, two of them found that the survival was statistically similar between the two groups [46, 131], but another two favored LT [129, 146]. As for the 5-year survival, two of them showed that the survival was statistically similar between the two groups [96, 98], but another four favored LT [25, 129, 131, 146]. As for the 10-year survival, the only one meta-analysis favored LT [98]. There were 3, 3, 4, and 1 meta-analyses to compare the 1-, 3-, 5-, and 10-year DFS, respectively. As for the 1-year DFS, two of them favored LT [131, 146], but another one found that the 1-year DFS was statistically similar between the two groups [98]. As for the 3-year DFS, all of them favored LT [46, 131, 146]. As for the 5-year DFS, all of them favored LT [98, 129, 131, 146]. As for the 10-year DFS, the only one meta-analysis favored LT [98]. Two meta-analyses compared the recurrence. Both of them favored LT in term of recurrence [129, 146].
Only non-RCT studies, rather than RCTs, were included in these meta-analyses.
The meta-analysis by Zhang had the largest number of included studies (n = 62) (Supplementary Table S12). By comparison, the number of included studies was less than 20 in 6 other meta-analyses.
Given its superiority in the quantity of non-RCT studies, the results of the meta-analysis by Zhang might be more reliable. In details, LT provides a significantly better survival and a lower recurrence.
Surgical resection
Surgical resection margin 1 cm versus 2 cm
Only one meta-analysis compared the outcomes of hepatectomy with a margin aiming at 2 cm versus those with a margin aiming at 1 cm [109]. Regardless of study design, the 1-year survival was statistically similar between the two groups [109]. In the subgroup analysis of randomized studies, the 3- and 5-year survival and DFS were better in patients undergoing hepatectomy with a margin aiming at 2 cm than in those with a margin aiming at 1 cm [109]. Contrarily, in the subgroup analysis of non-randomized studies, the 3- and 5-year survival and DFS were statistically similar between the two groups [109].
One RCT and 4 non-RCT studies were included in this meta-analysis.
Laparoscopic versus open resection
Nine meta-analyses compared the outcomes of laparoscopic versus open resection [30, 62, 94–95, 111, 126, 135, 137, 156]. All of them demonstrated that the OS and DFS/RFS at any time points were statistically similar between the two groups [30, 62, 94–95, 111, 126, 135, 137, 156]. Two of them also found that the recurrence was statistically similar between the two groups [62, 126]. Eight of them demonstrated statistically similar operative time between the two groups [30, 62, 95, 111, 126, 135, 137, 156], but one demonstrated significantly longer operative time in laparoscopic resection group [94]. All of them demonstrated that blood loss or intraoperative bleeding was significantly less in laparoscopic resection group [30, 62, 94–95, 111, 126, 135, 137, 156]. Among the 7 meta-analyses evaluating the blood transfusion, 6 demonstrated significantly less blood transfusion in laparoscopic resection group [30, 62, 111, 126, 137, 156], and one demonstrated statistically similar blood transfusion between the two groups [94]. Among the 6 meta-analyses evaluating the overall complications, 5 demonstrated significantly less complications in laparoscopic resection group [30, 62, 94, 111, 135], and one demonstrated statistically similar complications between the two groups [126]. Among the 8 meta-analyses evaluating the hospital length, all demonstrated significantly shorter hospital study in laparoscopic resection group [30, 62, 94, 111, 126, 135, 137, 156].
Only non-RCT studies, rather than RCTs, were included in these meta-analyses.
The meta-analyses by Park, Xiong, and Yin had the largest number of included studies (n = 15) followed by the meta-analyses by Yao (n = 13), Zhou (n = 10), Li (n = 10), Fancellu (n = 9), Pang (n = 7), and Twaij (n = 4) (Supplementary Table S13). The included studies were completely same between the two meta-analyses by Xiong and Yin. However, the studies included in the meta-analysis by Park were different from those included in the meta-analyses by Xiong and Yin.
Given its superiority in the quantity of non-RCT studies, the results of the meta-analyses by Park, Xiong, and Yin might be more reliable. In details, they suggested that the operative time was statistically similar between the two groups and that laparoscopic resection was superior to open resection in terms of blood loss, blood transfusion, complications, and hospital stay.
Anatomic resection versus non-anatomic resection
Six meta-analyses compared the outcomes of anatomic versus non-anatomic resection [15, 23, 60, 110, 136, 152]. Four of them demonstrated that the OS was statistically similar between the two groups [15, 60, 110, 136], but another two favored anatomic resection in term of 5-year survival [23, 152]. One of them found that the DFS was statistically similar between the two groups [60], but another four favored anatomic resection in term of DFS [15, 23, 136, 152]. Two of them showed that the recurrence was statistically similar between the two groups [15, 110], but another two favored anatomic resection in term of local intrahepatic recurrence [136, 152]. Post-operative complications were statistically similar between the two groups [23, 110, 136, 152].
Only non-RCT studies, rather than RCTs, were included in these meta-analyses.
The meta-analysis by Cucchetti had the largest number of included studies (n = 18) followed by the meta-analyses by Zhou (n = 16), Tang (n = 12), Ye (n = 11), Chen (n = 9), and Li (n = 4) (Supplementary Table S14).
Given its superiority in the quantity of non-RCT studies, the results of the meta-analysis by Zhang might be more reliable. In details, anatomic resection was superior to non-anatomic resection in terms of OS and DFS.
Surgical resection + I131 lipiodol versus surgical resection alone
Two meta-analyses compared the outcomes of surgical resection in combination with I131 lipiodol versus surgical resection alone [36, 40]. Both of them favored the combination therapy in terms of OS, DFS, and recurrence [36, 40].
Only non-RCT studies, rather than RCTs, were included in these meta-analyses.
The meta-analysis by Gong had a larger number of included studies than that by Furtado (10 versus 5) (Supplementary Table S15). Notably, there was an overlap of included studies between them. All studies which were included in the meta-analysis by Furtado were also included in the meta-analysis by Gong.
The results were completely consistent between the two meta-analyses. In details, surgical resection in combination with I131 lipiodol should be favored.
Surgical resection + TACE versus surgical resection alone
Pre-operative TACE
Four meta-analyses compared the outcomes of surgical resection in combination with pre-operative TACE versus surgical resection alone [17, 116, 138, 153]. All of them found that the OS, DFS, and recurrence were statistically similar between the two groups [17, 116, 138, 153].
RCT studies were included in the meta-analyses by Cheng (n = 4), Wang (n = 3), and Zhou (n = 4), but not in the meta-analysis by Yu (n = 0).
The meta-analysis by Zhou had the largest number of included studies (n = 21) followed by the meta-analyses by Yu (n = 7), Cheng (n = 4), and Wang (n = 3) (Supplementary Table S16). All studies which were included in the two meta-analyses by Cheng and Wang were also included in the meta-analysis by Zhou.
The results were completely consistent between the two meta-analyses. In details, pre-operative TACE did not improve the OS or DFS.
Post-operative TACE
Two meta-analyses compared the outcomes of surgical resection in combination with post-operative TACE versus surgical resection alone [17, 149]. Both of them favored post-operative TACE in terms of OS, DFS, and recurrence [17, 149].
Only RCT studies were included in the two meta-analyses.
Although the number of included studies was the same between the two meta-analysis by Cheng and Zhong (n = 6) (Supplementary Table S17), not all included studies were the same between them.
The results were completely consistent between the two meta-analyses. In details, post-operative TACE should be favored.
Surgical resection + adjuvant chemotherapy versus surgical resection alone
Five meta-analyses compared the outcomes of surgical resection in combination with adjuvant chemotherapy versus surgical resection alone [78, 92, 112, 147–148].
Oral systemic chemotherapy
Oral systemic chemotherapy was evaluated in two meta-analyses [78, 148]. The OS, RFS, and recurrence were statistically similar between patients with and without chemotherapy [78, 148].
RCT studies were included in the meta-analyses by Zhong (n = 3) and Mathurin (n = 1).
The meta-analysis by Zhong had a larger number of included studies than that by Mathurin (3 versus 2) (Supplementary Table S18). Not all included studies were the same between them.
The results were completely consistent between the two meta-analyses. In details, the adjunctive use of oral systemic chemotherapy should not be favored in patients undergoing surgical resection.
Transarterial chemotherapy
Transarterial chemotherapy was evaluated in one meta-analysis [78]. As for the pre-operative transarterial chemotherapy, the overall analysis of both RCTs and non-RCTs demonstrated that chemotherapy improved the 2-year survival, but not the 1- or 3-year survival. The subgroup analysis of RCTs showed that the 1-, 2-, and 3-year recurrence were statistically similar between the two groups. As for the post-operative transarterial chemotherapy, the overall analysis of both RCTs and non-RCTs demonstrated that chemotherapy improved the 1-, 2-, and 3-year survival. The subgroup analysis of RCTs showed that chemotherapy improved the 2- and 3-year survival, but not the 1-year survival.
Approaches of chemotherapy were mixed in three meta-analyses [92, 112, 147]. The statistical results were largely inconsistent among them. One of them favored the chemotherapy in term of OS [147]; one showed that the OS was statistically similar between the two groups [112]; one demonstrated that the OS was decreased by chemotherapy [92].
RCT studies were included in the meta-analyses by Zheng (n = 13), Wang (n = 8), and Ono (n = 3).
The meta-analysis by Zheng had a larger number of included studies than those by Wang and Ono (48 versus 8 and 3) (Supplementary Table S19).
Given its superiority in the quantity of RCT studies, the results of the meta-analysis by Zheng might be more reliable.
Surgical resection + immunotherapy versus surgical resection alone
Four meta-analyses compared the outcomes of surgical resection in combination with immunotherapy versus surgical resection alone [32, 75, 112, 124]. All of them demonstrated that the OS was statistically similar between the two groups [32, 75, 112, 124]. One of them favored the combination therapy in term of RFS. One of them favored the combination therapy in terms of 1- and 3-year recurrence [124]; one favored the combination therapy in term of 1-year recurrence, but not 3-year recurrence [75]; one showed that the recurrence was statistically similar between the two groups [32].
Only RCT studies were included in the meta-analyses by Xie (n = 6), Ma (n = 4), Wang (n = 3), and Flores (n = 2).
The meta-analysis by Xie had the largest number of included studies followed by those by Ma, Wang, and Flores (6 versus 4, 3, and 2) (Supplementary Table S20). Notably, there was an overlap of included studies among them.
Given its superiority in the quantity of RCT studies, the results of the meta-analysis by Xie might be more reliable. In details, the adjunctive use of immunotherapy might not be favored in patients undergoing surgical resection.
Surgical resection + PVE versus surgical resection alone
One meta-analysis compared the outcomes of surgical resection in combination with PVE versus surgical resection alone [145]. The 1-, 3-, and 5-year survival and intrahepatic and distant recurrence were statistically similar between the two groups [145].
Only non-RCT studies were included in the meta-analysis by Zhao.
Ablation therapy
RFA versus surgical resection
Eighteen meta-analyses compared the outcomes of RFA versus surgical resection [11, 16, 24, 27, 31, 33, 47, 61, 69, 72, 89, 97, 106, 117, 119, 127, 151, 153]. As for the OS, seven of them favored surgical resection [27, 31, 47, 61, 97, 106, 127]; four demonstrated that the OS was statistically similar between the two groups [11, 16, 119, 151]; four showed that the 1-year survival was statistically similar between the two groups, but the 5-year survival was better in surgical resection group [33, 72, 89, 117]; one found that the 1- and 5-year survival were statistically similar between the two groups, but the 3-year survival was better in surgical resection group [155]; one reported that surgical resection had better OS than RFA in the subgroup analyses of a single nodule 3–5 cm and ≤ 3 cm, but the OS was statistically similar between the two groups in the subgroup analyses of a single nodule < 2 cm and 2–3 nodules < 3 cm [24].
As for the DFS, nine of them favored surgical resection in terms of DFS/RFS at any time points [11, 27, 31, 61, 72, 89, 97, 106, 155]; three showed that the 1-year DFS was statistically similar between the two groups, but the 3- and/or 5-year DFS were better in surgical resection group than in RFA group [16, 33, 151]; one reported that surgical resection had better DFS than RFA in the subgroup analyses of a single nodule 3–5 cm and ≤ 3 cm, but the DFS was statistically similar between the two groups in the subgroup analyses of a single nodule < 2 cm and 2–3 nodules < 3 cm [24].
As for the recurrence, three of them favored surgical resection [11, 47, 61]; two favored RFA [127, 151]; one found that the recurrence was statistically similar between the two groups [24]; three showed that the 1-year recurrence was statistically similar between the two groups, but the 3-year recurrence was less in surgical resection group than in RFA group [31, 33, 117]; one reported that the 1- and 3-year recurrence were statistically similar between the two groups, but the recurrence at the end of follow-up was less in RFA group than in surgical resection group [69]; one demonstrated that the distant intrahepatic recurrence was statistically similar between the two groups, but the local intrahepatic recurrence was less in surgical resection group than in RFA group [153]; one favored surgical resection in term of recurrence at previous sites, but favored RFA in term of recurrence at new sites [72].
According to the description of each meta-analysis, RCT studies were included the meta-analyses by Liu (Surg Laparosc Endosc Percutan Tech, 2010) (n = 8), Ni (n = 6), Fu (n = 5), Zhou (Zhonghua Wai Ke Za Zhi, 2011) (n = 4), Hu (n = 4), Feng (n = 3), Qi (n = 3), Wang (n = 3), Weis (n = 3), Duan (n = 2), Li (n = 2), Sun (n = 2), Xu (n = 2), Chen (n = 1), and Zhou (BMC Gastroenterol, 2010) (n = 1). The information regarding the inclusion of RCT studies was not available in the meta-analyses by Cai and Cucchetti. After checking the relevant information, we confirmed the following: 1) in the meta-analysis by Liu (Surg Laparosc Endosc Percutan Tech, 2010), all included studies were non-RCTs; 2) in the meta-analysis by Ni, there were one RCT regarding resection v.s. PEI, one RCT regarding resection v.s. PEI or microwave ablation, and two RCTs with overlapped data; 3) in the meta-analysis by Fu, there were one RCT regarding comparison of resection v.s. PEI or microwave ablation and two RCTs with overlapped data; 4) in the meta-analysis by Zhou (Zhonghua Wai Ke Za Zhi, 2011), one included study was non-RCT; and 5) because no included studies were listed in the meta-analysis by Hu, we could not check the accuracy. Thus, the largest number of RCT studies included in the meta-analyses should be 3.
The meta-analysis by Wang had the largest number of included studies (n = 28) followed by the meta-analyses by Feng (n = 23), Hu (n = 18), Cucchetti (n = 17), Xu (n = 13), Duan (n = 12), Sun (n = 11), Zhou (BMC Gastroenterol, 2010) (n = 10), Ni (n = 10), Liu (World J Gastroenterol, 2010) (n = 10), Liu (Surg Laparosc Endosc Percutan Tech, 2010) (n = 8), Li (n = 6), Chen (n = 6), Fu (n = 5), Cai (n = 5), Zhou (Zhonghua Wai Ke Za Zhi, 2011) (n = 4), Weis (n = 3), and Qi (n = 3) (Supplementary Table S21).
Given the superiority in the quantity of RCT studies, the meta-analyses by Feng, Qi, Wang, and Weis might be more reliable. In details, surgical resection should be superior to RFA for the improvement of OS.
PEI versus surgical resection
Two meta-analyses compared the outcomes of PEI versus surgical resection [46, 100]. Both of them demonstrated that OS and RFS were statistically similar between the two groups [46, 100].
Only one RCT study was included in the meta-analysis by Schoppmeyer.
The meta-analysis by Hoshida had a larger number of included studies than that by Schoppmeyer (5 versus 1) (Supplementary Table S22). However, no included studies were overlapped between them.
The results were completely consistent between the two meta-analyses. In details, PEI was similar to surgical resection in terms of OS and RFS.
Non-surgical-resection ablation versus surgical resection
One meta-analysis compared the outcomes of non-surgical-resection ablation versus surgical resection [26]. The 1- and 3-year survival and DFS were statistically similar between the two groups [26].
RFA versus PEI or PAI
Eight meta-analyses compared the outcomes of RFA versus PEI or PAI [9, 20, 26, 38, 93, 102, 119, 130]. All of them favored RFA over PEI in terms of OS, DFS, and/or recurrence [9, 20, 26, 38, 93, 102, 119, 130]. Additionally, one of them found that the OS, local recurrence, de novo tumor, and adverse event were statistically similar between RFA and PAI groups [38].
RCT studies were included in the meta-analyses by Bouza (n = 6), Weis (n = 6), Xu (n = 6), Dong (n = 5), Germani (n = 5), Orlando (n = 5), Cho (n = 4), and Shen (n = 4).
The meta-analyses by Bouza, Weis, and Xu had the largest number of included studies (n = 6) followed by the meta-analyses by Dong (n = 5), Germani (n = 5), Orlando (n = 5), Shen (n = 5), and Cho (n = 4) (Supplementary Table S23).
The results regarding the comparison between RFA v.s. PEI were completely consistent among meta-analyses. In details, RFA should be superior to PEI for the improvement of OS and DFS.
RFA versus cryosurgery ablation
One meta-analysis compared the outcomes of RFA versus cryosurgery ablation [51]. Although the OS was statistically similar between the two groups, RFA had less recurrence and complications than cryosurgery ablation [51].
RFA versus other therapeutic methods
One meta-analysis compared the outcomes of RFA versus any other therapeutic methods [50]. RFA was superior to other treatment methods for early HCC in terms of local recurrence and 3-year survival [50]. However, no subgroup analysis was performed according to the different treatment modalities.
Additionally, one meta-analysis compared the outcomes of RFA versus microwave or laser ablation [119]. However, only one trial was identified for each comparison.
PEI versus PAI
Two meta-analyses compared the outcomes of PEI versus PAI [38, 100]. Both of them showed that the OS, RFS, and recurrence were statistically similar between the two groups [38, 100].
RCT studies were included in the meta-analyses by Germani (n = 2) and Schoppmeyer (n = 2).
Both of them had a similar number of included studies (n = 2) (Supplementary Table S24). However, not all of the included studies were identical.
The results were completely consistent between the two meta-analyses. In details, PEI was similar to PAI in terms of OS and RFS.
RFA + TACE versus mono-therapy
Eleven meta-analyses compared the outcomes of RFA in combination with TACE versus RFA or TACE alone [26, 45, 53, 55, 68, 71, 74, 87–88, 133, 144]. Seven of them favored the combination therapy in term of OS [45, 53, 55, 71, 88, 133, 144]; two favored the combination therapy in terms of 1- and 3-year survival, but not 5-year survival [74, 87]; one favored the combination therapy in term of 5-year survival, but not 1- or 3-year survival [26]; one found that the 1-year survival was statistically similar between the two groups [68].
Three meta-analyses compared the RFS of RFA in combination with TACE versus RFA or TACE alone [71, 87–88]. As for the 1-year RFS, one meta-analysis favored the combination therapy [71], but another two showed that the 1-year RFS was statistically similar between the two groups [87–88]. By comparison, all of them favored the combination therapy in term of 3-year RFS [71, 87–88].
RCT studies were included in the meta-analyses by Zhao (n = 21), Jiang (n = 8), Kong (n = 8), Ni (World J Gastroenterol, 2013) (n = 8), Yan (n = 8), Liu (n = 7), Lu (n = 7), Ni (J Cancer Res Clin Oncol, 2013) (n = 6), and Liao (n = 1), but not in the meta-analyses by Dong and Han.
The meta-analysis by Zhao had the largest number of included studies (n = 21), followed by those by Jiang (n = 19), Kong (n = 19), Yan (n = 19), Yan (n = 18), Han (n = 8), Ni (World J Gastroenterol, 2013) (n = 8), Liu (n = 7), Lu (n = 7), Ni (J Cancer Res Clin Oncol, 2013) (n = 6), Dong (n = 5), and Liao (n = 1) (Supplementary Table S25). Notably, all of the 19 included studies were completely identical among the three meta-analyses by Jiang, Kong, and Yan.
Given the superiority in the number of RCTs, the meta-analyses by Zhao, Jiang, Kong, Ni, and Yan should be more reliable. In details, RFA in combination with TACE should be favored in term of OS.
PEI + TACE versus mono-therapy
Three meta-analyses compared the outcomes of PEI in combination with TACE versus PEI or TACE alone [68, 114–115]. Two of them favored the combination therapy in term of OS [114–115]. Another one meta-analysis was performed according to the study design. In the subgroup analysis of RCTs, the combination therapy significantly improved the 3-year survival, rather than 1-year survival. By contrast, in the subgroup analysis of observational studies, the combination therapy significantly improved the 1-year survival, rather than 3-year survival [68].
RCT studies were included in all of the 3 meta-analyses by Wang N (Med Oncol, 2011) (n = 7), Wang W (Liver Int, 2010) (n = 6), and Liao (PLoS One, 2013) (n = 4).
The meta-analysis by Wang N (Med Oncol, 2011) had a larger number of included studies than those by Wang W (Liver Int, 2010) and Liao (7 versus 6 and 4) (Supplementary Table S26). However, not all studies included by Wang W and Liao were included by Wang N.
Given the superiority in the number of RCTs, the meta-analysis by Wang N (Med Oncol, 2011) might be more reliable. In details, PEI in combination with TACE should be favored in term of OS.
Any ablation therapy + TACE versus mono-therapy
Two meta-analyses compared the outcomes of unclassified ablation therapies in combination with TACE versus mono-therapy [42, 115]. Both of them favored the combination therapy in terms of OS, recurrence, and tumor response [42, 115].
RCT studies were included in the meta-analyses by Wang (n = 10) and Gu (n = 7).
The meta-analysis by Gu had a larger number of included studies than that by Wang (18 versus 10) (Supplementary Table S27). However, not all studies included by Wang were included by Gu.
The results were completely consistent between the two meta-analyses. In details, TACE in combination with ablation therapy was favored.
TACE
TACE/TAE versus no active treatment
Seven meta-analyses compared the outcomes of TACE/TAE versus no active treatment or supportive care [12, 39, 57, 73, 77, 91, 132]. Two of them showed that the OS was statistically similar between the two groups [39, 91]; another five favored TACE/TAE in term of OS [12, 57, 73, 77, 132].
RCT studies were included in the meta-analyses by Marelli (n = 9), Oliveri (n = 8), Llovet (n = 7), Camma (n = 5), Geschwind (n = 4), and Leng (n = 2), but not in the meta-analysis by Xue.
The meta-analysis by Marelli had the largest number of included studies (n = 9) followed by those by Oliveri (n = 8), Xue (n = 8), Llovet (n = 7), Camma (n = 5), Geschwind (n = 4), and Leng (n = 3) (Supplementary Table S28). However, not all included studies were completely overlapped among them.
Given the superiority in the number of RCTs, the meta-analysis by Marelli might be more reliable. In details, TACE/TAE should be favored.
TACE versus TAE
Three meta-analyses compared the outcomes of TACE versus TAE [12, 77, 125]. All of them showed that the OS was statistically similar between the two groups [12, 77, 125].
Only RCT studies were included in the meta-analyses by Xie (n = 5), Marelli (n = 3), and Camma (n = 2).
The meta-analysis by Xie had a larger number of included studies than those by Marelli and Camma (5 versus 3 and 2) (Supplementary Table S29). However, not all included studies were completely overlapped among them.
The results were completely consistent among them. In details, TACE was similar to TAE in term of OS.
Drug-eluting bead (DEB)-TACE versus conventional TACE (cTACE)
Three meta-analyses compared the outcomes of DEB-TACE versus cTACE [37, 44, 48]. One of them evaluated the OS [48]. DEB-TACE was significantly better than cTACE in terms of 1- and 2-year survival. But the 6-month and 3-year survival were statistically similar between the two groups.
Two of them demonstrated that tumor response or disease control rate was statistically similar between them. Another one meta-analysis demonstrated that tumor response rate was significantly higher in DEB-TACE group than in cTACE group.
Two of them evaluated the complications [37, 44]. The incidence of complications was statistically similar between the two groups.
RCT studies were included in the meta-analyses by Han (n = 3) and Huang (n = 2), but not in the meta-analysis by Gao.
The meta-analysis by Huang had a larger number of included studies than those by Han and Gao (7 versus 5 and 2) (Supplementary Table S30). However, not all included studies were completely overlapped among them.
Given the superiority in the number of RCTs, the meta-analysis by Han might be more reliable. In details, DEB-TACE was similar to cTACE in the term of tumor response.
TACE versus microsphere embolization
One meta-analysis compared the outcomes of TACE versus microsphere embolization [123]. Microsphere embolization was superior to TACE in terms of OS, TTP, and tumor response [123]. In the subgroup analyses, the benefit was statistically significant in patients undergoing 32P glass microspheres, but not in those undergoing 90Y microspheres.
RCT studies were included in the meta-analysis by Xie (n = 7).
TACE + sorafenib versus TACE
Four meta-analyses compared the outcomes of TACE in combination with sorafenib versus TACE alone [35, 70, 134, 140]. Three of them favored the combination therapy in term of OS [35, 134, 140], but another one found that the OS was statistically similar between the two groups [70]. The survival benefit of the combination therapy was statistically significant in the subgroup analysis of retrospective studies, but not in that of RCTs [134].
RCT studies were included in the meta-analyses by Liu (n = 3), Yang (n = 3), and Zhang (n = 2), but not in the meta-analysis by Fu.
The meta-analysis by Fu had the largest number of included studies (n = 9), followed by those by Liu (n = 7), Yang (n = 6), and Zhang (n = 6) (Supplementary Table S31). However, not all included studies were completely overlapped among the 4 meta-analyses.
Given the superiority in the number of RCTs, the meta-analysis by Liu and Yang might be more reliable. In details, TACE plus sorafenib was not favored in term of OS.
TACE + high-intensity focused ultrasound (HIFU) versus TACE
Two meta-analyses compared the outcomes of TACE in combination with HIFU versus TACE alone [13, 68]. One of them demonstrated that both OS and tumor response were improved by the combination therapy [13]. Another one meta-analysis was performed according to the study design [68]. In the subgroup analysis of observational studies, both 1- and 3-year survival were significantly improved by the combination therapy [68]. By comparison, in the subgroup analysis of RCTs, only 1-year survival, rather than 3-year survival, was significantly improved by the combination therapy [68].
RCT study was included in the meta-analysis by Liao (n = 1), but not in the meta-analysis by Cao.
The meta-analysis by Cao had a larger number of included studies than that by Liao (9 versus 5) (Supplementary Table S32). All studies which were included in the meta-analysis by Liao were also included in the meta-analysis by Cao.
Given the superiority in the number of RCTs, the meta-analysis by Liao might be more reliable. In details, TACE plus HIFU should be favored in term of 1-year survival, but not 3-year survival.
TACE + thermotherapy versus TACE
Only one meta-analysis compared the outcomes of TACE in combination with thermotherapy versus TACE alone [64]. Both 1- and 2-year survival were significantly improved by the combination therapy, but the 0.5-, 1.5-, and 3-year survival were statistically similar between the two groups [64]. Additionally, the overall effective rate and quality of life were improved by the combination therapy [64].
TACE + AHCS versus TACE or AHCS
Only one meta-analysis compared the outcomes of TACE in combination with AHCS versus TACE or AHCS alone [65]. Compared with TACE alone, the combination therapy had significantly better 0.5-, 1-, 1.5-, 2-, and 2.5-year survival, but the 3-year survival was statistically similar between the two groups [65]. Compared with AHCS alone, the combination therapy had significantly better 0.5-, 1.5-, 2-, and 2.5-year survival, but similar 1- and 3-year survival [65]. Additionally, the combination therapy was superior to the mono-therapy in terms of total effective rate, complete necrosis rate, recurrence, AFP reduction, and CD4 improvement.
TACE + radiotherapy versus TACE alone
Two meta-analyses compared the outcomes of TACE in combination with radiotherapy versus TACE alone [68, 80]. Both of them demonstrated that the combination therapy had significantly better 1-, 2-, 3-, and 5-year survival than TACE alone [68, 80]. Additionally, one of them showed that the combination therapy significantly increased the tumor response, but did not influence the development of adverse events, such as nausea/vomit, leukocyte count declined, alanine aminotransferase level increased, and total bilirubin level increased [80].
RCT studies were included in the meta-analyses by Meng (n = 5) and Liao (n = 3).
The meta-analysis by Meng had a larger number of included studies than that by Liao (17 versus 7) (Supplementary Table S33). All studies which were included in the meta-analysis by Liao were also included in the meta-analysis by Meng.
The results regarding the OS were completely consistent among them. In details, TACE plus radiotherapy should be favored in term of OS.
TACE + 3D-CRT versus TACE alone
Only one meta-analysis compared the outcomes of TACE in combination with 3D-CRT versus TACE alone [68]. Regardless of study design, the combination therapy was superior to TACE alone in terms of 1- and 3-year survival [68].
Only one RCT study was included in the meta-analysis by Liao.
TACE + TCMs versus TACE alone
Six meta-analyses compared the outcomes of TACE in combination with TCMs versus TACE alone [18–19, 79, 81, 108, 122]. Three of them favored the combination therapy in term of OS [18, 79, 108]; one favored the combination therapy in terms of 1-, 2-, and 3-year survival, but not 6-month survival [19]; one favored the combination therapy in term of 2-year survival, but not 1-year survival [122]; one did not report the survival data [81].
Five of them favored the combination therapy in term of tumor response [18–19, 79, 81, 122]. Another one did not report the relevant data [108].
Four of them favored the combination therapy in term of quality of life [18–19, 79, 108]. Another two did not report the relevant data [81, 122].
RCT studies were included in the meta-analyses by Cheung (n = 67), Cho (n = 30), and Meng (Explore (NY), 2011) (n = 11), but not in the meta-analyses by Sun and Wu. The information regarding the inclusion of RCTs was not reported in the meta-analysis by Meng (J Altern Complement Med, 2008).
The meta-analysis by Cheung had the largest number of included studies (n = 67), followed by those by Meng (n = 37), Cho (n = 30), Meng (n = 12), Sun (n = 10), and Wu (n = 9) (Supplementary Table S34). However, not all included studies were completely overlapped among the 6 meta-analyses.
Given the superiority in the number of RCTs, the meta-analysis by Cheung might be more reliable. In details, TACE plus TCMs should be favored in terms of OS, tumor response, and quality of life.
TACE + CIK cell therapy versus TACE alone
Two meta-analyses compared the outcomes of TACE in combination with CIK cell therapy versus TACE alone [14, 63]. The combination therapy was beneficial in terms of OS, RFS, TTP, quality of life, and liver and immune function [14, 63]. Additionally, one of them evaluated whether or not adjunctive CIK cell therapy could improve the outcomes of TACE in combination with RFA [63]. Adjunctive CIK cell therapy was beneficial in terms of OS and RFS [63].
RCT studies were included in the meta-analyses by Chen (n = 9) and Li (n = 6).
The meta-analysis by Li had a larger number of included studies than that by Chen (11 versus 9) (Supplementary Table S35). However, not all included studies were completely overlapped between them.
The results regarding the OS were completely consistent among them. In details, TACE in combination with CIK cell therapy should be favored.
Sorafenib
Seven meta-analyses compared the outcomes of sorafenib versus placebo (Supplementary Table S1) [22, 28, 101, 118, 141, 143, 160]. The use of sorafenib was beneficial in terms of OS, TTP, and disease control rate [22, 101, 118, 141, 143, 160]. However, the time to symptomatic progression was statistically similar between the two groups [22, 118, 160]. The incidence of adverse events was significantly increased by the use of sorafenib [28, 101, 118, 141, 143, 160].
RCT studies were included in the meta-analyses by Shen (n = 5), Duffy (n = 4), Wang (n = 4), Zhang T (Anticancer Drugs, 2010) (n = 3), Zhang X (Hepatobiliary Pancreat Dis Int, 2012) (n = 3), Cinco (n = 2), and Zou (n = 2).
The meta-analysis by Shen had a larger number of included studies than those by Wang, Duffy, Zhang T (Anticancer Drugs, 2010), Zhang X (Hepatobiliary Pancreat Dis Int, 2012), Zou, and Cinco (5 versus 4, 4, 3, 3, 2, and 2) (Supplementary Table S36). All studies which were included in the meta-analysis by Wang, Duffy, Zhang T (Anticancer Drugs, 2010), Zhang X (Hepatobiliary Pancreat Dis Int, 2012), and Zou were also included by Shen. In the meta-analysis by Cinco, the included studies were not reported.
The results were completely consistent among them. In details, sorafenib should be favored.
Antiviral therapy
Nineteen meta-analyses compared the outcomes of antiviral therapy versus no antiviral therapy (Supplementary Table S2) [10, 49, 54, 56, 58, 84–86, 103, 105, 107, 112, 120, 128, 139, 142, 154, 158–159]. Thirteen of them favored the use of antiviral therapy in term of OS [10, 49, 54, 84, 86, 105, 107, 112, 120, 128, 139, 142, 154]; one found that the use of antiviral therapy significantly improved the 5-year survival in HCV patients, but not HBV patients [58]; one demonstrated that the 1-year survival was statistically similar between the two groups [56]; one showed that 1-, 2-, 3-, 4-, and 5-year survival were statistically similar between the two groups [159]; another three did not report the survival data [85, 103, 158].
Five meta-analyses evaluated the DFS/RFS [49, 56, 103, 112, 154]. Four of them favored the use of antiviral therapy in term of DFS/RFS [56, 103, 112, 154]. Another one meta-analysis was performed according to the study design and type of viral hepatitis. In the subgroup analysis of RCTs, the DFS/RFS was statistically similar between the two groups regardless of HCV or HBV [49]. In the subgroup analysis of non-RCTs, antiviral therapy improved the DFS/RFS by in HCV patients, but not HBV patients [49].
Fifteen meta-analyses evaluated the recurrence [10, 54, 56, 58, 84–85, 105, 107, 120, 128, 139, 142, 154, 158–159]. Ten of them favored the use of antiviral therapy in term of recurrence [10, 56, 84–85, 105, 107, 120, 139, 154, 158]; one favored the use of antiviral therapy after TACE, but not surgical resection [54]; two favored the use of antiviral therapy in HCV patients, but not HBV patients [58, 128]; one favored the use of antiviral therapy in terms of 1-, 3-, and 4-year recurrence, but not 2- or 5-year recurrence [159]; one favored the use of antiviral therapy in terms of 1- and 2-year recurrence, but not late recurrence (> 2 year) [142].
RCT studies were included in the meta-analyses by Zhuang (PLoS One, 2013) (n = 13), Huang (n = 10), Shen (n = 9), Wang (n = 9), Zhang (Mol Clin Oncol, 2014) (n = 9), Jiang (n = 8), Li (n = 8), Zhuang (Zhonghua Gan Zang Bing Za Zhi, 2012) (n = 8), Breitenstein (n = 7), Zhang (Int J Cancer, 2009) (n = 6), Miao (n = 5), Singal (n = 5), Xu (n = 5), Moriguchi (n = 4), Miyake (n = 3), Sun (n = 1), and Zhou (n = 1), rather than those by Lan and Wong.
The meta-analysis by Huang had a larger number of included studies than those by Zhang, Zhou, Miao, Shen, Sun, Zhuang (PLoS One, 2013), Jiang, Lan, Miyake, Singal, Wang, Wong, Xu, Li, Zhang, Zhuang (Zhonghua Gan Zang Bing Za Zhi, 2012), Breitenstein, and Moriguchi (23 versus 19, 14, 13, 13, 13, 13, 10, 10, 10, 10, 9, 9, 9, 8, 8, 8, 7, and 4) (Supplementary Table S37). In the meta-analysis by Moriguchi, the included studies were not reported. However, not all included studies were completely overlapped between them.
Given the superiority in the number of RCTs, the meta-analysis by Zhuang (PLoS One, 2013) and Huang might be more reliable. In details, interferon therapy after curative treatment should be favored.
Vitamin
Five meta-analyses compared the outcomes of vitamin versus placebo (Supplementary Table S3) [21, 82, 99, 112, 150]. Two of them favored the use of vitamin in term of OS [112, 150]; two favored the use of vitamin in term of 2-year survival, but not 3-year survival [21, 82]; one showed that the 1- and 2-year survival were statistically similar between the two groups [99].
One meta-analysis favored the use of vitamin in term of RFS [112].
Two meta-analyses favored the use of vitamin in term of 1-year recurrence, but another two did not [21, 82]. Four meta-analyses favored the use of vitamin in terms of 2- and 3-year recurrence [21, 82].
RCT studies were included in the meta-analyses by Wang (n = 6), Zhong (n = 6), Chu (n = 5), Riaz (n = 5), and Meng (n = 4).
The meta-analysis by Zhong had a larger number of included studies than those by Chu, Wang, Riaz, and Meng (7 versus 6, 6, 5, and 4) (Supplementary Table S38). In the meta-analysis by Meng, the included studies were not reported. However, not all included studies were completely overlapped between them.
Given the superiority in the number of RCTs, the meta-analyses by Wang and Zhong should be more reliable. In details, the use of vitamin should be favored in term of OS. However, its benefit was weak.
Octreotide
Three meta-analyses compared the outcomes of octreotide versus placebo (Supplementary Table S4) [29, 43, 52]. As for the 6- and 12-month survival, one of them favored the use of octreotide [52], but another two did not show any significant difference between the two groups [29, 43]. As for the 24-month survival, two of them showed that the survival was statistically similar between the two groups [29, 43], but another one did not report the relevant data [52].
RCT studies were included in the meta-analyses by Ji (n = 9) and Guo (n = 6).
The meta-analysis by Ji had a larger number of included studies than those by Guo and Estanislao (11 versus 6 and 3) (Supplementary Table S39). In the meta-analysis by Estanislao, the included studies were not reported. All studies which were included in the meta-analysis by Guo were also included by Ji.
Given the superiority in the number of RCTs, the meta-analyses by Ji and Guo might be more reliable. In details, the benefit of octreotide remains uncertain.
TCM
One meta-analysis compared the outcomes of kanglaite injection plus hepatic arterial intervention versus hepatic arterial intervention alone (Supplementary Table S5) [34]. The combination therapy was beneficial in terms of tumor response, Karnofsky score improvement, and pain relief [34]. But neither OS nor DFS/RFS was evaluated [34].
One meta-analysis compared the outcomes of Chinese herbal medicine plus chemotherapy versus chemotherapy alone [104]. The combination therapy was beneficial in terms of OS and tumor response [104].
One meta-analysis compared the outcomes of TCM versus other treatment [121]. TCM was superior to other treatments in terms of OS and tumor response [121].
CIK cell therapy
One meta-analysis compared the outcomes of CIK cell therapy versus other treatment (Supplementary Table S6) [76]. CIK cell therapy was superior to other treatments in terms of OS, PFS, disease control rate, tumor response, and quality of life [76].
Tamoxifen
Two meta-analyses compared the outcomes of tamoxifen versus placebo or no treatment (Supplementary Table S7) [73, 90]. Both of them demonstrated that the OS was statistically similar between the two groups [73, 90].
RCT studies were included in the meta-analyses by Nowak (n = 10) and Llovet (n = 7).
Although the meta-analysis by Nowak had a larger number of included studies than that by Llovet (10 versus 7) (Supplementary Table S40), the included studies were not similar between them.
The results were completely consistent among them. In details, tamoxifen should not be favored.
Antibiotics
One meta-analysis compared the outcomes of antibiotics versus no antibiotics after hepatic transarterial therapy [113]. The incidence of fever, bacteremia, septicema, and sepsis were not significantly improved by antibiotics [113].
DISCUSSION
AASLD and EASL guidelines recommend BCLC staging algorithm for the management of HCC. Only 5 treatment modalities have been considered in the current guidelines. In details, the therapeutic modalities of HCC include the LT, surgical resection, and RFA for HCC in the stage 0 and A, TACE for HCC in the stage B, sorafenib for HCC in the stage C, and supportive treatment for HCC in the stage D. However, the BCLC staging algorithm is not flawless and needs to be persistently updated. Nowadays, more and more novel treatment modalities have been widely produced and adopted. Their efficacy and safety have been gradually established. In this circumstance, our study was worthwhile, because it attempted to collect the relevant evidence as many as possible and to provide an overview of outcomes of novel and well-established treatment modalities for HCC based on the results of meta-analyses. More notably, we found that lots of combination therapy might be more effective and safe. For example, the meta-analyses of RCTs demonstrated that RFA plus TACE was superior to mono-therapy, and that surgical resection plus post-operative TACE was superior to surgical resection alone. Given the quality of such meta-analyses, the guidelines should be updated regarding the use of combination therapy.
Limitations
This was a time-consuming work, because a large number of relevant meta-analyses were included. Several limitations should be acknowledged. First, we must clarify that only the results of meta-analyses, but not the accuracy of meta-analyses, were systematically reviewed. Because we cannot repeat every meta-analysis, we cannot guarantee that their findings were accurate. Second, we did not consider the heterogeneity among included studies in every meta-analysis. A significant heterogeneity could affect the stability of a meta-analysis. Third, we arbitrarily evaluated the reliability of meta-analyses according to the number of RCTs and non-RCTs.
Recommendations
LT
1. LDLT has lower DFS than DDLT (grade of recommendation: low).
2. Short- and long-term outcomes may be comparable between primary and salvage LT (grade of recommendation: low).
3. Sirolimus-based immunosuppression should be recommended after LT (grade of recommendation: low).
Surgical resection
1. Surgical resection margin aiming at 2 cm may be superior to 1 cm for the improvement of long-term outcomes (grade of recommendation: moderate).
2. Survival benefit may be comparable between laparoscopic and open resection. Additionally, laparoscopic resection had less blood loss, blood transfusion, and complications and shorter hospital stay (grade of recommendation: low).
3. Anatomic resection, but not non-anatomic resection, should be recommended (grade of recommendation: low).
4. Adjunctive I131 lipiodol therapy may be considered in patients undergoing surgical resection (grade of recommendation: low).
5. Post-operative TACE, but not pre-operative TACE, may be considered in patients undergoing surgical resection (grade of recommendation: high).
6. Immunotherapy may not be considered in patients undergoing surgical resection (grade of recommendation: high).
7. PVE may not be considered in patients undergoing surgical resection (grade of recommendation: low).
Ablation
1. Surgical resection should be superior to RFA in term of OS (grade of recommendation: high).
2. RFA, but not PEI or cryosurgery ablation, should be recommended (grade of recommendation: high).
3. RFA in combination with TACE may be superior to TACE or RFA mono-therapy (grade of recommendation: high).
4. PEI in combination with TACE may be superior to TACE or PEI mono-therapy (grade of recommendation: high).
TAE/TACE
1. TACE/TAE should be superior to placebo (grade of recommendation: high).
2. Survival benefit may be comparable between TACE and TAE (grade of recommendation: high).
3. DEB-TACE was comparable to conventional TACE (grade of recommendation: high).
4. 32P glass microspheres embolization may be superior to TACE for the improvement of OS (grade of recommendation: high).
5. Adjunctive HIFU therapy may further improve the outcomes of TACE (grade of recommendation: moderate).
6. Adjunctive radiotherapy therapy may further improve the outcomes of TACE (grade of recommendation: high).
7. Adjunctive 3D-CRT therapy may further improve the outcomes of TACE (grade of recommendation: moderate).
8. Adjunctive TCMs therapy may further improve the outcomes of TACE (grade of recommendation: high).
9. Adjunctive CIK cell therapy may further improve the outcomes of TACE (grade of recommendation: high).
Sorafenib
1. Sorafenib is superior to placebo for the improvement of OS (grade of recommendation: high).
Other treatments
1. Antiviral therapy should be recommended for the improvement of recurrence (grade of recommendation: high).
2. Vitamin should be recommended for the improvement of OS (grade of recommendation: high).
3. Tamoxifen should not be recommended (grade of recommendation: high).
Uncertainties
1. The superiority of LT to surgical resection for the improvement of OS remains inconclusive. The accurate candidates for LT and surgical resection need to be clearly established.
2. The superiority of surgical resection to RFA for the improvement of OS remains under debate. The indications of RFA should be refined.
3. Although transarterial radioembolization appears to be more advantageous than TACE, their cost-effectiveness should be further explored.
4. Although TACE appears to be more effective than no treatment, the survival benefit of TAE/TACE versus other active treatments should be confirmed.
5. The benefits of combination therapy may be confirmed in the future guidelines.
MATERIALS AND METHODS
Search strategy and study selection
We searched all meta-analysis papers regarding the treatment of HCC via the PubMed, EMBASE, and Cochrane library databases. Search items were as follows: (hepatocellular carcinoma) AND (meta-analysis). The last search was performed on October 1, 2014.
Eligibility criteria were as follows. 1) All meta-analyses regarding the treatment of HCC were included. 2) Duplicate publications were excluded. 3) Narrative reviews were excluded. 4) Only systematic reviews without meta-analyses were excluded. 5) Only systematic review protocols were excluded. 6) Patients without HCC were excluded. 7) Other topics, but not treatment modalities, were excluded.
Primary outcomes were overall survival (OS), diseases-free survival (DFS) or recurrence-free survival (RFS), progression or time-to-progression (TTP), progression-free survival (PFS), recurrence or time-to-recurrence, safety, and other endpoints.
Reliability of meta-analyses
As the results were different among the meta-analyses, the reliability was evaluated according to the quality and quantity of original studies included in every meta-analysis. First, we evaluated the quality of original studies. If a larger number of randomized controlled trials (RCTs) were included, the results of a meta-analysis would be more reliable. Second, if the number of randomized controlled trials was similar, we further evaluated the number of non-RCT studies. If a larger number of non-RCT studies were included, the results of a meta-analysis would be more reliable. Third, if the number of RCT and non-RCT studies included was similar but the results were different among meta-analyses, we further evaluated the statistical methods. Hazard ratio could reflect a general effect over time; by comparison, odds ratio or risk ratio reflected an individual effect at a fixed time point. Thus, if the hazard ratio was calculated, the results of a meta-analysis would be more reliable.
Grade of recommendations
High grade recommendation was considered, if the results of meta-analyses were based on more than 3 single-center RCTs or 1 multi-center RCT. Low grade recommendation was considered, if the results of meta-analyses were based on the non-RCT studies alone. As for something in between, moderate grade recommendation was considered.
Abbreviations
3D-CRT, three-dimensional conformal radiation therapy; AHCS, argon-helium cryotherapy system; CIK, cytokine-induced killer; DDLT, deceased donor liver transplantation; DEB, drug-eluting bead; DFS, diseases-free survival; HCC, hepatocellular carcinoma; HIFU, high-intensity focused ultrasound; LDLT, living donor liver transplantation; LT, liver transplantation; OS, overall survival; PEI, percutaneous ethanol injection; PAI, percutaneous acetic acid injection; PFS, progression-free survival; PVE, portal vein embolization; RCT, randomized controlled trials; RFA, radiofrequency ablation; RFS, recurrence-free survival; TACE, transarterial chemoembolization; TAE, transarterial embolization; TCMs, traditional Chinese medicine; TTP, time-to-progression.
CONFLICTS OF INTEREST
None.
Authors’ contributions
XQ: designed the study, performed the literature search and selection, data extraction, and drafted the manuscript; YZ and HL: performed the literature selection and data extraction; XG and GH: gave critical comments and revised the manuscript. All authors have made an intellectual contribution to the manuscript and approved the submission.
REFERENCES
1. Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012; 379:1245–55.
2. El-Serag HB. Hepatocellular carcinoma. N Engl J Med. 2011; 365:1118–27.
3. Wallace MC, Preen D, Jeffrey GP, Adams LA. The evolving epidemiology of hepatocellular carcinoma: a global perspective. Expert Rev Gastroenterol Hepatol. 2015; 9:765–79.
4. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011; 53:1020–2.
5. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012; 56:908–43.
6. Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: synthesis of best evidence for clinical decisions. Ann Intern Med. 1997; 126:376–80.
7. Oxford Centre for Evidence-based Medicine – Levels of Evidence (March 2009). [cited January 4, 2015]; Available from: http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/.
8. Al Hasan I, Emond JC. Liver trasplantation for HCC, does the type of donor graft really matter? Survival and recurrence meta-anlysis. Liver Transplantation. 2014; 20:S335.
9. Bouza C, Lopez-Cuadrado T, Alcazar R, Saz-Parkinson Z, Amate JM. Meta-analysis of percutaneous radiofrequency ablation versus ethanol injection in hepatocellular carcinoma. BMC Gastroenterol. 2009; 9:31.
10. Breitenstein S, Dimitroulis D, Petrowsky H, Puhan MA, Mullhaupt B, Clavien PA. Systematic review and meta-analysis of interferon after curative treatment of hepatocellular carcinoma in patients with viral hepatitis. Br J Surg. 2009; 96:975–81.
11. Cai H, Zhou T, Qiu YD. Comparison of radiofrequency ablation and surgical resection in patients with solitary hepatocellular carcinoma within 5 cm: A me. HPB. 2013; 15:221.
12. Camma C, Schepis F, Orlando A, Albanese M, Shahied L, Trevisani F, Andreone P, Craxi A, Cottone M. Transarterial chemoembolization for unresectable hepatocellular carcinoma: meta-analysis of randomized controlled trials. Radiology. 2002; 224:47–54.
13. Cao H, Xu Z, Long H, Zhang LL, Zhang J, Peng ZP, Li SL. Transcatheter arterial chemoembolization in combination with high-intensity focused ultrasound for unresectable hepatocellular carcinoma: a systematic review and meta-analysis of the chinese literature. Ultrasound Med Biol. 2011; 37:1009–16.
14. Chen B, Xu X, Xiang M, Yang J, Yu T, Hu Y. Cytokine-induced killer cell combination with TACE in the treatment of hepatocellular cancers: A meta-analysis. Chinese-German Journal of Clinical Oncology. 2013; 12:459–67.
15. Chen J, Huang K, Wu J, Zhu H, Shi Y, Wang Y, Zhao G. Survival after anatomic resection versus nonanatomic resection for hepatocellular carcinoma: a meta-analysis. Dig Dis Sci. 2011; 56:1626–33.
16. Chen RF, Xiao TH, Zhou QB. Therapeutic clinical effect of radiofrequency ablation for small hepatocellular carcinoma in cirrhotic patients: a meta-analysis. [Article in Chinese] Zhonghua Wai Ke Za Zhi. 2008; 46:1413–8.
17. Cheng X, Sun P, Hu QG, Song ZF, Xiong J, Zheng QC. Transarterial (chemo)embolization for curative resection of hepatocellular carcinoma: a systematic review and meta-analyses. J Cancer Res Clin Oncol. 2014; 140:1159–70.
18. Cheung F, Wang X, Wang N, Yuen MF, Ziea TC, Tong Y, Wong VT, Feng Y. Chinese Medicines as an Adjuvant Therapy for Unresectable Hepatocellular Carcinoma during Transarterial Chemoembolization: A Meta-Analysis of Randomized Controlled Trials. Evid Based Complement Alternat Med. 2013; 2013:487919.
19. Cho WC, Chen HY. Transcatheter arterial chemoembolization combined with or without Chinese herbal therapy for hepatocellular carcinoma: meta-analysis. Expert Opin Investig Drugs. 2009; 18:617–35.
20. Cho YK, Kim JK, Kim MY, Rhim H, Han JK. Systematic review of randomized trials for hepatocellular carcinoma treated with percutaneous ablation therapies. Hepatology. 2009; 49:453–9.
21. Chu KJ, Lai EC, Yao XP, Zhang HW, Lau WY, Fu XH, Lu CD, Shi J, Cheng SQ. Vitamin analogues in chemoprevention of hepatocellular carcinoma after resection or ablation—a systematic review and meta-analysis. Asian J Surg. 2010; 33:120–6.
22. Cinco RUC, Ignacio JG, Domingo F. Sorafenib in the treatment of advanced hepatocellular carcinoma: A meta-analysis of randomized trials. Hepatology International. 2011; 5:420.
23. Cucchetti A, Cescon M, Ercolani G, Bigonzi E, Torzilli G, Pinna AD. A comprehensive meta-regression analysis on outcome of anatomic resection versus nonanatomic resection for hepatocellular carcinoma. Ann Surg Oncol. 2012; 19:3697–705.
24. Cucchetti A, Piscaglia F, Cescon M, Colecchia A, Ercolani G, Bolondi L, Pinna AD. Cost-effectiveness of hepatic resection versus percutaneous radiofrequency ablation for early hepatocellular carcinoma. J Hepatol. 2013; 59:300–7.
25. Dhir M, Lyden ER, Smith LM, Are C. Comparison of outcomes of transplantation and resection in patients with early hepatocellular carcinoma: a meta-analysis. HPB (Oxford). 2012; 14:635–45.
26. Dong W, Zhang T, Wang ZG, Liu H. Clinical outcome of small hepatocellular carcinoma after different treatments: a meta-analysis. World J Gastroenterol. 2014; 20:10174–82.
27. Duan C, Liu M, Zhang Z, Ma K, Bie P. Radiofrequency ablation versus hepatic resection for the treatment of early-stage hepatocellular carcinoma meeting Milan criteria: a systematic review and meta-analysis. World J Surg Oncol. 2013; 11:190.
28. Duffy A, Wilkerson J, Greten TF. Hemorrhagic events in hepatocellular carcinoma patients treated with antiangiogenic therapies. Hepatology. 2013; 57:1068–77.
29. Estanislao NI, Ang E, Flores H, Salvana A, Tripon E, Velasquez ME, Ong JP. Octreotide for improving survival in patients with advanced hepatocellular carcinoma: A meta-analysis. Journal of Gastroenterology and Hepatology. 2009; 24.
30. Fancellu A, Rosman AS, Sanna V, Nigri GR, Zorcolo L, Pisano M, Melis M. Meta-analysis of trials comparing minimally-invasive and open liver resections for hepatocellular carcinoma. J Surg Res. 2011; 171:e33–45.
31. Feng Q, Chi Y, Liu Y, Zhang L, Liu Q. Efficacy and safety of percutaneous radiofrequency ablation versus surgical resection for small hepatocellular carcinoma: a meta-analysis of 23 studies. J Cancer Res Clin Oncol. 2014.
32. Flores HF, Ang ER, Estanislao INI. Adjuvant immunotherapy in patients with hepatocellular carcinoma who underwent curative resection: A meta-analysis. Journal of Gastroenterology and Hepatology. 2009; 24:A157.
33. Fu C, Liu N, Deng Q, Li X, Ma K, Bie P. Radiofrequency ablation vs. surgical resection on the treatment of patients with small hepatocellular carcinoma: A system review and meta-analysis of five randomized controlled trials. Hepato-Gastroenterology. 2014; 61:1722–9.
34. Fu F, Wan Y, Wu T. Kanglaite injection combined with hepatic arterial intervention for unresectable hepatocellular carcinoma: A meta-analysis. J Cancer Res Ther. 2014; 10:C38–41.
35. Fu QH, Zhang Q, Bai XL, Hu QD, Su W, Chen YW, Su RG, Liang TB. Sorafenib enhances effects of transarterial chemoembolization for hepatocellular carcinoma: a systematic review and meta-analysis. J Cancer Res Clin Oncol. 2014; 140:1429–40.
36. Furtado R, Crawford M, Sandroussi C. Systematic review and meta-analysis of adjuvant i lipiodol after excision of hepatocellular carcinoma. Ann Surg Oncol. 2014; 21:2700–7.
37. Gao S, Yang Z, Zheng Z, Yao J, Deng M, Xie H, Zheng S, Zhou L. Doxorubicin-eluting bead versus conventional TACE for unresectable hepatocellular carcinoma: a meta-analysis. Hepatogastroenterology. 2013; 60:813–20.
38. Germani G, Pleguezuelo M, Gurusamy K, Meyer T, Isgro G, Burroughs AK. Clinical outcomes of radiofrequency ablation, percutaneous alcohol and acetic acid injection for hepatocelullar carcinoma: a meta-analysis. J Hepatol. 2010; 52:380–8.
39. Geschwind JF, Ramsey DE, Choti MA, Thuluvath PJ, Huncharek MS. Chemoembolization of hepatocellular carcinoma: results of a metaanalysis. Am J Clin Oncol. 2003; 26:344–9.
40. Gong L, Shi L, Sun J, Yuan WS, Chen JF, Liu P, Gong F, Dong JH. Comparative survival analysis of adjuvant therapy with iodine-131-labeled lipiodol to hepatic resection of primary hepatocellular carcinoma: a meta-analysis. Nucl Med Commun. 2014; 35:484–92.
41. Grant RC, Sandhu L, Dixon PR, Greig PD, Grant DR, McGilvray ID. Living vs. deceased donor liver transplantation for hepatocellular carcinoma: a systematic review and meta-analysis. Clin Transplant. 2013; 27:140–7.
42. Gu L, Liu H, Fan L, Lv Y, Cui Z, Luo Y, Liu Y, Li G, Li C, Ma J. Treatment outcomes of transcatheter arterial chemoembolization combined with local ablative therapy versus monotherapy in hepatocellular carcinoma: a meta-analysis. J Cancer Res Clin Oncol. 2014; 140:199–210.
43. Guo TK, Hao XY, Ma B, Yang KH, Li YP, Li HL, Gu YH, Cai H, Liu YL, Li Y, Zhan WP. Octreotide for advanced hepatocellular carcinoma: a meta-analysis of randomized controlled trials. J Cancer Res Clin Oncol. 2009; 135:1685–92.
44. Han S, Zhang X, Zou L, Lu C, Zhang J, Li J, Li M. Does drug-eluting bead transcatheter arterial chemoembolization improve the management of patients with hepatocellular carcinoma? A meta-analysis. PLoS One. 2014; 9:e102686.
45. Han X, Lv WF. Transcatheter arterial chemoembolization combined with radiofrequency ablation for the treatment of hepatocellular carcinoma: A meta-analysis of long-term efficacy. Journal of Interventional Radiology (China). 2013; 22:387–91.
46. Hoshida Y, Shiratori Y, Omata M. Difficulties in conducting controlled trials in radical therapies for nonadvanced hepatocellular carcinoma. Hepatology. 2000; 32:877–80.
47. Hu P, Zhang SJ, Sun AX, Qian GJ. Meta-analysis of survival and disease recurrence for small hepatocellular carcinoma after radiofrequency ablation and surgical resection. HPB. 2013; 15:118.
48. Huang K, Zhou Q, Wang R, Cheng D, Ma Y. Doxorubicin-eluting beads versus conventional transarterial chemoembolization for the treatment of hepatocellular carcinoma. J Gastroenterol Hepatol. 2014; 29:920–5.
49. Huang TS, Shyu YC, Chen HY, Yuan SS, Shih JN, Chen PJ. A systematic review and meta-analysis of adjuvant interferon therapy after curative treatment for patients with viral hepatitis-related hepatocellular carcinoma. J Viral Hepat. 2013; 20:729–43.
50. Huang X, Lu B, Meng LN. A meta-analysis of radiofrequency ablation for early hepatocellular carcinoma. [Article in Chinese] Zhonghua Nei Ke Za Zhi. 2008; 47:217–20.
51. Huang YZ, Zhou SC, Zhou H, Tong M. Radiofrequency ablation versus cryosurgery ablation for hepatocellular carcinoma: a meta-analysis. Hepatogastroenterology. 2013; 60:1131–5.
52. Ji XQ, Ruan XJ, Chen H, Chen G, Li SY, Yu B. Somatostatin analogues in advanced hepatocellular carcinoma: an updated systematic review and meta-analysis of randomized controlled trials. Med Sci Monit. 2011; 17:RA169–76.
53. Jiang G, Xu X, Ren S, Wang L. Combining transarterial chemoembolization with radiofrequency ablation for hepatocellular carcinoma. Tumour Biol. 2014; 35:3405–8.
54. Jiang S, Liu Y, Wang L, Duan C, Liu M. A meta-analysis and systematic review: adjuvant interferon therapy for patients with viral hepatitis-related hepatocellular carcinoma. World J Surg Oncol. 2013; 11:240.
55. Kong QF, Jiao JB, Chen QQ, Li L, Wang DG, Lv B. Comparative effectiveness of radiofrequency ablation with or without transarterial chemoembolization for hepatocellular carcinoma. Tumour Biol. 2014; 35:2655–9.
56. Lan X, Liu HM, Zeng W, Gu HG, Yang JT, Xie B, Tang C, Chen P. Effects of lamivudine on outcome after initial treatment for hepatocellular carcinoma: A meta-analysis. Journal of Gastroenterology and Hepatology (Hong Kong). 2013; 2:924–8.
57. Leng JJ, Xu YZ, Dong JH. Efficacy of transarterial chemoembolization for hepatocellular carcinoma with portal vein thrombosis: a meta-analysis. ANZ J Surg. 2014.
58. Li CZ, Liu JY, Zhang ZM. Adjuvant interferon therapy for hepatocellular carcinoma after curative treatment: A meta-analysis of randomized controlled trials. Chinese Journal of Cancer Prevention and Treatment. 2013; 20:1030–5.
59. Li HY, Wei YG, Yan LN, Li B. Salvage liver transplantation in the treatment of hepatocellular carcinoma: a meta-analysis. World J Gastroenterol. 2012; 18:2415–22.
60. Li JD, Tian YH, Kanduri HK, Li QL, Li DX, Li Q. Prognosis in patients with small hepatocellular carcinoma: A meta-analysis. Hepato-Gastroenterology. 2011; 58:1708–12.
61. Li L, Zhang J, Liu X, Li X, Jiao B, Kang T. Clinical outcomes of radiofrequency ablation and surgical resection for small hepatocellular carcinoma: a meta-analysis. J Gastroenterol Hepatol. 2012; 27:51–8.
62. Li N, Wu YR, Wu B, Lu MQ. Surgical and oncologic outcomes following laparoscopic versus open liver resection for hepatocellular carcinoma: A meta-analysis. Hepatol Res. 2012; 42:51–9.
63. Li X, Dai D, Song X, Liu J, Zhu L, Xu W. A meta-analysis of cytokine-induced killer cells therapy in combination with minimally invasive treatment for hepatocellular carcinoma. Clin Res Hepatol Gastroenterol. 2014.
64. Li Z, Mi D, Yang K, Cao N, Tian J, Ma B. TACE combined with thermotherapy for primary hepatic carcinoma: A meta-analysis. Chinese Journal of Evidence-Based Medicine. 2012; 12:672–8.
65. Li Z, Mi DH, Yang KH, Cao N, Tian JH, Ma B, Liu YL. Effectiveness and safety of TACE combined with AHCS for primary hepatic carcinomas: A systematic review. Chinese Journal of Evidence-Based Medicine. 2013; 13:31–8.
66. Liang W, Wang D, Ling X, Kao AA, Kong Y, Shang Y, Guo Z, He X. Sirolimus-based immunosuppression in liver transplantation for hepatocellular carcinoma: a meta-analysis. Liver Transpl. 2012; 18:62–9.
67. Liang W, Wu L, Ling X, Schroder PM, Ju W, Wang D, Shang Y, Kong Y, Guo Z, He X. Living donor liver transplantation versus deceased donor liver transplantation for hepatocellular carcinoma: a meta-analysis. Liver Transpl. 2012; 18:1226–36.
68. Liao M, Huang J, Zhang T, Wu H. Transarterial chemoembolization in combination with local therapies for hepatocellular carcinoma: a meta-analysis. PLoS One. 2013; 8:e68453.
69. Liu JG, Wang YJ, Du Z. Radiofrequency ablation in the treatment of small hepatocellular carcinoma: a meta analysis. World J Gastroenterol. 2010; 16:3450–6.
70. Liu L, Chen H, Wang M, Zhao Y, Cai G, Qi X, Han G. Combination therapy of sorafenib and TACE for unresectable HCC: a systematic review and meta-analysis. PLoS One. 2014; 9:e91124.
71. Liu Z, Gao F, Yang G, Singh S, Lu M, Zhang T, Zhong Z, Zhang F, Tang R. Combination of radiofrequency ablation with transarterial chemoembolization for hepatocellular carcinoma: an up-to-date meta-analysis. Tumour Biol. 2014; 35:7407–13.
72. Liu Z, Zhou Y, Zhang P, Qin H. Meta-analysis of the therapeutic effect of hepatectomy versus radiofrequency ablation for the treatment of hepatocellular carcinoma. Surg Laparosc Endosc Percutan Tech. 2010; 20:130–40.
73. Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology. 2003; 37:429–42.
74. Lu Z, Wen F, Guo Q, Liang H, Mao X, Sun H. Radiofrequency ablation plus chemoembolization versus radiofrequency ablation alone for hepatocellular carcinoma: a meta-analysis of randomized-controlled trials. Eur J Gastroenterol Hepatol. 2013; 25:187–94.
75. Ma L, Zhong JH, Li LQ. Postoperative adjuvant adoptive immunotherapy for hepatocellular carcinoma: A Meta-analysis. Chinese Journal of Cancer Prevention and Treatment. 2011; 18:1551–5.
76. Ma Y, Xu YC, Tang L, Zhang Z, Wang J, Wang HX. Cytokine-induced killer (CIK) cell therapy for patients with hepatocellular carcinoma: efficacy and safety. Experimental Hematology and Oncology. 2012; 1:11. doi: 10.1186/2162-3619-1-11.
77. Marelli L, Stigliano R, Triantos C, Senzolo M, Cholongitas E, Davies N, Tibballs J, Meyer T, Patch DW, Burroughs AK. Transarterial therapy for hepatocellular carcinoma: which technique is more effective? A systematic review of cohort and randomized studies. Cardiovasc Intervent Radiol. 2007; 30:6–25.
78. Mathurin P, Raynard B, Dharancy S, Kirzin S, Fallik D, Pruvot FR, Roumilhac D, Canva V, Paris JC, Chaput JC, Naveau S. Meta-analysis: evaluation of adjuvant therapy after curative liver resection for hepatocellular carcinoma. Aliment Pharmacol Ther. 2003; 17:1247–61.
79. Meng MB, Cui YL, Guan YS, Ying Z, Zheng MH, Yuan CK, Zhang RM. Traditional Chinese medicine plus transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma. J Altern Complement Med. 2008; 14:1027–42.
80. Meng MB, Cui YL, Lu Y, She B, Chen Y, Guan YS, Zhang RM. Transcatheter arterial chemoembolization in combination with radiotherapy for unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Radiother Oncol. 2009; 92:184–94.
81. Meng MB, Wen QL, Cui YL, She B, Zhang RM. Meta-analysis: traditional Chinese medicine for improving immune response in patients with unresectable hepatocellular carcinoma after transcatheter arterial chemoembolization. Explore (NY). 2011; 7:37–43.
82. Meng W, Li Y, Li X, Zhou W, Zhu X, He W, Liu Y. Can vitamin K2 be applied to prevent the recurrence of hepatocellular carcinoma solely? Hepatology International. 2011; 5:421–2.
83. Menon KV, Hakeem AR, Heaton ND. Meta-analysis: recurrence and survival following the use of sirolimus in liver transplantation for hepatocellular carcinoma. Aliment Pharmacol Ther. 2013; 37:411–9.
84. Miao RY, Zhao HT, Yang HY, Mao YL, Lu X, Zhao Y, Liu CN, Zhong SX, Sang XT, Huang JF. Postoperative adjuvant antiviral therapy for hepatitis B/C virus-related hepatocellular carcinoma: a meta-analysis. World J Gastroenterol. 2010; 16:2931–42.
85. Miyake Y, Takaki A, Iwasaki Y, Yamamoto K. Meta-analysis: interferon-alpha prevents the recurrence after curative treatment of hepatitis C virus-related hepatocellular carcinoma. J Viral Hepat. 2010; 17:287–92.
86. Moriguchi H, Uemura T, Sato C, Raymond C. Tumor ablation plus interferon therapy can reduce the risk of death for patients with hepatitis B virus or hepatitis C virus-related resectable hepatocellular carcinoma - a meta-analysis of randomized controlled trials. Hepatology; 2006; 611a.
87. Ni JY, Liu SS, Xu LF, Sun HL, Chen YT. Meta-analysis of radiofrequency ablation in combination with transarterial chemoembolization for hepatocellular carcinoma. World J Gastroenterol. 2013; 19:3872–82.
88. Ni JY, Liu SS, Xu LF, Sun HL, Chen YT. Transarterial chemoembolization combined with percutaneous radiofrequency ablation versus TACE and PRFA monotherapy in the treatment for hepatocellular carcinoma: a meta-analysis. J Cancer Res Clin Oncol. 2013; 139:653–9.
89. Ni JY, Xu LF, Sun HL, Zhou JX, Chen YT, Luo JH. Percutaneous ablation therapy versus surgical resection in the treatment for early-stage hepatocellular carcinoma: a meta-analysis of 21,494 patients. J Cancer Res Clin Oncol. 2013; 139:2021–33.
90. Nowak A, Findlay M, Culjak G, Stockler M. Tamoxifen for hepatocellular carcinoma. Cochrane Database Syst Rev. 2004; CD001024.
91. Oliveri RS, Wetterslev J, Gluud C. Transarterial (chemo)embolisation for unresectable hepatocellular carcinoma. Cochrane Database Syst Rev. 2011; CD004787.
92. Ono T, Yamanoi A, Nazmy El Assal O, Kohno H, Nagasue N. Adjuvant chemotherapy after resection of hepatocellular carcinoma causes deterioration of long-term prognosis in cirrhotic patients: metaanalysis of three randomized controlled trials. Cancer. 2001; 91:2378–85.
93. Orlando A, Leandro G, Olivo M, Andriulli A, Cottone M. Radiofrequency thermal ablation vs. percutaneous ethanol injection for small hepatocellular carcinoma in cirrhosis: meta-analysis of randomized controlled trials. Am J Gastroenterol. 2009; 104:514–24.
94. Pang SJ, Xu J, Dong ZY. Laparoscopic hepatectomy compared with conventional open hepatectomy for hepatocellular carcinoma: A systematic review. Chinese Journal of Evidence-Based Medicine. 2010; 10:40–6.
95. Parks KR, Kuo YH, Davis JM, B OB, Hagopian EJ. Laparoscopic versus open liver resection: a meta-analysis of long-term outcome. HPB (Oxford). 2014; 16:109–18.
96. Proneth A, Zeman F, Schlitt HJ, Schnitzbauer AA. Is resection or transplantation the ideal treatment in patients with hepatocellular carcinoma in cirrhosis if both are possible? A systematic review and metaanalysis. Annals of Surgical Oncology. 2014; 21:3096–107.
97. Qi X, Tang Y, An D, Bai M, Shi X, Wang J, Han G, Fan D. Radiofrequency ablation versus hepatic resection for small hepatocellular carcinoma: a meta-analysis of randomized controlled trials. J Clin Gastroenterol. 2014; 48:450–7.
98. Rahman A, Assifi MM, Pedroso FE, Maley WR, Sola JE, Lavu H, Winter JM, Yeo CJ, Koniaris LG. Is resection equivalent to transplantation for early cirrhotic patients with hepatocellular carcinoma? A meta-analysis. J Gastrointest Surg. 2012; 16:1897–909.
99. Riaz IB, Riaz H, Riaz T, Rahman S, Amir M, Badshah MB, Kazi AN. Role of vitamin K2 in preventing the recurrence of hepatocellular carcinoma after curative treatment: a meta-analysis of randomized controlled trials. BMC Gastroenterol. 2012; 12:170.
100. Schoppmeyer K, Weis S, Mossner J, Fleig WE. Percutaneous ethanol injection or percutaneous acetic acid injection for early hepatocellular carcinoma. Cochrane Database Syst Rev. 2009; CD006745.
101. Shen A, Tang C, Wang Y, Chen Y, Yan X, Zhang C, Liu R, Wei X, Zhu Y, Zhang H, Wu Z. A systematic review of sorafenib in Child-Pugh A patients with unresectable hepatocellular carcinoma. J Clin Gastroenterol. 2013; 47:871–80.
102. Shen A, Zhang H, Tang C, Chen Y, Wang Y, Zhang C, Wu Z. Systematic review of radiofrequency ablation versus percutaneous ethanol injection for small hepatocellular carcinoma up to 3 cm. J Gastroenterol Hepatol. 2013; 28:793–800.
103. Shen YC, Hsu C, Chen LT, Cheng CC, Hu FC, Cheng AL. Adjuvant interferon therapy after curative therapy for hepatocellular carcinoma (HCC): a meta-regression approach. J Hepatol. 2010; 52:889–94.
104. Shu X, McCulloch M, Xiao H, Broffman M, Gao J. Chinese herbal medicine and chemotherapy in the treatment of hepatocellular carcinoma: a meta-analysis of randomized controlled trials. Integr Cancer Ther. 2005; 4:219–29.
105. Singal AK, Freeman DH, Jr., Anand BS. Meta-analysis: interferon improves outcomes following ablation or resection of hepatocellular carcinoma. Aliment Pharmacol Ther. 2010; 32:851–8.
106. Sun B, Zheng CS, Feng GS, Wang Y, Xia XW, Kan XF. Radiofrequency ablation versus surgical resection for small hepatocellular carcinoma: A meta-analysis. World Chinese Journal of Digestology. 2011; 19:3255–63.
107. Sun P, Dong X, Cheng X, Hu Q, Zheng Q. Nucleot(s)ide analogues for hepatitis B virus-related hepatocellular carcinoma after curative treatment: a systematic review and meta-analysis. PLoS One. 2014; 9:e102761.
108. Sun Q, Ma W, Gao Y, Zheng W, Zhang B, Peng Y. Meta-analysis: therapeutic effect of transcatheter arterial chemoembolization combined with compound kushen injection in hepatocellular carcinoma. Afr J Tradit Complement Altern Med. 2012; 9:178–88.
109. Tang YH, Wen TF, Chen X. Resection margin in hepatectomy for hepatocellular carcinoma: a systematic review. Hepatogastroenterology. 2012; 59:1393–7.
110. Tang YH, Wen TF, Chen X. Anatomic versus non-anatomic liver resection for hepatocellular carcinoma: a systematic review. Hepatogastroenterology. 2013; 60:2019–25.
111. Twaij A, Pucher PH, Sodergren MH, Gall T, Darzi A, Jiao LR. Laparoscopic vs open approach to resection of hepatocellular carcinoma in patients with known cirrhosis: systematic review and meta-analysis. World J Gastroenterol. 2014; 20:8274–81.
112. Wang J, He XD, Yao N, Liang WJ, Zhang YC. A meta-analysis of adjuvant therapy after potentially curative treatment for hepatocellular carcinoma. Can J Gastroenterol. 2013; 27:351–63.
113. Wang J, He XD, Zhang YC. Antibiotic prophylaxis in transarterial therapy of hepatocellular carcinoma: a meta-analysis. Can J Gastroenterol. 2012; 26:85–91.
114. Wang N, Guan Q, Wang K, Zhu B, Yuan W, Zhao P, Wang X, Zhao Y. TACE combined with PEI versus TACE alone in the treatment of HCC: a meta-analysis. Med Oncol. 2011; 28:1038–43.
115. Wang W, Shi J, Xie WF. Transarterial chemoembolization in combination with percutaneous ablation therapy in unresectable hepatocellular carcinoma: a meta-analysis. Liver Int. 2010; 30:741–9.
116. Wang X, Li J, Peng Y, Dai Y, Xu W. Influence of preoperative transarterial chemoembolization on the prognosis for patients with resectable hepatocellular carcinoma: a meta-analysis of randomized trials. Hepatogastroenterology. 2011; 58:869–74.
117. Wang Y, Luo Q, Li Y, Deng S, Wei S, Li X. Radiofrequency ablation versus hepatic resection for small hepatocellular carcinomas: a meta-analysis of randomized and nonrandomized controlled trials. PLoS One. 2014; 9:e84484.
118. Wang Z, Wu XL, Zeng WZ, Xu GS, Xu H, Weng M, Hou JN, Jiang MD. Meta-analysis of the efficacy of sorafenib for hepatocellular carcinoma. Asian Pac J Cancer Prev. 2013; 14:691–4.
119. Weis S, Franke A, Mossner J, Jakobsen JC, Schoppmeyer K. Radiofrequency (thermal) ablation versus no intervention or other interventions for hepatocellular carcinoma. Cochrane Database Syst Rev. 2013; 12:CD003046.
120. Wong JS, Wong GL, Tsoi KK, Wong VW, Cheung SY, Chong CN, Wong J, Lee KF, Lai PB, Chan HL. Meta-analysis: the efficacy of anti-viral therapy in prevention of recurrence after curative treatment of chronic hepatitis B-related hepatocellular carcinoma. Aliment Pharmacol Ther. 2011; 33:1104–12.
121. Wu P, Dugoua JJ, Eyawo O, Mills EJ. Traditional Chinese Medicines in the treatment of hepatocellular cancers: a systematic review and meta-analysis. J Exp Clin Cancer Res. 2009; 28:112.
122. Wu T, Sun R, Wang Z, Yang W, Shen S, Zhao Z. A meta-analysis of Cinobufacini combined with transcatheterarterial chemoembolization in the treatment of advanced hepatocellular carcinoma. J Cancer Res Ther. 2014; 10:C60–4.
123. Xie F, Zang J, Guo X, Xu F, Shen R, Yan L, Yang J, He J. Comparison of transcatheter arterial chemoembolization and microsphere embolization for treatment of unresectable hepatocellular carcinoma: a meta-analysis. J Cancer Res Clin Oncol. 2012; 138:455–62.
124. Xie F, Zhang X, Li H, Zheng T, Xu F, Shen R, Yan L, Yang J, He J. Adoptive immunotherapy in postoperative hepatocellular carcinoma: a systemic review. PLoS One. 2012; 7:e42879.
125. Xie ZB, Ma L, Wang XB, Bai T, Ye JZ, Zhong JH, Li LQ. Transarterial embolization with or without chemotherapy for advanced hepatocellular carcinoma: a systematic review. Tumour Biol. 2014; 35:8451–9.
126. Xiong JJ, Altaf K, Javed MA, Huang W, Mukherjee R, Mai G, Sutton R, Liu XB, Hu WM. Meta-analysis of laparoscopic vs open liver resection for hepatocellular carcinoma. World J Gastroenterol. 2012; 18:6657–68.
127. Xu G, Qi FZ, Zhang JH, Cheng GF, Cai Y, Miao Y. Meta-analysis of surgical resection and radiofrequency ablation for early hepatocellular carcinoma. World J Surg Oncol. 2012; 10:163.
128. Xu JB, Qi FZ, Xu G, Chen GF, Huang MD, Zhang JH. Adjuvant interferon therapy after surgical treatment for hepatitis B/C virus-related hepatocellular carcinoma: A meta-analysis. Hepatol Res. 2014; 44:209–17.
129. Xu QR, Zheng X, Yao YM, Yang W, Liu QG. Liver transplantation versus resection for treatment of hepatocellular carcinoma: A meta-analysis. Journal of Xi’an Jiaotong University (Medical Sciences). 2012; 33:576–82.
130. Xu RH, Gao W, Wang C, Guo DK, Tang L, Zhang H, Wang CJ. Systematic evaluation of percutaneous radiofrequency ablation versus percutaneous ethanol injection for the treatment of small hepatocellular carcinoma: a meta-analysis. Eur J Med Res. 2014; 19:39.
131. Xu XS, Liu C, Qu K, Song YZ, Zhang P, Zhang YL. Liver transplantation versus liver resection for hepatocellular carcinoma: a meta-analysis. Hepatobiliary Pancreat Dis Int. 2014; 13:234–41.
132. Xue TC, Xie XY, Zhang L, Yin X, Zhang BH, Ren ZG. Transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombus: a meta-analysis. BMC Gastroenterol. 2013; 13:60.
133. Yan S, Xu D, Sun B. Combination of radiofrequency ablation with transarterial chemoembolization for hepatocellular carcinoma: a meta-analysis. Dig Dis Sci. 2012; 57:3026–31.
134. Yang M, Yuan JQ, Bai M, Han GH. Transarterial chemoembolization combined with sorafenib for unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Mol Biol Rep. 2014; 41:6575–82.
135. Yao G, Cao J, Gu H, Zhang Jh, Han AYFHA, Cao XL, Wen H. Laparoscopic hepatectomy versus open hepatectomy for hepatocellular carcinoma: A meta-analysis. Chinese Journal of Evidence-Based Medicine. 2013; 13:588–95.
136. Ye JZ, Miao ZG, Wu FX, Zhao YN, Ye HH, Li LQ. Recurrence after anatomic resection versus nonanatomic resection for hepatocellular carcinoma: a meta-analysis. Asian Pac J Cancer Prev. 2012; 13:1771–7.
137. Yin Z, Fan X, Ye H, Yin D, Wang J. Short- and long-term outcomes after laparoscopic and open hepatectomy for hepatocellular carcinoma: a global systematic review and meta-analysis. Ann Surg Oncol. 2013; 20:1203–15.
138. Yu T, Xu X, Chen B. TACE combined with liver resection versus liver resection alone in the treatment of resectable HCC: A meta-analysis. Chinese-German Journal of Clinical Oncology. 2013; 12:P532-P6.
139. Zhang CH, Xu GL, Jia WD, Ge YS. Effects of interferon alpha treatment on recurrence and survival after complete resection or ablation of hepatocellular carcinoma: a meta-analysis of randomized controlled trials. Int J Cancer. 2009; 124:2982–8.
140. Zhang L, Hu P, Chen X, Bie P. Transarterial chemoembolization (TACE) plus sorafenib versus TACE for intermediate or advanced stage hepatocellular carcinoma: a meta-analysis. PLoS One. 2014; 9:e100305.
141. Zhang T, Ding X, Wei D, Cheng P, Su X, Liu H, Wang D, Gao H. Sorafenib improves the survival of patients with advanced hepatocellular carcinoma: a meta-analysis of randomized trials. Anticancer Drugs. 2010; 21:326–32.
142. Zhang W, Song TQ, Zhang T, Wu Q, Kong DL, Li Q, Sun HC. Adjuvant interferon for early or late recurrence of hepatocellular carcinoma and mortality from hepatocellular carcinoma following curative treatment: A meta-analysis with comparison of different types of hepatitis. Molecular and Clinical Oncology. 2014; 2:1125–34.
143. Zhang X, Yang XR, Huang XW, Wang WM, Shi RY, Xu Y, Wang Z, Qiu SJ, Fan J, Zhou J. Sorafenib in treatment of patients with advanced hepatocellular carcinoma: a systematic review. Hepatobiliary Pancreat Dis Int. 2012; 11:458–66.
144. Zhao S, Chen XC, Long QY, Zhang XL. Transcatheter arterial chemoembolization combined with radiofrequency ablation for the treatment of hepatocellular carcinoma: A systematic review and meta analysis. Journal of Interventional Radiology (China). 2013; 22:908–13.
145. Zhao WY, Luo M, Sun YW, Xu Q, Chen W, Zhao G, Wu ZY. The efficacy of preoperative portal vein embolization for extended hepatectomy: a meta-analysis. [Article in Chinese] Zhonghua Wai Ke Za Zhi. 2008; 46:1460–4.
146. Zheng Z, Liang W, Milgrom DP, Schroder PM, Kong NS, Yang C, Guo Z, He X. Liver transplantation versus liver resection in the treatment of hepatocellular carcinoma: a meta-analysis of observational studies. Transplantation. 2014; 97:227–34.
147. Zheng Z, Liang W, Wang D, Schroder PM, Ju W, Wu L, Shang Y, Guo Z, He X. Adjuvant chemotherapy for patients with primary hepatocellular carcinoma: A meta-analysis. Int J Cancer. 2014.
148. Zhong J, Xiang B, Ma L, Li L. Conventional oral systemic chemotherapy for postoperative hepatocellular carcinoma: A systematic review. Molecular and Clinical Oncology. 2014; 2:1091–6.
149. Zhong JH, Li LQ. Postoperative adjuvant transarterial chemoembolization for participants with hepatocellular carcinoma: A meta-analysis. Hepatol Res. 2010; 40:943–53.
150. Zhong JH, Li LQ, You XM, Xiang BD, Ma L, Gong WF. Oral vitamin K2 analogs for hepatocellular carcinoma after surgery: A meta-analysis. World Chinese Journal of Digestology. 2012; 20:2420–6.
151. Zhou DC, Geng XP, Zhu LX, Zhao HC, Liu FB, Zhao YJ. Percutaneous radiofrequency ablation versus hepatic resection for small hepatocellular carcinoma: a meta analysis. [Article in Chinese] Zhonghua Wai Ke Za Zhi. 2011; 49:1132–6.
152. Zhou Y, Xu D, Wu L, Li B. Meta-analysis of anatomic resection versus nonanatomic resection for hepatocellular carcinoma. Langenbecks Arch Surg. 2011; 396:1109–17.
153. Zhou Y, Zhang X, Wu L, Ye F, Su X, Shi L, Li B. Meta-analysis: preoperative transcatheter arterial chemoembolization does not improve prognosis of patients with resectable hepatocellular carcinoma. BMC Gastroenterol. 2013; 13:51.
154. Zhou Y, Zhang Z, Zhao Y, Wu L, Li B. Antiviral therapy decreases recurrence of hepatitis B virus-related hepatocellular carcinoma after curative resection: a meta-analysis. World J Surg. 2014; 38:2395–402.
155. Zhou Y, Zhang X, Wu L, Ye F, Su X, Shi L, Li B. Meta-analysis of radiofrequency ablation versus hepatic resection for small hepatocellular carcinoma. BMC Gastroenterol. 2010; 10:78.
156. Zhou YM, Shao WY, Zhao YF, Xu DH, Li B. Meta-analysis of laparoscopic versus open resection for hepatocellular carcinoma. Dig Dis Sci. 2011; 56:1937–43.
157. Zhu Y, Dong J, Wang WL, Li MX, Lu Y. Short- and long-term outcomes after salvage liver transplantation versus primary liver transplantation for hepatocellular carcinoma: a meta-analysis. Transplant Proc. 2013; 45:3329–42.
158. Zhuang L, Zeng X, Yang Z, Meng Z. Effect and safety of interferon for hepatocellular carcinoma: a systematic review and meta-analysis. PLoS One. 2013; 8:e61361.
159. Zhuang LP, Zeng XT, Meng ZQ. A systematic review and meta-analysis of randomized controlled trails. [Article in Chinese] Zhonghua Gan Zang Bing Za Zhi. 2012; 20:363–7.
160. Zou LL, Ma L, Tian JH, Yang KH. Sorafenib for advanced hepatocellular carcinoma: A systematic review. Acta Academiae Medicinae Sinicae. 2011; 33:51–7.