
Introduction
Epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (EGFR-TKIs) such as gefitinib and erlotinib are first-line treatments for advanced non-small cell lung cancer (NSCLC) harboring EGFR-activating mutations, and have been reported to improve the clinical outcome and quality-of-life of patients with this malignancy [1-4]. However, acquired resistance invariably develops, and the majority of EGFR-mutated NSCLCs that respond to EGFR-TKIs develop acquired resistance after approximately 12 months [5, 6]. The most common mechanism whereby acquired resistance to EGFR-TKIs develops is a secondary T790M mutation [7]. As well as this mechanism, c-MET amplification(5-10%), PIK3CA mutations(~5%), BRAF mutations(~1%) and small-cell lung cancer transformation(~5%) are also associated with acquired resistance to TKIs [8-10]. However, the mechanisms responsible for about 30% of cases of acquired resistance to EGFR-TKIs are still unknown [10].
Long non-coding RNAs (lncRNAs) are a group of non-coding transcripts of more than 200 nt that are involved in cell apoptosis, tumor invasion, metastasis, and drug resistance [11, 12]. Multiple studies have indicated that lncRNAs, including H19 [13], CUDR [14], and AK126698 [15] are related to chemotherapy resistance. In a previous study [16], we compared the expression of lncRNAs in gefitinib-sensitive and gefitinib-resistant human lung cancer cells by lncRNA microarray analysis, and found that some lncRNAs, including UCA1 (urothelial cancer-associated 1), were up-regulated in resistant cells.
In an effort to overcome resistance, we have investigated the molecular mechanisms of acquired resistance in epigenetic genetics. In the present study, we sought to determine whether the lncRNA UCA1 can induce acquired resistance to EGFR-TKIs via cell apoptosis and activation of the PI3K/AKT/mTOR pathway in EGFR-mutant lung cancer.
Results
Over-expression of UCA1 was correlated with acquired resistance to EGFR-TKIs
To identify the mechanisms of acquired resistance to EGFR-TKIs, we conducted microarray expression profiling of lncRNAs/mRNA for PC9 and PC9/R cells. UCA1 was found to have a high expression level in PC9/R cells with acquired resistance to gefitinib [16]. To validate the analysis of lncRNAs profiles, we assessed the mRNA expression of UCA1 by RT-PCR in lung cancer cell lines and patients with EGFR-mutant NSCLC. A total of 89 patients were enrolled in this study. Of them, the clinical characteristics of the 84 patients with EGFR-mutant NSCLC who had enough samples obtained from either before EGFR-TKIs treatment or after development of acquired resistance to EGFR-TKIs were shown in Table 1 and that of the other 5 patients who had matched samples were shown in Table 2.
Table 1: Clinical characteristics of the 47 patients with EGFR-mutant NSCLC(BT group) and 37 with acquired resistance to EGFR-TKIs(AR group)
Clinical characteristics |
BT group N = 47 (%) |
AR group N = 37 (%) |
Age: |
||
<65 years |
33 (70.2%) |
27 (73.0%) |
≥65 years |
14 (29.8%) |
10 (27.0%) |
Sex: |
||
Male |
18 (38.3%) |
21 (56.8%) |
Female |
29 (61.7%) |
16 (43.2%) |
EGFR: |
||
19DEL |
27 (57.4%) |
9 (24.3%) |
L858R |
20 (42.6%) |
8 (21.6%) |
T790M |
- |
20 (54.1%) |
Stage: |
||
IIIB |
2 (4.3%) |
8 (21.6%) |
IV |
45 (95.7%) |
29 (78.4%) |
Smoking: |
||
Never |
39 (83.0%) |
28 (75.7%) |
Ever |
8 (17.0%) |
9 (24.3%) |
Histology: |
||
Adenocarcinoma |
44 (93.6%) |
35 (92.9%) |
Non-adenocarcinoma |
3 (6.4%) |
2 (5.4%) |
UCA1: |
||
Low |
34 (72.3%) |
22 (59.5%) |
High |
13 (27.7%) |
15 (40.5%) |
EGFR-TKIs: |
||
Gefitinib |
39 (83.0%) |
17 (45.9%) |
Erlotinib |
8 (17.0%) |
20 (54.1%) |
EGFR: epidermal growth factor receptor; TKI: tyrosine kinase inhibitor; UCA1: urothelial carcinoma-associated 1; BT: before treatment; AR: acquired resistance.
Table 2: UCA1 is up-regulated in human EGFR-mutant NSCLC specimens from individuals with acquired resistance to EGFR-TKIs
ID |
Age |
Sex |
Tumor type |
EGFR mutation |
TKI |
Response |
PFS (months) |
2-ΔCt, UCA1 |
||
BT |
AR |
BT |
AR |
|||||||
1 |
49 |
M |
AC |
L858R |
L858R |
Erlotinib |
PR |
16.0 |
0.008 |
0.042 |
2 |
67 |
F |
AC |
19DEL |
19DEL |
Gefitinib |
PR |
17.3 |
0.105 |
0.204 |
3 |
63 |
F |
AC |
19DEL |
19DEL/T790M |
Erlotinib |
SD |
13.9 |
0.040 |
0.259 |
4 |
54 |
F |
AC |
19DEL |
19DEL |
Gefitinib |
PR |
13.0 |
0.031 |
0.357 |
5 |
37 |
M |
NSCLC |
L858R |
L858R/T790M |
Erlotinib |
SD |
8.5 |
0.004 |
0.188 |
Clinical characteristics in the 5 paired EGFR-mutant NSCLC specimens were obtained from patients both before treatment and upon acquired resistance to treatment with erlotinib or gefitinib.
AC: adenocarcinoma; AR: acquired resistance; BT: before treatment; EGFR: epidermal growth factor receptor; F: female; M: male; NSCLC: non-small cell lung cancer; PFS: progression-free survival; PR: Partial response; SD: stable disease; TKI: tyrosine kinase inhibitor; UCA1: urothelial carcinoma-associated 1.
Over-expression of UCA1 was observed in lung cancer cells with acquired resistance (PC9/R and H1975) [P < 0.01] (Figure 1A). And UCA1 mRNA expression level in patients who developed acquired resistance to EGFR-TKIs was significantly higher than in the baseline group with EGFR-TKI-sensitive NSCLC (0.58 ± 0.05 vs 0.21 ± 0.05, P = 0.0024; Figure 1B). We also measured the mRNA expression of UCA1 by RT-PCR in 5 matched EGFR-mutant NSCLC specimens, including 2 with T790M and 3 without T790M(Table 2) (Figure 1C), both before treatment (BT) with EGFR-TKIs and after the development of resistance to TKIs, and found that UCA1 expression was up-regulated in patients with acquired resistance. Whereas it was down-regulated in patients with primary resistance(0.072 ± 0.013 vs 0.21 ± 0.05, P = 0.0068; Figure 1D). On the basis of the UCA1 expression before treatment with EGFR-TKIs, the patients were divided into a high expression group (n = 20) and a low expression group (n = 32), depending on whether they were above or below the cut-off value 2-ΔCt = 0.068 (Supplementary Table S1). When progression free survival(PFS) was assessed, patients in the high UCA1 expression group had a significantly poorer prognosis than those in the low expression group (median PFS 8.5m vs 13.0m, P = 0.0068; Figure 1E). The objective response rate (ORR) in the high UCA1 expression group was significantly lower than in the low expression group (52.94% vs 84.21%, P = 0.014; Figure 1F). Univariate analysis of PFS revealed that the expression level of UCA1 and age were prognostic indicators (Table 3), while multivariate analysis indicated that the UCA1 expression level and age were independent prognostic factors for PFS in patients with EGFR-TKI-sensitive NSCLC. Therefore, we hypothesized that UCA1 may play an important role in acquired resistance to EGFR-TKIs and influence the efficacy of EGFR-TKIs.
Table 3: Univariate and multivariate analysis for progression-free survival (PFS)
Factors |
Univariate analysis |
Multivariate analysis |
||||
HR (95% CI) |
P |
HR (95% CI) |
P |
|||
Age (<65/ ≥65 years) |
0.298 (0.089-0.999) |
0.05 |
0.296 (0.088-0.993) |
0.049 |
||
Sex (male/female) |
0.591 (0.265-1.318) |
0.199 |
||||
Smoking (never/ever) |
1.944 (0.559-6.766) |
0.296 |
||||
EGFR (19DEL/L858R) |
1.167 (0.525-2.593) |
0.705 |
||||
Histology (adenocarcinoma/non-adenocarcinoma) |
1.15 (0.268-4.94) |
0.851 |
||||
Stage (IIIB/IV) |
2.702 (0.612-11.927) |
0.189 |
||||
UCA1 (low/high) |
3.339 (1.281-8.699) |
0.015 |
0.308 (0.111-0.851) |
0.023 |
||
EGFR-TKIs (gefitinib/erlotinib) |
0.946 (0.381-2.344) |
0.904 |
||||
CI: confidence interval; EGFR: epidermal growth factor receptor; HR: hazard ratio; TKI: tyrosine kinase inhibitor; UCA1: urothelial carcinoma-associated 1.
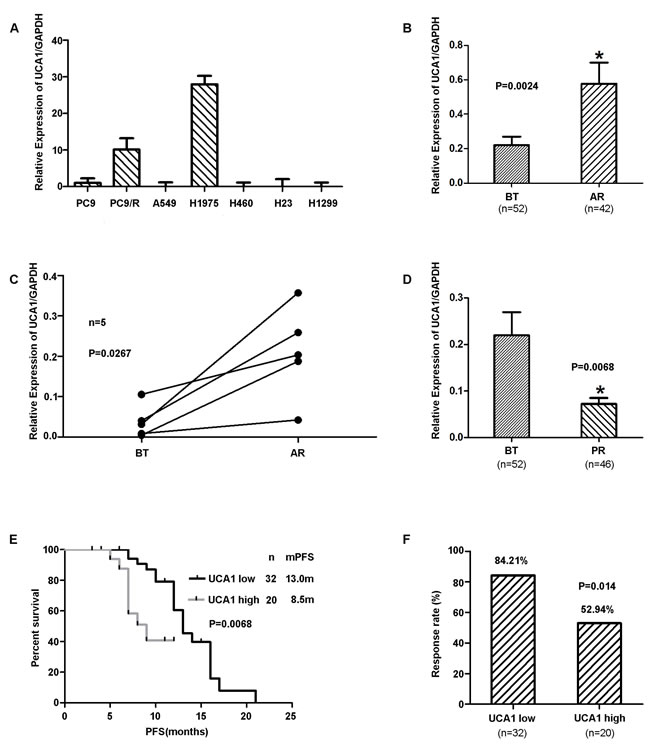
Figure 1: A. The expression of UCA1 in lung cancer cells. Over-expression of UCA1 was observed in lung cancer cells with acquired resistance (PC9/R and H1975cells); however, in primary resistant cells (A549, H460, H23 and H1299), UCA1 was down-regulated (P < 0.01). B. UCA1 expression levels in lung cancer tissues assessed by qRT-PCR in patients with EGFR-TKI-sensitive NSCLC (before treatment) and patients who developed acquired resistance to EGFR-TKIs. C. UCA1 expression levels assessed in 5 paired EGFR-mutant patients both before treatment and upon acquired resistance to EGFR-TKIs. D. UCA1 expression levels were assessed in EGFR-TKIs before treatment and primary resistance. E. Progression-free survival (PFS) in patients with high and low UCA1 expression levels before EGFR-TKI treatment. F. The objective response rate (ORR) in patients with high and low UCA1 expression levels before EGFR-TKI treatment. BT: before treatment; AR: acquired resistance; PR: primary resistance; PFS: progression-free survival.
The impact of over-expression of UCA1 on PFS for patients with acquired resistance to EGFR-TKIs was from T790M-negative subgroup
We observed the expression level of UCA1 was significantly higher in patients with acquired resistance to EGFR-TKIs regardless of the status of T790M mutation than in BT group (subgroup without T790M, 0.57 ± 0.24 vs 0.21 ± 0.05, P = 0.036; Figure 2A) (subgroup with T790M, 0.64 ± 0.18 vs 0.21 ± 0.05, P = 0.0028; Figure 2C). However, the expression of UCA1 was significantly associated with PFS in only patients without T790M mutations (P = 0.023; Figure 2B). The relationship was not observed in patients with T790M mutations (P = 0.778; Figure 2D). Therefore, we hypothesized that UCA1 may play an important role in acquired resistance to EGFR-TKIs in patients without T790M mutations.
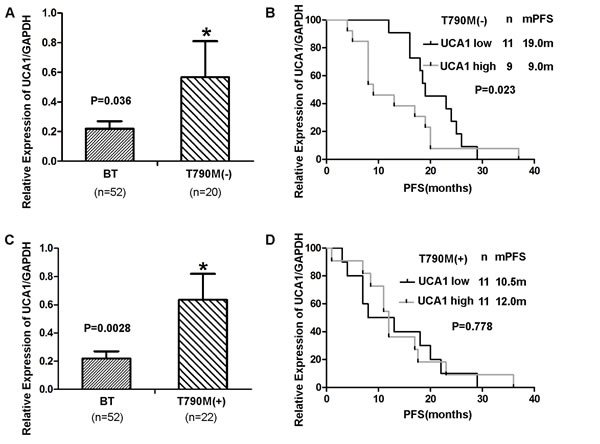
Figure 2: A., C. UCA1 expression levels assessed in patients treated with EGFR-TKI-sensitive NSCLC (baseline group) and patients who were without T790M and with T790M mutations. B., D. PFS in patients with acquired resistant patients who were without T790M mutations and with T790M mutations.
UCA1 inhibition restored gefitinib sensitivity in acquired resistant cell lines without T790M in vitro and in vivo
To assess the role of UCA1 in acquired resistance to EGFR-TKIs, the effect of UCA1 on cell proliferation and apoptosis was investigated. The silencing capacity of si-UCA1 was evaluated by using qRT-PCR. Si-UCA1-1 showed an optimal effect in comparison with si-UCA1-2 and the negative control (NC) (Figures 3A, 3C). After inhibiting the UCA1 gene, the sensitivity to gefitinib was partly restored in PC9/R cells, but this effect was not observed in H1975 cells (Figures 3B, 3D).
To further validate the effect of UCA1 on EGFR-TKI-resistant NSCLC cells in vivo, we established a gefitinib-resistant PC9/R model. Consistent with previous observations, we found that gefitinib plus si-UCA1 treatment inhibited tumor growth, but these changes were not observed in blank control and gefitinib plus negative control (NC)-treated tumors (Figure 3E, 3F). These results were consistent with our clinical data and further confirmed our hypothesis.
As refractoriness to apoptosis induced by EGFR-TKIs is one of the major features of resistance to targeted therapy in NSCLC, the effect of UCA1 on cell apoptosis was examined. We observed that caspase 3 and caspase 8 (the activation of which may be involved in cell apoptosis) were both increased by transfecting si-UCA1 (Figure 3G). A significantly higher percentage of apoptotic cells were found in si-UCA1-treated cells (26.8%) in comparison with those transfected with the negative control (7.9%) (Figure 3H). Taken together, these results indicate that inhibition of UCA1 induces apoptosis in cells resistant to EGFR-TKIs.
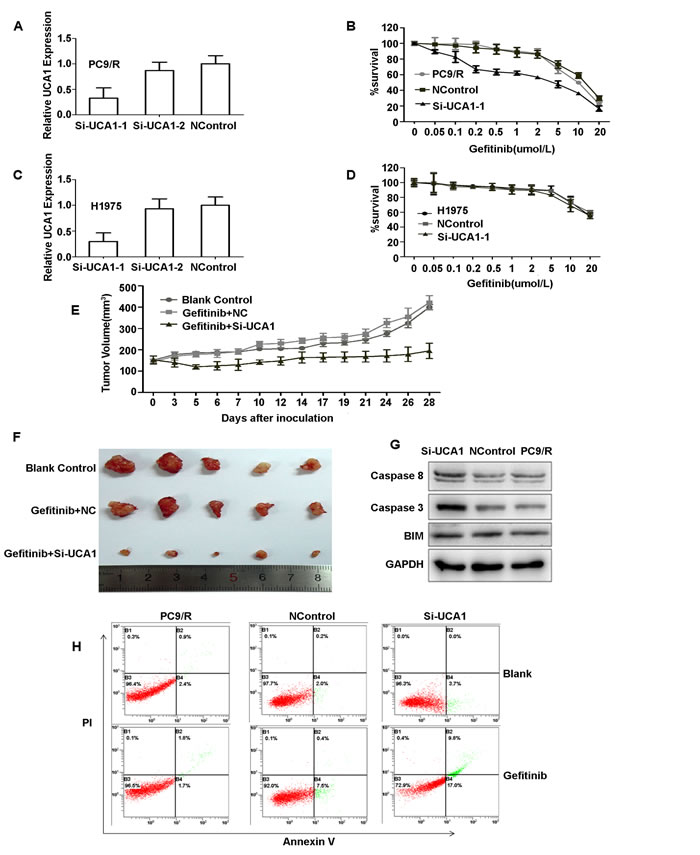
Figure 3: A., C. qRT-PCR detection of UCA1 expression in PC9/R and H1975 cells after silencing of UCA1 by si-RNA. The relative expression of UCA1 was 65% lower with si-UCA1 than with the negative control. B., D. The sensitivity to gefitinib of PC9/R and H1975 cells was detected by CCK-8 (Cell Counting Kit-8). Cells were exposed to various concentration of gefitinib for 72hours. Inhibiting the UCA1 gene resulted in an approximately 2-fold decrease in the gefitinib IC50 in PC9/R cells (IC50insi-UCA1-PC9/R and PC9/R cells, 7μmol/L and 15μmol/L, respectively), but the IC50 in H1975 cells was not changed (IC50, 20μmol/L). E., F. Tumor volumes of PC9/R cells transfected with si-UCA1, negative control (NC) and blank control after gefitinib treatment in vivo. After 4 weeks, tumor weights were represented as means ± SD. Western blot analysis G., caspase 3, caspase 8, and BIM(Bcl-2 interacting mediator of cell death). H. Gefitinib-induced apoptosis in PC9/R cells was demonstrated by flow cytometric analysis. Cells were treated with gefitinib for 72hours and then analyzed for early apoptotic cells (bottom right quadrant) and late apoptotic cells (top right quadrant).The percentages of cells in the two quadrants are shown.
UCA1 may promote activation of the PI3K/AKT/mTOR pathway and EMT
Based on the latest KEGG (Kyoto Encyclopedia of Genes and Genomes) database, a pathway analysis was performed for differentially expressed mRNAs in both PC9 and PC9/R cell lines before UCA1 knockdown. Among these, enriched pathways relating to mTOR signaling suggested a role in acquired resistance to EGFR-TKIs (Figure 4A). PI3K/AKT/mTOR and ERK are two crucial downstream signaling pathways for EGFR [17]. Therefore, to explore the underlying molecular mechanisms of EGFR-TKI resistance, we assessed whether UCA1 affects the expression of crucial proteins in these signaling pathways. Western blot analysis showed that the expressions of phospho-EGFR (pEGFR), phospho-AKT (pAKT), phospho-ERK (pERK), and phospho-mTOR (pmTOR) were positively correlated with the expressions of UCA1 among si-UCA1-treated PC9/R cells and negative control (NC)- treated PC9/R cells and non- treated PC9/R cells (Figure 4C), but the expressions of total EGFR, AKT, ERK, mTOR, MET, and pMET were not changed.
The mTOR inhibitor was effective in UCA1-expressing cell PC9/R, with IC50 of 8.3μmol/L. Inhibiting mTOR could change the expression of UCA1, although there was no significant difference. Therefore, we considered that UCA1 may have an impact on mTOR pathway(Supplementary Figure S4).
To confirm that si-UCA1 can inhibit PI3K/AKT and ERK signaling pathways in vivo, we assessed the expression of EGFR, pEGFR, AKT, pAKT, ERK, and pERK. Immunohistochemistry (IHC) revealed that the expression levels of pEGFR, pAKT and pERK were significantly higher in blank control and gefitinib plus NC-treated tumors than in gefitinib plus si-UCA1-treated tumors (Figure 4D) [Supplementary Figure S1]. Thus, these in vivo data complemented the functional studies of UCA1 in vitro in demonstrating that UCA1 is capable of promoting EGFR-TKI resistance in vivo. Accordingly, si-UCA1 may overcome gefitinib resistance which is not caused by T790M.
Epithelial-mesenchymal transition (EMT) plays a critical role in resistance to EGFR-TKIs, with a decrease of epithelial markers such as E-cadherin and an increase of mesenchymal markers such as vimentin [18, 19]. An association between UCA1 and markers of EMT was observed. The results indicated that knockdown of UCA1 enhanced the expression of E-cadherin, whereas the expression of vimentin, Snail, and N-cadherin were attenuated (Figure 4B).
Taken together, these findings indicate that the expression of UCA1 is positively correlated with pEGFR, pAKT, pERK and pmTOR, but is not related to MET. Thus, UCA1 may activate AKT/mTOR, ERK pathways and EMT to promote resistance to gefitinib.
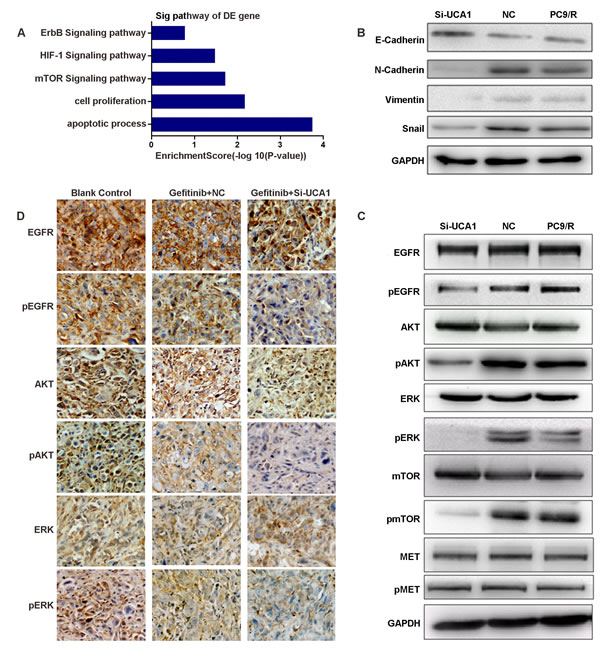
Figure 4: A. Signaling pathways of differentially expressed RNAs. B., C. Western blot analysis the proteins of epithelial-mesenchymal transition(EMT) and EGFR and its downstream proteins in si-UCA1-treated and negative control (NC)-treated PC9/R cells and non-treated PC9/R cells. D. Immunohistochemistry (IHC) revealed that pEGFR, pAKT and pERK were detected in control and gefitinib plus NC-treated tumors, but not in gefitinib plus si-UCA1-treated tumors. The experiments were repeated at least 3 times, and a representative one is shown.
Discussion
The majority of patients with EGFR-mutant lung cancers eventually develop acquired resistance to EGFR-TKIs [5, 6]. However, the mechanisms responsible for most patients with non-T790M acquired resistance to EGFR-TKIs are still unknown [10]. It is known that epigenetics especial non-coding RNAs play a key role in EGFR-TKIs resistance [20, 21]. In previous studies, we reported that miR-21, miR-214 and miR-200 are involved in both acquired resistance and primary resistance to EGFR-TKIs [22, 23]. However, lncRNAs can connect to transcription sites and regulate both the expression of alleles and a long fragment, whereas coding genes and micro-RNAs have no such functions, which suggests that lncRNAs may be better epigenetic regulators in controlling performance [24]. Moreover, the function of lncRNAs in the development of acquired resistance to EGFR-TKIs is still unknown. Therefore, we explored the role and possible molecular mechanism of lncRNAs in acquired resistance to EGFR-TKIs in NSCLC.
To gain insight into the molecular mechanisms of EGFR-TKI resistance, we compared the expression profile of lncRNAs between gefitinib-sensitive and gefitinib-resistant human lung cancer cells by lncRNA microarray and found that thousands of lncRNAs were up-regulated in gefitinib-resistant cells [16]. In addition, through bioinformatic analysis, we identified that the lncRNA-UCA1 is related to cell apoptosis, proliferation, and chemoresistance. UCA1 was first identified in bladder cancer cells and is involved in bladder cancer invasion and progression [25]. As it was observed that UCA1 is up-regulated in liver, colon and stomach cancers, it may be a biomarker for the diagnosis of these cancers [26, 27]. Of note, UCA1 has been shown to be up-regulated in lung cancer and induce chemoresistance [27].
One of important findings of this study was that over-expression of UCA1 in lung cancer cells and patients with acquired resistance to EGFR-TKIs. Our clinical data demonstrated that UCA1 expression levels were significantly higher in EGFR-mutant NSCLC patients who developed acquired resistance to EGFR-TKIs compared with before treatment levels, suggesting that high expression of UCA1 may be a mechanism of resistance to EGFR-TKIs. Meanwhile, the high expression of UCA1 was correlated with the poorer prognosis than those in the low expression group. Univariate and multivariate analysis of PFS revealed that UCA1 and age were independent prognostic factors. However, we found that over-expression UCA1 was not significantly associated with PFS for patients with T790M acquired resistance to EGFR-TKIs, although the significant high expression level of UCA1 in NSCLC with acquired resistance regardless of T790M status was observed. We therefore hypothesized that high expression of UCA1 may be one of the mechanisms of acquired resistance to EGFR-TKIs in EGFR-mutant NSCLC without T790M. We also validated the effect of UCA1 on EGFR-TKI resistance in NSCLC cells in vitro and in vivo.
In vitro, we observed that UCA1 knockdown can partly restore the sensitivity of PC9/R cells (19DEL, without T790M and MET amplification), but this change was not observed in H1975 cells (L858R/T790M). In vivo, we also found that gefitinib in combination with si-UCA1 inhibited tumor growth in gefitinib-resistant PC9/R model. The data were consistent with the cell experiments and further confirmed our hypothesis.
Our study also showed that UCA1-mediated acquired resistance to gefitinib may occur through activation of the AKT/mTOR pathway and EMT. Previous studies have implicated activation of the PI3K/AKT/mTOR and ERK pathways as well as EMT in resistance to EGFR-TKIs [28-30]. Subsequently, other studies have reported that UCA1 can promote cell proliferation and invasiveness by activating the PI3K/AKT pathway [31-33]. These studies confirm the validity of our results. In addition, the effects of UCA1 on cell proliferation and invasiveness in our study were similar to those of Nodal in breast cancer. Nodal has been demonstrated to promote invasiveness and metastasis in breast cancer cells via EMT and ERK pathway activation [34]. Besides, Li ZK et al. have reported that UCA1 promotes glycolysis through the mTOR pathway. They considered UCA1 was associated with the mTOR pathway [35]. Therefore, base on our data, we considered UCA1 may be associated with AKT/mTOR and ERK pathways and EMT. Further investigations will be required to elucidate the mechanisms by which UCA1 regulates the AKT/mTOR signaling pathway and EMT. We therefore hypothesized that UCA1-mediated acquired resistance in the absence of T790M mutations is likely to be related to activation of the AKT/mTOR and ERK pathways.
Recently, new generation EGFR-TKIs such as CO-1686 and AZD9291 have been found to be irreversible inhibitors that can overcome acquired resistance caused by T790M [36-39]. To date, however, patients without T790M mutations who develop acquired resistance to EGFR-TKIs have no effective treatment, as the mechanisms of acquired resistance remain unclear. Some studies have reported that the histone lysine-specific demethylase 1(LSD1) enzyme EZH2 may be a new “druggable” epigenetic target [40-42]. Therefore, we consider that UCA1 may play a key role in overcoming non-T790M acquired resistance to EGFR-TKIs by functioning as a new epigenetic regulator in NSCLC.
In conclusion, we have identified that UCA1 over-expression was significantly associated with poor outcome of NSCLC patients with acquired resistance to EGFR-TKIs and the impact of over-expression of UCA1 on PFS for patients with acquired resistance to EGFR-TKIs was from non-T790M subgroup. We consider over-expression of UCA1 as a novel mechanism by which acquired resistance to EGFR-TKIs can develop in EGFR-mutant NSCLC patients without T790M mutations. UCA1 may regulate resistance to gefitinib through activation of the AKT/mTOR pathway and EMT. Further studies will be required to elucidate the precise mechanisms of UCA1-mediated acquired resistance.
Materials and Methods
Cell culture and tissues collection
The human lung adenocarcinoma cell lines PC9 (EGFR exon 19 deletion), H1975 (L858R/T790M), A549 (EGFR wild-type), H460, H23, and H1299 were obtained from American Type Culture Collection (ATCC, Manassas, VA, USA). The gefitinib-resistant cell line PC9/R, which has no T790M and MET amplifications [43], was provided by Shanghai Pulmonary Hospital. All cells were cultured at 37°C in a humidified incubator with 5% CO2 in Dulbecco’s modified Eagle’s medium (DMEM) [Hyclone, Logan, UT, USA] supplemented with 10% fetal bovine serum(FBS) [Sigma Aldrich].
Ninety-four advanced lung adenocarcinoma tissues were collected from NSCLC patients who had either an exon 19 deletion (19DEL) or an exon 21 point mutation (L858R) in their EGFRs, and were treated with either gefitinib or erlotinib between January 2012 and December 2013, with the written consent of the patients involved and the approval of the Shanghai Pulmonary Hospital Ethics Committee. All patients had either prolonged stable disease (SD) of more than 6 months or a partial response (PR) to EGFR-TKIs therapy and 42 of 89 patients met the established clinical definition of acquired resistance to EGFR-TKIs [5]. Five of these 42 patients had available samples obtained before EGFR-TKIs treatment and after acquired resistance to EGFR-TKIs. Efficacy data were monitored until the end of June 2014. Of these 94 collected samples, 42 were collected from patients after they developed acquired resistance to EGFR-TKIs(defined as AR group), other 52 were collected from patients before EGFR-TKIs treatment(defined as BT group). Of note, there were 5 matched EGFR-mutant NSCLC samples.
We also collected fourty-six primary resistant patients. Primary resistance to EGFR-TKI was defined as progression on the first imaging evaluation or SD < 6 months after EGFR-TKI treatment in the first setting for patients with NSCLC harboring an activating EGFR mutation.
Quantitative reverse transcription polymerase chain reaction(qRT-PCR)
Total RNA was extracted from the lung cancer cell lines using TRIzol reagent (TaKaRa, Japan) or from tissue samples using an RNeasy Mini Kit(QIAGEN). The expression of UCA1 in lung cancer cell lines and tissues was measured by qPCR methodology using SYBR Premix Ex Taq (TaKaRa) and an MX3000P instrument. UCA1 primers were designed by Sangon Biotech (China). Glyceraldehyde 3-phosphate dehydrogenase(GAPDH) was used as a control. All experiments were performed in triplicate, and the median of each triplicate set of values was used to calculate relative lncRNA concentrations as follows:
△Ct (Cycle threshold) = Ct median lncRNA − Ct median GAPDH
Fold changes were calculated using 2−△△Ct methods.
Si-RNA transfection
PC9/R and H1975 lung cancer cells (2×105) were seeded into each well of 6-well plates and incubated overnight, and then transfected with 100nmol/L of small-interfering (si)-UCA1-1 or si-UCA1-2 and a negative control (NC) purchased from RiboBio (Guangzhou, China) that consisted of Lipofectamine 2000 transfection reagent (Invitrogen, USA). The target sequence for si-UCA1-1 was as follows:
sense strand, 5’-GCCACCUACAUUAAAGCUAdTdT-3’, antisense strand, 3‘-dTdT CGGUGGAUGUAAUUUCGAU-5’.
Forty-eight hours after transfection, the cells were harvested for real-time PCR or western blot analysis.
Cell proliferation and apoptosis assays
After transfection, the cells were seeded overnight at a density of 5×103 cells in 96-well plates in DMEM containing 10% FBS, and then exposed to various concentrations of gefitinib for 72hours. 10μLof CCK-8 reagent (Dojingdo Molecular Technology, Japan) was added to the cells for 1hour at 37°C, and the absorbance in each well was measured at 450 nm by an enzyme-labeled instrument.
The PC9/R cells were seeded in 6-well plates for 24hours and then transfected with si-UCA1-1 and the negative control. After gefitinib treatment for 72hours, the cells were trypsinized, washed twice with PBS, and resuspended in binding buffer. They were then stained with Annexin V/PI (Invitrogen, USA) for 15min in the dark at room temperature, and the cell populations were analyzed by a flow cytometer.
Western blot analysis
Cells were lysed using RIPA protein extraction reagent (Beyotime, Beijing, China) supplemented with phenylmethanesulfonyl fluoride (PMSF) [Riche, CA, USA]. Approximately 25µg of protein extracts were separated by 10% sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE), transferred onto nitrocellulose membranes (Sigma), and incubated with specific antibodies. An enhanced chemiluminescent (ECL) chromogenic substrate was used to visualize the bands. The blots were developed with a chemiluminescence system, and GAPDH was used as a control. All antibodies were purchased from Abcam(Cambridge, UK).
Xenograft study
For this part of the study, 5-week-old female specific pathogen-free (SPF) nude mice were used. The animal studies were approved by our Institutional Animal Care and Use Committee, and were performed according to institutional guidelines. PC9/R cells were injected into the right flanks of the mice, and gefitinib treatment was started 10 days after the tumor cell inoculation. Gefitinib was administered by oral gavage on 5 days per week at a dosage of 25mg/kg in 1% Tween 80 (Sigma). Si-UCA-1 or the negative control was administered as intratumoral injections.
Tumor sizes were assessed three times per week by a digital caliper. The tumor volumes were determined by measuring their length (l) and width (w) and calculating the volume (V) as follows: V = lw2/2. After 30 days, the mice were killed and paraffin-embedded tissues were prepared for immunohistochemical (IHC) staining.
Immunohistochemistry (IHC)
Formalin-fixed paraffin-embedded xenograft tumors 4µm thick were dewaxed in xylene, hydrated in graded alcohols, and washed with PBS. After blocking endogenous peroxidase activity with 3% H2O2 aqueous solution for 10 min, the sections were incubated with primary antibodies overnight. After washing with PBS, they were then incubated with general-type IgG-HRP Polymer (Beijing CoWin Biotech Co) for 10min, followed by 3, 3′-diaminobenzidine (DAB) for about 2 to 5min. Finally, the sections were restained with hematoxylin for 1 min and then dehydrated in graded alcohols, cleared in xylene, and covered with coverslips. We adopted the H-score system developed by Hirsch et al. and used by Pirker et al. in the FLEX study [44, 45] to calculate a score of intensity multiplied by the percentage of stained tumor cells. We used rabbit polyclonal to EGFR (1:100), pEGFR [pY1068](1:300), AKT (1:2000), pAKT [pS473](1:200), ERK (1:200), pERK [Thr202/Tyr204](1:400) as primary antibodies.
Statistical analysis
All statistical analyses were performed using SPSS version 17.0 software (SPSS, Inc., Chicago, IL, USA). Results were presented as the means ±standard deviation (SD) or Standard Error of Mean (SEM) of 3 separate assays. Differences between the different groups were assessed using a t-test (two-tailed). Cumulative survival was evaluated using the Kaplan-Meier method, and differences were assessed using the log-rank test. To determine independent prognostic factors, a Cox multivariate regression analysis was used. A P value < 0.05 was considered to indicate statistical significance.
Acknowledgments
This study was supported by grants from the National Natural Science Foundation of China (No.81372392 and 81172101) and the key project of the Science and Technology Commission of Shanghai Municipality (No.124119a800 and No.11JC1411301). Editorial support was provided by Content Ed Net, Shanghai Co. Ltd.
Conflicts of Interest
The authors declare no potential conflicts of interest.
References
1. Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, Zhou SW, Ren SX, Lu S, Zhang L, Hu CP, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735-742.
2. Keedy VL, Temin S, Somerfield MR, Beasley MB, Johnson DH, McShane LM, Milton DT, Strawn JR, Wakelee HA, Giaccone G. American Society of Clinical Oncology provisional clinical opinion: epidermal growth factor receptor (EGFR) mutation testing for patients with advanced non-small-cell lung cancer considering first-line EGFR tyrosine kinase inhibitor therapy. J Clin Oncol. 2011;29:2121-2127.
3. Han SW, Kim TY, Hwang PG, Jeong S, Kim J, Choi IS, Oh DY, Kim YT, Kim DW, Chung DH, Im SA, Kim YT, Lee JS, et al. Predictive and prognostic impact of epidermal growth factor receptor mutation in non-small-cell lung cancer patients treated with gefitinib. J Clin Oncol. 2005;23:2493-2501.
4. Somaiah N, Fidler MJ, Garrett-Mayer E, Wahlquist A, Shirai K, Buckingham L, Hensing T, Bonomi P, Simon GR. Epidermal growth factor receptor (EGFR) mutations are exceptionally rare in thyroid transcription factor (TTF-1)-negative adenocarcinomas of the lung. Oncoscience. 2014;1:522-528.
5. Gainor JF, Shaw AT. Emerging paradigms in the development of resistance to tyrosine kinase inhibitors in lung cancer. J Clin Oncol. 2013;31:3987-3996.
6. Wang Y, Xia H, Zhuang Z, Miao L, Chen X, Cai H. Axl-altered microRNAs regulate tumorigenicity and gefitinib resistance in lung cancer. Cell Death Dis. 2014;5:e1227.
7. Arcila ME, Oxnard GR, Nafa K, Riely GJ, Solomon SB, Zakowski MF, Kris MG, Pao W, Miller VA, Ladanyi M. Rebiopsy of lung cancer patients with acquired resistance to EGFR inhibitors and enhanced detection of the T790M mutation using a locked nucleic acid-based assay. Clin Cancer Res. 2011;17:1169-1180.
8. Bar J, Onn A. Overcoming molecular mechanisms of resistance to first-generation epidermal growth factor receptor tyrosine kinase inhibitors. Clin Lung Cancer. 2012;13:267-279.
9. Hammerman PS, Jänne PA, Johnson BE. Resistance to epidermal growth factor receptor tyrosine kinase inhibitors in non-small cell lung cancer. Clin Cancer Res. 2009;15:7502-7509.
10. Ohashi K, Maruvka YE, Michor F, Pao W. Epidermal growth factor receptor tyrosine kinase inhibitor-resistant disease. J Clin Oncol. 2013;31:1070-1080.
11. Esteller M. Non-coding RNAs in human disease. Nat Rev Genet. 2011;12:861-874.
12. Cheetham SW, Gruhl F, Mattick JS, Dinger ME. Long noncoding RNAs and the genetics of cancer. Br J Cancer. 2013;108:2419-2425.
13. Tsang WP, Kwok TT. Riboregulator H19 induction of MDR1-associated drug resistance in human hepatocellular carcinoma cells. Oncogene. 2007;26:4877-4881.
14. Tsang WP, Wong TW, Cheung AH, Co CN, Kwok TT. Induction of drug resistance and transformation in human cancer cells by the noncoding RNA CUDR. RNA. 2007;13:890-898.
15. Yang Y, Li H, Hou S, Hu B, Liu J, Wang J. The noncoding RNA expression profile and the effect of lncRNA AK126698 on cisplatin resistance in non-small-cell lung cancer cell. PLoS One. 2013;8:e65309.
16. Cheng NN, Li CF, Zhao C, Ren SX, Chen XX, Cai WJ, Zhao MC, Zhang YS, Li JY, Wang Q, Zhou CC. Microarray expression profile of long non-coding RNAs in EGFR-TKIs resistance of human non-small cell lung cancer. Oncology Rep. 2015;33:833-839.
17. Cappuzzo F, Magrini E, Ceresoli GL, Bartolini S, Rossi E, Ludovini V, Gregorc, V, Ligorio, C, Cancellieri, A, Damiani, S, Spreafico, A, Paties, C. T, Lombardo, L, et al. Akt phosphorylation and gefitinib efficacy in patients with advanced non-small-cell lung cancer. J Natl Cancer Inst. 2004;96:1133-1141.
18. Xie M, He CS, Wei SH, Zhang L. Notch-1 contributes to epidermal growth factor receptor tyrosine kinase inhibitor acquired resistance in non-small cell lung cancer in vitro and in vivo. Eur J Cancer. 2013;49:3559-3572.
19. Tam WL, Weinberg RA. The epigenetics of epithelial-mesenchymal plasticity in cancer. Nat Med. 2013;19:1438-1449.
20. Bird A. Perceptions of epigenetics. Nature. 2007;447:396-398.
21. Costa FF. Non-coding RNAs, epigenetics and complexity. Gene. 2008;410:9-17.
22. Li B, Ren S, Li X, Wang Y, Garfield D, Zhou S, Chen, X, Su, C, Chen, M, Kuang, P, Gao, G, He, Y, Fan, L, et al. MiR-21 overexpression is associated with acquired resistance of EGFR-TKI in non-small cell lung cancer. Lung Cancer. 2014;83:146-153.
23. Wang YS, Wang YH, Xia HP, Zhou SW, Schmid-Bindert G, Zhou CC. MicroRNA-214 regulates the acquired resistance to gefitinib via the PTEN/AKT pathway in EGFR-mutant cell lines. Asian Pac J Cancer Prev. 2012;13:255-260.
24. Wang Y, Chen W, Yang C, Wu W, Wu S, Qin X, Li X. Long non-coding RNA UCA1a(CUDR) promotes proliferation and tumorigenesis of bladder cancer. Int J Oncol. 2012;41:276-284.
25. Wang F, Li X, Xie X, Zhao L, Chen W. UCA1, a non-protein-coding RNA up-regulated in bladder carcinoma and embryo, influencing cell growth and promoting invasion. FEBS Lett. 2008;582:1919-1927.
26. Fan Y, Shen B, Tan M, Mu X, Qin Y, Zhang F, Liu Y. Long non-coding RNA UCA1 increases chemoresistances of bladder cancer cells by regulating Wnt signaling. FEBS J. 2014;281:1750-1758.
27. Li H, Schmid-Bindert G, Wang D, Zhao Y, Yang X, Su B, Zhou C. Blocking the PI3K/AKT and MEK/ERK signaling pathways can overcome gefitinib-resistance in non-small cell lung cancer cell lines. Adv Med Sci. 2011;56:275-284.
28. Rolfo C, Giovannetti E, Hong DS, Bivona T, Raez LE, Bronte G, Buffoni, L, Reguart, N, Santos, ES, Germonpre, P, Taron, M, Passiglia, F, Van Meerbeeck, JP, et al. Novel therapeutic strategies for patients with NSCLC that do not respond to treatment with EGFR inhibitors. Cancer Treat Rev. 2014;40:990-1004.
29. Yang C, Li X, Wang Y, Zhao L, Chen W. Long non-coding RNA UCA1 regulated cell cycle distribution via CREB through PI3-K dependent pathway in bladder carcinoma cells. Gene. 2012;496:8-16.
30. Hampton KK, Craven RJ. Pathways driving the endocytosis of mutant and wild-type EGFR in cancer. Oncoscience. 2014;1:504-512.
31. Wu W, Zhang S, Li X, Xue M, Cao S, Chen W. Ets-2 regulates cell cpoptosis via the Akt pathway,through the regulation of urothelial cancer associated1, a long non-coding RNA, in bladder cancer cells. PLoS One. 2013;8:e73920.
32. Tian Y, Zhang X, Hao Y, Fang Z, He Y. Potential roles of abnormally expressed long noncoding RNA UCA1 and Malat-1 in metastasis of melanoma. Melanoma Res. 2014;24:335-341.
33. Quail DF, Zhang G, Findlay SD, Hess DA, Postovit LM. Nodal promotes invasive phenotypes via a mitogen-activated protein kinase-dependent pathway. Oncogene. 2014;33:461-473.
34. Lee JT. Lessons from X-chromosome inactivation: long ncRNA as guides and tethers to the epigenome. Genes Dev. 2009;23:1831-1842.
35. Li ZK, Li X, Wu SZ, Xue M, Chen W. Long non-coding RNA UCA1 promotes glycolysis by upregulating hexokinase 2 through the mTOR–STAT3⁄microRNA143 pathway. Cancer Sci. 2014; 105:951-955.
36. Niu FY, Wu YL. Novel agents and strategies for overcoming EGFR TKIs resistance. Exp Hematol Oncol. 2014;3:2.
37. Peters S, Zimmermann S, Adjei AA. Oral epidermal growth factor receptor tyrosine kinase inhibitors for the treatment of non-small cell lung cancer: comparative pharmacokinetics and drug-drug interactions. Cancer Treat Rev. 2014;40:917-926.
38. Lee CC, Shiao HY, Wang WC, Hsieh HP. Small-molecule EGFR tyrosine kinase inhibitors for the treatment of cancer. Expert Opin Investig Drugs. 2014;23:1333-1348.
39. Cross DA, Ashton SE, Ghiorghiu S, Eberlein C, Nebhan CA, Spitzler PJ, Orme, J. P, Finlay, M. R, Ward, R. A, Mellor, M. J, Hughes, G, Rahi, A, Jacobs, V. N, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. 2014;4:1046-1061.
40. Qi W, Chan H, Teng L, Li L, Chuai S, Zhang R, Zeng J, Li M, Fan H, Lin Y, Gu J, Ardayfio O, Zhang J, et al. Selective inhibition of Ezh2 by a small molecule inhibitor blocks tumor cells proliferation. Proc Natl Acad Sci U S A. 2012;109:21360-21365.
41. Lan W, Zhang D, Jiang J. The roles of LSD1-mediated epigenetic modifications in maintaining the pluripotency of bladder cancer stem cells. Med Hypotheses. 2013;81:823-825.
42. Ding J, Zhang ZM, Xia Y, Liao GQ, Pan Y, Liu S, Zhang Y, Yan ZS. LSD1-mediated epigenetic modification contributes to proliferation and metastasis of colon cancer. Br J Cancer. 2013;109:994-1003.
43. Ju L, Zhou C, Li W, Yan L. Integrin beta1 over-expression associates with resistance to tyrosine kinase inhibitor gefitinib in non-small cell lung cancer. J Cell Biochem. 2010;111:1565-1574.
44. Hirsch FR, Varella-Garcia M, Bunn PA Jr, Di Maria MV, Veve R, Bremmes RM, Barón AE, Zeng C, Franklin WA. Epidermal growth factor receptor in non-small-cell lung carcinomas: correlation between gene copy number and protein expression and impact on prognosis. J Clin Oncol. 2003;21:3798-3807.
45. Pirker R, Pereira JR, von Pawel J, Krzakowski M, Ramlau R, Park K, de Marinis F, Eberhardt WEE, Paz-Ares L, Störkel, S, Schumacher, K-M, von Heydebreck, A, Celik, I, et al. EGFR expression as a predictor of survival for first-line chemotherapy plus cetuximab in patients with advanced non-small-cell lung cancer: analysis of data from the phase 3 FLEX study. Lancet Oncol. 2012;13:33-42.