
INTRODUCTION
Liver cancer is a leading cause of cancer deaths, accounting for more than 700,000 deaths per year worldwide. Current clinical risk predictions in hepatocellular carcinoma (HCC) are based on histopathological evaluation of the primary tumour tissue obtained during surgery. The Tumour-Node-Metastasis (TNM) staging system of the American Joint Committee on Cancer (AJCC)/International Union Against Cancer (UICC) has been verified to be valuable in the outcome estimation of patients with a variety of tumours. However, this traditional cancer staging system, which is based only on tumour invasion parameters, provides limited information in the estimation of the post-operative outcome of HCC patients. In some tumours, patients within the same histological tumour stage had clinical outcomes that varied significantly [1-2]. The focal point of this traditional classification is primarily on the tumour cells and pays essentially no attention to the effects of the host immune response. Recently, considerable data from large cohorts of various tumours have demonstrated that the number, type and location of tumour-infiltrating lymphocytes (TILs) are essential for the prediction of clinical outcome [3-8]. Based on these studies, Galon et al. recommended that IS should be used as a new prognostic tool and a component of cancer classification [5]; IS was further confirmed to be beneficial for the prognosis of disease-free survival (DFS) and overall survival (OS), particularly in early-stage cancers [9]. The fundamental parameter of the IS classification includes the density of the CD3+ and CD8+ T cells at the centre of the tumour (CT) and at its invasive margin (IM), which has previously been extensively used in a variety of tumour types, including colon, rectal, melanoma and breast cancers [3-5, 7-10].
However, the predictive role of IS in patients with HCC who underwent resection remains unknown. In this study, IS was highly correlated to the outcome of HCC patients (n = 359) if compared with TNM or BLCL staging, however, IS seems not to be the best prognostic factor. Among CD8CT, CD8IM, CD3CT, CD3IM and IS, CD8CT works as an independent indicator, demonstrating the highest prognostic impact not only on DFS and OS, but also on tumour relapse, tumour size and serum levels of ALT and AST in Cox multivariate regression analysis. We recommend that optimum cut-off value is 93 CD8CT cells per mm2, to be used to divide the patients into CD8CTHi group and CD8CTLo group in clinical settings. Our results suggest that CD8CT densities analysis improved the survival prediction with convenience of clinical manipulation in HCC.
RESULTS
Positive correlations of the densities of CD3+ or CD8+ cells/mm2 in centre tumour but not peritumour to overall survival in cohort 1
It has been observed that CD8+ lymphocytes infiltrated in HCC, which likewise has been correlated with the tumour progression [11]. However, the different densities of immune cells within different tumour regions and the clinical outcome of patients have never been reported in HCC. In this study, we used commercially available tissue microarray (TMA) from one HCC cohort with 90 patients and examined the distributions of CD3+ T cells and CD8+ T cells in HCC tissues through two identical TMAs, followed by immunostaining. The CD3+ and CD8+ T cells in the centre tumour (CT) and peritumour tissues (PT) from 12 representative samples are shown in Figure S1A-B, which demonstrated that the distribution and density of these lymphocytes varied in different HCC areas. Cox regression with time-to-event outcome analysis demonstrated that no positive correlations of the number of CD3+ or CD8+ cells/mm2 in the CT and PT regions to overall survival (OS) have been identified primarily due to the small sample size (Table. S2).To further assess the predictive potential of CD3+ or CD8+ cell densities in different tumour regions (CT and PT), the patients were divided into two groups using the minimum P-value cut-off values for CD3 or CD8 densities in each tumour region (Cut-off values were 214, 375, 97, and 186 for CD3CT, CD3PT, CD8CT and CD8PT, respectively). As expected, the survival curve by sub grouping showed that higher CD3+ or CD8+ cell densities in the CT (Figure 1A) but not PT (Figure 1B) regions from the HCC patients were correlated with longer OS (log-rank test corrected P < 0.05 for both CD3CT and CD8CT). Taken together, this small cohort study suggests that the distribution and their densities of CD3+ and CD8+ T cells in centre tumour regions have the predictive value for HCC progression.
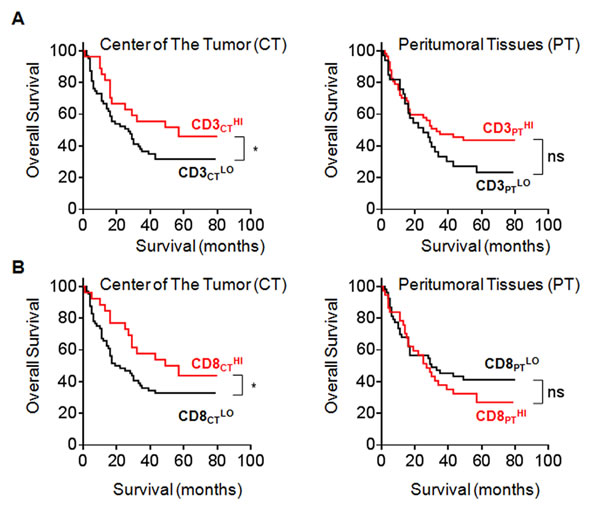
Figure 1: Correlation between the number of CD3+ or CD8+ cells/mm2 and OS in CT and PT regions. A., B. Kaplan-Meier curves for the duration in months of OS according to CD3+ A. and CD8+ B. cells densities evaluated in each tumour regions (CT and PT) (High densities, red line; Low densities, black line). Cut-off values were 214, 375, 97, and 186 cells/mm2 for CD3CT, CD3PT, CD8CT and CD8PT, respectively. In A. and B., log-rank statistical test, *, P < 0.05.
CD3+ or CD8+ T cells in invasive margin and centre tumour in a large cohort 2
It has been recognised that immune cells are scattered in the invasive margin (IM) tumour in addition to the CT and PT regions; however, the predictive role of CD3+ or CD8+ T cell density in the IM regions in HCC has not been addressed. Since the commercial supply of the HCC sample in Cohort 1 contains only PT and CT but not IM regions, we further investigated the role of the IM-infiltrating CD3+ or CD8+ T cells using TMAs containing CT and IM regions resection specimens from 359 HCC patients (Cohort 2). The strategy of designating tissue cores for TMAs from the tumour centre and the invasive margin was shown in Figure S3A. These tissue sections may clearly be divided into CT and IM regions and clearly demonstrate high or low densities of CD3+ or CD8+ T cells, according to the method described by Galonet et al. [4]. For the purpose of accuracy, in addition to the TMAs, the whole sections from 21 HCC patients were also used to investigate the expression of CD3+ and CD8+lymphocytes. Two representative sections exhibited the distinct high-density infiltrating areas of immune cells in the IM regions (Figure 2A). The double staining of CD3+ and CD8+ cells in the HCC tissue demonstrated that the lymphocyte densities differed significantly between the CT and IM regions, with a higher density and larger area of lymphocytes in the IM region (Figure 2B, Figure S3B). Consistent with this finding, the average number of CD3IM or CD8IM T cells was significantly higher than those of CD3CT or CD8CT T cells (P < 0.0001 for both) (Figure 2C); together, these findings suggest the IM T cell is a potential candidate indicator in the prediction of HCC prognosis.
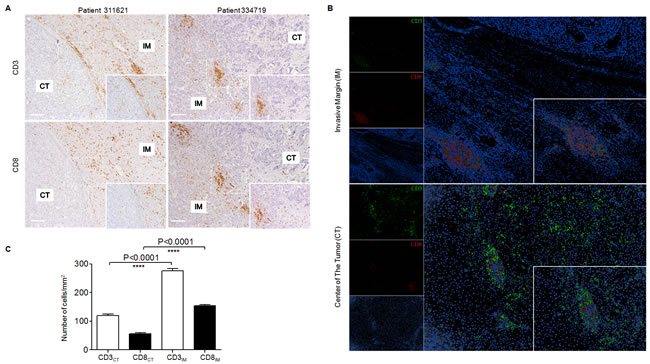
Figure 2: Different densities and locations of CD3+ or CD8+ cells in HCCpatients. A. Adjacent sections of paraffin-embedded hepatoma samples stained with anti-CD3 or anti-CD8 antibodies. Representative micrographs showing infiltrating CD3+ lymphocytes (Top) andCD8+ lymphocytes (Bottom) in the IM regions from 2 HCC patients (Left Pts311621: Capsule positive; Right Pts334719: Capsule negative). Original magnifications: ×10, ×20. B. Representative micrographs showing double staining of CD3+ and CD8+ cells in the IM region (Top) and CT region (Bottom), and Adobe Photoshop was used to convert the immunohistochemical staining to fluorescence. Original magnifications: ×10, ×40. C. Density of CD3+ (White) and CD8+ (Black) cells in the IM and CT regions were shown, respectively. Statistical significance were analysed by the one-way ANOVA test. ****, P < 0.0001.
To further assess the impact of different density of immune cells in each tumour region in HCC patients, we analysed the correlation between the immune cell densities in the CT and IM regions and the survival time of the patients from Cohort 2. As shown in TableS2, statistical analysis demonstrated that significant positive correlations of the number of CD3+ or CD8+ cells/mm2 in both CT and IM regions to disease-free survival (DFS) or overall survival (OS) have been identified (P < 0.0001 in all comparisons) due to the relatively large sample size. Moreover, the patients with higher density of CD3+ or CD8+cellin both CT and the IM regions had significantly lower tumour recurrence (n = 184), and those with lower density of T cells had higher tumour recurrence (n = 175) (Figure 3A).
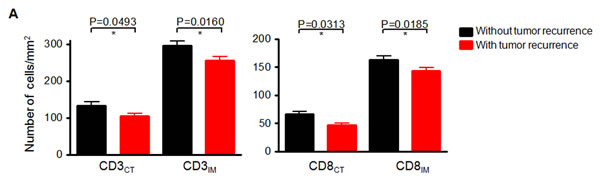
Figure 3: Negative correlation between the number of CD3+ or CD8+ cells/mm2 and tumour recurrence in HCC patients. A. Comparison of the immune cell densities in the CT and IM regions from patients with (Red bars) or without (Black bars) tumour recurrence. Comparisons were performed using Mann-Whitney test, P values are shown.
We next divided these patients into two groups according to the minimum P-value cut-offs for CD3+ or CD8+ density (164, 324, 93, and 164 for CD3CT, CD3IM, CD8CT, CD8IM , respectively) in each tumour region. The patients with high densities of CD3+or CD8+T cells in both CT and IM regions in Cohort 2 exhibited significantly longer DFS and OS (P < 0.0001 for all comparisons) (Figure 4A, 4B), almost similar to the performance of CD3+or CD8+ T cells in CT region in Cohort 1 (Figure 1). Importantly, among the four positive indicators (CD8CTHi, CD8IMHi, CD3CTHi, CD3IMHi), CD8CTHi and CD3CTHi were more efficient to predict DFS and OS (all log-rank test corrected P < 0.0001) when compared with CD8IMHi and CD3IMHi on Kaplan-Meier curves.
Univariate analysis further showed that TNM staging, T stage, tumour number, thrombus, CD8CTHi, CD8IMHi, CD3CTHi, and CD3IMHi significantly influenced DFS and OS (P < 0.05 for all comparisons in Table 1), respectively. However, among these indicators, lymphocytes in CT region were more positively influential on DFS and OS than those in IM region, and CD8+ T cells had more impact on DFS and OS than CD3+ T cells (HRs were 0.5 and 0.49 for CD3IM, 0.6 and 0.58 for CD8IM, 0.38 and 0.35 for CD3CT, 0.23 and 0.16 for CD8CT for DFS and OS, respectively; all P < 0.0004; Table 1). Next, patients with high density of CD3 or CD8 in both CT and IM regions were classified as “HiHi” group; patients with low density of each marker in both regions were classified as “LoLo” group; patients with a high density of one marker in either one region (CT or IM) were classified as “Het” group. It was also noted that HiHi for CD3+ T cells (HRs = 0.24) and HiHi for CD8+ T cells (HRs = 0.17) had more impact on DFS than LoLo groups (P < 0.0001 for all comparisons; Table 1).
One thing to note is that Univariate analysis showed that HRs did not progressively correlate to the severity of TNM stage (in response to the increasing staging from I to IV, the associated HRs were 1, 2.2, 1.81, 1.89 for DFS, and 1, 2.13, 2.18, 1.8 for OS, respectively) (Table 1), indicating that TNM classification might not be the accurate staging system in predicting the outcome of HCC patients. On the other hand, although there was a good correlation of the tumour size with T stages or UICC-TNM stages (Figure 4C), the CD8CT number alone was not correlated with these stages (Figure 4D), suggestive of TNM staging system could not indicated the immune contexture in the centre of tumour.
Table 1: Univariate Analysis of DFS and OS Among Patients With Liver Cancer (cohort 2) According to Clinical or Immune Parameters.
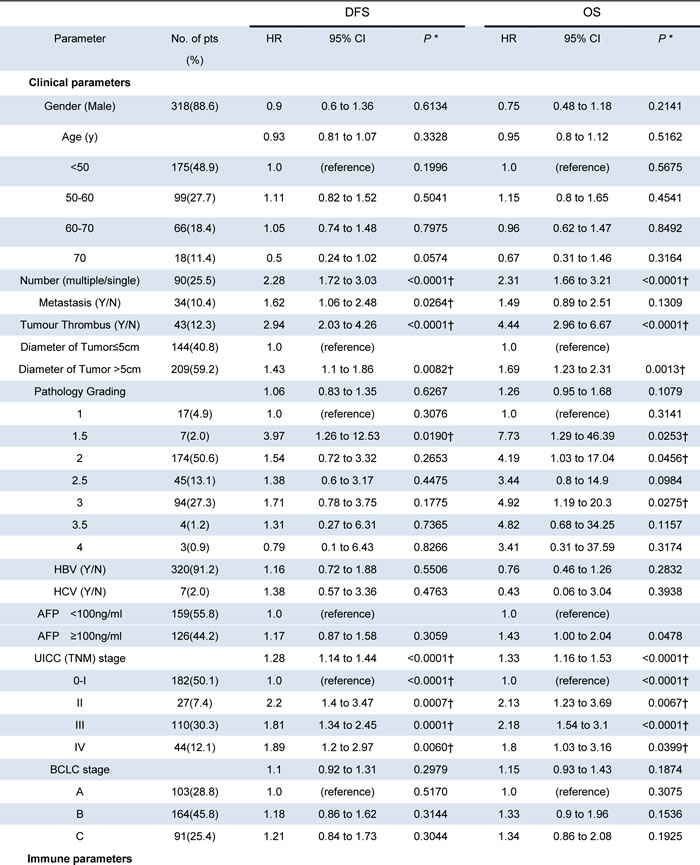
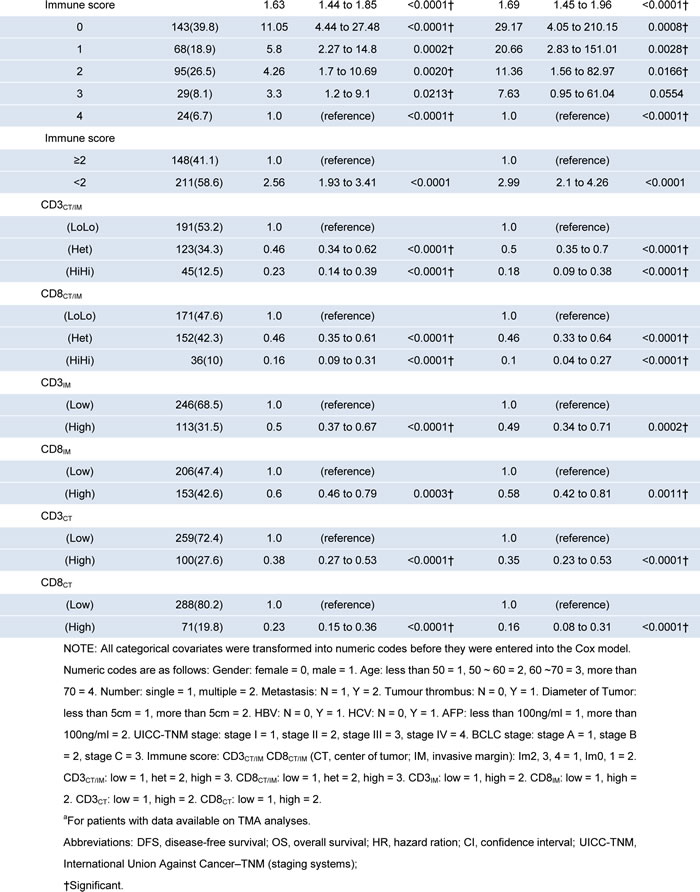
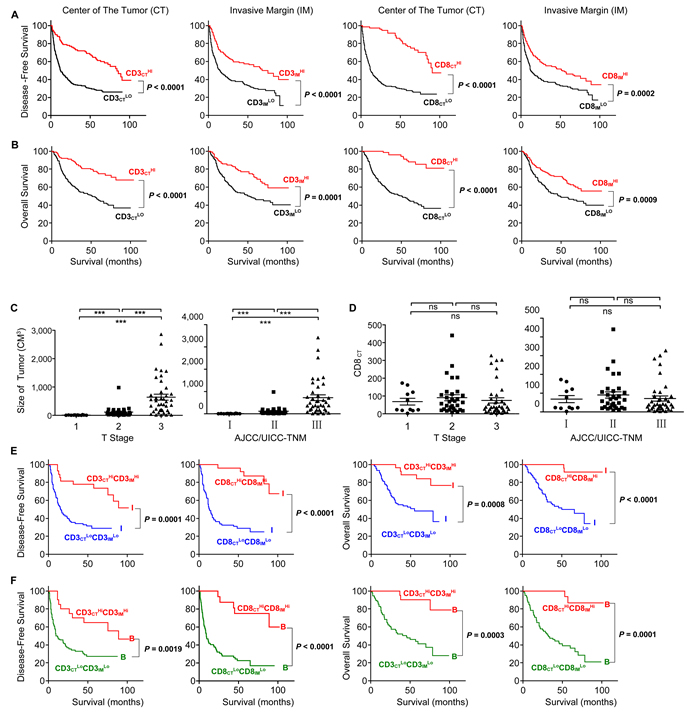
Figure 4: Increased survival time for the patients with high densities of CD3+ or CD8+ cells. Kaplan-Meier curves for the duration in months of DFS A. and OS B. according to CD3+ or CD8+ cells densities evaluated in each tumour regions (CT and IM) (High densities, Red line; Low densities, Black line). The tumour size C. and the density of CD8+ lymphocytes D. in the CT regions were compared with different T stages and AJCC/UICC-TNM stages, respectively. E. The TNM-I stage HCC patients were divided into two groups according to different densities of CD3+ or CD8+ cells in the combined tumour regions (CT and IM) (e.g. CD3CTHiCD3IMHi, CD3CTLoCD3IMLo, CD8CTHiCD3IMHi and CD8CTLoCD3IMLo; LoLo, blue lines; HiHi, red lines). Kaplan-Meier curves illustrated the durations of OS and DFS in each group. F. The BLCL-B stage HCC patients were divided into two groups according to different densities of CD3+ or CD8+ cells in the combined tumour regions (CT and IM) (e.g. CD3CTHiCD3IMHi, CD3CTLoCD3IMLo, CD8CTHiCD3IMHi and CD8CTLoCD3IMLo; LoLo, green lines; HiHi, red lines). Kaplan-Meier curves illustrated the durations of OS and DFS in each group. In Kaplan-Meier curves, log-rank statistical test, P values are shown.
CD8CT is a better indicator than IS to predict the prognosis of HCC
As expected, a combinational analysis of CD3 (e.g. CD3CTHi CD3IMHi vs. CD3CTLo CD3IMLo) efficiently predicted the HCC survival even within same TNM-I stage (Figure 4E) or BLCL-B stage (Figure 4F) patients, which might be repeated by a combinational analysis of location and density of CD8+ T cells [7-8]. We then further investigated whether the combined analysis (e.g. Immunoscore (IS)) of both high and low CD3+ and CD8+ T cell densities in tumour regions (CT or IM) could improve the prediction of patient outcome, which has been successfully used to predict outcome of colon cancer and rectal cancer [5, 10, 12]. The patients were divided into the HiHi (high densities in both regions) and LoLo (low densities in both regions) groups, which had been used in Figure 4; the highest score was 4 (e.g., CD3HiHi plus CD8HiHi), and the lowest score was 0 (e.g., CD3LoLo plus CD8LoLo). As shown in Figure 5A, the IS of the 359 HCC sections were divided into IS-0 (n = 143), IS-1 (n = 68), IS-2 (n = 95), IS-3 (n = 29) and IS-4 (n = 24). We found the DFS (Figure 5A) and OS (Figure 5C) of patients were gradually prolonged if correspondent IS increased: IS-4 (I4) with the longest survival. A strong association was identified between higher IS (IS≧2) and longer DFS and OS, and between lower IS (IS < 2) and shorter DFS and OS (P < 0.0001 for all comparisons) (Figure 5B, 5D), looking like IS was a satisfied marker in predicting survival. In our Cohort 2, however, we did not observe any strong differences in survival of patients subgrouping by TNM or BCLC staging (Figure 5E).Interestingly, when we used IS-2 as a cut-off value, the TNM stage II or III of HCC could be divided into two distinct groups: the patients with IS≧2 in TNM I or TNM III clearly exhibited longer survival compared with the patients with IS < 2 (Figure 5F). Consistent with the TNM classification, the patients with IS≧2 in BLCL-A, B or C also clearly exhibited longer survival (Figure 5F). These findings suggest that IS is a prognostic factor superior to or compensate for the AJCC/UICC TNM classification and BLCL staging for the current classifications in HCC, similar to findings in colorectal cancer and rectal cancer [8, 10].
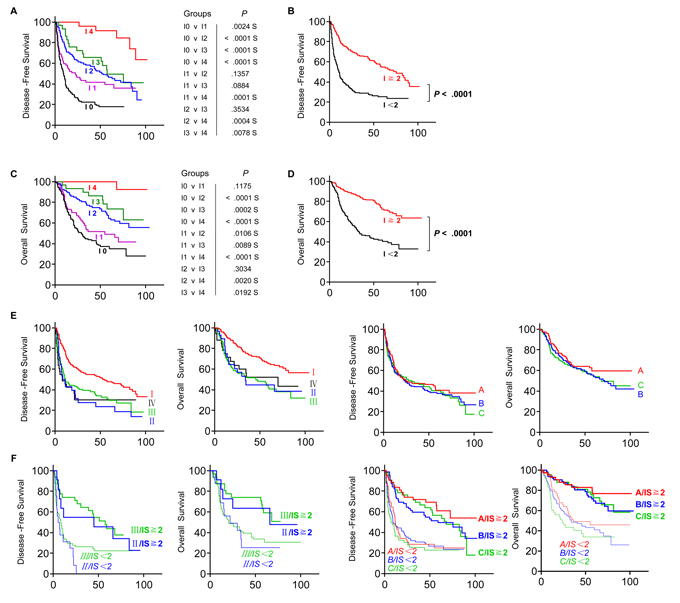
Figure 5: Increased survival time for the patient with high Immunoscore (IS). A. DFS and C. OS of patients with IS 0 (Black), IS 1 (Pink), IS 2 (Blue), IS 3 (Green) or IS 4 (Red) were shown. B. DFS and D. OS of patients with IS ≥2 (Red) and IS < 2 (Black). (E., two lefts) DFS and OS of patients with different TNM stages (TNM-I, Red; TNM-II, Blue; TNM-III, Green; TNM-IV, Black), and (E., two rights) DFS and OS of patients with BLCL-A (Red), BLCL-B (Blue) or BLCL-C (Green) stages. F. DFS and OS of TNM-II (Blue) or -III (Green), or BLCL-A (Red), -B (Blue) or -C (Green) HCC patients with IS ≥2 (Red) and IS < 2 (Black) were illustrated by Kaplan-Meier curves.
To further verify whether IS was an independent predictive tool, we built a multivariate analysis model combining CD8CT, CD8IM, CD3CT, CD3IM, IS and all clinical pathological variables with P < 0.05 from the Univariate analyses. Interestingly, only CD8CT, CD8IM and CD3IM remained significantly correlated to DFS (P = < 0.0001, 0.0107, 0.0017, respectively; Table 2) and only CD8CT and CD8IMsignificantly correlated to OS (P < 0.0001 and 0.0013, respectively; Table 2) in the model after backward-based Cox multivariate analysis. We then performed Cox multivariate regression analysis by adding CD8CT, CD8IM, CD3IM and IS into a model. Interestingly, only CD3IM, CD8IM and CD8CT remained significantly associated with DFS (HR: 0.43, 0.71, 0.17, respectively; P = 0.0004,0.049, < 0.0001; Table 2). Although IS was highly related to the outcome of HCC patients, however, the IS seemed not to be a best prognostic factor than CD8IM and CD8CT. Central CD8+ TIL density has independent and the highest significantly prognostic impact on DFS and OS (Both P < 0.0001; Table 2). When we nominated CD8CT density as a cut-off value, patients with the same TNM stage II or III could be clearly divided into two distinct groups: the patients with higher CD8CT density in TNM II or III stage clearly exhibited longer survival compared with the patients with lower CD8CT density (Figure 6A). A similar effect of division were also observed in the BLCL-A, B or C stage (Figure 6B), indicating that CD8CT density is a more favourite indicator for predictions.
We further observed that CD8CT performance on the disease parameters. It was noted that high densities of CD8CT were highly significantly associated with high levels of alanine aminotransferase (ALT, P = 0.0004) (Figure 6C), aspartate aminotransferase (AST, P = 0.0002) (Figure 6D) and massive tumour volume (P < 0.0001) (Figure 6E), suggesting that CD8CT cell densities also associated with the clinical characteristics of patients. However, no significant difference have been observed in the levels of alpha-fetoprotein (AFP, P = 0.2095) (Figure 6F). We also compared the relationship of IS to clinical characteristics of the HCC patients. The patients with higher IS exhibited a lower rate of recurrence or thrombus, but no correlations of tumour metastasis were observed to IS (Figure S2A).Interestingly, IS scores were also correlated with most clinical parameters, including AST (Figure S2C), AFP (Figure S2D) and tumour volume (Figure S2E), but no significant correlation between the IS and ALT (Figure S2B) or pathological grade (Figure S2F) have been observed. Our results suggest that CD8CT densities analysis notably improved the accuracy of survival prediction if compared with IS, UICC-TNM and BCLC stages. As a result, taking account of convenience of clinical manipulation, we recommend the direct use of CD8CT as an indicator for prognosis. The minimum P value cut-offs value 93 cells/mm2 can be used to divide the patients into CD8CTHi group and CD8CTLo group in clinical settings.
Table 2: Multivariate Cox Proportional Hazard Analysis for DFS and OS Among Patients With Liver Cancer From Cohort 2
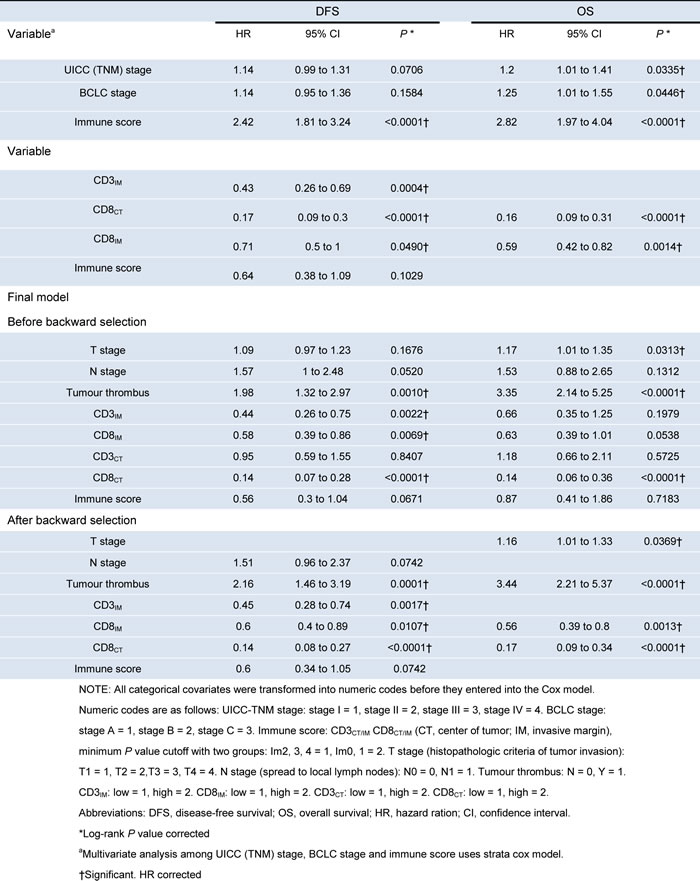
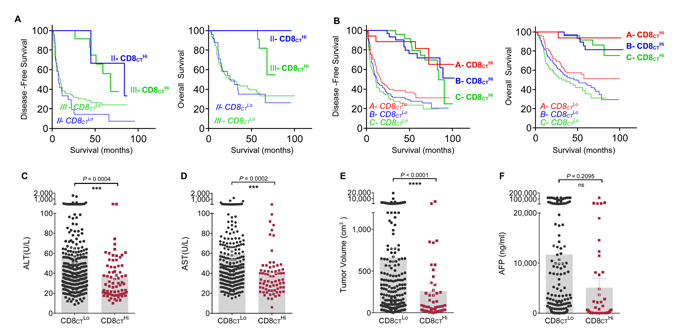
Figure 6: CD8CT directly predicts survival and associates with clinical characteristics of HCC. A. DFS and OS of TNM-II (Blue) or -III (Green), or B. BLCL-A (Red), -B (Blue) or -C (Green) HCC patients with CD8CTHI or CD8CTLo were illustrated by Kaplan-Meier curves. The levels of ALT C., AST D., the tumour volume E. and AFP F. for all HCC patients with CD8CTLo (Black) and CD8CTHi (Red) were analyzed. Cut-off values for CD8CTLo and CD8CTHiwere 93 cells/mm2. Comparisons were made using the Mann Whitney test, P values are shown, ***, P < 0.001, ****, P < 0.0001; ns, no significant.
DISCUSSION
HCC is a major public health problem with an annual incidence of more than 700,000 cases in the world. Simple and effective prognostic markers are needed to predict the survival, which is helpful to avoid under/over treatment in HCC patients in clinic settings. Herein, we evaluated the densities of CD8+ cells and CD3+ cells in PT and IT regions in a small Cohort 1 (90 patients), and observed a positive correlation between densities of lymphocytes and the overall survival time of patients was existed in CT region, but not in PT region. Based on this, we delivered to use a big Cohort 2 (359 patients contain the IM and IT regions) to investigate the prognostic capability of the infiltrated lymphocytes. We observed that patients with higher densities of CD3+or CD8+T cells in both regions exhibited significantly longer DFS and OS (Figure 4A, 4B). In order to more efficiently predict the survival, we combined the indicators of CD3+or CD8+T cells in CT or IM regions into a simple scoring method (IS), as established in colon cancer and rectal cancer [4, 6, 8-10], in our Cohort2. Our results demonstrated that patients with lower IS was significantly associated with poor prognosis, and patients with same TNM stage could even be clearly divided into two distinct groups, suggesting IS has an advantage over or compensates for current TNM tumour classification. However, using multivariate analysis model, we found the prognostic performance of the combinational IS (e.g. combining the density of CD8CT, CD8IM, CD3CT, CD3IM) was not advantaged over single analysis of the density of CD8CT. Patients with higher density of CD8CT cells not only strongest predicted the HCC survival but also associated with significantly high levels of ALT, AST and massive tumour volume (Figure 6C-6E). Importantly, we found that the density cut-off of CD8CT cells (e.g. 93 cells/mm2) can be used in future clinical settings to divide the CD8CTHi group and CD8CTLo group (Figure 4 and Figure S3C). Taken together, our data indicates that the density of CD8CT cells is a better indicator to predict the prognosis of HCC.
The predictive accuracy of IS staging system was first demonstrated in colorectal cancer (CRC) patients in 2006 [12]. Accumulating clinical data have suggested that the prognostic value of IS classification in CRC patients is superior to the AJCC/UICC TNM-classification [4-5, 7-8, 12-13]. Recently, the predictive value of IS system was reported in rectal cancer, melanoma and breast cancers patients [10]. To our knowledge, the predictive role of IS system in HCC has never been reported. As reported by us, the HCC patients with higher ISs are significantly associated with longer DFS and OS compared with lower ISs (Figure 5A, 5C). Univariate Analysis also confirmed the differences between IS and survival in HCC (HR of 1.63 for the DFS and HR of 1.69 for OS, both P < 0.0001; Table 1) is even more significant than that in rectal cancer patients (HR = 1.81, P = 0.0038 for the DFS and HR = 1.72, P = 0.0003 for OS).
Tumour-infiltrating CD8+ T cells have been associated with favourable outcomes for patients with multiple tumour types. In patients with similar-staged urothelial carcinoma, significantly longer DFS and OS have been observed in patients with a higher numbers of CD8+ cells in the CT regions by Kaplan-Meier curve [14]. Multivariate survival analysis revealed that tumour infiltrating CD4+ Thigh/CD8+ Thigh/%Treglow significantly correlated with longer survival time in 212 pancreatic cancer samples [15]. Analogously, this prognostic effect of CD8CT constantly been confirmed in a variety of tumours such as epithelial ovarian cancer [16-17], breast cancer [18], prostate cancer [19], renal cell cancer [20], non-small cell lung cancer [21], colorectal cancer [22] and esophageal cancer [23], suggesting the great potential of tumour-infiltrating CD8+ T cells as a predictor for survival. However, with relatively few reports, the prognostic performance of CD8+ cells is still controversial in HCC. On the one hand, two laboratories have confirmed that CD8+ T lymphocytes in CT regions strongly correlated to longer DFS in HCC [24-25]; on the other hand, interestingly, one of the same laboratory has reported a opposite conclusion in another study [26]. Possible causes for this contradiction are the selection of cut-off value and patient number in cohorts. Both articles used median values as cut-off (median: 35 and 17.74 per HPF, respectively) in two cohorts with patient number 123 and 302, respectively. In our study, based on comparison among several analysis methods and utilization of big cohort, we conclude that the density of CD8CT cells is the most valuable indicator to predict the survival of HCC, with the 93 cells/mm2 as the cut-off value.
It has been observed that tumour infiltrating lymphocytes can influence the outcome of patients with certain tumour types [27].Recent advances demonstrated that a variety of immune cells such as CD4+ (T helper cell), CD45RO+ (memory T cells), CD56+ (NK cells), Foxp3+ (regulatory T cells) and IL-33+ (interleukin-33-producing cells) cells were associated with prolonged survival in liver tumours [28-30], however, comparing which, CD3+ and CD8+ cells were considered as the most promising candidates [5, 7-8, 12, 26]. In this study, the Cox multivariate model showed that CD8CT cell is an independent parameter to better predict the DFS and the OS than other immune-related indicators. Based on our results from Kaplan-Meier curves and Cox multivariate model, the single analysis of central tumour CD8+ density is proved to be sufficient to achieve the desired prognostic power, making this immune prediction become easier, reproducible and even more economic in future practice.
According to univariate analysis, as shown in Table 1, tumour number (HR: 2.28, P < 0.0001), metastasis (HR: 1.62, P = 0.0264), tumour thrombus (HR: 2.94, P < 0.0001) and TNM stage (HR: 1.28, P < 0.0001) were significant prognostic indicators for DFS in the patients. However, a gradual HR decrease of DFS was not observed along with the raise of TNM stages. The BCLC staging, AFP, HBV infection, HCV infection and pathology grading have no statistical prognostic impact on DFS and OS of patients. Regarding tumour recurrence, we found the densities of CD3+ and CD8+ cells were significantly higher in both CT and IM regions in patients without tumour recurrence (Figure 3A). Inversely, patients with tumour relapse predominantly had a low densities of CD3+ and CD8+ cells in both regions of the primary tumour. Consistent with studies of Galon et al, a gradual decrease of the percentage of relapse patients were observed along the increase of ISs (Figure S2A). These data strongly suggests that local immune capacity in tumour regions is critical to prevent tumour recurrence. In addition, although a positive correlation of the tumour size with UICC-TNM stages were observed, the CD8CT number alone was not correlated with TNM stages (Figure 4D), suggesting that tumour classification based on histopathological parameters were lack of providing information about the immune reaction in tumours regions and consequently poor to predicting survival time and tumour recurrence.
Even though the central CD8+ density seems to be biologically meaningful and clinically reproducible, some issues should be considered before a routine clinical examination is initiated. In Cohort 1, we have observed the overall survival difference between patients with different densities of CD8CT (Figure 1). Such differences became even more significantly with the increased number of samples in Cohort 2 (Table S2), indicating a more accurate and reliable predication performance should be determined by a large number of patients.We have counted the positive points of CD8+/CD3+ cells in 50 random patients by pathologist and software respectively. Both calculation results are consistent in linear regression models (for CD3+ cells, R = 0.952; for CD8+ cells, R = 0.978; P < 0.0001 for both). These results verified the availability of software automate measurement(Figure S3). In our results, the overall survival time indeed decreased at 50-60 mouths post surgery. An immune therapeutic boosting for the patients with higher IS such as cytokine-induced killer cell, dendritic cell, natural killer cell therapy and other treatment of active potential T cell responses would be considerable to improve their survival time [31].TMAs in our study are mainly focus on revealing prognostic impact in large populations. Since the importance of sensitivity for every patient in clinical practice, whole slides of tumour regions should be used which can improve the accuracy of tumour localization and density calculation. The digital pathology and image analysis software may also improve the accuracy and comparability.
In summary, our findings confirm and extend to patients with HCC the density of CD8 cells in CT regions as a valuable marker in predicting patient survival time andtumour recurrence. Specifically, patients with the same TNM or BLCL stages could be clearly divided into two groups using the CD8CT density “93 cells/mm2” as a cut-off value. In each stage, patients with CD8CT densities > 93 cells/mm2 have significantly longer survival compared with patients with CD8CT densities < 93 cells/mm2. We further determined that the CD8CT density is a prognostic factor superior to IS classification in the Cox multivariate analysis model. Simple analysis of the density of CD8CT is already met the needs for survival prediction, which is economical and easy to be reproduced in clinical routines. For the first time, our results illustrate the significance of the CD8CT densities as an independent prognostic index in evaluating the prognosis in HCC patients.
MATERIALS AND METHODS
Patients and classification
This study involved two independent cohorts of HCC patients (Table S1).Paraffin-embedded tumour samples were prospectively obtained from 90 patients who underwent curative resection between 2006 and 2009 (designated Cohort 1). The TMAs contained 90 patients diagnosed with HCC in Taizhou Hospital of Zhejiang Province were purchased from Shanghai Outdo Biotech Company. Tumour samples from 359 untreated patients with pathologically confirmed HCC and underwent curative resection between 2002 and 2003 were obtained from the Bank of Tumour Resource at the Sun Yat-Sen University (designated Cohort 2). The main difference between cohort 1 and cohort 2 is the absence/presence of invasive margin (IM). The tissue samples from cohort 1 possess both PT and IT regions, while those from cohort 2 possess PT, IT and IM regions. The clinical characteristics of all patients are summarized in Table S1. The details of all patients have been provided according to REMARK in Table S3 [32]. All tumour samples were anonymously coded in accordance with the Declaration of Helsinki. The protocol of all study cohorts were approved by the Ethical Board of the Institutional Review Board of the University of Science and Technology of China.
Immunohistochemistry
The paraffin sections were dewaxed in xylene and rehydrated with distilled water. Following incubation with antibodies against either human CD3 (LN10) (Leica Biosystems) or human CD8 (SP16) (Biocare), the adjacent sections were stained with DAB Peroxidase Substrate Kit (SK-4100) and VECTOR VIP Peroxidase Substrate Kit (SK-4600) (Vector Laboratories). The positive cells were quantified using ImagePro Plus software (Media Cybernetics).All section stained TMA slides were examined by the reviewers who have no knowledge of any clinical data. Two cores of CT and IM regions were taken from the primary tumour as previously described.
Immunoscore calculation
Precise quantification was performed under the combination of two markers (CD3+ and CD8+) in two regions (CT and IM). High density of each marker in each region recorded as a score and low density without scoring. For instance, Immunoscore 0 (I0) was low densities of both cell types are found in both regions and Immunoscore 4 (I4) was high densities are found in both regions [4-5, 8, 13].
Statistical analysis
Statistical Product and Service Solutions (SPSS) statistics software (version 22.0) was used for all statistical analyses. Kaplan-Meier estimates of survival were used to illustrate the survival curves and to obtain the estimators of the median and survival rates for OS and DFS. The correlation between the densities of immune cells and survival time were using Cox regression with time-to-event outcome analysis. Significant differences between groups were determined using unpaired two-tailed t tests unless otherwise specified; P < 0.05 was considered significantly different.
CONFLICTs OF INTERESTS
The authors declare no conflict of interest.
GRANT SUPPORT
This work was supported by the Ministry of Science & Technology of China (973 Basic Science Project 2013CB944902), Natural Science Foundation of China (#91029303, #31390433, #81302599) and the National Science & Technology Major Projects (2013ZX10002002-002).
REFERENCES
1. Mlecnik B, Bindea G, Pages F and Galon J. Tumor immunosurveillance in human cancers. Cancer metastasis reviews. 2011; 30:5-12.
2. Nagtegaal ID, Quirke P and Schmoll HJ. Has the new TNM classification for colorectal cancer improved care? Nature reviews Clinical oncology. 2012; 9:119-123.
3. Emens LA, Silverstein SC, Khleif S, Marincola FM and Galon J. Toward integrative cancer immunotherapy: targeting the tumor microenvironment. Journal of translational medicine. 2012; 10:70.
4. Galon J, Pages F, Marincola FM, Angell HK, Thurin M, Lugli A, Zlobec I, Berger A, Bifulco C, Botti G, Tatangelo F, Britten CM, Kreiter S, Chouchane L, Delrio P, Arndt H, et al. Cancer classification using the Immunoscore: a worldwide task force. Journal of translational medicine. 2012; 10:205.
5. Galon J, Pages F, Marincola FM, Thurin M, Trinchieri G, Fox BA, Gajewski TF and Ascierto PA. The immune score as a new possible approach for the classification of cancer. Journal of translational medicine. 2012; 10:1.
6. Angell H and Galon J. From the immune contexture to the Immunoscore: the role of prognostic and predictive immune markers in cancer. Current opinion in immunology. 2013; 25:261-267.
7. Galon J, Angell HK, Bedognetti D and Marincola FM. The continuum of cancer immunosurveillance: prognostic, predictive, and mechanistic signatures. Immunity. 2013; 39:11-26.
8. Galon J, Mlecnik B, Bindea G, Angell HK, Berger A, Lagorce C, Lugli A, Zlobec I, Hartmann A, Bifulco C, Nagtegaal ID, Palmqvist R, Masucci GV, Botti G, Tatangelo F, Delrio P, et al. Towards the introduction of the ‘Immunoscore’ in the classification of malignant tumours. The Journal of pathology. 2014; 232:199-209.
9. Ascierto PA, Capone M, Urba WJ, Bifulco CB, Botti G, Lugli A, Marincola FM, Ciliberto G, Galon J and Fox BA. The additional facet of immunoscore: immunoprofiling as a possible predictive tool for cancer treatment. Journal of translational medicine. 2013; 11:54.
10. Anitei MG, Zeitoun G, Mlecnik B, Marliot F, Haicheur N, Todosi AM, Kirilovsky A, Lagorce C, Bindea G, Ferariu D, Danciu M, Bruneval P, Scripcariu V, Chevallier JM, Zinzindohoue F, Berger A, et al. Prognostic and predictive values of the immunoscore in patients with rectal cancer. Clinical cancer research : an official journal of the American Association for Cancer Research. 2014; 20:1891-1899.
11. Ikeguchi M, Oi K, Hirooka Y and Kaibara N. CD8+ lymphocyte infiltration and apoptosis in hepatocellular carcinoma. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2004; 30:53-57.
12. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pages C, Tosolini M, Camus M, Berger A, Wind P, Zinzindohoue F, Bruneval P, Cugnenc PH, Trajanoski Z, Fridman WH and Pages F. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science. 2006; 313:1960-1964.
13. Galon J, Fridman WH and Pages F. The adaptive immunologic microenvironment in colorectal cancer: a novel perspective. Cancer research. 2007; 67:1883-1886.
14. Sharma P, Shen Y, Wen S, Yamada S, Jungbluth AA, Gnjatic S, Bajorin DF, Reuter VE, Herr H, Old LJ and Sato E. CD8 tumor-infiltrating lymphocytes are predictive of survival in muscle-invasive urothelial carcinoma. Proc Natl Acad Sci U S A. 2007; 104:3967-3972.
15. Ino Y, Yamazaki-Itoh R, Shimada K, Iwasaki M, Kosuge T, Kanai Y and Hiraoka N. Immune cell infiltration as an indicator of the immune microenvironment of pancreatic cancer. Br J Cancer. 2013; 108:914-923.
16. Sato E, Olson SH, Ahn J, Bundy B, Nishikawa H, Qian F, Jungbluth AA, Frosina D, Gnjatic S, Ambrosone C, Kepner J, Odunsi T, Ritter G, Lele S, Chen YT, Ohtani H, et al. Intraepithelial CD8+ tumor-infiltrating lymphocytes and a high CD8+/regulatory T cell ratio are associated with favorable prognosis in ovarian cancer. Proc Natl Acad Sci U S A. 2005; 102:18538-18543.
17. Hamanishi J, Mandai M, Iwasaki M, Okazaki T, Tanaka Y, Yamaguchi K, Higuchi T, Yagi H, Takakura K, Minato N, Honjo T and Fujii S. Programmed cell death 1 ligand 1 and tumor-infiltrating CD8+ T lymphocytes are prognostic factors of human ovarian cancer. Proc Natl Acad Sci U S A. 2007; 104:3360-3365.
18. Mahmoud SM, Paish EC, Powe DG, Macmillan RD, Grainge MJ, Lee AH, Ellis IO and Green AR. Tumor-infiltrating CD8+ lymphocytes predict clinical outcome in breast cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2011; 29:1949-1955.
19. Karja V, Aaltomaa S, Lipponen P, Isotalo T, Talja M and Mokka R. Tumour-infiltrating lymphocytes: A prognostic factor of PSA-free survival in patients with local prostate carcinoma treated by radical prostatectomy. Anticancer Res. 2005; 25:4435-4438.
20. Nakano O, Sato M, Naito Y, Suzuki K, Orikasa S, Aizawa M, Suzuki Y, Shintaku I, Nagura H and Ohtani H. Proliferative activity of intratumoral CD8(+) T-lymphocytes as a prognostic factor in human renal cell carcinoma: clinicopathologic demonstration of antitumor immunity. Cancer research. 2001; 61:5132-5136.
21. Kawai O, Ishii G, Kubota K, Murata Y, Naito Y, Mizuno T, Aokage K, Saijo N, Nishiwaki Y, Gemma A, Kudoh S and Ochiai A. Predominant infiltration of macrophages and CD8(+) T Cells in cancer nests is a significant predictor of survival in stage IV nonsmall cell lung cancer. Cancer. 2008; 113:1387-1395.
22. Pages F, Berger A, Camus M, Sanchez-Cabo F, Costes A, Molidor R, Mlecnik B, Kirilovsky A, Nilsson M, Damotte D, Meatchi T, Bruneval P, Cugnenc PH, Trajanoski Z, Fridman WH and Galon J. Effector memory T cells, early metastasis, and survival in colorectal cancer. N Engl J Med. 2005; 353:2654-2666.
23. Schumacher K, Haensch W, Roefzaad C and Schlag PM. Prognostic significance of activated CD8(+) T cell infiltrations within esophageal carcinomas. Cancer research. 2001; 61:3932-3936.
24. Wada Y, Nakashima O, Kutami R, Yamamoto O and Kojiro M. Clinicopathological study on hepatocellular carcinoma with lymphocytic infiltration. Hepatology. 1998; 27:407-414.
25. Cai XY, Gao Q, Qiu SJ, Ye SL, Wu ZQ, Fan J and Tang ZY. Dendritic cell infiltration and prognosis of human hepatocellular carcinoma. J Cancer Res Clin Oncol. 2006; 132:293-301.
26. Gao Q, Qiu SJ, Fan J, Zhou J, Wang XY, Xiao YS, Xu Y, Li YW and Tang ZY. Intratumoral balance of regulatory and cytotoxic T cells is associated with prognosis of hepatocellular carcinoma after resection. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2007; 25:2586-2593.
27. Taube JM. Emerging immunologic biomarkers: setting the (TNM-immune) stage. Clinical cancer research : an official journal of the American Association for Cancer Research. 2014; 20:2023-2025.
28. Brunner SM, Rubner C, Kesselring R, Martin M, Griesshammer E, Ruemmele P, Stempfl T, Teufel A, Schlitt HJ and Fichtner-Feigl S. Tumor-infiltrating, interleukin-33-producing effector-memory CD8 T cells in resected hepatocellular carcinoma prolong patient survival. Hepatology. 2015.
29. Takata Y, Nakamoto Y, Nakada A, Terashima T, Arihara F, Kitahara M, Kakinoki K, Arai K, Yamashita T, Sakai Y, Mizukoshi E and Kaneko S. Frequency of CD45RO+ subset in CD4+CD25(high) regulatory T cells associated with progression of hepatocellular carcinoma. Cancer Lett. 2011; 307:165-173.
30. Sun C, Sun H, Zhang C and Tian Z. NK cell receptor imbalance and NK cell dysfunction in HBV infection and hepatocellular carcinoma. Cell Mol Immunol. 2015; 12:292-302.
31. Sun C, Sun HY, Xiao WH, Zhang C and Tian ZG. Natural killer cell dysfunction in hepatocellular carcinoma and NK cell-based immunotherapy. Acta Pharmacol Sin. 2015.
32. McShane LM, Altman DG, Sauerbrei W, Taube SE, Gion M and Clark GM. Reporting recommendations for tumor marker prognostic studies (REMARK). J Natl Cancer Inst. 2005; 97:1180-1184.