
INTRODUCTION
Diffuse gliomas are classified into astrocytomas, oligoastrocytomas and oligodendrogliomas of grade II, grade III and glioblastoma based on the 2007 World Health Organization (WHO) Classification of Tumors of the Central Nervous System [1]. Although patients with low grade gliomas (LGGs, grade II) [2] have a more favorable prognosis than patients with high grade gliomas (grade III and IV), in 50–75% of patients with low grade gliomas, the tumors grow continuously and tend to progress to a higher grade, leading to neurological disability and ultimately to death [3].
The mutations of IDH and ATRX occur in early stage of gliomagenesis and characterize specific subtypes of gliomas in adults [4, 5]. The majority of oncogenic IDH1 mutations are heterozygous missense mutations with a change of guanine to adenine at position 395 (G395A), leading to the replacement of arginine by histidine at codon 132 (IDH1-R132H) at the enzymatic active site [6, 7]. ATRX mutations or loss, companied by an alternative lengthening of telomeres (ALT) phenotype, impacted biological behaviors of astrocytic tumor cells, associated with favorable survival of patients with astrocytic tumors [8, 9].
According to the “ISN-Haarlem” consensus [10], the “integrated” diagnosis was recommended based on histology and stepwise analysis with initial immunohistochemistry for ATRX and IDH1-R132H followed by chromosome 1p/19q status analysis and IDH sequencing [11]. In this study, we collected 211 serial sampling of gliomas and detected ATRX and IDH1-R132H status in the progression of gliomas by immunohistochemistry. The result will help to evaluate the progressive pattern and time interval of patients with the initial gliomas using the reference histology combined with IDH1-R132H and ATRX status.
RESULTS
Frequency and diagnostic value of IDH1-R132H and ATRX loss in gliomas
To test the impact of IDH1-R132H and ATRX on routine diagnostic neuropathology and their evaluation for progression of gliomas, we analyzed a series of 211 serial sampling of glioma tissues, including 103 astrocytomas (A, AA), 25 oligodendrogliomas (O, AO), 123 oligoastrocytomas (OA, AOA) and 181 glioblastomas (pGBM, sGBM, rGBM) by immunohistochemistry for IDH1-R132H and ATRX evaluation.
IDH1-R132H staining positive and negative scoring was unequivocal. The majority of positive cases demonstrated a strong perinuclear cytoplasmic staining with additional weaker nuclear staining (Figure 1). In our series of 64 A II, 37 tumors were scored positive (57.81%, Figure 1A). There was an even higher rate of positive cases in OA II (40/49, 81.63%, Figure 1B) and O II (9/12, 75%, Figure 1C) labeled by H09. Rates for AA III, AOA III and AO III were also high, with 13 of 27 AA III (48.15%, Figure 1D), 38 of 68 AOA III (55.88%, Figure 1E) and 5 of 9 AO III (55.56%, Figure 1F) positive for H09. Among 114 pGBM, 17 positive cases were detected (14.91%, Figure 1G, 1H), while 40 of 59 sGBM (67.8%, Figure 1I) bound IDH1-R132H (Table 1, p = 0.009, Fisher’s exact test).
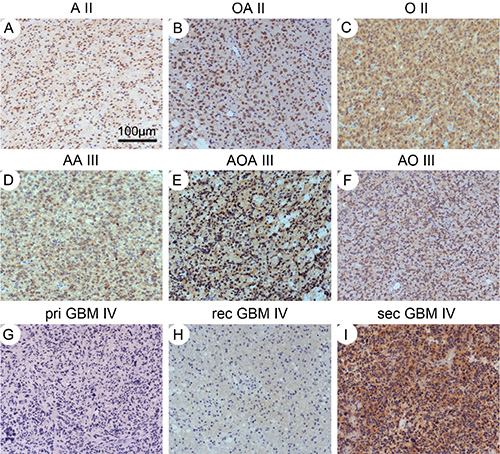
Figure 1: IHC staining for IDH1-R132H. Diffuse astrocytomas (A), oligoastrocytoma (B) and oligodendroglioma (C) with the IDH1-R132H positive tumor cells. Anaplastic astrocytomas (D), oligoastrocytoma (E) and oligodendroglioma (F) with the positive IDH1-R132Htumor cells. Primary (G) and recurrent glioblastoma (H) showed negative for H09, however, secondary glioblastoma showed the strongly positive tumor cells (I). Magnification: ×100.
Table 1: Frequency of IDH1-R132H and ATRX loss in gliomas
Histology |
IDH |
ATRX |
IDH_R132H+ATRX_loss |
||||||
|---|---|---|---|---|---|---|---|---|---|
total |
R132H |
frequency |
total |
loss |
frequency |
R132H |
loss |
frequency |
|
A |
64 |
37 |
57.81 |
64 |
49 |
76.56 |
37 |
34 |
91.89 |
AA |
27 |
13 |
48.15 |
27 |
21 |
77.78 |
13 |
10 |
76.92 |
O |
12 |
9 |
75.00 |
12 |
1 |
8.33 |
9 |
1 |
11.11 |
AO |
9 |
5 |
55.56 |
9 |
1 |
11.11 |
5 |
1 |
20.00 |
OA |
49 |
40 |
81.63 |
49 |
23 |
46.94 |
40 |
21 |
52.50 |
AOA |
68 |
38 |
55.88 |
68 |
20 |
29.41 |
38 |
15 |
39.47 |
pGBM |
114 |
17 |
14.91 |
114 |
14 |
12.28 |
17 |
5 |
29.41 |
sGBM |
59 |
40 |
67.80 |
59 |
45 |
76.27 |
40 |
36 |
90.00 |
Abbreviations: A, astrocytoma; AA, anaplastic astrocytoma; O, oligodendroglioma; AO, anaplastic oligodendroglioma; OA, oligoastrocytoma; AOA, anaplastic oligoastrocytoma; pGBM, primary glioblastoma; sGBM, secondary glioblastoma; IDH, isocitrate dehydrogenase, ATRX, alpha-thalassemia/mental retardation, X-linked.
ATRX immunohistochemistry was positive in 174 of 402 cases with a strong nuclear immune reaction in most cases (Figure 2). Loss of ATRX was evident in 228 of the 402 cases with the bulk of tumor cells negative for ATRX, whereas endothelia and infiltrating inflammatory cells as well as residual neurons retained ATRX expression. As reported earlier, the frequency of ATRX loss was higher in A, AA and sGBM (A, 49/64, 76.56%; AA, 21/27, 77.78%; sGBM, 45/59, 76.27%, Figure 2A, 2C, 2E) than in OA, AOA (OA, 23/49, 46.94%; AOA, 20/68, 29.41%) and low in O, AO and pGBM (O, 1/12, 8.33%; AO, 1/9, 11.11%; pGBM, 14/114, 12.28%, Table 1, p = 0.009, Fisher’s exact test). Our results revealed that IDH1-R132H dominated in grade II/III gliomas and secondary GBM. ATRX loss predominantly occurred in grade II/III astrocytoma and secondary GBM. These two events primarily co-occurred grade II/III astrocytoma and secondary GBM. In 30 cases, no immunoreaction in the entire tissue or specific patterns of immunoexpression in proximity to necrosis were observed, these cases were not scored and consequently not considered for statistical evaluation.
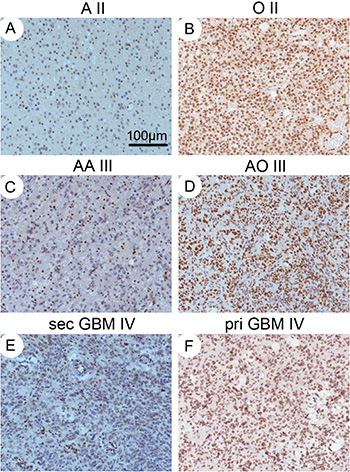
Figure 2: IHC staining for ATRX. Diffuse (A), anaplastic astrocytomas (C) and secondary glioblastoma (E) with loss of ATRX staining in tumor cell nuclei. Oligodendroglioma (B), anaplastic oligodendroglioma (D) and primary glioblastoma (F) with strong nuclear ATRX staining. The endothelial cells are always positive, serving as controls. Magnification: ×100.
Then we performed receiver operating characteristic (ROC) analysis to delineate the sensitivity and specificity of IDH1-R132H and (or) ATRX loss for WHO histology classification. As shown in Figure 3, the area under roc curve (AUC) of using IDH1-R132H as a diagnostic biomarker for discriminating between pGBM and grade II/III glioma, sGBM was 0.7414 (sensitivity 63.19%, specificity 85.09%, Figure 3A). The AUC of using ATRX loss as a diagnostic biomarker for discriminating between pGBM, oligodendroglioma (WHO grade II/III) and sGBM, astrocytoma (WHO grade II/III) was 0.8241 (sensitivity 76.67%, specificity 88.15%, Figure 3B). When combining IDH1-R132H with ATRX loss as diagnostic biomarkers for discriminating between pGBM, oligodendroglioma (WHO grade II/III) and sGBM, astrocytoma (WHO grade II/III), the AUC was 0.7407 (sensitivity 53.33%, specificity 94.815%, Figure 3C). We also performed ROC analysis for distinguishing primary and secondary GBMs using IDH1-R132H and (or) ATRX. When we just used IDH1-R132H status for ROC analysis, the AUC is 0.7644 (the sensitivity is 67.8%, the specificity is 85.09%, Figure 3D). When we just used ATRX loss status for ROC analysis, the AUC is 0.82 (the sensitivity is 87.72%, the specificity is 76.27%, Figure 3E). When we combined IDH1-R132H and ATRX loss status for ROC analysis, the AUC is 0.7832 (the sensitivity is 61.02%, the specificity is 95.61%, Figure 3F). These results indicated that IDH1-R132H and (or) ATRX loss status might have a good predictive ability for WHO histology diagnosis.
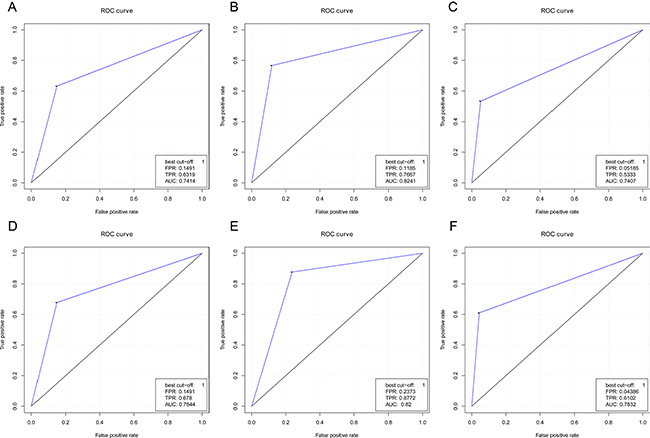
Figure 3: ROC curves of using IDH1-R132H and (or) ATRX status in discriminating the classification of glioma histology. The AUC of using IDH1-R132H as diagnostic biomarkers for discriminating between primary GBM and grade II/III glioma, secondary GBM is 0.7414 (the sensitivity is 63.19%, the specificity is 85.09%, (A). The AUC of using ATRX loss as diagnostic biomarkers for discriminating between primary GBM, oligodendroglioma (WHO grade II/III) and secondary GBM, astrocytoma (WHO grade II/III) is 0.8241 (the sensitivity is 76.67%, the specificity is 88.15%, (B). When IDH1-R132H combined with ATRX loss serves as diagnostic biomarkers for discriminating between astrocytoma (WHO grade II/III), secondary GBM, and primary GBM, oligodendroglioma (WHO grade II/III), the AUC is 0.7407 (the sensitivity is 53.33%, the specificity is 94.815%, (C).
Prognostic value of IDH1-R132H and ATRX loss in the evolution of gliomas
We analyzed the cohort of patients with primary and recurrent gliomas to observe the value of IDH1-R132H or ATRX as biomarkers evaluating the progression-free survival of patients with gliomas. In our cohort, we estimated the progression-free survival (PFS) in WHO grade II-IV patients and observed a remarkable separation (Median PFS of low grade gliomas, LGGs = 830 days, Median PFS of anaplastic gliomas, AGs = 495 days, Median PFS of GBMs = 394 days, p < 0.0001, log-rank test, Table 2).
Table 2: Analysis of the progression-free survival based on the WHO histology and grade of gliomas
Histology |
total |
Median PFS (days) |
1-year PFS survival rate |
2-year PFS survival rate |
3-year PFS survival rate |
4-year PFS survival rate |
5-year PFS survival rate |
p value |
|---|---|---|---|---|---|---|---|---|
LGG |
100 |
830 |
84 |
55 |
27 |
13 |
7 |
< 0.0001 |
pA |
50 |
693 |
82 |
50 |
28 |
14 |
8 |
|
pO |
9 |
721 |
67 |
44 |
22 |
22 |
11 |
|
pOA |
41 |
860 |
90 |
63 |
27 |
10 |
5 |
|
AG |
47 |
495 |
68 |
32 |
15 |
6 |
|
|
pAA |
10 |
611 |
70 |
50 |
20 |
10 |
|
|
pAO |
5 |
792 |
100 |
60 |
40 |
|
|
|
pAOA |
32 |
398 |
63 |
22 |
9 |
6 |
|
|
pGBM |
64 |
394 |
52 |
16 |
6 |
2 |
2 |
Abbreviations: WHO, World Health Organization; PFS, progression-free survival; LGG, low grade glioma; pA, primary astrocytoma; pO, primary oligodendroglioma; pOA, primary oligoastrocytoma; AG, anaplastic glioma; pAA, primary anaplastic astrocytoma; pAO, primary anaplastic oligodendroglioma; pAOA, primary anaplastic oligoastrocytoma; pGBM, primary glioblastoma.
PFS was significantly longer in patients with grade II gliomas harboring IDH1-R132H than in patients with IDH1 wild-type tumors (Median PFS of IDH1-R132H = 893 days, Median PFS of IDH1-wt = 580 days, p = 0.0009, log-rank test; Figure 4A). Although PFS was longer in patients with AG or pGBM harboring IDH1-mutated tumors than in patients with IDH1 wild-type tumors, this difference was not significant (p = 0.0702 and p = 0.0914, respectively, log-rank test; Figure 4B, 4C). Although there was no significant difference between ATRX loss and ATRX expression in the cohort of patients with grade II or grade III tumors (Figure 5A, 5B), ATRX loss was associated with longer progression-free survival in patients with grade II/III oligoastrocytomas or grade II/III gliomas (Figure 5C, 5D). Patients with astrocytic tumors losing ATRX had a longer progression-free survival than patients with tumors expressing ATRX (Figure 5E). In additions, there was a trend that patients with IDH1-R132H and ATRX loss grade II/III gliomas had longer PFS than patients with IDH1-R132H and ATRX positive grade II/III gliomas and PFS of patients with GBM was similar to that of patients with IDH wild type (Figure 5F). We have demonstrated the basic clinical characteristics among the IDH-R132H/ATRXloss, IDH-R132H/ATRXexpr, IDH-WT and GBM groups in the Supplementary Table1. After incorporation of age, WHO grade, IDH1 and ATRX status into the multivariate model, the prognostic value of IDH1-R132H was still significant (Table 3).
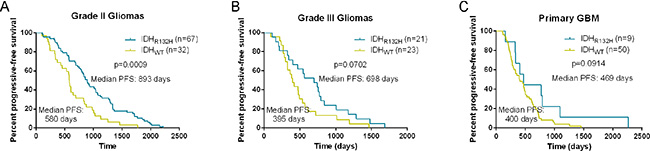
Figure 4: Kaplan-Meier analysis of progression-free survival in patients with IDH1-R132H and not. Progression-free survival was significantly longer in patients with grade II gliomas harboring IDH1-R132H than in patients with IDH1 wild-type tumors (A). Although PFS was longer in patients with anaplastic gliomas or primary GBM harboring IDH1-mutated tumors than in patients with IDH1 wild-type tumors, this difference was not significant (B) and (C).
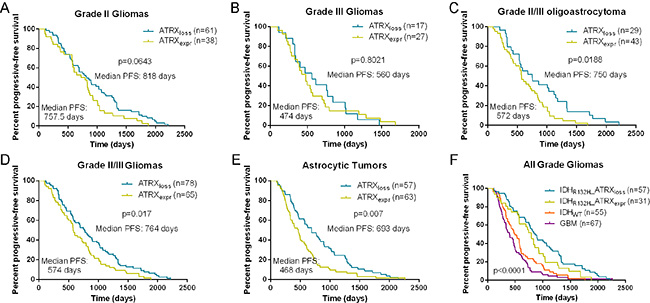
Figure 5: Kaplan-Meier analysis of progression-free survival in patients with ATRX protein loss and expression. In the cohort of patients with grade II or grade III tumors (A) and (B), patients with ATRX loss had a trend for longer PFS compared with those with ATRX expression. ATRX loss was associated with longer progression-free survival in patients with grade II/III oligoastrocytomas or grade II/III gliomas (C) and (D). Patients with astrocytic tumors losing ATRX had a longer progression-free survival than patients with tumors expressing ATRX (E). In additions, there was a trend that patients with IDH1-R132H and ATRX loss grade II/III gliomas had longer PFS than patients with IDH1-R132H and ATRX positive grade II/III gliomas and PFS of patients with GBM was similar to that of patients with IDH wild type (F).
Table 3: Cox regression analysis for the progression-free survival of patients with gliomas
|
Univariate Cox Model |
Mutivariate Cox Model |
||||
|---|---|---|---|---|---|---|
|
Hazard ratio |
95%CI |
p value |
Hazard ratio |
95%CI |
p value |
Age ≤ 45 vs. > 45 |
0.703 |
0.523–0.946 |
0.02 |
0.89 |
0.509–1.03 |
0.474 |
Male vs. Female |
0.906 |
0.686–1.197 |
0.488 |
|
|
|
Astrocytic vs. oligodendroglial |
1.123 |
0.849–1.486 |
0.417 |
|
|
|
IDH1-R132H positive vs. negative |
0.437 |
0.326–0.586 |
3.15E–08 |
0.517 |
0.369–0.723 |
1.19E–04 |
ATRX loss vs. expression |
0.645 |
0.486–0.856 |
0.002 |
0.913 |
0.659–1.264 |
0.584 |
WHO grade II/III vs. IV |
0.529 |
0.388–0.772 |
5.79E–05 |
0.724 |
0.509–1.030 |
0.072 |
Abbreviations: WHO, World Health Organization; PFS, progression-free survival; LGG, low grade glioma; pA, primary astrocytoma; pO, primary oligodendroglioma; pOA, primary oligoastrocytoma; AG, anaplastic glioma; pAA, primary anaplastic astrocytoma; pAO, primary anaplastic oligodendroglioma; pAOA, primary anaplastic oligoastrocytoma; pGBM, primary glioblastoma; IDH, isocitrate dehydrogenase, ATRX, alpha-thalassemia/mental retardation, X-linked.
IDH1-R132H and ATRX loss in matched primary and recurrent gliomas
First, we excluded these pairs that the primary gliomas were high grade tumor while the recurrence was lower grade tumor and then analyzed the pattern of glioma progression. As shown in Table 4, the recurrent tumors of primary LGGs included LGGs, AGs and GBMs of which rates corresponded to 29% (29/100), 35% (35/100) and 36% (36/100), respectively. The time interval of the three progressive patterns was analyzed. There was no difference in the progression-free survival when LGG malignantly recurred to LGG, AG or GBM (Median PFS = 802 days, 830 days and 835 days, respectively, Figure 6A). However, the time interval of AG to GBM was significantly shorter than that of AG to AG (Median PFS = 365 days and 611 days, respectively, p = 0.0067, log-rank test). The progressive time interval of GBM to GBM was similar to that of AG to GBM (Median PFS = 395 days, p = 0.8446, Figure 6B). IDH1-R132H occurred stably in the primary tumors and matched recurrent tumors, although not all the recurrent tumors showed consistent IDH1-R132H status as the corresponding primary tumors (Table 4). Because there was a too high or too low frequency of ATRX loss occurrence in the astrocytoma (WHO II/III) or oligodendroglioma (WHO II/III) and pGBM, the rate of ATRX loss was not observed between primary and matched recurrent tumors. After combining the IDH1-R132H and ATRX loss status, we also illustrated that most recurrences had a consistent IDH1 and ATRX status with their primary tumors (IDH1-R132H/ATRXloss: 43/59, 74.1%, p < 0.0001; IDH1-R132H/ATRXexpr: 18/36, 50%, p < 0.0001; IDH-WT: 77/102, 75.5%, p < 0.0001, Table 5).
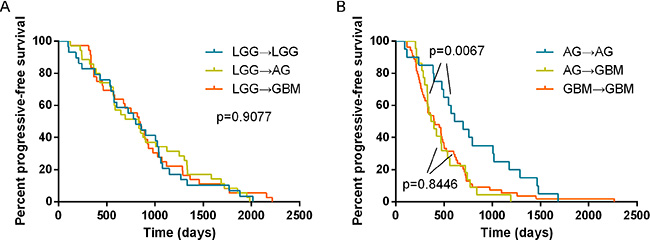
Figure 6: Analysis of the progression-free survival based on the different evolution patterns of gliomas. There was no difference in the progression-free survival when LGG malignantly recurred to LGG, AG or GBM (Median PFS = 802 days, 830 days and 835 days, respectively, (A). However, the time interval of AG to GBM was significantly shorter than that of AG to AG (Median PFS = 365 days and 611 days, respectively, p = 0.0067, log-rank test). The progressive time interval of GBM to GBM was similar to that of AG to GBM (Median PFS = 395 days, p = 0.8446, (B).
Table 4: Analysis of the progression-free survival based on the different evolution patterns of gliomas
Histology |
total |
Median PFS (days) |
IDH status in initial tumors |
IDH status in relapse tumors |
p value |
|---|---|---|---|---|---|
LGG→LGG |
29 |
802 |
20/27 |
20/28 |
|
LGG→AG |
35 |
830 |
20/34 |
21/34 |
|
LGG→GBM |
36 |
835 |
26/35 |
28/35 |
|
AG→AG |
20 |
611 |
10/20 |
12/20 |
0.0067 |
AG→GBM |
22 |
365 |
10/22 |
10/22 |
|
GBM→GBM |
54 |
395 |
8/53 |
8/52 |
|
Abbreviations: PFS, progression-free survival; LGG, low grade glioma; AG, anaplastic glioma; GBM, glioblastoma; IDH, isocitrate dehydrogenase, ATRX, alpha-thalassemia/mental retardation, X-linked.
Table 5: Frequency of IDH1-R132H and ATRX loss in matched primary and recurrent gliomas
Initial tumors |
total |
Median PFS (days) |
Recurrent tumors |
p value |
|||
|---|---|---|---|---|---|---|---|
IDHmut |
IDHwt |
IDHmut_ATRXloss |
IDHmut_ATRXexpr |
||||
IDHmut_ATRXloss |
59 |
839 |
78 (82%) |
17 |
43 (74.1%) |
8 |
< 0.0001 |
IDHmut_ATRXexpr |
36 |
770 |
8 |
18 (50%) |
< 0.0001 |
||
IDHwt |
102 |
455 |
25 |
77 (75.5%) |
12 |
13 |
< 0.0001 |
Abbreviations: mut, mutation; wt, wild type; expr, expression; IDH, isocitrate dehydrogenase, ATRX, alpha-thalassemia/mental retardation, X-linked.
Progressive pattern of primary glioma with or without IDH1-R132H
Generally, diffuse LGGs malignantly transformed into AGs, followed by secondary GBM, but occasionally, there might be no evidence of the former one. Meanwhile, some recurrences had different morphology from initial tumors (astrocytic to oligodendroglial and vice versa). In our cohort, we discriminated the IDH1-R132H initial tumors from the IDH1-WT tumors and analyzed the evolution pattern of 125 primary-recurrent paired tumors, 49 recurrences of which were originated from grade II A (Figure 7A), 47 were from grade II O (Figure 7B) and 29 were grade III AOA (Figure 7C). We observed that regardless of with or without IDH1-R132H, the histology of recurrences from initial grade II A could be sGBM, AOA and AA. Although with the similar evolution pattern, patients with IDH1-R132H grade II A had a longer progressive time interval compared with patients with IDH1-WT grade II A (Median PFS = 895 days, Median PFS = 574 days, respectively, p = 0.0096, Figure 7D). Recurrences from IDH1-R132H grade II O mainly showed sGBM, OA morphology. In contrast, there were no main histology characteristics in the recurrences from the initial IDH1-WT grade II O. Patients with IDH1-R132H grade II O had a longer progression-free survival than patients with IDH1-WT grade II O (Median PFS = 858.5 days, Median PFS = 605 days, respectively, p = 0.0325, Figure 7E). GBM and AOA were the main recurrent histology from primary AOA. However, most of relapses from IDH1-R132H AOA were recurrent AOA; most of relapses from IDH1-WT AOA were sGBM. Patients with IDH1-R132H AOA also had a longer progression-free survival than patients with IDH1-WT ones (Median PFS = 629 days, Median PFS = 328 days, respectively, p = 0.0037, Figure 7F).
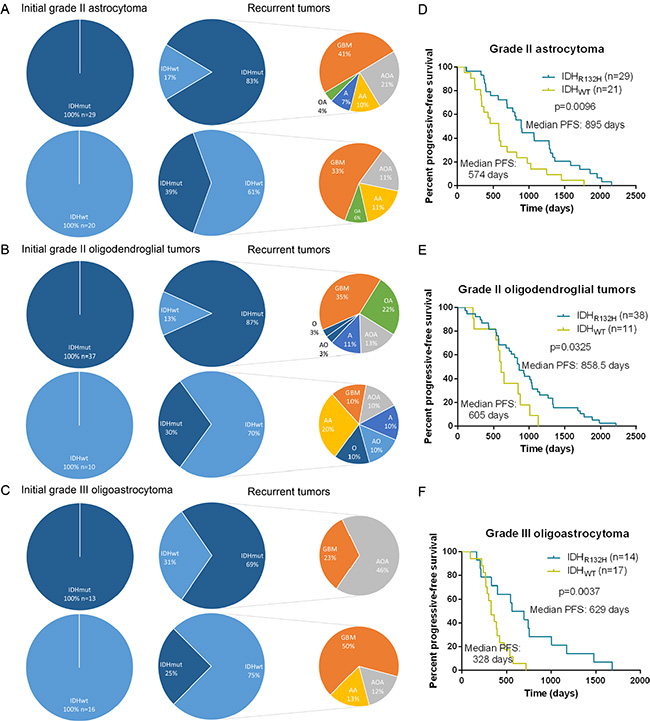
Figure 7: Progressive pattern of primary glioma with or without IDH1-R132H. Recurrences from initial grade II astrocytomas always referred to secondary GBM, anaplastic oligoastrocytomas and anaplastic astrocytomas regardless of with or without IDH1-R132H (A). Recurrences from IDH1-R132H grade II oligodendroglial tumors mainly showed secondary glioblastomas, oligoastrocytomas morphology. In contrast, there were no main histology characteristics in the recurrences from the initial IDH1-WT grade II oligodendroglial tumors (B). Glioblastomas and anaplastic oligoastrocytomas were occupied on the most percentage of relapses from primary anaplastic oligoastrocytomas. However, most of relapses from IDH1-R132H AOA were recurrent anaplastic oligoastrocytomas; most of relapses from IDH1-WT AOA were secondary GBM (C). Patients with IDH1-R132H tumors had a longer progression-free survival than patients with IDH1-WT tumors, irrespective of histology (D, E and F).
DISCUSSION
It is accepted that IDH mutation and ATRX mutation were used as diagnostic and prognostic biomarkers for molecular classification of gliomas [12, 13]. However, their prognostic value for glioma progression is not clear, especially ATRX loss.
In our study, we used immunohistochemistry to detect IDH1-R132H and ATRX status instead of sequencing, aiming to provide a mature and simple tool for clinical practice. In the light of the “ISN-Haarlem” consensus, the routine approach to all diffuse astrocytic and oligodendroglial gliomas begins with performing IHC for ATRX and IDH1-R132H expression. Our results showed that the IDH1-R132H and (or) ATRX loss status could be necessary to provide the basic molecular information for the “integrated diagnosis” of gliomas.
IDH mutation is thought to be an early if not the initial event in the development of low-grade astrocytomas and oligodendrogliomas. In support of this hypothesis, IDH mutation is found in secondary glioblastomas but rare in primary glioblastomas [6]. IDH1 mutations have been shown to alter the enzymatic activity of the encoded protein, leading to up-regulation of hypoxia inducible factor-1α (HIF-1α) [14, 15]. HIF-1α plays an important role in the process of angiogenesis while also supporting tumor cell survival and proliferation [14, 16]. Although the properties of the IDH1 mutation would promote tumor growth, IDH mutation commonly indicates a favorable prognosis independent of WHO grades [7, 17–19].
Mutations and loss of expression of alphathalassemia/mental retardation syndrome X-linked (ATRX) was first reported in pancreatic neuroendocrine tumors [20]. ATRX protein plays a variety of key roles at tandem repeat sequences within the genome, including prevention of replication fork stalling, the deposition of a histone variant, and the suppression of a homologous recombination-based pathway of telomere maintenance [9]. Recently, mutation/loss of ATRX was identified as a potent biomarker in grade II-III gliomas and was associated with recurrent ones [21]. ATRX gene mutations were significantly correlated with ALT positivity [22]. Loss of ATRX in ALT frees macroH2A1.1 to bind and sequester tankyrase 1, thereby preventing resolution of sister telomere cohesion. Forced resolution of sister telomere cohesion induces excessive recombination between non-homologs, genomic instability, and impaired cell growth, indicating the ATRX-macroH2A1. 1-tankyrase axis as a potential therapeutic target in ALT tumors [23]. Inhibition of the protein kinase ATR, a critical regulator of recombination recruited by RPA, disrupts ALT and triggers chromosome fragmentation and apoptosis in ALT cells. The cell death induced by ATR inhibitors is highly selective for cancer cells that rely on ALT, suggesting that such inhibitors may be useful for treatment of ALT-positive cancers [24]. In patients with 1p/19q noncodeleted tumors with IDH mutations, those who were ATRX positive might have benefitted more than those who were negative from pre-RT PCV [25]. Whether these noncodeleted ATRX-positive tumors are biologically identical to codeleted tumors, save for absence of visible loss of 1p/19q, or represent laboratory errors in codeletion testing is unknown.
We previously reported that reduced expression of ATRX inhibited the migration, promoted apoptosis and reduced proliferation of glioma cells, suggesting the important role of ATRX in gliomas. Similarly, a report depicted how loss of ATRX could affect neuroprogenitor cell apoptosis [26].
IDH1-R132H and ATRX expression status are essential to the diagnosis for gliomas. IDH1/2 mutations dominate in WHO grade II/III gliomas (also called as lower grade gliomas) and secondary GBM. According to several studies, IDH1–R132H (G395A) is the most common mutation (90%). The NOA-04 trial also showed that ATRX status and IDH1-R132H might be initially detected for the “integrated decision” in the further [11]. In addition, oligodendrogliomas have the 1p/19q codeletion and TERT promoter mutations phenotype, while TP53 and ATRX mutations predominantly occur in grade II/III astrocytoma and secondary GBM. Maybe, oligoastrocytomas (WHO grade II/III) may be separated into two groups, genetically matching oligodendroglioma on one and astrocytoma on the other side based on the molecular information, for example, IDH1/2, 1p/19q and ATRX and so on [27, 28]. The frequency of IDH mutations is rare in primary GBMs that have TERT promoter mutations, EGFR alteration and PTEN loss. Yao et al. analyzed IDH1 and IDH2 status at codon 132 of IDH1 and codon 172 of IDH2 by direct sequencing and anti-IDH1-R132H immunohistochemistry in 53 paired samples and their recurrences [29]. We also found that IDH1-R132H and ATRX expression status of the recurrent tumor was most consistent with that of their initial tumor and that IDH1-R132H positive gliomas had a significantly longer progression-free survival (PFS). In addition, our cohort contained a larger sample size, thus, we assessed the diagnosis value IDH1-R132H and (or) ATRX status for human gliomas and observed that the progressive pattern of gliomas based on the precious cohort [2, 11, 30–32]. The “Haarlem Consensus Guidelines for Nervous System Tumor Classification” [10] suggest that some entities will require molecular information to provide an “integrated” diagnosis, which is based on several layers comprising (i) the integrated diagnosis as top layer, followed by (ii) histological classification, (iii) WHO grade, and (iv) molecular information. In the present study, for the first time to our knowledge, we illustrated an evaluation formula for the evolution of gliomas by IDH1-R132H combined with ATRX immunohistochemistry and identified the association between IDH1-R132H/ATRX loss and longer progression time interval of gliomas. In addition, we also observed that most recurrences had a consistent IDH1 and ATRX status with their matched primary tumors and demonstrated the progressive pattern of grade II astrocytoma/oligodendroglial tumors and anaplastic oligoastrocytoma with or without IDH1-R132H.
MATERIALS AND METHODS
Patients and samples
211 serial sampling of glioma pairs were obtained from the Chinese Glioma Genome Atlas (CGGA), including 202 patients with primary and the first recurrent tumors, 8 patients with primary and two times recurrent tumors and 1 patient with primary and three times recurrent tumors. Tumor tissue samples were obtained by surgical resection during January 2008 through March 2015. The histological diagnoses were confirmed by two neuropathologists according to the 2007 World Health Organization (WHO) classification guidelines [1]. The distinction between primary and secondary GBM was based on the presence of prior specimens showing lower grade gliomas. All patients provided written informed consent, and the study was approved by the ethics committees of the participating hospitals. Patients’ progression-free survival data were recorded when the relapse occurred. Patients who underwent biopsy alone or lost follow-up were excluded from the survival analysis.
Immunohistochemistry for IDH1-R132H and ATRX
Immunostaining was performed according to the manufacturer’s protocol. In brief, formalin-fixed, paraffin-embedded tissue sections cut to four micrometer were dried at 80°C for 15 min and dewaxed in xylene, rinsed in graded ethanol, and rehydrated in double-distilled water. The sections were then treated with 3% H2O2 for 5 min at room temperature (RT) to block endogenous peroxidase activity. For antigen retrieval, slides were pretreated by steaming in sodium citrate buffer (10 mM sodium citrate, pH 6.0) for 15 min at 100°C. After washing with phosphate-buffered saline for 3 min, the sections were immunostained with an anti-human IDH1-R132H antibody (at 1:60 dilution, H09, Dianova, Hamburg, Germany) or an anti-human ATRX antibody (at 1:800 dilution, ab97508, Abcam), and incubated at 4°C over night. After washed by 3 changes of PBS buffer, the tissues were covered by anti-mouse/rabbit polymer HRP-label for 30 min at RT. Staining reaction was performed through covering tissue by prepared DAB chromogen solution, and incubating approximately for 10 min to allow for proper brown color development. Standard of IDH1-R312H staining: (1) a strong cytoplasmic immunoreaction product was scored positive; (2) a weak diffuse staining and staining of macrophages were not scored positive [33]. Standard of ATRX staining according to German Cancer Research Center (DKFZ) [11]: nuclear ATRX loss was scored as specific if tumor cell nuclei were unstained while nuclei of non-neoplastic cells such as endothelia, microglia, lymphocytes and reactive astrocytes were strongly positive.
Statistical analysis
Receiver operating characteristic (ROC) curves were constructed to determine the discriminatory capacity of IDH1-R132H and (or) ATRX loss for diagnosis. Kaplan-Meier analysis was performed to estimate the survival time of different subgroups and a log-rank test was used to test prognostic differences. Comparisons of binary and categorical patient characteristics between subgroups were performed by the use of the Fisher’s exact test All statistical computations were performed with the statistical software environment R version 3.2.0 (http://www.r-project.org/), GraphPad Prism Version 6.01 or Microsoft Excel 2013. P value < 0.05 was considered statistically significant.
ACKNOWLEDGMENTS AND FUNDING
We thank Yuling Yang for tissue sample collection and clinical data retrieval. Grant Support: 1. The Research Special Fund For Public Welfare Industry of Heath (No. 201402008); 2. National Natural Science Foundation of China (No. 91229121, No. 81201993, No. 81572701, No. 81502606, No. 81502495, No. 81502404, No. 81502494, No. 81501603, No. 81402053); 3. Beijing Science and Technology Plan (No.Z131100006113018); 4. National Key Technology Research and Development Program of the Ministry of Science and Technology of China (No. 2013BAI09B03); 5. National High Technology Research and Development Program (863) (No. 2012AA02A508); 6. Special Fund Project of Translational Medicine in the Chinese-Russian Medical Research Center (No. CR201417); 7. Research Project of Chinese Society of Neuro-oncology, CACA (CSNO-2014-MSD08); 8. Natural and Science Foundation of Heilongjiang Province (H201399); 9. Science and technology research project of Education Department of Heilongjiang Province (12511254).
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
1. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauer BW, Kleihues P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathologica. 2007; 114:97–109.
2. Cancer Genome Atlas Research N. Comprehensive, Integrative Genomic Analysis of Diffuse Lower-Grade Gliomas. The New England journal of medicine. 2015.
3. Chaichana KL, McGirt MJ, Laterra J, Olivi A, Quinones-Hinojosa A. Recurrence and malignant degeneration after resection of adult hemispheric low-grade gliomas. Journal of neurosurgery. 2010; 112:10–17.
4. Watanabe T, Nobusawa S, Kleihues P, Ohgaki H. IDH1 mutations are early events in the development of astrocytomas and oligodendrogliomas. The American journal of pathology. 2009; 174:1149–1153.
5. Jiao Y, Killela PJ, Reitman ZJ, Rasheed AB, Heaphy CM, de Wilde RF, Rodriguez FJ, Rosemberg S, Oba-Shinjo SM, Nagahashi Marie SK, Bettegowda C, Agrawal N, Lipp E, et al. Frequent ATRX, CIC, FUBP1 and IDH1 mutations refine the classification of malignant gliomas. Oncotarget. 2012; 3:709–722. doi: 10.18632/oncotarget.588.
6. Turkalp Z, Karamchandani J, Das S. IDH Mutation in Glioma: New Insights and Promises for the Future. JAMA neurology. 2014.
7. Cai J, Yang P, Zhang C, Zhang W, Liu Y, Bao Z, Liu X, Du W, Wang H, Jiang T, Jiang C. ATRX mRNA expression combined with IDH1/2 mutational status and Ki-67 expression refines the molecular classification of astrocytic tumors: evidence from the whole transcriptome sequencing of 169 samples samples. Oncotarget. 2014; doi: 10.18632/oncotarget.1838.
8. Napier CE, Huschtscha LI, Harvey A, Bower K, Noble JR, Hendrickson EA, Reddel RR. ATRX represses alternative lengthening of telomeres. Oncotarget. 2015; 6:16543–16558. doi: 10.18632/oncotarget.3846.
9. Cai J, Chen J, Zhang W, Yang P, Zhang C, Li M, Yao K, Wang H, Li Q, Jiang C, Jiang T. Loss of ATRX, associated with DNA methylation pattern of chromosome end, impacted biological behaviors of astrocytic tumors. Oncotarget. 2015; 6:18105–18115. doi: 10.18632/oncotarget.3906.
10. Louis DN, Perry A, Burger P, Ellison DW, Reifenberger G, von Deimling A, Aldape K, Brat D, Collins VP, Eberhart C, Figarella-Branger D, Fuller GN, Giangaspero F, et al. International Society Of Neuropathology–Haarlem consensus guidelines for nervous system tumor classification and grading. Brain pathology (Zurich, Switzerland). 2014; 24:429–435.
11. Reuss DE, Sahm F, Schrimpf D, Wiestler B, Capper D, Koelsche C, Schweizer L, Korshunov A, Jones DT, Hovestadt V, Mittelbronn M, Schittenhelm J, Herold-Mende C, et al. ATRX and IDH1-R132H immunohistochemistry with subsequent copy number analysis and IDH sequencing as a basis for an “integrated” diagnostic approach for adult astrocytoma, oligodendroglioma and glioblastoma. Acta Neuropathol. 2015; 129:133–146.
12. Wiestler B, Capper D, Holland-Letz T, Korshunov A, von Deimling A, Pfister SM, Platten M, Weller M, Wick W. ATRX loss refines the classification of anaplastic gliomas and identifies a subgroup of IDH mutant astrocytic tumors with better prognosis. Acta Neuropathol. 2013; 126:443–451.
13. Killela PJ, Pirozzi CJ, Healy P, Reitman ZJ, Lipp E, Rasheed BA, Yang R, Diplas BH, Wang Z, Greer PK, Zhu H, Wang CY, Carpenter AB, et al. Mutations in IDH1, IDH2, and in the TERT promoter define clinically distinct subgroups of adult malignant gliomas. Oncotarget. 2014; doi: 10.18632/oncotarget.1765.
14. Lv S, Teugels E, Sadones J, Quartier E, Huylebrouck M, S DUF, M LEM, O DEW, Salmon I, Michotte A, J DEG, Neyns B. Correlation between IDH1 gene mutation status and survival of patients treated for recurrent glioma. Anticancer research. 2011; 31:4457–4463.
15. Zhao S, Lin Y, Xu W, Jiang W, Zha Z, Wang P, Yu W, Li Z, Gong L, Peng Y, Ding J, Lei Q, Guan KL, et al. Glioma-derived mutations in IDH1 dominantly inhibit IDH1 catalytic activity and induce HIF-1alpha. Science. 2009; 324:261–265.
16. Marsh J, Mukherjee P, Seyfried TN. Akt-dependent proapoptotic effects of dietary restriction on late-stage management of a phosphatase and tensin homologue/tuberous sclerosis complex 2-deficient mouse astrocytoma. Clinical cancer research. 2008; 14:7751–7762.
17. Zhang CB, Bao ZS, Wang HJ, Yan W, Liu YW, Li MY, Zhang W, Chen L, Jiang T. Correlation of IDH1/2 mutation with clinicopathologic factors and prognosis in anaplastic gliomas: a report of 203 patients from China. J Cancer Res Clin Oncol. 2013.
18. Li MY, Wang YY, Cai JQ, Zhang CB, Wang KY, Cheng W, Liu YW, Zhang W, Jiang T. Isocitrate dehydrogenase 1 Gene Mutation Is Associated with Prognosis in Clinical Low-Grade Gliomas. PLoS One. 2015; 10:e0130872.
19. Xia L, Wu B, Fu Z, Feng F, Qiao E, Li Q, Sun C, Ge M. Prognostic role of IDH mutations in gliomas: a meta-analysis of 55 observational studies. Oncotarget. 2015; 6:17354–17365. doi: 10.18632/oncotarget.4008.
20. Jiao Y, Shi C, Edil BH, de Wilde RF, Klimstra DS, Maitra A, Schulick RD, Tang LH, Wolfgang CL, Choti MA, Velculescu VE, Diaz LA, Jr., et al. DAXX/ATRX, MEN1, and mTOR pathway genes are frequently altered in pancreatic neuroendocrine tumors. Science. 2011; 331:1199–1203.
21. E B. Mutational Analysis Reveals the Origin and Therapy-Driven Evolution of Recurrent Glioma. Science. 2013.
22. Heaphy CM, de Wilde RF, Jiao Y, Klein AP, Edil BH, Shi C, Bettegowda C, Rodriguez FJ, Eberhart CG, Hebbar S, Offerhaus GJ, McLendon R, Rasheed BA, et al. Altered telomeres in tumors with ATRX and DAXX mutations. Science. 2011; 333:425.
23. Ramamoorthy M, Smith S. Loss of ATRX Suppresses Resolution of Telomere Cohesion to Control Recombination in ALT Cancer Cells. Cancer Cell. 2015; 28:357–369.
24. Flynn RL, Cox KE, Jeitany M, Wakimoto H, Bryll AR, Ganem NJ, Bersani F, Pineda JR, Suva ML, Benes CH, Haber DA, Boussin FD, Zou L. Alternative lengthening of telomeres renders cancer cells hypersensitive to ATR inhibitors. Science. 2015; 347:273–277.
25. Cairncross JG, Wang M, Jenkins RB, Shaw EG, Giannini C, Brachman DG, Buckner JC, Fink KL, Souhami L, Laperriere NJ, Huse JT, Mehta MP, Curran WJ, Jr. Benefit from procarbazine, lomustine, and vincristine in oligodendroglial tumors is associated with mutation of IDH. Journal of clinical oncology. 2014; 32:783–790.
26. Iwase S, Xiang B, Ghosh S, Ren T, Lewis PW, Cochrane JC, Allis CD, Picketts DJ, Patel DJ, Li H, Shi Y. ATRX ADD domain links an atypical histone methylation recognition mechanism to human mental-retardation syndrome. Nature structural & molecular biology. 2011; 18:769–776.
27. Huse JT, Diamond EL, Wang L, Rosenblum MK. Mixed glioma with molecular features of composite oligodendroglioma and astrocytoma: a true “oligoastrocytoma”? Acta Neuropathol. 2015; 129:151–153.
28. Sahm F, Reuss D, Koelsche C, Capper D, Schittenhelm J, Heim S, Jones DT, Pfister SM, Herold-Mende C, Wick W, Mueller W, Hartmann C, Paulus W, et al. Farewell to oligoastrocytoma: in situ molecular genetics favor classification as either oligodendroglioma or astrocytoma. Acta Neuropathol. 2014; 128:551–559.
29. Mutation Analysis of IDH1 in Paired Gliomas Revealed IDH1 Mutation Was Not Associated with Malignant Progression but Predicted Longer Survival. plos one. 2013.
30. Eckel-Passow JE, Lachance DH, Molinaro AM, Walsh KM, Decker PA, Sicotte H, Pekmezci M, Rice T, Kosel ML, Smirnov IV, Sarkar G, Caron AA, Kollmeyer TM, et al. Glioma Groups Based on 1p/19q, IDH, and TERT Promoter Mutations in Tumors. The New England journal of medicine. 2015.
31. Suzuki H, Aoki K, Chiba K, Sato Y, Shiozawa Y, Shiraishi Y, Shimamura T, Niida A, Motomura K, Ohka F, Yamamoto T, Tanahashi K, Ranjit M, et al. Mutational landscape and clonal architecture in grade II and III gliomas. Nat Genet. 2015.
32. Leeper HE, Caron AA, Decker PA, Jenkins RB, Lachance DH, Giannini C. IDH mutation, 1p19q codeletion and ATRX loss in WHO grade II gliomas. Oncotarget. 2015; doi: 10.18632/oncotarget.4497.
33. Capper D, Weissert S, Balss J, Habel A, Meyer J, Jager D, Ackermann U, Tessmer C, Korshunov A, Zentgraf H, Hartmann C, von Deimling A. Characterization of R132H mutation-specific IDH1 antibody binding in brain tumors. Brain pathology (Zurich, Switzerland). 2010; 20:245–254.