
Introduction
Current guidelines suggest the use of Evans’ index [EI] as a marker for radiological diagnosis of hydrocephalus [1, 2]. EI is based on pneumoencephalographic findings for pediatric hydrocephalus reported in the early 1940s [3], and is calculated by dividing the maximum width of the frontal horns by the maximum width of the inner table of the cranium at the level of Monro’s foramens in the frontal horns. EI values >0.30 are considered indicative of hydrocephalus. Subsequent studies employing CT confirmed the diagnostic reliability of EI [4, 5].
Advanced neuroimaging techniques indicate that measuring ventricular volume is the best strategy for evaluating hydrocephalus [6, 7]. Unfortunately, this measure is complex and is not readily available in most resource-limited settings, thereby being of little use for daily, routine quantitation of ventricular size.
An easy-to-use, accessible, cost-effective, reliable tool for defining ventricular size in normal aging or neurological conditions would be extremely useful in clinical practice. We therefore designed this transversal radiological study to assess the reliability of Evans’ index (EI) as a radiological marker of abnormal ventricular enlargement (values >0.30) during aging, independently from eventually associated neurological conditions, in a large series of consecutive head scans from an emergency department (ED).
Results
Out of 1650 examined CT scans, 1221 were eligible for EI calculation (mean±SD EI value, 0.27±0.04). Scans came from 656 women (53.7%, aged 75.5±15.0 years) and 565 men (46.3%, aged 71.3±13.2 years; entire study population, 73.6±14.4 years). EI was significantly greater in men (0.28±0.04) than in women (0.27±0.04; p<0.01, Student’s t-test). EI increased with age in a similar fashion in both sexes (linear regression coefficient = 0.001, p<0.001; Figure 1). Kappa value of 0.86 indicated “almost perfect agreement” between observers in calculating EI.
EI values >0.30 were calculated for 236 scans (19.3%; EI 0.33±0.02; 121 men [21.4%], 115 women [17.5%]; p=0.036, chi-squared test). Multiple logistic regression analysis demonstrated that the risk of having an EI value >0.30 increased by 7.8% per year of age (p<0.001) and that males were at 83.9% greater risk than females (p<0.001). Stratified analysis of one-year cohorts showed that the mean EI value per class was invariably <0.30 (Figure 1).
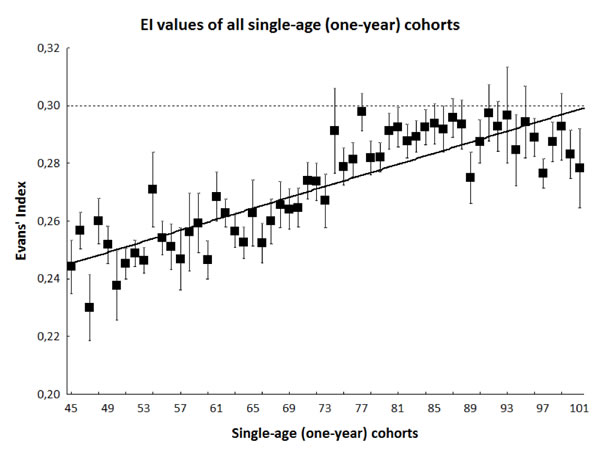
Figure 1: Black squares and bars indicate mean ± SE values of EI in each single-age (one-year) cohort. Continuous line indicates linear regression. Dashed line indicates the cut-off value of EI.
Discussion
This transversal radiological study of consecutive ED head CT scans provides evidence that roughly one out five CT scans is associated with EI values >0.30 and that EI values increase with age. Here, the mean EI values of all one-year cohorts were <0.30. Therefore an EI value ≥ 0.30 denotes an abnormally enlarged ventricular system, although it does not specify whether the enlargement relates to loss of brain volume (i.e. atrophy) or disturbance in cerebrospinal fluid dynamics.
In healthy elderly individuals, neuroimaging often shows evidence of both brain atrophy and ventricular enlargement [8-12]. When ventricular enlargement is measured through Evans’ index, MRI studies on normal elderly subjects show an EI >0.30 from 2.8 to 17% of scans [7, 13].
The rate of EI values >0.30 determined here likely reflects at least two concurrent factors. First, an age-based selection bias excluded scans from subjects younger than 45 years, who possess notoriously small ventricles. Second, ED-based enrollment may have caused subjects prone to falls to be over-represented, leading to the over-representation in our dataset of neurological conditions favoring frequent falling and head injury.
The observed increase in EI values with age indicates that aging per se induces progressive ventricular enlargement. However, stratified analysis indicated that mean EI values in all one-year cohorts were <0.30 (Figure 1). Thus, aging enlarges the ventricular system, but normally below the threshold for abnormal ventricular enlargement. On the other hand, neurological conditions leading to loss of brain volume or disturbance in cerebrospinal fluid dynamics become more and more frequent with increasing age. Therefore, we suggest that whatever the age of the patient, an EI >0.30 should prompt the physician to search for degenerative diseases such as Alzheimer’s disease or other primary dementias, Parkinson’s disease or other parkinsonisms, vascular diseases such as vascular cognitive, executive or gait impairment, and other conditions leading to the adult chronic hydrocephalus. The present study aimed simply to test EI as a radiological marker of abnormal ventricular enlargement during aging, independently from the eventually associated neurological conditions. The very high frequency of EI values >0.30 found here reflects over-representation in our ED-based series of neurological conditions related to loss of brain volume, obviously more frequent as age grows. The almost doubled risk of having an EI value >0.30 in men a brief comment, i.e. it may reflect a gender difference on brain size, or suggest that being male may favour abnormal ventricular enlargement.
In conclusion, this transversal study demonstrates that EI is a reliable tool for longitudinal assessment of ventricular size in normal aging, and confirms that >0.30 is a valid, age-independent cut-off for disclosing abnormal ventricular enlargement. EI >0.30 should be considered a red flag, motivating clinical and neuroimaging monitoring to identify the underlying neurological condition.
materials and Methods
A retrospective review, IRB-approved (ref. 3601 march 26 2015) of head CT data was conducted from all individuals (aged 45-101 years) who were admitted to our ED between June and December 2009. All scans were part of early work-up for acute neurological symptoms or head injury. We excluded from analysis all scans showing hemorrhagic strokes, neoplasms, or post-traumatic hemorrhages. Two observers (one neuroradiologist, one neurosurgeon) calculated the EI in the axial scans at the level of Monro’s foramens. Agreement between observers was evaluated using Kappa statistic. Student’s t-test, chi-squared test, and multiple logistic regression analysis of EI values were obtained from all scans, one-year [single-age] cohorts, and both sexes. Statistical significance was set at p<0.001.
Funding
The authors declare that they received no funding.
Conflict of Interest
The authors declare the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ishikawa M, Hashimoto M, Kuwana N, Mori E, Miyake H, Wachi A, Takeuchi T, Kazui H, Koyama H. Guidelines for management of idiopathic normal pressure hydrocephalus. Neurol Med Chir [Tokyo]. 2008; 48 Suppl:S1-23.
2. Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005; 57[3 Suppl]:S4-16.
3. Evans WA. An encephalographic ratio for estimating ventricular enlargement and cerebral atrophy. Arch Neurol Psychiat. 1942; 47:931-937.
4. Gawler J, Du Boulay GH, Bull JW, Marshall J. Computerized tomography [the EMI Scanner]: a comparison with pneumoencephalography and ventriculography. J Neurol Neurosurg Psychiatry. 1976; 39:203-211.
5. Synek V, Reuben JR, Du Boulay GH. Comparing Evans’ index and computerized axial tomography in assessing relationship of ventricular size to brain size. Neurology. 1976; 26:231-3.
6. Toma AK, Holl E, Kitchen ND, Watkins LD. Evans’ index revisited: the need for an alternative in normal pressure hydrocephalus. Neurosurgery. 2011; 68:939-44.
7. Ambarki K, Israelsson H, Wåhlin A, Birgander R, Eklund A, Malm J. Brain ventricular size in healthy elderly: comparison between Evans index and volume measurement. Neurosurgery. 2010; 67:94-9 .
8. Earnest MP, Heaton RK, Wilkinson WE, Manke WF. Cortical atrophy, ventricular enlargement and intellectual impairment in the aged. Neurology 1979; 29:1138-43.
9. Coffey CE, Kumar A, Ajilore O. Imaging the structure of the aging human brain. In: Coffey CE, Cummings JL, eds. Textbook of Geriatric Neuropsychiatry. Washington; 2011, 3d ed., pp 147-165.
10. Xu J, Kobayashi S, Yamaguchi S, Iijima K, Okada K, Yamashita K. Gender effects on age-related changes in brain structure. AJNR 2000; 21:112-8.
11. Kaye JA, DeCarli C, Luxenberg JS, Rapoport SI. The significance of age-related enlargement of the cerebral ventricles in healthy men and women measured by quantitative computed X-ray tomography. J Am Geriatr Soc. 1992; 40:225-31.
12. Laffey PA, Peyster RG, Nathan R, Haskin ME, McGinley JA. Computed tomography and aging: results in a normal elderly population. Neuroradiology. 1984; 26:273-8.
13. Inatomi Y, Yonehara T, Hashimoto Y, Hirano T, Uchino M. Correlation between ventricular enlargement and white matter changes. J Neurol Sci. 2008; 269:12-7.