
INTRODUCTION
Head and neck cancer is the sixth most common cancer worldwide. Oral squamous cell carcinoma (OSCC), a subset of this disease, accounts for more than 300,000 new cases each year. OSCC originates from the oral mucosal epithelia. Although efforts have been made to improve the prognosis of patients with OSCC for decades, the 5-year survival rate is still about 50% to 60%, and even lower in the patients at clinical late stage [1, 2].
Growth differentiation factor 15 (GDF15), also known as nonsteroidal anti-inflammatory drug-activated gene-1 (NAG-1), macrophage inhibitory cytokine 1(MIC-1), placental TGF-β (PTGF-β), prostate differentiation factor (PDF), and placental bone morphogenetic protein (PLAB), is a divergent member of the TGF-β superfamily [3]. The GDF15 gene is located at band p13.11 on chromosome 19 with two exons that encode a 308-amino-acid of GDF15 polypeptide, consisting of a 29-amino-acid signal peptide, a 167-amino-acid propeptide, and a 112-amino-acid mature protein. Cleavage of the propeptide allows the mature protein to be secreted as a disulfide-linked homo-dimer [3]. GDF15 is a TP53 transcriptional target that mediates G1 cell cycle arrest and apoptosis [4, 5].
GDF15 plays multiple roles in various pathologies, including inflammation, cancer, cardiovascular disease and obesity [6, 7]. Although the role of GDF15 in tumorigenesis is not universal, overexpression of GDF15 has been reported to play an important role in OSCC [8, 9], and indicates a poorer prognosis in OSCC patients [10]. Recent advances in molecular biology have demonstrated that mutations or single nucleotide polymorphisms of relevant genes may affect the risk and prognosis in head and neck squamous cell carcinoma [11, 12]. Unfortunately, there is still no clinical evidence of GDF15 mutations on prognostic evaluation in OSCC; the relationship between TP53/GDF15 mutations and GDF15 expression remains unclear.
In the present study, we tested the GDF15 and TP53 mutations using next-generation sequencing by Ion Torrent Personal Genome Machine (PGM) and GDF15 expression using immunohistochemistry in formalin-fixed paraffin-embedded (FFPE) biopsy samples from 46 patients with locally advanced OSCC. We hypothesized the prognostic usefulness of GDF15 mutations and potential relationship between TP53/GDF15 mutations and GDF15 expression in OSCC.
RESULTS
GDF15 mutations in biopsy samples from OSCC patients
By analyzing the matched non-cancerous tissues and the reference sequences of GDF15, twenty-nine GDF15 mutations were identified in 19 out of 46 patients (41.3%), including eighteen missense mutations, two nonsense mutations and nine synonymous mutations (Supplementary Table 1). Of the 19 patients, synonymous GDF15 mutations only were found in two patients; missense GDF15 mutation was the majority of single nucleotide variants (18/29) leading to a single amino acid alteration in 17 patients. Among the 18 missense GDF15 mutations which lead to amino acid alterations, ten (55.6%) amino acid alterations were located at the propeptide region, four amino acid alterations (22.2%) were located at the mature peptide region, and the other four amino acid alterations (22.2%) were at the signal peptide region (Table 1). No significant difference of proportion of GDF15 mutations was found according to baseline characteristics (Table 2).
Table 1: Summary of GF15 mutations in the different domains in the 17 patients with oral squamous cell carcinoma
Case |
GDF15 domains |
||
|---|---|---|---|
Signal peptide |
Propeptide |
Mature peptide |
|
1 |
P41T |
||
2 |
P111L |
||
3 |
E181K |
||
4 |
P204S |
||
5 |
S219L |
||
6 |
G11D |
||
7 |
P2L |
P186S, Q187Tera |
|
8 |
A152V |
||
9 |
H100Y |
||
10 |
L127P |
||
11 |
T78A |
||
12 |
P2L |
||
13 |
A176V |
||
14 |
G3R |
||
15 |
S128F |
||
16 |
W73Tera |
V292M |
|
17 |
D304N |
||
aTer was a nonsense mutation
Table 2: Baseline characteristics and missense GDF15 mutations in patients with oral squamous cell carcinoma
Characteristics |
Total number |
missense GDF15 mutations |
P value* |
|
|---|---|---|---|---|
+ |
− |
|||
Gender |
||||
Male |
12 (26.1) |
5 (29.4) |
7 (24.1) |
0.737 |
Female |
34 (73.9) |
12 (70.6) |
22 (75.9) |
|
Age (years) |
||||
<60 |
27 (58.7) |
11 (64.7) |
16 (55.2) |
0.555 |
≥60 |
19 (41.3) |
6 (35.3) |
13 (44.8) |
|
Site |
||||
Tongue |
19 (41.3) |
10 (58.8) |
9 (31.0) |
0.152 |
Buccal |
4 (8.7) |
0 (0.0) |
4 (13.8) |
|
Gingiva |
8 (17.4) |
3 (17.6) |
5 (17.2) |
|
Floor of mouth |
3 (6.5) |
0 (0.0) |
3 (10.3) |
|
Palate |
9 (19.6) |
2 (11.8) |
7 (24.1) |
|
Retromolar trigone |
3 (6.5) |
2 (11.8) |
1 (3.4) |
|
T stage |
||||
T1/T2 |
13 (28.3) |
5 (29.4) |
8 (27.6) |
1.000 |
T3/T4 |
33 (71.7) |
12 (70.6) |
21 (72.4) |
|
N stage |
||||
N0 |
14 (30.4) |
5 (29.4) |
9 (31.0) |
0.522 |
N1 |
12 (26.1) |
6 (35.3) |
6 (20.7) |
|
N2 |
20 (43.5) |
6 (35.3) |
14 (48.3) |
|
TNM stage |
||||
III |
22 (47.8) |
9 (52.9) |
13 (44.8) |
0.761 |
IVA |
24 (52.2) |
8 (47.1) |
16 (55.2) |
|
Pathologic differentiation grade |
||||
Well |
13 (28.3) |
6 (35.3) |
7 (24.1) |
0.505 |
Moderately/Poorly |
33 (71.7) |
11 (64.7) |
22 (75.9) |
|
Smoking status** |
||||
Never |
19 (41.3) |
8 (47.1) |
11 (37.9) |
0.757 |
Current/former |
27 (58.9) |
9 (52.9) |
18 (62.1) |
|
Alcohol use*** |
||||
Negative |
24 (52.2) |
10 (58.8) |
14 (48.3) |
0.552 |
Positive |
22 (47.8) |
7 (41.2) |
15 (51.7) |
|
*P value from the chi-square test was reported to compare the difference between the patients with wild-type GDF15 and missense mutant GDF15 based on the different baseline factors.
**Former/current smokers defined as at least a one pack-year history of smoking.
***Positive alcohol use was defined as current alcohol use of more than one drink per day for 1 year (12 ounces of beer with 5% alcohol, or 5 ounces of wine with 12%-15% alcohol, or one ounce of liquor with 45%-60% alcohol). All other patients were classified as negative alcohol use.
Missense GDF15 mutations indicates poorer patients' outcomes
Compared with the patients of wild-type GDF15, the patients of missense GDF15 mutations had significantly poorer outcomes, including overall survival (P = 0.035), disease-free survival (P = 0.032) and locoregional recurrence-free survival (P = 0.015) (Figure 1A-1C). Although, there was no significant difference on distant metastasis-free survival (P = 0.070), there was a tendency that the patients of wild-type GDF15 had a better distant metastasis-free survival than those of missense GDF15mutations (Figure 1D).
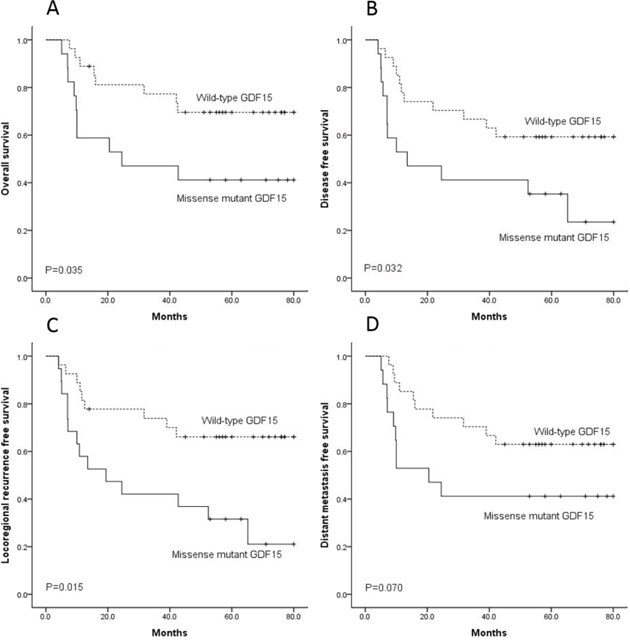
Figure 1: The 27 patients with wild-type GDF15 had better outcome than the 17 patients with missense GDF15 mutation on overall survival. A. disease-free survival B. locoregional recurrence-free survival C. and distant metastasis-free survival D.
Univariate Cox model was used to analyze the impact of baseline characteristics on the time-to-event end points, only the GDF15 mutations and TNM staging were found as risk factors of prognosis. GDF15 mutation (missense mutation versus wild-type) was a significant risk factor of overall survival (P = 0.042, HR = 2.627, 95% CI:1.035–6.670), disease-free survival (P = 0.038, HR = 2.383, 95% CI:1.048–5.417), locoregional recurrence-free survival (P = 0.020, HR = 2.790, 95% CI:1.172–6.643) and distant metastasis-free survival (P = 0.078, HR = 2.207, 95% CI:0.961–5.318); TNM staging (stage III versus stage IVA) was a significant risk factor of overall survival (P = 0.047, HR = 0.369, 95% CI:0.138–0.986) and locoregional recurrence-free survival (P = 0.049, HR = 0.408, 95% CI:0.167–0.995), while not significant of disease-free survival (P = 0.068, HR = 0.455, 95% CI:0.195–1.059) or distant metastasis-free survival (P = 0.069, HR = 0.425, 95% CI:0.169–1.068).
Multivariate Cox model analysis was performed using the risk factors of GDF15 mutations and TNM staging. Only missense GDF15 mutations was the independent increased risk factor of overall survival (P = 0.003), disease-free survival (P = 0.015), locoregional recurrence-free survival (P = 0.008) and distant metastasis-free survival (P = 0.009) (Table 3). When the pathologic differentiation grade, smoking status and alcohol use were inputted into the multivariate Cox model analysis, only the missense GDF15 mutations was independent increased risk factor of poor prognosis (Supplementary Table 2).
Table 3: Multivariate Cox model analysis with missense GDF15 mutation and TNM staging as well as their interaction analysis
Characteristics |
HR |
95% CI |
P value |
|---|---|---|---|
Overall survival |
|||
Missense GDF15 mutation (yes vs. no) |
5.993 |
1.856–19.346 |
0.003 |
TNM staging (stage III vs. stage IVA) |
0.596 |
0.142–2.497 |
0.479 |
Missense GDF15 mutation by TNM staging |
0.239 |
0.033–1.732 |
0.156 |
Disease-free survival |
|||
Missense GDF15 mutation (yes vs. no) |
3.764 |
1.295–10.945 |
0.015 |
TNM staging (stage III vs. stage IVA) |
0.509 |
0.148–1.751 |
0.284 |
Missense GDF15 mutation by TNM staging |
0.538 |
0.099–2.933 |
0.474 |
Locoregional recurrence-free survival |
|||
Missense GDF15 mutation (yes vs. no) |
4.555 |
1.494–13.889 |
0.008 |
TNM staging (stage III vs. stage IVA) |
0.426 |
0.105–1.719 |
0.231 |
Missense GDF15 mutation by TNM staging |
0.561 |
0.091–3.467 |
0.534 |
Distant metastasis-free survival |
|||
Missense GDF15 mutation (yes vs. no) |
4.420 |
1.145–13.433 |
0.009 |
TNM staging (stage III vs. stage IVA) |
0.668 |
0.188–2.368 |
0.532 |
Missense GDF15 mutation by TNM staging |
0.270 |
0.042–1.740 |
0.168 |
TP53 mutations in OSCC patients
Thirty-six missense TP53 mutations, five insert or deletion mutations, four nonsense mutations, and five splice-site mutations were identified in 37 of 46 patients (80.4%) (Supplementary Table 3). The mutations derived from the PGM were confirmed using Sanger sequencing. Among the 37 patients, three patients had a splice-site mutation only, which was stratified by EAp53 as low risk; eighteen patients were stratified by EAp53 as high risk, and the other sixteen patients were stratified as low risk (Table 4).
Table 4: TP53 mutations in different domains in patients with oral squamous cell carcinoma according to the EAp53 evaluation system
Case |
Risk (EAp53) |
DNA-binding core |
Tetramerization |
The Othersa |
|---|---|---|---|---|
1 |
Low |
V216M |
||
2 |
Low |
P151T |
||
3 |
High |
R175H |
||
4 |
Low |
R282W |
R337C |
|
5 |
High |
C135F |
||
6 |
Low |
K319*† |
||
7 |
Low |
A159V |
||
8 |
High |
F113C |
||
9 |
Low |
R273H |
||
10 |
High |
R248Q, C176F |
||
11 |
Low |
R282W |
||
12 |
High |
H193L |
||
13 |
Low |
H178* |
||
14 |
Low |
W53Ter‡ |
||
15 |
High |
G245S |
||
16 |
High |
P152L |
||
17 |
Low |
T329I |
||
18 |
High |
H179L |
||
19 |
High |
Y220C |
S15I |
|
20 |
High |
Q331Ter |
||
21 |
Low |
V272L |
||
22 |
High |
C135Y |
||
23 |
Low |
P151H |
||
24 |
Low |
R213Q |
||
25 |
High |
R342Ter |
||
26 |
High |
E286K, P191* |
||
27 |
Low |
V274F |
||
28 |
High |
T253I, D184H, C135F |
||
29 |
High |
V218E |
E326* |
|
30 |
High |
R175H |
||
31 |
High |
R273C, I255F, P152L |
S15I |
|
32 |
Low |
R282W |
||
33 |
High |
R213Ter |
||
34 |
Low |
V216M, P128S |
L93* |
aThe domain contains N-ter Transactivation domain (1–42), Proline rich domain (61–94), C-ter domain (301–393) but out of Tetramerization domain (324–355) and the others.
†*Insert or deletion mutation
‡Ter nonsense mutation
Correlation between TP53 mutations, GDF15 mutations and GDF15 protein expression
Using the Chi-square test, there was no significant relationship between GDF15 mutation and GDF15 protein expression, or between TP53 mutation and GDF15 protein expression (Table 5). Spearman rank correlation coefficient was calculated, there was no significant correlation between TP53 mutation and GDF15 protein expression, nor GDF15 mutation and GDF15 protein expression (P > 0.05).
Table 5: Correlation between TP53/GDF15 mutation and GDF15 protein expression
GDF15 protein expression |
GDF15 mutation |
P value |
TP53 mutation |
P value |
|||
|---|---|---|---|---|---|---|---|
Wild-type |
Missense mutation |
Wild-type |
Low risk mutation |
High risk mutation |
|||
GDF15 staining percentage score |
|||||||
0 |
2 |
4 |
0.687 |
2 |
2 |
2 |
0.308 |
1 |
4 |
2 |
3 |
1 |
2 |
||
2 |
5 |
4 |
1 |
5 |
3 |
||
3 |
12 |
6 |
3 |
9 |
6 |
||
4 |
4 |
3 |
0 |
2 |
5 |
||
GDF15 staining intensity score |
|||||||
0 |
2 |
4 |
0.159 |
2 |
2 |
2 |
0.589 |
1 |
5 |
0 |
1 |
2 |
2 |
||
2 |
10 |
7 |
4 |
9 |
4 |
||
3 |
10 |
8 |
2 |
6 |
10 |
||
DISCUSSION
In this study, we report that GDF15 mutations happens in 41.3% of OSCC patients using the next-generation sequencing by Ion Torrent PGM, and that patients with missense GDF15 mutations have significantly poorer survival than those with wild-type GDF15. Missense GDF15 mutations could be used as an independent increased risk factor of poor prognosis in OSCC patients.
GDF15 overexpression has been reported in several type of cancers, including OSCC [8, 10, 13–16]. Prognostic value of GDF15 overexpression in OSCC has also been reported in our previous study showing that the patients with high GDF15 expression have a lower survival than those with low GDF15 expression [10]. In the present study, we find that patients with missense GDF15 mutations have a poorer prognosis than those with wild-type GDF15. Although there is no other literature reporting the familiar results in any other type of cancers, our results indicate that the OSCC patients with missense GDF15 mutations would have a worse prognosis than those with wild-type GDF15. More aggressive treatment might be helpful for the patients with missense GDF15 mutations to improving prognosis, such as postoperative chemoradiotherapy, induction chemotherapy, or possible target therapy on mutant GDF15. However, before the more aggressive treatment applied in the patients with missense GDF15 mutations, prospective clinical trials should be performed to confirm the benefit of the more aggressive treatment.
It is interesting that there is no significant relationship between GDF15 mutations and GDF15 expression in this study; however, patients with missense GDF15 mutations have a relatively higher GDF15 expression intensity than those with wild-type GDF15. The GDF15 protein is synthesized as a precursor containing an NH2-terminal propeptide and a COOH-terminal mature GDF15 domain. It undergoes disulfide-linked dimerization in the endoplasmic reticulum. Only correctly folded and dimerized GDF15 precursor could leave the endoplasmic reticulum to the Golgi apparatus, where they are cleaved by a furin-like proconvertase proteolytically. Then, the propeptide is separated from the mature COOH-terminal domain [3, 17]. In the present study, 59% of amino acid alterations were located within the propeptide region; unfortunately, the detection of mature GDF15 expression in the FFPE sample could not be performed. In other studies investigating the role of GDF15 propeptide and mature GDF15, xenograft models bearing tumors secreting various engineered forms of GDF15 show that the propeptide regulates the balance between the extracellular matrix stores and mature GDF15 in vivo. The absence of GDF15 propeptide results in about a 20-fold increase in mature GDF15 level in serum [18]. Therefore, GDF15 mutation in the propeptide region might lead to the accumulation of GDF15 expression, and the increase of GDF15 store might enhance the interactive cross-talk of GDF15 with other oncogenic signaling pathways [10, 19–22]. Larger sample size studies are recommended to reveal the relationship between GDF15 mutations and GDF15 expression, as well as the detail mechanism of GDF15 mutations in different gene regions on GDF15 expression.
TP53 is the most frequently mutated gene in head and neck cancer, and patients with TP53 mutation have a poorer prognostic outcome than those with wild-type TP53. Mutant TP53 could stratify head and neck cancer patients with tumors harboring TP53 mutations as high or low risk, and the patients with high risk TP53 mutation have the poorest survival outcomes [23–26]. Recently, some mutant TP53 displays oncogenic properties, termed gain of function, that could regulate numerous genes on a transcriptional level [27]. GDF15 is a TP53 transcriptional target and there are two consensus p53-binding sites in the GDF15 gene promoter, which could be activated by the wild-type p53 protein [5]. Unfortunately, in the present study, we find no relationship between TP53 mutation and GDF15 expression. Further investigations with large sample size are recommended to reveal the molecular relationship between mutant TP53 and GDF15 expression.
There are some limitations in our study. The sample size is relatively small and therefore mutation frequencies reported here might be biased. A larger sample size is recommended in future studies. Only one high-throughput next-generation sequencing platform is used for mutation analysis and other sequencing platforms and independent cohorts are suggested to validate our findings.
In conclusion, our results indicate that missense GDF15 mutations could be used as an independent increased risk factor of poor prognosis in OSCC patients. Further investigations are suggested to reveal the molecular relationship between GDF15 mutations in different gene regions and GDF15 expression, as well as the molecular relationship between TP53 mutations and GDF15 expression. Understanding the GDF15 function in OSCC might be useful for identification of novel therapeutic targets and, ultimately, the personalization of cancer treatment based on the GDF15 mutations.
MATERIALS AND METHODS
Patients and samples
From 2008 to 2010, 46 patients with untreated locally advanced OSCC were involved in this study. Written informed consent was obtained from all patients, which was approved by the Human Research Ethics Committee of Ninth People's Hospital Shanghai Jiao Tong University School of Medicine (approved number: 2008 [12]). All these patients at clinical stage III and IVA received radical surgery followed by radiotherapy (four patients received TPF induction chemotherapy) and were followed up routinely with a median follow-up period of 57 months (up to June, 2014). During the follow-up period, death event occurred in 19 patients, locoregional tumor recurrence was confirmed in nine patients and distant metastasis occurred in three patients. The FFPE biopsy samples were used for GDF15 and TP53 mutation sequencing and GDF15 immunohistochemistry. A non-cancerous FFPE tissue sample from the neck dissection of each patient was used as control for genetic analysis.
DNA extraction and quantification
The tissue samples were reviewed by two pathologists, and the tumor areas on hematoxylin-eosin stained slide were determined for microdissection and subsequent DNA sequencing. Five 10 μm FFPE sections from each block were deparaffinized and the DNA was extracted using QIAamp DNA FFPE Tissue Kit (Qiagen, Germany). Quality and quantity of the purified DNA were measured using the Qubit and Nano-Drop platforms (Thermo Fisher Scientific, USA).
Deep sequencing of PCR amplicons
Ten nanogram of DNA were used for multiplex PCR amplification. Libraries were constructed using the Ion AmpliSeq Library Kit v2.0 (Thermo Fisher Scientific, USA) according to the manufacturer's instructions. The quality of obtained library was evaluated by the Agilent 2100 Bioanalyzer on-chip electrophoresis (Agilent Technologies, USA).
Emulsion PCR was performed with the OneTouch DL or OneTouch 2 system (Thermo Fisher Scientific, USA). Sequencing was run on the Ion Torrent Personal Genome Machine (Thermo Fisher Scientific, USA), loading with 316™ or 318™v2 chip as per manufacturer's protocol. Data analysis, including alignment to the hg19 human reference genome as well as variant calling and filtering, was done using the Torrent Suite Software v.3.6 (Thermo Fisher Scientific, USA). Filtered variants were annotated using Ion Reporter software v4.4 (Thermo Fisher Scientific, USA). Alignments were visually verified with the Integrative Genomics Viewer; v.2.3. The mean coverage achieved was 1361-fold and 2338-fold in the tumor tissues for GDF15 and TP53 sequencing, respectively, and the same deep sequencing was done (two sample in 316™ chip or four sample in 318™v2 chip) on the control tissues. 90% and 95% of the targeted bases were represented by at least 10 reads for GDF15 and TP53, respectively.
Classification of GDF15 mutation
In order to investigate the correlation between missense GDF15 mutations and survival in OSCC patients, the gene status of GDF15 was classified as missense GDF15 mutations and wild-type GDF15.
Classification of TP53 mutation
In order to investigate the correlation between TP53 mutations and GDF15 protein expression in the biopsy samples from OSCC patients, the gene status of TP53 was classified as wild-type TP53, low risk TP53 and high risk TP53 according to the method of Evolutionary Action (EAp53) [23, 28, 29].
Mutation confirmation
Sanger sequencing was used to confirm the DNA variants derived from the PGM. Sequence variants were compared with dbSNP, 1000 Genomes, ClinVar database, COSMIC, 5000Exomes, OMIM, and Pfam. SIFT, Polyphen, Phylop, and Grantham score were used to estimate evolutionary conservation and the effects of the amino acid substitution on the structure and function of the protein.
Immunohistochemical staining against GDF15
Immunohistochemistry was performed as previously described [10]. Briefly, sections were incubated with the rabbit polyclonal antibody against GDF15 (1:100) (Abcam, UK) overnight at 4°C and visualized using 3,3′-diaminobenzidine (DAB) detection kit (Dako Cytomation, Denmark) containing goat secondary antibody molecules against rabbit immunoglobulin and DAB chromogen. Negative control was performed by using PBS instead of anti-GDF15 antibody. Two pathologists performed blind examination with a microscope. The GDF15 positive proportion score was the percentage ratio of positive GDF15-stained tumor cells to the total number of tumor cells, classified as: 0 (0%), 1 (1–10%), 2 (11–50%), 3 (51–80%), 4 (>80%). The GDF15 intensity score was the staining intensity by visual assessment and was scored as: 0 (negative), 1 (weak), 2 (moderate), and 3 (strong).
Statistical analysis
Overall survival was calculated from the date of pathological diagnosis to the date of death; disease-free survival/locoregional recurrence-free survival/distant metastasis-free survival were calculated, respectively, from the date of pathological diagnosis to recurrence/locoregional recurrence/distant metastasis or death from any cause. For descriptive analysis, categorical data were expressed as number and percentage. Chi-square test was applied to compare the difference between the baseline characteristics and GDF15 mutation and expression. The survival analysis was conducted using the Kaplan-Meier method. Hazard ratios (HR) were calculated using the Cox proportional hazards model. All hypothesis-generating tests were two-sided at a significance level of 0.05. Data were analyzed with the statistical software SPSS18.0 for Windows (SPSS Inc., USA).
ACKNOWLEDGMENTS
This study was supported by research grants 81272979 and 81472519 from National Natural Science Foundation of China; by research grant 13QH1401700 from Science and Technology Commission of Shanghai Municipality; by research grant 201447 from Shanghai Municipal Human Resources and Social Security Bureau; by research grant 15ZH2008 from Shanghai Jiao Tong University School of Medicine.
CONFLICTS OF INTEREST
The authors have no potential conflicts of interest to disclose.
REFERENCES
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA: a cancer journal for clinicians. 2015; 65:87–108.
2. Leemans CR, Braakhuis BJ, Brakenhoff RH. The molecular biology of head and neck cancer. Nature reviews cancer. 2011; 11:9–22.
3. Bootcov MR, Bauskin AR, Valenzuela SM, Moore AG, Bansal M, He XY, Zhang HP, Donnellan M, Mahler S, Pryor K, Walsh BJ, Nicholson RC, Fairlie WD, et al. MIC-1, a novel macrophage inhibitory cytokine, is a divergent member of the TGF-beta superfamily. Proceedings of the National Academy of Sciences of the United States of America. 1997; 94:11514–11519.
4. Osada M, Park HL, Park MJ, Liu JW, Wu G, Trink B, Sidransky D. A p53-type response element in the GDF15 promoter confers high specificity for p53 activation. Biochemical and biophysical research communications. 2007; 354:913–918.
5. Tan M, Wang Y, Guan K, Sun Y. PTGF-beta, a type beta transforming growth factor (TGF-beta) superfamily member, is a p53 target gene that inhibits tumor cell growth via TGF-beta signaling pathway. Proceedings of the National Academy of Sciences of the United States of America. 2000; 97:109–114.
6. Breit SN, Johnen H, Cook AD, Tsai VW, Mohammad MG, Kuffner T, Zhang HP, Marquis CP, Jiang L, Lockwood G, Lee-Ng M, Husaini Y, Wu L, et al. The TGF-beta superfamily cytokine, MIC-1/GDF15: a pleotrophic cytokine with roles in inflammation, cancer and metabolism. Growth factors. 2011; 29:187–195.
7. Mimeault M, Batra SK. Divergent molecular mechanisms underlying the pleiotropic functions of macrophage inhibitory cytokine-1 in cancer. Journal of cellular physiology. 2010; 224:626–635.
8. Schiegnitz E, Kammerer PW, Koch FP, Kruger M, Berres M, Al-Nawas B. GDF 15 as an anti-apoptotic, diagnostic and prognostic marker in oral squamous cell carcinoma. Oral oncology. 2012; 48:608–614.
9. Zhang L, Yang X, Pan HY, Zhou XJ, Li J, Chen WT, Zhong LP, Zhang ZY. Expression of growth differentiation factor 15 is positively correlated with histopathological malignant grade and in vitro cell proliferation in oral squamous cell carcinoma. Oral oncology. 2009; 45:627–632.
10. Yang CZ, Ma J, Zhu DW, Liu Y, Montgomery B, Wang LZ, Li J, Zhang ZY, Zhang CP, Zhong LP. GDF15 is a potential predictive biomarker for TPF induction chemotherapy and promotes tumorigenesis and progression in oral squamous cell carcinoma. Annals of oncology. 2014; 25:1215–1222.
11. Song X, Xia R, Li J, Long Z, Ren H, Chen W, Mao L. Common and complex Notch1 mutations in Chinese oral squamous cell carcinoma. Clinical cancer research. 2014; 20:701–710.
12. Izumchenko E, Sun K, Jones S, Brait M, Agrawal N, Koch W, McCord CL, Riley DR, Angiuoli SV, Velculescu VE, Jiang WW, Sidransky D. Notch1 mutations are drivers of oral tumorigenesis. Cancer prevention research (Philadelphia, Pa). 2015; 8:277–286.
13. Brown DA, Lindmark F, Stattin P, Bälter K, Adami HO, Zheng SL, Xu J, Isaacs WB, Grönberg H, Breit SN, Wiklund FE. Macrophage inhibitory cytokine 1: a new prognostic marker in prostate cancer. Clinical cancer research. 2009; 15:6658–6664.
14. Wallin U, Glimelius B, Jirström K, Darmanis S, Nong RY, Pontén F, Johansson C, Påhlman L, Birgisson H. Growth differentiation factor 15: a prognostic marker for recurrence in colorectal cancer. British journal of cancer. 2011; 104:1619–1627.
15. Staff AC, Bock AJ, Becker C, Kempf T, Wollert KC, Davidson B. Growth differentiation factor-15 as a prognostic biomarker in ovarian cancer. Gynecologic oncology. 2010; 118:237–243.
16. Staff AC, Trovik J, Eriksson AG, Wik E, Wollert KC, Kempf T, Salvesen HB. Elevated plasma growth differentiation factor-15 correlates with lymph node metastases and poor survival in endometrial cancer. Clinical cancer research. 2011; 17:4825–4833.
17. Bauskin AR, Zhang HP, Fairlie WD, He XY, Russell PK, Moore AG, Brown DA, Stanley KK, Breit SN. The propeptide of macrophage inhibitory cytokine (MIC-1), a TGF-beta superfamily member, acts as a quality control determinant for correctly folded MIC-1. The EMBO journal. 2000; 19:2212–2220.
18. Bauskin AR, Brown DA, Junankar S, Rasiah KK, Eggleton S, Hunter M, Liu T, Smith D, Kuffner T, Pankhurst GJ, Johnen H, Russell PJ, Barret W, et al. The propeptide mediates formation of stromal stores of PROMIC-1: role in determining prostate cancer outcome. Cancer research. 2005; 65:2330–2336.
19. Griner SE, Joshi JP, Nahta R. Growth differentiation factor 15 stimulates rapamycin-sensitive ovarian cancer cell growth and invasion. Biochemical pharmacology. 2013; 85:46–58.
20. Joshi JP, Brown NE, Griner SE, Nahta R. Growth differentiation factor 15-mediated HER2 phosphorylation reduces trastuzumab sensitivity of HER2-overexpressing breast cancer cells. Biochemical pharmacology. 2011; 82:1090–1099.
21. Lee DH, Yang Y, Lee SJ, Kim KY, Koo TH, Shin SM, Song KS, Lee YH, Kim YJ, Lee JJ, Choi I, Lee JH. Macrophage inhibitory cytokine-1 induces the invasiveness of gastric cancer cells by up-regulating the urokinase-type plasminogen activator system. Cancer research. 2003; 63:4648–4655.
22. Kim KK, Lee JJ, Yang Y, You KH, Lee JH. Macrophage inhibitory cytokine-1 activates AKT and ERK-1/2 via the transactivation of ErbB2 in human breast and gastric cancer cells. Carcinogenesis. 2008; 29:704–712.
23. Neskey DM, Osman AA, Ow TJ, Katsonis P, McDonald T, Hicks SC, Hsu TK, Pickering CR, Ward A, Patel A, Yordy JS, Skinner HD, Giri U, et al. Evolutionary action score of TP53 identifies high-risk mutations associated with decreased survival and increased distant metastases in head and neck cancer. Cancer research. 2015; 75:1527–1536.
24. Lindenbergh-van der Plas M, Brakenhoff RH, Kuik DJ, Buijze M, Bloemena E, Snijders PJ, Leemans CR, Braakhuis BJ. Prognostic significance of truncating TP53 mutations in head and neck squamous cell carcinoma. Clinical cancer research. 2011; 17:3733–3741.
25. Poeta ML, Manola J, Goldwasser MA, Forastiere A, Benoit N, Califano JA, Ridge JA, Goodwin J, Kenady D, Saunders J, Westra W, Sidransky D, Koch WM. TP53 mutations and survival in squamous-cell carcinoma of the head and neck. New England journal of medicine. 2007; 357:2552–2561.
26. Gross AM, Orosco RK, Shen JP, Egloff AM, Carter H, Hofree M, Choueiri M, Coffey CS, Lippman SM, Hayes DN, Cohen EE, Grandis JR, Nguyen QT, Ideker T. Multi-tiered genomic analysis of head and neck cancer ties TP53 mutation to 3p loss. Nature genetics. 2014; 46:939–943.
27. Brosh R, Rotter V. When mutants gain new powers: news from the mutant p53 field. Nature reviews cancer. 2009; 9:701–713.
28. Osman AA, Neskey DM, Katsonis P, Patel AA, Ward AM, Hsu TK, Hicks SC, McDonald TO, Ow TJ, Alves MO, Pickering CR, Skinner HD, Zhao M, et al. Evolutionary action score of TP53 coding variants is predictive of platinum response in head and neck cancer patients. Cancer research. 2015; 75:1205–1215.
29. Osman AA, Monroe MM, Ortega Alves MV, Patel AA, Katsonis P, Fitzgerald AL, Neskey DM, Frederick MJ, Woo SH, Caulin C, Hsu TK, McDonald TO, Kimmel M, et al. Wee-1 kinase inhibition overcomes cisplatin resistance associated with high-risk TP53 mutations in head and neck cancer through mitotic arrest followed by senescence. Molecular cancer therapeutics. 2015; 14:608–619.