
Introduction
Graft-versus-host disease (GVHD) is an immune driven disorder where donor T cells react and proliferate in response to host antigens [1]. GVHD remains one of the leading causes of morbidity and mortality associated with allogeneic transplantation in patients and stands as a significant barrier to the broader use of hematopoietic stem cell transplantation (HSCT) [2]. The development of GVHD appears to be determined by genetic and environmental factors. Many genes have been shown to be involved in its pathogenesis [3].
Transforming growth factor (TGF)-β is a multiplicity factor mediating cellular processes, including cell growth, cell differentiation, apoptosis, and cellular homeostasis [4]. Recent studies have proposed a role for TGF-β in controlling T-cell alloreactivity and have confirmed that G-CSF administration to human stem-cell donors results in an increase in TGF-β from CD4 T cells [6]. This is also consistent with the clinical association of reduced serum TGF-β levels after engraftment and severe GVHD [6]. Additionally, Li et al. showed that a significant decrease in the levels of TGF-β was seen with increased severity of GVHD [7].
Some studies have investigated the associations between the TGF-β1 polymorphisms and susceptibility of GVHD [8-15]. Most of the studies focused on two polymorphisms: +869C/T (rs1800470) and -509C/T (rs1800469). However, the associations observed between two polymorphisms and the risk for GVHD were controversial and inconclusive. This meta-analysis aimed to comprehensively explore the associations between the TGF-β1 polymorphisms and risk of GVHD.
Results
Study characteristics
The baseline characteristics of the literatures enrolled were summarized in Table 1. Nine studies were included in this meta-analysis. All studies were published between 2001 and 2014. Of these, the majority of the studies were executed in Caucasian (n = 7). Others were conducted in Asian (n = 2). The total sample size from all studies was 1651 and the sample size was 20–394 patients and the range of medium age was 22–48 years. Two studies reported the associations between TGF-β1 polymorphisms and GVHD severity, while other studies reported the associations between TGF-β1 polymorphisms and GVHD risk. All studies were assessed by NOS. The quality scores ranged from 6 to 8, suggesting that the methodological quality was acceptable.
Table 1: Characteristics of the studies included in this meta-analysis
Study |
Year |
Ethnicity |
Age |
No. of Subjects |
No. of GVHD (+) |
No. of GVHD (-) |
HLA matched |
GVHD grade |
Quality assessment |
| Holweg | 2001 | Caucasian | 47 | 236 | 72 | 164 | Mixed | NA | 7 |
| Visentainer | 2005 | Caucasian | 30 | 118 | 19 | 99 | Yes | Mixed | 7 |
| Noori-Daloii | 2007 | Caucasian | 25 | 84 | 42 | 42 | Yes | NA | 8 |
| Shah | 2009 | Caucasian | 42 | 46 | 46 | 0 | Yes | Reported | 7 |
| Berro | 2010 | Caucasian | NA | 427 | 117 | 310 | Mixed | Mixed | 8 |
| Karimi | 2010 | Caucasian | NA | 20 | 20 | 0 | NA | Reported | 6 |
| Rashidi–Nezhad | 2010 | Caucasian | 22 | 86 | 43 | 43 | Yes | NA | 7 |
| Xiao 1 | 2010 | Asian | 24 | 138 | 94 | 44 | Mixed | Mixed | 8 |
| Xiao 2 | 2010 | Asian | 32 | 102 | 24 | 78 | Yes | NA | 8 |
| Kim | 2014 | Asian | 48 | 394 | 307 | 87 | Mixed | NA | 7 |
GVHD, acute graft versus host disease; HLA, human leukocyte antigen; NA, not available.
Quantitative Data Synthesis
TGF-β1 polymorphisms and GVHD risk in donors
Four studies reported the association between TGF-β1 rs1800469 polymorphism and the susceptibility to GVHD in donors. According to the heterogeneity test, the studies showed no significant heterogeneity (I2=10%, P=0.34). Our findings demonstrated that TGF-β1 rs1800469 polymorphism reduced the susceptibility to GVHD (OR=0.56; 95%CI, 0.32–0.98; P=0.04; Figure 1). In the subgroup analyses by ethnicity, the significant association was only found among Asians (OR=0.38; 95%CI, 0.18–0.80; P=0.01), while no significant association was found among Caucasians (OR=0.95; 95%CI, 0.40–2.25; P=0.12). In addition, no significant association was found among HLA-matched subjects (OR=0.23; 95%CI, 0.04–1.32; P=0.10).
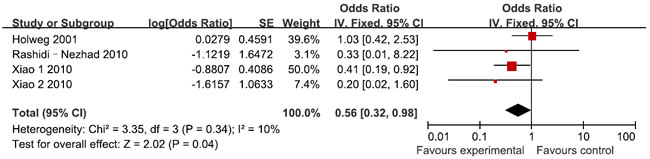
Figure 1: Meta-analysis for for TGF-β1 rs1800469 polymorphism and GVHD risk in donors
Four studies reported the association between TGF-β1 rs1800470 polymorphism and the susceptibility to GVHD in donors. According to the heterogeneity test, the studies showed no heterogeneity (I2=0%, P=0.47). Our findings demonstrated that TGF-β1 rs1800470 polymorphism reduced the susceptibility to GVHD (OR=0.65; 95%CI, 0.46–0.94; P=0.02; Figure 2). In the subgroup analyses by ethnicity, no significant association was found among Caucasians (OR=0.70; 95%CI, 0.47–1.06; P=0.09). All the results are listed in Table 2.
Table 2: Results of the meta-analysis.
Polymorphisms |
Subgroup |
Heterogeneity Test of association |
|||||
OR (95% CI) |
P Value |
Model |
I2 (%) |
P Value |
|||
Donor |
|||||||
rs1800469 |
Overall |
0.56 (0.32-0.98) |
0.04 |
F |
10 |
0.34 |
|
Caucasian |
0.95 (0.40-2.25) |
0.12 |
F |
0 |
0.50 |
||
Asian |
0.38 (0.18-0.80) |
0.01 |
F |
0 |
0.52 |
||
HLA-matched |
0.23 (0.04-1.32) |
0.10 |
F |
0 |
0.80 |
||
rs1800470 |
Overall |
0.65 (0.46-0.94) |
0.02 |
F |
0 |
0.47 |
|
Caucasian |
0.70 (0.47-1.06) |
0.09 |
F |
0 |
0.37 |
||
Recipient |
|||||||
rs1800469 |
Overall |
0.73 (0.63-0.85) |
<0.0001 |
F |
7 |
0.37 |
|
Caucasian |
0.51 (0.22-1.18) |
0.12 |
F |
0 |
0.78 |
||
Asian |
0.74 (0.63-0.86) |
0.0001 |
F |
42 |
0.18 |
||
HLA-matched |
0.32 (0.08-1.27) |
0.11 |
F |
0 |
0.99 |
||
rs1800470 |
Overall |
1.28 (0.81-2.01) |
0.29 |
F |
0 |
0.72 |
|
Caucasian |
1.32 (0.80-2.17) |
0.28 |
F |
0 |
0.44 |
||
F, fixed effects model; HLA, human leukocyte antigen.
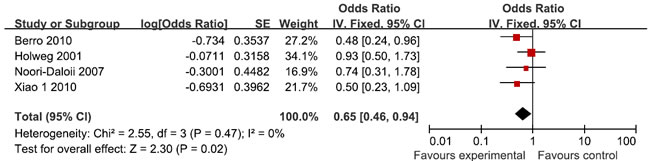
Figure 2: Meta-analysis for for TGF-β1 rs1800470 polymorphism and GVHD risk in donors
TGF-β1 polymorphisms and GVHD risk in recipients
Five studies reported the association between TGF-β1 rs1800469 polymorphism and the susceptibility to GVHD in recipients. According to the heterogeneity test, the studies showed no significant heterogeneity (I2=7%, P=0.37). Our findings demonstrated that TGF-β1 rs1800469 polymorphism reduced the susceptibility to GVHD (OR=0.73; 95%CI, 0.63–0.85; P<0.0001; Figure 3). In the subgroup analyses by ethnicity, the significant association was only found among Asians (OR=0.74; 95%CI, 0.63–0.86; P=0.0001), while no significant association was found among Caucasians (OR=0.51; 95%CI, 0.22–1.18; P=0.12). In addition, no significant association was found among HLA-matched subjects (OR=0.32; 95%CI, 0.08–1.27; P=0.11).
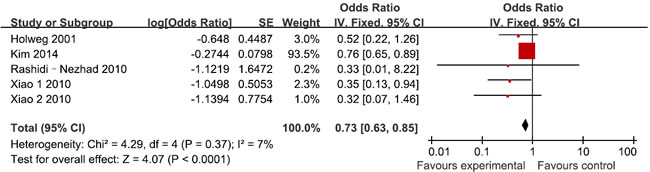
Figure 3: Meta-analysis for for TGF-β1 rs1800469 polymorphism and GVHD risk in recipients
Three studies reported the association between TGF-β1 rs1800470 polymorphism and the susceptibility to GVHD in recipients. According to the heterogeneity test, the studies showed no heterogeneity (I2=0%, P=0.72). Our findings demonstrated that TGF-β1 rs1800470 polymorphism did not influence the susceptibility to GVHD (OR=1.28; 95%CI, 0.81–2.01; P=0.29; Figure 4). In the subgroup analyses by ethnicity, no significant association was found among Caucasians (OR=1.32; 95%CI, 0.80–2.17; P=0.28). All the results are listed in Table 2.
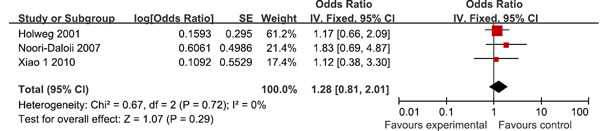
Figure 4: Meta-analysis for for TGF-β1 rs1800470 polymorphism and GVHD risk in recipients
Discussion
TGF-β can inhibit TH1 and TH2 differentiation and the acquisition of most, if not all, effector functions by naive T cells [16]. During GVHD, systemic levels of IFN-γ were increased in the presence of TGF-β neutralization, suggesting the augmentation of type 1 differentiation. Acute GVHD has been established as a T-cell-dependent and a TH1-dominant disease [17], and the enhancement of T-cell proliferation or TH1 differentiation because of a reduction in regulation appears the predominant mechanism by which the neutralization of TGF-β augments the severity of GVHD. TGF-β1 rs1800470 and rs1800469 polymorphisms have been identified. These allelic variants were associated with increased level of TGF-β1 expression and plasma concentration [18, 19]. Therefore, it is possible that TGF-β1 rs1800470 and rs1800469 polymorphisms could decrease the risk of GVHD.
This meta-analysis assessed the association between TGF-β1 rs1800470 and rs1800469 polymorphisms and GVHD risk systematically. Donors or recipients with TGF-β1 rs1800469 polymorphism showed decreased GVHD risk. Donors with TGF-β1 rs1800470 polymorphism were also observed to have lower GVHD risk. However, TGF-β1 rs1800470 polymorphism in recipients were not associated with GVHD risk. There was only three studies investigated the association between TGF-β1 rs1800470 polymorphism and GVHD risk. Thus, more studies are needed to determine whether recipients with TGF-β1 rs1800470 polymorphism have lower GVHD risk. Only two studies evaluated the association between TGF-β1 polymorphisms and GVHD severity. Thus, meta-analysis was not conducted. Furthermore, all these two studies did not find significant association TGF-β1 polymorphisms and GVHD severity.
Limitations of the present study should be acknowledged. First, the sample sizes in several of the incorporated studies were relatively small, which may reduce the strength of our conclusions. Second, all eligible studies were published in English and indexed by the selected databases. It is possible that studies published in other languages or unpublished studies could be missed, which might bias the results. In addition, the result was on the basis of unadjusted estimates, while a more accurate analysis should be carried out if more detailed individual information was available, which would allow for an adjusted estimate by other factors.
In summary, despite the limitations, this meta-analysis suggests that donors or recipients with TGF-β1 rs1800469 polymorphism and donors with TGF-β1 rs1800470 polymorphism might be associated with reduced GVHD risk. More future studies with good methodology design are warranted.
Materials and methods
Publication search
PubMed, EMBASE, Web of Science, and the Cochrane Library were searched to obtain relevant articles published up until May 2015. The following medical subject heading (Mesh) terms were used in combination with Boolean operators AND or OR: graft-versus-host disease, GVHD, Transforming growth factor, TGF, and TGF-β1. Furthermore, the references in relevant articles were screened manually to identify additional eligible studies. No language restriction was imposed during the electronic search.
Inclusion and exclusion criteria
We selected eligible studies based on the following criteria: (1) cohort or case-control study; (2) investigated associations between TGF-β1 rs1800470 or rs1800469 polymorphism and GVHD; (3) provided sufficient data of allele and genotype frequencies of SNPs or required information could be calculated; (4) if serial studies on the same population were published, only the most recent study was included; (5) proper methodology design. Two independent investigators performed study selection and reached final consensus. The details of literature search and selection were shown in Figure 5 in standard PRISMA flow diagram style.
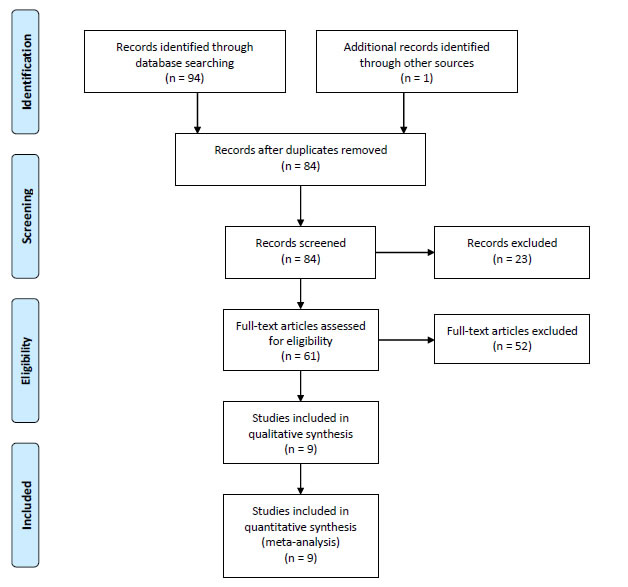
Figure 5: Flow chart for the literature search strategy.
Qualitative assessment
Two authors completed the quality assessment independently. The Newcastle–Ottawa Scale (NOS) was used to evaluate the methodological quality, which scored studies by the selection of the study groups, the comparability of the groups, and the ascertainment of the outcome of interest. We considered a study awarded 0-3, 4-6, or 7-9 as a low-, moderate-, or high-quality study, respectively [20].
Data extraction
The data were extracted from each included study by two independent investigators, and the following information was collected: surname of the first author, year of publication, ethnicity, age, sample size, human leukocyte antigen (HLA) status, and GVHD grade. Disagreement on the inclusion of any study was resolved by consultation with a third investigator.
Statistical analysis
The associations between TGF-β1 polymorphisms and GVHD risk was assessed using odds ratios (ORs) and the corresponding 95% confidence intervals (CIs) in donors and recipients, respectively. Dominant model was used in this meta-analysis, because most of the studies reported the results in this model. The heterogeneity of the included trials was assessed by the Cochrane’s Q statistic for each meta-analysis. We carried out both fixed-effects (Mantel–Haenszel method) and random effects (DerSimonian–Laird method) models and producted the pooled HRs. In addition, subgroup analyses were performed to investigate the potential causes of heterogeneity according to ethnicity and HLA status. Publication bias was evaluated if more than ten studies were included. All analyses were performed by using stata 12.0 statistical software (Stata Corporation, College Station, TX, USA). All P values were two-sided.
Acknowledgments
We thank the hospital for providing a good research platform for us, and thank the family for their support and understand in work and study.
Conflicts of interest
The authors declare no conflict of interest.
References
1. Appelbaum FR. Hematopoietic-cell transplantation at 50. N Engl J Med. 2007 Oct 11;357:1472-5.
2. Jacobsohn DA, Vogelsang GB. Acute graft versus host disease. Orphanet J Rare Dis. 2007 Sep 4;2:35.
3. Ogawa S, Matsubara A, Onizuka M, Kashiwase K, Sanada M, Kato M, Nannya Y, Akatsuka Y, Satake M, Takita J, Chiba S, Saji H, Maruya E, Inoko H, Morishima Y, Kodera Y, Takehiko S; Japan Marrow Donation Program (JMDP). Exploration of the genetic basis of GVHD by genetic association studies. Biol Blood Marrow Transplant. 2009 Jan;15:39-41.
4. Verrecchia F, Mauviel A. Transforming growth factor-beta signaling through the Smad pathway: role in extracellular matrix gene expression and regulation. J Invest Dermatol. 2002 Feb;118:211-5.
5. Zheng SG, Wang JH, Koss MN, Quismorio F Jr, Gray JD, Horwitz DA. CD4+ and CD8+ regulatory T cells generated ex vivo with IL-2 and TGF-beta suppress a stimulatory graft-versus-host disease with a lupus-like syndrome. J Immunol. 2004 Feb 1;172:1531-9.
6. Li Q, Zhai Z, Xu X, Shen Y, Zhang A, Sun Z, Liu H, Geng L, Wang Y. Decrease of CD4(+)CD25(+) regulatory T cells and TGF-beta at early immune reconstitution is associated to the onset and severity of graft-versus-host disease following allogeneic haematogenesis stem cell transplantation. Leuk Res. 2010 Sep;34:1158-68.
7. Holweg CT, Baan CC, Balk AH, Niesters HG, Maat AP, Mulder PM, Weimar W. The transforming growth factor-beta1 codon 10 gene polymorphism and accelerated graft vascular disease after clinical heart transplantation. Transplantation. 2001 May 27;71:1463-7.
8. Laguila Visentainer JE, Lieber SR, Lopes Persoli LB, Dutra Marques SB, Vigorito AC, Penteado Aranha FJ, de Brito Eid KA, Oliveira GB, Martins Miranda EC, Bragotto L, de Souza CA. Relationship between cytokine gene polymorphisms and graft-versus-host disease after allogeneic stem cell transplantation in a Brazilian population. Cytokine. 2005 Nov 3;32:171-7.
9. Noori-Daloii MR, Rashidi-Nezhad A, Izadi P, Hossein-Nezhad A, Sobhani M, Derakhshandeh-Peykar P, Alimoghaddam K, Ghavamzadeh A. Transforming growth factor-beta1 codon 10 polymorphism is associated with acute GVHD after allogenic BMT in Iranian population. Ann Transplant. 2007;12:5-10.
10. Shah R, Selby ST, Yokley B, Slack RS, Hurley CK, Posch PE. TNF, LTA and TGFB1 genotype distributions among acute graft-vs-host disease subsets after HLA-matched unrelated hematopoietic stem cell transplantation: a pilot study. Tissue Antigens. 2009 Jul;74:50-6.
11. Berro M, Mayor NP, Maldonado-Torres H, Cooke L, Kusminsky G, Marsh SG, Madrigal JA, Shaw BE.Berro M1, Mayor NP, Maldonado-Torres H, Cooke L, Kusminsky G, Marsh SG, Madrigal JA, Shaw BE. Association of functional polymorphisms of the transforming growth factor B1 gene with survival and graft-versus-host disease after unrelated donor hematopoietic stem cell transplantation. Haematologica. 2010 Feb;95:276-83.
12. Karimi MH, Daneshmandi S, Pourfathollah AA, Geramizadeh B, Ramzi M, Yaghobi R, Ebadi P. The IFN-gamma allele is correlated to moderate-to-severe acute graft-versus-host disease after allogeneic stem cell transplant. Exp Clin Transplant. 2010 Jun;8:125-9.
13. Rashidi-Nezhad A, Azimi C, Alimoghaddam K, Ghavamzadeh A, Hossein-Nezhad A, Izadi P, Sobhani M, Noori-Daloii AR, Noori-Daloii MR. TGF-Beta codon 25 polymorphism and the risk of graft-versus-host disease after allogenic hematopoietic stem cell transplantation. Iran J Allergy Asthma Immunol. 2010 Mar;9:1-6.
14. Xiao H, Cao W, Lai X, Luo Y, Shi J, Tan Y, He J, Xie W, Meng X, Zheng W, Zheng G, Han X, Jin L, Zhang L, Wang Y, Yu X, Cai Z, Lin M, Ye X, Huang H. Immunosuppressive cytokine gene polymorphisms and outcome after related and unrelated hematopoietic cell transplantation in a chinese population. Biol Blood Marrow Transplant. 2011 Apr;17:542-9.
15. Kim D, Won HH, Su S, Cheng L, Xu W, Hamad N, Uhm J, Gupta V, Kuruvilla J, Messner HA, Lipton JH. Risk stratification of organ-specific GVHD can be improved by single-nucleotide polymorphism-based risk models. Bone Marrow Transplant. 2014 May;49:649-56.
16. Gorelik L, Flavell RA. Transforming growth factor-beta in T-cell biology. Nat Rev Immunol. 2002 Jan;2:46-53.
17. Hill GR, Ferrara JL. The primacy of the gastrointestinal tract as a target organ of acute graft-versus-host disease: rationale for the use of cytokine shields in allogeneic bone marrow transplantation. Blood. 2000 May 1;95:2754-9.
18. Grainger DJ, Heathcote K, Chiano M, Snieder H, Kemp PR, Metcalfe JC, Carter ND, Spector TD. Genetic control of the circulating concentration of transforming growth factor type beta1. Hum Mol Genet. 1999 Jan;8:93-7.
19. Pooja S, Francis A, Rajender S, Tamang R, Rajkumar R, Saini KS, Megu K, Goel MM, Surekha D, Rao DR, Rao L, Ramachandra L, Kumar S, Kumar S, Vishnupriya S, Satyamoorthy K, Negi MP, Thangaraj K, Konwar R. Strong impact of TGF-β1 gene polymorphisms on breast cancer risk in Indian women: a case-control and population-based study. PLoS One. 2013;8:e75979
20. GA Wells, B Shea, D O’Connell, J Peterson, V Welch, M Losos, P Tugwell. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. URL: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.