
INTRODUCTION
Nasopharyngeal carcinoma (NPC) has a distinct epidemiology and geographic distribution, with the highest incidence of 20-50 cases per 100,000 males in Southern China [1]. Radiotherapy (RT) is the primary treatment modality for non-disseminated NPC due to its anatomical location and radiosensitivity [2]; however, the results with radiotherapy alone for locoregionally advanced NPC patients are usually unsatisfactory with 5-year overall survival (OS) rates of 67%-77% in stage III-IVB [3]. Various chemoradiotherapy (CRT) strategies have been explored, including concomitant chemoradiotherapy (CCRT), induction chemotherapy (IC) and adjuvant chemotherapy (AC)[4].
At present, standard clinical practice is to stage NPC according to the tumor-node-metastasis (TNM) staging system, which is based on the anatomic extent of the tumor and excluded patient-based prognostic factors. Comorbidity which is defined as the presence of medical ailments not caused by the primary tumor may add difficulty to treatment decisions for the use of chemotherapy [5]. In addition, as CRT strategies are widely used, it may exacerbate comorbidity, which may ultimately compromise survival or quality of life [6]. Therefore, The risks, decision making and potential benefit of CRT are necessary to assess for NPC patients with comorbidity before treatment.
Previous studies showed that patients with comorbidities received less, similar or more frequent uses of chemotherapy in different solid tumor [6]. However, little is known about outcome of CRT in patients with comorbidity, as comorbidities are generally not considered in the design of cancer data sets or assessed in observational research on the selection of CRT [7]. For NPC patients, no studies have investigated the impact of comorbidity on the selection of CRT and clinical outcome in NPC. We conducted this retrospective study to assess the impact of comorbidity on treatment selection and its ultimate effect on survival, in order to help optimize cancer care for patients with NPC undergoing CRT.
RESULTS
The median follow-up was 75.3 months (range, 2.7-126.5 months). A total of 125/1316 (9.5%) patients developed local failure, 52/1316 (4.9%) developed regional failure, 19/1316 (1.4%) developed both local and regional failure, 233/1316 (17.7%) developed distant metastases, and 291/1316 (22.1%) patients died. The 5-year DFS, OS, DMFS and LRRFS rates were 71.7%, 79.5%, 82.5% and 87.9%, respectively.
Differences of the patients with or without comorbidity
The overall distribution of stage I, II, III and IVA-B diseases was 8.7%, 25.4%, 36.9% and 29.0%, respectively. There was no association between disease stage and comorbidity, as indicated by ACE-27; however, the stage III-IV NPC patients with comorbidity (ACE-27 > 0) significantly received decreased chemotherapy compared with patients without comorbidity (67.6%vs.74.0%; P = 0.037). Furthermore, the significant associations were also observed between comorbidity and gender, age and type of radiotherapy (P < 0.05; Table 1).
Table 1: Characteristics of the 1316 patients with nasopharyngeal carcinoma.
Patient characteristics |
Without comorbidity (ACE-27=0) |
With Comorbidity (ACE-27>0) |
P-value |
No |
761 |
555 |
|
Age |
<0.001 |
||
< 45 years |
444 (58.3) |
239(43.1) |
|
≥ 45 years |
317( 41.7) |
316(56.9) |
|
Gender |
<0.001 |
||
Male |
537 (70.6) |
449 (80.6) |
|
Female |
224 (29.4) |
106 (19.1) |
|
Histology |
0.660 |
||
WHO type I |
4 (0.5) |
2 (0.4) |
|
WHO type II/III |
757(99.5) |
553 (99.6) |
|
T classification* |
0.744 |
||
T1 |
171 (22.5) |
119 (21.4) |
|
T2 |
175 (23.0) |
128 (23.1) |
|
T3 |
254 (33.4) |
177 (31.9) |
|
T4 |
161 (21.2) |
131 (23.6) |
|
N classification* |
0.203 |
||
N0 |
211 (27.7) |
177 (31.9) |
|
N1 |
344 (45.2) |
235 (42.3) |
|
N2 |
147 (19.3) |
92(16.6) |
|
N3 |
59 (7.8) |
51 (9.2) |
|
Clinical stage* |
0.339 |
||
I |
63 (8.3) |
52 (9.4) |
|
II |
201 (26.4) |
133 (24.0) |
|
III |
289 (38.0) |
197 (35.5) |
|
IVA-B |
208 (27.3) |
173 (31.2) |
|
Radiotherapy |
0.002 |
||
2-DRT |
418 (54.9) |
352 (63.4) |
|
3-DRT or IMRT |
343 (45.1) |
203 (36.6) |
|
Chemotherapy in stage III-IV |
0.037 |
||
RT only |
129 (26.0) |
120 (32.4) |
|
RT+chemotherapy |
368 (74.0) |
250 (67.6) |
Abbreviations: WHO, World Health Organization; 2-DRT, two-dimensional radiotherapy; 3-DCRT, three-dimensional conformal radiotherapy; IMRT, intensity-modulated radiotherapy; RT
* According to the 7th AJCC/UICC staging system.
Prevalence, types and prognostic value of comorbidity
Of the 1316 patients, 555 (42.2%) had one or more comorbidity; 442 (33.6%) patients had ACE-27 scores of 1, 106 (8.1%) had scores of 2, and 7 (0.5%) had scores of 3. Gastrointestinal disease (24.9%), substance abuse (12.9%) and cardiovascular disease (5.4%) were most frequently observed (Table 2).
Table 2: Presence and severity of comorbidity in the study population of 1316 patients with NPC
Disease classification according to ACE-27 |
Grade 1: mild |
Grade 2: moderate |
Grade 3: severe |
|
Overall ACE27 score |
442 (33.6%) |
106 (8.1%) |
7 (0.5%) |
|
Specific ACE27 categories |
||||
Cardiovascular system |
64 (4.9%) |
7 (0.5%) |
0 (0.0%) |
|
Respiratory system |
25 (1.9%) |
4 (0.3%) |
0 (0.0%) |
|
Gastrointestinal system |
317 (24.1%) |
11 (0.8%) |
0 (0.0%) |
|
Renal system |
34 (2.6%) |
0 (0.0%) |
0 (0.0%) |
|
Endocrine system |
21 (1.6%) |
2 (0.2%) |
0 (0.0%) |
|
Neurological system |
6 (0.5%) |
0(0.0%) |
0 (0.0%) |
|
Psychiatric |
1 (0.1%) |
0 (0.0%) |
0 (0.0%) |
|
Rheumatologic |
2 (0.2%) |
0 (0.0%) |
0 (0.0%) |
|
Immunological system |
0 (0.0%) |
0 (0.0%) |
0 (0.0%) |
|
Malignancy |
4 (0.3%) |
5 (0.4%) |
5 (0.4%) |
|
Substance abuse |
89 (6.8%) |
80 (6.1%) |
0 (0.0%) |
|
Body weight |
1 (0.1%) |
1 (0.1%) |
0 (0.0%) |
|
Abbreviation: ACE-27, Adult Comorbidity Evaluation-27.
In univariate analysis, the 5-year OS rates of patients with ACE-27 grades of 0, 1 and ≥ 2 were 85.2%, 74.3% and 63.2% (P < 0.001; Figure 1A). The 5-year DFS rates of patients with ACE-27 grades of 0, 1 and ≥ 2 were 77.6%, 67.4% and 50.2% (P < 0.001; Figure 1B). In multivariate analysis, ACE-27 had significant independent prognostic value for OS (hazard ratio [HR] = 1.577; P < 0.001) and DFS (HR = 1.509; P < 0.001; Table 3).
Table 3: Multivariate analysis of the impact of all variables on survival
Endpoint |
Variable |
HR |
HR (95% CI) |
P-value‡ |
Overall survival |
ACE-27 |
1.577 |
1.345-1.850 |
<0.001 |
T classification* |
1.548 |
1.374-1.744 |
<0.001 |
|
N classification* |
1.695 |
1.499-1.916 |
<0.001 |
|
Age |
1.376 |
1.088-1.740 |
0.008 |
|
Disease-free survival |
ACE-27 |
1.509 |
1.314-1.734 |
<0.001 |
T classification* |
1.452 |
1.314-1.605 |
<0.001 |
|
N classification* |
1.527 |
1.373-1.698 |
<0.001 |
Abbreviation: ACE-27, Adult Comorbidity Evaluation-27; CI, confidence interval; HR, hazard ratio.
*According to the 7th AJCC/UICC staging system.
‡ Multivariate P values were calculated using an adjusted Cox proportional-hazards model. The following parameters were included in the Cox proportion hazard model by backward elimination: age, gender, World Health Organization (WHO) histological grade, T classification, N classification, radiotherapy (conformal vs. 3D and intensity modulated radiation therapy), use of chemotherapy (with vs. without) and ACE-27.
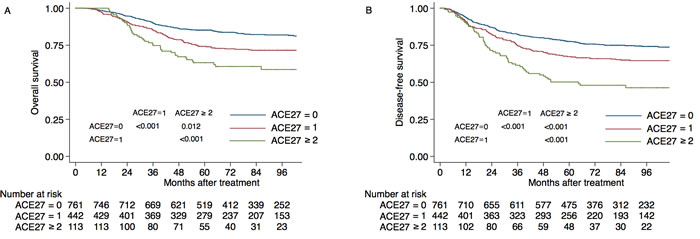
Figure 1: Kaplan-Meier estimates of survival for the 1316 study patients with nasopharyngeal cancer, according to ACE27 grade. A. Overall survival, B. disease-free survival.
Factors associated with initiation of CRT in advanced stage disease
For stage III-IV NPC patients, T classification, N classification, age, sex and hemoglobin before treatment and comorbidity (with vs. without) were significantly associated with the initiation of CRT in univariate analysis (P < 0.05; Table 4). And the T classification, N classification, age, sex and hemoglobin before treatment were significantly associated with the initiation of CRT in multivariable logistic regression (P < 0.05; Table 4). Furthermore, patients with a higher renal system burden and substance abuse were less likely to receive CRT (P = 0.068; P = 0.017; Table 4).
Table 4: Logistic regression analyses of factors associated with the uptake of chemotherapy by patients with stage III-IV nasopharyngeal carcinoma
Characteristic |
No. |
HR |
95% CI for HR |
Univariate P-value† |
Multivariate P-value‡ |
Age (y) |
867 |
0.977 |
0.961-0.993 |
<0.001 |
0.003 |
Sex |
0.008 |
<0.001 |
|||
Male |
649 |
1 |
Reference |
||
Female |
218 |
0.317 |
0.196-0.512 |
||
Histological type |
0.362 |
NS |
|||
WHO type I |
4 |
Reference |
|||
WHO type II-III |
863 |
1.392 |
0.169-11.443 |
||
Hematology |
|||||
Hemoglobin |
867 |
0.968 |
0.955-0.981 |
<0.001 |
<0.001 |
Platelet |
867 |
1.001 |
0.995-1.007 |
0.907 |
NS |
White blood cell |
867 |
0.860 |
0.590-1.254 |
0.110 |
NS |
Neutrophil |
867 |
1.077 |
0.671-1.729 |
0.076 |
NS |
Comorbidity present (Overall) |
0.037 |
0.089 |
|||
Cardiovascular system |
867 |
0.999 |
0.495-2.017 |
0.300 |
NS |
Respiratory system |
867 |
0.756 |
0.282-2.024 |
0.264 |
NS |
Gastrointestinal system |
867 |
0.890 |
0.625-1.266 |
0.212 |
NS |
Renal system |
867 |
0.372 |
0.128-1.077 |
0.077 |
0.068 |
Endocrine system |
867 |
0.784 |
0.246-2.498 |
0.159 |
NS |
Neurological system |
867 |
0.899 |
0.112-7.220 |
0.580 |
NS |
Malignancy |
867 |
1.165 |
0.280-4.849 |
0.751 |
NS |
Substance abuse |
867 |
0.596 |
0.434-0.820 |
0.020 |
0.001 |
Staging |
|||||
T classification§ |
|||||
T1 |
62 |
1.00 |
Reference |
||
T2 |
82 |
0.218 |
0.085-0.554 |
0.507 |
0.001 |
T3 |
431 |
0.219 |
0.095-0.502 |
0.109 |
<0.001 |
T4 |
292 |
0.462 |
0.297-0.721 |
0.001 |
0.001 |
N classification§ |
|||||
N0 |
184 |
1.00 |
Reference |
||
N1 |
334 |
0.123 |
0.049-0.310 |
<0.001 |
<0.001 |
N2 |
239 |
0.206 |
0.085-0.499 |
0.049 |
<0.001 |
N3 |
110 |
0.363 |
0.163-0.808 |
0.038 |
0.013 |
Abbreviations: ACE-27, Adult Comorbidity Evaluation-27; CI, confidence interval; HR, hazard ratio; NS, not statistically significant; RT, radiotherapy; WHO, World Health Organization.
† Univariate P values were calculated using the binary logistic regession model.
‡ Multivariate P values were calculated using the binary logistic regession model.
§ According to the 7th AJCC/UICC staging system.
Effect of comorbidity on CRT treatment outcomes
For stage III-IV patients with a comorbidity (ACE > 0), the 5-year OS rate in the CCRT group was 74.5% vs. 56.9% for RT only (P = 0.008), 65.0% for CCRT + AC/IC (P = 0.318) and 54.9% for IC/AC (P = 0.024; Figure 2A). The 5-year DFS rates was 64.0% in the CCRT group vs. 49.4% for RT only (P = 0.015), 57.9% for CCRT + AC/IC (P = 0.505) and 45.9% for IC/AC (P = 0.014; Figure 2B).
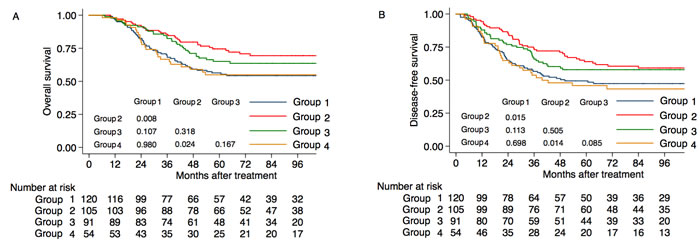
Figure 2: Kaplan-Meier overall survival curves for patients with Stage III-IV nasopharyngeal cancer according to the chemotherapy strategy A. Overall survival for patients with comorbidity (ACE scores > 0); B. disease-free survival for patients with comorbidity (ACE scores > 0). Group 1: radiotherapy (RT) only; Group 2: concomitant chemoradiotherapy (CCRT); Group 3: concomitant chemoradiotherapy plus induction chemotherapy/adjuvant chemotherapy (CCRT + IC/AC): Group 4: induction chemotherapy or adjuvant chemotherapy (IC/AC).
DISCUSSION
Patients with comorbidities present considerable challenges to cancer management because they are often excluded from clinical trials. To our knowledge, this is a single-institutional study with the largest sample size to report the impact of comorbidity on the uptake of chemotherapy in NPC patients.
The prevalence of comorbidity for NPC in south China
Comorbidities occur in 33%-65% of patients with head and neck cancer, with cardiovascular and pulmonary diseases most common [7-13]. In our research, 42.2% of patients with NPC had comorbidity; however, the most common comorbidities were gastrointestinal disease, which, according to the ACE-27, includes liver disease. This was not surprising as southern China has one of the highest incidences of chronic hepatitis B virus (HBV) infection, with hepatitis B surface antigen (HBsAg) positivity rates of 10-12% in the general population [14]. Therefore, chronic HBV infection may be an important gastrointestinal comorbidity in patients with NPC in southern China. An increased frequency and severity of comorbidity were noted with increasing age and in male patients. Piccirillo et al. also reported that increased age was associated with an increasing number and severity of comorbidities [15] with similar results obtained in other studies [13, 16, 17]. In this study, the second most frequent comorbidity was substance abuse, mainly in male patients.
Factors associated with the initiation of chemotherapy in advanced stage NPC
Age, T classification, N classification, pretreatment hemoglobin were independent predictive factors for initiation of CRT; in agreement with previous studies demonstrating elderly patients tend to receive less intensive treatment [18]. However, The reduction in the use of CRT was only in patients with renal disease. Chemotherapy strategies for NPC include cisplatin, the use of which is limited by its severe acute and chronic nephro-, oto- and neuro-toxicity[19]. In everyday practice, the initiation of CRT is not primarily determined by comorbidity conditions, but renal disease.
Implications of CRT in patients with comorbidity
Little is known about the toxicity and outcomes of CRT regimes in patients with s comorbidity, as these patients are often excluded from clinical trials. Our results indicate CCRT improved OS compared to RT only for patients with mild, moderate and severe comorbidity. Nevertheless, adding IC or AC to CCRT had no significant OS benefit. CCRT also improved OS compared to RT alone in patients with comorbidity (ACE > 0). Therefore, if patients with advanced NPC and comorbidity desire curative treatment, we consider CCRT to be the most appropriate approach; further studies are required to identify more intensive systemic approaches and novel agents, such as molecular-targeted agents, to improve the treatment outcomes for these patients. Moreover, patients with comorbidity should receive complete supportive care during treatment to ensure optimal outcome. ACE-27 requires no special technological expertise and can be applied by any healthcare professional. Comorbidity assessment could easily be included in research into prognostic factors and could represent a major confounder in clinical trials.
Since this was a retrospective sample, we had no control over the nature and quality of the medical records. Nevertheless, the records were detailed and provided accurate information on the patients’ clinical characteristics. More importantly, these results clearly demonstrate that comorbidity must be routinely considered with other significant prognostic factors in both clinical work and research. This study also justifies the need for prospective collection of comorbidity data in routine clinical practice.
Conclusions
Comorbidity information should be incorporated into treatment strategy decision-making processes, to aid patient consultation and improve clinician decision-making. Concomitant chemoradiotherapy is feasible and effective in patients with comorbidity in locoregionally advanced stages.
materials and Methods
Patient selection
Between February 2003 and January 2007, 1403 newly-diagnosed patients with non-metastatic, histologically-proven NPC at Sun Yat-sen University Cancer Center (Guangzhou, People’s Republic of China) were retrospectively reviewed. Of these, 87 were excluded due to a lack of substantial data on comorbidity; the remaining 1316 cases were included. This retrospective analysis of the patient data was approved by the ethics committee of Sun Yat-sen University Cancer Center. Written consent was waived, while oral consent from the patients was obtained via telephone and documented by telephone recording.
All patients completed pretreatment evaluations, including complete medical history, physical examination, MRI of the nasopharynx and neck, hematology and biochemistry profiles, abdominal ultrasonography, chest radiography and whole body bone scan using single photon emission computed tomography (ECT); 139 (10.6%) patients also underwent positron emission tomography CT (PET-CT). All patients were restaged according to the 7th edition of the International Union against Cancer/American Joint Committee on Cancer (UICC/AJCC) system [20]. All MRI records were separately reviewed by two radiologists to minimize heterogeneity, disagreements were resolved by consensus.
Comorbidity assessment
Comorbidity was evaluated by the Adult Comorbidity Evaluation-27 (ACE-27), a validated 27-item comorbidity index specifically developed for head and neck cancer [21-23]. The detailed information on the patients’ baseline medical condition and comorbidities (collected before diagnosis of primary NPC) were reviewed by one physician for ACE-27 scores. ACE-27 defines specific conditions using three grades (grade 0 = none; 1 = minimal; 2 = moderate; 3 = severe) according to organ system decompensation. The overall comorbidity score for each patient was based on the highest-ranked single ailmen. When two or more moderate ailments occurred in different organ systems, the overall comorbidity score was graded as severe.
Treatment
Radiotherapy: All patients underwent definitive RT as reported previously [24-26]; 770/1316 (58.5%) received two-dimensional radiotherapy (2D-CRT) and 546/1,316 (41.5%) received three-dimensional conformal radiotherapy (3-DCRT) or intensity-modulated radiotherapy (IMRT).
Chemotherapy: The majority of the patients (618 of 867; 71.3%) with stage III or IV NPC (classified as T3-T4 and = or N2-N3 disease) received chemotherapy, including CCRT+/-IC/AC. Of these, 28.3% (245/867) patients received CCRT only, 30.8% (267/867) received CCRT+IC/AC, 12.2% (106/867) received RT+IC/AC. IC or AC consisted of cisplatin (80 mg/m2) with 5-fluorouracil (800 mg/m2/day over 120 h), or cisplatin (80 mg/m2) with taxanes (80 mg/m2) every 3 weeks for two or three cycles. CCRT consisted of cisplatin (80 or 100 mg/m2) on weeks 1, 4 and 7 of radiotherapy, or cisplatin (40 mg/m2) weekly.
Follow-up and statistical analyses
The following end points (time to the first defining event) were assessed: overall survival (OS), disease-free survival (DFS), locoregional relapse-free survival (LRRFS) and distant metastasis-free survival (DMFS). Follow-up was calculated from first day of therapy to the day of death or last examination. Patients were followed-up every 3 months during the first 2 years, and every 6-12 months thereafter until death.
We used univariate analyses to examine the association of various factors with CRT. Then, multivariable logistic regression was used to calculate adjusted hazard ratio HRs. Actuarial rates were estimated by the Kaplan-Meier method, survival curves compared using the log-rank test. Multivariate analysis using a Cox proportional hazards model was used to test the different factors by backward elimination. Host factors (sex, age, ACE-27), tumor factors (histology, T and N classification), and treatment factors (RT technique and chemotherapy) were included as covariates in all analyses. Stata Statistical Package (STATA 12; StataCorp LP, College Station, Texas, USA) was used for all analysis. All tests were two-sided, P < 0.05 was considered significant.
CONFLICTS OF INTEREST
The authors indicate no actual or potential conflicts of interest exist.
GRANT SUPPORT
This work was supported by grants from the Health & Medical Collaborative Innovation Project of Guangzhou City, China (201400000001), the National Science & Technology Pillar Program during the Twelfth Five-year Plan Period (2014BAI09B10), the Innovation Team Development Plan of the Ministry of Education (No.IRT1297), the National Natural Science Foundation of China (No.81230056), the Science and Technology Project of Guangzhou (Nos. 12BppZXaa2060002), Key Laboratory Construction Project of Guangzhou City, China (No.121800085).
REFERENCES
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E and Forman D. Global cancer statistics. CA Cancer J Clin. 2011; 61:69-90.
2. Chan AT. Nasopharyngeal carcinoma. Ann Oncol. 2010; 21 Suppl 7:vii308-312.
3. Yi JL, Gao L, Huang XD, Li SY, Luo JW, Cai WM, Xiao JP and Xu GZ. Nasopharyngeal carcinoma treated by radical radiotherapy alone: Ten-year experience of a single institution. Int J Radiat Oncol Biol Phys. 2006; 65:161-168.
4. OuYang PY, Xie C, Mao YP, Zhang Y, Liang XX, Su Z, Liu Q and Xie FY. Significant efficacies of neoadjuvant and adjuvant chemotherapy for nasopharyngeal carcinoma by meta-analysis of published literature-based randomized, controlled trials. Ann Oncol. 2013; 24:2136-2146.
5. Piccirillo JF and Feinstein AR. Clinical symptoms and comorbidity: significance for the prognostic classification of cancer. Cancer. 1996; 77:834-842.
6. Lee L, Cheung WY, Atkinson E and Krzyzanowska MK. Impact of comorbidity on chemotherapy use and outcomes in solid tumors: a systematic review. J Clin Oncol. 2011; 29:106-117.
7. Piccirillo JF, Tierney RM, Costas I, Grove L and Spitznagel EL, Jr. Prognostic importance of comorbidity in a hospital-based cancer registry. JAMA. 2004; 291: 2441-2447.
8. Alho OP, Hannula K, Luokkala A, Teppo H, Koivunen P and Kantola S. Differential prognostic impact of comorbidity in head and neck cancer. Head Neck. 2007; 29:913-918.
9. Boje CR, Dalton SO, Gronborg TK, Primdahl H, Kristensen CA, Andersen E, Johansen J, Andersen LJ and Overgaard J. The impact of comorbidity on outcome in 12 623 Danish head and neck cancer patients: a population based study from the DAHANCA database. Acta oncologica. 2013; 52:285-293.
10. Datema FR, Ferrier MB, van der Schroeff MP and Baatenburg de Jong RJ. Impact of comorbidity on short-term mortality and overall survival of head and neck cancer patients. Head Neck. 2010; 32:728-736.
11. Hall SF, Groome PA, Irish J and O’Sullivan B. Towards further understanding of prognostic factors for head and neck cancer patients: the example of hypopharyngeal cancer. Laryngoscope. 2009; 119:696-702.
12. Homma A, Sakashita T, Oridate N, Suzuki F, Suzuki S, Hatakeyama H, Mizumachi T, Taki S and Fukuda S. Importance of comorbidity in hypopharyngeal cancer. Head Neck. 2010; 32:148-153.
13. Liu CT, Chiu TJ, Huang TL, Chien CY and Fang FM. Impact of comorbidity on survival for locally advanced head and neck cancer patients treated by radiotherapy or radiotherapy plus chemotherapy. Chang Gung Med J. 2010; 33:283-291.
14. Te HS and Jensen DM. Epidemiology of hepatitis B and C viruses: a global overview. Clin Liver Dis. 2010; 14:1-21, vii.
15. Piccirillo JF, Vlahiotis A, Barrett LB, Flood KL, Spitznagel EL and Steyerberg EW. The changing prevalence of comorbidity across the age spectrum. Crit Rev Oncol Hematol. 2008; 67:124-132.
16. Sanabria A, Carvalho AL, Vartanian JG, Magrin J, Ikeda MK and Kowalski LP. Comorbidity is a prognostic factor in elderly patients with head and neck cancer. Ann Surg Oncol. 2007; 14:1449-1457.
17. Ramakrishnan Y, Paleri V, Shah R, Steen IN, Wight RG and Kelly CG. Comorbidity in nasopharyngeal carcinoma: a preliminary communication on the prevalence, descriptive distribution and impact on outcome. Clin Otolaryngol. 2007; 32:484-488.
18. Reid BC, Alberg AJ, Klassen AC, Samet JM, Rozier RG, Garcia I and Winn DM. Comorbidity and survival of elderly head and neck carcinoma patients. Cancer. 2001; 92:2109-2116.
19. Wensing KU and Ciarimboli G. Saving ears and kidneys from cisplatin. Anticancer Res. 2013; 33:4183-4188.
20. Edge SB, FritzAG, Byrd DR, Greene FL, Compton CC, Trotti A, editors. AJCC cancer staging manual. New York: Springer; 2010. p. 41-56.
21. Charlson ME, Pompei P, Ales KL and MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987; 40:373-383.
22. Deyo RA, Cherkin DC and Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992; 45:613-619.
23. Paleri V and Wight RG. Applicability of the adult comorbidity evaluation - 27 and the Charlson indexes to assess comorbidity by notes extraction in a cohort of United Kingdom patients with head and neck cancer: a retrospective study. J Laryngol Otol. 2002; 116:200-205.
24. Zhao C, Han F, Lu LX, Huang SM, Lin CG, Deng XW, Lu TX and Cui NJ. Intensity modulated radiotherapy for local-regional advanced nasopharyngeal carcinoma. Ai Zheng. 2004; 23: 1532-1537
25. Li WF, Sun Y, Chen M, Tang LL, Liu LZ, Mao YP, Chen L, Zhou GQ, Li L and Ma J. Locoregional extension patterns of nasopharyngeal carcinoma and suggestions for clinical target volume delineation. Chin J Cancer. 2012; 31:579-587.
26. Liang SB, Sun Y, Liu LZ, Chen Y, Chen L, Mao YP, Tang LL, Tian L, Lin AH, Liu MZ, Li L and Ma J. Extension of local disease in nasopharyngeal carcinoma detected by magnetic resonance imaging: improvement of clinical target volume delineation. Int J Radiat Oncol Biol Phys. 2009; 75:742-750.