
INTRODUCTION
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is commonly perceived as the only curable option for refractory leukemia [1-4]. However, patients with advanced stage who proceed directly to HSCT, especially those with high leukemia burden pre-transplantation, are likely to do poorly [5, 6]. The relapse rate exceeds 50% in these patients with standard myeloablative regimen consisting of total body irradiation (TBI) or busulfan (Bu) combined with cyclophosphamide (CY) [6, 7]. Some data showed that intensified conditioning could reduce leukemia relapse, but it might simultaneously increase non-relapse mortality (NRM) [6, 8, 9]. Therefore, maintaining the balance of efficacy and toxicity of conditioning is essential for long-term survival of recipient [10-12]. Recent studies have demonstrated that salvage chemotherapy with sequential conditioning could reduce leukemia relapse and had an acceptable toxicity for refractory leukemia [11-14].
In addition to conditioning regimens, the efficacy of allo-HSCT also relies on the graft-versus-leukemia (GVL) effect. We previously introduced a strategy of sequential intensified conditioning, consisting of fludarabine (Flu)/cytarabine (Ara-C) salvage chemotherapy followed by TBI/CY/etoposide (VP-16) myeloablative conditioning, and early rapid tapering of immunosuppressant for inducing GVL in refractory advanced leukemia undergoing allo-HSCT [15]. The results indicated that this strategy had an acceptable toxicity profile and improved outcome for refractory leukemia, with 5-year overall survival (OS) and disease-free survival (DFS) of 44.6% and 38.2% [15]. Despite these encouraging results, relapse in our cohort was still considerable, with 3-year relapse rate of 33.3% [15]. Based on these, in this study, we modified our historical strategy mainly by interventions with prophylactic donor lymphocyte infusion (DLI) for inducing GVL. The aim of this study was to evaluate whether this new strategy could reduce leukemia relapse and not increase NRM in refractory advanced acute leukemia.
RESULTS
Patient and transplant characteristics
Patient and transplant characteristics are summarized in Table 1. From January 2009 to June 2014, 153 patients with refractory advanced acute leukemia undergoing allo-HSCT were enrolled in the study group. Except for two who died of infections and two who died of regimen-related toxicities (RRTs) within 2 weeks post-transplantation, 149 patients surviving more than 30 days were evaluable for engraftment, disease response and Cyclosporine A (CsA) withdrawal.
Table 1: Patient, donor and transplant characteristics
Patient characteristics |
Study group (n=153) |
Historical group (n=48) |
P-value |
|---|---|---|---|
Female/Male |
51(33.3%)/102(66.7%) |
17(35.4%)/31(64.6%) |
P=0.790 |
Median age, years (range) |
29(12-57) |
29(14-53) |
P=0.837 |
Disease category |
|||
AML |
57(37.3%) |
23(47.9%) |
P=0.112 |
ALL |
77(50.3%) |
16(33.3%) |
|
ABL |
19(12.4%) |
9(18.8%) |
|
Genetics a |
|||
Favorable |
3(2.0%) |
4(8.3%) |
*P=0.003 |
Intermediate |
57(37.3%) |
18(37.5%) |
|
Unfavorable |
84(54.9%) |
17(35.4%) |
|
Unknown |
9(5.9%) |
9(18.8%) |
|
Stage of treatment before transplantation |
P=0.058 |
||
Primary induction failure |
85(55.6%) |
27(56.25%) |
|
Refractory relapse after CR1 |
46(30.1%) |
15(31.25%) |
|
Refractory relapse after CR2 |
21(13.7%) |
3(6.25%) |
|
Previous autologous transplantation |
1(0.7%) |
3(6.25%) |
|
Median BM blasts before conditioning (range) |
30.0% (9.0%-96.0%) |
24.0% (8.0%-92.0%) |
P=0.436 |
Median circulating blasts before conditioning (range) |
11.0% (0.0%-90.0%) |
11.0% (0.0%-82.0%) |
P=0.699 |
Median number of chemotherapy cycles before transplantation (range) |
4 (2-8) |
5 (2-13) |
P=0.710 |
Extramedullary disease at the time of transplantation |
16 (10.5%) |
6 (12.5%) |
P=0.693 |
CNSL |
8 (5.2%) |
2 (4.2%) |
|
Soft tissue and lymph node involvement |
8 (5.2%) |
4 (8.3%) |
|
Donor source |
|||
Sibling donor |
84(54.9%) |
27(56.3%) |
*P=0.018 |
Family donor |
41(26.8%) |
5(10.4%) |
|
Unrelated donor |
28(18.3%) |
16(33.3%) |
|
HLA typing |
|||
HLA-identical |
87(56.9%) |
32(66.7%) |
*P=0.003 |
One allele mismatched |
12(7.8%) |
8(16.65%) |
|
Two alleles mismatched |
14(9.2%) |
8(16.65%) |
|
Three alleles mismatched |
12(7.8%) |
0(0.0%) |
|
Four alleles mismatched |
9(5.9%) |
0(0.0%) |
|
Five alleles mismatched |
19(12.4%) |
0(0.0%) |
|
Stem cell source |
|||
PBSCs |
97(63.4%) |
33(68.75%) |
*P<0.001 |
BM |
0(0.0%) |
8(16.65%) |
|
PBSCs + BM |
56(36.6%) |
7(14.6%) |
|
Median CD34+ cells per graft, ×106/kg (range) |
9.1(5.4-12.7) |
8.3(4.0-21.4) |
P=0.681 |
AML=acute myelogenous leukemia; ALL=acute lymphoblastic leukemia; ABL= acute biphenotypic leukemia; CR1=first complete remission; CR2=second complete remission; BM=bone marrow; CNSL= central nervous system leukemia; PBSCs= peripheral blood stem cells; BM=bone marrow. agenetics in the study group indicated cytogenetics and molecular genetics; genetics in the historical group only indicated cytogenetics. * P<0.05.
Within the study population, 21 had comorbidities; 6 had hypertension, 3 had frequent ventricular premature beats, 8 had diabetes mellitus, and 4 had hypertension and diabetes mellitus. Two had a history of pulmonary tuberculosis, and 43 had a history of invasive fungal disease (IFD) pre-transplantation, including 19 with active Aspergillus pneumonia at the time of transplantation.
Engraftment and disease response
All patients achieved hematopoietic reconstitution except for two who died of infections and two who died of RRTs within 2 weeks post-transplantation. The median time to neutrophil and platelet reconstitution were 12.0 (range, 9.0 to 31.0) days and 19.0 (range, 9.0 to 70.0) days, respectively. At the time of neutrophil reconstitution, 149 evaluable patients all achieved donor chimerism, including 61 with complete chimerism and 88 with mixed chimerism (with donor chimerism ranging from 67.0% to 95.0%). All 149 evaluable patients had complete chimerism by day +30 post-transplantation. At the time of neutrophil reconstitution, all 149 evaluable patients achieved complete remission (CR).
RRTs
The conditioning was tolerated by all patients except two who died of RRTs. All 153 patients developed RRTs, and 44 grade III-IV RRTs. The incidence and mortality of RRTs were 100.0% and 1.3%. Toxicity was most common in the gastrointestinal tract. Organ toxicity is summarized in Table 2.
Table 2: Organ toxicity according to Bearman’s criteria
Grade I-II RRTs, n (%) |
Grade III-IV RRTs, n (%) |
Overall RRTs, n (%) |
|
|---|---|---|---|
Heart |
43(28.1) |
9(5.9) |
52(34.0) |
Bladder |
23(15.0) |
16(10.5) |
39(25.5) |
Kidneys |
11(7.2) |
3(2.0) |
14(9.2) |
Lungs |
4(2.6) |
1(0.7) |
5(3.3) |
Liver |
26(17.0) |
10(6.5) |
36(23.5) |
CNS |
9(5.9) |
1(0.7) |
10(6.5) |
Mucosa |
67(43.8) |
23(15.0) |
90(58.8) |
Gut |
104(68.0) |
25(16.3) |
129(84.3) |
RRTs= regimen-related toxicities, CNS=central nervous system.
Infections
Within the first 100 days post-transplantation, 85 patients developed 101 episodes of infections, including 33 bacteria, 12 fungi, 15 viruses (excluding viremia), 16 mixed infections (10 bacteria and fungi; 6 bacteria and viruses) and 9 infections of unknown etiology. Seven patients died of infections within the first 100 days post-transplantation. Active Aspergillus pneumonia was effectively controlled post-transplantation in the 19 patients with active IFD pre-transplantation. Compared with 257 acute leukemia undergoing allo-HSCT with standard myeloablative conditioning (TBI+CY, Bu+CY or Bu+Flu) at Nanfang Hospital at the same time, the incidence and mortality of infectious diseases within 100 days post-transplantation were similar between the two groups (P=0.296, P=0.730).
The 1-year cumulative incidences of cytomegalovirus (CMV)-emia, CMV-associated diseases, Epstein-Barr virus (EBV)-emia and EBV-associated diseases were 40.5%±4.1%, 4.2%±2.1%, 36.4%±5.5% and 18.7%±4.1%, respectively. The 1-year cumulative mortalities of CMV-associated diseases and EBV-associated diseases were 2.7%±1.9% and 5.9%±2.5%, respectively. Compared with 257 acute leukemia undergoing allo-HSCT with standard conditioning at Nanfang Hospital at the same time, the incidence of EBV-emia was higher in the study group (P=0.037), and the incidences of EBV-associated diseases, CMV-emia and CMV-associated diseases were similar between the two groups (P=0.317, P=0.802, P=0.534).
CsA withdrawal and DLI
Of the 149 evaluable patients, 115 fulfilled the above criteria for CsA withdrawal from day +30. Of the 144 patients surviving day +60, 80 fulfilled the above criteria for prophylactic DLI (76 from day +60 and 4 from day +90), and 64 did not receive DLI. Twenty-one did not receive DLI due to the unavailability of donor lymphocytes. Other 43 with acute graft-versus-host disease (aGVHD) by day +30 or grade II/>II aGVHD by day +60 post-transplantation did not receive DLI, as a result of negative minimal residual disease (MRD) by day +90 (n=34), GVHD by day +90 (n=5) and death before day +90 (n=4).
GVHD
Of the 149 evaluable patients, 34 developed grade I-IV aGVHD (grade I, n=8; grade II, n=14; grade III, n=8; grade IV, n=4) by day +30 post-transplantation and 2 died of aGVHD. Of the 115 patients withdrawing CsA, 34 developed aGVHD (grade I, n=16; grade II, n=13; grade III, n=5) by day +60 post-transplantation and one died from aGVHD. A total of 129 doses of DLI were administered in 80 patients, with a median of 2 (range, 1-4) doses per patient and a median dosage of 2.06 (range: 0.67-5.62) ×107 CD3+ T cells/kg. Twenty-five developed (grade I, n=3; grade II, n=18; grade III, n=4) aGVHD, 52 developed chronic GVHD (cGVHD), and 1 died of aGVHD after DLI.
Overall, 89 patients developed aGVHD, and 77 of 138 surviving more than 100 days developed cGVHD. The 1-year cumulative incidences of overall and grade III-IV aGVHD were 62.1%±4.1% and 14.4%±2.9%, including aGVHD after DLI (overall: 31.6%±5.7%, grade III-IV: 3.9%±2.2%). The 2-year cumulative incidences of overall and extensive cGVHD were 61.4%±4.5% and 21.1%±3.7%. The 5-year mortality of GVHD was 14.1%±6.1%.
Relapse
Thirty-two patients experienced leukemia relapse at a median time of 191 (range, 61 to 1079) days post-transplantation. Nine abandoned treatment and 23 received treatment, including 15 with chemotherapy and DLI, 5 with chemotherapy alone and 3 with chemotherapy and radiotherapy. Six achieved CR after treatment, and the others all died of disease progress or treatment-related complications. The 1-, 3- and 5-year cumulative incidence of leukemia relapse were 20.6%±3.5%, 27.3%±4.4% and 27.3%±4.4%. Fifteen of the 80 (18.8%) patients receiving DLI relapsed at a median time of 271 (range, 94 to 1079) days post-transplantation, and 17 of the 64 (26.6%) patients not receiving DLI relapsed at a median time of 165 (range, 61 to 611) days post-transplantation. The 5-year cumulative incidence of relapse in patients receiving DLI was 22.7%±5.5%, compared with 33.9%±7.2% in those not receiving DLI (P=0.048, Figure 1A). Univariate and multivariate analyses both revealed that DLI, cGVHD and lower bone marrow (BM) blasts on day 0 were associated with lower relapse (Table 3).
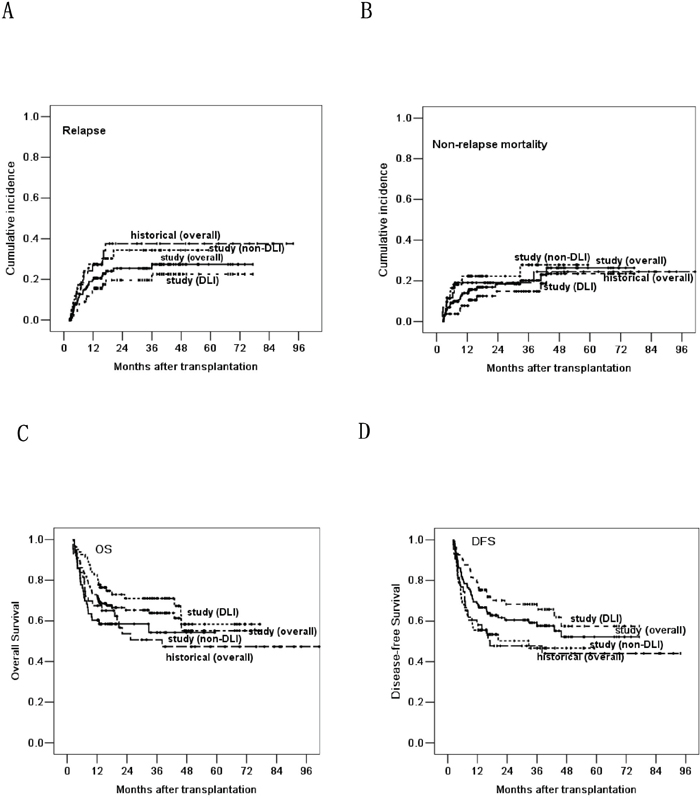
Figure 1: Based on the landmark analysis at 60 days, comparing the relapse rate A., non-relapse mortality B., overall survival C. and disease-free survival D. post-transplantation in the three groups of historical control, DLI and non-DLI.
Table 3: Risk factors for leukemia relapse, OS and DFS
Risk factors |
Relapse |
OS |
DFS |
|||
|---|---|---|---|---|---|---|
Univariate |
Multivariate (HR) |
Univariate |
Multivariate (HR) |
Univariate |
Multivariate (HR) |
|
male vs female |
NS |
NS |
NS |
NS |
NS |
NS |
Age, < 29vs ≥ 29 years (median) |
NS |
NS |
NS |
NS |
NS |
NS |
Disease category, AML/ALL/ABL |
NS |
NS |
NS |
NS |
NS |
NS |
Genetic status, unfavorable vs other |
NS |
NS |
NS |
NS |
NS |
NS |
Stage of treatment before HSCT, PIF vs other |
NS |
NS |
NS |
NS |
NS |
NS |
Number of chemotherapy cycles pre-HSCT, < 4 vs ≥4 (median) |
NS |
NS |
NS |
NS |
NS |
NS |
BM blasts before conditioning, <30.0% vs ≥30.0% (median) |
NS |
NS |
NS |
NS |
NS |
NS |
Circulating blasts before conditioning, <11.0% vs ≥11.0% (median) |
NS |
NS |
NS |
NS |
NS |
NS |
BM blasts on day 0, < 3.3% vs ≥3.3% (median) |
P=0.001 |
P<0.001 (1.329) |
P=0.008 |
P<0.001(1.236) |
P=0.003 |
P<0.001(1.239) |
Circulating blasts on day 0, none vs present |
NS |
NS |
NS |
NS |
NS |
NS |
CD34+ counts in the graft, less than vs greater than or equal to median |
NS |
NS |
NS |
NS |
NS |
NS |
Donor source, related vs unrelated donor |
NS |
NS |
NS |
NS |
NS |
NS |
HLA typing, matched vs mismatched |
NS |
NS |
NS |
NS |
NS |
NS |
No aGVHD vs I-II aGVHD vs III – IV aGVHD |
NS |
NS |
NS |
NS |
NS |
NS |
No cGVHD vs limited cGVHD vs extensive cGVHD |
P=0.026 |
P=0.036(0.474) |
P=0.033 |
P=0.028 (0.573) |
P=0.037 |
P=0.011(0.482) |
No early CsA withdrawal vs early CsA withdrawal |
NS |
NS |
NS |
NS |
NS |
NS |
No DLI vs DLI |
P=0.033 |
P=0.048(0.495) |
P=0.044 |
P=0.046 (0.623) |
P=0.045 |
P=0.015(0.595) |
OS=overall survival; DFS=disease-free survival;HR= hazard risk; vs=versus; AML= acute myelocytic leukemia; ALL= acute lymphoblastic leukemia; ABL= acute biphenotypic leukemia; HSCT= hematopoietic stem cell transplantation; PIF=primary induction failure; BM=bone marrow; HLA= human leukocyte antigen; aGVHD=acute graft-versus-host disease; cGVHD=chronic graft-versus-host disease; CsA=cyclosporine A; DLI= donor lymphocyte infusion; NS= not significant;CI=confidence interval.
OS and DFS
With a median follow up of 421 (range, 0 to 2319) days post-transplantation, 92 patients survived and 61 died. Causes of death included leukemia relapse (n=26), infections (n=19, including 5 EBV-associated diseases), GVHD (n=9), diffuse alveolar hemorrhage (n=2), RRTs (n=2), cerebral hemorrhage (n=1), thrombotic microangiopathy (n=1) and secondary dyshematopoiesis (n=1). The 5-year NRM post-transplantation was 29.7%±5.3%, and it was similar between DLI and non-DLI groups (P=0.104, Figure 1B). The 5-year OS and DFS were 51.1%±5.7% and 49.2%±5.3%. The 5-year OS and DFS in patients receiving DLI were 58.1%±8.0% and 57.2%±7.5%, compared with 54.9%±7.0% and 47.3%±7.1% in those not receiving DLI (P=0.043, P=0.018, Figure 1C and 1D). Univariate and multivariate analyses both demonstrated that DLI and cGVHD were the protective factors for longer OS and DFS; higher BM blasts on day 0 was the only risk factor for longer OS and DFS (Table 3).
Comparison with historical group
To maintain consistency of primary disease category and minimum follow-up (12 months) between the study and historical groups, we removed 6 patients with chronic myelogenous leukemia with blast crisis (CML-BC) from historical data, and re-analyzed historical data on December 31, 2009 [15]. A total of 48 refractory acute leukemia undergoing allo-HSCT but not receiving DLI from May 2001 to December 2008 were enrolled in the historical group (patient’s characteristics as shown in Table 1). Except for one who died of infection and one who died of RRT on day +3 post-transplantation, 46 patients surviving more than 30 days were evaluable for engraftment, disease response and CsA withdrawal. Fourteen of the 48 (29.2%) patients experienced leukemia relapse at a median time of 209 (range, 35 to 511) days post-transplantation in the historical group. Two achieved CR after treatment, and the others all died of disease progress or treatment-related complications. With a median follow up of 566 (range, 3 to 3034) days post-transplantation, 21 patients survived and 27 died in the historical group. Causes of death included leukemia relapse (n=12), infections (n=6, including 1 EBV-associated diseases), GVHD (n=7), RRT (n=1) and second tumor (lung cancer, n=1).
To further evaluate the efficacy of DLI, we compared the outcomes of patients in the study group with our historical group. Based on the landmark analysis at 60 days, the outcome of patients receiving DLI in the study group was significantly improved in relapse rate, OS and DFS, when compared with the historical group (36.5%±8.4%, 47.3%±8.2% and 44.1%±8.0%) (P=0.045, P=0.031 and P=0.025, Figure 1). The relapse rate, OS and DFS were similar between historical and non-DLI groups (P=0.918, P=0.689 and P=0.877). The NRM was similar in the historical, DLI and non-DLI groups (P=0.261).
DISCUSSION
For refractory leukemia undergoing allo-HSCT, the major obstacle is leukemia relapse [16, 17]. Reports in the literature indicate that the 5-year OS, DFS and relapse rate are estimated to range from 7% to 30%, 5% to 30%, and 44% to 63% in refractory leukemia post-transplantation [2, 17-19]. The intensity of the conditioning regimen has been shown to directly affect the relapse rate and DFS after allo-HSCT for refractory leukemia [20, 21]. Reduced-intensity conditioning (RIC) regimens have been advocated to reduce transplantation-associated toxicity in elderly or medically unfit patients; however, disappointing results have been reported with RIC transplantation in refractory leukemia [21, 22]. Intensified conditioning can reduce leukemia burden pre-transplantation and improve long-term survival for refractory leukemia [15, 20, 23]. The Flu/Ara-C regimen for salvage chemotherapy in refractory leukemia has a reported 40% to 50% probability of achieving CR [24, 25]. Based on these results, we used Flu/Ara-C regimen as salvage chemotherapy followed by a myeloablative regimen. In myeloablative regimen, TBI/CY regimen showed lower relapse and higher DFS than Bu/CY regimen for refractory acute leukemia [7, 26]. On account of the chemoresistance of drugs which patients with refractory acute leukemia were medicated with in previous treatment, VP-16 was applied less frequently and the possibility of resistance was comparatively lower. Therefore, we chose TBI/CY/VP16 as myeloablative regimen for refractory acute leukemia undergoing allo-HSCT. Our result showed that all 149 evaluable patients achieved CR at the time of neutrophil reconstitution, which confirmed the suitability of using Flu/Ara-C with TBI/CY/VP16 myeloablative regimen in refractory leukemia to decrease leukemia burden pre-transplantation and increase the CR rate post-transplantation. Meanwhile, it further verified our historical result that sequential intensified conditioning had an acceptable toxicity profile [15].
Immunosupressant withdrawal and DLI are generally used to induce GVL for refractory leukemia after allo-HSCT [27-30]. Our historical study adopted early rapid tapering of immunosuppressant to induce GVL, with 3-year relapse rate of 33.3% [15]. In this study, to enhance the GVL effect, DLI was conducted on the basis of early immunosuppressant withdrawal, reducing the relapse rate to 27.3%. Prophylactic DLI showed less relapse than no DLI. Multivariate analysis also revealed that DLI was the favorable factor for reducing relapse. These data suggested that interventions with prophylactic DLI post-transplantation could reduce relapse.
The two methods both face the risk of GVHD, especially in the early period post-transplantation. In our historical study, CsA was withdrawn by 20%/week in patients without aGVHD by day +30 post-transplantation, and the incidence of grade III-IV aGVHD was 11.5% [15]. In this study, to avoid an overwhelming GVHD, CsA was withdrawn by 10%/week in patients without aGVHD by day +30, and granulocyte colony-stimulating factor (G-CSF)-mobilized DLI was administrated in patients without grade II/>II aGVHD by day +60 or in those without GVHD but MRD positive by day +90. The results showed that the incidences of grade III-IV aGVHD after CsA withdrawal and DLI were 4.3% and 5.0%. The non-increased incidence of GVHD might be due to the following two reasons: the percentage of CSA withdrawal reduced from 20% per week in historical group to 10% in the study group; G-CSF-mobilized DLI had a comparative GVL effect but a lower morbidity and mortality of GVHD compared with steady DLI [29-31].
Intensified conditioning regimens might increase NRM, including RRTs and early infections [6, 9]. In this study, the mortality of RRTs was 1.3%, which had no significant difference compared with standard myeloablative conditioning [7, 32]. The incidence of infections in our cohort was similar to that in patients undergoing allo-HSCT with standard conditioning in a corresponding time period within 100 days post-transplantation, and was also similar to that reported in other literatures [33, 34]. Nonetheless, the 5-year NRM and mortality of GVHD post-transplantation were 29.7% and 14.1%. Therefore, decreasing NRM, especially the lethality of GVHD, is a worthy goal that merits further research.
Schmid and coworkers reported a very promising study that improved survival for refractory AML through a sequential regimen of Flu/Ara-c/amsacrine chemotherapy and reduced-intensity conditioning, along with immunosupressant withdrawal and prophylactic DLI, with 2-year OS and leukemia mortality of 40.0% and 39.3% [12]. In this study, we adopted the strategy of Flu/Ara-C salvage chemotherapy and TBI/CY/VP-16 myeloablative conditioning followed by early rapid tapering of immunosuppressant and prophylactic DLI, with 5-year OS and relapse rate of 51.1% and 27.3%. The favorable efficacy might be attributed to the two aspects: salvage chemotherapy and myeloablative conditioning decreased the leukemia burden at the time of transplantation; early tapering of immunosuppressant combined with DLI accelerated the GVL effect. Our strategy for refractory acute leukemia undergoing allo-HSCT was similar to that described by Schmid. Salvage chemotherapy was performed pre-conditioning, and the strategies of GVL induction, including immunosupressant withdrawal combined with prophylactic DLI, were conducted post-transplantation in the two strategies. However, our results were likely to be superior to theirs with respect to survival and relapse [12]. Along with the heterogeneity of patients included in our cohort, our protocol differed from theirs in terms of drugs used in conditioning, the interval between salvage chemotherapy and conditioning, intervention time for immunosupressant withdrawal and DLI, and other aspects. These might be the reasons why our result was superior. At the same time, there are some limitations of the study. For example, treatment modalities and doctor experience changed through years (historical group: from year 2001 to 2008; study group: from year 2009 to 2014). Since it is not a randomized study, patient selection bias and imbalanced features between groups could not be avoided. Well-designed prospective clinical trials are needed to establish better treatments for refractory acute leukemia.
In conclusion, prophylactic DLI achieves better outcomes than no DLI for refractory acute leukemia undergoing allo-HSCT with intensified conditioning. The strategy of sequential intensified conditioning followed by early immunosupressant withdrawal and DLI could reduce relapse of refractory acute leukemia after allo-HSCT.
PATIENTS AND METHODS
Patients and eligibility criteria
We conducted a prospective and non-randomized controlled study. Patients were included if they were refractory acute leukemia, not in CR pre-transplantation and age between 12 and 55 years. Refractory acute leukemia was defined according to the literature [35-37]. Exclusion criteria included: CML-BC, creatinine clearance <50 mL/min, bilirubin or transaminase level >2 times the upper limit of normal, cardiac shortening fraction <30% and pregnancy. The study performed in accordance with modified Helsinki Declaration, and the protocol was approved by respective ethical review boards before study initiation. All recipients, donors and/or guardians provided written informed consent.
Conditioning regimen and strategies of inducing GVL
The conditioning regimen was modified by increasing the dosage of VP-16 from 10 mg/kg/day to 15 mg/kg/day on the basis of our historical intensified conditioning (Figure 2) [15]. CsA withdrawal and DLI were conducted in patients who met the following criteria (Figure 3). CsA was withdrawn by 10%/week in patients without aGVHD by day +30, and ended in complete withdrawal by day +90 post-transplantation in patients without aGVHD. For patients without grade II/>II aGVHD by day +60 post-transplantation, G-CSF mobilized DLI was administered at a median dose of 1.0 (range 0.7-1.4) ×108 mononuclear cells/kg if donor lymphocytes were available. DLI was given once to all patients regardless of MRD, and was then administered based on GVHD and MRD status. If patients were MRD negative, DLI was not given again; if patients were MRD positive and without GVHD, DLI was given monthly until GVHD occurred or MRD became negative or for a total of four times. For patients with aGVHD by day +30 or with grade II/>II aGVHD by day +60 post-transplantation, the application of DLI was based on the status of GVHD and MRD by day +90 and the availability of donor lymphocytes. If patients remained MRD+ and had no GVHD by day +90, DLI was administered according to the description above.
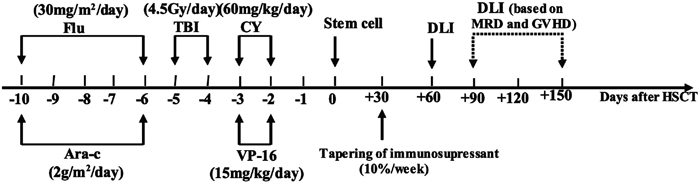
Figure 2: Protocol of sequential intensified conditioning followed by early tapering of immunosupressant and donor lymphocyte infusion for patients with refractory advanced acute leukemia undergoing allo-HSCT. Flu, fludarabine; Ara-C, cytarabine; TBI, total body irradiation; CY, cyclophosphamide; VP-16, etoposide; DLI, donor lymphocyte infusion; MRD, minimal residual disease; GVHD, graft-versus-host disease; HSCT, hematopoietic stem cell transplantation.
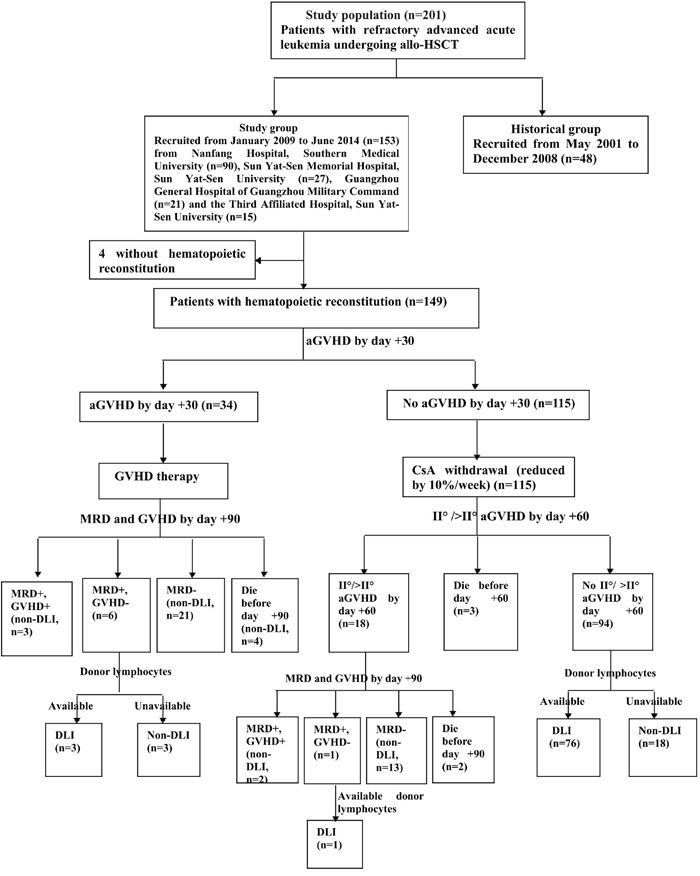
Figure 3: Strategies of inducing graft-versus-leukemia. allo-HSCT, allogeneic hematopoietic stem cell transplantation; GVHD, graft-versus-host disease; aGVHD, acute GVHD; CsA, cyclosporine A; MRD, minimal residual disease; DLI, donor lymphocyte infusion.
Donor lymphocyte preparation
Donor lymphocytes were obtained from original donors. Collections were performed on the fifth day of G-CSF mobilization, and consecutive daily collections were performed until acquiring the target numbers of stem cells planned for transplantation and DLI. Donor lymphocytes was cryopreserved separately for DLI.
GVHD prophylaxis and treatment
GVHD prophylaxis was described in our reports [15, 38]. CsA alone or CsA plus methotrexate (MTX) were administered in patients undergoing HLA-matched sibling donor transplants. CsA +MTX +antithymocyte globulin (ATG, Genzyme, Cambridge, MA) and/or mycophenolate were used in patients undergoing HLA-mismatched related and unrelated donor transplants. Methylprednisolone was used to treat aGVHD. CD25 monoclonal antibody (Novartis) alone or combined with ATG and other immunosupressant were used to treat glucocorticosteroid-resistant aGVHD. Corticosteroids and CsA in combination with various immunosupressant were used to treat cGVHD. Mesenchymal stem cells were also used to treat some patients with refractory aGVHD and cGVHD [39, 40].
Infection prophylaxis
Acyclovir was given daily from the beginning of conditioning to engraftment, and was then administered daily for 7 days every 2 weeks until 1 year post-transplantation. Ganciclovir was given for 2 weeks pre-transplantation for prophylaxis of CMV infection, and was administered once again when CMV-emia occurred [4]. Preemptive therapy for EBV-emia was according to our previous description [38, 41]. Antifungal agents were administered 5 days pre-transplantation and continued for +30 to +90 days post-transplantation or disease control according to the history and state of IFD pre-transplantation [42].
MRD monitoring
Two methods, including flow cytometry (FCM) and real-time quantitative polymerase chain reaction (RQ-PCR), were used for MRD detection. FCM positive was defined as >0.001% of cells with leukemia-associated aberrant immune phenotypes in BM samples post-transplantation. A total of 1 000 000 events were collected for analysis routinely. When cell numbers were limited, a minimal 750 000 events were collected. RQ-PCR was used for detection of leukemia-related genes including WT1, AML1/ETO, CBFβ/MYH11, MLL-PTD, MLL-AF9, MLL/AF4, BCR/ABL and E2A/PBX1 genes, defining the transcript level≥0.001% as PCR positive. MRD was monitored once a month in the first six months post-transplantation, once every two months until the 18th month, once every three months during the 19th to 36th month. If MRD was positive, it was monitored twice a month until MRD became negative. Subjects were scored as MRD positive if they had 2 consecutive positive results using FCM or PCR or were both FCM and PCR positive in a single sample.
Evaluation points and definitions
Our study data was analyzed on June 30, 2015. The primary evaluation point was relapse, and secondary endpoints included engraftment, disease response, RRTs, infections, GVHD, NRM, OS and DFS. Leukemia relapse was defined as BM, extramedullary, or both by common morphological criteria. FCM and molecular data were not used to define relapse. Hematopoietic reconstitution, chimerism and disease response were defined according to described criteria [15]. RRTs were defined as toxicities directly due to the conditioning regimen, and were graded according to Bearman’s criteria [43]; aGVHD and cGVHD were graded as described previously [44, 45]. Genetic subgroups were classified according to literature reported, including favorable, intermediate and unfavorable subgroups [46, 47]. NRM was defined as death from any cause other than relapse. EBV-associated disease was defined as infectious disease, rather than secondary tumor.
Statistics
Comparisons of categorical variables were made by means of chi-squared tests or Fisher exact test. Differences between numerical variables were calculated by means of Mann-Whitney U-test. Incidence of time-dependent variables was estimated by Kaplan-Meier method. Univariate and multivariate Cox regression models were used to analyze risk factors for leukemia relapse and survival post-transplantation. Additionally, the landmark analysis at 60 days was used to compare the outcomes of the DLI and non-DLI in the study group with our historical group in terms of relapse rate, NRM, OS and DFS. Log-rank test was used for the analysis with P values reported as 2-sided and <0.05 as statistical significance.
ACKNOWLEDGMENTS
This work was supported by National High Technology Research and Development Program of China (863 Program) (No. 2011AA020105), National Natural Science Foundation of China (No. 81270647, No. 81300445, No. 81200388, No. 81470349), Natural Science Foundation of Guangdong Province (No. S2012010009299, No. 2014A030310171) and the project of health collaborative innovation of Guangzhou city (No. 201400000003-4, No. 201400000003-1).
CONFLICTS OF INTEREST
The authors declare no competing financial interests.
REFERENCES
1. Oyekunle AA, Kroger N, Zabelina T, Ayuk F, Schieder H, Renges H, Fehse N, Waschke O, Fehse B, Kabisch H, Zander AR. Allogeneic stem-cell transplantation in patients with refractory acute leukemia: a long-term follow-up. Bone marrow transplantation. 2006; 37:45-50.
2. Fung HC, Stein A, Slovak M, O'Donnell M R, Snyder DS, Cohen S, Smith D, Krishnan A, Spielberger R, Bhatia R, Bhatia S, Falk P, Molina A, et al. A long-term follow-up report on allogeneic stem cell transplantation for patients with primary refractory acute myelogenous leukemia: impact of cytogenetic characteristics on transplantation outcome. Biol Blood Marrow Transplant. 2003; 9:766-771.
3. Saito T, Kanda Y, Kami M, Kato K, Shoji N, Kanai S, Ohnishi T, Kawano Y, Nakai K, Ogasawara T, Matsubara H, Makimoto A, Tanosaki R, et al. Therapeutic potential of a reduced-intensity preparative regimen for allogeneic transplantation with cladribine, busulfan, and antithymocyte globulin against advanced/refractory acute leukemia/lymphoma. Clin Cancer Res. 2002; 8:1014-1020.
4. Xiao H, Wang LM, Luo Y, Lai X, Li C, Shi J, Tan Y, Fu S, Wang Y, Zhu N, He J, Zheng W, Yu X, et al. Mutations in epigenetic regulators are involved in acute lymphoblastic leukemia relapse following allogeneic hematopoietic cell transplantation. Oncotarget. 2016; 7:2696-708. doi:10.18632/oncotarget.6259.
5. Sierra J, Storer B, Hansen JA, Martin PJ, Petersdorf EW, Woolfrey A, Matthews D, Sanders JE, Storb R, Appelbaum FR, Anasetti C. Unrelated donor marrow transplantation for acute myeloid leukemia: an update of the Seattle experience. Bone marrow transplantation. 2000; 26:397-404.
6. Mengarelli A, Iori A, Guglielmi C, Romano A, Cerretti R, Torromeo C, Micozzi A, Fenu S, Laurenti L, Donato V, De Felice L, Arcese W. Standard versus alternative myeloablative conditioning regimens in allogeneic hematopoietic stem cell transplantation for high-risk acute leukemia. Haematologica. 2002; 87:52-58.
7. Ringden O, Labopin M, Tura S, Arcese W, Iriondo A, Zittoun R, Sierra J, Gorin NC. A comparison of busulphan versus total body irradiation combined with cyclophosphamide as conditioning for autograft or allograft bone marrow transplantation in patients with acute leukaemia. Acute Leukaemia Working Party of the European Group for Blood and Marrow Transplantation (EBMT). British journal of haematology. 1996; 93:637-645.
8. Aschan J. Risk assessment in haematopoietic stem cell transplantation: conditioning. Best practice & research. 2007; 20:295-310.
9. Engelhard D, Elishoov H, Or R, Naparstek E, Nagler A, Strauss N, Cividalli G, Aker M, Ramu N, Simhon A, et al. Cytosine arabinoside as a major risk factor for Streptococcus viridans septicemia following bone marrow transplantation: a 5-year prospective study. Bone marrow transplantation. 1995; 16:565-570.
10. van Besien K. Allogeneic transplantation for AML and MDS: GVL versus GVHD and disease recurrence. Hematology. 2013; 2013: 56-62.
11. Schmid C, Schleuning M, Ledderose G, Tischer J, Kolb HJ. Sequential regimen of chemotherapy, reduced-intensity conditioning for allogeneic stem-cell transplantation, and prophylactic donor lymphocyte transfusion in high-risk acute myeloid leukemia and myelodysplastic syndrome. J Clin Oncol. 2005; 23:5675-5687.
12. Schmid C, Schleuning M, Schwerdtfeger R, Hertenstein B, Mischak-Weissinger E, Bunjes D, Harsdorf SV, Scheid C, Holtick U, Greinix H, Keil F, Schneider B, Sandherr M, et al. Long-term survival in refractory acute myeloid leukemia after sequential treatment with chemotherapy and reduced-intensity conditioning for allogeneic stem cell transplantation. Blood. 2006; 108: 1092-1099.
13. Saure C, Schroeder T, Zohren F, Groten A, Bruns I, Czibere A, Galonska L, Kondakci M, Weigelt C, Fenk R, Germing U, Haas R, Kobbe G. Upfront allogeneic blood stem cell transplantation for patients with high-risk myelodysplastic syndrome or secondary acute myeloid leukemia using a FLAMSA-based high-dose sequential conditioning regimen. Biol Blood Marrow Transplant. 2012; 18:466-472.
14. Zohren F, Czibere A, Bruns I, Fenk R, Schroeder T, Graf T, Haas R, Kobbe G. Fludarabine, amsacrine, high-dose cytarabine and 12 Gy total body irradiation followed by allogeneic hematopoietic stem cell transplantation is effective in patients with relapsed or high-risk acute lymphoblastic leukemia. Bone marrow transplantation. 2009; 44:785-792.
15. Liu QF, Fan ZP, Zhang Y, Jiang ZJ, Wang CY, Xu D, Sun J, Xiao Y, Tan H. Sequential intensified conditioning and tapering of prophylactic immunosuppressants for graft-versus-host disease in allogeneic hematopoietic stem cell transplantation for refractory leukemia. Biol Blood Marrow Transplant. 2009; 15:1376-1385.
16. Witherspoon RP, Deeg HJ, Storer B, Anasetti C, Storb R, Appelbaum FR. Hematopoietic stem-cell transplantation for treatment-related leukemia or myelodysplasia. J Clin Oncol. 2001; 19:2134-2141.
17. Singhal S, Powles R, Henslee-Downey PJ, Chiang KY, Treleaven J, Godder K, Kulkarni S, van Rhee F, Sirohi B, Pinkerton CR, Meller S, Mehta J. Allogeneic transplantation from HLA-matched sibling or partially HLA-mismatched related donors for primary refractory acute leukemia. Bone marrow transplantation. 2002; 29:291-295.
18. Michallet M, Thomas X, Vernant JP, Kuentz M, Socie G, Esperou-Bourdeau H, Milpied N, Blaise D, Rio B, Reiffers J, Jouet JP, Cahn JY, Bourhis JH, et al. Long-term outcome after allogeneic hematopoietic stem cell transplantation for advanced stage acute myeloblastic leukemia: a retrospective study of 379 patients reported to the Societe Francaise de Greffe de Moelle (SFGM). Bone marrow transplantation. 2000; 26:1157-1163.
19. Duval M, Klein JP, He W, Cahn JY, Cairo M, Camitta BM, Kamble R, Copelan E, de Lima M, Gupta V, Keating A, Lazarus HM, Litzow MR, et al. Hematopoietic stem-cell transplantation for acute leukemia in relapse or primary induction failure. J Clin Oncol. 2010; 28:3730-3738.
20. Tang W, Fan X, Wang L, Hu J. Busulfan and fludarabine conditioning regimen given at hematological nadir of cytoreduction fludarabine, cytarabine, and idarubicin chemotherapy in patients with refractory acute myeloid leukemia undergoing allogeneic stem cell transplantation: a single arm pilot consort study. Medicine. 2015; 94: e706.
21. Giralt S, Thall PF, Khouri I, Wang X, Braunschweig I, Ippolitti C, Claxton D, Donato M, Bruton J, Cohen A, Davis M, Andersson BS, Anderlini P, et al. Melphalan and purine analog-containing preparative regimens: reduced-intensity conditioning for patients with hematologic malignancies undergoing allogeneic progenitor cell transplantation. Blood. 2001; 97:631-637.
22. Baron F, Zachee P, Maertens J, Kerre T, Ory A, Seidel L, Graux C, Lewalle P, Van Gelder M, Theunissen K, Willems E, Emonds MP, De Becker A, et al. Non-myeloablative allogeneic hematopoietic cell transplantation following fludarabine plus 2 Gy TBI or ATG plus 8 Gy TLI: a phase II randomized study from the Belgian Hematological Society. Journal of hematology & oncology. 2015; 8:4.
23. Mineishi S, Longo WL, Atkinson ME, Smith EP, Hamielec M, Wiersma SR, Kinsella TJ, Schuening FG. Addition of high-dose Ara-C to the BMT conditioning regimen reduces leukemia relapse without an increase in toxicity. Bone marrow transplantation. 1999; 23:1217-1222.
24. Thomas MB, Koller C, Yang Y, Shen Y, O'Brien S, Kantarjian H, Davis J, Estey E. Comparison of fludarabine-containing salvage chemotherapy regimens for relapsed/refractory acute myelogenous leukemia. Leukemia. 2003; 17:990-993.
25. Mato AR, Morgans A, Luger SM. Novel strategies for relapsed and refractory acute myeloid leukemia. Current opinion in hematology. 2008; 15:108-114.
26. Shi-Xia X, Xian-Hua T, Hai-Qin X, Bo F, Xiang-Feng T. Total body irradiation plus cyclophosphamide versus busulphan with cyclophosphamide as conditioning regimen for patients with leukemia undergoing allogeneic stem cell transplantation: a meta-analysis. Leukemia & lymphoma. 2010; 51:50-60.
27. Bachireddy P, Wu CJ. Understanding anti-leukemia responses to donor lymphocyte infusion. Oncoimmunology. 2014; 3:e28187.
28. Elmaagacli AH, Beelen DW, Trenn G, Schmidt O, Nahler M, Schaefer UW. Induction of a graft-versus-leukemia reaction by cyclosporin A withdrawal as immunotherapy for leukemia relapsing after allogeneic bone marrow transplantation. Bone marrow transplantation. 1999; 23:771-777.
29. Yan CH, Liu DH, Liu KY, Xu LP, Liu YR, Chen H, Han W, Wang Y, Qin YZ, Huang XJ. Risk stratification-directed donor lymphocyte infusion could reduce relapse of standard-risk acute leukemia patients after allogeneic hematopoietic stem cell transplantation. Blood. 2012; 119:3256-3262.
30. Wang Y, Liu DH, Fan ZP, Sun J, Wu XJ, Ma X, Xu LP, Liu KY, Liu QF, Wu DP, Huang XJ. Prevention of relapse using DLI can increase survival following HLA-identical transplantation in patients with advanced-stage acute leukemia: a multi-center study. Clinical transplantation. 2012; 26:635-643.
31. Huang XJ, Wang Y, Liu DH, Xu LP, Chen H, Chen YH, Han W, Shi HX, Liu KY. Modified donor lymphocyte infusion (DLI) for the prophylaxis of leukemia relapse after hematopoietic stem cell transplantation in patients with advanced leukemia—feasibility and safety study. Journal of clinical immunology. 2008; 28:390-397.
32. Liu H, Zhai X, Song Z, Sun J, Xiao Y, Nie D, Zhang Y, Huang F, Zhou H, Fan Z, Tu S, Li Y, Guo X, et al. Busulfan plus fludarabine as a myeloablative conditioning regimen compared with busulfan plus cyclophosphamide for acute myeloid leukemia in first complete remission undergoing allogeneic hematopoietic stem cell transplantation: a prospective and multicenter study. Journal of hematology & oncology. 2013; 6:15.
33. Arai Y, Aoki K, Takeda J, Kondo T, Eto T, Ota S, Hashimoto H, Fukuda T, Ozawa Y, Kanda Y, Kato C, Kurokawa M, Iwato K, et al. Clinical significance of high-dose cytarabine added to cyclophosphamide/total-body irradiation in bone marrow or peripheral blood stem cell transplantation for myeloid malignancy. Journal of hematology & oncology. 2015; 8:102.
34. Martin-Pena A, Aguilar-Guisado M, Espigado I, Parody R, Miguel Cisneros J. Prospective study of infectious complications in allogeneic hematopoietic stem cell transplant recipients. Clinical transplantation. 2011; 25:468-474.
35. Estey E. Treatment of refractory AML. Leukemia. 1996; 10:932-936.
36. Kern W, Schoch C, Haferlach T, Braess J, Unterhalt M, Wormann B, Buchner T, Hiddemann W. Multivariate analysis of prognostic factors in patients with refractory and relapsed acute myeloid leukemia undergoing sequential high-dose cytosine arabinoside and mitoxantrone (S-HAM) salvage therapy: relevance of cytogenetic abnormalities. Leukemia. 2000; 14:226-231.
37. Li X, Liu L, Zhang Y, Qu Q, Yao Y, Wang T, Jiao W, Wu D. Efficacy of cytarabine, aclarubicin and granulocyte colony-stimulating factor (CAG) regimen compared to FLAG regimen for adult patients with relapsed/refractory Philadelphia chromosome-negative acute lymphoblastic leukemia. Leukemia research. 2015; doi:10.1016/j.leukres. 2015.08. 013.
38. Xuan L, Huang F, Fan Z, Zhou H, Zhang X, Yu G, Zhang Y, Liu C, Sun J, Liu Q. Effects of intensified conditioning on Epstein-Barr virus and cytomegalovirus infections in allogeneic hematopoietic stem cell transplantation for hematological malignancies. Journal of hematology & oncology. 2012; 5:46.
39. Zhao K, Lou R, Huang F, Peng Y, Jiang Z, Huang K, Wu X, Zhang Y, Fan Z, Zhou H, Liu C, Xiao Y, Sun J, et al. Immunomodulation effects of mesenchymal stromal cells on acute graft-versus-host disease after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2015; 21:97-104.
40. Peng Y, Chen X, Liu Q, Zhang X, Huang K, Liu L, Li H, Zhou M, Huang F, Fan Z, Sun J, Liu Q, Ke M, et al. Mesenchymal stromal cells infusions improve refractory chronic graft versus host disease through an increase of CD5+ regulatory B cells producing interleukin 10. Leukemia. 2015; 29: 636-646.
41. Liu Q, Xuan L, Liu H, Huang F, Zhou H, Fan Z, Zhao K, Wu M, Xu L, Zhai X, Zhang F, Liu C, Sun J, et al. Molecular monitoring and stepwise preemptive therapy for Epstein-Barr virus viremia after allogeneic stem cell transplantation. American journal of hematology. 2013; 88: 550-555.
42. Liu Q, Lin R, Sun J, Xiao Y, Nie D, Zhang Y, Huang F, Fan Z, Zhou H, Jiang Q, Zhang F, Zhai X, Xu D, et al. Antifungal agents for secondary prophylaxis based on response to initial antifungal therapy in allogeneic hematopoietic stem cell transplant recipients with prior pulmonary aspergillosis. Biol Blood Marrow Transplant. 2014; 20:1198-1203.
43. Bearman SI, Appelbaum FR, Buckner CD, Petersen FB, Fisher LD, Clift RA, Thomas ED. Regimen-related toxicity in patients undergoing bone marrow transplantation. J Clin Oncol. 1988; 6:1562-1568.
44. Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, Thomas ED. 1994 Consensus Conference on Acute GVHD Grading. Bone marrow transplantation. 1995; 15: 825-828.
45. Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR, Lee SJ, Martin P, Chien J, Przepiorka D, Couriel D, Cowen EW, Dinndorf P, Farrell A, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005; 11:945-956.
46. Mrozek K, Heerema NA, Bloomfield CD. Cytogenetics in acute leukemia. Blood reviews. 2004; 18:115-136.
47. Bacher U, Schnittger S, Haferlach C, Haferlach T. Molecular diagnostics in acute leukemias. Clin Chem Lab Med. 2009; 47:1333-1341.