
INTRODUCTION
The multi-targeted anaplastic lymphoma kinase (ALK) inhibitor crizotinib has demonstrated significant improvement in progression-free survival (PFS) over chemotherapy as both first-line or second-line treatment of ALK-rearranged non-small cell lung cancer (NSCLC) [1, 2] and has firmly established that ALK rearrangement is a targetable driver mutation in NSCLC. ALK breakapart fluorescence in situ (FISH) was until recently the only companion diagnostic assay approved by the US Food and Drug Administration (FDA) for the detection of ALK rearrangement [3]. ALK IHC has been approved as a companion diagnostic kit in other countries such as China and Taiwan and in the US in June, 2015.
ALK rearrangement has also been identified in 0.4% to 2.5% of colorectal carcinoma (CRC) by exon array profiling [4], fluorescence in situ hybridization (FISH) [5], and next generation sequencing (NGS) [6] assays performed on archival tumor specimens. Given the relative low incidence of ALK rearrangement in CRC and the unknown clinical significance of this rearrangement in CRC, a routine and cost-effective diagnostic assay is needed to allow broad screening for ALK rearrangement in CRC and identify these patients for potential enrollment into clinical trials. ALK immunohistochemistry (IHC) has been shown to be sensitive and specific and cost effective to screen for ALK rearrangement in NSCLC [7]. Given that both ALK and ROS1 rearrangements have been identified in CRC [5] and we have previously identified ROS1 rearrangement in GC [8], we performed a screening study for ALK rearrangement in GC and CRC using ALK IHC.
RESULTS
Patient characteristics
A total of 172 CRC and 432 GC patient samples were analyzed by ALK IHC. Primary site of CRC was colon in 100 patients (58.1%) and rectum in 72 patients (41.9%) (Table 1). For the GC patients group, slightly more than half of patients (53.3%) presented with distal GC (Table 2).
Table 1: Characteristics of the colorectal adenocarcinoma patients screened (N = 172)
Characteristic |
Number |
(%) |
Age (years) |
59 |
(28–84) |
Sex |
103 |
(59.9) |
Primary site |
100 |
(58.1) |
Operation |
54 |
(31.4) |
Pathologic stage |
20 |
(11.6) |
Gross type |
151 |
(87.8) |
Differentiation |
161 |
(93.6) |
Lymphovascular invasion |
25 |
(14.5) |
Neural invasion |
4 |
(2.3) |
Adjuvant treatment |
79 |
(45.9) |
Table 2: Characteristics of the gastric carcinoma patients screened (N = 432)
Characteristics |
N = 432 |
Age (yrs) |
53, 23–74 |
Sex |
280 (64.8%) |
Type of gastrectomy |
256 (59.3%) |
Location of tumor |
231 (53.5%) |
Grade |
111 (25.7%) |
Lauren type |
139 (32.2%) |
Lymphovascular invasion |
212 (49.1%) |
pT1 stage |
38 (8.8%) |
pN stage |
40 (9.3%) |
AJCC stage |
68 (15.7%) |
Identification of a novel CAD-ALK fusion variant
One rectal adenocarcinoma patient (0.6%) showed intense, granular staining (3+) by ALK IHC. ALK protein expression was observed in the cytoplasm of tumor cells with diffuse staining pattern in both differentiated and undifferentiated carcinoma areas with strong intensity (Figure 1A). ALK FISH revealed 25% of tumor cells had red and green signals that were two or more signal diameters apart were observed (Figure 1B). The nCounter assays demonstrated the loss of 5′portion of the ALK gene (Figure 1C) but failed to detect fusion partner gene using the selected fusion gene sets of KIF5B, EML4, KLC1, SMCF1 and C2orf44.
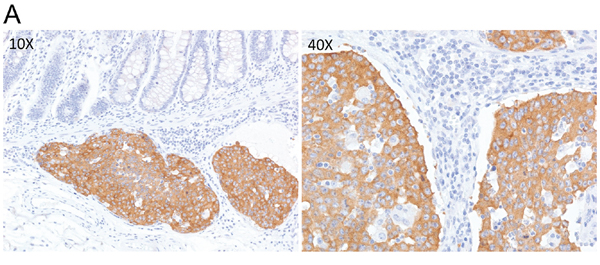
Figure 1A: ALK IHC (3+) staining in a rectal adenocarcinoma patient tumor sample. Low power field examination (10X; Left) shows strong cytoplasmic staining in cancer cells compared to control normal colonic crypts. High power examination (40X) shows dense brown granular cytoplasmic staining.
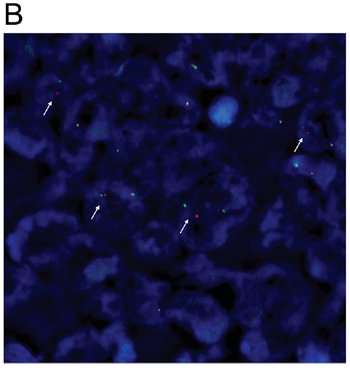
Figure 1B: Detection of ALK rearrangement by ALK break-apart by fluorescence in situ hybridization (FISH) in the ALK IHC (3+) rectal adenocarcinoma patient (white arrows).
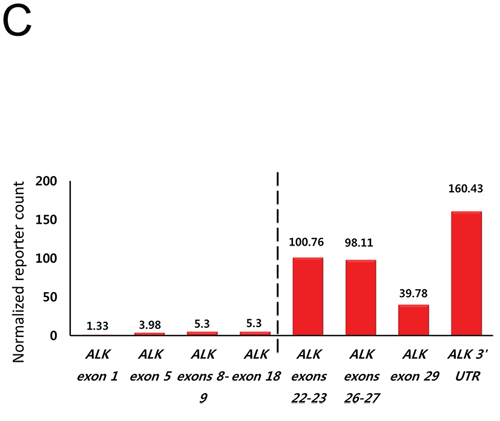
Figure 1C: Nanostring 3′/5′ ratio of ALK reporter readout indicating the loss of the 5′portion of ALK gene.
A novel CAD-ALK fusion variant was identified by CGP in this patient case. The CAD (Carbamoyl-phosphate synthetase 2, Aspartate transcarbamylase, and Dihydroorotase) gene is located on chromosome 2p21–22 and contains 45 exons [15] and is transcribed in the opposite direction as ALK (Figure 2A). The CAD-ALK fusion variant is generated by an intra-chromosomal inversion event fusing the exons 1–35 of CAD to exons 20–29 of ALK (Figure 2A). The full-length CAD protein is comprised of 2, 225 amino acids and is a “multifunctional” protein responsible for four enzymatic activities of the pyrimidine pathway (gluymine amidotransferase [GATase], carbamoly-phosphate synthase [CPSase], dihydroorotase [DHOase], and aspartate transcarbamylase [ATCase]) (Figure 2B). The CAD-ALK fusion variant results in the first 1864 amino acids of CAD, which includes the GATase, CPSase, and DHOase enzymes but not the ATCase domains, fused to the full length kinase domain of ALK (Figure 2B). Both KRAS and BRAF were wildtype by CGP (Table 3) and no additional kinase fusions were identified.
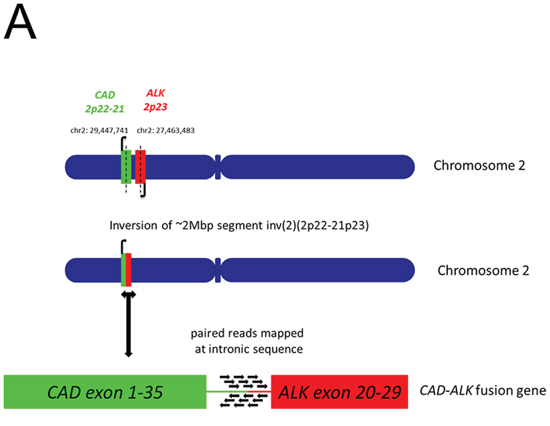
Figure 2A: Schematic of chromosomal location and transcription direction and breakpoint of CAD and ALK genes in the CAD-ALK positive CRC patient.
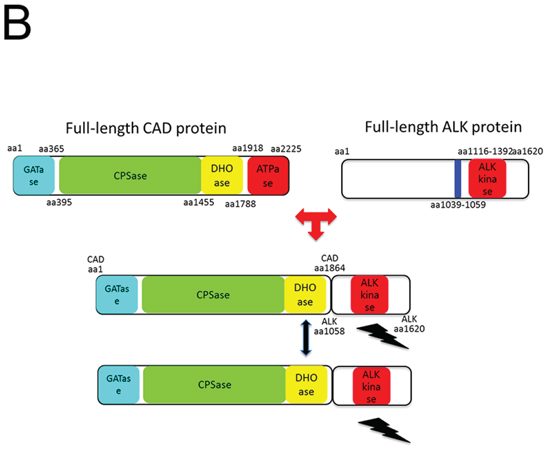
Figure 2B: Schematic of the CAD-ALK fusion protein domains and potential dimerization domains.
Table 3: Comparison of the methods and clinicopathologic characteristics of ALK+ CRC patients identified from this study and in the literature
Study |
Aisner et al. [5] |
Huoang et al. [17] |
This report |
This report |
Frequency |
1/236* (0.4%) |
1/1889 (0.05%) |
1/172 (0.6%-total) |
1 out of 50 CRC (2%) |
Screening Method |
FISH |
IHC (5A4 antibody) |
IHC (5A4 antibody) |
IHC (5A4 antibody) |
Confirmation method |
RT-PCR |
FISH (Vysis Abbott Molecular) |
FISH (Vysis Abbott Molecular), |
FISH (Vysis Abbott Molecular), Nanostring, |
Source of tissue |
TMA |
TMA |
TMA |
Patient tumor tissue |
Location |
Rectum |
Colon (distal transverse) |
Rectum |
Colon |
Age |
84 |
87 |
46 |
65 |
Ethnicity |
Australian |
Australian |
Korean |
Korean |
Gender |
Female |
Female |
Female |
Male |
ALK Fusion partner |
EML4 |
NR |
CAD |
EML4 |
ALK fusion variant |
EML4-ALK (E6, A20) |
NR |
CAD-ALK (C35; A20) |
EML4-ALK (E21; A20) |
Histologic differentiation |
NR |
NR |
Poor |
Poor |
Signet ring features |
No |
No |
No |
No |
Site of metastasis |
Lymph nodes, lung |
None |
Lymph nodes, lung, pericardium |
Mediastinal/cervical lymph nodes |
Pattern of expression of ALK rearrangement |
Scattered, in areas of high grade dysplasia, with intratumoral heterogeneity |
Diffuse |
Diffuse, cytoplasmic |
Diffuse |
KRAS status |
KRAS G12A |
Wildtype |
Wildtype |
Wildtype |
BRAF status |
NR |
Wildtype |
Wildtype |
Wildtype |
*236 out of 286 tumor samples evaluable;
CAD: carbamoyl-phosphate synthetase 2, aspartate transcarbamylase, and dihydroorotase; EML4: echinoderm microtubule associated protein like 4;
IHC: immunohistochemistry; FISH: fluorescence in situ hybridization; MSI: microsatellite instability; MSS: microsatellite stable NA; not applicable; NGS; next generation sequencing; NR: not reported; RT-PCR: reverse transcriptase-polymerase chain reaction; TMA: tissue microarray;
The CAD-ALK patient was a 46 years old Korean woman who underwent low anterior resection and the pathology revealed a 6.5 cm poorly-differentiated adenocarcinoma with perirectal soft tissue extension and metastasis in 4 out of 34 regional lymph nodes (AJCC stage IIIB). She received adjuvant 5-fluorouracil (5-FU)-based concurrent chemoradiation but developed metastatic disease shortly and died of pericardial tamponade 2 months later. In the remaining CRC and all of the GC cases, ALK protein expression was not observed.
Identification of an EML4-ALK rearranged colon cancer patient
One out of a total of 50 CRC patients enrolled in the NEXT-1 trial was screened positive by ALK IHC. This patient is 65-year old male patient who initially presented with stage IV colon adenocarcinoma with multiple retroperitoneal lymph nodes and supraclavicular lymph nodes (Figure 3A). After 12 cycles of cetuximab/FOLFIRI (5-fluorouracil, leucovorin, irinotecan) chemotherapy, the patient underwent palliative surgical resection of colon cancer which revealed poorly differentiated adenocarcinoma, demonstrated diffuse and intense ALK staining (3+) by ALK IHC (Figure 3B). ALK FISH was positive with 50% cells demonstrating breakapart signals (Figure 3C). CGP revealed EML4-ALK (E21; A20) fusion variant. The tumor was found to be KRAS and BRAF wildtype (Table 3).

Figure 3A: 2-deoxy-2-(18F)fluoro-D-glucose positron emission tomography (PET) scan of the EML4-ALK CRC patient at the time of presentation demonstrating metastatic retroperitoneal and cervical lymph nodes metastasis.
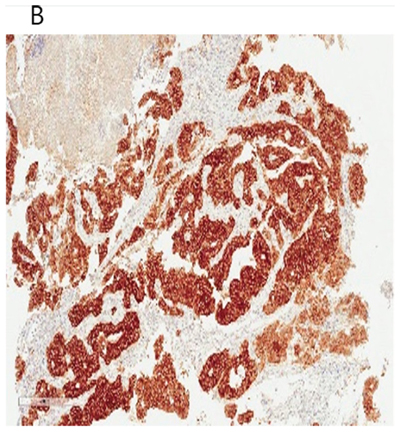
Figure 3B: ALK IHC showing strong diffuse staining of ALK antibody (3+) of the EML4-ALK (E21; A20) adenocarcinoma of the colon patient after palliative resection.
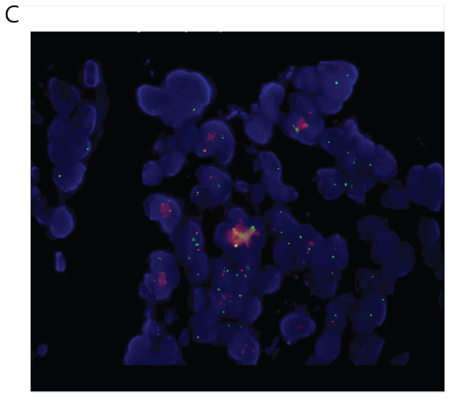
Figure 3C: Break-apart ALK FISH of the EML4-ALK (E21;A20) colon patient demonstrating the presence of breakapart signals in 50% cells.
Tumor cell line derived from this patient was inhibited by 1 μM crizotinib (p < 0.0001, one-way ANOVA test) or to a greater extent with 1 μM entrectinib (p < 0.0001 vs. no ALK inhibitor; p < 0.0001 vs. crizotinib one-way ANOVA test) (Figure 3D). Both crizotinib and entrectinib inhibited the phosphorylation of ALK and its downstream signal molecules, including ERK1/2 and AKT from this EML4-ALK rearranged colon patient tumor derived cell line (Figure 3E).
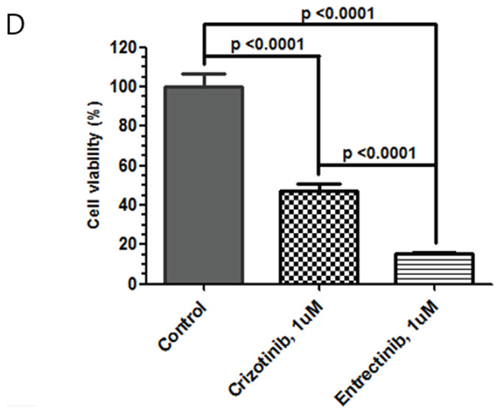
Figure 3D: Inhibition of the growth of the EML4-ALK CRC patient derived tumor cells with 1 μM crizotinib or 1 μM entrectinib.
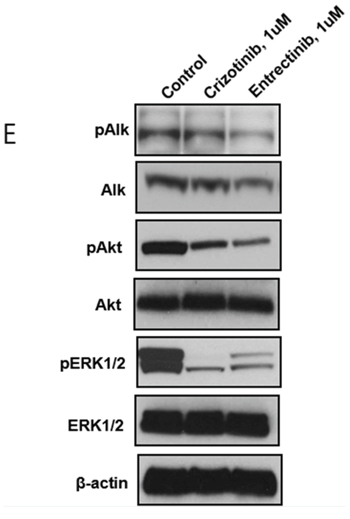
Figure 3E: Western blot demonstrating Inhibition of the phosphorylation of the ALK protein and other downstream signal molecules in the EML4-ALK CRC patient tumor derived cell line after inhibition by crizotinib or entrectinib.
DISCUSSION
We demonstrated that IHC is a viable screening strategy for detecting ALK rearrangement in CRC and during the process identified a novel CAD-ALK fusion in CRC. The frequency of ALK rearrangement in CRC in this study was of 0.6% (1/172) among Korean CRC tumor samples. The discrepancy may be due to the TMAs were more than 10 years old which may affect the performance of the diagnostic assays. Lin and colleagues identified two EML4-ALK fusion CRC (2/83, 2.4%) and identified potentially up to 5 ALK rearranged CRC out of 83 (6%) CRC samples using an exon scanning method [4]. Aisner and colleagues identified one EML4-ALK CRC tumor out of 236 patient tumor samples (0.4%) using FISH as a screening assay (Table 3) [5]. Lipson and colleagues identified one C2orf44-ALK (WDCP-ALK) CRC patient among 40 CRC patients (2.5%) using CGP [6]. Chromosome 2 open reading frame 44 (C2orf44) was recently shown to encode WD repeat and coiled-coil containing protein (WDCP) [16]. Houang and colleagues performed a large scale screening for both ALK and ROS1 rearrangements in CRC and found only one case among 1889 (0.05%) CRC cases was FISH positive (ALK IHC 3+), but no fusion partner was identified [17] (Table 3). The study by Houang and colleagues and our study indicated ALK IHC can be a very specific assay for detection of ALK rearrangement in CRC. Although signet-ring histology has been associated with ALK-rearranged NSCLC [18], none of the reports identified signet-ring histology in the colon adenocarcinoma [5, 6, 17]. Indeed Miller and colleagues have utilized signet ring histology as a screening criterion but failed to detect ALK rearrangement by break-apart FISH in upper gastrointestinal malignancies [19]. Given the low frequency of ALK rearrangement in CRC, a precise clinicopathologic profile of ALK-rearranged CRC remains to be determined. We were not able to detect ALK rearrangement in GC as there was no ALK IHC positivity among the 432 GC samples screened. It remains possible that ALK rearrangement exists but is likely to be extremely infrequent in GC.
We identified two different ALK fusions (CAD-ALK, EML4-ALK) in CRC in this report. CAD is located on chromosome 2p22-p21 in close proximity to ALK (and EML4) [15] and the transcription of CAD is in the opposite direction of ALK (Figure 2A). Thus the CAD-ALK fusion is likely generated by an intra-chromosomal inversion event similar to the event that generated EML4-ALK in NSCLC [20, 21]. Furthermore it has been shown that the DHoase domain, which is retained in the CAD-ALK fusion, can homo-multimerize with other CAD proteins [22] thus functioning analogously as the classical “coiled-coil” domain found in EML4 protein and leading to the aberrant activation of the ALK kinase [20, 21]. The ALK-rearranged CRC patient identified as part of the NEXT-1 trial harbors the EML4-ALK (E21:A20) where exons 1–21 of EML4 is fused to exons 20–29 of ALK which has been reported only once in CRC [5] but so far has not been reported in ALK-rearranged NSCLC. Recently, suppressor of MEK1 homolog 2 (SMEK2)-ALK fusion variant SMEK2-ALK (S11; A2) has been reported in rectal adenocarcinoma, which fused the first 11 exons of SMEK2 to exons 2–29 of ALK, independently providing further evidence the existence of ALK rearrangement in CRC [24].
The success of crizotinib in ALK-rearranged NSCLC [1, 2] has opened the door for potential treatment of other “ALKoma” [23] with crizotinib and other ALK inhibitors. There are ongoing clinical trials of ALK inhibitors that are organ agnostic [i.e. TSR-011 (NCT02048488); entrectinib (NCT02097810)]. The inhibition of tumor derived cell line from our EML4-ALK CRC patient by two separate ALK inhibitors is encouraging and provides pre-clinical rationale for enrolling ALK-rearranged CRC patients onto clinical trials with ALK inhibitor. ALK IHC has been automated for comprehensive screening for ALK rearrangement in NSCLC with 100% sensitivity and 98% specificity (98%) [25] and could be employed as the screening strategy for ALK rearrangement in CRC.
MATERIALS AND METHODS
Patients and tissue microarrays
The GC patient in this study has been described [9]. For the CRC patients included in this study, all received surgical resection with curative intent at Samsung Medical Center, Seoul, Korea, between January 2000 and December 2001. Inclusion criteria were as follows: (1) pathologically confirmed adenocarcinoma of stomach, colon and rectum; (2) adequate amount and quality of paraffin-embedded tumor blocks; (3) available data on clinicopathologic characteristics; (4) no prior chemotherapy or chemoradiation for GC or CRC. For tissue microarray construction, all H&E stained slides were reviewed and the representative area was carefully selected and marked on all paraffin blocks. A 3 mm tissue core was taken from the representative region of each tumor specimen using Accumax (ISU Abxis, Seoul, Korea) as previously described [8]. The study protocol was approved by Institutional Review Board of Samsung Medical Center.
ALK immunohistochemistry (IHC)
ALK IHC was carried out on 3-μm thick tissue using a Ventana automated immunostainer (Ventana Medical Systems, Tucson, AZ) according to the manufacturer’s protocol. Briefly, the slides were deparaffinized using EZ Prep (Ventana Medical Systems) at 75°C for 4 minutes and heat pretreatment at 100°C for 20 minutes. The antibody for ALK (mouse monoclonal, clone 5A4, Novocastra, Newcastle, United Kingdom) was diluted to 1:30 and incubated at 42°C for 2 hours. Signals were detected with an iView detection kit (Ventana Medical Systems) based on a streptavidin-biotin method. Mayer’s hematoxylin was used for counterstaining for 2 minutes at room temperature. ALK expression was semiquantitatively assessed based on the intensity of staining and the proportion of stained cells and scored by two independent pathologists (IG Do and KM Kim). An IHC score was assigned as 0 (no staining), 1+ (faint cytoplasmic staining in ≤10% of tumor cells), 2+ (moderate, smooth cytoplasmic staining), and 3+ (intense, granular cytoplasmic staining). IHC scores of 2+ or 3+ were regarded as ALK IHC positive.
ALK florescence in situ hybridization (FISH)
ALK FISH analysis was performed in ALK IHC positive cases. A commercially available break-apart probe specific to the ALK locus (Vysis LSI ALK Dual Color, break-apart probe; Abbott Molecular, Des Plaines, IL, USA) was used. FISH analysis was considered positive for ALK rearrangement if >15% of tumor cells (≥50 tumor cells counted) showed isolated red signals and/or split red and green signals. Interpretation of FISH analysis was performed by two independent pathologists (IG Do and KM Kim).
ALK fusion transcript assay by nCounter anchored multiplex polymerase chain reaction assays
nCounter anchored multiplex polymerase chain reaction assays were performed according to the manufacturer’s protocol (NanoString, Seattle, WA). Briefly, 500 ng of total RNA was hybridized to nCounter probe sets for 16 hours at 65°C. Samples were processed using an automated nCounter Sample Prep Station (NanoString Technologies, Inc., Seattle, WA). Cartridges containing immobilized and aligned reporter complex were subsequently imaged on an nCounter Digital Analyzer (NanoString Technologies, Inc.). Reporter counts were collected using NanoString’s nSolver analysis software version 1, normalized, and analyzed as previously described [10]. This technology has been shown to successfully identify novel fusion partners to ALK- and RET-rearranged NSCLC [11, 12]. To identify fusion partners of ALK in CRC and GC, primers for KIF5B, EML4, KLC1, SMCF1 and C2orf44 were designed and used for analyses.
NGS-based comprehensive genomic profiling (CGP) assay
Ten 4 μm unstained, formalin-fixed paraffin-embedded (FFPE) tissue slides of ALK IHC positive cases were sent to a Clinical Laboratory Improvement Amendments (CLIA)-certified and College of American Pathologists (CAP)-accredited laboratory (Foundation Medicine Inc, Cambridge, MA) for CGP testing. Macro-dissection to enrich specimens of ≥20% tumor content was performed as warranted. DNA was extracted from unstained FFPE sections and quantified by a Picogreen fluorescence assay. 50–100 ng of DNA was used for library construction. Hybridization capture of all coding exons of 405 cancer-related genes and selected introns of 31 genes frequently rearranged in solid tumors was performed. Hybrid-capture libraries were then sequenced to >500x average unique coverage with >100x at >99% of exons using Illumina HiSeq instrument. Sequencing data were processed using a customized analysis pipeline designed to detect all classes of genomic alterations, including base substitutions, short insertions and deletions, copy number alterations, and genomic rearrangements [13].
Screening of patients for ALK rearrangement for a pathway-directed therapy trial
Between November 2013 to August 2014, eligible patients with metastatic solid tumors were enrolled into an institutional review board approved, pathway-directed therapy NEXT-1 (Next generation pErsonalized tX with mulTi-omics and preclinical model) trial; http://www.clinicaltrials.gov, NCT02141152) at Samsung Medical Center. ALK IHC was performed when sufficient tumor tissue were available. As part of the NEXT trial, patient derived tumor cell lines were isolated from tumor tissue in patients with targetable mutations after obtaining informed consent form.
Culture and treatment of patient tumor derived cell lines
After tumors were surgically removed and homogenized, the cells were cultured in RPMI media supplemented with 10% fetal bovine serum, 0.5 μg/ml of hydrocortisone (Sigma Aldrich), 5 μg/ml of insulin (PeproTech, Rocky Hill, NJ, USA), 5 ng of EGF and FGF (PeproTech). Crizotinib was purchase from Selleck Chemical (Houston, TX, USA). Entrectinib was provided by Ignyta, Inc (San Diego, CA, USA) under a material transfer agreement. After pathologic confirmation, cells were seeded on 1~2 × 106 cells/10 mm dishes or 5000 cells/well/96well plate, treated with 1 μM of crizotinib or 1 μM of entrectinib (RXDX-101) and incubated for 72 hours at 37°C in a humidified atmosphere of 5% carbon dioxide for analysis of Immunoblotting and cell proliferation inhibition assay in triplicates. Entrectinib is an ALK, ROS1, NTRK1, NTRK2, NTRK3 inhibitor that is currently undergoing a phase 1/2 clinical trial in the US (http://www.clinicaltrials.gov; NCT02097810) and a first in human study in Italy [14]. Inhibition of tumor derived cell lines proliferation inhibition was determined via Cell Titer Glo (Promega, Madison, WI, USA) according to the manufacturer’s protocol.
Immunoblot analysis
Total proteins from patient tumor derived cell lines were isolated using RIPA buffer (Sigma-Aldrich, St. Louis, MO, USA) containing a protease inhibitor cocktail (Roche, Mannheim, Germany) and phosphatase inhibitor cocktail (Roche), and protein concentrations were determined according to Bradford procedure using a Quick Start Bradford Protein Assay (Bio-Rad, Hercules, CA, USA). Thirty μg of proteins were subjected to 10% SDS-polyacrylamide gel electrophoresis, and electro-transferred onto nitrocellulose membranes. The membranes were blocked with 5% nonfat dry milk in Tris-buffered saline containing 0.1% v/v Tween 20, and probed overnight at 4°C with specific antibodies: pALK (Tyr 1586), ALK (C-19) from Santa Cruz biotechnology (Santa Cruz, CA, USA), and pERK1/2 (Thr202/Tyr204), ERK1/2 (Thr202/Tyr204) from Cell Signaling Technology (Beverly, MA, USA), and beta actin from Sigma Aldrich. Horseradish peroxidase-conjugated anti-rabbit or mouse IgG (Vector, Burlingame, CA, USA) were used as secondary antibodies, and signals were detected by chemiluminescence using ECL Western Blotting Substrate (Thermo Scientific, Rockford, IL, USA), and visualized by using LAS-4000 (Fujifilm, Tokyo, Japan).
ACKNOWLEDGMENTS
This work was supported by a grant from the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HI13C1951, HI14C2188). Support was also provided by a grant from the 20 by 20 project of Samsung Medical Center (GF01140111).
FINANCIAL SUPPORT
This research was supported by a grant of the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI13C2096, HI13C1951). Additional support was also provided by a grant from the 20 by 20 project of Samsung Medical Center (GF01140111).
DISCLOSURE STATEMENT
KW, SB, PJS, JSR, SMA, and VAM are employed by and own stocks of Foundation Medicine Inc.
GGL and ZH are employed by and own stocks of Ignyta Inc.
Authors’ contributions
Conception and design: J Lee, KM Kim, SHI Ou.
Development of methodology: J Lee, K Wang, KM Kim, PJ Stevens, GG Li, SHI Ou.
Acquisition of data (provided animals, acquired and managed patients, provided facilities, etc.): J. Lee, HC Kim, JY Hong, SY Kim, J Jang, ST Kim, JO Park, HY Lim, WK Kang, YS Park, Jiyun Lee, WY Lee, YA Park, JW Huh, SH Yun, IG Do, SH Kim, K Wang, S Balasubramanian, PJ Stevens, JS Ross, GG Li, Z Hornby, SM Ali, VA Miller, KM Kim, SHI Ou.
Analysis and interpretation of data (e.g., statistical analysis, biostatistics, computational analysis): J. Lee, HC Kim, JY Hong, SY Kim, J Jang, ST Kim, JO Park, HY Lim, WK Kang, YS Park, Jiyun Lee, WY Lee, YA Park, JW Huh, SH Yun, IG Do, SH Kim, K Wang, S Balasubramanian, PJ Stevens, JS Ross, GG Li, Z Hornby, SM Ali, VA Miller, KM Kim, SHI Ou.
Writing, review, and/or revision of the manuscript: J. Lee, HC Kim, JY Hong, SY Kim, J Jang, ST Kim, JO Park, HY Lim, WK Kang, YS Park, Jiyun Lee, WY Lee, YA Park, JW Huh, SH Yun, IG Do, SH Kim, K Wang, S Balasubramanian, PJ Stevens, JS Ross, GG Li, Z Hornby, SM Ali, VA Miller, KM Kim, SHI Ou.
Administrative, technical, or material support (i.e., reporting or organizing data, constructing databases): J. Lee, HC Kim, JY Hong, SY Kim, J Jang, ST Kim, JO Park, HY Lim, WK Kang, YS Park, Jiyun Lee, WY Lee, YA Park, JW Huh, SH Yun, IG Do, SH Kim, K Wang, S Balasubramanian, PJ Stevens, JS Ross, GG Li, Z Hornby, SM Ali, VA Miller, KM Kim, SHI Ou.
REFERENCES
1. Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa K, Mekhail T, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014; 371:2167–2177.
2. Shaw AT, Kim DW, Nakagawa K, Seto T, Crinó L, Ahn MJ, et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med. 2013; 20368:2385–2394.
3. Kazandjian D, Blumenthal GM, Chen HY, He K, Patel M, Justice R, et al. FDA approval summary: crizotinib for the treatment of metastatic non-small cell lung cancer with anaplastic lymphoma kinase rearrangements. Oncologist. 2014; 19:e5–11.
4. Lin E, Li L, Guan Y, Soriano R, Rivers CS, Mohan S, et al. Exon array profiling detects EML4-ALK fusion in breast, colorectal, and non-small cell lung cancers. Mol Cancer Res. 2009; 7:1466–1476.
5. Aisner DL, Nguyen TT, Paskulin DD, Le AT, Haney J, Schulte N, et al. ROS1 and ALK fusions in colorectal cancer, with evidence of intratumoral heterogeneity for molecular drivers. Mol Cancer Res. 2014; 12:111–118.
6. Lipson D, Capelletti M, Yelensky R, Otto G, Parker A, Jarosz M, et al. Identification of new ALK and RET gene fusions from colorectal and lung cancer biopsies. Nat Med. 2012; 18:382–384.
7. Sullivan HC, Fisher KE, Hoffa AL, Wang J, Saxe D, Siddiqui MT, et al. The role of immunohistochemical analysis in the evaluation of EML4-ALK gene rearrangement in lung cancer. Appl Immunohistochem Mol Morphol. 2014. [Epub ahead of print].
8. Lee J, Lee SE, Kang SY, Do IG, Lee S, Ha SY, et al. Identification of ROS1 rearrangement in gastric adenocarcinoma. Cancer. 2013; 119:1627–1635.
9. Lee J, Sohn I, Do IG, Kim KM, Park SH, Park JO, et al. Nanostring-based multigene assay to predict recurrence for gastric cancer patients after surgery. PLoS ONE. 9:e90133.
10. Lira ME, Kim TM, Huang D, Deng S, Koh Y, Jang B, et al. Multiplexed gene expression and fusion transcript analysis to detect ALK fusions in lung cancer. J Mol Diagn. 2013; 15:51–61.
11. Choi YL, Lira ME, Hong M, Kim RN, Choi SJ, Song JY, et al. A novel fusion of TPR and ALK in lung adenocarcinoma. J Thorac Oncol. 2014; 9:563–566.
12. Lira ME, Choi YL, Lim SM, Deng S, Huang D, Ozeck M, et al. A single-tube multiplexed assay for detecting ALK, ROS1, and RET fusions in lung cancer. J Mol Diagn. 2014; 16:229–243.
13. Frampton GM, Fichtenholtz A, Otto GA, Wang K, Downing SR, He J, et al. Development and validation of a clinical cancer genomic profiling test based on massively parallel DNA sequencing. Nat Biotechnol. 2013; 31:1023–1031.
14. De Braud FG, Pilla L, Niger M, Damian S, Bardazza B, Martinetti A, et al. Phase 1 open label, dose escalation study of RXDX101, an oral pan-trk, ROS1, and ALK inhibitor, in patients with advanced solid tumors with relevant molecular alterations. J Clin Oncol. 322014; 5. abstr 2502.
15. http.//www.ncbi.nlm.nih.gov/gene/57223, (assessed 1 February, 2015).
16. Yokoyama N, Miller WT. Molecular characterization of WDCP, a novel fusion partner for the anaplastic lymphoma tyrosine kinase ALK. Biomed Rep. 2015; 3:9–13.
17. Houang M, Toon CW, Clarkson A, Sioson L, de Silva K, Watson N, et al. ALK and ROS1 overexpression is very rare in colorectal adenocarcinoma. Appl Immunohistochem Mol Morphol. 2014; Jul 2;. [Epub ahead of print].
18. Nishino M, Klepeis VE, Yeap BY, Bergethon K, Morales-Oyarvide V, Dias-Santagata D, et al. Histologic and cytomorphologic features of ALK-rearranged lung adenocarcinomas. Mod Pathol. 2012; 25:1462–1472.
19. Miller J, Peng Z, Wilcox R, Evans M, Ades S, Verschraegen C. Absence of anaplastic lymphoma kinase translocations in signet ring cell carcinomas of the upper gastrointestinal tract. Gastrointest Cancer Res. 2014; 7:39–41.
20. Soda M, Choi YL, Enomoto M, Takada S, Yamashita Y, Ishikawa S, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007; 448:561–566.
21. Mano H. Non-solid oncogenes in solid tumors: EML4-ALK fusion genes in lung cancer. Cancer Sci. 2008; 99:2349–2355.
22. Grande-García A, Lallous N, Díaz-Tejada C, Ramón-Maiques S. Structure, functional characterization, and evolution of the dihydroorotase domain of human CAD. Structure. 2014; 22:185–198.
23. Mano H. ALKoma: a cancer subtype with a shared target. Cancer Discov. 2012; 2:495–502.
24. Stransky N, Cerami E, Schalm S, Kim JL, Lengauer C. The landscape of kinase fusions in cancer. Nat Commun. 2014; 5:4846.
25. Ying J, Guo L, Qiu T, Shan L, Ling Y, Liu X, et al. Diagnostic value of a novel fully automated immunochemistry assay for detection of ALK rearrangement in primary lung adenocarcinoma. Ann Oncol. 2013; 24:2589–2593.